
Effect of High-Intensity Interval Training Combined with Fasting in the Treatment of Overweight and Obese Adults: A Systematic Review and Meta-Analysis


Abstract
:1. Introduction
2. Method
2.1. Inclusion and Exclusion Criteria
- (1)
- Participants: The participants were ≥18-year-old adults diagnosed with overweight or obesity. The definitions of overweight and obesity were based on age and sex-specific BMI cut-off points as indicated by WHO (overweight, ≥25 kg/m2; obesity, ≥30 kg/m2); age-incompatible, normal-weight adults, and animal-based subjects were excluded (considering that obese patients often have complications and some obesity is disease-caused, the participants with complications will also be included and illustrated in the results).
- (2)
- Intervention: Only participants who received HIIT + fasting were included in this study. HIIT intervention measures were used: the exercise intensity at 80 to 100% HRmax/peak oxygen consumption (VO2peak) for 30 s to 4 min, passive recovery, or low-intensity aerobic exercise in the intermittent period for a maximum of 4 min [31]. The frequency of HIIT was more than twice a week. Fasting programs involved different forms of fasting and energy-restricting diets (e.g., low-calorie diet (LCD), low-carbohydrate diet, intermittent fasting, and intermittent energy restriction) [32].
- (3)
- Study: Randomized controlled trials (RCT) were included.
- (4)
- Outcomes: Data types related to body composition, glucose metabolism, and cardiorespiratory fitness were included. Body composition: Body mass, BMI, WC were objectively measured on a digital scale, a stadiometer and a plastic tape (WC was measured 2 cm above the umbilicus). FM and fat-free mass (FFM) were measured on hydrostatic weighing, dual-energy X-ray absorptiometry (DXA), bioelectrical impedance analysis (BIA), computed tomography (CT), or magnetic resonance imaging (MRI) [33]. Percent fat mass (PFM) was measured indirectly. Cardiorespiratory fitness: VO2peak was assessed by a stepwise cardiopulmonary exercise test (CPET) by bicycle, a continuous incremental test on a cycle ergometer with indirect calorimetry, or the Vmax Encore System (CareFusion Corp., San Diego, CA, USA). Glucose metabolism: Fasting plasma glucose (FPG) was measured by a kit assay (Pointe Scientific, Canton, MI). Fasting glucose insulin (FPI) was analyzed by ELISA (ALPCO Immunoassays, Salem, NH, USA).
2.2. Literature Retrieval Strategy
2.3. Literature Selection
2.4. Data Extraction
2.5. Risk of Bias Assessment
2.6. Statistical Analysis
2.7. Certainty Assessment
3. Result
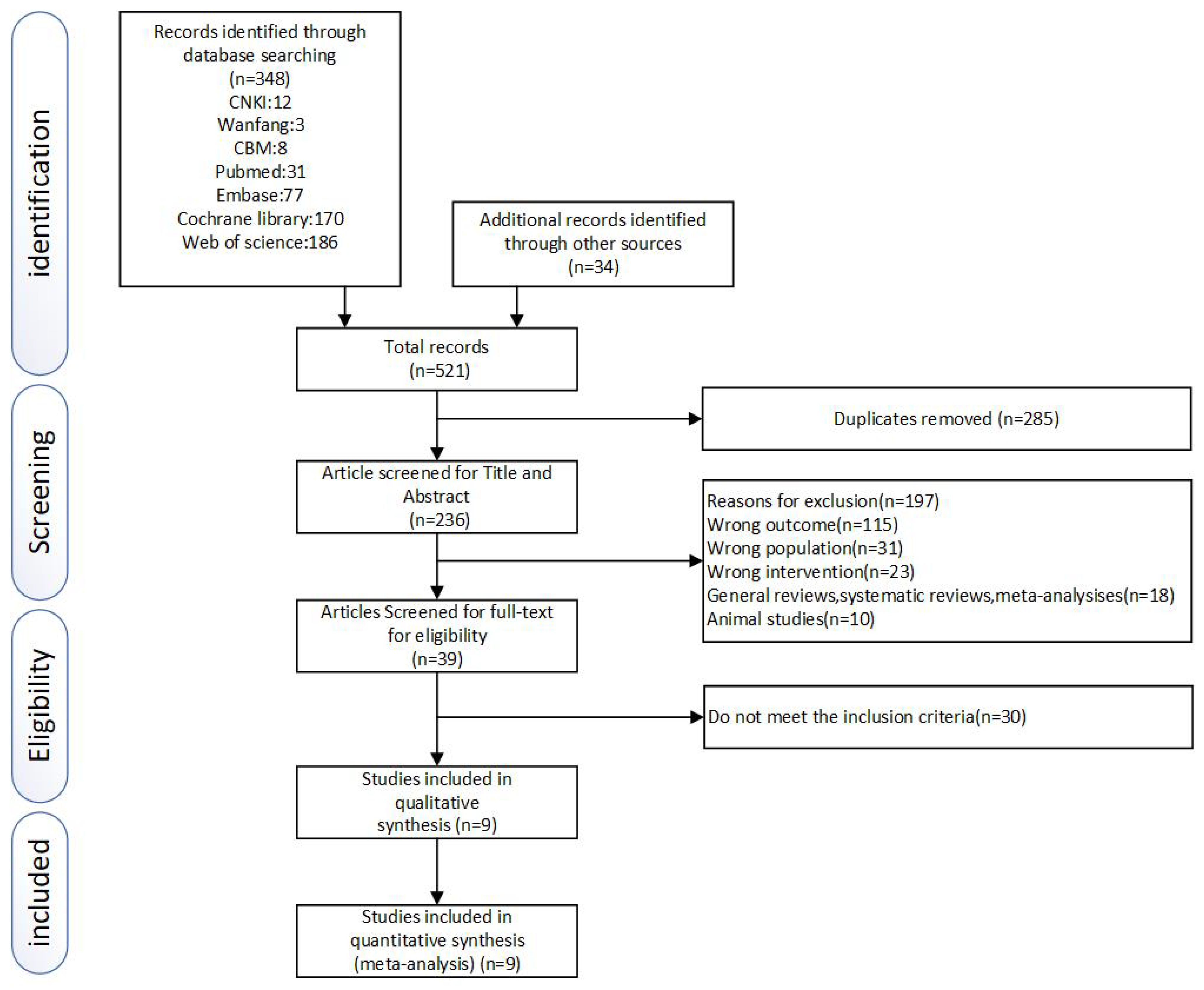
3.1. Study Identification and Selection
3.2. Characteristics of Included Studies and Participants
