
A Systematic Umbrella Review of the Effects of Teledentistry on Costs and Oral-Health Outcomes

 ,
, 
 ,
,
Abstract
1. Introduction
1.1. The Need for Cost-Effective Care
1.2. Telehealth
1.3. Definition of Teledentistry and Related Terms
“Teledentistry represents the uses of information and telecommunication technology to provide oral healthcare services between an oral healthcare provider and a patient/recipient or other health care providers, who are separated by distance.”
1.4. The Current Study
2. Materials and Methods
2.1. Data Sources and Search Strategy
2.2. Eligibility Criteria
2.2.1. Design
2.2.2. Teledentistry Interventions
2.2.3. Population and Setting
2.2.4. Outcomes
2.2.5. Language
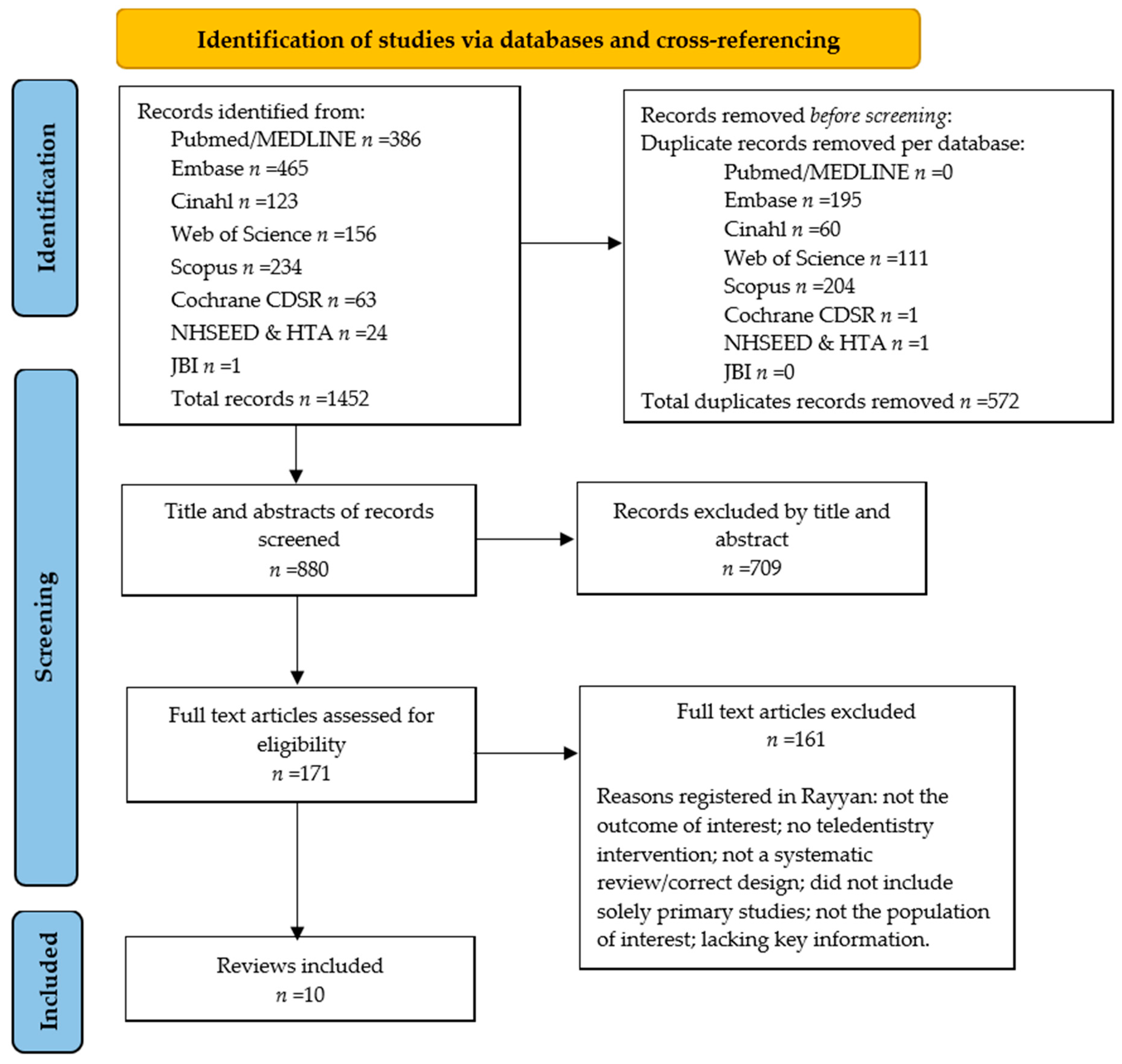
2.3. Study Selection
2.4. Data Extraction
2.5. Quality Assessment of the Selected Studies
2.6. Data Analysis
3. Results
3.1. An Overview of the Outcomes Reported by the Teledentistry Reviews
3.1.1. Oral-Health Outcomes
3.1.2. Economic Evaluations and Costs
3.2. Results of Quality Appraisal
4. Discussion
4.1. Main Findings
4.2. Quality Assessment of the Included Reviews
4.3. Strengths, Limitations and Recommendations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Deml, M.J.; Jungo, K.T.; Maessen, M.; Martani, A.; Ulyte, A. Megatrends in Healthcare: Review for the Swiss National Science Foundation’s National Research Programme 74 (NRP74) “Smarter Health Care”. Public Health Rev. 2022, 43, 1604434. [Google Scholar] [CrossRef] [PubMed]
- Ernst and Young. Health Reimagined: A New Participatory Health Paradigm. 2015. Available online: https://eysweeney.com.au/Documents/EYHealthReimagined2016.pdf (accessed on 22 December 2022).
