

Potential Factors Conditioning the Compliance to Mandatory Face Covering in the Public Space Due to SARS-CoV-2 Pandemic

 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Sample
2.2. Measures
- To evaluate the general level of anxiety, the Generalized Anxiety Disorder 7-item Scale (GAD-7) was used. The GAD-7 is a useful tool for screening for generalized anxiety disorder and assessing the severity of anxiety symptoms over the past two weeks. It has been shown to produce reliable and valid scores in community studies.
- The Fear of COVID-19 was measured by FCV-19S [16,22]: FCV-19S is a brief instrument consisting of seven items, e.g., item 1, “I am most afraid of coronavirus-19”; item 5, “When watching news and stories about coronavirus-19 on social media, I become nervous or anxious.” Responders are asked to indicate their level of agreement with each of the seven statements using a five-item Likert type scale (1 = strongly disagree to 5 = strongly agree).
- The Questionnaire of Social Approval (KAS) is designed to monitor the level of social approval, understood as a personality trait and a tendency to present oneself in a falsely favorable light. The questionnaire consists of 29 statements that require the respondent to answer “true” or “false”, describing behaviors and traits with explicit social approval or disapproval.
- Vaccination, participants answer are they decided to vaccinate themselves or not.
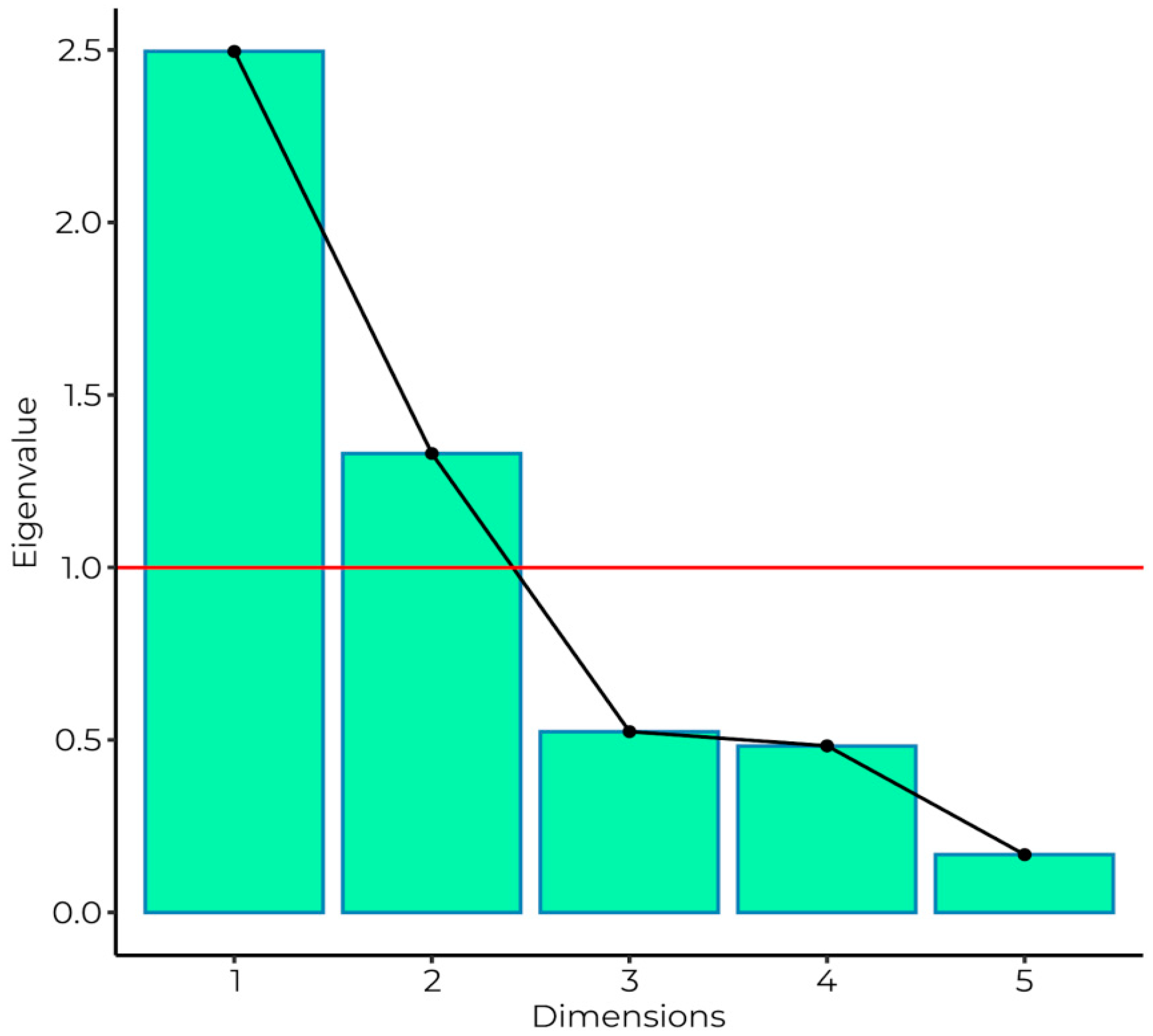
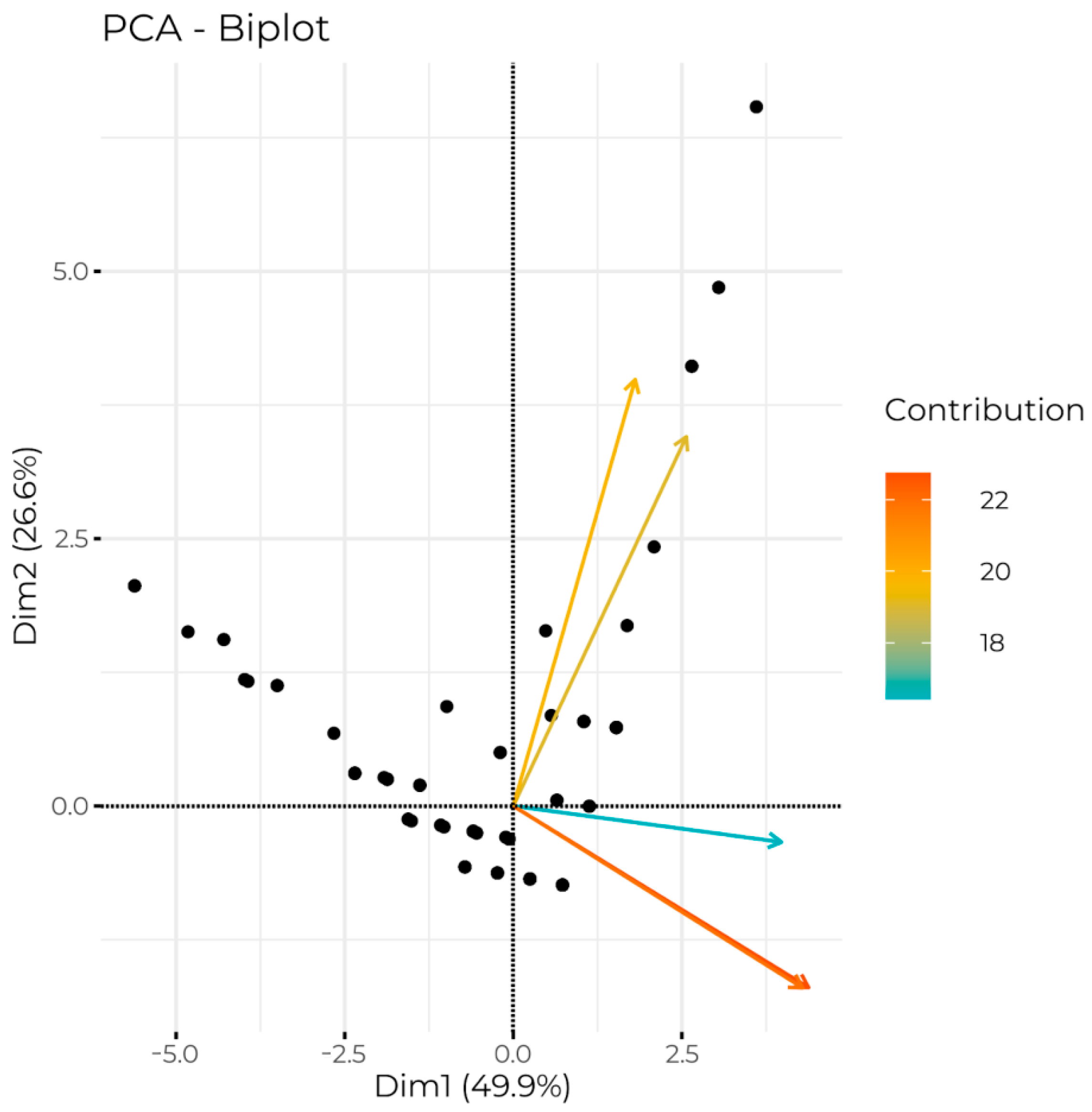
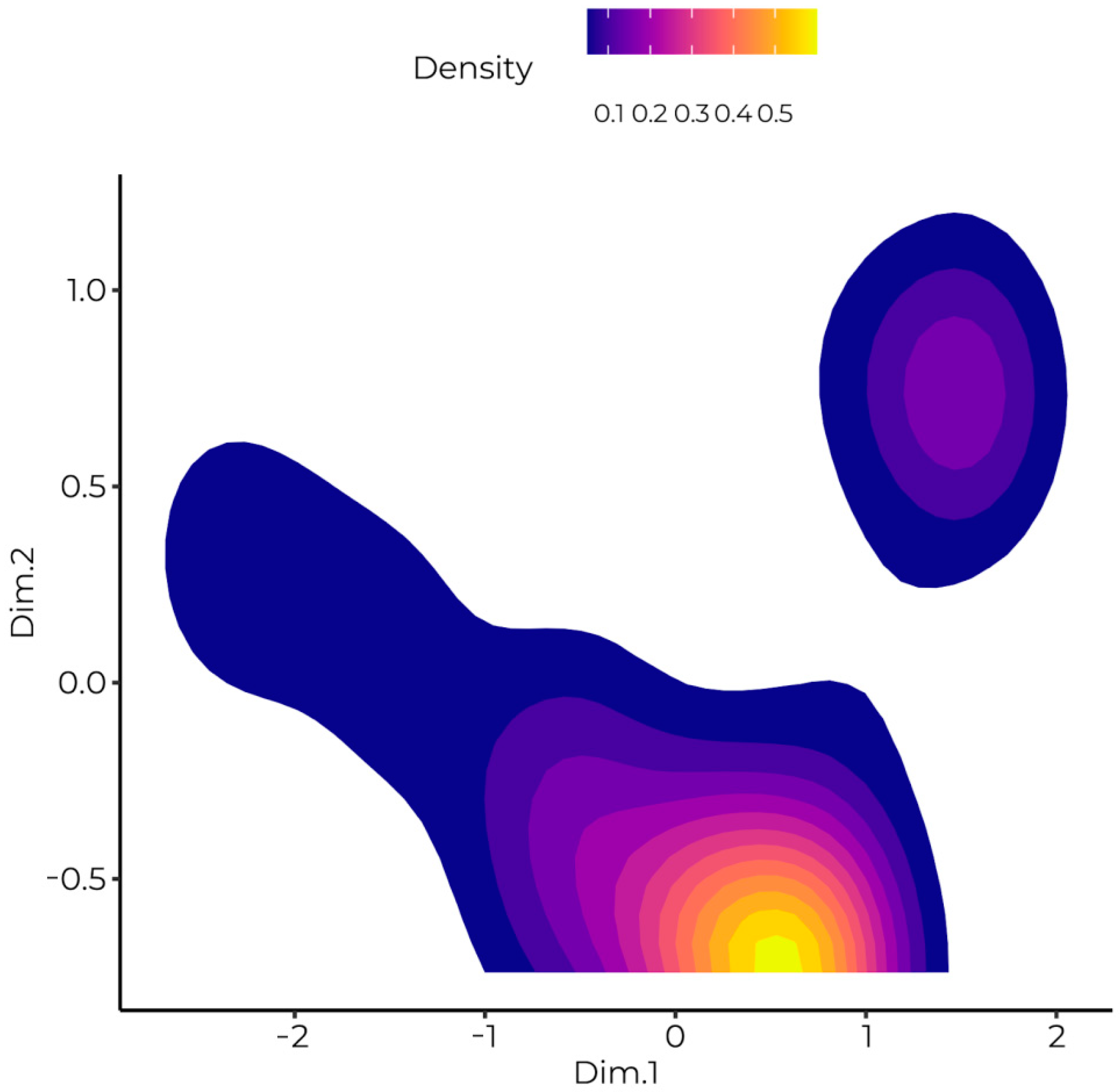
- Mask willingness is a scale designed to measure the willingness to cover the face and nose in various environments. Based on PCA outcome there was found two factors: indoor face covering and outdoor face covering.