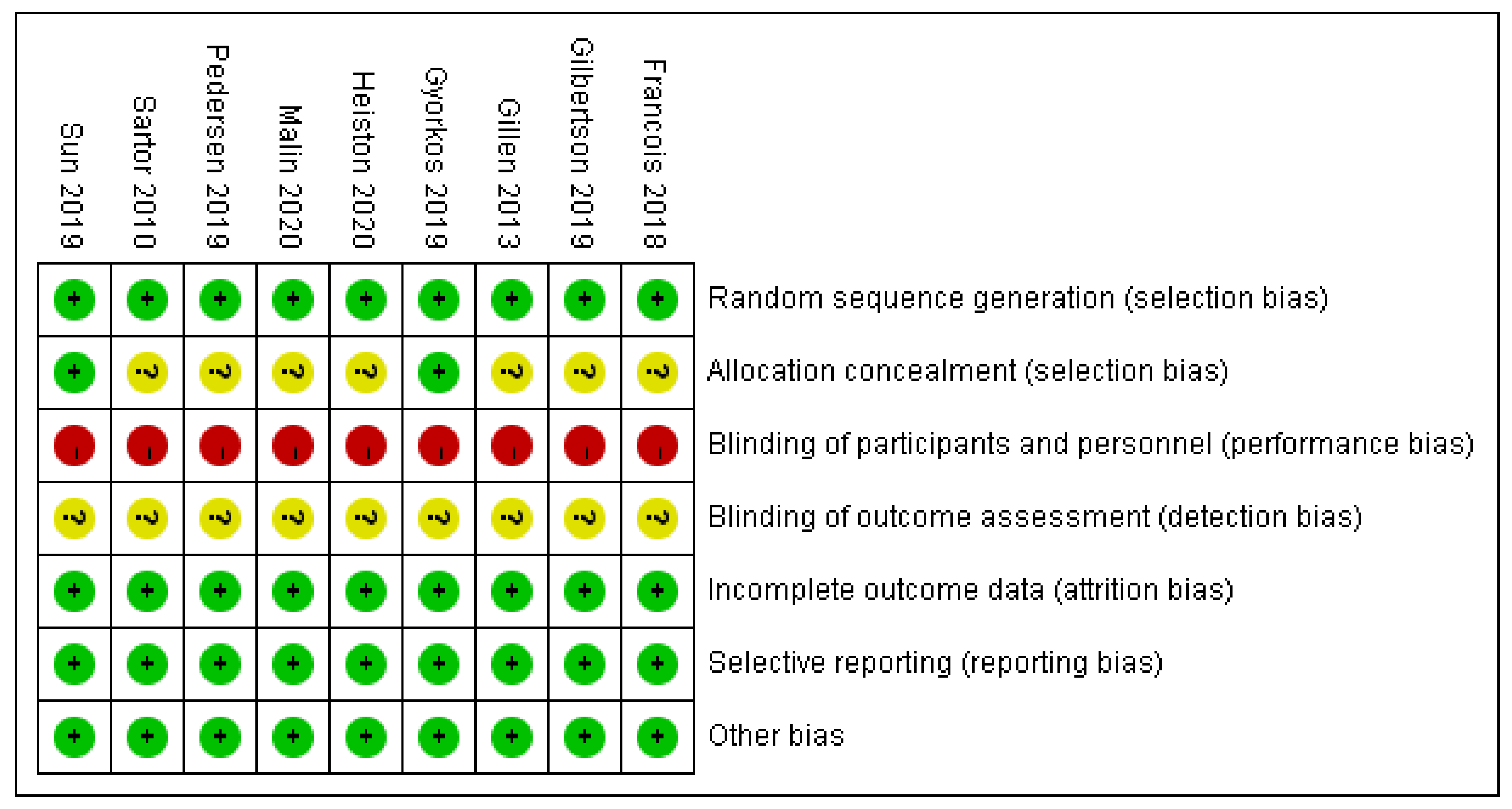
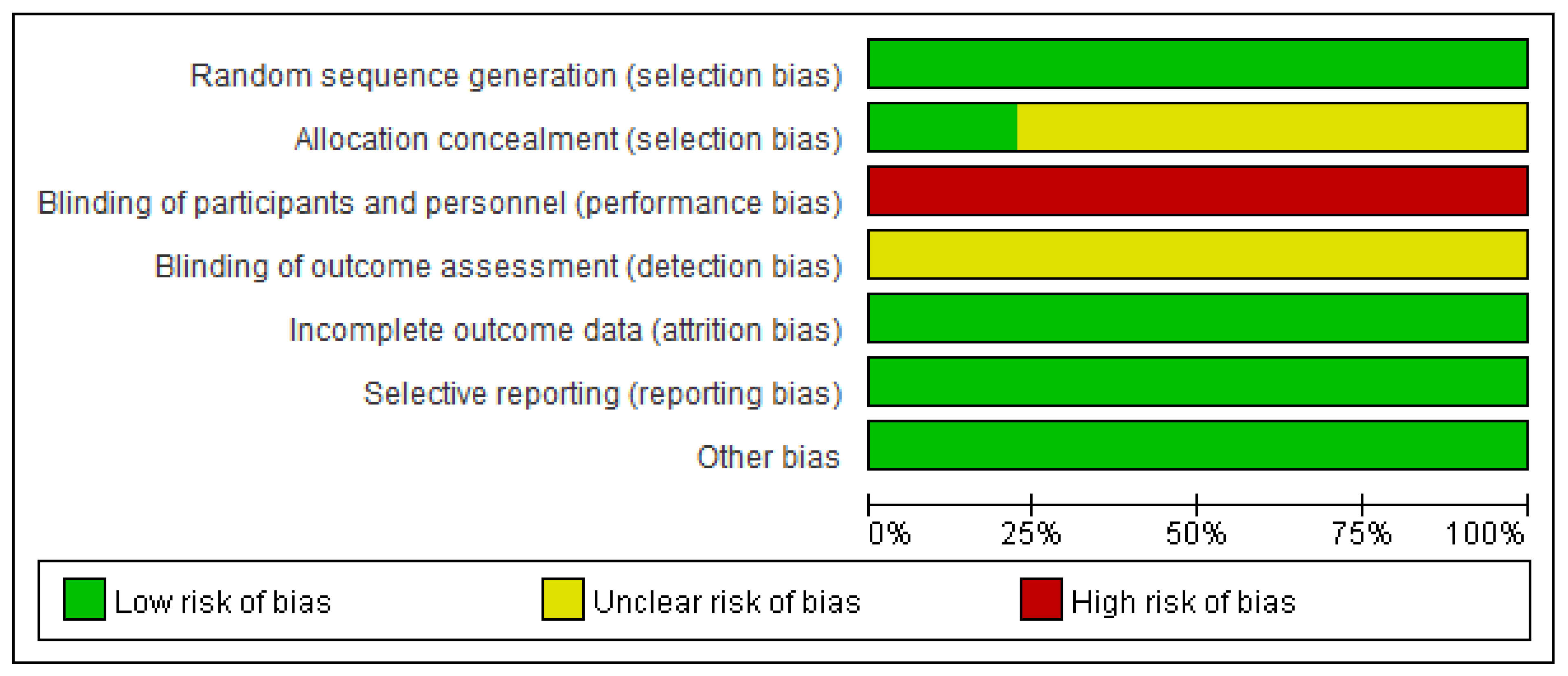
3.3. The Risk of Bias Assessment
3.4. Meta-Analysis
3.5. Subgroup Analysis
3.6. GRADE Assessment
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Piché, M.E.; Tchernof, A.; Després, J.P. Obesity Phenotypes, Diabetes, and Cardiovascular Diseases. Circ. Res. 2020, 126, 1477–1500. [Google Scholar] [CrossRef] [PubMed]
- Houghton, S.C.; Eliassen, H.; Tamimi, R.M.; Willett, W.C.; Rosner, B.A.; Hankinson, S.E. Central Adiposity and Subsequent Risk of Breast Cancer by Menopause Status. J. Natl. Cancer Inst. 2021, 113, 900–908. [Google Scholar] [CrossRef] [PubMed]
- Nemesure, B.; Wu, S.Y.; Hennis, A.; Leske, M.C. Prostate Cancer in a Black Population (PCBP) Study Group: Central adiposity and Prostate Cancer in a Black Population. Cancer Epidemiol. Biomark. Prev. 2012, 21, 851–858. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singh, S.; Sharma, A.N.; Murad, M.H.; Buttar, N.S.; El–Serag, H.B.; Katzka, D.A.; Iyer, P.G. Central adiposity is associated with increased risk of esophageal inflammation, metaplasia, and adenocarcinoma: A systematic review and meta-analysis. Clin. Gastroenterol. Hepatol. 2013, 1, 1399–1412.e7. [Google Scholar] [CrossRef] [Green Version]
- Chooi, Y.C.; Ding, C.; Magkos, F. The epidemiology of obesity. Metabolism 2019, 92, 6–10. [Google Scholar] [CrossRef] [Green Version]
- Upadhyay, J.; Farr, O.; Perakakis, N.; Ghaly, W.; Mantzoros, C. Obesity as a disease. Med. Clin. 2018, 102, 13–33. [Google Scholar] [CrossRef]
- Shaw, K.; Gennat, H.; O’Rourke, P.; Del Mar, C. Exercise for overweight or obesity. Cochrane Database Syst Rev. 2006, 4, CD003817. [Google Scholar] [CrossRef] [Green Version]
- Mora-Gonzalez, J.; Esteban-Cornejo, I.; Cadenas-Sanchez, C.; Migueles, J.H.; Molina-Garcia, P.; Rodriguez-Ayllon, M.; Henriksson, P.; Pontifex, M.B.; Catena, A.; Ortega, F.B. Physical Fitness, Physical Activity, and the Executive Function in Children with Overweight and Obesity. J. Pediatr. 2019, 208, 50–56.e1. [Google Scholar] [CrossRef]
- Gar, C.; Rottenkolber, M.; Haenelt, M.; Potzel, A.L.; Kern-Matschilles, S.; Then, C.; Seissler, J.; Bidlingmaier, M.; Lechner, A. Altered metabolic and hormonal responses to moderate exercise in overweight/obesity. Metabolism 2020, 107, 154219. [Google Scholar] [CrossRef]
- Verheggen, R.J.; Maessen, M.F.; Green, D.J.; Hermus, A.R.; Hopman, M.T.; Thijssen, D.H. A systematic review and meta-analysis on the effects of exercise training versus hypocaloric diet: Distinct effects on body weight and visceral adipose tissue. Obes. Rev. 2016, 17, 664–690. [Google Scholar] [CrossRef]
