
Usefulness of Ultrasound Examination in the Assessment of the Nail Apparatus in Psoriasis



Abstract
:1. Introduction
2. Methods
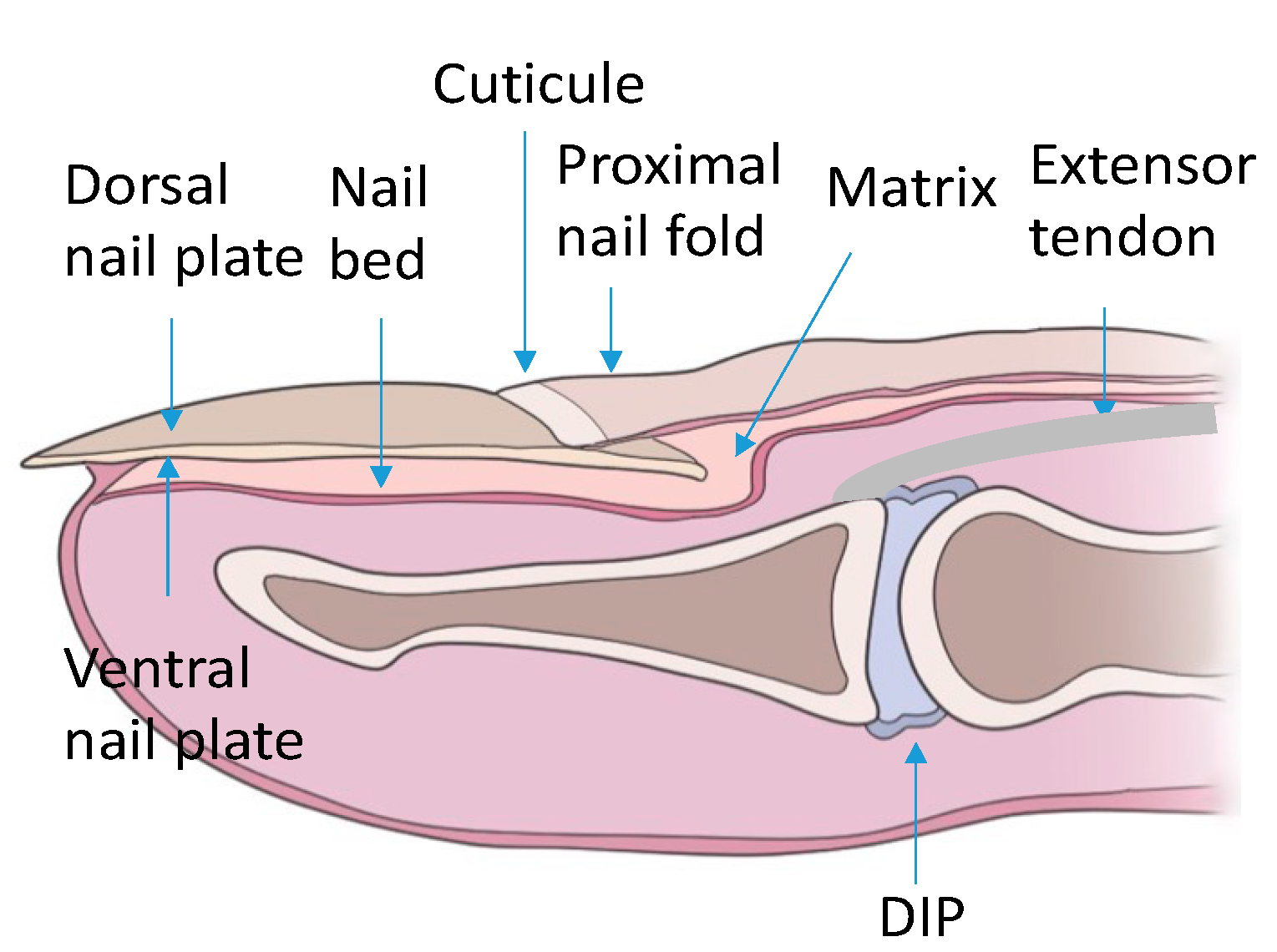
3. The Structure of the Nail Apparatus
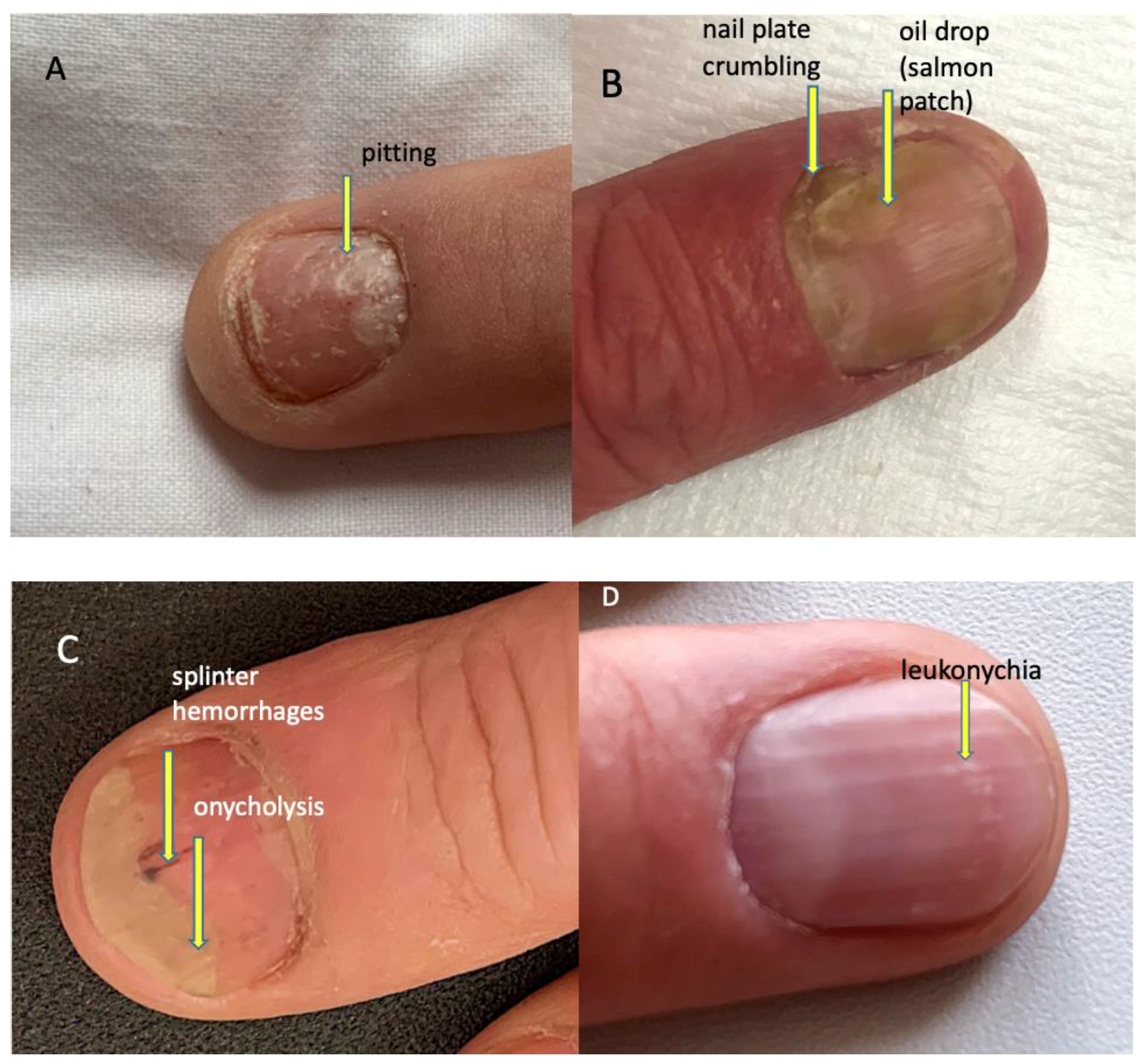
4. Psoriatic Nail Changes
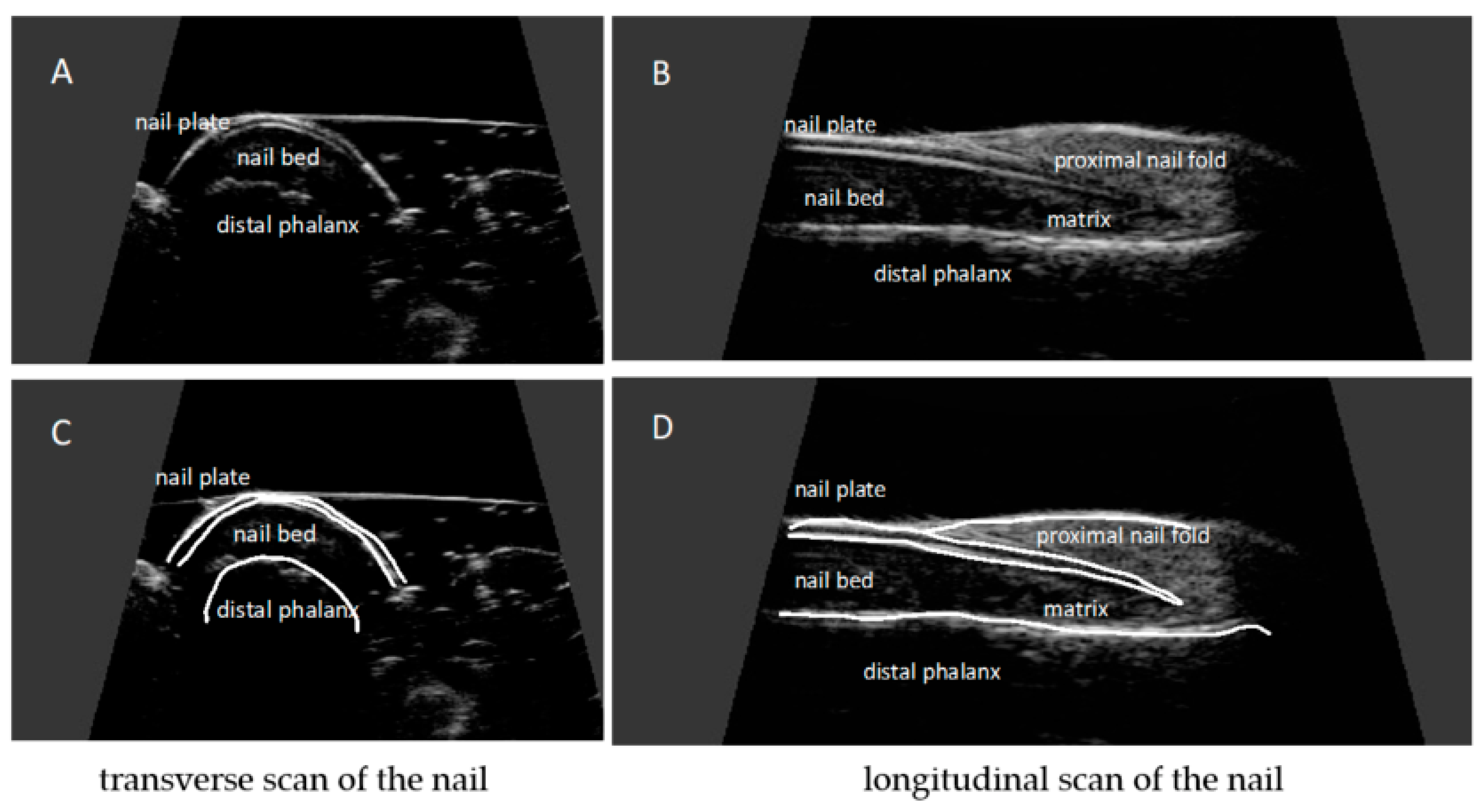
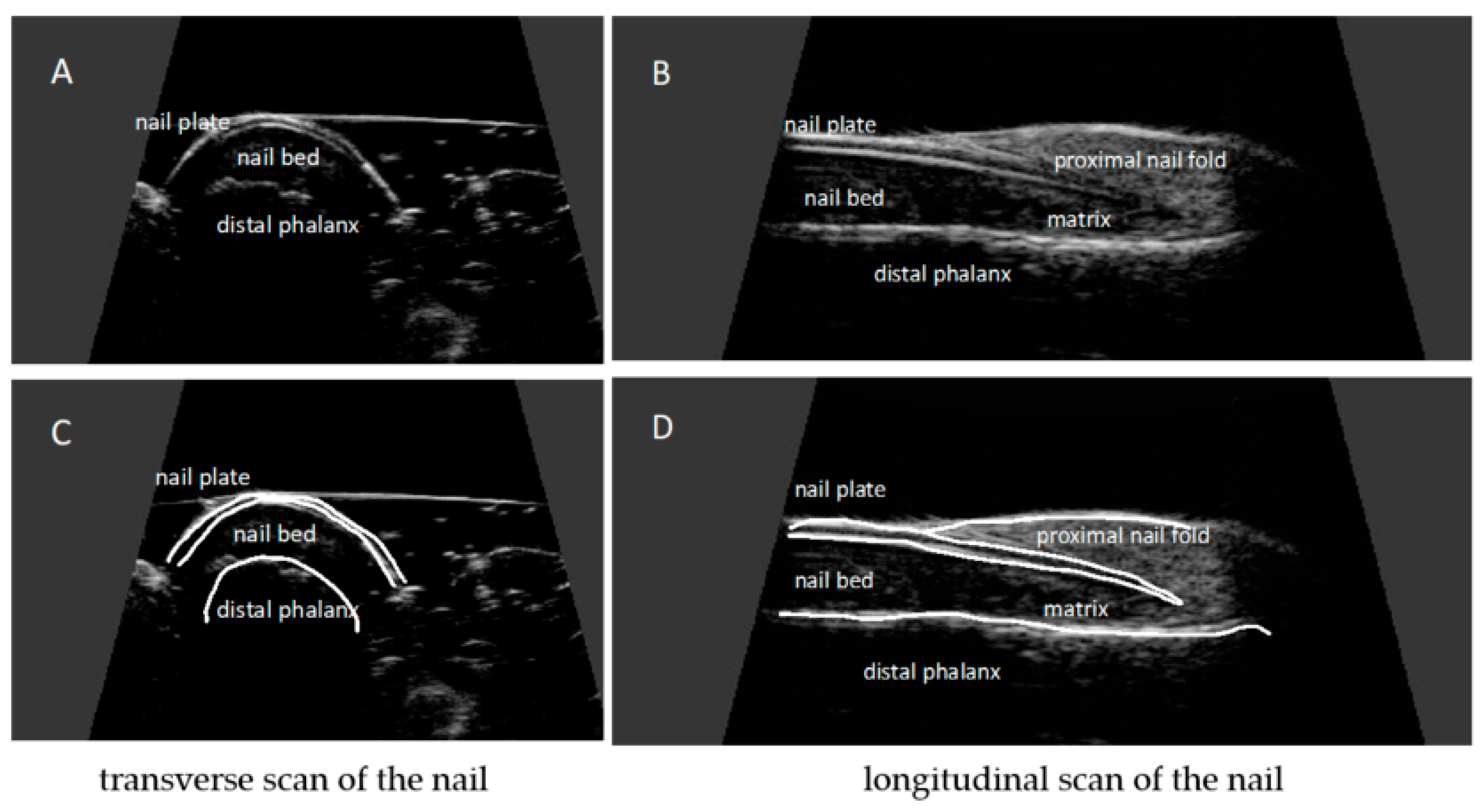
5. Ultrasonographic Image of the Nail Apparatus
6. Examination Technique
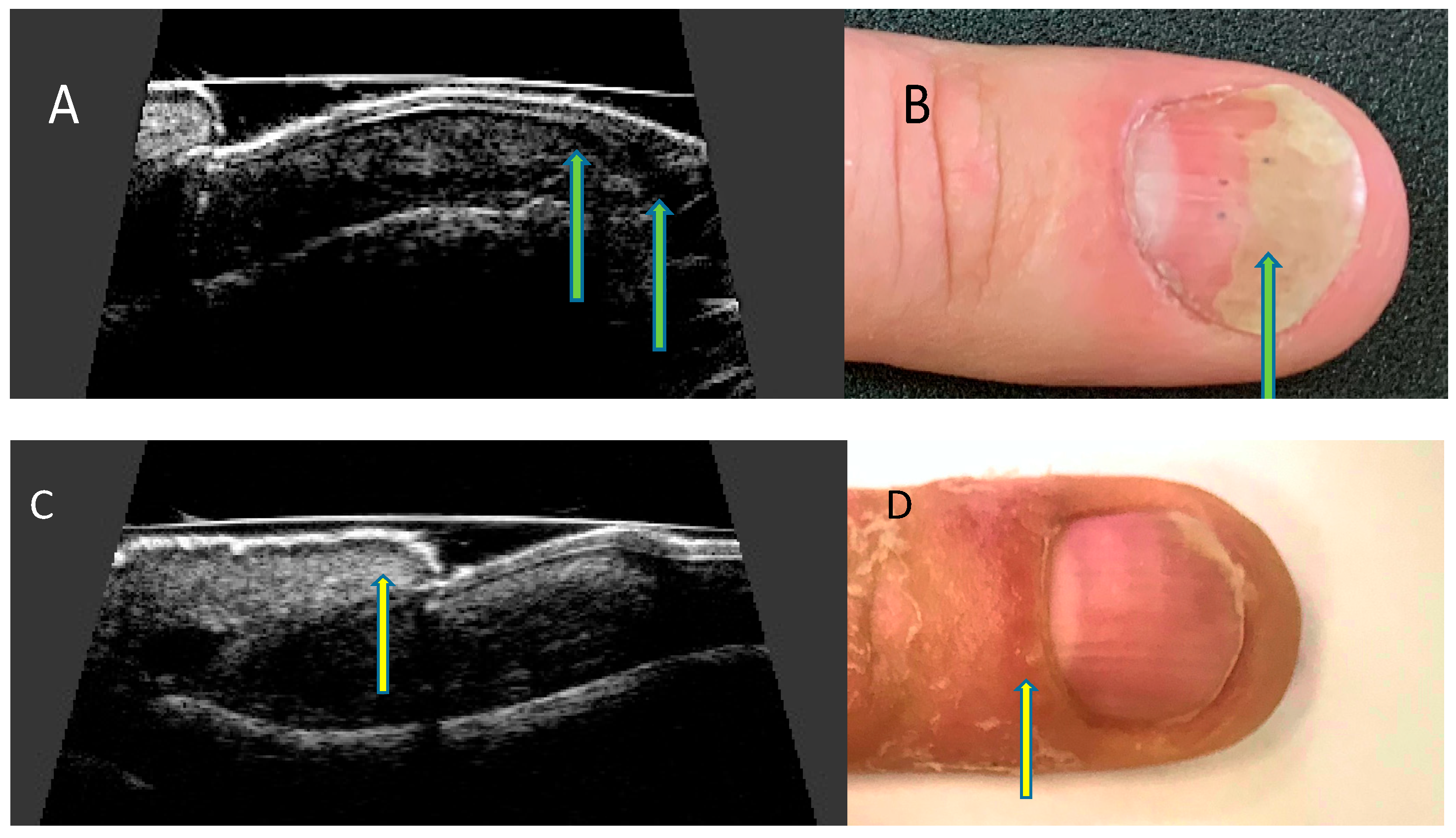
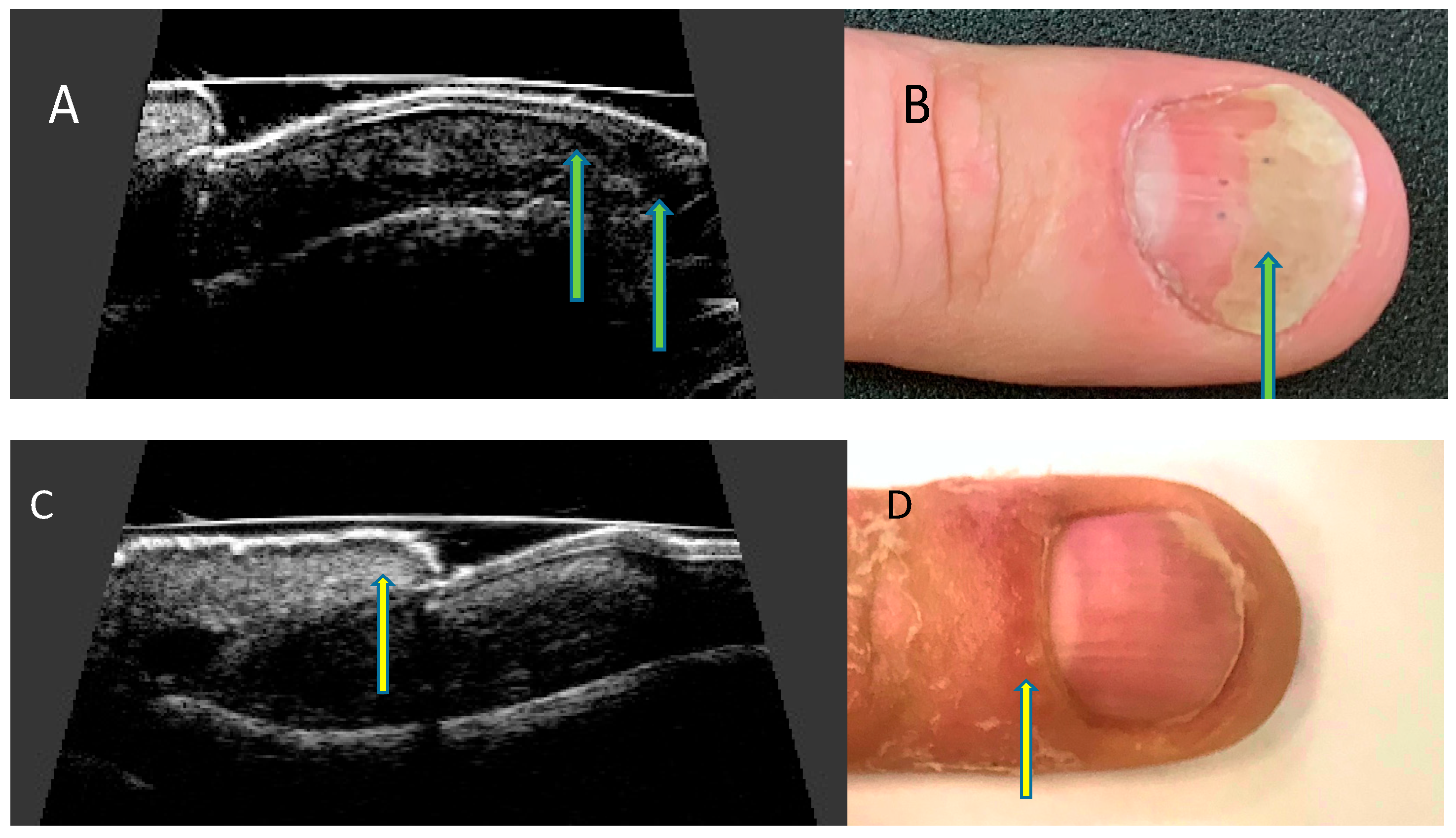
7. Ultrasonographic Changes of the Nail Apparatus in Psoriasis and Psoriatic Arthritis
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Wilson, F.C.; Icen, M.; Crowson, C.S.; McEvoy, M.T.; Gabriel, S.E.; Kremers, H.M. Incidence and clinical predictors of psoriatic arthritis in patients with psoriasis: A population-based study. Arthritis Rheum. 2009, 61, 233–239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Williamson, L.; Dalbeth, N.; Dockerty, J.L.; Gee, B.C.; Weatherall, R.; Wordsworth, B.P. Extended report: Nail disease in psoriatic arthritis--clinically important, potentially treatable and often overlooked. Rheumatology 2004, 43, 790–794. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McGonagle, D. Enthesitis: An autoinflammatory lesion linking nail and joint involvement in psoriatic disease. J. Eur. Acad. Dermatol. Venereol. 2009, 23 (Suppl. 1), 9–13. [Google Scholar] [CrossRef]
- McGonagle, D.; Tan, A.L.; Benjamin, M. The nail as a musculoskeletal appendage--implications for an improved understanding of the link between psoriasis and arthritis. Dermatology 2009, 218, 97–102. [Google Scholar] [CrossRef]
- Aydin, S.Z.; Ash, Z.R.; Tinazzi, I.; Castillo-Gallego, C.; Kwok, C.; Wilson, C.; Goodfield, M.; Gisondi, P.; Tan, A.L.; Marzo-Ortega, H.; et al. The link between enthesitis and arthritis in psoriatic arthritis: A switch to a vascular phenotype at insertions may play a role in arthritis development. Ann. Rheum. Dis. 2013, 72, 992–995. [Google Scholar] [CrossRef]
- Benjamin, M.; McGonagle, D. The enthesis organ concept and its relevance to the spondyloarthropathies. Adv. Exp. Med. Biol. 2009, 649, 57–70. [Google Scholar] [CrossRef]
- Rich, P.; Scher, R.K. Nail Psoriasis Severity Index: A useful tool for evaluation of nail psoriasis. J. Am. Acad. Dermatol. 2003, 49, 206–212. [Google Scholar] [CrossRef]
- Cassell, S.E.; Bieber, J.D.; Rich, P.; Tutuncu, Z.N.; Lee, S.J.; Kalunian, K.C.; Wu, C.W.; Kavanaugh, A. The modified Nail Psoriasis Severity Index: Validation of an instrument to assess psoriatic nail involvement in patients with psoriatic arthritis. J. Rheumatol. 2007, 34, 123–129. [Google Scholar]
- Bandinelli, F.; Prignano, F.; Bonciani, D.; Bartoli, F.; Collaku, L.; Candelieri, A.; Lotti, T.; Matucci-Cerinic, M. Ultrasound detects occult entheseal involvement in early psoriatic arthritis independently of clinical features and psoriasis severity. Clin. Exp. Rheumatol. 2013, 31, 219–224. [Google Scholar]
