
Culture Requests and Multi-Drug Resistance among Suspected Urinary Tract Infections in Two Tertiary Hospitals in Freetown, Sierra Leone (2017–21): A Cross-Sectional Study

 , , , and
, , , and 
Abstract
1. Introduction
2. Material and Methods
2.1. Study Design
2.2. Setting
2.2.1. General Setting
2.2.2. Specific Setting
2.2.3. Bacteriological Procedures for Suspected Urinary Tract Infections
2.2.4. Routine Data Quality
2.3. Study Population and Period
2.4. Data Variables, Collection, and Source of Data
2.5. Analysis and Statistics
3. Results
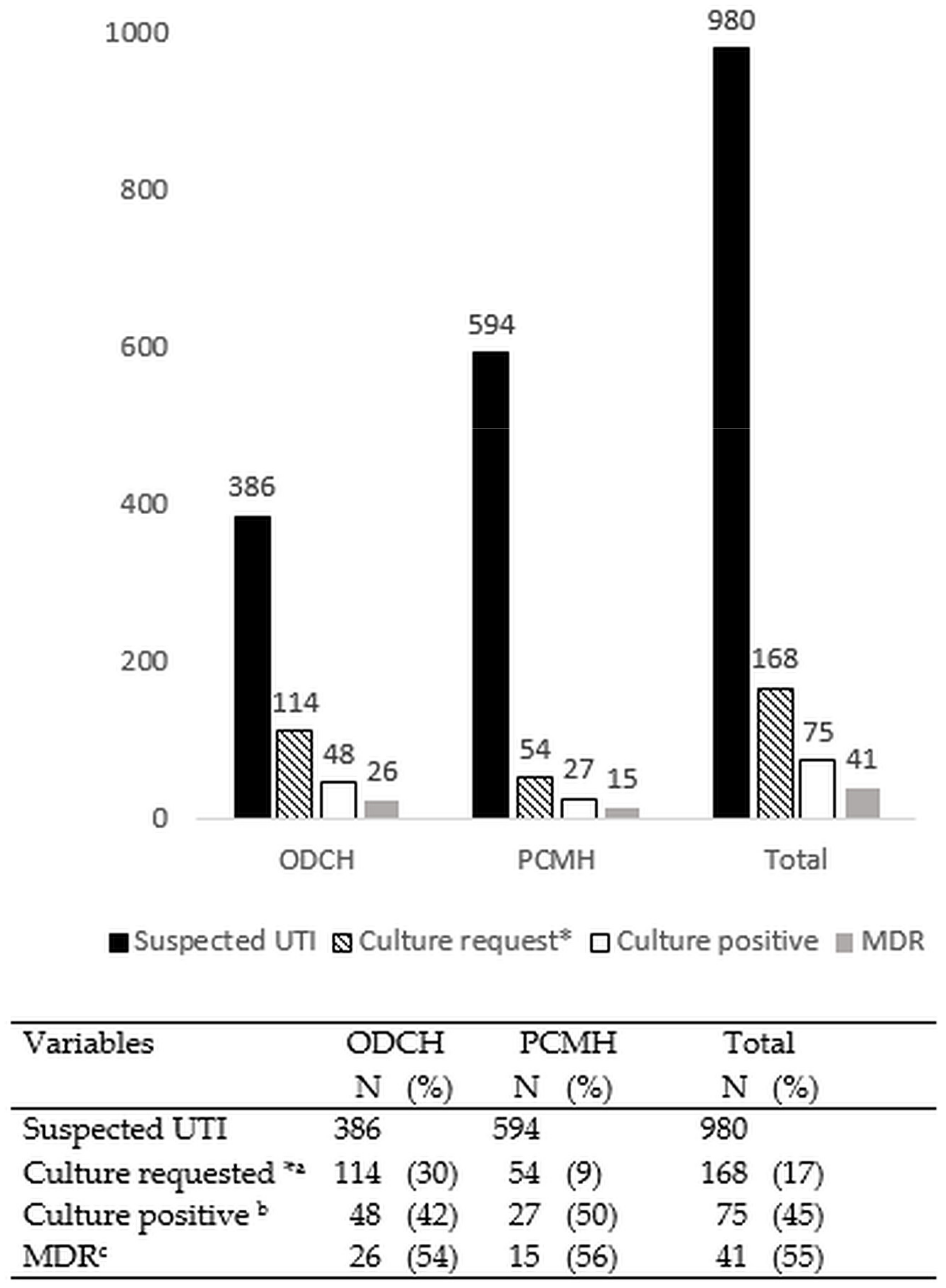
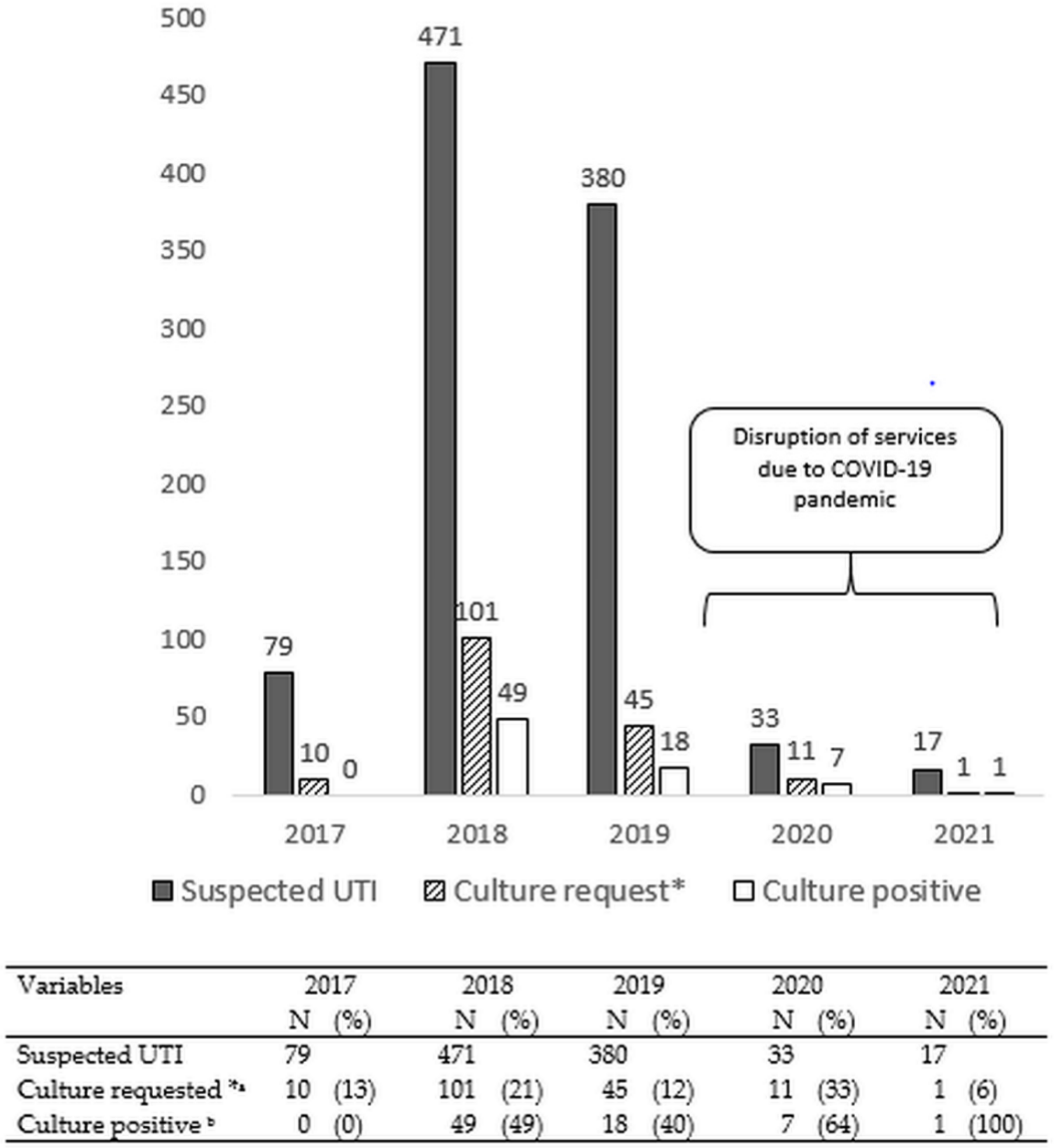
3.1. Urine Culture Requests and Culture Positivity
3.2. Bacterial Isolates and Their AMR Patterns
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Laxminarayan, R.; Matsoso, P.; Pant, S.; Brower, C.; Røttingen, J.A.; Klugman, K.; Davies, S. Access to effective antimicrobials: A worldwide challenge. Lancet 2016, 387, 168–175. [Google Scholar] [CrossRef]
- Lim, C.; Takahashi, E.; Hongsuwan, M.; Wuthiekanun, V.; Thamlikitkul, V.; Hinjoy, S.; Day, N.P.J.; Peacock, S.J.; Limmathurotsakul, D. Epidemiology and burden of multidrug-resistant bacterial infection in a developing country. eLife 2016, 5, e18082. [Google Scholar] [CrossRef] [PubMed]
- Stamm, W.E.; Norrby, S.R. Urinary tract infections: Disease panorama and challenges. J. Infect. Dis. 2001, 183, S1–S4. [Google Scholar] [CrossRef] [PubMed]
