
Effects of Forest Healing Anti-Aging Program on Psychological, Physiological, and Physical Health of Older People with Mild Cognitive Impairment

 ,
,  , ,
, ,  ,
,  and
and
Abstract
1. Introduction
2. Materials and Methods
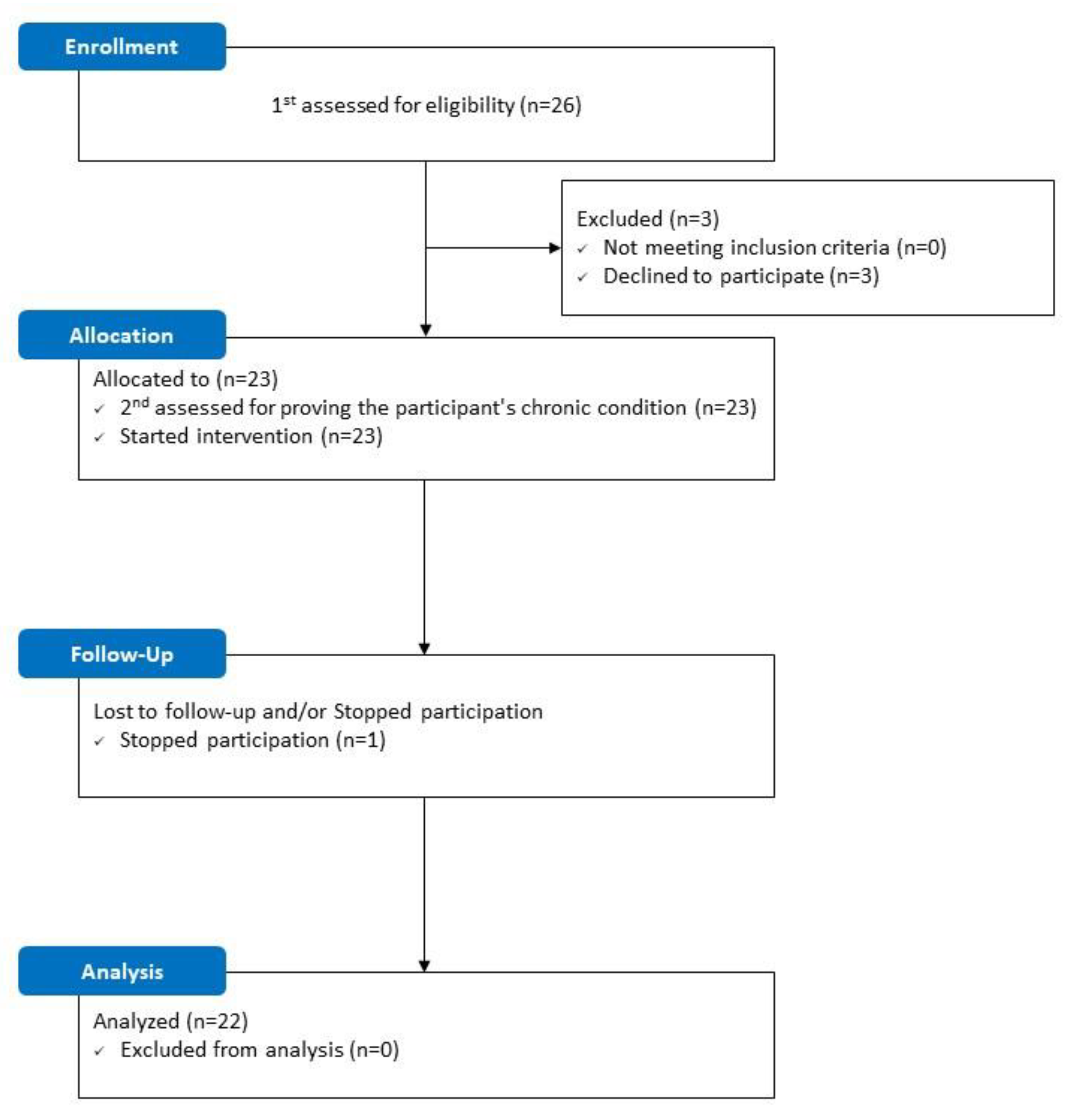
2.1. Participants
2.2. Study Sites
2.3. Procedure
2.4. Measurement
2.4.1. Psychological Variables
2.4.2. Physiological Variables
2.4.3. Physical Variables
2.5. Intervention
2.6. Statistics Analysis
3. Results
3.1. General Characteristics of Participants
3.2. Baseline Background Characteristics
3.2.1. Psychological Effects of the Forest Healing Anti-Aging Program
3.2.2. Physiological Effects of the Forest Healing Anti-Aging Program
3.2.3. Physical Effects of the Forest Healing Anti-Aging Program
4. Discussion
4.1. Effects of Forest Healing Anti-Aging Program on Psychological Health
4.2. Effect of Forest Healing Anti-Aging Program on Physiological Health
4.3. Effects of Forest Healing Anti-Aging Program on Physical Health
4.4. Sustainability of Forest Healing Program Effects
4.5. Significance and Limitations of This Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
| Variables | Reagent Name | Cat.no | Manufacturer | Country of Manufacture | Analysis Equipment |
|---|---|---|---|---|---|
| Cathepsin-B (pg/mL) | Human Cathepsin B | MBS175975 | Mybiosource | USA | spectramax190 |
| Cortisol (ug/dL) | Cortisol II | 7027150190 | Roche | Germany | cobas e801 |
| IGF-1 (ng/mL) | IGF | L2KIGF2 | Siemens | USA | Immulite xpi 2000 |
| CRP (mg/L) | CRPHS | 04628918190 | Roche | Germany | Cobas c502 |
| Variables | Pre 1 | Pre 2 | p-Value |
|---|---|---|---|
| Psychological variables | |||
| MMSE (score) | 26.41 ± 0.67 | 26.64 ± 0.79 | 0.132 b |
| BDI (score) | 8.68 ± 5.69 | 8.36 ± 5.12 | 0.530 a |
| POMS (score) | |||
| Tension-Anxiety | 9.00 ± 5.44 | 8.73 ± 4.10 | 0.835 a |
| Depression-Dejection | 12.41 ± 9.42 | 12.27 ± 9.64 | 0.972 b |
| Anger-Hostility | 6.86 ± 6.74 | 7.00 ± 5.85 | 0.875 b |
| Fatigue-Inertia | 7.50 ± 5.20 | 7.36 ± 4.93 | 0.858 a |
| Confusion-Bewilderment | 8.41 ± 5.15 | 8.23 ± 4.02 | 0.838 a |
| Vigor-Activity | 18.64 ± 6.04 | 18.41 ± 6.08 | 0.789 a |
| Total mood disturbance | 25.55 ± 27.71 | 25.18 ± 24.86 | 0.715 b |
| WHOQOL-BREF (score) | |||
| Overall QOL and General health | 6.59 ± 1.22 | 6.45 ± 1.26 | 0.477 b |
| Physical health | 23.05 ± 3.37 | 23.18 ± 4.00 | 0.583 b |
| Psychological | 17.23 ± 3.16 | 18.23 ± 3.05 | 0.090 a |
| Social relationship | 9.68 ± 1.39 | 9.09 ± 1.15 | 0.097 b |
| Environmental | 24.91 ± 5.10 | 24.68 ± 4.70 | 0.795 a |
| Total | 81.45 ± 11.59 | 81.64 ± 12.45 | 0.916 a |
| PSQI (score) | |||
| Sleep quality | 1.23 ± 0.81 | 1.23 ± 0.61 | 1.000 b |
| Sleep latency | 1.45 ± 1.18 | 1.45 ± 0.80 | 1.000 b |
