
The Role of Psychological Wellbeing in a Cross-Provider Worksite Healthcare Management Program for Employees with Musculoskeletal Disorders



_Choi.png)
Abstract
:1. Introduction
2. Materials and Methods
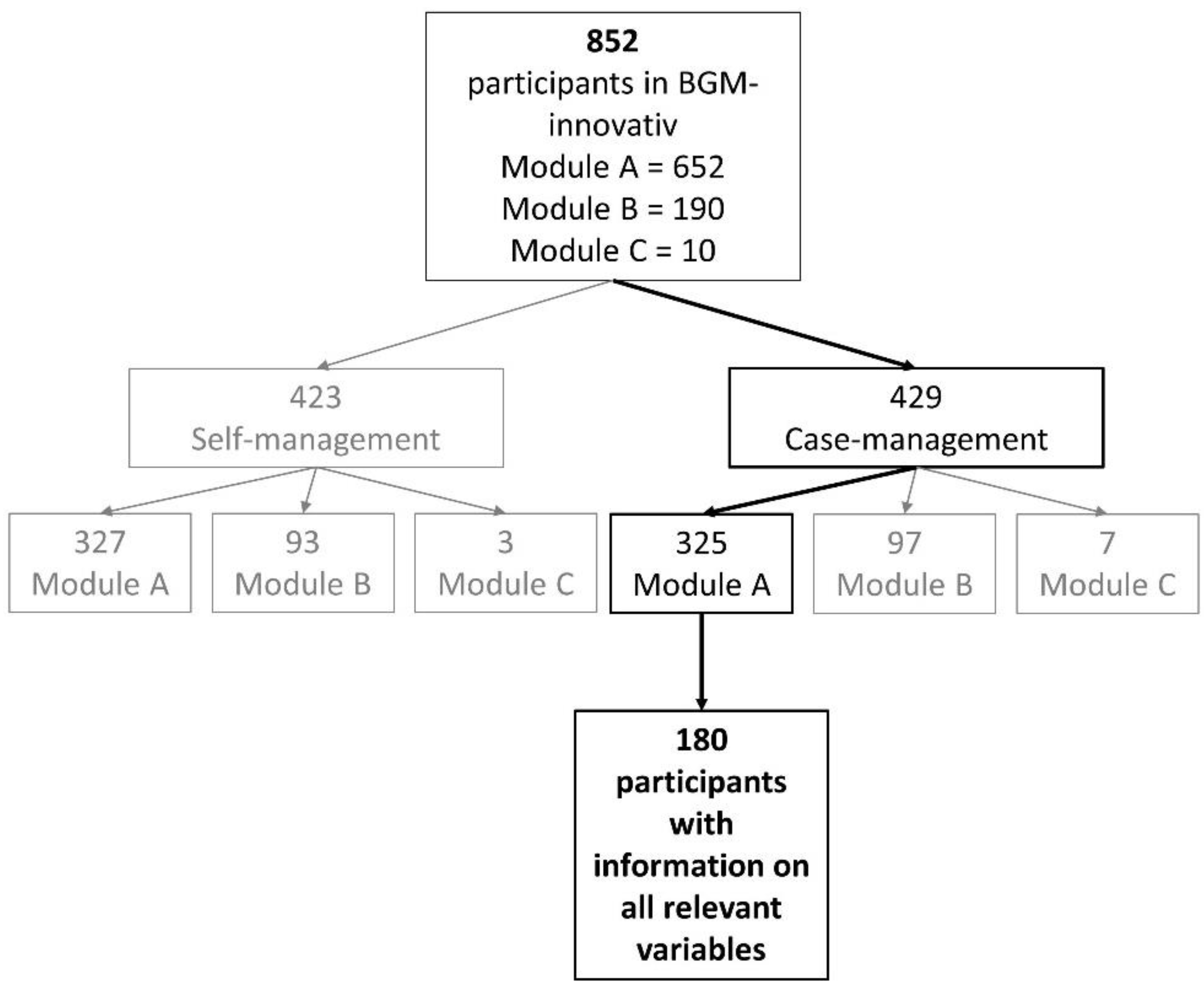
2.1. Study Design and Participants
2.2. Measures
2.3. Statistical Analysis
- H3: In model I, we used psychological wellbeingt1 as the dependent variable and pain intensity∆ as the independent variable. As confounding variables, we considered psychological wellbeingt0, motivationt0, satisfactiont1, training qualityt1, and age, gender, and educational degree at t0 as the independent variables. In model II, we added the disability score∆ to test for mediation.