- Foxman, B. The epidemiology of urinary tract infection. Nat. Rev. Urol. 2010, 7, 653–660. [Google Scholar] [CrossRef] [PubMed]
- Gupta, K.; Hooton, T.M.; Naber, K.G.; Wullt, B.; Colgan, R.; Miller, L.G.; Moran, G.J.; Nicolle, L.E.; Raz, R.; Schaeffer, A.J.; et al. International Clinical Practice Guidelines for the Treatment of Acute Uncomplicated Cystitis and Pyelonephritis in Women: A 2010 Update by the Infectious Diseases Society of America and the European Society for Microbiology and Infectious Diseases. Clin. Infect. Dis. 2011, 52, e103–e120. [Google Scholar] [CrossRef]
- Hooton, T.M. Uncomplicated Urinary Tract Infection. N. Engl. J. Med. 2012, 366, 1028–1037. [Google Scholar] [CrossRef]
- Schito, G.C.; Naber, K.G.; Botto, H.; Palou, J.; Mazzei, T.; Gualco, L.; Marchese, A. The ARESC study: An international survey on the antimicrobial resistance of pathogens involved in uncomplicated urinary tract infections. Int. J. Antimicrob. Agents 2009, 34, 407–413. [Google Scholar] [CrossRef]
- Kengne, M.; Dounia, A.T.; Nwobegahay, J.M. Bacteriological profile and antimicrobial susceptibility patterns of urine culture isolates from patients in Ndjamena, Chad. Pan Afr. Med. J. 2017, 28, 258. [Google Scholar] [CrossRef]