| Sleep duration | 0.45 ± 0.60 | 0.41 ± 0.67 | 0.564 b |
| Habitual sleep efficiency | 0.41 ± 0.91 | 0.36 ± 0.85 | 0.887 b |
| Sleep disturbance | 1.36 ± 0.49 | 1.32 ± 0.57 | 0.763 b |
| Use of sleeping medication | 0.32 ± 0.89 | 0.23 ± 0.69 | 0.317 b |
| Daytime dysfunction | 1.36 ± 1.00 | 1.45 ± 0.74 | 0.527 b |
| Total | 6.59 ± 3.63 | 6.45 ± 3.04 | 0.825 a |
| Physiological variables | |||
| Vital signs | |||
| Systolic pressure (mmHg) | 126.45 ± 15.05 | 128.55 ± 12.63 | 0.471 a |
| Diastolic pressure (mmHg) | 73.95 ± 9.06 | 74.59 ± 7.59 | 0.604 a |
| Pulse pressure (mmHg) | 52.50 ± 7.93 | 53.95 ± 8.39 | 0.550 a |
| Heart rate (bpm) | 75.09 ± 8.51 | 73.55 ± 11.71 | 0.478 a |
| Body compositions | |||
| Skeletal muscle mass (kg) | 22.90 ± 4.16 | 23.15 ± 4.03 | 0.082 b |
| Body fat mass (kg) | 19.31 ± 3.67 | 19.12 ± 3.61 | 0.110 a |
| Total body water (L) | 30.39 ± 5.32 | 30.55 ± 5.18 | 0.356 b |
| Blood compositions | |||
| Cathepsin-B (pg/mL) | - | 183497.71 ± 71436.06 | - |
| Cortisol (μg/dL) | - | 13.04 ± 3.31 | - |
| IGF-1 (ng/mL) | - | 121.40 ± 32.78 | - |
| CRP (mg/L) | - | 1.07 ± 0.87 | - |
| Physical variables | |||
| Senior Fitness Test | |||
| Arm curl (n) | 17.36 ± 3.67 | 17.68 ± 4.06 | 0.167 a |
| 30-sec chair stand (n) | 11.45 ± 3.60 | 11.73 ± 3.71 | 0.110 a |
| 2-min step walk (n) | 90.95 ± 13.44 | 92.50 ± 12.63 | 0.054 a |
| 8-ft up and go (sec) | 7.94 ± 1.38 | 7.71 ± 1.13 | 0.074 a |
| Back scratch (cm) | −8.84 ± 11.47 | −8.50 ± 10.81 | 0.955 b |
| Chair sit and reach (cm) | 12.25 ± 9.59 | 13.09 ± 6.41 | 0.945 b |
| Muscle strength | |||
| Elbow flexor (kg) | 12.50 ± 3.04 | 11.35 ± 3.61 | 0.051 a |
| Knee extensor (kg) | 13.30 ± 2.05 | 13.01 ± 1.85 | 0.118 a |
| Ankle plantar flexor (kg) | 13.42 ± 2.18 | 13.16 ± 2.08 | 0.087 a |
| Grip (kg) | 25.74 ± 7.40 | 25.52 ± 7.18 | 0.673 a |
| Pinch (kg) | 7.30 ± 1.48 | 7.12 ± 1.46 | 0.083 b |
| Spatiotemporal parameter of gait | |||
| Velocity (cm/s) | 117.91 ± 17.71 | 121.02 ± 16.19 | 0.083 a |
| Cadence (steps/min) | 117.92 ± 10.57 | 119.99 ± 10.08 | 0.059 a |
| Step length—Rt. (cm) | 60.07 ± 5.93 | 61.03 ± 5.14 | 0.180 a |
| Stride length—Rt. (cm) | 119.72 ± 11.25 | 121.06 ± 10.29 | 0.309 a |
| Step time—Rt. (sec) | 0.51 ± 0.05 | 0.50 ± 0.05 | 0.066 a |
| Swing time—Rt. (sec) | 0.39 ± 0.03 | 0.38 ± 0.03 | 0.155 a |
| Stance time—Rt. (sec) | 0.64 ± 0.07 | 0.62 ± 0.06 | 0.115 b |
| Cycle time—Rt. (sec) | 1.02 ± 0.10 | 1.01 ± 0.09 | 0.075 b |
| Static balance | |||
| EO-Sway area (mm2) | 1.52 ± 1.35 | 1.47 ± 0.87 | 0.835 b |
| EO-Sway velocity (mm/s) | 1.07 ± 0.30 | 1.11 ± 0.29 | 0.177 a |
| EC-Sway area (mm2) | 2.35 ± 2.40 | 3.13 ± 3.43 | 0.200 b |
| EC-Sway velocity (mm/s) | 1.54 ± 0.55 | 1.80 ± 0.78 | 0.057 b |
