
Parentification Vulnerability, Reactivity, Resilience, and Thriving: A Mixed Methods Systematic Literature Review
 ,
,
Abstract
1. Introduction
1.1. Dimensions of Parentification
1.2. Sources of Parentification
1.3. Consequences of Parentification
1.4. Purpose of Current Review
2. Materials and Methods
2.1. Eligibility Criteria—Inclusion and Exclusion
2.2. Information Sources
2.3. Search Strategy
2.4. Selection and Data Collection Processes
2.5. Data Items
2.6. Study Risk of Bias Assessment
2.7. Synthesis Methods
2.8. Certainty Assessment
3. Results
3.1. Included Study Description
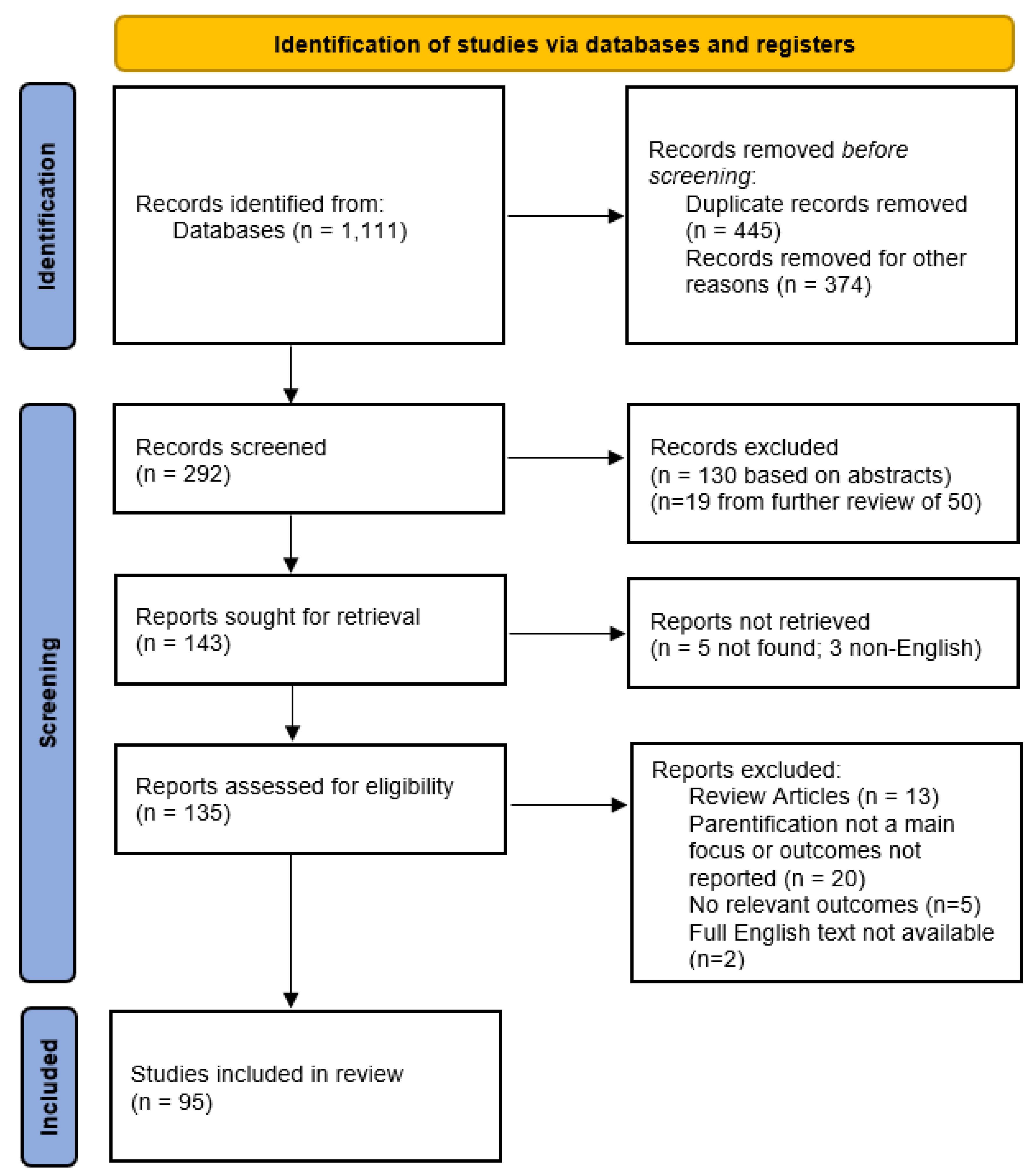
3.1.1. Study Selection
3.1.2. Study Characteristics

{kind=link}
| Author(s) | Year | Sample Size | Participants | Participants’ Age^ | Participants’ Sex (Female) | Sample Context | Country | Study Type |
|---|---|---|---|---|---|---|---|---|
| Mayseless et al. [25] | 2004 | 128 quan; 16 qual | Adults | 37.4 (SD = 12.6) | 53.13% | Community sample | Canada | Mixed |
| Callaghan et al. [26] | 2016 | 2 sibling dyads | Children | range: 7–11 | 25% | Families affected by domestic violence; case studies drawn from the larger interviews | UK | Qual |
| Chademana, and van Wyk [27] | 2021 | 7 | Children | 17.57 (range: 14–20) | 14.29% | Selected based on survey findings; orphans living in child- and youth-headed households in Zimbabwe | Zimbabwe | Qual |
| Chee et al. [28] | 2014 | 5 (mother-child dyads) | Mothers, children | 40 (range: 28–54, mothers); 10.4 (range: 7–12, children) | not specified | Low-income families | Singapore | Qual |
| Collado [29] | 2021 | 10 | Young adults | range: 19–23 | 60% | Convenience sampling; young adult children among internally displaced, refugee families due to political conflict | Philippines | Qual |
| Gelman and Rhames [30] | 2018 | 4 (mother-child dyads) | Mothers, children | 47.5 (range: 43–51, mothers); 18 (range: 15–20, children) | 62.50% (children) | Children living at home with a parent with younger-onset Alzheimer’s disease or other dementia | US | Qual |
| Kabat [31] | 1996 | 2 (mother-daughter dyads) | Adults | 18 and 23 (daughters) | 100% | Clinical case studies | US | Qual |
| Keigher et al. [32] | 2005 | 7 | Mothers | 42 (range: 39–45) | 100% | Mothers with HIV | US | Qual |
| Kosner et al. [33] | 2014 | 34 | Adolescents, young adults | 16 (range: 15–18, adolescents); 25.70 (range: 23–31, young adults) | 64.71% | Young immigrants to Israel from the former Soviet Union during adolescence; adolescents’ current experiences and Young adults’ retrospective accounts | Israel | Qual |
| Petrowski and Stein [34] | 2016 | 10 | Adults | 20.1 (SD = 1.37) | 100% | College students; women with mothers diagnosed with a long-term mental illness | US | Qual |
| Rizkalla et al. [35] | 2020 | 23 | Mothers | 37.62 (SD = 8.93) | 100% | Syrian refugee families, mothers’ accounts | US | Qual |
| Saha [36] | 2016 | 30 | Adolescents | range: 11–18 | not specified | High school students; middle socioeconomic status; first-born child with siblings | India | Qual |
| Tahkola et al. [37] | 2020 | 18 | Young adults | 25.4 (range: 18–32) | 77.78% | Finnish young adults with foster care background | Finland | Qual |
| Tedgård et al. [38] | 2019 | 19 | Adults | range: 21–40 (mothers), range: 27–40 (fathers) | 68.42% | Parent of children between 1 and 5 years old; parents grew up with drug-abusing parents | Sweden | Qual |
| Abraham and Stein [39] | 2013 | 116 | Adults | 19.79 (SD = 2.34) | 81% | Emerging adults who have a mother with/without mental illness and poor psychological adjustment | US | Quan |
| Arellano et al. [40] | 2018 | 1796 | Adults | 21.23 (SD = 5.25) | 79.99% | College students | US | Quan |
| Baggett et al. [41] | 2015 | 1632 | Adults | 19.29 (SD = 1.36) | 100% | College students | US | Quan |
| Beffel and Nuttall [42] | 2020 | 108 | Adults | 20.37 (SD = 1.55) | 69.44% | College students; typically developing (TD) who reported having a sibling with Autism Spectrum Disorder (ASD) | US | Quan |
| Borchet and Lewandowska-Walter [43] | 2017 | 264 | Late adolescents | 21.39 (SD = 2.52) | 87.50% | Individuals | Poland | Quan |
| Borchet et al. [46] | 2016 | 89 family triads (31 mothers, 27 fathers, 31 late adolescents) | Triads of father, mother and late adolescents | 49.58 (SD = 5.14, mothers); 51.04 (SD = 5.32, fathers); 22.58 (SD = 1.52, late adolescents) | 53.45% (parents), 64.52% (adolescents) | Family triads; families recruited through students | Poland | Quan |
| Borchet et al. [8] | 2021 | 191 | Adolescents | 14.61 (SD = 1.26) | 55% | High school students | Poland | Quan |
| Borchet, Lewandowska-Walter, Polomski, and Peplinska [44] | 2020 | 641 | Adolescents | 14.96 (SD = 0.36) | 60.70% | College students | Poland | Quan |
| Borchet, Lewandowska-Walter, Polomski, Peplinska, and Hooper [45] | 2020 | 218 | Late adolescents | 21.37 (SD = 2.49) | 86.20% | Majority self-identified college students | Poland | Quan |
| Boumans & Dorant [47] | 2018 | 297 | Adults | 18.9 (SD = 1.64) | 82.87% | College students; carers/non-carers | Netherlands | Quan |
| Burton et al. [48] | 2018 | 314 | Adolescents | range: 12–13 (63.7%) | 50.60% | Middle and high school students | US | Quan |
| Carroll & Robinson [49] | 2000 | 207 | Adults | range: 18–25 (72%) | 87.92% | College students; have/do not have alcoholic and/or workaholic parents | US | Quan |
| Castro et al. [50] | 2004 | 213 | Adults | 31 (range: 20–59) | 85% | College students in clinical and counseling psychology graduate programs | US | Quan |
| Champion et al. [51] | 2009 | 72 (mother-adolescent dyads; 34 with depression & 38 without depression) | Mothers, adolescents | 41.7 (SD = 5.13, mothers); 12.2 (SD = 1.07, adolescents) | 50% (adolescents) | Mother with/without history of depression from urban area | US | Quan |
| Chen and Panebianco [52] | 2020 | 132 | Adolescents | 14.38 (SD = 2.03) | 39.39% | Middle and high school students with at least one parent with a chronic illness | US | Quan |
| Chen et al. [53] | 2018 | 83 | Adults | 21.37 (SD = 1.87) | 60% | Transitional-aged youth | US | Quan |
| Cho and Lee [54] | 2019 | 316 | Adults | 21.86 (range: 18–29) | 66.10% | College students | Korea | Quan |
| Cimsir and Akdogan [55] | 2021 | 147 | Adults | 20.20 (SD = 1.12) | 74.10% | College students | Turkey | Quan |
| Dragan and Hardt [56] | 2016 | 508 (Poland), 500 (Germany) | Adults | 38.7 (SD = 14.4, Poland); 44.8 (SD = 16.1, Germany) | 56.3% (Poland), 50.0% (Germany) | Subjects all registered with a market research company | Poland, Germany | Quan |
| Duval et al. [57] | 2018 | 263 | Adolescents | 17.08 (SD = 4.45) | 78% | High school and college students | Canada | Quan |
| Fitzgerald et al. [58] | 2008 | 499 | Adults | 19.29 (SD = 1.95) | 100% | College students | US | Quan |
| Fortin, A., et al. [59] | 2011 | 79 (mother-child dyads) | Mothers, children | 37.72 (SD = 5.78, mothers); 10.26 (SD = 1.27, children) | 48.10% (children) | Children exposed to domestic violence | Canada | Quan |
| Godsall et al. [60] | 2004 | 416 | Children | 14.09 (SD = 1.68) | 45.20% | High-functioning/low-functioning children; students | US | Quan |
| Golan and Goldner [61] | 2019 | 80 | Adults | 33.47 (SD = 4.76) | 100% | Young, first-time Jewish mothers of children aged 12–36 months | Israel | Quan |
| Goldner et al. [62] | 2017 | 351 | Adolescents | 14.00 (SD = 0.69) | 53% | Middle school students | Israel | Quan |
| Goldner et al. [63] | 2019 | 334 | Adolescents | 13.95 (SD = 0.69) | 55% | Convenience sample; drawn from mid- to high-SES middle schools | Israel | Quan |
| Hoffman and Shrira [64] | 2019 | 341 (parent-adult dyads) | Adults | 80.05 (SD = 6.10, parents); 53.50 (SD = 5.57, children) | 65.4% (parents), 64.2% (adult offspring) | Community sample; Jewish parents of European origin born before 1945 and their offspring born after 1945; parents were alive during World War II and either Holocaust survivors or had no Holocaust background | Israel | Quan |
| Hooper, Doehler et al. [65] | 2012 | 51 (parent-adolescent dyads) | Parents, adolescents | 41.74 (SD = 6.64, parents); 13.80 (SD = 1.28, adolescent) | 92% (parents), 51% (children) | Rural community sample | US | Quan |
| Hooper et al. [17] | 2008 | 156 | Adults | 22.45 (SD = 6.04) | 69.20% | College students | US | Quan |
| Hooper et al. [66] | 2015 | 977 | Adults | 21.39 (SD = 5.84) | 81% | College students | US | Quan |
| Hooper, Wallace et al. [3] | 2012 | 314 | Adults | 22.57 (SD = 6.19, Black); 20.37 (SD = 1.91, White) | 56.05% | College students | US | Quan |
| Jankowski and Hooper [67] | 2014 | 565 | Adults | 20.78 (SD = 3.79) | 81.20% | College students | US | Quan |
| Jankowski et al. [68] | 2013 | 783 | Adults | 20.92 (SD = 3.73) | 76.40% | College students | US | Quan |
| Katz et al. [69] | 2009 | 163 | Adults | >18 (not specified) | 100% | College students; grew up in an intact family with one mother and one father | US | Quan |
| Khafi et al. [70] | 2014 | 143 (mother-child dyads) | Mothers, children | 10.17 (SD = 1.59, children, T1); 14.89 (SD = 1.60, children, T2) | 52.40% (children) | Sample overrepresents mothers with anxiety, affective, and/or substance use disorders; predominantly low-income | US | Quan |
| King and Mallinckrodt [71] | 2000 | 65 | Adults | 22.41 (SD = 3.21, clinical); 21.53 (SD = 1.64, nonclinical) | 85% (clinical), 69% (nonclinical) | College students; clinical/nonclinical samples | US | Quan |
| Lester et al. [72] | 2010 | 264 (mother- adolescent dyads) | Mothers, adolescent | 40.6 (SD = 5.78, mothers); 15.6 (SD = 2.4, adolescent) | 58% (adolescent) | Adolescent with HIV/AIDS-infected mothers, or adolescent of neighborhood control mothers | US | Quan |
| Macfie et al. [74] | 2008 | 138 families | Families (mothers, fathers, children) | 27 (range: 18–35, mothers); prenatally, 3 mos., 12 mos., 24 mos., 60 mos., 70 mos. (children) | 54.35% (children) | First-time parents | US | Quan |
| Macfie et al. [73] | 2005 | 57 | Families (mothers, fathers, adolescents) | 27 mos. (children, Wave 1); 70 mos. (children, Wave 2); 26 (mothers); 28 (fathers) | 52.63% (children) | Rural families; waves of data collected on families at 27 months and 70 months from the child’s birth. | US | Quan |
| Madden and Shaffer [75] | 2016 | 52 | Adults | 19.49 (SD = 1.39) | 80.70% | College students | US | Quan |
| McGauran et al. [76] | 2019 | 137 | Adults | 36.90 (SD = 13.91, offender from probation service); 31.83 (SD = 13.25, non-offender) | 8% (offender), 69% (non-offender) | Offender/non-offender samples; all white | UK | Quan |
| McMahon and Luthar [77] | 2007 | 356 (mother-child dyads) | Mothers, children | 38.23 (SD = 6.20, mothers); 12.09 (SD = 2.80, children) | 54% (children) | Urban, low-income children living with biological mothers; includes mothers (a) with drug problem, (b) with psychiatric problem, or (c) none of the two | US | Quan |
| Murrin et al. [78] | 2021 | 108 | Adults | 20.37 (SD = 1.55) | 69.44% | College students; typically developing (TD) who reported having a sibling with Autism Spectrum Disorder (ASD) | US | Quan |
| Nebbitt and Lombe [79] | 2010 | 238 | Adolescents | 15.62 (SD = 2.08) | 47.48% | African Americans living in urban, public housing developments | US | Quan |
| Nuttall et al. [82] | 2012 | 374 (mother-child dyads) | Mothers, children | 21.47 (SD = 5.32, mothers); prenatally, 12 mos., 36 mos. (children) | 49% (children) | Community sample; high-risk, first-time adolescent and adult mothers | US | Quan |
| Nuttall, Ballinger et al. [80] | 2021 | 374 (mother-child dyads) | Mothers, children | 21.47 (SD = 5.32, mothers); 36 mos. (children) | 49% (children) | Majority of mother sample were non-White (78.4%) and unmarried (74%) | US | Quan |
| Nuttall et al. [81] | 2018 | 108 | Adults | 20.37 (SD = 1.55) | 69.44% | College students; typically developing (TD) who reported having a sibling with Autism Spectrum Disorder (ASD) | US | Quan |
| Nuttall et al. [84] | 2019 | 110 mother-child dyads | Mothers, children | 30.76 (SD = 7.04) | 55% | Predominantly low-income and ethnic minorities; college students; psychosis-proneness sample | US | Quan |
| Nuttall, Valentino, et al. [83] | 2021 | 235 family triads | Families (mothers, fathers, children) | 35.02 (SD = 5.60, mothers, Wave 1); 36.84 (SD = 6.15, fathers, Wave 1); 6.00 (SD = 0.48, children, Wave 1) | 45% (children) | Data collected when children were in kindergarten (Wave 1), first grade (Wave 2), and second grade (Wave 3) | US | Quan |
| Oznobishin and Kurman [85] | 2009 | 184 (Study 1), 180 (Study 2) | Adults, adolescents | 23.73 (SD = 2.23, Study 1); 16.73 (SD = 0.94, Study 2) | 60.87% (Study 1), 57.78% (Study 2) | College students (Study 1) and high school students (Study 2); both studies include immigrant or Israeli-born | Israel | Quan |
| Peris et al. [86] | 2008 | 83 family triads | Families (mothers, fathers, adolescents) | 15.26 (range: 14–18, adolescents) | 48% (children) | Family triads, longitudinal design | US | Quan |
| Perrin et al. [87] | 2013 | 120 | Adults | 19.4 (SD = 1.52) | 57.67% | College students | Canada | Quan |
| Prussien et al. [88] | 2018 | 78 (mother-child dyads) | Mothers, children | 38.68 (SD = 7.52, mothers); 10.35 (SD = 3.67, children) | 45% (children) | Mothers with children diagnosed with cancer | US | Quan |
| Rodriguez and Margolin [89] | 2018 | 80 (mother-adolescent dyads) | Mothers, adolescents | 16 (SD = 1.2) | 53.75% (children) | Adolescents in active-duty military families | US | Quan |
| Rogers and Lowrie [90] | 2016 | 226 | Adults | 39.0 (SD = 16.3) | 50.90% | Age ranged from 19 to 92 years old; 82.4% Caucasian | UK | Quan |
| Sang et al. [20] | 2014 | 176 (mother-daughter dyads) | Mothers, daughters | 40.89 (SD = 7.13, mothers); 15.8 (SD = 1.55, daughters) | 100% | African American and Hispanic mother; HIV-negative daughter; low-income inner-city, recruited in agencies that provided services to HIV-infected women; victims of intimate partner violence, and those in substance use recovery | US | Quan |
| Schier et al. [91] | 2015 | 500 (extraction), 500 (cross-validation) | Adults | 44.8 (SD = 16.1; extraction), 39.3 (SD = 11.2; cross-validation) | 50% (extraction), 55% (cross-validation) | Internet survey; extraction and cross-validation samples | Germany | Quan |