- Day, G.E. Is our health workforce prepared for future health megatrends? Aust. Health Rev. 2015, 39, 487–488. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Strategy on Digital Health 2020–2025; Licence: CC BY-NC-SA 3.0 IGO; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- Butcher, C.J.; Hussain, W. Digital healthcare: The future. Future Healthc. J. 2022, 9, 113–117. [Google Scholar] [CrossRef] [PubMed]
- Gentili, A.; Failla, G.; Melnyk, A.; Puleo, V.; Tanna, G.L.D.; Ricciardi, W.; Cascini, F. The cost-effectiveness of digital health interventions: A systematic review of the literature. Front. Public Health 2022, 10, 787135. [Google Scholar] [CrossRef] [PubMed]
- Mariño, R.J.; Uribe, S.E.; Chen, R.; Schwendicke, F.; Giraudeau, N.; Scheerman, J.F.M. Terminology of e-Oral Health: Consensus Report of the IADR’s e-Oral Health Network Terminology Task Force. BMC Oral Health 2024, 24, 280. [Google Scholar] [CrossRef] [PubMed]
- Eze, N.D.; Mateus, C.; Cravo Oliveira Hashiguchi, T. Telemedicine in the OECD: An umbrella review of clinical and cost-effectiveness, patient experience and implementation. PLoS ONE 2020, 15, e0237585. [Google Scholar] [CrossRef] [PubMed]
- Mariño, R.; Ghanim, A. Teledentistry: A systematic review of the literature. J. Telemed. Telecare 2013, 19, 179–183. [Google Scholar] [CrossRef] [PubMed]
- Grant, M.J.; Booth, A. A typology of reviews: An analysis of 14 review types and associated methodologies. Health Inf. Libr. J. 2009, 26, 91–108. [Google Scholar] [CrossRef]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; PRISMA-P Group. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [PubMed]
- Aromataris, E.; Fernandez, R.; Godfrey, C.M.; Holly, C.; Khalil, H.; Tungpunkom, P. Summarizing systematic reviews: Methodological development, conduct and reporting of an umbrella review approach. Int. J. Evid. Based Health 2015, 13, 132–140. [Google Scholar] [CrossRef]
- Lima, I.F.P.; de Andrade Vieira, W.; de Macedo Bernardino, I.; Costa, P.A.; Lima, A.P.B.; Pithon, M.M.; Paranhos, L.R. Influence of reminder therapy for controlling bacterial plaque in patients undergoing orthodontic treatment: A systematic review and meta-analysis. Angle Orthod. 2018, 88, 483–493. [Google Scholar] [CrossRef] [PubMed]
- Al-Moghrabi, D.; Alkadhimi, A.; Tsichlaki, A.; Pandis, N.; Fleming, P.S. The influence of mobile applications and social media-based interventions in producing behavior change among orthodontic patients: A systematic review and meta-analysis. Am. J. Orthod. Dentofac. Orthop. 2022, 161, 338–354. [Google Scholar] [CrossRef] [PubMed]
- Fernandez, C.E.; Maturana, C.A.; Coloma, S.I.; Carrasco-Labra, A.; Giacaman, R.A. Teledentistry and mHealth for Promotion and Prevention of Oral Health: A Systematic Review and Meta-analysis. J. Dent. Res. 2021, 100, 914–927. [Google Scholar] [CrossRef]
- Hofmann, U.K.; Hildebrand, F.; Mederake, M.; Migliorini, F. Telemedicine in orthopaedics and trauma surgery during the first year of COVID pandemic: A systematic review. BMC Musculoskelet. Disord. 2023, 24, 101. [Google Scholar] [CrossRef] [PubMed]
- Van den Bosch, S.C.; van de Voort, N.E.M.; Xi, T.; Kool, R.B.; Bergé, S.J.; Faber, M.J. Oral & Maxillofacial surgery is ready for patient-centred eHealth interventions − the outcomes of a scoping review. Int. J. Oral Maxillofac. Surg. 2019, 48, 830–840. [Google Scholar]
- Drummond, M.F.; Sculpher, M.J.; Claxton, K.; Stoddart, G.L.; Torrance, G.W. Methods for the Economic Evaluation of Health Care Programmes; Oxford University Press: Oxford, UK, 2015; ISBN 978-0-19-164358-3. [Google Scholar]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan-a web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef] [PubMed]
- Bramer, W.M.; Giustini, D.; de Jonge, G.B.; Holland, L.; Bekhuis, T. De-duplication of database search results for systematic reviews in EndNote. J. Med. Libr. Assoc. 2016, 104, 240–243. [Google Scholar] [CrossRef] [PubMed]
- Shea, B.J.; Reeves, B.C.; Wells, G.; Thuku, M.; Hamel, C.; Moran, J.; Moher, D.; Tugwell, P.; Welch, V.; Kristjansson, E.; et al. AMSTAR 2: A critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ 2017, 358, j4008. [Google Scholar] [CrossRef] [PubMed]
- Al-Shammery, D.; Alqhtani, N.; Alotaibi, A.N.; AlSharidah, M.; AlShehri, K.; AlShamrani, A. Contributions and Concerns about the Use of Teledentistry in Clinical Orthodontics. Oral Health Prev. Dent. 2021, 19, 465–469. [Google Scholar]
- Dailah, H.G. Mobile Health (mHealth) Technology in Early Detection and Diagnosis of Oral Cancer-A Scoping Review of the Current Scenario and Feasibility. J. Health Eng. 2022, 2022, 4383303. [Google Scholar] [CrossRef] [PubMed]
- Da Silva, H.E.C.; Santos, G.N.M.; Ferreira Leite, A.; Mesquita, C.R.M.; de Souza Figueiredo, P.T.; Miron Stefani, C.; de Santos Melo, N. The feasibility of telehealth in the monitoring of head and neck cancer patients: A systematic review on remote technology, user adherence, user satisfaction, and quality of life. Support. Care Cancer 2022, 30, 8391–8404. [Google Scholar] [CrossRef] [PubMed]