- Tuem, K.B.; Desta, R.; Bitew, H.; Ibrahim, S.; Hishe, H.Z. Antimicrobial resistance patterns of uropathogens isolated between 2012 and 2017 from a tertiary hospital in Northern Ethiopia. J. Glob. Antimicrob. Resist. 2019, 18, 109–114. [Google Scholar] [CrossRef]
- Gambrah, E.; Owusu-Ofori, A.; Biney, E.; Oppong, C.; Coffin, S.E. Diagnosis and treatment of urinary tract infections in hospitalized adults in Ghana: The role of the clinical microbiology laboratory in improving antimicrobial stewardship. Int. J. Infect. Dis. 2021, 102, 497–500. [Google Scholar] [CrossRef]
- Leski, T.A.; Taitt, C.R.; Bangura, U.; Stockelman, M.G.; Ansumana, R.; Cooper, W.H.; Stenger, D.A.; Vora, G.J. High prevalence of multidrug resistant Enterobacteriaceae isolated from outpatient urine samples but not the hospital environment in Bo, Sierra Leone. BMC Infect. Dis. 2016, 16, 167. [Google Scholar] [CrossRef]
- Lakoh, S.; Li, L.; Sevalie, S.; Guo, X.; Adekanmbi, O.; Yang, G.; Adebayo, O.; Yi, L.; Coker, J.M.; Wang, S.; et al. Antibiotic resistance in patients with clinical features of healthcare-associated infections in an urban tertiary hospital in Sierra Leone: A cross-sectional study. Antimicrob. Resist. Infect. Control 2020, 9, 38. [Google Scholar] [CrossRef]
- World Health Organization (WHO) 2021 AWaRe Classification. WHO Access, Watch, Reserve, Classification of Antibiotics for Evaluation and Monitoring of Use. Available online: https://www.who.int/publications/i/item/2021-aware-classification (accessed on 31 January 2022).