| Shaffer and Egeland [92] | 2011 | 196 (mother-offspring dyads) | Mothers, offsprings | Longitudinal: offspring followed from 24 mos initially to adolescent years (age 13, 16, 17.5 years) | 42.85% (offspring) | Mother of low socioeconomic status recruited through a public health clinic for prenatal care | US | Quan |
| Sheinbaum et al. [93] | 2015 | 214 | Adults | 21.4 (SD = 2.4) | 78% | College students | Spain | Quan |
| Shin and Hecht [94] | 2012 | 697, 605, and 526 across Waves 4, 5, 6 | Adolescents | 12.31 (SD = 0.58) | 53% | Mexican-heritage; middle school students; use Wave 4–6 only | US | Quan |
| Stein et al. [95] | 1999 | 183 (parent-adolescent dyads) | Parents, adolescents | 37.67 (SD = 5.64, parents); 14.75 (SD = 2.07, children) | 80% (parents), 54% (adolescent) | Non-infected adolescents of parents with AIDS | US | Quan |
| Stein et al. [19] | 2007 | 213 | Adolescents | 14.9 (range: 11–19) | 56% | Children with HIV/AIDS-infected mothers | US | Quan |
| Sullivan et al. [96] | 2018 | 1441 | Adolescents | grades 7, 9, and 11 (proxy for age) | 50.87% | Middle and high school students | US | Quan |
| Telzer and Fuligni [97] | 2009 | 752 | Adolescents | 14.88 (SD = 0.39) | not provided | High school students; ethnically diverse sample of adolescents from predominantly Latin American, Asian, and European backgrounds | US | Quan |
| Titzmann [98] | 2012 | 382 (mother-adolescent dyads) | Mothers, adolescent | 15.2 (SD = 2.55, adolescent) | 56.54% (children) | Ethnic (185) and 197 native German families | Germany | Quan |
| Titzmann and Gniewosz [99] | 2018 | 185 (mother-child dyads) | Mothers, children | 15.7 (SD = 2.7, children) | 60.4% (children) | Ethnic German immigrant mother-adolescent dyads from the former Soviet Union | Germany | Quan |
| Tomeny et al. [101] | 2017a | 60 | Adults | 29.65 (SD = 13.17) | 85% | College students; typically developing (TD) who reported having a sibling with Autism Spectrum Disorder (ASD) | US | Quan |
| Tomeny et al. [100] | 2017b | 41 | Adults | 25.83 (SD = 5.36) | 80% | Typically developing (TD) who reported having a sibling with Autism Spectrum Disorder (ASD) | US | Quan |
| Tompkins [102] | 2007 | 43 (mother-child dyads) | Mothers, children | 12.8 (range: 9–16, children) | not specified | Children with HIV/AIDS-infected mother (23) vs. children with HIV-seronegative mother (20). | US | Quan |
| van der Mijl and Vingerhoet [103] | 2017 | 265 | Adults | 20.2 (SD = 3.1) | 73% | College students | Netherlands | Quan |
| Van Loon et al. [104] | 2017 | 118 | Adolescents | 13.47 (SD = 1.40) | 50.80% | Adolescents living with a parent with mental health problems | Netherlands | Quan |
| Walsh et al. [105] | 2006 | 140 (Study 1), 123 (Study 2) | Adolescents | 16.8 (SD = 5.60, Study 1); 16.96 (SD = 1.39, Study 2) | 45.7% (Study 1), 47% (Study 2) | Study 1: Immigrants from former Soviet Union in Israel vs. Israel born; Study 2: Immigrants from former Soviet Union in Israel | Israel | Quan |
| Wang et al. [106] | 2017 | 1073 | Children | range: 9–17.7 (grades 3–12) | 51.80% | Two elementary school and three high school students | China | Quan |
| Wei et al. [114] | 2020 | 1648 | Adolescents | Junior and senior high students (age not specified) | 46.30% | Junior and senior high school students | Taiwan | Quan |
| Wells and Jones [108] | 1998 | 124 | Adults | 21 (range: 17–48) | 65% | College students | US | Quan |
| Wells and Jones [109] | 2000 | 197 | Adults | 21 (range: 17–38) | 65% | College students | US | Quan |
| Wells et al. [107] | 1999 | 200 | Adults | 21 (range: 17–48) | 65% | College students | US | Quan |
| Williams and Francis [110] | 2010 | 99 | Adults | 23.76 (SD = 5.55) | 84% | College students | Canada | Quan |
| Woolgar and Murray [111] | 2010 | 94 (55 depressed and 39 nondepressed mother-child dyads) | Mothers, children | 60.3 mos. (SD = 0.84, index); 60.5 mos. (SD = 0.94, control) | 46% (index children), 53% (control children) | Community sample; children and mothers with/without postnatal depression; index and control groups | UK | Quan |
| Yew et al. [112] | 2017 | 419 | Adults | 21.9 (SD = 2.04) | 62.80% | College students in clinical and nonclinical academic programs | Malaysia | Quan |
| Zvara et al. [113] | 2018 | 557 (mother-child dyads) | Mothers, children | 25.6 (SD = 6.1, mothers); 7.7 (SD = 1.5, children) | 49.6% (children) | Rural, low-income families | US | Quan |
3.2. Risk of Bias and Certainty Assessment
3.3. Measurement Pattern Synthesis
3.3.1. Parentification Measures
| Measure Name & Description | Literature | Participant Group | Modifications | Alpha | Sample Context |
|---|---|---|---|---|---|
| The Parentification Questionnaire (PQ) [115]: 42 Items, self-report, rate from 1 (usually not true/strongly disagree) to 5 (usually true/strongly agree) or true/false; 3 subscales: emotional and instrumental parentification, and perceived unfairness [17]: says only instrumental and emotional) (one article said that there are no official subscales). Includes emotional, expressive, and physical statements. The questions were summed. | Arellano et al., 2018 [40] | Adults | Use continuous PQ subscale scores and dichotomized subscale scores (subscales dichotomized into never/rarely experienced as scored less than 2 vs. some/repeated experiences as scored 2 and above); This study also used Parentification Inventory | Instrumental: 0.85 Emotional: 0.85 Unfairness: 0.92 | College students |
| PQ | Carroll and Robinson, 2000 [49] | Adults | None | None reported | College students; have/do not have alcoholic and/or workaholic parents |
| PQ | Castro et al., 2004 [50] | Adults | None | None reported | College students in clinical and counseling psychology graduate programs |
| PQ | Hooper et al., 2008 [17] | Adults | None | Emotional: 0.75 Instrumental: 0.80 | College students |
| PQ | Jankowski and Hooper, 2014 [67] | Adults | Only used the perceived unfairness scale (PQ-UN) | Perceived Unfairness: 0.89 | College students |
| PQ | Jankowski et al., 2013 [68] | Adults | None | Instrumental: 0.84 Emotional: 0.84 Perceived Unfairness: 0.90 | College students |
| PQ | McGauran et al., 2019 [76] | Adults | None | 0.83 | Offender/non-offender samples; all white |
| PQ | Oznobishin and Kurman, 2009 [85] | Study 1: Adults Study 2: Adolescents | Study 1: Combined PQ with Parent–Child Role Reversal Scale from the Family Structure Survey [121] (49 items total); Two factors emerged: child dominance (16 items) and family support (9 items) Study 2: Child dominance (27 items; from Study 1 and other role reversal questionnaires assessing emotional and instrumental) Both studies: translated into Hebrew and Russian | Study 1: child dominance: 0.80 (immigrants); 0.85 (Israeli- born) Study 2: child dominance: 0.89 (immigrants); 0.91 (Israeli-born) | College students (Study 1) and high school students (Study 2); both studies include immigrant or Israeli-born |
| PQ | Rogers and Lowrie, 2016 [90] | Adults | Only used 21 items without specification what items they selected | Age ranged from 19 to 92 years old; 82.4% Caucasian | |
| PQ | Titzmann, 2012 [98] | Adolescents and their mothers | Translated into Russian and German; Used 2 subscales: Emotional and instrumental [17,110]; Items based on PQ and Parentification scale [117,120]; Emotional and Instrumental: mean of five items rated on a six-point scale | Emotional: 0.70 Instrumental: 0.69 | Ethnic (185) and 197 native German families |
| PQ | Titzmann and Gniewosz, 2018 [99] | Adolescents and their mothers | Only assessed instrumental; mean of 5 items; 6 pt Likert scale; based on Parentification Scale [117] too | Instrumental: 0.69 | Ethnic German immigrant mother-adolescent dyads from the former Soviet Union |
| PQ | Van der Mijl and Vingerhoets, 2017 [103] | Adults | None | 0.84 | College students |
| PQ | Wei et al., 2020 [114] | Young adults | Three items were used from each subscale | Instrumental: 0.61 Emotional: 0.66 Perceived fairness: 0.77 | Junior and senior high school students |
| PQ | Wells and Jones, 1998 [108] | Adults | None | None reported | College students |
| PQ | Wells and Jones, 2000 [109] | Adults | None | None reported | College students |
| PQ | Wells et al., 1999 [107] | Adults | None | None reported | College students |
| PQ | Williams and Francis, 2010 [110] | Adults | None | None reported | College students |
| PQ | Yew et al., 2017 [112] | Adults | None | 0.79 | College students in clinical and nonclinical academic programs |
| The Parentification Inventory (PI) [122,123]: adult self-report, 22 items on a 1 (never true) to 5 (always true) response scale; three subscales include parent-focused parentification (PFP), sibling-focused parentification (SFP), and perceived benefits of parentification (PBP). Scales are summed and averaged | Arellano et al., 2018 [40] | Adults | NA as an option on PI; Only parent-focused and sibling-focused parentification subscales; subscales were dichotomized (rarely or never experienced vs. those who had some level of or repeated experience); Also used the PQ [118] | Parent-focused: 0.78 Sibling-focused: 0.65 | College students |
| PI | Beffel and Nuttall, 2020 [42] | Adults | None | PFP: 0.83 SFP: 0.79 PBP: 0.88 | College students; typically developing (TD) who reported having a sibling with Autism Spectrum Disorder (ASD) |
| PI | Borchet and Lewandowska-Walter, 2017 [43] | Late adolescents | Experimental version of the Polish adaptation | PFP: 0.80 SFP: 0.58 PBP: 0.81 | Individuals |
| PI | Borchet et al., 2016 [46] | Late adolescents and their parents | Used Kwestionariusz Parentyfikacji (KP)- experimental version of the Polish adaptation of the PI | PFP: 0.75 SFP: 0.60 PBP: 0.89 | Family triads; families recruited through students |
| PI | Borchet, Lewandowska-Walter, Połomski, Peplińska, and Hooper, 2020 [45] | Late adolescents | Used a Polish adaptation of PI; used the perceived benefits of parentification subscale only | PBP: 0.77 | School students |
| PI | Burton et al., 2018 [48] | Early adolescents | None | PFP: 0.82 SFP: 0.63 PBP: 0.85 | Middle and high school students |
| PI | Chen et al., 2018 [53] | Adolescents (18–24) | Used 19-item three-factor structure of the scale: household responsibility, perceived benefits, and spousal parentification | Household responsibility: 0.87; Perceived benefits: 0.84; Spousal parentification: 0.77 | Transitional-aged youth |
| PI | Cimsir and Akdogan, 2021 [55] | Adults | Only used PFP subscale; adapted the PI into Turkish: Factor structure varied slightly for subscales (Turkish culture normalizing parentification) | PFP: 0.84 | College students |
| PI | Hooper et al., 2015 [66] | Adults | None | Total Sample: PFP: 0.79 SFP: 0.58 PBP: 0.80 | College students |
| PI | Hooper, Wallace et al., 2012 [3] | Adults | None | PFP: 0.83 SFP: 0.80 PBP: 0.80 Black: PFP: 0.83 SFP: 0.76 PBP: 0.80 White: PFP: 0.85 SFP: 0.79 PBP: 0.81 | College students |
| PI | Murrin et al., 2021 [78] | Adults | Only mentions PFP and SFP; likely only used 19 items | PFP: 0.83 SFP: 0.79 | College students; typically developing (TD) who reported having a sibling with Autism Spectrum Disorder (ASD) |
| PI | Nuttall et al., 2018 [81] | Adults | None | PFP: 0.83 SFP: 0.79 PBP: 0.88 | College students; TD who reported having a sibling with ASD |
| PI | Tomeny, Barry, and Fair, 2017 [101] | Adults | Only used PFP and SFP | Each of the PI subscales ranged from 0.64 to 0.88 | College students; TD who reported having a sibling with ASD |
| PI | Tomeny, Barry, Fair, and Riley, 2017 [100] | Adults | 1 item removed from SFP to improve internal consistency | SFP: 0.72–0.88 | TD who reported having a sibling with ASD |
| Parentification Scale [117]: adult self-report, 30 items on a 1 (never or does not apply) to 5 (very often) response scale; subscales where child is functioning (1) as a parent to parent(s), (2) as a spouse to parents, (3) as a parent to sibling(s), and (4) in ways which transcend these subtypes. Includes particular subtypes (e.g., consoler, adviser, confidant, or peacemaker). Questions asked how often behavior occurred before the age of 14 and how often it occurred between the ages of 14 and 16. Differential weights were assigned to the questions depending on the age and physical/emotional burden | Fitzgerald et al., 2008 [58] | Adults | Only used 3 subscales (acting as a parent to parent, spouse to parent, and parent to siblings); Items were summed | Parent to parent: 0.76 Spouse to parent: 0.78 Parent sibling: 0.86 | College students |
| PS | Perrin et al., 2013 [87] | Adults | Only used 1 item from Parental Role with Parents subscale; The final scale included 17 items; Items were also drawn from Parent-Child Boundaries Scale III [124], Family Structure Survey [121], and Filial Responsibility Scale-Adult; Item sets asked about mothers and fathers | 17-item Parentification Scale created; Mothers: 0.94 Fathers: 0.93 | College students |
| PS | Sang et al., 2014 [20] | Adolescents and their mothers | Only used 3 of 4 subscales: (a) spousal role vis-a-vis parents (8 items); (b) parental role vis-a-vis parents (6 items); (c) parental role vis-a-vis siblings (12 items) | Range: 0.84 to 0.92 | Black and Hispanic mother; HIV-negative daughter; low-income inner-city sample recruited in agencies that provided services to HIV-infected women; victims of intimate partner violence; and those in substance use recovery |
| PS | Shin and Hecht, 2012 [94] | Adolescents | Two items from Parentification scale operationalized problem-solving parentification; 5 point scale, but went from strongly disagree to strongly agree; used FRS as well | None reported | Mexican-heritage; middle school students; use Wave 4–6 only |
| PS | Stein et al., 1999 [95] | Adolescents and one of their parents | Parental role with siblings was not used because not applicable to many of the study participants | Adult role-taking: 0.77 Spousal role: 0.75 Parental role: 0.67 | Non-infected adolescents of parents with AIDS |
| PS | Stein et al., 2007 [19] | Adolescents and one of their parents | Parental role with siblings was not used; many participants did not have siblings; used the mean | None reported | Children with HIV/AIDS-infected mothers |
| PS | Titzmann, 2012 [98] | Adolescents and their mothers | Translated into Russian and German; items based on PS and PQ [117,120] (Emotional and Instrumental: mean of five items rated on a six-point scale; selected individual items from subscales) | Emotional: 0.70 Instrumental: 0.69 | Ethnic (185) and 197 native German families |