| Dynamic balance (cm) | |||
| Anterior | 49.87 ± 7.45 | 49.41 ± 12.18 | 0.861 a |
| Right | 30.66 ± 3.81 | 32.25 ± 3.07 | 0.073 a |
| Left | 28.50 ± 4.69 | 30.55 ± 5.46 | 0.058 a |
References
- Korean Statistical Information Service. Available online: https://kosis.kr/index/index.do (accessed on 10 January 2022).
- World Health Organization. Dementia. Available online: https://www.who.int/news-room/fact-sheets/detail/dementia (accessed on 10 January 2022).
- Kim, H.; Hong, J.P.; Kang, J.M.; Kim, W.; Maeng, S.; Cho, S.; Na, K.; Oh, S.H.; Park, J.W.; Cho, S.; et al. Cognitive Reserve and the Effects of Virtual Reality-based Cognitive Training on Elderly Individuals with Mild Cognitive Impairment and Normal Cognition. Psychogeriatrics 2021, 21, 552–559. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health and Welfare of South Korea. Mild Cognitive Impairment, A Stage before Dementia, Has Increased 4.3 Times in the Past 5 Years. Available online: https://www.korea.kr/news/pressReleaseView.do?newsId=156074845#sitemap-layer (accessed on 10 January 2022).
- Kabisch, N.; van den Bosch, M.; Lafortezza, R. The Health Benefits of Nature-Based Solutions to Urbanization Challenges for Children and the Elderly—A Systematic Review. Environ. Res. 2017, 159, 362–373. [Google Scholar] [CrossRef] [PubMed]
- White, M.P.; Alcock, I.; Grellier, J.; Wheeler, B.W.; Hartig, T.; Warber, S.L.; Bone, A.; Depledge, M.H.; Fleming, L.E. Spending at Least 120 Minutes a Week in Nature Is Associated with Good Health and Wellbeing. Sci. Rep. 2019, 9, 7730. [Google Scholar] [CrossRef] [PubMed]
- Barton, J.; Griffin, M.; Pretty, J. Exercise-, Nature- and Socially Interactive-Based Initiatives Improve Mood and Self-Esteem in the Clinical Population. Perspect. Public Health 2012, 132, 89–96. [Google Scholar] [CrossRef]
- Thompson Coon, J.; Boddy, K.; Stein, K.; Whear, R.; Barton, J.; Depledge, M.H. Does Participating in Physical Activity in Outdoor Natural Environments Have a Greater Effect on Physical and Mental Wellbeing than Physical Activity Indoors? A Systematic Review. Environ. Sci. Technol. 2011, 45, 1761–1772. [Google Scholar] [CrossRef]
- Choi, J.-H.; Shin, C.-S.; Yeoun, P.-S. Effects of Forest-Walking Exercise on Functional Fitness and Gait Pattern in the Elderly. J. Korean For. Soc. 2014, 103, 503–509. [Google Scholar] [CrossRef][Green Version]
- Korea Forest Service. Article 2, No. 4 of the Forest Culture and Recreation Act. Available online: https://www.law.go.kr/LSW/lsInfoP.do?lsId=010004#J2:0 (accessed on 10 January 2022).
- Korea Forest Welfare Institute. Forest Therapy. Available online: https://www.fowi.or.kr/user/contents/contentsView.do?cntntsId=39 (accessed on 10 January 2022).