- Soscia, E.; Scarpa, R.; Cimmino, M.A.; Atteno, M.; Peluso, R.; Sirignano, C.; Costa, L.; Iervolino, S.; Caso, F.; Del Puente, A.; et al. Magnetic resonance imaging of nail unit in psoriatic arthritis. J. Rheumatol. Suppl. 2009, 83, 42–45. [Google Scholar] [CrossRef]
- Berritto, D.; Iacobellis, F.; Rossi, C.; Reginelli, A.; Cappabianca, S.; Grassi, R. Ultra high-frequency ultrasound: New capabilities for nail anatomy exploration. J. Dermatol. 2017, 44, 43–46. [Google Scholar] [CrossRef] [PubMed]
- Szymoniak-Lipska, M.; Polańska, A.; Jenerowicz, D.; Lipski, A.; Żaba, R.; Adamski, Z.; Dańczak-Pazdrowska, A. High-Frequency Ultrasonography and Evaporimetry in Non-invasive Evaluation of the Nail Unit. Front. Med. 2021, 8, 686470. [Google Scholar] [CrossRef] [PubMed]
- Krajewska-Włodarczyk, M.; Owczarczyk-Saczonek, A.; Placek, W.; Wojtkiewicz, M.; Wiktorowicz, A.; Wojtkiewicz, J. Ultrasound Assessment of Changes in Nails in Psoriasis and Psoriatic Arthritis. BioMed Res. Int. 2018, 2018, 8251097. [Google Scholar] [CrossRef] [PubMed]
- Perrin, C. Nail Anatomy, Nail Psoriasis, and Nail Extensor Enthesitis Theory: What Is the Link? Am. J. Dermatopathol. 2019, 41, 399–409. [Google Scholar] [CrossRef]
- de Berker, D. Nail anatomy. Clin. Dermatol. 2013, 31, 509–515. [Google Scholar] [CrossRef]
- Ji, C.; Wang, H.; Bao, C.; Zhang, L.; Ruan, S.; Zhang, J.; Gong, T.; Cheng, B. Challenge of Nail Psoriasis: An Update Review. Clin. Rev. Allergy Immunol. 2021, 61, 377–402. [Google Scholar] [CrossRef]
- Cecchini, A.; Montella, A.; Ena, P.; Meloni, G.B.; Mazzarello, V. Ultrasound anatomy of normal nails unit with 18 mHz linear transducer. Ital. J. Anat. Embryol. 2009, 114, 137–144. [Google Scholar]
- Wortsman, X.; Gutierrez, M.; Saavedra, T.; Honeyman, J. The role of ultrasound in rheumatic skin and nail lesions: A multi-specialist approach. Clin. Rheumatol. 2011, 30, 739–748. [Google Scholar] [CrossRef]
- Wakefield, R.J.; Balint, P.V.; Szkudlarek, M.; Filippucci, E.; Backhaus, M.; D’Agostino, M.A.; Sanchez, E.N.; Iagnocco, A.; Schmidt, W.A.; Bruyn, G.A.; et al. Musculoskeletal ultrasound including definitions for ultrasonographic pathology. J. Rheumatol. 2005, 32, 2485–2487. [Google Scholar]
- Cunha, J.S.; Qureshi, A.A.; Reginato, A.M. Nail Enthesis Ultrasound in Psoriasis and Psoriatic Arthritis: A Report from the 2016 GRAPPA Annual Meeting. J. Rheumatol. 2017, 44, 688–690. [Google Scholar] [CrossRef]