| PS | Titzmann and Gniewosz, 2018 [99] | Adolescents and their mothers | Only assessed instrumental; mean of 5 items; 6 pt Likert scale; based on PQ [120] too | Instrumental: 0.69 | Ethnic German immigrant mother-adolescent dyads from the former Soviet Union |
| PS | Tompkins, 2007 [102] | Adults and Adolescents | 3 items deleted of the parental role to parent scale due to inadequate reliability (involved fathers or illness) | Mother/Child: Spousal role: 0.76 Parental role to siblings: 0.95/0.86 Non-specific adult responsibilities: 0.78/0.65 Parental role to parent: 0.69/0.71 | Children with HIV/AIDS-infected mother (n = 23) vs. children with HIV-seronegative mother (n = 20) |
| PS | Walsh et al., 2006 [105] | Adolescents | Translated into Hebrew and Russian; Deleted 3 items | Hebrew/Russian: Spousification: 0.73/0.84 Parental role for parents: 0.57/0.79 Parental role for siblings: 0.80/0.87 Nonspecific adult role taking: 0.82/0.78. | Study 1: Immigrants from former Soviet Union in Israel vs. Israel born; Study 2: Immigrants from former Soviet Union in Israel |
| Filial Responsibility Scale, Adult Version (FRS) [118]: adult self-report; 60 items on a 1 (strongly disagree) to 5 (strongly agree) response scale; 6 subscales: Past Instrumental Caregiving, Past Emotional Caregiving, Past Unfairness, Current Instrumental Caregiving, Current Emotional Caregiving, Current Unfairness | Cho and Lee, 2019 [54] | Adults | Only used past subscales | Instrumental: 0.74 Emotional: 0.78 Unfairness: 0.87 | College students |
| FRS | Madden and Shaffer, 2016 [75] | Adults | Only used past Emotional and past Instrumental subscales | Emotional: 0.82 Instrumental: 0.80 | College students |
| FRS | Nuttall, Ballinger, Levendosky and Borkowski, 2021 [80] | Adults | Only used three subscales (past) | 0.92 | Majority of mother sample were non-White (78.4%) and unmarried (74%) |
| FRS | Nuttall et al., 2012 [82] | Adults | Only used three subscales (past); summed subscales | 0.92 | Community sample; high-risk, first-time adolescent and adult mothers |
| FRS | Nuttall et al., 2019 [84] | Adults, adolescents | Used past emotional and past instrumental only | Both: 0.78 | Predominantly low-income and ethnic minorities; college students; psychosis-proneness sample |
| FRS | Perrin et al., 2013 [87] | Adults | Only used 4 items from Current Emotional Caregiving subscale (final scale created included 17 items); items written twice (one asked about mothers and one fathers); also used items from Parent- Child Boundaries Scale III [124], Family Structure Survey [121], and Parentification Scale [117]; never to almost always | 17 item Parentification Scale created: Mothers: 0.94 Fathers: 0.93 | College students |
| FRS | Shin and Hecht, 2012 [94] | Adolescents | Used two items from FRS operationalized adult parentification; used the Parentification Scale [117] as well | None reported | Mexican-heritage; middle school students; use Wave 4–6 only |
| Parentification Questionnaire for Youth (PQ-Y) [119]: 20 items, yes/no format, no official subscales, but some more emotional or instrumental in nature; modified version of the PQ-A [120]: items changed to present tense and 3rd grade vocab | Chen and Panebianco, 2020 [52] | Adolescents | Only used Emotional Parentification subscale; created instrumental parentification with 22 items from three other instruments | Kuder-Richardson reliability coefficient was 0.72 | Middle and high school students with at least one parent with a chronic illness |
| PQ-Y | Fortin et al., 2011 [59] | Children and their mothers | Remove 5 items that measured the family’s recognition of the child’s parentification due to reduced instrument reliability | 0.64 reported | Children exposed to domestic violence |
| PQ-Y | Godsall et al., 2004 [60] | Children and adolescents | Item total reduced to 20 (not appropriate for children, and did not meet item total correlation) | 0.76 Cross-validation: 0.75 | High-functioning/low-functioning children; students |
| PQ-Y | Hooper, Doehler et al., 2012 [65] | Adolescent and parent pairs | None | 0.80 | Rural community sample |
| PQ-Y | Van Loon et al., 2017 [104] | Adolescents and one parent | Translated into Dutch; no clear factor structure (emotional vs. instrumental) so used sum score | 0.69 | Adolescents living with a parent with mental health problems |
| Family Structure Survey (FSS) [121]: adult self-report; 50 items on a 1 (completely false) to 5 (completely true) response scale; adults’ recalled perceptions of their family interactions on four dimensions of dysfunctional family structure: parent-child over involvement, fear of separation, parent-child role reversal, and marital conflict; total scale scores are not used | King and Mallinckrodt, 2000 [71] | Adults | None | Parent-child role reversal: 0.74 | College students; clinical/nonclinical samples |
| FSS | Oznobishin and Kurman, 2009 [85] | Study 1: Adults Study 2: Adolescents | Study 1: Combined PQ with Parent–Child Role Reversal Scale from the Family Structure Survey [121] (49 items total); Two factors emerged: child dominance (16 items) and family support (9 items) Study 2: Child dominance (27 items; from Study 1 and other role reversal questionnaires assessing emotional and instrumental) Both studies: translated into Hebrew and Russian | Study 1: child dominance: 0.80 (immigrants); 0.85 (Israeli- born) Study 2: Child dominance: 0.89 (immigrants); 0.91 (Israeli-born) | College students (Study 1) and high school students (Study 2); both studies include immigrant or Israeli-born |
| FSS | Perrin et al., 2013 [87] | Adults | Final scale created included 17 items; 3 items from the Parent-Child Role Reversal subscale; also used items from the Parent-Child Boundaries Scale III [124], Filial Responsibility scale and PS [117]; never to almost always | 17 item Parentification Scale created: Mothers: 0.94 Fathers: 0.93 | College students |
| Inadequate Boundaries Questionnaire [125]: adult self-report; 34 items on a 1 (almost never) to 5 (almost always) response scale for different types of boundary dissolution with their own mothers as children; dimensions include guilt induction, blurring of psychological boundaries, parentification (emotional and instrumental), triangulation, and the use of psychological control | Golan and Goldner, 2019 [61] | Adults | Made a guilt-psychological control scale and boundaries-parentification scale | Triangulation: 0.87 Blurring boundaries: 0.62 Parentification: 0.87 Boundaries-Parentification: 0.89 | Young, first-time Jewish mothers of children aged 12–36 months |
| IBQ | Goldner et al., 2017 [62] | Adolescents | Parentification (both): 0.74 | Middle school students | |
| IBQ | Goldner et al., 2019 [63] | Adolescents | Completed the Parentification and the Enmeshment with the Mother subscales | Parentification: 0.74 Enmeshment: 0.69 | Convenience sample; drawn from mid- to high-SES middle schools |
| Child Caretaking Scale [126]: child self-report; 30 items on a 1 (strongly disagree) to 5 (strongly agree) response scale; designed originally for children living with a mother experiencing psychiatric difficulties | Khafi et al., 2014 [70] | Children and their mothers | 18 items were used to identified emotional (8 items) and instrumental (10 items) subscales | T1 Emotional: 0.59 T2 Emotional: 0.70 T1 Instrumental: 0.66 T2 Instrumental: 0.66 | Sample overrepresents mothers with anxiety, affective, and/or substance use disorders; predominantly low-income |
| CCS | McMahon and Luthar, 2007 [77] | Children and their mothers | 25 items used to define three dimensions of caretaking burden: responsibility to care for mother, responsibility for household chores, and responsibility to care for siblings | Care for mother: 0.63 Household chores: 0.61 Care for siblings: 0.75 | Urban, low-income children living with biological mothers; includes mothers (a) with drug problem, (b) with psychiatric problem, or (c) none of the two |
| Childhood Questionnaire (CQ) [127]: adult self-report; first 14 years; mothers and fathers; 20 items (only including subscales) assess parent-child relationships; dimensions include Perceived Love, Control, Ambition and Role Reversal (4 item scale on SES, individual items on separation and divorce of parents, eventual death of either or both of the parents, and education and occupation of the parents during the subject’s childhood); 4 pt Likert scale from not true at all to absolutely true | Dragan and Hardt, 2016 [56] | Adults | None | None reported | Subjects all registered with a market research company |
| CQ | Schier et al., 2015 [91] | Adults | None | None reported | Internet survey; extraction and cross-validation samples |
| Parent–Child Boundaries Scale III (PBS-III) [124]: is a 53-item self-report measure. Measures general parentification (no empirically supported subscales of emotional or instrumental parentification, but have items indicative of these); 5-point Likert-type scale ranging from 1 (never) to 5 (almost always) | Perrin et al., 2013 [87] | Adults | 17 items were also drawn from the Filial Responsibility Scale—Adult, Family Structure Survey [121], and Parentification Scale [117]; items were asked about mothers and fathers) | 17 item Parentification Scale created: Mothers: 0.94 Fathers: 0.93 | College students |
| PBS-III | Baggett et al., 2015 [41] | Adults | Only used 6 items; items combined to create global parentification scale | 0.89 | College students |
| Relationship with Parents Scale (RPS) [128]: A 42-item (21 items: mother, 21 items: father) self-report retrospective measure of parent-child role reversal; 5-point scale 1 (strongly disagree)- 5 (strongly agree) | Abraham and Stein, 2013 [39] | Adults | Only used 21 items (Mother version: reflected mothers using guilt to elicit nurturing from them, demanding their attention or company, and their perception of their mother’s competence as a parent) | 0.93 | Emerging adults who have a mother with/without mental illness and poor psychological adjustment |
| RPS | Katz et al., 2009 [69] | Adults | None | Fathers: 0.89 Mothers: 0.92 | College students; grew up in an intact family with one mother and one father |
| Maastricht Parentification Scale [129]: self-report; 22 items on a 1 (completely disagree) to 4 (completely agree) response scale for parents reporting on both their own parenting and the parenting of their partner; low scores are indicative of psychological autonomy, whereas high scores are indicative of psychological control; 6 subscales of parentification: emotional care parents, buffer between parents, household care family, financial care family, instrumental care siblings, emotional care siblings | Boumans and Dorant, 2018 [47] | Adults | None | Emotional care parents: 0.78 Buffer between parents: 0.71 Household care family: 0.76 Financial care family: 0.68 Instrumental care siblings: 0.76 Emotional care siblings: 0.71 | College students; carers/non-carers |
| Parentification Questionnaire for Youth (PQY) [44]: self-report, 26 items on a 1 (never true) to 5 (always true) response scale, four subscales: emotional parentification toward parents, instrumental parentification toward parents, sense of injustice, and satisfaction with the role; and two subscales for adolescents who have siblings: instrumental parentification toward siblings and emotional parentification toward siblings. scores are calculated as the mean of the ratings for the subscale items | Borchet et al., 2021 [8] | Adolescents | None | 0.70 to 0.80 | Polish sample; majority self-identified college students |
| Perceived Parental Rearing Behavior Questionnaire [130]: adult self-report; 30 items on a 1 (not at all) to 5 (all the time) response scale; dimensions include transmission, affection, punishing, over-involvement/protection | Hoffman and Shrira, 2019 [64] | Adults | Included 20 items; conceptualizes transmission as role reversal; translated to English | Role reversal: 0.71 Affection: 0.88 Punishing: 0.66 Overinvolvement: 0.70 | Community sample; Jewish parents of European origin born before 1945 and their offspring born after 1945; parents were alive during World War II and either Holocaust survivors or had no Holocaust background |
| Triangulation [131]: 45 items, 1 (totally disagree) to 3 (totally agree); 3 dimensions: cross-generation coalition, scapegoating, parentification | Wang et al., 2017 [106] | Children | 22 items were removed due to length consideration, or lack of association with other items as determined by exploratory factor analysis | Coalition: 0.79 Scapegoating: 0.75 Parentification: 0.72 | Two elementary school and three high school students |
3.3.2. Outcome Measures
| Outcome Construct | Description | Literature | Sample Context | Modifications | Alpha | Associations with Parentification |
|---|---|---|---|---|---|---|
| Depression | The Beck Depression Inventory II (BDI-II) [134]: 21 questions, self-report, rate on a 4-point scale from 0 (absence of symptoms) to 3 (severe presence of symptoms) for depressive symptoms. Items are summed | Arellano et al., 2018 [40] | College students | Used continuous score and the dichotomized score for BDI-II (20 and above high; rest low) | 0.91 | PFP+, SFP ns, EP+, IP+, Unfairness+ |
| Carroll and Robinson, 2000 [49] | College students; have/do not have alcoholic and/or workaholic parents | None | None stated | Overall no direct test | ||
| Hooper, Doehler et al., 2012 [65] | Rural community sample | Adolescent self-report; parent self-report | Parent report: 0.94; Adolescent: 0.92 | Overall ns | ||
| Hooper et al., 2015 [66] | College students | 0.92 | PFP +, SFP +, PBP − | |||
| Hooper, Wallace et al., 2012 [3] | College students | None | Overall: 0.91 Black: 0.90 White: 0.92 | White: PFP ns, SFP ns, PBP −; Black: PFP +, SFP ns, PBP − | ||
| Jankowski et al., 2013 [68] | College students | Used it together with GSI from BSI to create a latent variable of mental health symptoms | 0.92 | Overall + | ||
| Prussien et al., 2018 [88] | Mothers with children diagnosed with cancer | Mother self-reported | 0.93 | Emotional caregiving ns | ||