- Hong, J.; Park, S.; Lee, J. Changes in Depression and Stress of the Middle-Aged and Older through Participation in a Forest Therapy Program for Dementia Prevention. J. People Plants Environ. 2019, 22, 699–709. [Google Scholar] [CrossRef]
- Kobayashi, H.; Song, C.; Ikei, H.; Park, B.-J.; Lee, J.; Kagawa, T.; Miyazaki, Y. Population-Based Study on the Effect of a Forest Environment on Salivary Cortisol Concentration. Int. J. Environ. Res. Public Health 2017, 14, 931. [Google Scholar] [CrossRef]
- Ochiai, H.; Ikei, H.; Song, C.; Kobayashi, M.; Miura, T.; Kagawa, T.; Li, Q.; Kumeda, S.; Imai, M.; Miyazaki, Y. Physiological and Psychological Effects of a Forest Therapy Program on Middle-Aged Females. Int. J. Environ. Res. Public Health 2015, 12, 15222–15232. [Google Scholar] [CrossRef]
- Ochiai, H.; Ikei, H.; Song, C.; Kobayashi, M.; Takamatsu, A.; Miura, T.; Kagawa, T.; Li, Q.; Kumeda, S.; Imai, M.; et al. Physiological and Psychological Effects of Forest Therapy on Middle-Aged Males with High-Normal Blood Pressure. Int. J. Environ. Res. Public Health 2015, 12, 2532–2542. [Google Scholar] [CrossRef]
- Song, C.; Ikei, H.; Kobayashi, M.; Miura, T.; Taue, M.; Kagawa, T.; Li, Q.; Kumeda, S.; Imai, M.; Miyazaki, Y. Effect of Forest Walking on Autonomic Nervous System Activity in Middle-Aged Hypertensive Individuals: A Pilot Study. Int. J. Environ. Res. Public Health 2015, 12, 2687–2699. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.-Y.; Lee, D.-C. Cardiac and Pulmonary Benefits of Forest Walking versus City Walking in Elderly Women: A Randomised, Controlled, Open-Label Trial. Eur. J. Integr. Med. 2014, 6, 5–11. [Google Scholar] [CrossRef]
- Kim, J.Y.; Shin, C.S.; Lee, J.K. The Effects of Forest Healing Program on Mental Health and Melatonin of the Elderly in the Urban Forest. J. Korea Soc. Plants People Environ. 2017, 20, 95–106. [Google Scholar] [CrossRef]
- Zaudig, M. A New Systematic Method of Measurement and Diagnosis of “Mild Cognitive Impairment” and Dementia According to ICD-10 and DSM-III-R Criteria. Int. Psychogeriatr. 1992, 4, 203–219. [Google Scholar] [CrossRef] [PubMed]
- Park, J.H.; Park, S.H.; Lee, H.J.; Kang, J.W.; Lee, K.M.; Yeon, P.S. Study on NVOCs Concentration Characteristics by Season, Time and Climatic Factors: Focused on Pinus Densiflora Forest in National Center for Forest Therapy. J. People Plants Environ. 2018, 21, 403–409. [Google Scholar] [CrossRef]
- Kim, J.M.; Shin, I.S.; Yoon, J.S.; Lee, H.Y. Comparison of diagnostic validities between MMSE-K and K-MMSE for screening of dementia. J. Korean Neuropsychiatr. Assoc. 2003, 42, 124–130. [Google Scholar] [CrossRef]
- Song, Y.M.; Lee, H.K.; Kim, J.W.; Lee, K. Reliability and validity of the Korean Version of Beck Depression Inventory-II via the internet: Results from a university student sample. J. Korean Neuropsychiatr. Assoc. 2012, 51, 402–408. [Google Scholar] [CrossRef]
- Kim, E.J.; Lee, S.I.; Jeong, D.U.; Shin, M.S.; Yoon, I.Y. Standardization and reliability and validity of the Korean edition of Profile of Mood States (K-POMS). Sleep Med. Psychophysiol. 2003, 10, 39–51. [Google Scholar]
- Min, S.K.; Lee, C.I.; Kim, K.I.; Suh, S.Y.; Kim, D.K. Development of Korean version of WHO quality of life scale abbreviated version (WHOQOL-BREF). J. Korean Neuropsychiatr. Assoc. 2000, 39, 571–579. [Google Scholar]
- Sohn, S.I.; Kim, D.H.; Lee, M.Y.; Cho, Y.W. The Reliability and Validity of the Korean Version of the Pittsburgh Sleep Quality Index. Sleep Breath. 2012, 16, 803–812. [Google Scholar] [CrossRef]
- Kim, B.; Kang, S. Regular Leisure-Time Physical Activity Is Effective in Boosting Neurotrophic Factors and Alleviating Menopause Symptoms. Int. J. Environ. Res. Public Health 2020, 17, 8624. [Google Scholar] [CrossRef] [PubMed]