- Berge, J.; Hjelmesæth, J.; Hertel, J.K.; Gjevestad, E.; Småstuen, M.C.; Johnson, L.K.; Martins, C.; Andersen, E.; Helgerud, J.; Støren, Ø. Effect of Aerobic Exercise Intensity on Energy Expenditure and Weight Loss in Severe Obesity-A Randomized Controlled Trial. Obesity 2021, 29, 359–369. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.J.; He, J.; Pan, L.L.; Ma, Z.M.; Han, C.K.; Chen, C.S.; Chen, Z.; Han, H.W.; Chen, S.; Sun, Q.; et al. Effects of Moderate and Vigorous Exercise on Nonalcoholic Fatty Liver Disease: A Randomized Clinical Trial. JAMA Intern. Med. 2016, 176, 1074–1082. [Google Scholar] [CrossRef] [PubMed]
- Longo, V.D.; Mattson, M.P. Fasting: Molecular mechanisms and clinical applications. Cell Metab. 2014, 19, 181–192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Cabo, R.; Mattson, M.P. Effects of Intermittent Fasting on Health, Aging, and Disease. N. Engl. J. Med. 2020, 382, 978. [Google Scholar] [CrossRef] [PubMed]
- Marin-Alejandre, B.A.; Abete, I.; Cantero, I.; Monreal, J.I.; Elorz, M.; Herrero, J.I.; Benito-Boillos, A.; Quiroga, J.; Martinez-Echeverria, A.; Uriz-Otano, J.I.; et al. The Metabolic and Hepatic Impact of Two Personalized Dietary Strategies in Subjects with Obesity and Nonalcoholic Fatty Liver Disease: The Fatty Liver in Obesity (FLiO) Randomized Controlled Trial. Nutrients 2019, 11, 2543. [Google Scholar] [CrossRef] [Green Version]
- Zouhal, H.; Bagheri, R.; Ashtary-Larky, D.; Wong, A.; Triki, R.; Hackney, A.C.; Laher, I.; Abderrahman, A.B. Effects of Ramadan intermittent fasting on inflammatory and biochemical biomarkers in males with obesity. Physiol. Behav. 2020, 225, 113090. [Google Scholar] [CrossRef]
- Zouhal, H.; Bagheri, R.; Triki, R.; Saeidi, A.; Wong, A.; Hackney, A.C.; Laher, I.; Suzuki, K.; Ben Abderrahman, A. Effects of Ramadan Intermittent Fasting on Gut Hormones and Body Composition in Males with Obesity. Int. J. Environ. Res. Public Health 2020, 17, 5600. [Google Scholar] [CrossRef]
- Cho, A.R.; Moon, J.Y.; Kim, S.; An, K.Y.; Oh, M.; Jeon, J.Y.; Jung, D.H.; Choi, M.H.; Lee, J.W. Effects of alternate day fasting and exercise on cholesterol metabolism in overweight or obese adults: A pilot randomized controlled trial. Metabolism 2019, 93, 52–60. [Google Scholar] [CrossRef]
- Ho, M.; Garnett, S.P.; Baur, L.A.; Burrows, T.; Stewart, L.; Neve, M.; Collins, C. Impact of dietary and exercise interventions on weight change and metabolic outcomes in obese children and adolescents: A systematic review and meta-analysis of randomized trials. JAMA Pediatr. 2013, 167, 759–768. [Google Scholar] [CrossRef]
- Videira-Silva, A.; Hetherington-Rauth, M.; Sardinha, L.B.; Fonseca, H. Combined high-intensity interval training as an obesity-management strategy for adolescents. Eur. J. Sport Sci. 2021, 1–12. [Google Scholar] [CrossRef]