| The Center for Epidemiologic Studies Depression Scale (CES-D) [135]: 20 items, self-report, rate on a 4-point scale from 0 (rarely or not at all) to 3 (most of the time). Items are summed. | Chen and Panebianco, 2020 [52] | Middle and high school students with at least one parent with a chronic illness | None | 0.90 | EP +, IP ns | |
| Cho and Lee, 2019 [54] | College students | None | 0.91 | EP ns, IP ns, Unfairness + | ||
| Katz et al., 2009 [69] | College students; grew up in an intact family with one mother and one father | None | 0.90 | Role reversal ns | ||
| Murrin et al., 2021 [78] | College students; typically developing (TD) who reported having a sibling with Autism Spectrum Disorder (ASD) | None | 0.87 | PFP ns, SFP ns | ||
| Nebbitt and Lombe, 2010 [79] | African Americans living in urban, public housing developments | Rated frequency of symptoms in terms of days per week from 0 (less than 1 day) to 3 (5–7 days) | 0.88 | Household contribution— | ||
| Wang et al., 2017 [106] | Two elementary school and three high school students | None | 0.86 | Coalition +, scapegoating +, Parentification − | ||
| The Children’s Depression Inventory (CDI) [136]: 27-item, self-report, depressed mood. Rate from 0 (once in a while) to 2 (all the time) | Fortin et al., 2011 [59] | Children exposed to domestic violence | Used with the anxiety construct to form a latent variable internalizing problems | 0.84 | Overall + | |
| Khafi et al., 2014 [70] | Sample overrepresents mothers with anxiety, affective, and/or substance use disorders; predominantly low-income | T1: 0.81 T2: 0.87 | T1 IP and T2 dep ns, T1 EP and T2 dep + | |||
| Rodriguez and Margolin, 2018 [89] | Adolescents in active-duty military families | Omitted suicidal ideation item due to ethical and reporting concerns | 0.83 | IP −, EP ns, Observed emotional validation − | ||
| Tompkins, 2007 [102] | Children with HIV/AIDS-infected mother (23) vs. children with HIV-seronegative mother (20) | Only have range for all measures (0.70–0.89) | Mother report child’s parentification—(correlate only) | |||
| The Brief Symptom Inventory-18 (BSI-18) [137]: 18 items, self-report, rate on a 5-point Likert scale from 0 (not at all) to 4 (very much). But Depression subscale only has 6 items. Mean score of 6 items for depression | Hoffman and Shrira, 2019 [64] | Community sample; Jewish parents of European origin born before 1945 and their offspring born after 1945; parents were alive during World War II and either Holocaust survivors or had no Holocaust background | Hebrew version; Parent completed interview and offspring completed questionnaires including depression subscale derived from BSI-18 | 0.86 | Role reversal + | |
| Positive and Negative Affect Schedule for Children (PANAS-C) [138]: 30 items, self-report, rate on a 5-point scale form 1 (very slightly or not at all) to 5 (extremely). 15 items each for the positive affect and negative affect scales | Burton et al., 2018 [48] | Middle and high school students | Positive affective is used as wellbeing; and negative affective is used as depressive symptoms | NA: 0.90 PA: 0.91 | PFP +, SFP ns, PBP − | |
| The Symptom Checklist-27-plus (SCL-27-plus) [139] 27 items, self-report, rate on a 5 point scale how often (‘‘never’’ to ‘‘very often’’) symptoms occur in past 2 weeks. 5 dimensions in total | Schier et al., 2015 [91] | Internet survey; extraction and cross-validation samples | Used depression (5 items) only | None stated | Maternal EP +, Paternal EP +, | |
| The Weinberger Adjustment Inventory (WAI) [140]: 62-item, self-report, rate on a 5-point Likert scale from 1 (false) to 5 (true). Distress and Restraint as 2 primary dimensions, each defined with 4 subscales | Williams and Francis, 2010 [110] | College students | Only used depression and happiness subscales, each contains contain 7 items | None stated | Overall + | |
| Distress | The Brief Symptom Inventory (BSI) [141]: 53 items, self-report, rate on a 5-point Likert scale from 0 (not at all) to 4 (extremely). Three broad global indices are global severity index, positive symptom distress index and positive symptom total. | Hooper et al., 2008 [17] | College students | Used just the positive symptom total to capture “distress” | 0.96 | EP +, IP ns |
| Jankowski et al., 2013 [68] | College students | Summed all items and divided by 53 to get GSI; Used it together with BDI to create a latent variable mental health symptom | GSI: 0.97 | Overall + | ||
| Lester et al., 2010 [72] | Adolescent with HIV/AIDS-infected mothers, or adolescent of neighborhood control mothers | Child report; Used depression and anxiety subscale to form a latent variable for emotional distress | Depression: 0.81 anxiety: 81 | Role reversal ns | ||
| Oznobishin and Kurman, 2009 [85] | College students (Study 1) and high school students (Study 2); both studies include immigrant or Israeli-born | Sum score; called it “psychological distress” | Immigrant: 0.96 Israel born: 0.95 | Child dominance ns, Language brokerage ns | ||
| Stein et al., 1999 [95] | Non-infected adolescents of parents with AIDS | Used mean scores from each of three subscales depression, anxiety, and phobic anxiety as indicators for latent variable internalized emotional distress | 0.79, 0.79, 0.80, respectively | PFP ns, SFP ns, Non-specific adult role ns. | ||
| Stein et al., 2007 [19] | Children with HIV/AIDS-infected mothers | Used mean scores from each of three subscales depression, anxiety, and phobic anxiety as indicators for latent variable emotional distress; Assessment time window: during the past week, including today; Assessed at baseline and at year 6 | None stated | Overall parentification and distress 6 yrs later ns | ||
| The Depression, Anxiety, and Stress Scale 21 (DASS-21): 21 items, self-report, rate on a 4-point scale from 0 (not at all) to 3 (very much/most of the time). Sum scores multiplied by 2 [142] to make it comparable to the 42-item DASS | Tomeny, Barry, and Fair, 2017 [101] | College students; typically developing (TD) who reported having a sibling with Autism Spectrum Disorder (ASD) | Used overall score as “distress” | 0.84 to 0.91 for subscales, but did not report overall scale | PFP ns, SFP ns | |
| The Profile of Mood States (POMS) [143]: daily diary studies commonly used measure for stress and psychological well-being, rate on a 5-point scale from 1 (not at all) to 5 (extremely) to indicate the extent to which they felt distress with 7 items | Telzer and Fuligni, 2009 [97] | High school students; ethnically diverse sample of adolescents from predominantly Latin American, Asian, and European backgrounds | Each evening during the 2-week period, adolescents’ daily mood assessed | 0.76 and 0.94 for daily level and individual level | Perceived demand +, Role fulfilment − | |
| Internalizing and externalizing problems | Child behavior Checklist/teacher report form (CBCL/TRF) [144]: 113 items, teacher rating, rate on a 3 point scale form 0 (not true) to 2 (very or often true). 8 subscale symptoms: internalizing problems—withdrawn, somatic complaints, anxiety and depression. Externalizing problems—aggressive behavior, and delinquent behaviors | Champion et al., 2009 [51] | Mother with/without history of depression from urban area | Used only the depression-anxiety symptoms, and the social competence; Mother reported on adolescents’ symptoms | None stated | EP +, IP ns |
| Macfie et al., 2005 [73] | Rural families; waves of data collected on families | Used four composite scores: internalizing, externalizing, attention problems, and social problems; Teacher report child behavior when child is 5 yr 10 mos | None stated | Paternal role reversal ns, maternal role reversal ns | ||
| Nuttall, Valentino, Cummings, and Davies, 2021 [83] | Data collected when children were in kindergarten (Wave 1), first grade (Wave 2), and second grade (Wave 3) | Mother reported, and father reported at Wave 1–3 | Ext: 0.87–0.90 Int: 0.84–0.88 | |||
| Peris et al., 2008 [86] | Family triads, longitudinal design | None stated | Maternal EP and EXT/INT+ | |||
| Prussien et al., 2018 [88] | Mothers with children diagnosed with cancer | Mother reported; only look at anxious/depressed symptom subscale | T1: 0.74 T3: 0.86 | Emotional caregiving ns boys, + girls | ||
| Youth Self Report (YSR) [145]: 112 items, self-report, rate from 0 (not true) to 2 (Very true or often true). 8 subscale symptoms: internalizing problems—withdrawn, somatic complaints, anxiety and depression. Externalizing problems—aggressive behavior, and delinquent behaviors | Champion et al., 2009 [51] | Mother with/without history of depression from urban area | Used only the depression-anxiety symptoms, and the social competence | None stated | EP+, IP ns | |
| Peris et al., 2008 [86] | Family triads, longitudinal design | None stated | Maternal EP and EXT/INT+ | |||
| Shaffer and Egeland, 2011 [92] | Mother of low socioeconomic status recruited through a public health clinic for prenatal care | Internalizing and externalizing symptom were self-reported at age 16 T scores were used | Externalizing: 0.93. Internalizing: 0.91 | For both EXT and INT: Childhood BD ns, Adolescent BD + (control for childhood BD) | ||
| Van Loon et al., 2017 [104] | Adolescents living with a parent with mental health problems | EXT, INT measured at T1 and T2 one year apart | Ext: 0.82 at T1; 0.83 at T2; INT: 0.87 at T1; and 0.89 at T2 | Overall + | ||
| Wang et al., 2017 [106] | Two elementary school and three high school students | Only used the 17-item aggression subscale | None reported | Coalition ns, Scapegoating +, Parentification − | ||
| The Behavior Assessment System for Children (BASC) [146]: 5 separate rating forms, including a teacher rating scale (TRS), a parent rating scale (PRS) a self-report of personality (SRP), student observation system (SOS) and a structured developmental history (SDH). The full measure has 105–165 items and uses 4-point scale from 0 (never) to 3 (almost always | Khafi et al., 2014 [70] | Sample overrepresents mothers with anxiety, affective, and/or substance use disorders; predominantly low-income | Mothers completed PRS for the Child (ages 8–11) or Adolescent (ages 12–18 version depending on the child’s age | Child externalizing: child form 0.93 and adolescent form 0.96 and 0.94 at T1 and T2 | T1 EP for T2 EXT: Blacks ns, Whites +; T1 IP for T2 EXT ns | |
| McMahon and Luthar, 2007 [77] | Urban, low-income children living with biological mothers; includes mothers (a) with drug problem, (b) with psychiatric problem, or (c) none of the two | Parent report using PRS; and child report using the SRP child report INT, school maladjustment and social competence; mother report INT, EXT and social competence of the child | None stated | Linear and quadratic term of care for mother + | ||
| The Infant-Toddler Social and Emotional Assessment (ITSEA) [147]: parent report, include a scale for externalizing problems (conceptualized as aggression, defiance, negative emotional reactivity and high activity) | Nuttall et al., 2012 [82] | Community sample; high-risk, first-time adolescent and adult mothers | Mother report child’s externalizing problems at 36 month of age | none stated | Overall + | |
| The Strengths and Difficulties Questionnaire (SDQ) [148]: 25-item, rate on a 3-point ordinal scale (0 = not true, 2 = certainly true) | Zvara et al., 2018 [113] | Rural, low-income families | Teacher rated version of the SDQ for children’s internalizing, externalizing symptoms, and peer problems at Grade 1 | Internalizing: 0.80 Externalizing: 0.84 Peer problem: 0.73 | INT: Role confusion + EXT: role confusion ns | |
| Anti-social Behavior | 10 items measuring antisocial behavior in the last 12 months at baseline and at follow-up. These items have been used in other national studies (e.g., The National Longitudinal Study of Adolescent to Adult Health). Participants responded on 5-point scale (0 = never; 1 = once, 2 = twice; 3 = 3 or 4 times; and 4 = 5 or more). Scores on each item were dichotomized then summed to a variety score | Chen et al., 2018 [53] | Transitional-aged youth | Baseline: 0.75 1-year follow up: 0.67 | PFP ns, SFP ns, PBP − | |
| The Antisocial Behaviour Questionnaire (ABQ) [149]: 10 items, self-reports, rate on a 5-point scale form 1 (never) to 5 (always), sum score | McGauran et al., 2019 [76] | Offender/non-offender samples; all white | None | 0.86 | Overall ns | |
| The Conduct Disorder scale [150], 27 items, self-report about past 3 months. Rated on 1 (no) and 2 (yes) and sum items for score. Have three scales: aggression (5 items), criminal behavior (14 items) and rebellious behavior (3 items) | Stein et al., 1999 [95] | Non-infected adolescents of parents with AIDS | Excluded five items and used only 22 items; Used the three subscale to form a latent variable called conduct problem | 0.78 for 27 item; 0.78 for 22-item | Parental role + | |
| Substance use | The Alcohol Use Disorders Identification Test (AUDIT) [151]: 10 items, self-report, rate on a 5-point Likert scale from 0 (never) to 4 (daily or almost daily). Sum score | Hooper, Doehler, et al., 2012 [65] | Rural community sample | Parent self-report | None stated | Overall ns |
| Hooper, Wallace, et al., 2012 [3] | College students | None | Total: 0.78 Black: 0.70 White: 0.79 | PFP ns, SFP ns, PBP ns | ||
| Jankowski and Hooper, 2014 [67] | College students | None | 0.78 | Unfairness + | ||
| CAGE questionnaire [152]: The name CAGE derives from the four items: “Cut back on drinking”, “Annoyance at criticisms about drinking”, “Feeling Guilty about drinking” and “Using alcohol as an Eye opener”. All items require “yes” or “no” answers | Dragan and Hardt, 2016 [56] | Subjects all registered with a market research company | The item “Guilt” was excluded from the analysis due to the excessive difference between the samples of Poles and Germans; A binary variable “problematic alcohol use” was set to “1” whenever at least one of the three items was endorsed | None stated | Paternal role reversal ns | |
| One item only, derived from the Youth Risk Behavior Surveillance System (Centers for Disease Control and Prevention), “During the past 30 days, on how many days did you have at least one drink of alcohol?’’. Rate on a scale from 0 (0 days) to 7 (all 30 days) | Hooper, Doehler, et al., 2012 [65] | Rural community sample | Adolescent self-report | None stated | Overall ns | |