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
6. Study Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Nerlich, B.; Jaspal, R. Social Distancing’ in Response to COVID-19 in the UK Media. Curr. Sociol. 2021, 69, 566–583. [Google Scholar] [CrossRef]
- Koh, D. COVID-19 lockdowns throughout the world. Occup. Med. 2020, 70, 322. [Google Scholar] [CrossRef]
- Wąsikowski, A. Civil rights and freedoms under the COVID-19 epidemic conditions. Zbliżenia Cywilizacyjne 2021, 17, 11–32. [Google Scholar] [CrossRef]
- Gostin, L.O.; Chertoff, M. Lockdowns, quarantines, and travel restrictions, during Covid and beyond: What’s the law, and how should we decide? Health Aff. Blog 2021, 2375, 1–8. [Google Scholar] [CrossRef]
- Talic, S.; Shah, S.; Wild, H.; Gasevic, D.; Maharaj, A.; Ademi, Z.; Li, X.; Xu, W.; Mesa-Eguiagaray, I.; Rostron, J.; et al. Effectiveness of public health measures in reducing the incidence of COVID-19, SARS-CoV-2 transmission, and COVID-19 mortality: Systematic review and meta-analysis. BMJ 2021, 375, e068302. [Google Scholar] [CrossRef] [PubMed]
- Howard, J.; Huang, A.; Li, Z.; Tufekci, Z.; Zdimal, V.; van der Westhuizen, H.M.; von Delft, A.; Price, A.; Fridman, L.; Tang, L.H.; et al. Face mask against COVID-19: An evidence review. Br. Med. J. 2020, 118, 1–8. [Google Scholar] [CrossRef]
- Setti, L.; Passarini, F.; De Gennaro, G.; Barbieri, P.; Perrone, M.G.; Borelli, M.; Palmisani, J.; Di Gilio, A.; Piscitelli, P.; Miani, A. Airborne Transmission Route of COVID-19: Why 2 Meters/6 Feet of Inter-Personal Distance Could Not Be Enough. Int. J. Environ. Res. Public Health 2020, 17, 2932. [Google Scholar] [CrossRef] [PubMed]
- Polska Agencja Prasowa. Available online: https://www.pap.pl/aktualnosci/news%2C751336%2Cprof-gut-w-rozmowie-z-pap-brak-maseczki-znacznie-zwieksza-ryzyko-zakazenia (accessed on 30 October 2022).
- Business Insider. Available online: https://www.businessinsider.com/who-no-need-for-healthy-people-to-wear-face-masks-2020-4 (accessed on 27 August 2020).
- Jefferson, T.; Jones, M.A.; Al-Ansary, L.; Bawazeer, G.A.; Beller, E.M.; Clark, J.; Conly, J.M.; Del Mar, C.; Doodley, E.; Ferroni, E.; et al. Physical interventions to interrupt or reduce the spread of respiratory viruses. Part 1-Face masks, eye protection and person distancing: Systematic review and meta-analysis. MedRxiv 2020, 1–50, preprint. [Google Scholar] [CrossRef]
- Rzeczpospolita. Available online: https://www.rp.pl/spoleczenstwo/art19084191-sondaz-ogolnokrajowy-lockdown-popiera-1-5-proc-polakow-ale-lokalne-juz-ponad-42-proc (accessed on 10 November 2022).