- García-Hermoso, A.; Cerrillo-Urbina, A.J.; Herrera-Valenzuela, T.; Cristi-Montero, C.; Saavedra, J.M.; Martínez-Vizcaíno, V. Is high-intensity interval training more effective on improving cardiometabolic risk and aerobic capacity than other forms of exercise in overweight and obese youth? A meta-analysis. Obes. Rev. 2016, 17, 531–540. [Google Scholar] [CrossRef] [PubMed]
- Wu, Z.J.; Wang, Z.Y.; Gao, H.E.; Zhou, X.F.; Li, F.H. Impact of high-intensity interval training on cardiorespiratory fitness, body composition, physical fitness, and metabolic parameters in older adults: A meta-analysis of randomized controlled trials. Exp. Gerontol. 2021, 150, 111345. [Google Scholar] [CrossRef] [PubMed]
- Maillard, F.; Pereira, B.; Boisseau, N. Effect of High-Intensity Interval Training on Total, Abdominal and Visceral Fat Mass: A Meta-Analysis. Sports Med. 2018, 48, 269–288. [Google Scholar] [CrossRef] [PubMed]
- Wewege, M.; van den Berg, R.; Ward, R.E.; Keech, A. The effects of high-intensity interval training vs. moderate-intensity continuous training on body composition in overweight and obese adults: A systematic review and meta-analysis. Obes. Rev. 2017, 18, 635–646. [Google Scholar] [CrossRef]
- Mattson, M.P.; Longo, V.D.; Harvie, M. Impact of intermittent fasting on health and disease processes. Ageing Res. Rev. 2017, 39, 46–58. [Google Scholar] [CrossRef] [PubMed]
- Choi, I.Y.; Piccio, L.; Childress, P.; Bollman, B.; Ghosh, A.; Brandhorst, S.; Suarez, J.; Michalsen, A.; Cross, A.H.; Morgan, T.E.; et al. A Diet Mimicking Fasting Promotes Regeneration and Reduces Autoimmunity and Multiple Sclerosis Symptoms. Cell Rep. 2016, 15, 2136–2146. [Google Scholar] [CrossRef] [Green Version]
- Johnstone, A. Fasting for weight loss: An effective strategy or latest dieting trend? Int. J. Obes. 2015, 39, 727–733. [Google Scholar] [CrossRef]
- Crupi, A.N.; Haase, J.; Brandhorst, S.; Longo, V.D. Periodic and Intermittent Fasting in Diabetes and Cardiovascular Disease. Curr. Diab. Rep. 2020, 20, 83. [Google Scholar] [CrossRef]
- Park, J.; Seo, Y.G.; Paek, Y.J.; Song, H.J.; Park, K.H.; Noh, H.M. Effect of alternate-day fasting on obesity and cardiometabolic risk: A systematic review and meta-analysis. Metabolism 2020, 111, 154336. [Google Scholar] [CrossRef]
- Shamseer, L.; Moher, D.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: Elaboration and explanation. BMJ 2015, 350, g7647. [Google Scholar] [CrossRef] [Green Version]
- Keating, S.E.; Johnson, N.A.; Mielke, G.I.; Coombes, J.S. A systematic review and meta-analysis of interval training versus moderate-intensity continuous training on body adiposity. Obes. Rev. 2017, 18, 943–964. [Google Scholar] [CrossRef] [PubMed]