| 3 items, including the number of cigarettes smoked per day, total frequency of drinks of any form, and quantity of alcohol use on the day of alcohol consumptions over the past 3 months | Stein et al., 2007 [19] | Children with HIV/AIDS-infected mothers | Used as latent variable | N/A | Overall predict use 6 yrs later − | |
| 3 frequency indicators showing use of alcohol, hard drugs, and marijuana within the past 90 days | Lester et al., 2010 [72] | Adolescent with HIV/AIDS-infected mothers, or adolescent of neighborhood control mothers | Formed a latent variable with 3 indicators | N/A | Role reversal − | |
| 3 primary indicators, alcohol frequency, marijuana frequency, and drug problems (sum of 5 items (no = 1, yes = 2) that assessed whether they had any problems with drug such as feelings of dependency or withdrawal symptoms) in past 3 months | Stein et al., 1999 [95] | Non-infected adolescents of parents with AIDS | Used to form a latent variable | None stated | Parental role +, Spousal role ns, | |
| self-report regarding lifetime use: Six response options ranged from 0 to 7 or more times. Recent use of substances: Six response options ranged from 0 days to 20–30 days | Sullivan et al., 2018 [96] | Middle and high school students | Only used the 4 most endorsed substances: (a) a whole cigarette, (b) one full drink of alcohol, (c) marijuana, and (d)inhalants | None stated | High parentification class have lower prob to be polysubstance user than in abstained class | |
| 2 items, whether they ever use alcohol or marijuana | Sang et al., 2014 [20] | African American and Hispanic mother; HIV-negative daughter; low-income inner-city, recruited in agencies that provided services to HIV-infected women; victims of intimate partner violence, and those in substance use recovery | Lifetime use of substance; separated them for analyses | N/A | Overall ns, Spousal, parent or sibling vis-a-via parent ns | |
| 3 items [153]: self-report, “How many drinks of alcohol have you had in the last 30 days?” (replaced with cigarettes and marijuana). Rate on a 7-point scale to report alcohol consumption (1 = none to 7 = more than 30), cigarette use (1 = none to 7 = more than 20 cigarettes), and marijuana hits (1 = none to 7 = more than 40 hits) | Shin and Hecht, 2012 [94] | Mexican-heritage; middle school students; use Wave 4–6 only | Assessed at wave 4 and wave 6; Did not specify whether sum or other coding for substance use construct | None stated | W4 adult parentification ns, W4 problem-solving parentification ns | |
| Risky sex | Two items, self-report, indicating both lifetime sexual activity (yes/no) and sexual intention (5 point scale from 1-disagree strongly to 5-agree strongly) | Sang et al., 2014 [20] | African American and Hispanic mother; HIV-negative daughter; low-income inner-city, recruited in agencies that provided services to HIV-infected women; victims of intimate partner violence, and those in substance use recovery | Daughter report; analyzed separately as two outcomes | N/A | Overall—(intention), Overall ns (lifetime) |
| One item, self-report, the number of times they had sex without a condom in the past 6 months | Lester et al., 2010 [72] | Adolescent with HIV/AIDS-infected mothers, or adolescent of neighborhood control mothers | Due to skewed and kurtoses of scores, they were transformed to square root for the analysis | N/A | Role reversal ns | |
| Two items: (1) Total partners, the total number of different people with whom they had sex in the last 3 months. (2) Sex last 3 months, whether they had sex within the last 3 months (no = 1/yes = 2) | Stein et al., 1999 [95] | Non-infected adolescents of parents with AIDS | Formed latent variable with the two indicators | N?A | Parental role +, Spousal role ns, Nonspecific adult role ns | |
| Psychological/psychiatric Symptom | The Trauma Symptoms Checklist (TSC-33) [154]: 33-item, self-report, rate on a 4-point scale ranging from never to very often for psychological symptoms in the last 2 months | Mayseless et al., 2004 [25] | Community sample | Used total distress score across the 5 subscales to evaluate current functioning | 0.88 | Role reversal ns |
| The Comprehensive Assessment of At-Risk Mental States (CAARMS) [155]: Items are scored on a 3-point scale form “absent/false” to “threshold/true”. Subscales assess 7 domains of the psychosis prodrome, severity and frequency/duration for each subscale rate from 0 to 6. The severity of subclinical positive and negative symptoms was calculated by summing the individual severity subscales within each symptom domain to get the severity of subclinical positive and negative symptoms. Sum the severity subscales within symptom domain | Sheinbaum et al., 2015 [93] | College students | Three dimensional scores: paranoid, schizotypal and schizoid; Two subclinical symptom scores: positive and negative symptoms | None stated | Role reversal all + | |
| The Schedule for Affective Disorders and Schizophrenia—Child version (K-SADS) [156]: structural clinical interview to assess psychiatric symptomatology in three domains: affective, behavioral, and anxiety disorder | Shaffer and Egeland, 2011 [92] | Mother of low socioeconomic status recruited through a public health clinic for prenatal care | Children at age of 17.5 completed the interview; The final composite score for total symptoms is computed as the averages of the natural log transformed scores in each of the three domains | None stated | Childhood BD ns, Adolescent BD + (control for childhood BD) | |
| Self-esteem | The Rosenberg Self-esteem Scale [157]: 10-item, self-report, rate on a 4-point Likert scale from 1 (strongly disagree) to 4 (strongly agree). Sum score | Borchet, Lewandowska-Walter, Połomski, Peplińska, and Hooper, 2020 [45] | Polish sample; majority self-identified college students | Adapted Polish version of the scale | 0.90 | PB + |
| Murrin et al., 2021 [78] | College students; typically developing (TD) who reported having a sibling with Autism Spectrum Disorder (ASD) | 0.90 | PFP ns, SFP ns | |||
| Oznobishin and Kurman, 2009 [85] | College students (Study 1) and high school students (Study 2); both studies include immigrant or Israeli-born | 0.86 for both groups | Child dominance ns, Language brokering ns | |||
| Nuttall, Ballinger, Levendosky, and Borkowski, 2021 [80] | Majority of mother sample were non-White (78.4%) and unmarried (74%) | Six items rated on 7-point Likert scale instead; derived from the Rosenberg Self-esteem Scale but it is a subscale in the Psychological Coping Resources | 6, 24 and 36 months: 0.82, 70, 89 | EP ns, IP ns, Unfairness - | ||
| Wang et al., 2017 [106] | Two elementary school and three high school students | None stated | Coalition ns, Scapegoating −, Parentification + | |||
| Satisfaction with life | Satisfaction With Life Scale (SWLS) [158]: 5 items, self-report, rate on 5-point scale from 1 (strongly disagree) to 5 (strongly agree) | Çimşir and Akdoğan, 2021 [55] | College students | Turkish version | 0.89 | PFP ns |
| Hooper et al., 2015 [66] | College students | Used rating on a 7-point Likert-type scale from 7 (strongly agree) to 1 (strongly disagree) | 0.89 | PFP −, SFP −, PBP + | ||
| Oznobishin and Kurman, 2009 [85] | College students (Study 1) and high school students (Study 2); both studies include immigrant or Israeli-born | 0.77 and 0.81 for immigrant and for Israeli-born groups | Child dominance + | |||
| Self-efficacy | The parenting self-efficacy subscale was an expansion of the Psychological Coping Resources measure [159]: 6 items, self-report, rate on a 7-point scale assess parental evaluative cognitions about their abilities to adequately care for their children | Nuttall, Ballinger, et al., 2021 [80] | Majority of mother sample were non-White (78.4%) and unmarried (74%) | 0.75 (36 month visit) | EP ns, IP ns, Unfairness + | |
| Generalized self-efficacy scale [160]: 8 items, rate on a 6-point scale from 1 (not at all true) to 6 (absolutely true) | Oznobishin and Kurman, 2009 [85] | College students (Study 1) and high school students (Study 2); both studies include immigrant or Israeli-born | 0.90 and 0.94 for the immigrant and Israeli-born groups. | Child dominance ns, Language brokering - | ||
| Titzmann, 2012 [98] | Ethnic (185) and 197 native German families | Adolescent self-report | 0.86 | EP ns, IP+ |
3.4. Substantive Themes—Quantitative Studies
3.5. Substantive Themes—Qualitative and Mixed Methods Studies
3.6. Integrated Themes—Quantitative, Mixed, and Qualitative Studies
| Qualitative/Mixed Themes | Quantitative Themes | Alignment/Integration | |
|---|---|---|---|
| Resilience, Positive Outcomes, and Self-Preservation | Personal Growth and Strengthened Sibling Relationships Come from Adversity
| Positive Outcomes of Self-Esteem, Efficacy, and Satisfaction with Life had many null findings; when a direction was reported, it trended toward parentification being linked with some positive outcomes. (Quant theme 3)
| Across qualitative, quantitative, and mixed methods studies, positive outcomes in the form of resilience and positive coping were reported. Influential factors include the type of parentification—instrumental and the strengthening of relationships such as those with siblings. Although specific outcome constructs varied, these factors confer feelings of contributing to the household or family and opportunities to develop skills related to empathy, agency, esteem, and prioritization of others. |
Self-Preservation Protective Mechanisms—Self-sacrifice and Distancing
| Exploration of moderators to explain effect heterogeneity: exacerbating effect of maternal depression and protective roles of disclosure of worries, social support, and religious service attendance (Quant Theme 5).
| Youth employed several strategies to protect themselves or their parents from additional trauma. Mechanisms include not sharing information with parents that would increase their worry and stress; distancing themselves from parents even though they experience a tension between desired closeness and avoiding additional suffering. The family environment (e.g., maternal mental health or support) served to either protect or place youth at greater risk for negative outcomes. | |
| Compromised Development or Negative Outcomes | Premature Transitions, Compromised Human and Social Capital, Lost Childhood, and Difficulty Forming Adult Relationships | Not measured or mentioned. | Not applicable. |
Suboptimal Mental and Physical Health among Parentified Youth—Vulnerabilities and Stacking Risk Factors
| 1. Internalizing Problems Linked to Parentification in General and Emotional Parentification in Particular (Quant Theme 1)2. Emotional Parentification Related to Broad-Spectrum Externalizing Problems (Quant Theme 2) | Parentified children experienced negative outcomes in the areas of mental health or internalizing problems (e.g., depression, anxiety), externalizing problems (e.g., substance use, sexual risk-taking), and physical health (e.g., physical abuse, poor nutrition). Relationships with physical health and externalizing outcomes were more present in qualitative accounts than in quantitative statistical tests. | |
| Moderators and Measurement Implications | Modifying Influences: Perceptions, Acknowledgement, Initial Competencies, and Supports Make the Difference between Floundering, Resilience, and Thriving
| Mechanisms and Parentification as Mediators. (Quant Theme 4)
| The report of positive or negative outcomes was influenced by afflicted youths’ characteristics (e.g., self-differentiation, rejection sensitivity), attachment style, and perceptions of the benefits or fairness of these adult responsibilities. These factors mediate how family risk factors relate to outcomes—protective/buffering or increasing risk. The buffering effect of other social supports (e.g., community members, teachers, and others) was reported to reduce the outcome severity youth experienced. Perceived benefits and fairness were associated with fewer negative mental health outcomes. These factors influenced the type of trajectory youth traversed (e.g., severity degree and positive/negative nature). |
4. Discussion
4.1. Summary of Findings
4.2. The Role of Culture and Context
4.3. Dimensions of Parentification and Promising Research Directions
4.4. Perceptions and Perceived Benefits of Parentification
4.5. Adverse and Positive Life Outcomes
4.6. Adopting a Developmental and Systems Perspective
4.7. Youth Measure and Non-Linear Modeling and Explanation Considerations
4.8. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Burton, L. Childhood Adultification in Economically Disadvantaged Families: A Conceptual Model. Fam. Relat. 2007, 56, 329–345. [Google Scholar] [CrossRef]
- Hooper, L.M. Parentification, in Encyclopedia of Adolescence; Levesque, R.J.R., Ed.; Springer: New York, NY, USA, 2011; pp. 2023–2031. [Google Scholar]
- Hooper, L.M.; Wallace, S.A.; Doehler, K.; Dantzler, J. Parentification, Ethnic Identity, and Psychological Health in Black and White American College Students: Implications of Family-of-Origin and Cultural Factors. J. Comp. Fam. Stud. 2012, 43, 811–835. [Google Scholar] [CrossRef]
- Carver, C.S. Resilience and Thriving: Issues, Models, and Linkages. J. Soc. Issues A J. Soc. Psychol. Study Soc. Issues. 1998, 54, 245–266. [Google Scholar] [CrossRef]
- Ireland, M.S. Reconceiving Women: Separating Motherhood from Female Identity; Guilford Press: New York, NY, USA, 1993. [Google Scholar]
- Siskowski, C. Young caregivers: Effect of family health situations on school performance. J. Sch. Nurs. 2006, 22, 163–169. [Google Scholar] [CrossRef]
- King, T.L. Young carers in the COVID-19 pandemic: Risks for mental health. Lancet Reg. Health West. Pac. 2021, 16, 100307. [Google Scholar] [CrossRef]
- Borchet, J.; Lewandowska-Walter, A.; Połomski, P.; Peplińska, A.; Hooper, L.M. The Relations Among Types of Parentification, School Achievement, and Quality of Life in Early Adolescence: An Exploratory Study. Front. Psychol. 2021, 12, 635171. [Google Scholar] [CrossRef]
- First Focus on Children. Fact Sheet: Kids & COVID by the Numbers. 2022. Available online: https://firstfocus.org/resources/fact-sheet/kids-and-covid-by-the-numbers* (accessed on 16 June 2023).