- H4: In model III, we used the disability scoret1 as the dependent variable and psychological wellbeing∆ as the independent variable. As confounding variables, we considered the disability scoret0, pain intensity∆, motivationt0, satisfactiont1, training qualityt1, and age, gender, and educational degree at t0 as independent variables.
3. Results
4. Discussion
- H1: T-tests’ results confirmed the hypothesis that the psychological wellbeing of employees significantly increased after the intervention.
- H2: Regarding differences in individuals with low and high psychological wellbeingt0, we found significant results for the disability scoret0,t1, pain intensityt0,t1, and motivationt1. The disability scoret0,t1 and pain intensityt0,t1 were higher in individuals with low psychological wellbeingt0; motivationt0 was higher in individuals with high psychological wellbeingt0.
- H3: Pain intensity∆ was not significant for psychological wellbeingt1 after adding the disability score∆ in model II. This indicates that, in our study sample, impairment due to pain totally mediates the impact of pain intensity on psychological wellbeing.
- H4: Results in model III indicate that the more the psychological wellbeing of participants increased, the better their disability scoret1 was.
Strenghts and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
| Variable | N | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| (1) Psychological wellbeingt1 | 180 | - | 0.492 *** | 0.274 *** | 0.246 ** | 0.432 *** | 0.409 * | −0.148 | 0.029 | 0.103 | −0.058 |
| (2) Psychological wellbeingt0 | 180 | - | 0.004 | −0.104 | 0.387 *** | 0.081 | −0.041 | 0.036 | 0.047 | −0.034 | |
| (3) Pain intensity∆ | 180 | - | 0.581 *** | 0.069 | 0.242 ** | −0.188 * | −0.043 | 0.072 | −0.058 | ||
| (4) Disability score∆ | 180 | - | 0.092 | 0.284 *** | 0.055 | −0.080 | −0.072 | −0.132 | |||
| (5) Motivation | 180 | - | 0.341 *** | 0.033 | 0.106 | 0.105 | 0.019 | ||||
| (6) Satisfaction | 180 | - | −0.324 *** | 0.004 | 0.113 | 0.008 | |||||
| (7) Training quality | 180 | - | 0.154 * | −0.027 | −0.116 | ||||||
| (8) Gender | 180 | - | 0.043 | −0.012 | |||||||
| (9) Educational degree | 180 | - | −0.134 | ||||||||
| (10) Age | 180 | - |
| Variable | N | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| (1) Disability scoret1 | 180 | - | 0.419 *** | 0.406 *** | −0.272 *** | −0.237 ** | −0.343 *** | 0.133 | 0.025 | −0.101 | 0.118 |
| (2) Disability scoret0 | 180 | - | 0.224 ** | 0.104 | −0.130 | −0.029 | 0.184 * | −0.061 | −0.173 * | −0.026 | |
| (3) Pain intensity∆ | 180 | - | 0.263 *** | 0.069 | 0.242 ** | −0.188 * | −0.043 | 0.072 | −0.058 | ||
| (4) Psychological wellbeing∆ | 180 | - | 0.031 | 0.317 *** | −0.102 | −0.008 | 0.054 | −0.022 | |||
| (5) Motivation | 180 | - | 0.341 *** | 0.033 | 0.106 | 0.105 | 0.019 | ||||
| (6) Satisfaction | 180 | - | −0.324 *** | 0.004 | 0.113 | 0.008 | |||||
| (7) Training quality | 180 | - | 0.154 * | −0.027 | −0.116 | ||||||
| (8) Gender | 180 | - | 0.043 | −0.012 | |||||||
| (9) Educational degree | 180 | - | −0.134 | ||||||||
| (10) Age | 180 | - |
References