- Statistics Sierra Leone. 2015 Population and Housing Census. Summary of Final Results; Statistics Sierra Leone: Freetown, Sierra Leone, 2015. [Google Scholar]
- Sierra Leone Ministry of Health and Sanitation. National Operational Handbook for Primary Health Care; Government of Sierra Leone: Freetown, Sierra Leone, 2004.
- Clinical and Laboratory Standards Institute (CLSI). Performance Standards for Antimicrobial Disk Susceptibility Tests, 13th ed.; Available online: https://clsi.org/standards/products/microbiology/documents/m02/ (accessed on 31 January 2022).
- Newman, M.J.; Frimpong, E.; Donkor, E.S.; Opintan, J.A.; Asamoah-Adu, A. Resistance to antimicrobial drugs in Ghana. Infect. Drug Resist. 2011, 4, 215–220. [Google Scholar] [CrossRef]
- Opintan, J.A.; Newman, M.J.; Arhin, R.E.; Donkor, E.S.; Gyansa-Lutterodt, M.; Mills-Pappoe, W. Laboratory-based nationwide surveillance of antimicrobial resistance in Ghana. Infect. Drug Resist. 2015, 8, 379–389. [Google Scholar] [CrossRef]
- Magiorakos, A.-P.; Srinivasan, A.; Carey, R.B.; Carmeli, Y.; Falagas, M.E.; Giske, C.G.; Harbarth, S.; Hindler, J.F.; Kahlmeter, G.; Olsson-Liljequist, B.; et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: An international expert proposal for interim standard definitions for acquired resistance. Clin. Microbiol. Infect. 2012, 18, 268–281. [Google Scholar] [CrossRef]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for reporting observational studies. Lancet 2007, 370, 1453–1457. [Google Scholar] [CrossRef]
- Bryce, A.; Hay, A.D.; Lane, I.F.; Thornton, H.V.; Wootton, M.; Costelloe, C. Global prevalence of antibiotic resistance in paediatric urinary tract infections caused by Escherichia coli and association with routine use of antibiotics in primary care: Systematic review and meta-analysis. BMJ 2016, 352, i939. [Google Scholar] [CrossRef]
- Dautt-Leyva, J.G.; Canizalez-Román, A.; Acosta Alfaro, L.F.; Gonzalez-Ibarra, F.; Murillo-Llanes, J. Maternal and perinatal complications in pregnant women with urinary tract infection caused by Escherichia coli. J. Obstet. Gynaecol. Res. 2018, 44, 1384–1390. [Google Scholar] [CrossRef]
- Mansouri, F.; Sheibani, H.; Javedani Masroor, M.; Afsharian, M. Extended-spectrum beta-lactamase (ESBL)-producing Enterobacteriaceae and urinary tract infections in pregnant/postpartum women: A systematic review and meta-analysis. Int. J. Clin. Pract. 2019, 73, e13422. [Google Scholar] [CrossRef]
- Ekeng, B.E.; Ochang, E.A.; Elem, D.E.; Owai, P.A.; Monjol, B.E.; Ukweh, I.H.; Nwagboso, C.I.; Abraka, B.A.; Ereh, S.E. Antibiotic Resistance Pattern of Uropathogens in a Tertiary Care Hospital in Calabar, Nigeria. Annu. Res. Rev. Biol. 2021, 36, 10–18. [Google Scholar] [CrossRef]