- Kirkwood, B. Development of Military Teledentistry. Med. J. 2021, 33–39. [Google Scholar]
- Minervini, G.; Russo, D.; Herford, A.S.; Gorassini, F.; Meto, A.; D’Amico, C.; Cervino, G.; Cicciù, M.; Fiorillo, L. Teledentistry in the Management of Patients with Dental and Temporomandibular Disorders. BioMed Res. Int. 2022, 2022, 7091153. [Google Scholar] [CrossRef] [PubMed]
- Poirier, B.; Jensen, E.; Sethi, S. The evolution of the teledentistry landscape in Australia: A scoping review. Aust. J. Rural Health 2022, 30, 434–441. [Google Scholar] [CrossRef] [PubMed]
- Saccomanno, S.; Quinzi, V.; Albani, A.; D’Andrea, N.; Marzo, G.; Macchiarelli, G. Utility of Teleorthodontics in Orthodontic Emergencies during the COVID-19 Pandemic: A Systematic Review. Healthcare 2022, 10, 1108. [Google Scholar] [CrossRef] [PubMed]
- Soegyanto, A.I.; Siregar, K.N.; Maharani, D.A.; Wimardhani, Y.S. Teledentistry for Improving Oral Medicine Diagnosis: A Systematic Review. J. Int. Dent. Med. Res. 2022, 15, 365–369. [Google Scholar]
- Aljohani, M.A.B.; Alanazi, A.; Alotaibi, G. Effect of Teledentistry and Outcome for Dental Professionals at Saudi Arabia: A Systematic scoping Review. J. Res. Med. Dent. Sci. 2021, 9, 157–162. [Google Scholar]
- Aquilanti, L.; Santarelli, A.; Mascitti, M.; Procaccini, M.; Rappelli, G. Dental Care Access and the Elderly: What Is the Role of Teledentistry? A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 9053. [Google Scholar] [CrossRef] [PubMed]
- Ben-Omran, M.O.; Livinski, A.A.; Kopycka-Kedzierawski, D.T.; Boroumand, S.; Williams, D.; Weatherspoon, D.J.; Iafolla, T.J.; Fontelo, P.; Dye, B.A. The use of teledentistry in facilitating oral health for older adults: A scoping review. J. Am. Dent. Assoc. 2021, 152, 998–1011.e17. [Google Scholar] [CrossRef] [PubMed]
- Costa, C.; Peralta, F.; Mello, A. How Has Teledentistry Been Applied in Public Dental Health Services? An Integrative Review. Telemed. e-Health 2020, 26, 945–954. [Google Scholar] [CrossRef] [PubMed]
- Flores, A.; Lazaro, S.; Molina-Bastos, C.; Guattini, V.; Umpierre, R.; Goncalves, M.; Carrard, V.C. Teledentistry in the diagnosis of oral lesions: A systematic review of the literature. J. Am. Med. Inform. Assoc. JAMIA 2020, 27, 1166–1172. [Google Scholar] [CrossRef] [PubMed]
- Daniel, S.; Wu, L.; Kumar, S. Teledentistry: A systematic review of clinical outcomes, utilization and costs. J. Dent. Hyg. JDH/Am. Dent. Hyg. Assoc. 2013, 87, 345–352. [Google Scholar]
- Emami, E.; Harnagea, H.; Shrivastava, R.; Ahmadi, M.; Giraudeau, N. Patient satisfaction with e-oral health care in rural and remote settings: A systematic review. Syst. Rev. 2022, 11, 234. [Google Scholar] [CrossRef] [PubMed]
- Estai, M.; Kanagasingam, Y.; Tennant, M.; Bunt, S. A systematic review of the research evidence for the benefits of teledentistry. J. Telemed. Telecare 2018, 24, 147–156. [Google Scholar] [CrossRef] [PubMed]
- Irving, M.; Stewart, R.; Spallek, H.; Blinkhorn, A. Using teledentistry in clinical practice, an enabler to improve access to oral health care: A qualitative systematic review. J. Telemed. Telecare 2018, 24, 129–146. [Google Scholar] [CrossRef] [PubMed]
- Joshi, V.; Bhardwaj, P.; Joshi, N.; Singh, K.; Bajaj, K.; Suthar, P. A Scoping review of challenges, scope and assessment approaches of teledentistry: An Indian perspective. Indian J. Community Health 2021, 33, 559–567. [Google Scholar] [CrossRef]
- Uhrin, E.; Domokos, Z.; Czumbel, L.; Kói, T.; Hegyi, P.; Hermann, P.; Borbély, J.; Cavalcante, B.G.N.; Németh, O. Teledentistry: A Future Solution in the Diagnosis of Oral Lesions: Diagnostic Meta-Analysis and Systematic Review. Telemed. J. E Health 2023, 29, 1591–1600. [Google Scholar] [CrossRef] [PubMed]
- Oxford Centre for Evidence-Based Medicine. Levels of Evidence; Oxford Centre for Evidence-Based Medicine: Oxford, UK, 2009; Available online: https://ec.europa.eu/health/scientific_committees/scheer/docs/sunbeds_co241_en.pdf (accessed on 22 December 2023).
- Hrynyschyn, R.; Prediger, C.; Stock, C.; Helmer, S.M. Evaluation Methods Applied to Digital Health Interventions: What Is Being Used beyond Randomised Controlled Trials?—A Scoping Review. Int. J. Environ. Res. Public Health 2022, 19, 5221. [Google Scholar] [CrossRef] [PubMed]
- Bergmo, T.S. Can economic evaluation in telemedicine be trusted? A systematic review of the literature. Cost Eff. Resour. Alloc. 2009, 7, 18. [Google Scholar] [CrossRef] [PubMed]
- Belbasis, L.; Bellou, V.; Ioannidis, J. Conducting umbrella reviews. BMJ Med. 2022, 1, e000071. [Google Scholar] [CrossRef] [PubMed]
- Council of Australian Governments; Oral Health Monitoring Group. Healthy Mouths, Healthy Lives: Australia’s National Oral Health Plan 2015–2024; COAG: Canberra, Australia, 2015. Available online: http://www.coaghealthcouncil.gov.au/Publications/Reports/ArtMID/514/ArticleID/81/Australias-National-Oral-Health-Plan-2015-2024 (accessed on 22 December 2023).