- Gutierrez, M.; Filippucci, E.; De Angelis, R.; Filosa, G.; Kane, D.; Grassi, W. A sonographic spectrum of psoriatic arthritis: “The five targets”. Clin. Rheumatol. 2010, 29, 133–142. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krajewska-Włodarczyk, M.; Owczarczyk-Saczonek, A.; Placek, W.; Wojtkiewicz, M.; Wiktorowicz, A.; Wojtkiewicz, J. Distal interphalangeal joint extensor tendon enthesopathy in patients with nail psoriasis. Sci. Rep. 2019, 9, 3628. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gisondi, P.; Idolazzi, L.; Girolomoni, G. Ultrasonography reveals nail thickening in patients with chronic plaque psoriasis. Arch. Dermatol. Res. 2012, 304, 727–732. [Google Scholar] [CrossRef] [PubMed]
- Aydin, S.Z.; Castillo-Gallego, C.; Ash, Z.R.; Marzo-Ortega, H.; Emery, P.; Wakefield, R.J.; Wittmann, M.; McGonagle, D. Ultrasonographic assessment of nail in psoriatic disease shows a link between onychopathy and distal interphalangeal joint extensor tendon enthesopathy. Dermatology 2012, 225, 231–235. [Google Scholar] [CrossRef]
- Idolazzi, L.; Zabotti, A.; Fassio, A.; Errichetti, E.; Benini, C.; Vantaggiato, E.; Rossini, M.; De Vita, S.; Viapiana, O. The ultrasonographic study of the nail reveals differences in patients affected by inflammatory and degenerative conditions. Clin. Rheumatol. 2019, 38, 913–920. [Google Scholar] [CrossRef]
- Ally Essayed, S.M.; Al-Shatouri, M.A.; Nasr Allah, Y.S.; Atwa, M.A. Ultrasonographic characterization of the nails in patients with psoriasis and onychomycosis. Egypt. J. Radiol. Nucl. Med. 2015, 46, 733–739. [Google Scholar] [CrossRef] [Green Version]
- Sandobal, C.; Carbó, E.; Iribas, J.; Roverano, S.; Paira, S. Ultrasound nail imaging on patients with psoriasis and psoriatic arthritis compared with rheumatoid arthritis and control subjects. J. Clin. Rheumatol. 2014, 20, 21–24. [Google Scholar] [CrossRef]
- Scarpa, R.; Soscia, E.; Peluso, R.; Atteno, M.; Manguso, F.; Del Puente, A.; Spanò, A.; Sirignano, C.; Oriente, A.; Di Minno, M.N.; et al. Nail and distal interphalangeal joint in psoriatic arthritis. J. Rheumatol. 2006, 33, 1315–1319. [Google Scholar]
- Acosta-Felquer, M.L.; Ruta, S.; Rosa, J.; Marin, J.; Ferreyra-Garrot, L.; Galimberti, M.L.; Galimberti, R.; Garcia-Monaco, R.; Soriano, E.R. Ultrasound entheseal abnormalities at the distal interphalangeal joints and clinical nail involvement in patients with psoriasis and psoriatic arthritis, supporting the nail-enthesitis theory. Semin. Arthritis Rheum. 2017, 47, 338–342. [Google Scholar] [CrossRef]
- Moya Alvarado, P.; Roé Crespo, E.; Muñoz-Garza, F.Z.; López-Ferrer, A.; Laiz Alonso, A.; Vilarrassa Rull, E.; Casademont I Pou, J.; Puig Sanz, L. Subclinical enthesopathy of extensor digitorum tendon is highly prevalent and associated with clinical and ultrasound alterations of the adjacent fingernails in patients with psoriatic disease. J. Eur. Acad. Dermatol. Venereol. 2018, 32, 1728–1736. [Google Scholar] [CrossRef]