- Gazeta Wyborcza. Available online: https://wyborcza.pl/7,75398,27829243,sondaz-wyborczej-wiekszosc-polakow-za-obostrzeniami-dla-niezaszczepionych.html (accessed on 11 November 2022).
- ARC Rynek i Opinia. Available online: https://arc.com.pl/polacy-niezdecydowani-w-kwestii-szczepienia-na-COVID-19/ (accessed on 11 November 2022).
- Salari, N.; Hosseinian-Far, A.; Jalali, R.; Vaisi-Raygani, A.; Rasoulpoor, S.; Mohammadi, M.; Rasoulpoor, S.; Khaledi-Paveh, B. Prevalence of stress, anxiety, depression among the general population during the COVID-19 pandemic: A systematic review and meta-analysis. Glob. Health 2020, 16, 57. [Google Scholar] [CrossRef]
- Menzies, R.E.; Menzies, R.G. Death anxiety in the time of COVID-19: Theoretical explanations and clinical implications. Cogn. Behav. Ther. 2020, 13, 1–24. [Google Scholar] [CrossRef] [PubMed]
- Ahorsu, D.K.; Lin, C.Y.; Imani, V.; Saffari, M.; Griffiths, M.D.; Pakpour, A.H. The Fear of COVID-19 Scale: Development and Initial Validation. Int. J. Ment. Health Addict. 2020, 20, 1537–1545. [Google Scholar] [CrossRef]
- Haktanir, A.; Seki, T.; Dilmaç, B. Adaptation and evaluation of Turkish version of the fear of COVID-19 Scale. Death Stud. 2020, 46, 719–727. [Google Scholar] [CrossRef]
- Satici, B.; Gocet-Tekin, E.; Deniz, M.E.; Satici, S.A. Adaptation of the Fear of COVID-19 Scale: Its Association with Psychological Distress and Life Satisfaction in Turkey. Int. J. Ment. Health Addict. 2021, 19, 1980–1988. [Google Scholar] [CrossRef]
- Soraci, P.; Ferrari, A.; Abbiati, F.A.; Del Fante, E.; De Pace, R.; Urso, A.; Griffiths, M.D. Validation and Psychometric Evaluation of the Italian Version of the Fear of COVID-19 Scale. Int. J. Ment. Health Addict. 2020, 58, 496–503. [Google Scholar] [CrossRef] [PubMed]
- Bitan, D.; Grossman-Giron, A.; Bloch, Y.; Mayer, Y.; Shiffman, N.; Mendlovic, S. Fear of COVID-19 scale: Psychometric characteristics, reliability and validity in the Israeli population. Psychiatry Res. 2020, 289, 113100. [Google Scholar] [CrossRef]
- Alyami, M.; Henning, M.; Krägeloh, C.U.; Alyami, H. Psychometric Evaluation of the Arabic Version of the Fear of COVID-19 Scale. Int. J. Ment. Health Addict. 2020, 19, 2219–2232. [Google Scholar] [CrossRef] [PubMed]
- Tsipropoulou, V.; Nikopoulou, V.A.; Holeva, V.; Nasika, Z.; Diakogiannis, I.; Sakka, S.; Kostikidou, S.; Varvara, C.; Spyridopoulou, E.; Parlapani, E. Psychometric Properties of the Greek Version of FCV-19S. Int. J. Ment. Health Addict. 2021, 19, 2279–2288. [Google Scholar] [CrossRef]
- Perz, C.A.; Lang, B.A.; Harrington, R. Validation of the Fear of COVID-19 Scale in a US College Sample. Int. J. Ment. Health Addict. 2020, 20, 273–283. [Google Scholar] [CrossRef]
- Masuyama, A.; Shinkawa, H.; Kubo, T. Validation and Psychometric Properties of the Japanese Version of the Fear of COVID-19 Scale Among Adolescents. Int. J. Ment. Health Addict. 2020, 20, 387–397. [Google Scholar] [CrossRef] [PubMed]
- Huarcaya-Victoria, J.; Villarreal-Zegarra, D.; Podestà, A.; Luna-Cuadros, M.A. Psychometric properties of a Spanish version of the fear of COVID-19 scale in general population of Lima, Peru. Int. J. Ment. Health Addict. 2020, 20, 249–262. [Google Scholar] [CrossRef] [PubMed]
- R Core Team. R: A Language and Environment for Statistical Computing. R Foundation for Statistical Computing; R Core Team: Vienna, Austria, 2021; Available online: https://www.R-project.org (accessed on 11 November 2022).