- Knieps, F.; Pfaff, H.; Bernickel, R. Mobilität–Arbeit–Gesundheit: Zahlen, Daten, Fakten; BKK Gesundheitsreport: Berlin, Germany, 2020. [Google Scholar]
- Rothe, I.; Adolph, L.; Beermann, B.; Schütte, M.; Windel, A.; Grewer, A.; Lenhardt, U.; Michel, J.; Thomson, B.; Formazin, M. Psychische Gesundheit in der Arbeitswelt: Wissenschaftliche Standortbestimmung; BauA: Dortmund, Germany, 2017. [Google Scholar]
- Zeike, S.; Bradbury, K.; Lindert, L.; Pfaff, H. Digital Leadership Skills and Associations with Psychological Well-Being. Int. J. Environ. Res. Public Health 2019, 16, 2628. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zeike, S.; Choi, K.-E.; Lindert, L.; Pfaff, H. Manager’s Well-Being in the Digital Era: Is it Associated with Perceived Choice Overload and Pressure from Digitalization? An Exploratory Study. Int. J. Environ. Res. Public Health 2019, 16, 1746. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bernal, D.; Campos-Serna, J.; Tobias, A.; Vargas-Prada, S.; Benavides, F.G.; Serra, C. Work-related psychosocial risk factors and musculoskeletal disorders in hospital nurses and nursing aides: A systematic review and meta-analysis. Int. J. Nurs. Stud. 2015, 52, 635–648. [Google Scholar] [CrossRef] [PubMed]
- Lacey, R.J.; Lewis, M.; Sim, J. Piecework, musculoskeletal pain and the impact of workplace psychosocial factors. Occup. Med. 2007, 57, 430–437. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simon, M.; Tackenberg, P.; Nienhaus, A.; Estryn-Behar, M.; Conway, P.M.; Hasselhorn, H.-M. Back or neck-pain-related disability of nursing staff in hospitals, nursing homes and home care in seven countries—Results from the European NEXT-Study. Int. J. Nurs. Stud. 2008, 45, 24–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, D.R.; Wei, N.; Zhao, L.; Wang, R.-S. Musculoskeletal complaints and psychosocial risk factors among Chinese hospital nurses. Occup. Med. 2004, 54, 579–582. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sobeih, T.M.; Salem, O.; Daraiseh, N.; Genaidy, A.; Shell, R. Psychosocial factors and musculoskeletal disorders in the construction industry: A systematic review. Theor. Issues Ergon. Sci. 2006, 7, 329–344. [Google Scholar] [CrossRef]
- Heikkinen, J.; Honkanen, R.; Williams, L.; Leung, J.; Rauma, P.; Quirk, S.; Koivumaa-Honkanen, H. Depressive disorders, anxiety disorders and subjective mental health in common musculoskeletal diseases: A review. Maturitas 2019, 127, 18–25. [Google Scholar] [CrossRef] [PubMed]
- de Kok, J.; Vroonhof, P.; Snijders, J.; Roullis, G.; Clarke, M.; Peereboom, K.; van Dorst, P.; Isusi, I. Work-Related Musculoskeletal Disorders: Prevalence, Costs and Demographics in the EU: European Risk Observatory. Report; European Agency for Safety and Health at Work: Luxembourg, 2019. [Google Scholar]
- Kelsall, H.L.; McKenzie, D.P.; Forbes, A.B.; Roberts, M.H.; Urquhart, D.M.; Sim, M.R. Pain-related musculoskeletal disorders, psychological comorbidity, and the relationship with physical and mental well-being in Gulf War veterans. Pain 2014, 155, 685–692. [Google Scholar] [CrossRef] [PubMed]
