Case report
An 87-year-old lady with hypertension being her only cardiovascular risk factor was investigated for dyspnoea and chest oppression three years ago, and acute coronary syndrome could be excluded. She stayed asymptomatic for a longer period, but was admitted again with similar symptoms and suspected atrial fibrillation.
Twice, 12-lead-ECG and cardiac biomarkers were within normal limits. 24-hour-Holter monitoring was ordered to document atrial fibrillation. Twenty hours later she was found unconscious in her room. Circulation was restored within five minutes after immediate mechanical and electrical resuscitation. The first documented rhythm had been ventricular fibrillation. As the 12-lead ECG then showed ST-segment elevation in all anterior leads, PCI of a critical stenosis of the proximal LAD was performed (Figure 1 and Figure 2). The patient fully recovered and was sent home ten days later.

Figure 1.
Critical stenosis of the RIVA (arrow).

Figure 2.
RIVA after PCI/stenting.
Analysis of the Holter ECG revealed that in a moment without ST depression or ST elevation in any of the three leads, an extrasystole with a relatively short coupling interval of 330 ms (QT interval just before the event: 430 ms) induced a fast ventricular tachycardia (Figure 3) at a heart rate of 260/min. Due to the severe anterior wall ischaemia, the ventricular tachycardia rapidly degenerated into ventricular fibrillation lasting until external defibrillation (Figure 4).
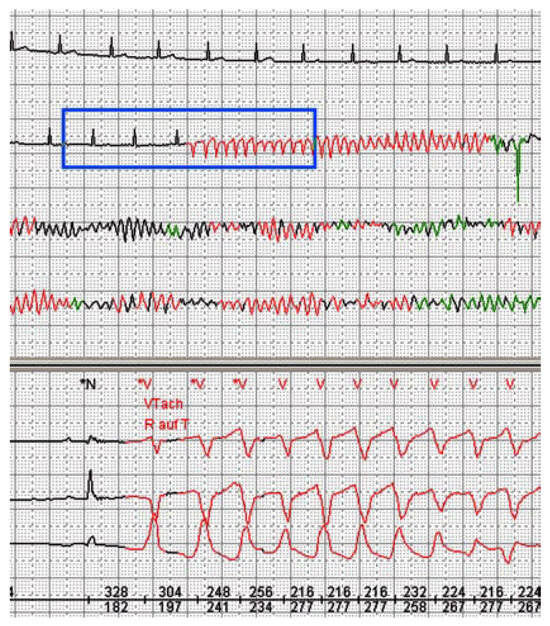
Figure 3.
Beginning of ventricular tachycardia.
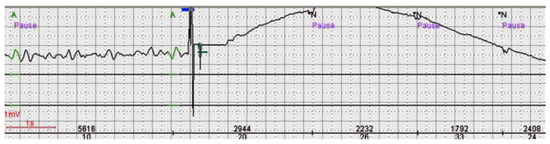
Figure 4.
Defibrillation (arrow) and restoration of sinus rhythm.
Discussion
Sudden cardiac death (SCD) in women has recently been investigated [1] in the nurses’ health study cohort. Ninety percent of SCD occurred outside of a hospital, the risk increased strongly with advancing age, and only 10% of affected patients experienced symptoms consistent with acute coronary syndrome in the three weeks before death. The vast majority of patients had at least one cardiovascular risk factor. Hypertension, eg, was associated with a threefold increased risk of SCD.
Primarily, it was thought that premature ventricular beats during early repolarisation (“R-on-T” phenomenon) might not initiate ventricular tachycardia or fibrillation [2]. However, a study done in patients with “variant angina” using Holter ECG showed different results [3]. During coronary artery occlusion, ie, at the beginning of coronary spasms, a short coupling interval of an extrasystole (around 50% of the preceding RR interval) was more successful to start ventricular tachycardia than longer intervals (p <0.00001).
Although the underlying pathology in our case was a fixed stenosis and not coronary spasm, the same fateful spiral was initiated leading to a fortunately aborted sudden cardiac death.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Albert, C.M.; Chae, C.U.; Grodstein, F.; Rose, L.M.; Rexrode, K.M.; Ruskin, J.N.; et al. Prospective study of sudden cardiac death among women in the United States. Circulation 2003, 107, 2096–2101. [Google Scholar] [CrossRef] [PubMed]
- Engel, T.R.; Meister, S.G.; Frankl, W.S. The “R-on-T” phenomenon: an update and critical review. Ann. Intern. Med. 1978, 88, 221–225. [Google Scholar] [CrossRef] [PubMed]
- Turitto, G.; Dini, P.; Prati, P.L. The R on T phenomenon during transient myocardial ischemia. Am. J. Cardiol. 1989, 63, 1520–1522. [Google Scholar] [CrossRef] [PubMed]




© 2008 by the authors. Attribution - Non-Commercial - NoDerivatives 4.0.