- Batra, P.; Tagra, H.; Katyal, S. Artificial Intelligence in Teledentistry. Discoveries 2022, 10, 153. [Google Scholar] [CrossRef]


{kind=link}
| Reference | Type of Review and Study Objective Mentioned in the Review | Teledentistry Modalities and Application Researched | (4) Participant Details; (5) Setting and Context. | (6) Number of Databases Sourced and Searched; (7) Date Range of Database Searching; (8) Publication Date Range. | (9) Number of Studies, Types of Studies and Country of Origin of Studies Included in Each Review. | (10) Instrument Used to Appraise the Primary Studies and the Rating of Their Quality. | Main Findings |
|---|---|---|---|---|---|---|---|
| Aquilanti et al. (2020) [31] | The aim of the systematic review is to assess the feasibility of teledentistry in the provision of oral healthcare to older adults living in residential aged-care facilities. In particular, the review focused on the evaluation of the accuracy and the effectiveness of teledentistry compared to traditional face-to-face dental visits, the patient acceptability, and the costs related to the implementation of oral-health information technology provision. | Both synchronous and real-time teledentistry. Results for different types of teledentistry applications are not mentioned. | (4,5) Studies involving elderly people in nursing homes, in communities, or within in-home assistance were included. Young persons were excluded. | (6) n = 5; PubMed, Cochrane Library, Web of Science, Scopus and CINAHL databases. (7) Until 30 June 2020 (8) 2024–2018 | (9) Six studies were included in the review, but only three studies measured the outcome of interest (two measured the effects of teledentistry on indirect costs and one measured cost analyses). Types of studies measuring the effects on costs and indirect costs included a pilot study with a cost analysis; at 6 months, a quality-improvement study and cost analysis and a cost-analysis comparison study; a multicentre, cross-sectional study; and a mixed-methods comparative study. The included studies were performed in Australia, France and Germany. | (10) The quality of the studies included in the review was evaluated by the two independent reviewers using the protocol described by Hailey et al. The overall quality score/the strength of evidence was defined by both the performance and study design. The review included mostly articles with poor or poor to fair quality, characterized by substantial limitations in the study and only one with fair to good quality. The quality assessment of the studies that included a cost analysis was performed in accordance with the Drummond et al. 10-point checklist. | The review included three studies reporting on the economic evaluations of teledentistry. Teledentistry was found to be as cost-effective as traditional face-to-face dental examinations. |
| Ben-Omran et al. (2021) [32] | The aim of the scoping review was to systematically explore and describe the literature on various uses of teledentistry in older adults, including its reported effectiveness and limitations. | Both synchronous and real-time teledentistry. Types of teledentistry applications researched are tele-consultation, tele-diagnoses and tele-intervention. | (4) Older adult population (≥60 years) (5) Medical and dental settings: academia, private practice, community clinics or hospital (nursing home, dentist practice, pharmacy, community dental clinic, hospital, academic institution, long-term facilities, primary care clinics and private clinics). | (6) n = 9 PubMed/MEDLINE (National Library of Medicine), Cochrane Library: Database of Systematic Reviews, Cochrane Library CENTRAL, Embase, Scopus, Web of Science Core Collection, Cumulative Index of Nursing and Allied Health Literature (CINAHL), Health Technology Assessment database, and National Health Service Economic Evaluations Database. (7) Searches were conducted in January 2020 (8) and limited to articles published from 1991 through to 2020. | (9) n = 19, (of which n = 4 measured the effects of teledentistry on costs—only one study included a cost analysis). Types of studies: non-rct; cross-sectional; rct; and observational with mixed retrospective and prospective designs. Countries: Japan, United States, Northern Ireland, China, Australia, United Kingdom, Brazil, France, India, Germany, Finland, and Portugal. | (10) The instrument used to appraise the primary studies was not mentioned in the article. The only mentioned in the discussion the overall rating of their quality (unclear how this was measured): “A limitation was the quality of the studies included, as many were cross-sectional studies with no clear methodology stated, non-RCTs with small sample sizes, or clinical trials that were dependent on self-reports or subjective opinions of participants or their caregivers.” | The authors identified cost reductions as a result of reducing avoidable dental visits to nurses with the guidance of a remote-dentist model. No significant difference was found between intervention and control groups in terms of Geriatric Oral Health Assessment Index scores, measuring the oral-health-related quality of life. Despite positive findings, Ben-Omran and his colleagues concluded that there was insufficient evidence to firmly advocate for the long-term clinical effectiveness of teledentistry. |