- Larsson, B.; Dragioti, E.; Gerdle, B.; Björk, J. Positive psychological well-being predicts lower severe pain in the general population: A 2-year follow-up study of the SwePain cohort. Ann. Gen. Psychiatry 2019, 18, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Budtz, C.R.; Mose, S.; Christiansen, D.H. Socio-demographic, clinical and psychological predictors of healthcare utilization among patients with musculoskeletal disorders: A prospective cohort study. BMC Health Serv. Res. 2020, 20, 1–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Müller-Schwefe, G.H.H.; Überall, M.A. Schmerz und Lebensqualität. Gesundh. Qual. 2011, 16, S20–S22. [Google Scholar] [CrossRef]
- A Abas, M.; Punpuing, S.; Jirapramupitak, T.; Tangchonlatip, K.; Leese, M. Psychological wellbeing, physical impairments and rural aging in a developing country setting. Health Qual. Life Outcomes 2009, 7, 66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Finnes, A.; Enebrink, P.; Ghaderi, A.; Dahl, J.; Nager, A.; Öst, L.-G. Psychological treatments for return to work in individuals on sickness absence due to common mental disorders or musculoskeletal disorders: A systematic review and meta-analysis of randomized-controlled trials. Int. Arch. Occup. Environ. Health 2018, 92, 273–293. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liebers, F.; Caffier, G. Berufsspezifische Arbeitsunfähigkeit durch Muskel-Skelett-Erkrankungen in Deutschland: Forschung Projekt F 1996; Bundesanst. für Arbeitsschutz und Arbeitsmedizin: Dortmund, Germany, 2009. [Google Scholar]
- Choi, K.-E.; Lindert, L.; Schlomann, L.; Samel, C.; Hellmich, M.; Pfaff, H. A Cross-Provider Healthcare Management Program for Musculoskeletal Disorders: Results of a Randomized Controlled Trial in 22 German Companies. Int. J. Environ. Res. Public Health 2021, 18, 11844. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO (Fünf)-Fragebogen zum Wohlbefinden (Version 1998); Psychiatric Research Unit, WHO Collaborating Center for Mental Health: Hillerød, Denmark, 1998. [Google Scholar]
- Löwe, B.; Spitzer, R.L.; Gräfe, K.; Kroenke, K.; Quenter, A.; Zipfel, S.; Buchholz, C.; Witte, S.; Herzog, W. Comparative validity of three screening questionnaires for DSM-IV depressive disorders and physicians’ diagnoses. J. Affect. Disord. 2004, 78, 131–140. [Google Scholar] [CrossRef]
- Pfingsten, M.; Nagel, B.; Emrich, O.; Seemann, H.; Lindena, G. Deutscher Schmerz-Fragebogen: Handbuch; DGSS: Berlin, Germany, 2015. [Google Scholar]
- Emerson, N.D.; Merrill, D.A.; Shedd, K.; Bilder, R.; Siddarth, P. Effects of an employee exercise programme on mental health. Occup. Med. 2016, 67, 128–134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Macdonald, W.; Oakman, J. Requirements for more effective prevention of work-related musculoskeletal disorders. BMC Musculoskelet. Disord. 2015, 16, 293. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moormann, T.; Lindert, L.; Choi, K.-E.A.; Leineweber, B. BGM-innovativ: Starke Netzwerke geben Rück(en)halt. In Netzwerke(n) für Gesundheit; Kliner, K., Rennert, D., Richter, M., Eds.; MWV Medizinisch Wissenschaftliche Verlagsgesellschaft: Berlin, Germany, 2019; pp. 11–18. ISBN 978-3-95466-443-6. [Google Scholar]

| N | % | |||
|---|---|---|---|---|
| Age | ||||
| ≤29 years | 9 | 5.0 | ||