- The Jamovi Project. Jamovi, Version 1.6; Jamovi Project: Sydney, Australia, 2021; Available online: https://www.jamovi.org (accessed on 11 November 2022).
- Wickham, H.; Hester, J.; Bryan, J. Readr: Read Rectangular Text Data, R Package Version 2.1.2; Jamovi Project: Sydney, Australia, 2021; Available online: https://CRAN.R-project.org/package=readr (accessed on 11 November 2022).
- Kassambara, A. Rstatix: Pipe-Friendly Framework for Basic Statistical Tests, R Package Version 0.7.0; Jamovi Project: Sydney, Australia, 2021; Available online: https://CRAN.R-project.org/package=rstatix (accessed on 11 November 2022).
- Revelle, W. Psych: Procedures for Personality and Psychological Research, Version 2.2.5; Northwestern University: Evanston, IL, USA, 2022; Available online: https://CRAN.R-project.org/package=psych (accessed on 11 November 2022).
- Le, S.; Josse, J.; Husson, F. FactoMineR: An R Package for Multivariate Analysis. J. Stat. Softw. 2008, 25, 1–18. [Google Scholar] [CrossRef]
- Kassambara, A.; Mundt, F. factoextra: Extract and Visualize the Results of Multivariate Data Analyses, R Package Version 1.0.7; Jamovi Project: Sydney, Australia, 2020; Available online: https://CRAN.R-project.org/package=factoextra (accessed on 11 November 2022).
- Kassambara, A. Ggpubr: ‘ggplot2’ Based Publication Ready Plots, R Package Version 0.4.0; Jamovi Project: Sydney, Australia, 2020; Available online: https://CRAN.R-project.org/package=ggpubr (accessed on 11 November 2022).
- Wickham, H. Data Analysis. In ggplot2. Use R! Springer: New York, NY, USA, 2016; pp. 1–13. Available online: https://doi.org/10.1007/978-3-319-24277-4_9 (accessed on 11 November 2022).
- Schloerke, B.; Cook, D.; Larmarange, J.; Briatte, F.; Marbach, M.; Thoen, E.; Elberg, A.; Crowley, J. GGally: Extension to ‘ggplot2’, R Package Version 2.1.2; Jamovi Project: Sydney, Australia, 2021; Available online: https://CRAN.R-project.org/package=GGally (accessed on 11 November 2022).