- Sarma, N. Evidence and Suggested Therapeutic Approach in Psoriasis of Difficult-to-treat Areas: Palmoplantar Psoriasis, Nail Psoriasis, Scalp Psoriasis, and Intertriginous Psoriasis. Indian J. Dermatol. 2017, 62, 113–122. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Xie, B.; He, Y. Efficacy of Systemic Treatments of Nail Psoriasis: A Systemic Literature Review and Meta-Analysis. Front. Med. 2021, 8, 620562. [Google Scholar] [CrossRef] [PubMed]
- Krajewska-Włodarczyk, M.; Owczarczyk-Saczonek, A.; Placek, W.; Wojtkiewicz, M.; Wojtkiewicz, J. Effect of Methotrexate in the Treatment of Distal Interphalangeal Joint Extensor Tendon Enthesopathy in Patients with Nail Psoriasis. J. Clin. Med. 2018, 7, 546. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krajewska-Włodarczyk, M.; Żuber, Z.; Owczarczyk-Saczonek, A. Ultrasound Evaluation of the Effectiveness of the Use of Acitretin in the Treatment of Nail Psoriasis. J. Clin. Med. 2021, 10, 2122. [Google Scholar] [CrossRef] [PubMed]
- Molina-Leyva, A.; Garrido-Pareja, F.; Ruiz-Carrascosa, J.C.; Ruiz-Villaverde, R. TNF-alpha inhibition could reduce biomarkers of endothelial dysfunction in patients with moderate to severe psoriasis: A 52-week echo-Doppler based quasi-experimental study. Med. Clin. 2018, 150, 465–468. [Google Scholar] [CrossRef]
- De Rossi, S.D.; Mendonça, J.A.; Palominos, P.E.; Kohem, C.L.; Cestari, T.F.; da Silva Chakr, R.M. Ultrasonographic and resistance index evaluation of nails in psoriatic arthritis, psoriasis, and control groups: A cross-sectional study. Adv Rheumatol. 2021, 61, 48. [Google Scholar] [CrossRef]
- Mendonça, J.A.; Pansani, L.N.; Mimoto, M.B.; Ferreira, I.T.G.; Sanches, F.B.; de Campos Ferreira Pinto, T.; Leandro-Merhi, V.A.; de Aquino, J.L.B. Nail enthesis ultrasound and automated software-guided assessment of bilateral common carotid intima-media thickness in psoriasis and psoriatic arthritis: Is there a correlation with clinical and laboratory findings? Drugs Context. 2020, 9, 2020-1-2. [Google Scholar] [CrossRef]
- Moreno, M.; Lisbona, M.P.; Gallardo, F.; Deza, G.; Ferran, M.; Pontes, C.; Luelmo, J.; Maymó, J.; Gratacós, J. Ultrasound Assessment of Psoriatic Onychopathy: A Cross-sectional Study Comparing Psoriatic Onychopathy with Onychomycosis. Acta Derm. Venereol. 2019, 99, 164–169. [Google Scholar] [CrossRef] [Green Version]
- Naredo, E.; Janta, I.; Baniandrés-Rodríguez, O.; Valor, L.; Hinojosa, M.; Bello, N.; Serrano, B.; Garrido, J. To what extend is nail ultrasound discriminative between psoriasis, psoriatic arthritis and healthy subjects? Rheumatol. Int. 2019, 39, 697–705. [Google Scholar] [CrossRef]
- Bakirci Ureyen, S.; Kara, R.O.; Erturk, Z.; Yaldiz, M. The microvascular and morphostructural changes of nails in psoriatic patients with nail disease; a link between ultrasound and videocapillaroscopy findings in the nailfold. Med. Ultrason. 2018, 20, 185–191. [Google Scholar] [CrossRef] [Green Version]