- Nobari, H.; Kargarfard, M.; Minasian, V.; Cholewa, J.M.; Pérez-Gómez, J. The Effects of 14-Week Betaine Supplementation on Endocrine Markers, Body Composition and Anthropometrics in Professional Youth Soccer Players: A Double Blind, Randomized, Placebo-Controlled Trial. J. Int. Soc. Sports Nutr. 2021, 18, 20. [Google Scholar] [CrossRef] [PubMed]
- Widmer, I.E.; Puder, J.J.; König, C.; Pargger, H.; Zerkowski, H.R.; Girard, J.; Müller, B. Cortisol Response in Relation to the Severity of Stress and Illness. J. Clin. Endocrinol. Metab. 2005, 90, 4579–4586. [Google Scholar] [CrossRef] [PubMed]
- Hapuarachchi, J.R.; Chalmers, A.H.; Winefield, A.H.; Blake-Mortimer, J.S. Changes in Clinically Relevant Metabolites with Psychological Stress Parameters. Behav. Med. 2003, 29, 52–59. [Google Scholar] [CrossRef] [PubMed]
- Jeon, S.; Kim, J. Effects of Augmented-Reality-Based Exercise on Muscle Parameters, Physical Performance, and Exercise Self-Efficacy for Older Adults. Int. J. Environ. Res. Public Health 2020, 17, 3260. [Google Scholar] [CrossRef]
- Hesseberg, K.; Bentzen, H.; Bergland, A. Reliability of the Senior Fitness Test in Community-Dwelling Older People with Cognitive Impairment. Physiother. Res. Int. 2015, 20, 37–44. [Google Scholar] [CrossRef]
- Bohannon, R.W. Test-Retest Reliability of Hand-Held Dynamometry during a Single Session of Strength Assessment. Phys. Ther. 1986, 66, 206–209. [Google Scholar] [CrossRef]
- Lindstrom-Hazel, D.; Kratt, A.; Bix, L. Interrater Reliability of Students Using Hand and Pinch Dynamometers. Am. J. Occup. Ther. 2009, 63, 193–197. [Google Scholar] [CrossRef]
- Van Uden, C.J.; Besser, M.P. Test-Retest Reliability of Temporal and Spatial Gait Characteristics Measured with an Instrumented Walkway System (GAITRite®). BMC Musculoskelet. Disord. 2004, 5, 13. [Google Scholar] [CrossRef]
- Swanenburg, J.; de Bruin, E.D.; Favero, K.; Uebelhart, D.; Mulder, T. The Reliability of Postural Balance Measures in Single and Dual Tasking in Elderly Fallers and Non-Fallers. BMC Musculoskelet. Disord. 2008, 9, 162. [Google Scholar] [CrossRef]
- Thompson, M.; Medley, A. Forward and Lateral Sitting Functional Reach in Younger, Middle-Aged, and Older Adults. J. Geriatr. Phys. Ther. 2007, 30, 43–48. [Google Scholar] [CrossRef] [PubMed]
- Yu, C.-P.; Hsieh, H. Beyond Restorative Benefits: Evaluating the Effect of Forest Therapy on Creativity. Urban For. Urban Green. 2020, 51, 126670. [Google Scholar] [CrossRef]
- Gurland, B. The Impact of Depression on Quality of Life of the Elderly. Clin. Geriatr. Med. 1992, 8, 377–386. [Google Scholar] [CrossRef]
- Kim, H.; Lee, Y.W.; Ju, H.J.; Jang, B.J.; Kim, Y.I. An Exploratory Study on the Effects of Forest Therapy on Sleep Quality in Patients with Gastrointestinal Tract Cancers. Int. J. Environ. Res. Public Health 2019, 16, 2449. [Google Scholar] [CrossRef]
- Tyrovolas, S.; Koyanagi, A.; Olaya, B.; Ayuso-Mateos, J.L.; Miret, M.; Chatterji, S.; Tobiasz-Adamczyk, B.; Koskinen, S.; Leonardi, M.; Haro, J.M. Factors Associated with Skeletal Muscle Mass, Sarcopenia, and Sarcopenic Obesity in Older Adults: A Multi-Continent Study. J. Cachexia Sarcopenia Muscle 2016, 7, 312–321. [Google Scholar] [CrossRef]
- Erickson, K.I.; Hillman, C.H.; Kramer, A.F. Physical Activity, Brain, and Cognition. Curr. Opin. Behav. Sci. 2015, 4, 27–32. [Google Scholar] [CrossRef]
- Kobayashi, H.; Song, C.; Ikei, H.; Park, B.-J.; Lee, J.; Kagawa, T.; Miyazaki, Y. Forest Walking Affects Autonomic Nervous Activity: A Population-Based Study. Front. Public Health 2018, 6, 278. [Google Scholar] [CrossRef]
- Taha, M.M.; Mounir, K.M. Acute Response of Serum Cortisol to Different Intensities of Resisted Exercise in the Elderly. Bull. Fac. Phys. Ther. 2019, 24, 20–25. [Google Scholar] [CrossRef]
- World Health Organization. Physical Activity. Available online: https://www.who.int/news-room/fact-sheets/detail/physical-activity (accessed on 10 January 2022).