- Fatahi, S.; Nazary-Vannani, A.; Sohouli, M.H.; Mokhtari, Z.; Kord-Varkaneh, H.; Moodi, V.; Tan, S.C.; Low, T.Y.; Zanghelini, F.; Shidfar, F. The effect of fasting and energy restricting diets on markers of glucose and insulin controls: A systematic review and meta-analysis of randomized controlled trials. Crit. Rev. Food Sci. Nutr. 2021, 61, 3383–3394. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.Y.; Gallagher, D. Assessment methods in human body composition. Curr. Opin. Clin. Nutr. Metab. Care 2008, 11, 566–572. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions Version 6.3 (Updated February 2022); Cochrane: London, UK, 2022; Available online: https://training.cochrane.org/handbook (accessed on 26 February 2022).
- Higgins, J.P.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A. The cochrane collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, 889–893. [Google Scholar] [CrossRef] [Green Version]
- Guyatt, G.H.; Oxman, A.D.; Vist, G.E.; Kunz, R.; Falck-Ytter, Y.; Alonso-Coello, P.; Schünemann, H.J. GRADE: An emerging consensus on rating quality of evidence and strength of recommendations. BMJ 2008, 336, 924–926. [Google Scholar] [CrossRef] [Green Version]
- Francois, M.E.; Gilbertson, N.M.; Eichner, N.Z.M.; Heiston, E.M.; Fabris, C.; Breton, M.; Mehaffey, J.H.; Hassinger, T.; Hallowell, P.T.; Malin, S.K. Combining Short-Term Interval Training with Caloric Restriction Improvesß-Cell Function in Obese Adults. Nutrients 2018, 10, 717. [Google Scholar] [CrossRef] [Green Version]
- Gilbertson, N.M.; Eichner, N.Z.; Heiston, E.M.; Gaitán, J.M.; Francois, M.E.; Mehaffey, J.H.; Hassinger, T.E.; Hallowell, P.T.; Weltman, A.; Malin, S.K. A low-calorie diet with or without interval exercise training improves adiposopathy in obese women. Appl. Physiol. Nutr. Metab. 2019, 44, 1057–1064. [Google Scholar] [CrossRef]
- Gillen, J.B.; Percival, M.E.; Ludzki, A.; Tarnopolsky, M.A.; Gibala, M.J. Interval training in the fed or fasted state improves body composition and muscle oxidative capacity in overweight women. Obesity 2013, 21, 2249–2255. [Google Scholar] [CrossRef]
- Gyorkos, A.; Baker, M.H.; Miutz, L.N.; Lown, D.A.; Jones, M.A.; Houghton-Rahrig, L.D. Carbohydrate-restricted Diet and High-intensity Interval Training Exercise Improve Cardio-metabolic and Inflammatory Profiles in Metabolic Syndrome: A Randomized Crossover Trial. Cureus 2019, 11, e5596. [Google Scholar] [CrossRef] [Green Version]
- Heiston, E.M.; Gilbertson, N.M.; Eichner, N.Z.M.; Malin, S.K. A Low-Calorie Diet with or without Exercise Reduces Postprandial Aortic Waveform in Females with Obesity. Med. Sci. Sports Exerc. 2021, 53, 796–803. [Google Scholar] [CrossRef]