| Da Costa et al. (2019) [33] | The purpose of this integrative review was to collect information regarding the inclusion of the application of teledentistry tools in the public dental-health services. | Types of teledentistry applications researched are tele-diagnosis and tele-screening. | (4) a wide range of dental-patient groups, including paediatric, orthodontic and elderly patients, as well as prisoners. (5) Dental public-health services, including dental-health programs or dental-health-related actions taken at a community, state or federal level. | (6) Searches were conducted on five electronic databases (PubMed/Medline, Virtual Health Library, CINAHL, Scopus and Web of Science); (7) studies that were published from 2007 to June 2019 were included. (8) Publication date range: 2007–2018 | (9) Twenty-four studies were included, of which four measured the outcome of interest: economic evaluation (two in paediatric dentistry, one in older adults and one in oral medicine). Types of studies included economic evaluations, exploratory descriptive studies, mixed-method comparative studies; cost-minimization analyses; cross-sectional studies. Country-of-origin of studies: Australia and Brazil. | (10) Due to the variety of research methods employed in the included studies, the mixed-methods appraisal tool (MMAT) was used to assess their quality. Among the 24 studies that met the eligibility criteria, 7 studies could not be assessed using MMAT because they did not have enough information regarding the methods and criteria that were employed; however, the remaining 17 studies were assessed using MMAT. Most of them (14 studies) had good-quality scores, meeting three or more of the four criteria. Furthermore, three studies were considered to have moderate-quality scores, meeting only two of the four criteria. | The authors concluded that teledentistry is cost-effective; however, no in-depth economic design is presented. |
| (Da Costa) Flores et al. (2020) [34] | The purpose of this systematic review is to summarize information on the use of teledentistry in the telediagnosis of oral lesions. | The type of teledentistry application and modulation were not mentioned. | (4, 5) Dental-clinic community patients (n = 41) | (6) Four databases: PubMed, Embase, LILACS (Latin American and Caribbean Literature in Health Sciences and SUMSearch. The CAPES (bancodetes.capes.gov.br/) and Google Scholar databases were used to identify additional grey literature. (7) articles published until December 2018. (8) Range: 1999–2018; the included study was performed in 2010 | (9) Eleven studies were included, of which only one feasibility study performed in New Zealand reported on the outcome of interest; | (10) The bias risk and quality analyses of the study were performed independently by two authors using the Quality Assessment of Diagnostic Accuracy Studies questionnaire. The original study presented good quality, as 12 out of 14 questions were answered with yes. | The authors concluded that teledentistry is likely to be a cost-effective alternative compared with the standard practice of face-to-face consultation. However, this contention is not supported for any economic evaluation. |
| Daniel et al. (2013) [35] | The purpose of this systematic review is to identify clinical outcomes, healthcare utilization and costs associated with teledentistry. | Types of teledentistry applications researched are tele-triage and tele-screening. | (4) In the review of Daniel et al., there is no data-extraction table present nor did the text describe the participants’ details, setting and context for each original study, so we are unable to give a precise overview of the participants details of the original studies. Mentioned in the text: preschool urban children and orthodontics. | (6) Literature searches were conducted in 15 databases: PubMed/Medline, EMBASE, CINAHL with Full Text, PsychINFO, EBM Reviews (e.g., Cochrane Database of Systematic Reviews, ACP Journal Club, Database of Abstracts of Reviews of Effects, Cochrane Central Register of Controlled Trials, Cochrane Methodology Register, Health Technology Assessment and NHS Economic Evaluation Database), Scopus, Education Resource Information Center (ERIC), Google Scholar and Turning Research into Practice (TRIP). (7) Publication date from the earliest available date for each database to March 2012. (8) Publication dates ranged from 2009–2019 | (9) Nineteen studies were included, of which four of the included original studies measured the outcome of interest. Cost-analysis and comparative effectiveness study. The country of origin of the cost-analysis study is United Kingdom | (10) The instrument that was used to appraise the primary studies and rate