| 30 to 39 years | 23 | 12.8 | ||
| 40 to 49 years | 52 | 28.9 | ||
| 50 to 59 years | 81 | 45.0 | ||
| 60 to 69 years | 15 | 8.3 | ||
| ≥70 years | 0 | 0.00 | ||
| Gender | ||||
| Male | 136 | 75.6 | ||
| Female | 44 | 24.4 | ||
| Educational degree | ||||
| No vocational degree | 8 | 4.4 | ||
| Completed vocational education | 101 | 56.1 | ||
| completed training at a technical school, master school, vocational academy, or technical academy | 45 | 25.0 | ||
| College degree | 19 | 10.6 | ||
| University degree | 7 | 3.9 | ||
| N | M | SD | Median (min/max) | |
| Disability scoret0 | 180 | 40.33 | 22.24 | 40.00 (0.00/90.00) |
| Disability scoret1 | 180 | 24.54 | 21.23 | 20.00 (0.00/100.00) |
| Pain intensityt0 | 180 | 49.52 | 19.65 | 50.00 (3.33/93.33) |
| Pain intensityt1 | 180 | 35.02 | 20.85 | 33.33 (0.00/93.33) |
| Psychological wellbeingt0 | 180 | 13.34 | 5.09 | 14.00 (5.00/24.00) |
| Psychological wellbeingt1 | 180 | 15.09 | 4.92 | 16.00 (1.00/25.00) |
| Motivationt0 | 180 | 8.09 | 1.49 | 8.00 (2.00/10.00) |
| Satisfactiont1 | 180 | 4.24 | 0.77 | 4.00 (1.00/5.00) |
| Training qualityt1 | 180 | 3.28 | 0.74 | 3.00 (3.00/9.00) |
| Low Psychological Wellbeingt0 1 | High Psychological Wellbeingt0 1 | t-Test p-Value | |||||||
|---|---|---|---|---|---|---|---|---|---|
| N | M | SD | Median | N | M | SD | Median | ||
| Pain intensityt0 | 73 | 54.93 | 18.01 | 56.67 | 107 | 45.83 | 19.94 | 46.67 | 0.002 ** |
| Pain intensityt1 | 73 | 41.14 | 20.66 | 40.00 | 107 | 30.84 | 20.02 | 30.00 | 0.001 ** |
| Disability scoret0 | 73 | 48.45 | 20.09 | 50.00 | 107 | 34.80 | 22.02 | 30.00 | 0.000 *** |
| Disability scoret1 | 73 | 29.68 | 22.20 | 26.67 | 107 | 21.03 | 19.89 | 16.67 | 0.007 * |
| Training qualityt1 | 73 | 3.34 | 0.67 | 3.00 | 107 | 3.23 | 0.78 | 3.00 | 0.334 |
| Motivationt0 | 73 | 7.55 | 1.62 | 8.00 | 107 | 8.46 | 1.27 | 8.00 | 0.000 *** |
| Satisfactiont1 | 73 | 4.23 | 0.76 | 4.00 | 107 | 4.25 | 0.79 | 4.00 | 0.869 |
| Variable Response Trait | Low psychological wellbeingt0 1 (Percentage) | High psychological wellbeingt0 1 (Percentage) | Chi-Square Test p-value | ||||||
| Gender | |||||||||
| Men | 53 (29.4) | 83 (46.1) | 0.446 | ||||||
| Women | 20 (11.1) | 24 (13.3) | |||||||
| Age 2 | |||||||||
| ≤29 to 49 years | 32 (17.8) | 52 (28.9) | 0.529 | ||||||
| 50 to ≥70 years | 41 (22.8) | 55 (30.6) | |||||||
| Educational status 2 | |||||||||
| no vocational degree/completed vocational education | 44 (24.4) | 65 (36.1) | 0.949 | ||||||
| higher | 29 (16.1) | 42 (23.3) | |||||||
| Determinant Factors 1 | Regression Coefficient B (SE) | Beta | p-Value | 95% Confidence Interval | R2 (Adjusted) | |
|---|---|---|---|---|---|---|
| Lower Value | Upper Value | |||||
| Psychological wellbeingt0 | 0.387 (0.061) | 0.400 | <0.001 *** | 0.267 | 0.507 | 0.438 (0.412) |
| Pain intensity∆ | 0.048 (0.015) | 0.190 | 0.002 ** | 0.018 | 0.077 | |
| Motivationt0 | 0.576 (0.224) | 0.174 | 0.011 * | 0.133 | 1.019 | |
| Satisfactiont1 | 1.673 (0.425) | 0.263 | <0.001 *** | 0.834 | 2.512 | |
| Training qualityt1 | −0.140 (0.422) | −0.021 | 0.741 | −0.972 | 0.692 | |
| Gender | 0.064 (0.668) | 0.006 | 0.924 | −1.255 | 1.382 | |