- Mondal, S.; Dutta, S.; Lahiri, D.; Sinha, D.; Sircar, G.; Mandal, A.K.; Kejriwal, M.; Ghosh, A. Assessment of nail unit structures by ultrasound in patients with psoriatic arthritis and their correlations with disease activity indices: A case-control study. Rheumatol. Int. 2018, 38, 2087–2093. [Google Scholar] [CrossRef]
- Idolazzi, L.; Gisondi, P.; Fassio, A.; Viapiana, O.; Giollo, A.; Rossini, M.; Girolomoni, G.; Gatti, D. Ultrasonography of the nail unit reveals quantitative and qualitative alterations in patients with psoriasis and psoriatic arthritis. Med. Ultrason. 2018, 20, 177–184. [Google Scholar] [CrossRef] [Green Version]
- Acquitter, M.; Misery, L.; Saraux, A.; Bressollette, L.; Jousse-Joulin, S. Detection of subclinical ultrasound enthesopathy and nail disease in patients at risk of psoriatic arthritis. Jt. Bone Spine 2017, 84, 703–707. [Google Scholar] [CrossRef]
- Arbault, A.; Devilliers, H.; Laroche, D.; Cayot, A.; Vabres, P.; Maillefert, J.F.; Ornetti, P. Reliability, validity and feasibility of nail ultrasonography in psoriatic arthritis. Jt. Bone Spine. 2016, 83, 539–544. [Google Scholar] [CrossRef]
- Marina, M.E.; Solomon, C.; Bolboaca, S.D.; Bocsa, C.; Mihu, C.M.; Tătaru, A.D. High-frequency sonography in the evaluation of nail psoriasis. Med. Ultrason. 2016, 18, 312–317. [Google Scholar] [CrossRef] [Green Version]
- Gutierrez, M.; Di Geso, L.; Salaffi, F.; Bertolazzi, C.; Tardella, M.; Filosa, G.; Filippucci, E.; Grassi, W. Development of a preliminary US power Doppler composite score for monitoring treatment in PsA. Rheumatology 2012, 51, 1261–1268. [Google Scholar] [CrossRef] [Green Version]
- Husein El-Ahmed, H.; Garrido-Pareja, F.; Ruiz-Carrascosa, J.C.; Naranjo-Sintes, R. Vessel resistance to blood flow in the nailfold in patients with psoriasis: A prospective case-control echo Doppler-based study. Br. J. Dermatol. 2012, 166, 54–58. [Google Scholar] [CrossRef]
- Gutierrez, M.; Wortsman, X.; Filippucci, E.; De Angelis, R.; Filosa, G.; Grassi, W. High-frequency sonography in the evaluation of psoriasis: Nail and skin involvement. J. Ultrasound Med. 2009, 28, 1569–1574. [Google Scholar] [CrossRef]
- Fournié, B.; Margarit-Coll, N.; Champetier de Ribes, T.L.; Zabraniecki, L.; Jouan, A.; Vincent, V.; Chiavassa, H.; Sans, N.; Railhac, J.J. Extrasynovial ultrasound abnormalities in the psoriatic finger. Prospective comparative power-doppler study versus rheumatoid arthritis. Jt. Bone Spine 2006, 73, 527–531. [Google Scholar] [CrossRef]
- Wollina, U.; Berger, M.; Karte, K. Calculation of nail plate and nail matrix parameters by 20 MHz ultrasound in healthy volunteers and patients with skin disease. Skin Res. Technol. 2001, 7, 60–64. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Population | Study Design | Imaging Sites | Equipment |
|---|---|---|---|---|