their quality was not described in the review. The discussion stated the following: Common methodological weaknesses in these studies included the lack of blinding of dentists, patients or assessors. While in teledentistry it is not always feasible to design studies with patients and dentists who are not aware of the group assignment, the use of outside assessors reduces the potential for evaluation bias. Many of the studies used convenience samples based on the geographical location of patients or patient preference, clearly introducing the possibility of selection bias. A total of 12 studies (60%) had sample sizes of fewer than 20 subjects, and only 1 of the studies provided power calculations. Small sample sizes can lead authors to conclude that no significant difference exists between groups, i.e., a type-II error, whereas the study may have insufficient power to identify a significant difference. Nevertheless, larger studies often remain challenging to carry out, as many of the teledentistry programs are still in their pilot phases and there is often a limited availability of the patient population concerned. | In terms of economic evaluation, one study concluded on the cost-effectiveness of the teledentistry approach. |
| Emami et al. (2022) [36] | This systematic review evaluated the literature on patient satisfaction with e-oral healthcare in rural and remote communities. | The teledentistry application researched is tele-consultation. Most studies used teledentistry consultations, either live or store-and-forward. | (4) Participant details not reported; (5) in rural and remote settings. | (6) Searches were carried out in four databases: Cochrane Central Register of Controlled Trials, MEDLINE, EMBASE and Global Health. (7) date range of database searching: published between 1946 and 2021; (8) publication date range: studies carried out in 1998 and 2019 | (9) In total, 16 studies were included in the review, of which 7 studies focused on the outcome of interest.The types of studies comprised non-randomized clinical trials, observational studies, pilot intervention studies and cost analyses. In total, five studies were from Australia, three from India, two studies were conducted in the USA, two in Spain, one in Canada, one in the UK, one in Italy, and one in Finland. | (10) The risk of bias using the ROBINS-I risk-of-bias assessment tool for non-randomized studies. Thirteen of the selected studies were found to have a moderate risk of bias, and two other studies had critical risk in the overall assessment. One article was found to be ineligible for performing risk for bias assessment using the ROBINS-I tool. The majority of studies (11 out of 16) were considered level 4 and 3b. | Only a few studies reported the cost per unit of outcomes gained; rather, the level of satisfaction was related to reduced waiting time, the number of visits, travel, and the cost of care for patients. The review also commented on the heterogeneity and inconsistency of methodologies of the studies reviewed in terms of study design, perspective, sampling, setting, etc. |
| Estai et al. (2018) [37] | This systematic review of the benefits of teledentistry aims to inform decisionmakers who are doubtful about the capability and merit of integrating teledentistry into routine health services by presenting an objective overview of good-quality evidence for the effectiveness and economic impact of teledentistry. | Studies were clustered into two major applications, telediagnosis and teleconsultation. | (4) The majority of the reviewed studies were solely focused on the specialty of oral medicine, paediatric dentistry and orthodontics. (5) The majority of the reviewed articles did not explicitly report the setting of the study (rural or urban); however, it appears that studies were carried out in either urban or rural settings such as hospitals, clinics, childcare centres or workplaces. | (6) n = 3; PubMed, EMBASE and CINAHL databases (7) Through November 2016 (8) 2001–2016 | (9) n = 6; This review included three studies that performed economic evaluations. Of these, two studies were deemed to be of fair to good quality. The review included nine articles considering various clinical outcomes, of which three studies specifically addressing on the clinical outcome of interest, i.e., DFS scores, periodontal indices and oral hygiene scores. The studies included in the review were conducted in seven different countries, with the majority of studies from Europe (n = 5) and the USA (n = 3), with one each from Japan, India and Australia | (10) The quality of each study, other than those aspects related to economic analysis, was evaluated independently by two authors using the protocol established by Hailey et al., taking into account the study performance and study design. | Despite the diverse objectives, methodologies and outcome measures employed across the included studies, teledentistry interventions were comparable to, or had advantages over, non-telemedicine approaches. However, Estai and his colleagues’ overall conclusion was that there is not yet enough conclusive evidence for the effectiveness and long-term use of teledentistry. |