- Malin, S.K.; Heiston, E.M.; Gilbertson, N.M.; Eichner, N.Z.M. Short-term interval exercise suppresses acylated ghrelin and hunger during caloric restriction in women with obesity. Physiol. Behav. 2020, 223, 112978. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, L.R.; Olsen, R.H.; Anholm, C.; Astrup, A.; Eugen-Olsen, J.; Fenger, M.; Simonsen, L.; Walzem, R.L.; Haugaard, S.B.; Prescott, E. Effects of 1 year of exercise training versus combined exercise training and weight loss on body composition, low-grade inflammation and lipids in overweight patients with coronary artery disease:a randomized trial. Cardiovasc. Diabetol. 2019, 18, 127. [Google Scholar] [CrossRef] [PubMed]
- Sartor, F.; de Morree, H.M.; Matschke, V.; Marcora, S.M.; Milousis, A.; Thom, J.M.; Kubis, H.P. High-intensity exercise and carbohydrate-reduced energy-restricted diet in obese individuals. Eur. J. Appl. Physiol. 2010, 110, 893–903. [Google Scholar] [CrossRef] [PubMed]
- Sun, S.; Kong, Z.; Shi, Q.; Hu, M.; Zhang, H.; Zhang, D.; Nie, J. Non-Energy-Restricted Low-Carbohydrate Diet Combined with Exercise Intervention Improved Cardiometabolic Health in Overweight Chinese Females. Nutrients 2019, 11, 3051. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Flegal, K.M.; Kit, B.K.; Orpana, H.; Graubard, B.I. Association of all-cause mortality with overweight and obesity using standard body mass index categories: A systematic review and meta-analysis. JAMA 2013, 309, 71–82. [Google Scholar] [CrossRef] [Green Version]
- Moholdt, T.; Silva, C.P.; Lydersen, S.; Hawley, J.A. Isolated and combined effects of high-intensity interval training and time-restricted eating on glycaemic control in reproductive-aged women with overweight or obesity: Study protocol for a four-armed randomised controlled trial. BMJ Open 2021, 11, e040020. [Google Scholar] [CrossRef] [PubMed]
- Martin-Smith, R.; Cox, A.; Buchan, D.S.; Baker, J.S.; Grace, F.; Sculthorpe, N. High Intensity Interval Training (HIIT) Improves Cardiorespiratory Fitness (CRF) in Healthy, Overweight and Obese Adolescents: A Systematic Review and Meta-Analysis of Controlled Studies. Int. J. Environ. Res. Public Health 2020, 17, 2955. [Google Scholar] [CrossRef]
- Miguet, M.; Fearnbach, N.S.; Metz, L.; Khammassi, M.; Julian, V.; Cardenoux, C.; Pereira, B.; Boirie, Y.; Duclos, M.; Thivel, D. Effect of HIIT versus MICT on body composition and energy intake in dietary restrained and unrestrained adolescents with obesity. Appl. Physiol. Nutr. Metab. 2020, 45, 437–445. [Google Scholar] [CrossRef]