- World Bank. Learning Losses from COVID-19 Could Cost this Generation of Students Close to $17 Trillion in Lifetime Earnings. 2021. Available online: https://www.unicef-irc.org/article/2199-the-state-of-global-education.html (accessed on 16 June 2023).
- Greenberg, R.; Jurkovic, G.J. Lost Childhoods: The Plight of the Parentified Child; Brunner/Mazel, Inc.: New York, NY, USA, 1997. [Google Scholar]
- Anderson, L.R.; Hemez, P.F.; Kreider, R.M. Living Arrangments of Children: 2019, in Current Population Reports; Census Bureau: Washington, DC, USA, 2022; pp. 70–174. [Google Scholar]
- Friedenberg, E.Z.; Minuchin, S. Families of the Slums; Basic Books: New York, NY, USA, 1967. [Google Scholar]
- Patterson, J.M. Integrating Family Resilience and Family Stress Theory. J. Marriage Fam. 2002, 64, 349–360. [Google Scholar] [CrossRef]
- Hendricks, B.A.; Vo, J.B.; Dionne-Odom, J.N.; Bakitas, M.A. Parentification Among Young Carers: A Concept Analysis. Child Adolesc. Soc. Work. J. 2021, 38, 519–531. [Google Scholar] [CrossRef]
- Hooper, L.M. Expanding the Discussion Regarding Parentification and Its Varied Outcomes: Implications for Mental Health Research and Practice. J. Ment. Health Couns. 2007, 29, 322–337. [Google Scholar] [CrossRef]
- Hooper, L.M.; Marotta, S.A.; Lanthier, R.P. Predictors of Growth and Distress Following Childhood Parentification: A Retrospective Exploratory Study. J. Child Fam. Stud. 2008, 17, 693–705. [Google Scholar] [CrossRef]
- Boszormenyi-Nagy, I.; Spark, G.M. Invisible Loyalties: Reciprocity in Intergenerational Family Therapy; Harper & Row: Hagerstown, MD, USA, 1973. [Google Scholar]
- Stein, J.A.; Lester, P.; Rotheram-Borus, M.J. Impact of Parentification on Long-Term Outcomes Among Children of Parents With HIV/AIDS. Fam. Process. 2007, 46, 317–333. [Google Scholar] [CrossRef] [PubMed]
- Sang, J.; Cederbaum, J.A.; Hurlburt, M.S. Parentification, Substance Use, and Sex among Adolescent Daughters from Ethnic Minority Families: The Moderating Role of Monitoring. Fam. Process. 2013, 53, 252–266. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, 105906. [Google Scholar]
- Page, M.J.; Moher, D.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. PRISMA 2020 explanation and elaboration: Updated guidance and exemplars for reporting systematic reviews. BMJ 2021, 372, n160. [Google Scholar] [CrossRef] [PubMed]
- Hong, Q.N.; Fàbregues, S.; Bartlett, G.; Boardman, F.; Cargo, M.; Dagenais, P.; Gagnon, M.-P.; Griffiths, F.; Nicolau, B.; O’cathain, A.; et al. The Mixed Methods Appraisal Tool (MMAT) version 2018 for information professionals and researchers. Educ. Inf. 2018, 34, 285–291. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef]
- Mayseless, O.; Bartholomew, K.; Henderson, A.; Trinke, S. “I was more her Mom than she was mine“: Role Reversal in a Community Sample. Fam. Relat. 2004, 53, 78–86. [Google Scholar] [CrossRef]
- Callaghan, J.E.M.; Alexander, J.H.; Sixsmith, J.; Fellin, L. Children’s experiences of domestic violence and abuse: Siblings’ accounts of relational coping. Clin. Child Psychol. Psychiatry 2016, 21, 649–668. [Google Scholar] [CrossRef]
- Chademana, K.E.; van Wyk, B. Life in a child-headed household: Exploring the quality of life of orphans living in child-headed households in Zimbabwe. Afr. J. AIDS Res. 2021, 20, 172–180. [Google Scholar] [CrossRef]
- Chee, L.P.; Goh, E.C.L.; Kuczynski, L. Oversized Loads: Child Parentification in Low-Income Families and Underlying Parent–Child Dynamics. Fam. Soc. J. Contemp. Soc. Serv. 2014, 95, 204–212. [Google Scholar] [CrossRef]
- Collado, Z. Displacement, miseries, and responsibilities: What does it mean to rebuild the home among young people affected by conflict in the southern Philippines? Vulnerable Child. Youth Stud. 2021, 16, 259–266. [Google Scholar] [CrossRef]
- Gelman, C.R.; Rhames, K. In their own words: The experience and needs of children in younger-onset Alzheimer’s disease and other dementias families. Dement. Int. J. Soc. Res. Pract. 2018, 17, 337–358. [Google Scholar] [CrossRef] [PubMed]
- Kabat, R. A role-reversal in the mother-daughter relationship. Clin. Soc. Work. J. 1996, 24, 255–269. [Google Scholar] [CrossRef]
- Keigher, S.; Zabler, B.; Robinson, N.; Fernandez, A.; Stevens, P.E. Young caregivers of mothers with HIV: Need for supports. Child. Youth Serv. Rev. 2005, 27, 881–904. [Google Scholar] [CrossRef]
- Kosner, A.; Roer-Strier, D.; Kurman, J. Changing Familial Roles for Immigrant Adolescents from the Former Soviet Union to Israel. J. Adolesc. Res. 2014, 29, 356–379. [Google Scholar] [CrossRef]
- Petrowski, C.E.; Stein, C.H. Young Women’s Accounts of Caregiving, Family Relationships, and Personal Growth When Mother Has Mental Illness. J. Child Fam. Stud. 2016, 25, 2873–2884. [Google Scholar] [CrossRef]
- Rizkalla, N.; Mallat, N.K.; Arafa, R.; Adi, S.; Soudi, L.; Segal, S.P. “Children Are Not Children Anymore; They Are a Lost Generation”: Adverse Physical and Mental Health Consequences on Syrian Refugee Children. Int. J. Environ. Res. Public Health 2020, 17, 8378. [Google Scholar] [CrossRef]
- Saha, A. Parentification: Boon or Bane? J. Psychosoc. Res. 2016, 11, 289–301. [Google Scholar]
- Tahkola, E.; Metsäpelto, R.; Ruohotie-Lyhty, M.; Poikkeus, A. Relationships of young adults with foster care backgrounds: Tensions and management strategies. Child Fam. Soc. Work. 2020, 26, 358–369. [Google Scholar] [CrossRef]
- Tedgård, E.; Råstam, M.; Wirtberg, I. An upbringing with substance-abusing parents: Experiences of parentification and dysfunctional communication. Nord. Stud. Alcohol Drugs 2019, 36, 223–247. [Google Scholar] [CrossRef]
- Abraham, K.M.; Stein, C.H. When Mom has a Mental Illness: Role Reversal and Psychosocial Adjustment Among Emerging Adults. J. Clin. Psychol. 2013, 69, 600–615. [Google Scholar] [CrossRef] [PubMed]
- Arellano, B.; Mier-Chairez, J.; Tomek, S.; Hooper, L.M. Parentification and Language Brokering: An Exploratory Study of the Similarities and Differences in Their Relations to Continuous and Dichotomous Mental Health Outcomes. J. Ment. Health Couns. 2018, 40, 353–373. [Google Scholar] [CrossRef]
- Baggett, E.; Shaffer, A.; Muetzelfeld, H. Father–Daughter Parentification and Young Adult Romantic Relationships Among College Women. J. Fam. Issues 2015, 36, 760–783. [Google Scholar] [CrossRef]
- Beffel, J.H.; Nuttall, A.K. Influences of parentification and benefit finding on prosocial behavior among typically developing siblings of individuals with autism spectrum disorder. Res. Dev. Disabil. 2020, 104, 103694. [Google Scholar] [CrossRef] [PubMed]
- Borchet, J.; Lewandowska-Walter, A. Parentification—Its direction and perceived benefits in terms of connections with late adolescents’ emotional regulation in the situation of marital conflict. Curr. Issues Pers. Psychol. 2017, 5, 113–122. [Google Scholar] [CrossRef]
- Borchet, J.; Lewandowska-Walter, A.; Połomski, P.; Peplińska, A. Construction of a Parentification Questionnaire for Youth. Health Psychol. Rep. 2020, 8, 175–188. [Google Scholar] [CrossRef]
- Borchet, J.; Lewandowska-Walter, A.; Połomski, P.; Peplińska, A.; Hooper, L.M. We are in this Together: Retrospective Parentification, Sibling Relationships, and Self-Esteem. J. Child Fam. Stud. 2020, 29, 2982–2991. [Google Scholar] [CrossRef]
- Borchet, J.; Lewandowska-Walter, A.; Rostowska, T. Parentification in late adolescence and selected features of the family system. Health Psychol. Rep. 2016, 4, 116–127. [Google Scholar] [CrossRef][Green Version]
- Boumans, N.P.G.; Dorant, E. A cross-sectional study on experiences of young adult carers compared to young adult noncarers: Parentification, coping and resilience. Scand. J. Caring Sci. 2018, 32, 1409–1417. [Google Scholar] [CrossRef]
- Burton, S.; Hooper, L.M.; Tomek, S.; Cauley, B.; Washington, A.; Pössel, P. The Mediating Effects of Parentification on the Relation Between Parenting Behavior and Well-Being and Depressive Symptoms in Early Adolescents. J. Child Fam. Stud. 2018, 27, 4044–4059. [Google Scholar] [CrossRef]
- Carroll, J.J.; Robinson, B.E. Depression and Parentification among Adults as Related to Parental Workaholism and Alcoholism. Fam. J. 2000, 8, 360–367. [Google Scholar] [CrossRef]
- Castro, D.M.; Jones, R.A.; Mirsalimi, H. Parentification and the Impostor Phenomenon: An Empirical Investigation. Am. J. Fam. Ther. 2004, 32, 205–216. [Google Scholar] [CrossRef]
- Champion, J.E.; Jaser, S.S.; Reeslund, K.L.; Simmons, L.; Potts, J.E.; Shears, A.R.; Compas, B.E. Caretaking behaviors by adolescent children of mothers with and without a history of depression. J. Fam. Psychol. 2009, 23, 156–166. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.Y.-C.; Panebianco, A. Physical and psychological conditions of parental chronic illness, parentification and adolescent psychological adjustment. Psychol. Health 2020, 35, 1075–1094. [Google Scholar] [CrossRef] [PubMed]
- Chen, F.R.; Dariotis, J.K.; Granger, D.A. Linking testosterone and antisocial behavior in at-risk transitional aged youth: Contextual effects of parentification. Psychoneuroendocrinology 2018, 91, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Cho, A.; Lee, S. Exploring effects of childhood parentification on adult-depressive symptoms in Korean college students. J. Clin. Psychol. 2019, 75, 801–813. [Google Scholar] [CrossRef]
- Çimşir, E.; Akdoğan, R. Childhood Emotional Incest Scale (CEIS): Development, validation, cross-validation, and reliability. J. Couns. Psychol. 2021, 68, 98–111. [Google Scholar] [CrossRef]
- Dragan, M.; Hardt, J. Childhood adversities and risk for problematic alcohol use. Addict. Behav. 2016, 59, 65–71. [Google Scholar] [CrossRef]
- Duval, J.; Ensink, K.; Normandin, L.; Fonagy, P. Mentalizing Mediates the Association Between Childhood Maltreatment and Adolescent Borderline and Narcissistic Personality Traits. Adolesc. Psychiatry 2018, 8, 156–173. [Google Scholar] [CrossRef]
- Fitzgerald, M.M.; Schneider, R.A.; Salstrom, S.; Zinzow, H.M.; Jackson, J.; Fossel, R.V. Child sexual abuse, early family risk, and childhood parentification: Pathways to current psychosocial adjustment. J. Fam. Psychol. 2008, 22, 320–324. [Google Scholar] [CrossRef]
- Fortin, A.; Doucet, M.; Damant, D. Children’s Appraisals as Mediators of the Relationship Between Domestic Violence and Child Adjustment. Violence Vict. 2011, 26, 377–392. [Google Scholar] [CrossRef] [PubMed]
- Godsall, R.E.; Jurkovic, G.J.; Emshoff, J.; Anderson, L.; Stanwyck, D. Why some kids do well in bad situations: Relation of parental alcohol misuse and parentification to children’s self-concept. Subst. Use Misuse 2004, 39, 789–809. [Google Scholar] [CrossRef] [PubMed]
- Golan, Y.; Goldner, L. The contributions of boundary dissolution and trust in the romantic partner to young mothers’ parenting representations. Early Child Dev. Care 2019, 189, 463–475. [Google Scholar] [CrossRef]
- Goldner, L.; Abir, A.; Sachar, C.S. Adolescents’ True-Self Behavior and Parent-Adolescent Boundary Dissolution: The Mediating Role of Rejection Sensitivity. Child Indic. Res. 2017, 10, 381–402. [Google Scholar] [CrossRef]
- Goldner, L.; Sachar, S.C.; Abir, A. Mother-Adolescent Parentification, Enmeshment and Adolescents’ Intimacy: The Mediating Role of Rejection Sensitivity. J. Child Fam. Stud. 2019, 28, 192–201. [Google Scholar] [CrossRef]
- Hoffman, Y.; Shrira, A. Variables Connecting Parental PTSD to Offspring Successful Aging: Parent–Child Role Reversal, Secondary Traumatization, and Depressive Symptoms. Front. Psychiatry 2019, 10, 718. [Google Scholar] [CrossRef]
- Hooper, L.M.; Doehler, K.; Jankowski, P.J.; Tomek, S.E. Patterns of Self-Reported Alcohol Use, Depressive Symptoms, and Body Mass Index in a Family Sample: The Buffering Effects of Parentification. Fam. J. 2012, 20, 164–178. [Google Scholar] [CrossRef]
- Hooper, L.M.; Tomek, S.; Bond, J.M.; Reif, M.S. Race/Ethnicity, Gender, Parentification, and Psychological Functioning: Comparisons Among a Nationwide University Sample. Fam. J. 2015, 23, 33–48. [Google Scholar] [CrossRef]
- Jankowski, P.J.; Hooper, L.M. Parentification and Alcohol Use: Conditional Effects of Religious Service Attendance. Couns. Values 2014, 59, 174–191. [Google Scholar] [CrossRef]