- Kozakai, R.; Doyo, W.; Tsuzuku, S.; Yabe, K.; Miyamura, M.; Ikegami, Y.; Niino, N.; Ando, F.; Shimokata, H. Relationships of Muscle Strength and Power with Leisure-Time Physical Activity and Adolescent Exercise in Middle-Aged and Elderly Japanese Women. Geriatr. Gerontol. Int. 2005, 5, 182–188. [Google Scholar] [CrossRef]
- Prossegger, J.; Huber, D.; Grafetstätter, C.; Pichler, C.; Weisböck-Erdheim, R.; Iglseder, B.; Wewerka, G.; Hartl, A. Effects of Moderate Mountain Hiking and Balneotherapy on Community-Dwelling Older People: A Randomized Controlled Trial. Exp. Gerontol. 2019, 122, 74–84. [Google Scholar] [CrossRef]
- Antonelli, M.; Donelli, D.; Barbieri, G.; Valussi, M.; Maggini, V.; Firenzuoli, F. Forest Volatile Organic Compounds and Their Effects on Human Health: A State-of-the-Art Review. Int. J. Environ. Res. Public Health 2020, 17, 6506. [Google Scholar] [CrossRef] [PubMed]

| Date | Time | Program | Place |
|---|---|---|---|
| 1 day | 12:00–13:00 | Lunch | Cafeteria |
| 13:00–14:00 | Orientation | Auditorium | |
| 14:00–14:30 | Warm-up for the brain and body | Forest | |
| 14:30–15:00 | Move to the place | ||
| 15:00–16:00 | Memorization training or Calculation training | Forest | |
| 16:00–17:00 | Recreational exercise | Forest | |
| 17:00–18:00 | Move to the place | ||
| 18:00–19:00 | Dinner | Cafeteria | |
| 19:00–20:00 | Eating meditation or Walking meditation | Wood cabin | |
| 20:00–20:20 | Sharing thoughts | Wood cabin | |
| 2 day | 08:00–09:00 | Breakfast | Cafeteria |
| 09:00–09:30 | Warm-up for the brain and body | Forest | |
| 09:30–10:00 | Move to the place | ||
| 10:00–11:00 | Association training or Retrieval training | Forest | |
| 11:00–12:00 | Recreational exercise | Forest | |
| 12:00–12:20 | Sharing thoughts | Wood cabin | |
| 12:20– | Lunch | Cafeteria |
| Program | Description |
|---|---|
| Warm-up for the brain and body | Warm-up of light movements to activate the body and brain |
| Memorization training | Activities to observe and memorize kinds of natural objects while walking in the forest |
| Association training | Memorizing and associating milestones in the forest to create a story |
| Calculation training | Brain activation through mental arithmetic activities through understanding and memorizing tree types |
| Retrieval training | Activities to remember yesterday, today, and last week and express emotions through pictures or words |
| Recreational exercise | Stimulation of extremities of the body, promotion of blood circulation through stretching and strength exercise, improvement of exercise capacity |
| Eating meditation and tea meditation | Sensory activities focusing on movements and senses that occur when eating help stabilize the mind and body Eating nuts that are good for brain health (nutrition) |
| Sensory activities focusing on movements and senses that occur when drinking tea help stabilize the mind and body Chrysanthemum tea to help calm the mind and body (nutrition) | |
| Walking meditation | Focus on walking on forest paths, which stabilizes emotions and improves immunity |
| Sharing thoughts | Communicate and empathize with participants Mind and body stabilization through breathing meditation |
| Variables | Mean ± SD |
|---|---|
| Age (y) | 61.90 ± 1.14 |
| Male/Female (n) | 7/15 |
| Height (cm) | 157.10 ± 7.18 |
| Weight (kg) | 59.54 ± 10.19 |
| BMI (kg/m2) | 24.02 ± 2.93 |
| MMSE (score) | 26.64 ± 0.79 |
| BDI (score) | 8.68 ± 5.69 |
| Variables | Pre | Post | Follow-Up | p-Value | Post Hoc | ||
|---|---|---|---|---|---|---|---|
| Pre vs. Post | Pre vs. Follow-Up | Post vs. Follow-Up | |||||
| MMSE (score) | 26.64 ± 0.79 | 28.00 ± 1.27 | 27.14 ± 0.83 | <0.001 † | 0.001 † | 0.022 | 0.001 † |
| BDI (score) | 8.36 ± 5.12 | 6.77 ± 4.47 | 6.14 ± 4.38 | 0.013 * | 0.034 * | 0.049* | 0.777 |