| Age 2 | −0.379 (0.577) | −0.039 | 0.512 | −1.518 | 0.760 | |
| Educational degree 2 | 0.173 (0.588) | 0.017 | 0.769 | −0.988 | 1.334 | |
| Determinant Factors 1 | Regression Coefficient B (SE) | Beta | p-Value | 95% Confidence Interval | R2 (Adjusted) | |
|---|---|---|---|---|---|---|
| Lower Value | Upper Value | |||||
| Psychological wellbeingt0 | 0.406 (0.061) | 0.419 | 0.000 *** | 0.286 | 0.526 | 0.451 (0.422) |
| Pain intensity∆ | 0.026 (0.018) | 0.102 | 0.166 | −0.011 | 0.062 | |
| Disability score∆ | 0.033 (0.016) | 0.155 | 0.046 * | 0.001 | 0.064 | |
| Motivationt0 | 0.555 (0.223) | 0.167 | 0.014 * | 0.116 | 0.995 | |
| Satisfactiont1 | 1.442 (0.437) | 0.227 | 0.001 ** | 0.580 | 2.304 | |
| Training qualityt1 | 0.375 (0.434) | −0.056 | 0.389 | −1.231 | 0.482 | |
| Gender | 0.217 (0.666) | 0.019 | 0.745 | −1.098 | 1.533 | |
| Age 2 | −0.228 (0.577) | −0.023 | 0.693 | −1.367 | 0.911 | |
| Educational degree 2 | 0.392 (0.593) | 0.039 | 0.509 | −0.779 | 1.563 | |
| Determinant Factors 1 | Regression Coefficient B (SE) | Beta | p-Value | 95% Confidence Interval | R2 (Adjusted) | |
|---|---|---|---|---|---|---|
| Lower Value | Upper Value | |||||
| Disability scoret0 | 0.543 (0.054) | 0.568 | <0.001 *** | 0.435 | 0.650 | 0.542 (0.517) |
| Pain intensity∆ | −0.499 (0.062) | −0.462 | <0.001 *** | −0.622 | −0.377 | |
| Psychological wellbeing∆ | −0.678 (0.237) | −0.161 | 0.005 ** | −1.145 | −0.211 | |
| Motivationt0 | −1.064 (0.818) | −0.074 | 0.195 | −2.679 | 0.552 | |
| Satisfactiont1 | −5.227 (1.722) | −0.191 | 0.003 ** | −8.627 | −1.827 | |
| Training qualityt1 | −3.754 (1.695) | −0.131 | 0.028 * | −7.100 | −0.407 | |
| Gender | 3.206 (2.613) | 0.065 | 0.222 | −1.952 | 8.363 | |
| Age 2 | 4.289 (2.249) | 0.101 | 0.058 | −0.149 | 8.728 | |
| Educational degree 2 | 3.255 (2.335) | 0.075 | 0.165 | −1.355 | 7.865 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lindert, L.; Schlomann, L.; Pfaff, H.; Choi, K.-E. The Role of Psychological Wellbeing in a Cross-Provider Worksite Healthcare Management Program for Employees with Musculoskeletal Disorders. Int. J. Environ. Res. Public Health 2022, 19, 5452. https://doi.org/10.3390/ijerph19095452
Lindert L, Schlomann L, Pfaff H, Choi K-E. The Role of Psychological Wellbeing in a Cross-Provider Worksite Healthcare Management Program for Employees with Musculoskeletal Disorders. International Journal of Environmental Research and Public Health. 2022; 19(9):5452. https://doi.org/10.3390/ijerph19095452
Chicago/Turabian StyleLindert, Lara, Lara Schlomann, Holger Pfaff, and Kyung-Eun (Anna) Choi. 2022. "The Role of Psychological Wellbeing in a Cross-Provider Worksite Healthcare Management Program for Employees with Musculoskeletal Disorders" International Journal of Environmental Research and Public Health 19, no. 9: 5452. https://doi.org/10.3390/ijerph19095452
APA StyleLindert, L., Schlomann, L., Pfaff, H., & Choi, K.-E. (2022). The Role of Psychological Wellbeing in a Cross-Provider Worksite Healthcare Management Program for Employees with Musculoskeletal Disorders. International Journal of Environmental Research and Public Health, 19(9), 5452. https://doi.org/10.3390/ijerph19095452