- Jankowski, P.J.; Hooper, L.M.; Sandage, S.J.; Hannah, N.J. Parentification and mental health symptoms: Mediator effects of perceived unfairness and differentiation of self. J. Fam. Ther. 2013, 35, 43–65. [Google Scholar] [CrossRef]
- Katz, J.; Petracca, M.; Rabinowitz, J. A Retrospective Study of Daughters’ Emotional Role Reversal with Parents, Attachment Anxiety, Excessive Reassurance-Seeking, and Depressive Symptoms. Am. J. Fam. Ther. 2009, 37, 185–195. [Google Scholar] [CrossRef]
- Khafi, T.Y.; Yates, T.M.; Luthar, S.S. Ethnic Differences in the Developmental Significance of Parentification. Fam. Process. 2014, 53, 267–287. [Google Scholar] [CrossRef] [PubMed]
- King, J.; Mallinckrodt, B. Family environment and alexithymia in clients and non-clients. Psychother. Res. 2000, 10, 78–86. [Google Scholar] [CrossRef]
- Lester, P.; Stein, J.A.; Bursch, B.; Rice, E.; Green, S.; Penniman, T.; Rotheram-Borus, M.J. Family-based processes associated with adolescent distress, substance use and risky sexual behavior in families affected by maternal HIV. J. Clin. Child Adolesc. Psychol. 2010, 39, 328–340. [Google Scholar] [CrossRef][Green Version]
- Macfie, J.; Houts, R.M.; McElwain, N.L.; Cox, M.J. The Effect of Father-Toddler and Mother- Toddler Role Reversal on the Development of Behavior Problems in Kindergarten. Soc. Dev. 2005, 14, 514–531. [Google Scholar] [CrossRef]
- Macfie, J.; Houts, R.M.; Pressel, A.S.; Cox, M.J. Pathways from infant exposure to marital conflict to parent–toddler role reversal. Infant Ment. Health J. 2008, 29, 297–319. [Google Scholar] [CrossRef]
- Madden, A.R.; Shaffer, A. The relation between parentification and dating communication: The role of romantic attachment-related cognitions. Fam. J. 2016, 24, 313–318. [Google Scholar] [CrossRef]
- McGauran, A.; Brooks, M.; Khan, R. The role of emotional resilience, childhood parentification, and attachment style on antisocial behaviour in adulthood: A comparison of an offender and normative population. J. Crim. Psychol. 2019, 9, 75–87. [Google Scholar] [CrossRef]
- McMahon, T.J.; Luthar, S.S. Defining characteristics and potential consequences of caretaking burden among children living in urban poverty. Am. J. Orthopsychiatry 2007, 77, 267–281. [Google Scholar] [CrossRef]
- Murrin, M.; Beffel, J.H.; Nuttall, A.K. The Moderating Role of Self-Disclosure Among Typically Developing Siblings of Individuals with Autism Spectrum Disorder. J. Child Fam. Stud. 2021, 30, 364–374. [Google Scholar] [CrossRef]
- Nebbitt, V.E.; Lombe, M. Urban African American adolescents and adultification. Fam. Soc. J. Contemp. Soc. Serv. 2010, 91, 234–240. [Google Scholar] [CrossRef]
- Nuttall, A.K.; Ballinger, A.L.; Levendosky, A.A.; Borkowski, J.G. Maternal parentification history impacts evaluative cognitions about self, parenting, and child. Infant Ment. Health J. 2021, 42, 315–330. [Google Scholar] [CrossRef] [PubMed]
- Nuttall, A.K.; Coberly, B.; Diesel, S.J. Childhood Caregiving Roles, Perceptions of Benefits, and Future Caregiving Intentions Among Typically Developing Adult Siblings of Individuals with Autism Spectrum Disorder. J. Autism Dev. Disord. 2018, 48, 1199–1209. [Google Scholar] [CrossRef]
- Nuttall, A.K.; Valentino, K.; Borkowski, J.G. Maternal history of parentification, maternal warm responsiveness, and children’s externalizing behavior. J. Fam. Psychol. 2012, 26, 767–775. [Google Scholar] [CrossRef] [PubMed]
- Nuttall, A.K.; Valentino, K.; Cummings, E.M.; Davies, P.T. Contextualizing children’s caregiving responses to interparental conflict: Advancing assessment of parentification. J. Fam. Psychol. 2021, 35, 276–287. [Google Scholar] [CrossRef]
- Nuttall, A.K.; Zhang, Q.; Valentino, K.; Borkowski, J.G. Intergenerational Risk of Parentification and Infantilization to Externalizing Moderated by Child Temperament. J. Marriage Fam. 2019, 81, 648–661. [Google Scholar] [CrossRef]
- Oznobishin, O.; Kurman, J. Parent–child role reversal and psychological adjustment among immigrant youth in Israel. J. Fam. Psychol. 2009, 23, 405–415. [Google Scholar] [CrossRef]
- Peris, T.S.; Goeke-Morey, M.C.; Cummings, E.M.; Emery, R.E. Marital conflict and support seeking by parents in adolescence: Empirical support for the parentification construct. J. Fam. Psychol. 2008, 22, 633–642. [Google Scholar] [CrossRef]
- Perrin, M.B.; Ehrenberg, M.F.; Hunter, M.A. Boundary Diffusion, Individuation, and Adjustment: Comparison of Young Adults Raised in Divorced Versus Intact Families. Fam. Relat. 2013, 62, 768–782. [Google Scholar] [CrossRef]
- Prussien, K.V.; Murphy, L.K.; Gerhardt, C.A.; Vannatta, K.; Bemis, H.; Desjardins, L.; Ferrante, A.C.; Shultz, E.L.; Keim, M.C.; Cole, D.A.; et al. Longitudinal associations among maternal depressive symptoms, child emotional caretaking, and anxious/depressed symptoms in pediatric cancer. J. Fam. Psychol. 2018, 32, 1087–1096. [Google Scholar] [CrossRef]
- Rodriguez, A.J.; Margolin, G. Stepping Up, Sticking Together: Military Adolescents’ Support of Their Civilian Parents and Concurrent Depression Symptoms. J. Clin. Child Adolesc. Psychol. 2018, 47, S278–S290. [Google Scholar] [CrossRef] [PubMed]
- Rogers, P.; Lowrie, E. Varieties of childhood maltreatment as predictors of adult paranormality and New Age Orientation. Pers. Individ. Differ. 2016, 92, 37–45. [Google Scholar] [CrossRef]
- Schier, K.; Herke, M.; Nickel, R.; Egle, U.T.; Hardt, J. Long-Term Sequelae of Emotional Parentification: A Cross-Validation Study Using Sequences of Regressions. J. Child Fam. Stud. 2015, 24, 1307–1321. [Google Scholar] [CrossRef]
- Shaffer, A.; Egeland, B. Intergenerational Transmission of Familial Boundary Dissolution: Observations and Psychosocial Outcomes in Adolescence. Fam. Relat. 2011, 60, 290–302. [Google Scholar] [CrossRef]
- Sheinbaum, T.; Bifulco, A.; Ballespí, S.; Mitjavila, M.; Kwapil, T.; Barrantes-Vidal, N. Interview Investigation of Insecure Attachment Styles as Mediators between Poor Childhood Care and Schizophrenia-Spectrum Phenomenology. PLoS ONE 2015, 10, e0135150. [Google Scholar] [CrossRef] [PubMed]
- Shin, Y.; Hecht, M.L. Does parentification place Mexican-heritage youth at risk for substance use? Identifying the intervening nature of parent–child communication about alcohol. J. Adolesc. 2012, 36, 149–159. [Google Scholar] [CrossRef]
- Stein, J.A.; Riedel, M.; Rotheram-Borus, M.J. Parentification and Its Impact on Adolescent Children of Parents with AIDS. Fam. Process. 1999, 38, 193–208. [Google Scholar] [CrossRef]
- Sullivan, K.S.; Capp, G.; Gilreath, T.D. The association of parentification indicators with substance use patterns among military-connected adolescents. Am. J. Orthopsychiatry 2018. [Google Scholar] [CrossRef]
- Telzer, E.H.; Fuligni, A.J. Daily family assistance and the psychological well-being of adolescents from Latin American, Asian, and European backgrounds. Dev. Psychol. 2009, 45, 1177–1189. [Google Scholar] [CrossRef]
- Titzmann, P.F. Growing Up Too Soon? Parentification Among Immigrant and Native Adolescents in Germany. J. Youth Adolesc. 2012, 41, 880–893. [Google Scholar] [CrossRef]
- Titzmann, P.F.; Gniewosz, B. With a little help from my child: A dyad approach to immigrant mothers’ and adolescents’ socio-cultural adaptation. J. Adolesc. 2018, 62, 198–206. [Google Scholar] [CrossRef]
- Tomeny, T.S.; Barry, T.D.; Fair, E.C.; Riley, R. Parentification of Adult Siblings of Individuals with Autism Spectrum Disorder. J. Child Fam. Stud. 2017, 26, 1056–1067. [Google Scholar] [CrossRef]
- Tomeny, T.S.; Barry, T.D.; Fair, E.C. Parentification of adult siblings of individuals with autism spectrum disorder: Distress, sibling relationship attitudes, and the role of social support. J. Intellect. Dev. Disabil. 2017, 42, 320–331. [Google Scholar] [CrossRef]
- Tompkins, T.L. Parentification and Maternal HIV Infection: Beneficial Role or Pathological Burden? J. Child Fam. Stud. 2007, 16, 108–118. [Google Scholar] [CrossRef]
- van der Mijl, R.C.W.; Vingerhoets, A.J.J.M. The Positive Effects of Parentification: An Exploratory Study among Students. Psychol. Top. 2017, 26, 417–430. [Google Scholar] [CrossRef]
- Van Loon, L.M.A.; Van De Ven, M.O.M.; Van Doesum, K.T.M.; Hosman, C.M.H.; Witteman, C.L.M. Parentification, Stress, and Problem Behavior of Adolescents who have a Parent with Mental Health Problems. Fam. Process. 2017, 56, 141–153. [Google Scholar] [CrossRef]
- Walsh, S.; Shulman, S.; Bar-On, Z.; Tsur, A. The Role of Parentification and Family Climate in Adaptation Among Immigrant Adolescents in Israel. J. Res. Adolesc. 2006, 16, 321–350. [Google Scholar] [CrossRef]
- Wang, M.; Liu, S.; Belsky, J. Triangulation processes experienced by children in contemporary China. Int. J. Behav. Dev. 2017, 41, 688–695. [Google Scholar] [CrossRef]
- Wells, M.; Glickauf-Hughes, C.; Jones, R. Codependency: A Grass Roots Construct’s Relationship to Shame-Proneness, Low Self-Esteem, and Childhood Parentification. Am. J. Fam. Ther. 1999, 27, 63–71. [Google Scholar] [CrossRef]
- Wells, M.; Jones, R. Relationship among childhood parentification, splitting, and dissociation: Preliminary findings. Am. J. Fam. Ther. 1998, 26, 331–339. [Google Scholar] [CrossRef]
- Wells, M.; Jones, R. Childhood Parentification and Shame-Proneness: A Preliminary Study. Am. J. Fam. Ther. 2000, 28, 19–27. [Google Scholar] [CrossRef]
- Williams, K.; Francis, S.E. Parentification and Psychological Adjustment: Locus of Control as a Moderating Variable. Contemp. Fam. Ther. Int. J. 2010, 32, 231–237. [Google Scholar] [CrossRef]
- Woolgar, M.; Murray, L. The representation of fathers by children of depressed mothers: Refining the meaning of parentification in high-risk samples. J. Child Psychol. Psychiatry 2010, 51, 621–629. [Google Scholar] [CrossRef]
- Yew, W.P.; Siau, C.S.; Kwong, S.F. Parentification and Resilience Among Students with Clinical and Nonclinical Aspirations: A Cross-Sectional Quantitative Study. J. Multicult. Couns. Dev. 2017, 45, 66–75. [Google Scholar] [CrossRef]
- Zvara, B.J.; The Family Life Project Key Investigators; Macfie, J.; Cox, M.; Mills-Koonce, R. Mother–child role confusion, child adjustment problems, and the moderating roles of child temperament and sex. Dev. Psychol. 2018, 54, 1891–1903. [Google Scholar] [CrossRef] [PubMed]
- Wei, H.-S.; Shih, A.-T.; Chen, Y.-F.; Hong, J.S. The impact of adolescent parentification on family relationship and civic engagement. J. Soc. Work. 2020, 21, 1413–1432. [Google Scholar] [CrossRef]
- Wolkin, J.R. Childhood Parentification: An Exploration of Long-Term Effects; Georgia State University: Atlanta, GA, USA, 1984. [Google Scholar]
- Hooper, L.M.; Doehler, K.; Wallace, S.A.; Hannah, N.J. The Parentification Inventory: Development, Validation, and Cross-Validation. Am. J. Fam. Ther. 2011, 39, 226–241. [Google Scholar] [CrossRef]
- Mika, P.; Bergner, R.M.; Baum, M.C. The development of a scale for the assessment of parentification. Fam. Ther. 1987, 14, 229–235. [Google Scholar]
- Jurkovic, G.J.; Thirkield, A.; Morrell, R. Parentification of Adult Children of Divorce: A Multidimensional Analysis. J. Youth Adolesc. 2001, 30, 245–257. [Google Scholar] [CrossRef]
- Godsall, R.E.; Jurkovic, G.J. The Parentification Questionnaire-Youth; Department of Psychology, Georgia State University: Atlanta, GA, USA, 1995. [Google Scholar]
- Jurkovic, G.J.; Sessions, M.W. (Department of Psychology, Georgia State University, Atlanta, GA, USA, 1986). Parentification Questionnaire-Adult. Unpublished instrument.
- Lopez, F.G. Family Structure and Depression: Implications for the Counseling of Depressed College Students. J. Couns. Dev. 1986, 64, 508–511. [Google Scholar] [CrossRef]
- Hooper, L. Parentification inventory [measurement instrument]; The University of Alabama: Tuscaloosa, AL, USA, 2009. [Google Scholar]
- Hooper, L.M.; DeCoster, J.; White, N.; Voltz, M.L. Characterizing the magnitude of the relation between self-reported childhood parentification and adult psychopathology: A meta-analysis. J. Clin. Psychol. 2011, 67, 1028–1043. [Google Scholar] [CrossRef] [PubMed]
- Kerig, P. (Department of Psychology, Miami University, Oxford, OH, USA, 2006). The Parent-Child Boundaries Scale-III (PBS-III). Unpublished measure.