| De Rossi et al. (2021) [36] | 35 PsO, 31 PsA, and 35 controls patients | Cross-sectional | bilateral 2nd and 3rd fingernails | MyLab 50 system (Esaote Biomedica, Genova, Italy), with a linear 10 to 18 MHz transducer and a 6.6 to 8.0 MHz transducer for power Doppler. |
| Krajewska-Włodarczyk et al. (2021) [34] | 41 patients with nail Ps (without PsA), 28 HCs | Prospective | All fingernails | DermaMed (DRAMIŃSKI, Olsztyn, Poland), with linear probe with a frequency of 24 MHz. MyLab Omega (Esaote, Genova, Italy) and with the power Doppler (PD) technique |
| Mendonça et al. (2020) [37] | 30 patients with PsO and PsA (15 for each disease). | Cross-sectional | All fingernails | Esaote MyLab 50, 18 MHz linear probe, power Doppler frequency of 6.6–8 MHz, pulse repetition frequency that varied from 0.5 Hz to 1.0 MHz, and low filter |
| Idolazzi et al. (2019) [25] | 51 patients with PsA, 31 with Ps, 37 with RA, 34 with OA, 50 HCs | Cross-sectional | the middle third of the second fingernail, dominant side hand. | General Electric Logiq S8 machine or Esaote MyLabClassC with a multifrequency linear probe with a frequency of 18 MHz. The power Doppler parameters: a pulse repetition frequency (PRF) of 600 KHz and frequency of 10 MHz |
| Krajewska-Włodarczyk et al. (2019) [22] | 41 patients with Ps and 31 with PsA, 30 HCs | Cross-sectional | All fingernails | DermaMed (DRAMIŃSKI, Olsztyn, Poland). The US nail examinations were conducted with a linear head with a frequency of 24 MHz. |
| Moreno et al. (2019) [38] | 35 patients with Ps onychopathy and 25 with nail dystrophy secondary to onychomycosis | Cross-sectional | One (most affected) nail | Esaote My Lab 60© Ultrasound System (Esaote, Genova, Italy), transducer frequency range of 7–13 MHz, equipped with Doppler |
| Naredo et al. (2019) [39] | 60 patients with PsA, 21 with PsO, and 20 HCs | Cross-sectional | All fingers of both hands | Esaote Mylab Twice, (Genoa, Italy) equipped with a multifrequency (10–22 MHz) linear transducer |
| Bakirci et al. (2018) [40] | 34 patients with nail Ps and 15 HCs | Cross-sectional | right second finger. | LOGIQ P9 (General Electric Company, United Kingdom), with a 7–13 MHz linear transducer |
| Moya Alvarado et al. (2018) [30] | 48 patients with Ps and asymptomatic PsA (25 Ps, 23 PsA) | Prospective | Five nails of the dominant hand | MyLab Touch, Esaote Biomedica, Italy) with a variable frequency transducer with a linear array of 18 to 22 MHz in mode B |
| Mondal et al. (2018) [41] | 45 patients with PsA and 45 HCs | Case-control | All fingernails | My Lab 25 gold, Esaote, with 18 MHz linear array transducer |
| Krajewska-Włodarczyk et al. (2018) [22] | 69 patients with psoriatic changes in nails (38 with Ps and 31 with PsA) and 30 HCs | Cross-sectional | All fingernails | DermaMed (DRAMIŃSKI, Olsztyn, Poland) with a linear head with a frequency of 24 MHz. |