- McElfish, P.A.; Willis, D.E.; Shah, S.K.; Bryant-Moore, K.; Rojo, M.O.; Selig, J.P. Sociodemographic Determinants of COVID-19 Vaccine Hesitancy, Fear of Infection, and Protection Self-Efficacy. J. Prim. Care Community Health 2021, 12, 21501327211040746. [Google Scholar] [CrossRef] [PubMed]
- Pakpour, A.H.; Griffiths, M.D. The fear of COVID-19 and its role in preventive behaviors. J. Concurr. Disord. 2020, 2, 58–63. [Google Scholar]
- Jørgensen, F.; Bor, A.; Petersen, M.B. Compliance without fear: Individual-level protective behaviour during the first wave of the COVID-19 pandemic. Br. J. Health Psychol. 2021, 26, 679–696. [Google Scholar] [CrossRef]
- Krings, V.C.; Steeden, B.; Abrams, D.; Hogg, M.A. Social attitudes and behavior in the COVID-19 pandemic: Evidence and prospects from research on group processes and intergroup relations. Group Process. Intergroup Relat. 2021, 24, 195–200. [Google Scholar] [CrossRef]
- Klein, W.M.P.; Zajac, L.E.; Monin, M.M. Worry as a moderator of the association between risk perceptions and quitting intentions in young adult and adult smokers. Ann. Behav. Med. 2009, 38, 256–261. [Google Scholar] [CrossRef]
- Jin, Y. The effects of public’s cognitive appraisal of emotions in crises on crisis coping and strategy assessment. Public Relat. Rev. 2009, 35, 310–313. [Google Scholar] [CrossRef]
- Ferrer, R.A.; Klein, W.M. Risk perceptions and health behavior. Curr. Opin. Psychol. 2015, 5, 85–89. [Google Scholar] [CrossRef]
- Bendau, A.; Plag, J.; Petzold, M.B.; Ströhle, A. COVID-19 vaccine hesitancy and related fears and anxiety. Int. Immunopharmacol. 2021, 97, 107724. [Google Scholar] [CrossRef]
- Chu, H.; Liu, S. Integrating health behavior theories to predict American’s intention to receive a COVID-19 vaccine. Patient Educ. Couns. 2021, 104, 1878–1886. [Google Scholar] [CrossRef]
- Szmyd, B.; Bartoszek, A.; Karuga, F.F.; Staniecka, K.; Błaszczyk, M.; Radek, M. Medical students and SARS-CoV-2 vaccination: Attitude and behaviors. Vaccines 2021, 9, 128. [Google Scholar] [CrossRef] [PubMed]
- Szmyd, B.; Karuga, F.F.; Bartoszek, A.; Staniecka, K.; Siwecka, N.; Bartoszek, A.; Błaszczyk, M.; Radek, M. Attitude and behaviors towards SARS-CoV-2 vaccination among healthcare workers: A cross-sectional study from Poland. Vaccines 2021, 9, 218. [Google Scholar] [CrossRef] [PubMed]
- Fisher, K.A.; Bloomstone, S.J.; Walder, J.; Crawford, S.; Fouayzi, H.; Mazor, K.M. Attitudes Toward a Potential SARS-CoV-2 Vaccine. Ann. Intern. Med. 2020, 173, 964–973. [Google Scholar] [CrossRef]
- Seddig, D.; Maskileyson, D.; Davidov, E.; Ajzen, I.; Schmidt, P. Correlates of COVID-19 vaccination intentions: Attitudes, institutional trust, fear, conspiracy beliefs, and vaccine skepticism. Soc. Sci. Med. 2022, 302, 114981. [Google Scholar] [CrossRef] [PubMed]
- Snook, D.W.; Kaczkowski, W.; Fodeman, A.D. Mask On, Mask Off: Risk Perceptions for COVID-19 and Compliance with COVID-19 Safety Measures. Behav. Med. 2022, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Kahan, D.M.; Braman, D.; Gastil, J.; Slovic, P.; Mertz, C. Culture and identity-protective cognition: Explaining the white male effect in risk perception. J. Empir. Leg. Stud. 2007, 4, 465–505. [Google Scholar] [CrossRef]