- Dougnon, V.; Assogba, P.; Gnimatin, J.P.; Agbankpé, J.; Koudokpon, H.; Déguénon, E.; Fabiyi, K.; Fagla, S.R.M.; Loko, Y.L.E.; Koukoui, O.; et al. Modeling the antimicrobial resistance of enterobacteria responsible for Urinary Tract Infections in Benin: Another way to control Antimicrobial Resistance. Res. Squ. 2020. [Google Scholar] [CrossRef]
- Alechenu, E.C.; Nweze, J.A.; Lerum, N.I.; Aniebonam Eze, E. Prevalence and Antibiotic Resistance Patterns of Gram-Negative Uropathogens among Paediatric Patients in Nigeria. Open J. Med. Microbiol. 2019, 9, 215–229. [Google Scholar] [CrossRef][Green Version]
- Negeri, A.A.; Ibrahim, R.; Asamene, N.; Dinku, S.F. Bacteriological profile and antibiotic resistance pattern of urinary tract pathogens isolated at national reference laboratory, Ethiopian Public Health Bacteriological profile and antibiotic resistance pattern of urinary tract pathogens isolated at Natio. Ethiop. J. Public Health Nutr. 2019, 2, 1–6. [Google Scholar]
- Odoki, M.; Almustapha Aliero, A.; Tibyangye, J.; Nyabayo Maniga, J.; Wampande, E.; Drago Kato, C.; Agwu, E.; Bazira, J. Prevalence of Bacterial Urinary Tract Infections and Associated Factors among Patients Attending Hospitals in Bushenyi District, Uganda. Int. J. Microbiol. 2019, 2019, 4246780. [Google Scholar] [CrossRef]
- Nji, C.P.; Nguedia Assob, J.C.; Kihla Akoachere, J.F.T. Predictors of urinary tract infections in children and antibiotic susceptibility pattern in the Buea Health district, South West Region, Cameroon. Biomed Res. Int. 2020, 2020, 2176569. [Google Scholar] [CrossRef]
- Koroma, Z.; Moses, F.; Delamou, A.; Hann, K.; Ali, E.; Kitutu, F.E.; Namugambe, J.S.; Harding, D.; Hermans, V.; Takarinda, K.; et al. High levels of antibiotic resistance patterns in two referral hospitals during the post-ebola era in free-town, sierra leone: 2017–2019. Trop. Med. Infect. Dis. 2021, 6, 103. [Google Scholar] [CrossRef]
- Derbie, A.; Hailu, D.; Mekonnen, D.; Abera, B.; Yitayew, G. Antibiogram profile of uropathogens isolated at bahir dar regional health research laboratory centre, northwest ethiopia. Pan Afr. Med. J. 2017, 26, 134. [Google Scholar] [CrossRef]
- Kotb, D.; Mahmoud, S.; Mahdi, W.; Khairy, R. Prevalence and Antimicrobial Resistance of Urinary Tract Infections in Upper Egypt. Malays. J. Med. Res. 2019, 30, 78–85. [Google Scholar]
- World Health Organizaton (WHO). Global Antimicrobial Resistance and Use Surveillance System (GLASS). Available online: https://www.who.int/initiatives/glass (accessed on 31 January 2022).