| Krajewska-Włodarczyk et al. (2018) [33] | 32 patients with nail Ps and with DIP joint extensor tendon enthesopathy in at least one finger revealed in a US examination (19 with Ps and 13 with PsA) | Prospective | All fingernails | DermaMed (DRAMIŃSKI, Olsztyn, Poland) with a linear probe with a frequency of 24 MHz. |
| Idolazzi et al. (2018) [42] | 82 patients with Ps and/or PsA, and 50 HCs | Cross-sectional | the middle third of the second fingernail, dominant side hand. | General Electric Logiq S8 with a multifrequency linear probe (Li8-18) with setting at 18 MHz. Power Doppler parameters were set selecting a PRF of 600 KHz and frequency of 10 MHz. |
| Molina-Leyva et al. (2018) [35] | 15 patients with moderate-severe Ps | Prospective | proximal nailfold of the fourth finger of the nondominant hand | n/a |
| Acosta-Felquer et al. (2017) [29] | 54 patients with PsO and 56 with PsA | Cross-sectional | All fingernails | MyLab 70 (Esaote Biomedica, Genoa, Italy) linear head (6–18 MHz) |
| Acquitter et al. (2017) [43] | 18 nail PsO, 19 scalp or inverse PsO | Prospective | Every patient was scanned for 14 entheses and 12 nails (10 fingernails and 2 toenails) | IU 22 machine (Philips) linear probe at 12.5 MHz. |
| Arbault et al. (2016) [44] | 27 patients with PsA | Pilot prospective study | All fingernails | ESAOTE MyLab 70 XVG fitted with a high frequency transducer of 22 mHz |
| Marina et al. (2016) [45] | 23 patients with moderate-to-severe psoriasis, (14 with nail psoriasis and 9 without nail involvement), and 11 HCs | Cross-sectional | 79 fingernails with Ps changes, 43 fingernails without Ps changes 82 fingernails in HCs | Ultrasonix Medical Corporation, (Richmond, Canada) with a variable-frequency (from 8 to 40 MHz) transducer (focal range 0.2–3 cm, image field 16 mm) and Hitachi EUB 8500 System with a variable-frequency transducer (6.5–13 MHz) |
| Sandobal et al. (2014) [27] | 35 patients with PsA, 20 with Ps, and 2 control groups (28 control subjects and 27 patients with RA) | Cross-sectional | All nails of both hands | Esaote Biomedica, Genoa, Italy) with a variable-frequency transducer ranging from 10 to 18 MHz and a Doppler frequency ranging from 6 to 8 MHz |
| Aydin et al. (2013) [5] | 5 patients with PsO, 13 with PsA with at least one involved nail, 12 healthy controls | Cross-sectional | All fingernails | Logiq E9 machine (General Electric, Wauwatosa, Wisc., USA) with a linear probe at 9–14 MHz |
| Aydin et al. (2012) [24] | 86 Ps patients and 20 healthy controls | Cross-sectional | 2 fingernails (one on each hand) | Logiq E9 machine (General Electric, Wauwatosa, Wisc., USA) with a linear probe at 10–18 MHz |
| Gisondi et al. (2012) [23] | 138 patients with Ps, 46 healthy controls, 37 with chronic eczema | Cross-sectional | Right hand fingernails | Voluson I portable ultra- sound machine (General Electrics, United States) with linear 10–18 MHz probe equipped with a variable-fre- quency transducer of 18 MHz |