| Irving et al. (2017) [38] | This qualitative systematic review aims to explore the quantitative and qualitative framework associated with the effectiveness of teledentistry in an effort to uncover the interaction of multiple influences on its delivery and sustainability. | The teledentistry application researched is tele-consultation. | (4) General dental patients/orthodontics, oral-surgery patients, hospital-referral patients and adults with tetraplegia. (5) Dental practice in both general and specialist dental settings | (6) Literature searches were conducted in nine databases: MEDLINE, Embase, CINAHL, PsychINFO, AMED, EBM Reviews, ERIC, Global Health and PREMEDLINE databases. We also searched the grey literature. (7) Database searches were conducted on 5 January 2015. (8) Publication date range: 2001–2013 | (9) In total, 19 studies were included, but only 4 studies measured the outcome of interest. Study type: practitioner cohort, patient cohort and controlled trial. The country of origin of studies included in each review: UK (n = 2), Spain (n = 2) and USA. | (10) A modified Downs and Black criterion scale, which examines validity, bias, power and other study attributes, was used to assess the methodological quality of the included papers. They modified the original Downs and Black scale, as described and recommended in prior methodological systematic reviews, to exclude items that were not applicable to the designs of eligible studies. For example, items specific to randomized trials were removed for observational studies. A percentage quality score was calculated by dividing the total score received by the maximum score possible for each study. The majority of included studies were only rated as being of fair quality. The majority of the studies were reported on by the developers of the programs, creating a possible opportunity for a bias in the reporting of the results included from the studies. | The review concluded that teledentistry is a cost-saving alternative to conventional practice. However, the reduction of costs and cost-effectiveness is assumed, as no actual reviews of economic evaluation in teledentistry were provided. |
| Joshi et al. (2021) [39] | The aim of the scoping review was to identify the challenges, scope and assessment approaches of teledentistry from an Indian perspective. | Both synchronous and real-time teledentistry. Types of teledentistry applications researched are tele-consultation, tele-diagnoses and tele-screening. | (4, 5) Not described | (6) n = 3; Google Scholar, PubMed/Medline and Scopus; (7) searched from April to August 2020; (8) publication dates ranged | (9) Twenty studies were included in the scoping review. Only five studies reported on the outcome of interest. Types of studies were not reported; however, the review did report on the type of analyses. Analyses that have been carried out included cost-minimization analyses, cost-effectiveness analyses, model-based and cost-effectiveness analyses, and teledental asynchronous patient assessments and remote real-time oral examination. The review did not report on the countries of origin of studies. | (10) It did not assess the rigor or quality of studies. Note: outcomes were not described in detail, E.g., it was stated “Teledentistry is a cost-saving”, but no details on the design or outcome were reported. | The authors concluded that the use of teledentistry is potentially cost-effective and cost-saving compared to traditional dentistry. However, none of the studies conducted in India provide any support for that assumption. |
| Uhrin et al. (2023) [40] | The aim of the systematic review was to collect available data on how oral medicine could benefit from teledentistry solutions, and to investigate whether teledentistry could provide a reliable diagnostic method compared with clinical oral examination (COE) in the diagnosis of oral potentially malignant disorders. | Virtual examination. | (4, 5) The review included adults with suspected oral lesions. One of the included articles that measured the outcome of interest included patients of a special care clinic, with intellectual disability, cerebral palsy, Down’s syndrome, autism, seizures, HIV, liver disease, neurologic disorders, stroke or schizophrenia; the other article included <18-year-old patients referred to the clinic with oral lesions. The mean age of the population was 47 (n = 29) and 50 (n = 33). | (6) Three databases (Medline, EMBASE and CENTRAL); (7) date of searching: until November 2021. (8) Publication dates ranged | (9) Thirteen studies were included; however, only two studies investigated the outcome of interest: time effectiveness. These studies included an observational study and a cross-sectional study. The review included a meta-analysis for the primary outcome, but not for the secondary outcome. These