- Sirijatuphat, R.; Pongsuttiyakorn, S.; Supapueng, O.; Kiratisin, P.; Thamlikitkul, V. Implementation of global antimicrobial resistance surveillance system (GLASS) in patients with bacteriuria. J. Glob. Antimicrob. Resist. 2020, 20, 60–67. [Google Scholar] [CrossRef]
- Antimicrobial Resistance Collaborators. Global burden of bacterial antimicrobial resistance in 2019: A systematic analysis. Lancet 2022, 9, 114. [Google Scholar] [CrossRef]
- The Lancet. Antimicrobial resistance: Time to repurpose the Global Fund. Lancet 2022, 399, 335. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Isolates and Their Resistance Patterns | E. coli | K. pneumoniae | S. aureus | Pseudomonas spp. | Coliforms | Proteus mirabilis | Other * | Total | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n | (%) | n | (%) | n | (%) | n | (%) | n | (%) | n | (%) | n | (%) | n | (%) | |
| Total isolates | 36 | 10 | 9 | 6 | 4 | 3 | 7 | 75 | ||||||||
| Resistant to | ||||||||||||||||
| Cephalothin A | 5 | (14) | - | - | - | - | - | - | 1 | (25) | - | - | 3 | (43) | 9 | (12) |
| Gentamicin A | 3 | (8) | 1 | (10) | 2 | (22) | - | - | - | - | 2 | (67) | 3 | (43) | 11 | (15) |
| Ciprofloxacin Wa | 6 | (17) | 1 | (10) | - | - | - | - | - | - | 1 | (33) | 3 | (43) | 11 | (15) |
| Colistin Sulphate Re | 2 | (6) | - | - | 2 | (22) | - | - | 1 | (25) | - | - | 2 | (29) | 7 | (9) |
| Nalidixic acid | 15 | (42) | 2 | (20) | 4 | (44) | 1 | (17) | 1 | (25) | 3 | (100) | 7 | (100) | 33 | (44) |
| Nitrofurantoin A | 10 | (28) | 4 | (40) | - | - | 4 | (67) | 2 | (50) | 1 | (33) | 3 | (43) | 24 | (32) |
| TMP-SMX A | 17 | (47) | 4 | (40) | - | - | 3 | (50) | 4 | (100) | 2 | (67) | 5 | (71) | 35 | (47) |
| Cefotaxime Wa | 14 | (39) | 2 | (20) | 6 | (67) | 2 | (33) | - | - | - | - | 3 | (43) | 27 | (36) |
| Oxacillin A | - | - | - | - | - | - | - | - | - | - | - | - | 1 | (14) | 1 | (1) |
| Erythromycin Wa | - | - | - | - | - | - | - | - | - | - | - | - | 1 | (14) | 1 | (1) |
| Imipenem Wa | 3 | (8) | - | - | - | - | 2 | (33) | - | - | - | - | 1 | (14) | 6 | (8) |
| Multi-drug resistance | 21 | (58) | 2 | (20) | 4 | (44) | 3 | (50) | 1 | (25) | 3 | (100) | 7 | (100) | 41 | (55) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Campbell, J.S.O.; van Henten, S.; Koroma, Z.; Kamara, I.F.; Kamara, G.N.; Shewade, H.D.; Harries, A.D. Culture Requests and Multi-Drug Resistance among Suspected Urinary Tract Infections in Two Tertiary Hospitals in Freetown, Sierra Leone (2017–21): A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2022, 19, 4865. https://doi.org/10.3390/ijerph19084865
Campbell JSO, van Henten S, Koroma Z, Kamara IF, Kamara GN, Shewade HD, Harries AD. Culture Requests and Multi-Drug Resistance among Suspected Urinary Tract Infections in Two Tertiary Hospitals in Freetown, Sierra Leone (2017–21): A Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2022; 19(8):4865. https://doi.org/10.3390/ijerph19084865
Chicago/Turabian StyleCampbell, Julian S. O., Saskia van Henten, Zikan Koroma, Ibrahim Franklyn Kamara, Gladys N. Kamara, Hemant Deepak Shewade, and Anthony D. Harries. 2022. "Culture Requests and Multi-Drug Resistance among Suspected Urinary Tract Infections in Two Tertiary Hospitals in Freetown, Sierra Leone (2017–21): A Cross-Sectional Study" International Journal of Environmental Research and Public Health 19, no. 8: 4865. https://doi.org/10.3390/ijerph19084865
APA StyleCampbell, J. S. O., van Henten, S., Koroma, Z., Kamara, I. F., Kamara, G. N., Shewade, H. D., & Harries, A. D. (2022). Culture Requests and Multi-Drug Resistance among Suspected Urinary Tract Infections in Two Tertiary Hospitals in Freetown, Sierra Leone (2017–21): A Cross-Sectional Study. International Journal of Environmental Research and Public Health, 19(8), 4865. https://doi.org/10.3390/ijerph19084865