- Mayseless, O.; Scharf, M. Too close for comfort: Inadequate boundaries with parents and individuation in late adolescent girls. Am. J. Orthopsychiatry 2009, 79, 191–202. [Google Scholar] [CrossRef] [PubMed]
- Baker, M.; Tebes, J. The Child Caretaking Scale.; Yale University School of Medicine: New Haven, CT, USA, 1994. [Google Scholar]
- Hardt, J.; Dragan, M.; Schultz, S.; Engfer, A. Parent-Child Relationships in Poland and Germany: A Retrospective Study. Psychology 2011, 02, 502–508. [Google Scholar] [CrossRef][Green Version]
- Alexander, P.C. Parent-Child Role Reversal: Development of a Measure and Test of an Attachment Theory Model. J. Syst. Ther. 2003, 22, 31–44. [Google Scholar] [CrossRef]
- Dorant, E.B.N. Parentification van Jonge Mantelzorgers: De Ontwikkeling van de Maastrichtse Parentificatie Schaal (Parentification of Young Caregivers: Development of the Maastricht Parentification Scale); Maastricht University, Faculty of Health, Medicine and Life Sciences: Maastricht, The Netherlands, 2015. [Google Scholar]
- Kellermann, N.P. Perceived parental rearing behavior in children of Holocaust survivors. Isr. J. Psychiatry Relat. Sci. 2001, 38, 58–68. [Google Scholar] [PubMed]
- Zhang, H. The relationship between triangle operation in parental quarrels and behavior problems among children of elementary school. Chin. Annu. Rep. Guid. Couns. 2000, 8, 77–110. [Google Scholar]
- Dariotis, J.K.; Sonenstein, F.L.; Gates, G.J.; Capps, R.; Astone, N.M.; Pleck, J.H.; Sifakis, F.; Zeger, S. Changes in Sexual Risk Behavior as Young Men Transition to Adulthood. Perspect. Sex. Reprod. Health 2008, 40, 218–225. [Google Scholar] [CrossRef]
- Groves, R.M. Survey Methodology; John Wiley & Sons: Hoboken, NJ, USA, 2011. [Google Scholar]
- Beck, A.T.; Steer, R.A.; Brown, G. Beck Depression Inventory–II; Psychological Corporation: San Antonio, TX, USA, 1996. [Google Scholar]
- Radloff, L.S. The CES-D scale: A self-report depression scale for research in the general population. Appl. Psychol. Meas. 1977, 1, 385–401. [Google Scholar] [CrossRef]
- Kovacs, M. Children’s Depression Inventory Manual; Multi-Health Systems, Inc.: North Tonawanda, NY, USA, 1992. [Google Scholar]
- Derogatis, L.R. Brief Symptom Inventory 18; Johns Hopkins University: Baltimore, MD, USA, 2001. [Google Scholar]
- Laurent, J.; Catanzaro, S.J.; Joiner, T.E.; Rudolph, K.D.; Potter, K.I.; Lambert, S. A measure of positive and negative affect for children: Scale development and preliminary validation. Psychol. Assess. 1999, 11, 326. [Google Scholar] [CrossRef]
- Hardt, J.; Dragan, M.; Kappis, B. A short screening instrument for mental health problems: The Symptom Checklist-27 (SCL-27) in Poland and Germany. Int. J. Psychiatry Clin. Pr. 2011, 15, 42–49. [Google Scholar] [CrossRef]
- Weinberger, D.A.; Schwartz, G.E. Distress and Restraint as Superordinate Dimensions of Self-Reported Adjustment: A Typological Perspective. J. Pers. 1990, 58, 381–417. [Google Scholar] [CrossRef] [PubMed]
- Derogatis, L.R.; Spencer, P. The Brief Symptom Inventory Manual; National Computer Systems: Minneapolis, MN, USA, 1993. [Google Scholar]
- Lovibond, P.F.; Lovibond, S.H. The structure of negative emotional states: Comparison of the Depression Anxiety Stress Scales (DASS) with the Beck Depression and Anxiety Inventories. Behav. Res. Ther. 1995, 33, 335–343. [Google Scholar] [CrossRef] [PubMed]
- Lorr, M.; McNair, D.M. The Profile of Mood States Manual 1971; Educational and Institutional Testing Service: San Francisco, CA, USA, 1973. [Google Scholar]
- Achenback, T.; Edelbrock, C. Manual for the Teacher’s Report Form and Teacher Version of the Child Behavior Profile; University of Vermont, Department of Psychiatry: Burlington, VT, USA, 1986. [Google Scholar]
- Achenbach, T.; Edelbrock, C. Manual for the Youth Self-Report. Burlington: University of Vermont; Research Center for Children, Youth & Families: Burlington, VT, USA, 1991. [Google Scholar]
- Reynolds, C.; Kamphaus, R. Manual for the Behavior Assessment System for Children; American Guidance Service: Circle Pines, MN, USA, 1992. [Google Scholar]
- Carter, A.S.; Briggs-Gowan, M.J. (University of Massachusetts Boston Department of Psychology, Yale University, Boston, MA, USA, 1993). The Infant–Toddler Social and Emotional Assessment (ITSEA). Unpublished Manual.
- Goodman, R. The Strengths and Difficulties Questionnaire: A Research Note. J. Child Psychol. Psychiatry Allied Discip. 2006, 38, 581–586. [Google Scholar] [CrossRef] [PubMed]
- Khan, R.; Cooke, D.J. Risk factors for severe inter-sibling violence: A preliminary study of a youth forensic sample. J. Interpers. Violence 2008, 23, 1513–1530. [Google Scholar] [CrossRef] [PubMed]
- Rotheram-Borus, M.J.; Rosario, M.; Van Rossem, R.; Reid, H.; Gillis, R. Prevalence, course, and predictors of multiple problem behaviors among gay and bisexual male adolescents. Dev. Psychol. 1995, 31, 75. [Google Scholar] [CrossRef]
- Babor, T.F.; Higgins-Biddle, J.C.; Saunders, J.B. The Alcohol Use Disorders Identification Test; World Health Organization: Geneva, Switzerland, 2001. [Google Scholar]
- Bush, B.; Shaw, S.; Cleary, P.; Delbanco, T.L.; Aronson, M.D. Screening for alcohol abuse using the cage questionnaire. Am. J. Med. 1987, 82, 231–235. [Google Scholar] [CrossRef]
- Graham, J.W.; Flay, B.; Johnson, C.A.; Hansen, W.B.; Grossman, L.; Sobel, J.L. Reliability of Self-Report Measures of Drug Use in Prevention Research: Evaluation of the Project Smart Questionnaire via the Test-Retest Reliability Matrix. J. Drug Educ. 1984, 14, 175–193. [Google Scholar] [CrossRef]
- Briere, J.; Runtz, M. The Trauma Symptom Checklist (TSC-33) early data on a new scale. J. Interpers. Violence 1989, 4, 151–163. [Google Scholar] [CrossRef]
- Yung, A.R.; Yuen, H.P.; Mcgorry, P.D.; Phillips, L.J.; Kelly, D.; Dell’Olio, M.; Francey, S.M.; Cosgrave, E.M.; Killackey, E.; Stanford, C.; et al. Mapping the Onset of Psychosis: The Comprehensive Assessment of At-Risk Mental States. Aust. N. Zeal. J. Psychiatry 2005, 39, 964–971. [Google Scholar] [CrossRef]
- Puig-Antich, J.; Chambers, W. The Schedule for Affective Disorders and Schizophrenia for School-Age Children (Kiddie-SADS); New York State Psychiatric Institute: New York, NY, USA, 1978. [Google Scholar]
- Rosenberg, M. Society and the Adolescent Self-Image; Princeton University Press: Princeton, NJ, USA, 1965. [Google Scholar]
- Diener, E.; Emmons, R.A.; Larsen, R.J.; Griffin, S. The satisfaction with life scale. J. Personal. Assess. 1985, 49, 71–75. [Google Scholar] [CrossRef]
- Pearlin, L.I.; Schooler, C. The structure of coping. J. Health Soc. Behav. 1978, 19, 2–21. [Google Scholar] [CrossRef] [PubMed]
- Schwarzer, R.; Jerusalem, M. Generalized self-efficacy scale. J. Weinman, S. Wright, & M. Johnston, Measures in health psychology: A user’s portfolio. Causal Control Beliefs 1995, 35, 37. [Google Scholar]
- Macfie, J.; Fitzpatrick, K.L.; Rivas, E.M.; Cox, M.J. Independent influences upon mother-toddler role reversal: Infant-mother attachment disorganization and role reversal in mother’s childhood. Attach. Hum. Dev. 2008, 10, 29–39. [Google Scholar] [CrossRef]
- Casey, B.J.; Getz, S.; Galvan, A. The adolescent brain. Dev. Rev. 2008, 28, 62–77. [Google Scholar] [CrossRef] [PubMed]
- Casey, B.; Jones, R.M. Neurobiology of the Adolescent Brain and Behavior: Implications for Substance Use Disorders. J. Am. Acad. Child Adolesc. Psychiatry 2010, 49, 1189–1201. [Google Scholar] [CrossRef]
- Kaufman, J.; Weder, N. Neurobiology of early life stress: Evolving concepts. In Pediatric Psychopharmacology: Principles and Practice; Oxford University Press: Oxford, UK, 2010; pp. 112–123. [Google Scholar]
- Hooper, L.M. Assessing Parentification in South American College Students: A Factor Analytic Study of a Spanish Version of the Parentification Inventory. J. Multicult. Couns. Dev. 2014, 42, 93–106. [Google Scholar] [CrossRef]
- Hooper, L.M.; Mugoya, G.C.; Burton, S.; Tomek, S. Psychometric evaluation of the parentification inventory–Swahili version with Kenyan adults: Factor structure, reliability, and validity. J. Multicult. Couns. Dev. 2020, 48, 58–78. [Google Scholar] [CrossRef]
- Borchet, J.; Schneider, W.S.; Lewandowska-Walter, A.; Tomek, S.; Hooper, L.M. Psychometric Evaluation of the Parentification Inventory in a Polish Adolescent Sample. Fam. J. 2022, 31, 488–497. [Google Scholar] [CrossRef]
- Alexander, C. Unequal Conditions of Care and the Implications for Social Policies on Young Carers. Child Adolesc. Soc. Work. J. 2021, 38, 505–518. [Google Scholar] [CrossRef]
- Dunn, J.; Plomin, R. Why Are Siblings So Different? The Significance of Differences in Sibling Experiences Within the Family. Fam. Process. 1991, 30, 271–283. [Google Scholar] [CrossRef] [PubMed]
- Stierman, B.; Afful, J.; Carroll, M.D.; Chen, T.C.; Davy, O.; Fink, S.; Akinbami, L.J. National Health and Nutrition Examination Survey 2017–March 2020 Prepandemic Data Files Development of Files and Prevalence Estimates for Selected Health Outcomes. In National Health Statistics Reports; NCHS: Washington, DC, USA, 2021. [Google Scholar]
- Hasson, R.; Sallis, J.F.; Coleman, N.; Kaushal, N.; Nocera, V.G.; Keith, N. COVID-19: Implications for Physical Activity, Health Disparities, and Health Equity. Am. J. Lifestyle Med. 2022, 16, 420–433. [Google Scholar] [CrossRef] [PubMed]

| Search Terms (Same in All Three Data Bases) | Articles Count | Database |
|---|---|---|
| (spousif* or parentif* or adultif* or “role reversal”) AND (outcome* or resilien* or thriv* or stress or react* or benefit* or impact* or effect* or affect* or positiv* or negativ*) | 227 | PsycInfo |
| 313 | Academic Search Complete | |
| 571 | Web of Science |
| Data Item | Definition |
|---|---|
| Study Citation Information | Full citation; separate columns for year and title |
| Population | Description of the target population (e.g., adults, young adults, children) |
| Location | Country context |
| Participants | Description of sample characteristics and sampling |
| Methods | Description of data collection procedures |
| Focus of the Study | Specify outcomes of focus (e.g., mental health, externalizing problems) |
| Type of Research | Specify study design including three categories (qualitative, quantitative, mixed methods) and other relevant details |
| Parentification Measures | Specify parentification measures used (name and scale/subscale description) |
| Parentification Constructs | Specify parentification constructs measured including instrumental, emotional, perceptions |
| Mediators, Moderators, Mechanisms | Describe any mediators, moderators, or mechanisms explored (e.g., coping, social support) |
| Analytic Approach | Description of analyses conducted |
| Key Findings | Summary of major findings reported by authors |
| Positive Outcomes | Description of positive or resilient outcomes as well as significance level and direction |
| Negative Outcomes | Description of negative or floundering outcomes as well as significance level and direction |
| Strengths | Summary of study strengths |
| Limitations | Summary of study limitations |
| Future Directions | Summary of future directions |
| Round 1 Notes | Questions or impressions about relevance |
| Round 1 Site Reviewer | Institution of reviewer |
| Round 2 Tier | Random split articles into first, second, and third tier for sequence of review |
| Round 2 Updates | Indicate whether data extraction fields were updated upon verification |
| Round 2 Notes | Specified data extraction field changes; additional questions about relevance or interpretation of outcomes |
| Round 3 Site Reviewer | Assessed study quality using MMAT; reviewers independently rated criteria; 10% were cross-validated |
| Round 3 Notes | Questions or discrepancies in criteria rating; final articles to exclude were noted; misclassification of study design was resolved and appropriate MMAT applied |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dariotis, J.K.; Chen, F.R.; Park, Y.R.; Nowak, M.K.; French, K.M.; Codamon, A.M. Parentification Vulnerability, Reactivity, Resilience, and Thriving: A Mixed Methods Systematic Literature Review. Int. J. Environ. Res. Public Health 2023, 20, 6197. https://doi.org/10.3390/ijerph20136197
Dariotis JK, Chen FR, Park YR, Nowak MK, French KM, Codamon AM. Parentification Vulnerability, Reactivity, Resilience, and Thriving: A Mixed Methods Systematic Literature Review. International Journal of Environmental Research and Public Health. 2023; 20(13):6197. https://doi.org/10.3390/ijerph20136197
Chicago/Turabian StyleDariotis, Jacinda K., Frances R. Chen, Ye Rang Park, Montana K. Nowak, Katherine M. French, and Anisa M. Codamon. 2023. "Parentification Vulnerability, Reactivity, Resilience, and Thriving: A Mixed Methods Systematic Literature Review" International Journal of Environmental Research and Public Health 20, no. 13: 6197. https://doi.org/10.3390/ijerph20136197
APA StyleDariotis, J. K., Chen, F. R., Park, Y. R., Nowak, M. K., French, K. M., & Codamon, A. M. (2023). Parentification Vulnerability, Reactivity, Resilience, and Thriving: A Mixed Methods Systematic Literature Review. International Journal of Environmental Research and Public Health, 20(13), 6197. https://doi.org/10.3390/ijerph20136197