- Ma, H.; Miller, C.H. The effects of agency assignment and reference point on responses to COVID-19 messages. Health Commun. 2021, 36, 59–73. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Scale | Average Pearson’s Correlation | Alpha | Omega |
|---|---|---|---|
| FCV-19S | 0.52 | 0.87 (0.85–0.89) | 0.88 (0.83–0.97) |
| GAD-7 | 0.62 | 0.92 (0.90–0.93) | 0.92 (0.91–0.98) |
| KAS | 0.09 | 0.75 (0.70–0.79) | 0.79 (0.75–0.98) |
| Mask | 0.35 | 0.72 (0.66–0.77) | 0.92 (0.87–1.00) |
| F1 | 0.65 | 0.81 (0.76–0.84) | 0.86 (0.81–0.91) |
| F2 | 0.48 | 0.56 (0.44–0.65) | 0.83 (0.65–1.00) |
| Wearing a Mas | Dimension 1 (Closed Places) | Dimension 2 (Open Places) |
|---|---|---|
| Shop/commercial | 0.87 | −0.34 |
| Restaurants | 0.79 | −0.07 |
| Public transport | 0.85 | −0.34 |
| Park/playground | 0.51 | 0.69 |
| Forest | 0.36 | 0.79 |
| Variable | M | SD | Me | MAD | Min | Max | Skew. | Kurt. | W | p |
|---|---|---|---|---|---|---|---|---|---|---|
| Age | 22.77 | 6.81 | 21.00 | 2.97 | 14.00 | 60.00 | 2.93 | 9.81 | 0.66 | <0.001 |
| Mask | 12.95 | 2.57 | 13.00 | 1.48 | 5.00 | 20.00 | −0.72 | 1.51 | 0.93 | <0.001 |
| Anxiety COVID-19 | 13.65 | 5.54 | 13.00 | 5.93 | 7.00 | 34.00 | 0.83 | 0.34 | 0.93 | <0.001 |
| Anxiety generalised | 6.54 | 5.24 | 5.00 | 4.45 | 0.00 | 21.00 | 0.95 | 0.33 | 0.91 | <0.001 |
| KAS | 16.66 | 2.77 | 17.00 | 2.97 | 9.00 | 23.00 | −0.08 | −0.35 | 0.99 | 0.007 |
| F1 indoor | 0.00 | 1.58 | 0.25 | 0.72 | −5.62 | 3.60 | −1.46 | 2.97 | 0.86 | <0.001 |
| F2 outdoor | 0.00 | 1.16 | −0.63 | 0.17 | −0.74 | 6.54 | 2.81 | 10.16 | 0.66 | <0.001 |
| Dependent Variable | Group | t | p | Cohen’s d | Magnitude | |
|---|---|---|---|---|---|---|
| Not Vaccinated (n = 68) | Vaccinated (n = 194) | |||||
| AC | 11.38 ± 4.88 | 14.44 ± 5.55 | −4.04 | <0.001 | −0.57 | moderate |
| GA | 5.40 ± 4.84 | 6.94 ± 5.32 | −2.11 | 0.036 | −0.30 | small |
| SA | 17.00 ± 3.09 | 16.54 ± 2.65 | 1.17 | 0.241 | 0.16 | negligible |
| M | −0.81 ± 1.95 | 0.29 ± 1.33 | −4.32 | 0.001 | −0.66 | moderate |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Józefacka, N.M.; Karpiński, E.A.; Superson, B.; Kołek, M.F.; Skrzypczak, A.R.; Kania, G. Potential Factors Conditioning the Compliance to Mandatory Face Covering in the Public Space Due to SARS-CoV-2 Pandemic. Int. J. Environ. Res. Public Health 2023, 20, 726. https://doi.org/10.3390/ijerph20010726
Józefacka NM, Karpiński EA, Superson B, Kołek MF, Skrzypczak AR, Kania G. Potential Factors Conditioning the Compliance to Mandatory Face Covering in the Public Space Due to SARS-CoV-2 Pandemic. International Journal of Environmental Research and Public Health. 2023; 20(1):726. https://doi.org/10.3390/ijerph20010726
Chicago/Turabian StyleJózefacka, Natalia Maja, Emil Andrzej Karpiński, Barbara Superson, Mateusz Franciszek Kołek, Andrzej Robert Skrzypczak, and Gabriela Kania. 2023. "Potential Factors Conditioning the Compliance to Mandatory Face Covering in the Public Space Due to SARS-CoV-2 Pandemic" International Journal of Environmental Research and Public Health 20, no. 1: 726. https://doi.org/10.3390/ijerph20010726
APA StyleJózefacka, N. M., Karpiński, E. A., Superson, B., Kołek, M. F., Skrzypczak, A. R., & Kania, G. (2023). Potential Factors Conditioning the Compliance to Mandatory Face Covering in the Public Space Due to SARS-CoV-2 Pandemic. International Journal of Environmental Research and Public Health, 20(1), 726. https://doi.org/10.3390/ijerph20010726