| Gutierrez et al. (2012) [46] | 21 patients with PsA | Prospective | 16 joints, 9 tendons, 11 enthesis, 16 psoriatic plaques and 8 psoriatic onychopathies | MyLab 70 XVG (Esaote SpA, Genoa, Italy) with a broadband frequency transducer ranging from 6 to 18 MHz and Doppler frequency ranging from 5.9 to 14.3 MHz |
| Husein El-Ahmed et al. (2012) [47] | 23 patients with moderate-to-severe Ps and 23 controls without Ps | Cross-sectional | Echo Doppler examination on the proximal third of the nail plate of the fourth finger of the nondominant hand. | n/a |
| Gutierrez et al. (2010) [21] | 30 patients with PsA | Cross-sectional | n/a | MyLab 70 XVG US system (Esaote Biomedica Genoa, Italy) with a 6–18 MHz linear transducer (B-mode frequency of 18 MHz and Doppler frequency of 9.1 MHz) |
| Gutierrez et al. (2009) [48] | 30 patients with Ps, 15 HCs | Cross-sectional | Nails with psoriatic changes | MyLab 70 XVG system (Esaote Biomedica, Genoa, Italy) equipped with a variable-frequency transducer ranging from 6 to 18 MHz |
| Fournié et al. (2006) [O] [49] | 21 patients with RA, 20 with PsA | Cross-sectional | 25 fingers in RA (1 finger in 18 patients, 2 in 2 patients, and 3 in 1 patient) and 25 fingers in PsA (1 finger in 15 patients and 2 in 5 patients) | Siemens Sonoline Elegra (Cheshire, CT, USA) with 13.5-MHz linear transducer |
| Wollina et al. (2001) [P] [50] | 37 patients with nail diseases (11 with SLE, 8 with systemic sclerosis, 9 with Ps, 5 with chronic hand eczema and others, and 34 healthy controls | Cross-sectional | All fingernails | Derma-scan C, Cortex Technology (Hadsund, Denmark) with a 20 MHz probe in B-scan mode. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Krajewska-Włodarczyk, M.; Owczarczyk-Saczonek, A. Usefulness of Ultrasound Examination in the Assessment of the Nail Apparatus in Psoriasis. Int. J. Environ. Res. Public Health 2022, 19, 5611. https://doi.org/10.3390/ijerph19095611
Krajewska-Włodarczyk M, Owczarczyk-Saczonek A. Usefulness of Ultrasound Examination in the Assessment of the Nail Apparatus in Psoriasis. International Journal of Environmental Research and Public Health. 2022; 19(9):5611. https://doi.org/10.3390/ijerph19095611
Chicago/Turabian StyleKrajewska-Włodarczyk, Magdalena, and Agnieszka Owczarczyk-Saczonek. 2022. "Usefulness of Ultrasound Examination in the Assessment of the Nail Apparatus in Psoriasis" International Journal of Environmental Research and Public Health 19, no. 9: 5611. https://doi.org/10.3390/ijerph19095611
APA StyleKrajewska-Włodarczyk, M., & Owczarczyk-Saczonek, A. (2022). Usefulness of Ultrasound Examination in the Assessment of the Nail Apparatus in Psoriasis. International Journal of Environmental Research and Public Health, 19(9), 5611. https://doi.org/10.3390/ijerph19095611