- Chin, S.H.; Kahathuduwa, C.N.; Binks, M. Physical activity and obesity: What we know and what we need to know. Obes. Rev. 2016, 17, 1226–1244. [Google Scholar] [CrossRef]
- Batacan, R.B., Jr.; Duncan, M.J.; Dalbo, V.J.; Tucker, P.S.; Fenning, A.S. Effects of high-intensity interval training on cardiometabolic health: A systematic review and meta-analysis of intervention studies. Br. J. Sports Med. 2017, 51, 494–503. [Google Scholar] [CrossRef]
- Taylor, J.L.; Holland, D.J.; Keating, S.E.; Leveritt, M.D.; Gomersall, S.R.; Rowlands, A.V.; Bailey, T.G.; Coombes, J.S. Short-term and Long-term Feasibility, Safety, and Efficacy of High-Intensity Interval Training in Cardiac Rehabilitation: The FITR Heart Study Randomized Clinical Trial. JAMA Cardiol. 2020, 5, 1382–1389. [Google Scholar] [CrossRef] [PubMed]
- Tinsley, G.M.; La Bounty, P.M. Effects of intermittent fasting on body composition and clinical health markers in humans. Nutr. Rev. 2015, 73, 661–674. [Google Scholar] [CrossRef] [PubMed]
- Viana, R.B.; Naves, J.P.A.; Coswig, V.S.; De Lira, C.A.B.; Steele, J.; Fisher, J.P.; Gentil, P. Is interval training the magic bullet for fat loss? A systematic review and meta-analysis comparing moderate-intensity continuous training with high-intensity interval training (HIIT). Br. J. Sports Med. 2019, 53, 655–664. [Google Scholar] [CrossRef]
- Gripp, F.; Nava, R.C.; Cassilhas, R.C.; Esteves, E.A.; Magalhães, C.O.D.; Dias-Peixoto, M.F.; de Castro Magalhães, F.; Amorim, F.T. HIIT is superior than MICT on cardiometabolic health during training and detraining. Eur. J. Appl. Physiol. 2021, 121, 159–172. [Google Scholar] [CrossRef]
- Martins, C.; Kazakova, I.; Ludviksen, M.; Mehus, I.; Wisloff, U.; Kulseng, B.; Morgan, L.; King, N. High-Intensity Interval Training and Isocaloric Moderate-Intensity Continuous Training Result in Similar Improvements in Body Composition and Fitness in Obese Individuals. Int. J. Sport Nutr. Exerc. Metab. 2016, 26, 197–204. [Google Scholar] [CrossRef] [PubMed]
- Trepanowski, J.F.; Kroeger, C.M.; Barnosky, A.; Klempel, M.; Bhutani, S.; Hoddy, K.K.; Rood, J.; Ravussin, E.; Varady, K.A. Effects of alternate-day fasting or daily calorie restriction on body composition, fat distribution, and circulating adipokines: Secondary analysis of a randomized controlled trial. Clin. Nutr. 2018, 37, 1871–1878. [Google Scholar] [CrossRef]
- Smith, U. Abdominal obesity: A marker of ectopic fat accumulation. J. Clin. Investig. 2015, 125, 1790–1792. [Google Scholar] [CrossRef] [Green Version]
- Dhawan, D.; Sharma, S. Abdominal Obesity, Adipokines and Non-communicable Diseases. J. Steroid Biochem. Mol. Biol. 2020, 203, 105737. [Google Scholar] [CrossRef]