| POMS (score) | |||||||
| Tension-anxiety | 8.73 ± 4.10 | 7.09 ± 4.53 | 7.36 ± 3.98 | 0.208 | - | - | - |
| Depression-dejection | 12.27 ± 9.64 | 7.59 ± 7.32 | 7.64 ± 7.45 | 0.001 † | 0.002† | 0.006 † | 0.896 |
| Anger-hostility | 7.00 ± 5.85 | 5.00 ± 5.62 | 4.41 ± 5.05 | 0.007 † | 0.086 | 0.001 † | 0.420 |
| Fatigue-inertia | 7.36 ± 4.93 | 5.59 ± 4.24 | 5.27 ± 4.03 | 0.001 * | 0.021* | 0.009 * | 1.000 |
| Confusion-bewilderment | 8.23 ± 4.02 | 7.18 ± 3.39 | 7.32 ± 3.90 | 0.181 | - | - | - |
| Vigor-activity | 18.41 ± 6.08 | 19.59 ± 4.70 | 18.45 ± 5.02 | 0.058 | - | - | - |
| Total mood disturbance | 25.18 ± 24.86 | 12.86 ± 22.67 | 13.55 ± 21.79 | 0.001 † | 0.002 † | 0.003 † | 0.637 |
| WHOQOL-BREF (score) | |||||||
| Overall QOL and general health | 6.45 ± 1.26 | 6.82 ± 1.37 | 6.95 ± 1.25 | 0.036 † | 0.059 | 0.012 † | 0.512 |
| Physical health | 23.18 ± 4.00 | 24.00 ± 3.65 | 24.77 ± 4.01 | 0.013 * | 0.358 | 0.036 * | 0.283 |
| Psychological | 18.23 ± 3.05 | 18.68 ± 3.50 | 19.36 ± 3.67 | 0.761 | - | - | - |
| Social relationship | 9.09 ± 1.15 | 10.00 ± 1.60 | 9.77 ± 1.57 | 0.007 † | 0.003 † | 0.030 | 0.364 |
| Environmental | 24.68 ± 4.70 | 25.00 ± 5.59 | 25.64 ± 5.18 | 0.447 | - | - | - |
| Total | 81.64 ± 12.45 | 84.50 ± 13.36 | 86.50 ± 14.11 | 0.400 | - | - | - |
| PSQI (score) | |||||||
| Sleep quality | 1.23 ± 0.61 | 0.95 ± 0.58 | 1.09 ± 0.68 | 0.118 | - | - | - |
| Sleep latency | 1.45 ± 0.80 | 1.55 ± 1.06 | 1.36 ± 1.05 | 0.402 | - | - | - |
| Sleep duration | 0.41 ± 0.67 | 0.32 ± 0.65 | 0.18 ± 0.39 | 0.174 | - | - | - |
| Habitual sleep efficiency | 0.36 ± 0.85 | 0.09 ± 0.29 | 0.23 ± 0.69 | 0.074 | - | - | - |
| Sleep disturbance | 1.32 ± 0.57 | 1.18 ± 0.39 | 1.18 ± 0.39 | 0.325 | - | - | - |
| Use of sleeping medication | 0.23 ± 0.69 | 0.09 ± 0.43 | 0.00 ± 0.00 | 0.061 | - | - | - |
| Daytime dysfunction | 1.45 ± 0.74 | 1.45 ± 0.91 | 1.27 ± 0.94 | 0.328 | - | - | - |
| Total | 6.45 ± 3.04 | 5.64 ± 2.46 | 5.32 ± 2.15 | 0.022 * | 0.076 | 0.047* | 1.000 |
| Variables | Pre | Post | Follow-Up | p-Value | Post Hoc | ||
|---|---|---|---|---|---|---|---|
| Pre vs. Post | Pre vs. Follow-Up | Post vs. Follow-Up | |||||
| Vital signs | |||||||
| Systolic pressure (mmHg) | 128.55 ± 12.63 | 129.77 ± 14.05 | 124.14 ± 18.42 | 0.074 | |||
| Diastolic pressure (mmHg) | 74.59 ± 7.59 | 77.23 ± 9.97 | 74.05 ± 11.86 | 0.072 | |||
| Pulse pressure (mmHg) | 53.95 ± 8.39 | 52.55 ± 7.29 | 50.09 ± 8.27 | 0.070 | |||
| Heart rate (bpm) | 73.55 ± 11.71 | 74.00 ± 7.93 | 74.91 ± 8.05 | 0.601 | |||
| Body compositions | |||||||
| Skeletal muscle mass (kg) | 23.15 ± 4.03 | 23.81 ± 4.44 | 23.17 ± 4.35 | 0.002 † | 0.001 † | 0.845 | 0.001 † |
| Body fat mass (kg) | 19.12 ± 3.61 | 16.88 ± 3.63 | 19.06 ± 3.77 | <0.001 † | <0.001 † | 0.709 | <0.001 † |
| Total body water (L) | 30.55 ± 5.18 | 31.35 ± 5.68 | 30.59 ± 5.56 | 0.010 † | 0.003 † | 0.935 | 0.005 † |
| Blood compositions | |||||||
| Cathepsin-B (pg/mL) | 183497.71 ± 71436.06 | 184544.84 ± 105302.59 | - | 0.189 | - | - | - |
| Cortisol (μg/dL) | 13.04 ± 3.31 | 7.01 ± 2.56 | - | < 0.001 † | - | - | - |
| IGF-1 (ng/mL) | 121.40 ± 32.78 | 124.43 ± 29.00 | - | 0.390 | - | - | - |
| CRP (mg/L) | 1.07 ± 0.87 | 0.88 ± 0.74 | - | 0.073 | - | - | - |
| Variables | Pre | Post | Follow-Up | p-Value | Post Hoc | ||
|---|---|---|---|---|---|---|---|
| Pre vs. Post | Pre vs. Follow-Up | Post vs. Follow-Up | |||||
| Senior Fitness Test | - | - | - | ||||
| Arm curl (n) | 17.68 ± 4.06 | 24.68 ± 4.89 | 25.14 ± 5.06 | <0.001 * | <0.001 * | <0.001 * | 0.874 |
| 30-sec chair stand (n) | 11.73 ± 3.71 | 16.95 ± 3.58 | 17.55 ± 3.35 | <0.001 * | <0.001 * | <0.001 * | 0.290 |
| 2-min step walk (n) | 92.50 ± 12.63 | 111.95 ± 12.89 | 114.00 ± 12.59 | <0.001 * | <0.001 * | <0.001 * | 1.000 |
| 8-ft up and go (sec) | 7.71 ± 1.13 | 6.64 ± 0.88 | 6.57 ± 0.73 | <0.001 † | <0.001 † | <0.001† | 0.548 |