were only described narratively. One study was conducted in the US and the other one in Brazil. | (10) Risk of bias was assessed using the QUADAS-2 tool. Certainty of evidence was evaluated based on the Grades of Recommendation, Assessment, Development and Evaluation (GRADE) workgroup’s recommendations. Four articles were excluded due to a lack of data. The QUADAS-2 tool showed that most of the domains had a low risk of bias. | The authors performed a meta-analysis on the primary outcomes; however, no statistical analysis could be performed on the secondary outcome’s time-effectiveness. One of the original studies measured the difference in time during in-person examinations (mean: 4.2 min, SD: 1.6) and virtual examinations (2.83 min, SD: 1.0). |
| Review First Author (Year) | Q1 | Q2 | Q3 | Q4 | Q5 | Q6 | Q7 | Q8 | Q9 | Q10 | Q11 | Q12 | Q13 | Q14 | Q15 | Q16 | Overall Quality |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Aquilanti et al. (2020) [31] | Y | P | N | P | Y/U | Y | N | N | N | N | N/A | N/A | N | N | N/A | Y | Critically Low Quality |
| Ben-Omran et al. (2021) [32] | Y | N | N | N | Y | N | N | N | N | N | N/A | N/A | N | N | N/A | N | Critically Low Quality |
| Da Costa et al. (2019) [33] | N | N | N | P | Y | Y | N | N | U/N | N | N/A | N/A | N | N | N/A | Y | Critically Low Quality |
| (Da Costa) Flores et al. (2020) [34] | N | P | N | P | Y | Y | N | N | U | N | N/A | N/A | N | N | N/A | Y | Critically Low Quality |
| Daniel et al. (2013) [35] | Y | N | N | N | N | N | N | N | N | N | N/A | N/A | N | Y | N/A | N | Critically Low Quality |
| Emami et al. (2022) [36] | Y | Y | N | P | Y | Y | N | Y | Y | N | N/A | N/A | Y? | N | N/A | Y | Low Quality |
| Estai et al. (2018) [37] | Y | N | Y | P | Y | Y | N | Y | Y | N | N/A | N/A | Y | Y | N/A | Y | Critically Low Quality |
| Irving et al. (2017) [38] | Y | N | N | P | Y | Y | N | Y | Y | N | N/A | N/A | Y | Y | N/A | Y | Critically Low Quality |
| Joshi et al. (2021) [39] | N | N | N | N | Y | Y | N | N | N | N | N/A | N/A | N | N | N/A | N | Critically Low Quality |
| Uhrin et al. (2023) [40] | Y | P | N | P | Y | Y | N | Y | Y | N | N/A | N/A | Y | Y | N/A | Y | Low Quality |
| Assessment Questions | |||||||||||||||||
| Critical domains (grey highlight) | Q2: Protocol registration Q4: Adequacy of the literature search Q7: Justification for excluding studies Q9: Risk of bias from studies included in review Q11: Appropriateness of meta-analytical methods Q13: Consideration of risk of bias in the interpretation of results Q15: Assessment of presence and likely impact of publication bias. | ||||||||||||||||
| Non-critical domains (no highlight) | Q1: Inclusion of PICO elements in review question Q3: Explain selection of study design Q5: Duplicate study selection Q6: Duplicate data extraction Q8: Description of studies Q10: Report sources of funding for primary studies Q12: Impact of risk of bias assessment on evidence Q14: Explanation for heterogeneity Q16: Report potential conflicts of interest and funding sources by review authors. | ||||||||||||||||
| Grading criteria | |||||||||||||||||
| Y (Yes): Criterion met; “P” (Partial yes): Criterion partly met; “N” (No): Criterion not met; “N/A” (Not applicable), U (Unclear) | |||||||||||||||||
| High Quality | No or one non-critical weakness | ||||||||||||||||
| Moderate Quality | More than one non-critical weakness | ||||||||||||||||
| Low Quality | One critical flaw with or without non-critical weaknesses | ||||||||||||||||
| Critically Low Quality | More than one critical flaw with or without non-critical weaknesses | ||||||||||||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Scheerman, J.F.M.; Qari, A.H.; Varenne, B.; Bijwaard, H.; Swinckels, L.; Giraudeau, N.; van Meijel, B.; Mariño, R. A Systematic Umbrella Review of the Effects of Teledentistry on Costs and Oral-Health Outcomes. Int. J. Environ. Res. Public Health 2024, 21, 407. https://doi.org/10.3390/ijerph21040407
Scheerman JFM, Qari AH, Varenne B, Bijwaard H, Swinckels L, Giraudeau N, van Meijel B, Mariño R. A Systematic Umbrella Review of the Effects of Teledentistry on Costs and Oral-Health Outcomes. International Journal of Environmental Research and Public Health. 2024; 21(4):407. https://doi.org/10.3390/ijerph21040407
Chicago/Turabian StyleScheerman, Janneke F. M., Alaa H. Qari, Benoit Varenne, Harmen Bijwaard, Laura Swinckels, Nicolas Giraudeau, Berno van Meijel, and Rodrigo Mariño. 2024. "A Systematic Umbrella Review of the Effects of Teledentistry on Costs and Oral-Health Outcomes" International Journal of Environmental Research and Public Health 21, no. 4: 407. https://doi.org/10.3390/ijerph21040407
APA StyleScheerman, J. F. M., Qari, A. H., Varenne, B., Bijwaard, H., Swinckels, L., Giraudeau, N., van Meijel, B., & Mariño, R. (2024). A Systematic Umbrella Review of the Effects of Teledentistry on Costs and Oral-Health Outcomes. International Journal of Environmental Research and Public Health, 21(4), 407. https://doi.org/10.3390/ijerph21040407