| Back scratch (cm) | −8.50 ± 10.81 | −8.05 ± 11.00 | −7.32 ± 10.77 | 0.123 | |||
| Chair sit and reach (cm) | 13.09 ± 6.41 | 13.59 ± 9.29 | 15.27 ± 8.42 | 0.354 | |||
| Muscle strength (kg) | |||||||
| Elbow flexor (kg) | 11.35 ± 3.61 | 15.60 ± 4.83 | 16.61 ± 4.75 | <0.001 * | <0.001 * | <0.001 * | 0.433 |
| Knee extensor (kg) | 13.01 ± 1.85 | 14.21 ± 2.24 | 15.41 ± 2.48 | <0.001 * | 0.010 | <0.001 * | 0.114 |
| Ankle plantar flexor (kg) | 13.16 ± 2.08 | 14.14 ± 1.62 | 13.50 ± 2.13 | 0.042 * | 0.014 | 1.000 | 0.285 |
| Grip (kg) | 25.52 ± 7.18 | 26.22 ± 6.96 | 26.45 ± 7.13 | 0.151 | |||
| Pinch (kg) | 7.12 ± 1.46 | 7.34 ± 1.51 | 7.35 ± 1.70 | 0.409 | |||
| Spatiotemporal parameter of gait | |||||||
| Velocity (cm/s) | 121.02 ± 16.19 | 128.96 ± 15.19 | 127.04 ± 16.21 | 0.002 * | 0.001 * | 0.099 | 1.000 |
| Cadence (steps/min) | 119.99 ± 10.08 | 124.33 ± 9.95 | 123.71 ± 10.81 | 0.013 † | 0.001 † | 0.035 | 0.144 |
| Step length—Rt. (cm) | 61.03 ± 5.14 | 63.47 ± 4.95 | 61.39 ± 5.48 | 0.002 * | 0.002 * | 1.000 | 0.007* |
| Stride length—Rt. (cm) | 121.06 ± 10.29 | 126.65 ± 9.65 | 123.39 ± 10.75 | 0.001 * | 0.001 * | 0.566 | 0.031 * |
| Step time—Rt. (sec) | 0.50 ± 0.05 | 0.48 ± 0.04 | 0.49 ± 0.04 | 0.001 † | < 0.001 † | 0.054 | 0.205 |
| Swing time—Rt. (sec) | 0.38 ± 0.03 | 0.37 ± 0.03 | 0.37 ± 0.03 | 0.001 * | 0.004 * | 0.030 * | 1.000 |
| Stance time—Rt. (sec) | 0.62 ± 0.06 | 0.60 ± 0.06 | 0.60 ± 0.06 | 0.028 † | 0.004 † | 0.014 † | 0.673 |
| Cycle time—Rt. (sec) | 1.01 ± 0.09 | 0.97 ± 0.08 | 0.97 ± 0.08 | 0.025 † | 0.001 † | 0.049 | 0.217 |
| Static balance | |||||||
| EO—Sway area (mm2) | 1.47 ± 0.87 | 1.43 ± 0.99 | 1.45 ± 0.69 | 0.244 | |||
| EO—Sway velocity (mm/s) | 1.11 ± 0.29 | 1.14 ± 0.32 | 1.11 ± 0.18 | 0.811 | |||
| EC—Sway area (mm2) | 3.13 ± 3.43 | 2.64 ± 2.25 | 3.13 ± 3.42 | 0.727 | |||
| EC—Sway velocity (mm/s) | 1.80 ± 0.78 | 1.58 ± 0.57 | 1.75 ± 0.74 | 0.428 | |||
| Dynamic balance (cm) | |||||||
| Anterior | 49.41 ± 12.18 | 48.18 ± 8.27 | 51.82 ± 6.88 | 0.117 | |||
| Right | 32.25 ± 3.07 | 34.68 ± 3.72 | 34.45 ± 5.63 | 0.049 * | 0.012 | 0.265 | 1.000 |
| Left | 30.55 ± 5.46 | 33.41 ± 4.10 | 31.86 ± 5.63 | 0.026 * | 0.015 | 0.816 | 0.344 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baek, J.-E.; Jung, J.-H.; Shin, H.-J.; Kim, S.-H.; Sung, S.-Y.; Park, S.-J.; Hahm, S.-C.; Cho, H.-Y.; Lee, M.-G. Effects of Forest Healing Anti-Aging Program on Psychological, Physiological, and Physical Health of Older People with Mild Cognitive Impairment. Int. J. Environ. Res. Public Health 2022, 19, 4863. https://doi.org/10.3390/ijerph19084863
Baek J-E, Jung J-H, Shin H-J, Kim S-H, Sung S-Y, Park S-J, Hahm S-C, Cho H-Y, Lee M-G. Effects of Forest Healing Anti-Aging Program on Psychological, Physiological, and Physical Health of Older People with Mild Cognitive Impairment. International Journal of Environmental Research and Public Health. 2022; 19(8):4863. https://doi.org/10.3390/ijerph19084863
Chicago/Turabian StyleBaek, Ji-Eun, Jin-Hwa Jung, Ho-Jin Shin, Sung-Hyeon Kim, Si-Yoon Sung, Su-Jin Park, Suk-Chan Hahm, Hwi-Young Cho, and Min-Goo Lee. 2022. "Effects of Forest Healing Anti-Aging Program on Psychological, Physiological, and Physical Health of Older People with Mild Cognitive Impairment" International Journal of Environmental Research and Public Health 19, no. 8: 4863. https://doi.org/10.3390/ijerph19084863
APA StyleBaek, J.-E., Jung, J.-H., Shin, H.-J., Kim, S.-H., Sung, S.-Y., Park, S.-J., Hahm, S.-C., Cho, H.-Y., & Lee, M.-G. (2022). Effects of Forest Healing Anti-Aging Program on Psychological, Physiological, and Physical Health of Older People with Mild Cognitive Impairment. International Journal of Environmental Research and Public Health, 19(8), 4863. https://doi.org/10.3390/ijerph19084863