- Frączek, B.; Pięta, A.; Burda, A.; Mazur-Kurach, P.; Tyrała, F. Paleolithic Diet-Effect on the Health Status and Performance of Athletes? Nutrients 2021, 13, 1019. [Google Scholar] [CrossRef]
- Elagizi, A.; Kachur, S.; Lavie, C.J.; Carbone, S.; Pandey, A.; Ortega, F.B.; Milani, R.V. An Overview and Update on Obesity and the Obesity Paradox in Cardiovascular Diseases. Prog. Cardiovasc. Dis. 2018, 61, 142–150. [Google Scholar] [CrossRef] [Green Version]
- Lu, Y.; Shu, H.; Zheng, Y.; Li, C.; Liu, M.; Chen, Z.; He, X. Comparison of fat-free mass index and fat mass index in Chinese adults. Eur. J. Clin. Nutr. 2012, 66, 1004–1007. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hu, J.; Wang, Z.; Lei, B.; Li, J.; Wang, R. Effects of a Low-Carbohydrate High-Fat Diet Combined with High-Intensity Interval Training on Body Composition and Maximal Oxygen Uptake: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 18, 10740. [Google Scholar] [CrossRef] [PubMed]
- Yancy, W.S., Jr.; Olsen, M.K.; Guyton, J.R.; Bakst, R.P.; Westman, E.C. A low-carbohydrate, ketogenic diet versus a low-fat diet to treat obesity and hyperlipidemia: A randomized, controlled trial. Ann. Intern. Med. 2004, 140, 769–777. [Google Scholar] [CrossRef] [PubMed]
- Moon, S.; Kang, J.; Kim, S.H.; Chung, H.S.; Kim, Y.J.; Yu, J.M.; Cho, S.T.; Oh, C.M.; Kim, T. Beneficial Effects of Time-Restricted Eating on Metabolic Diseases: A Systemic Review and Meta-Analysis. Nutrients 2020, 12, 1267. [Google Scholar] [CrossRef]
- Fernando, H.A.; Zibellini, J.; Harris, R.A.; Seimon, R.V.; Sainsbury, A. Effect of Ramadan Fasting on Weight and Body Composition in Healthy Non-Athlete Adults: A Systematic Review and Meta-Analysis. Nutrients 2019, 11, 478. [Google Scholar] [CrossRef] [Green Version]
- Wen, D.; Utesch, T.; Wu, J.; Robertson, S.; Liu, J.; Hu, G.; Chen, H. Effects of different protocols of high intensity interval training for VO2max improvements in adults: A meta-analysis of randomised controlled trials. J. Sci. Med. Sport 2019, 22, 941–947. [Google Scholar] [CrossRef]
- Fisher, G.; Brown, A.W.; Bohan Brown, M.M.; Alcorn, A.; Noles, C.; Winwood, L.; Resuehr, H.; George, B.; Jeansonne, M.M.; Allison, D.B. High Intensity Interval- vs. Moderate Intensity- Training for Improving Cardiometabolic Health in Overweight or Obese Males: A Randomized Controlled Trial. PLoS ONE 2015, 10, e0138853. [Google Scholar] [CrossRef]
- Ryan, B.J.; Schleh, M.W.; Ahn, C.; Ludzki, A.C.; Gillen, J.B.; Varshney, P.; Van Pelt, D.W.; Pitchford, L.M.; Chenevert, T.L.; Gioscia-Ryan, R.A.; et al. Moderate-Intensity Exercise and High-Intensity Interval Training Affect Insulin Sensitivity Similarly in Obese Adults. J. Clin. Endocrinol. Metab. 2020, 105, e2941–e2959. [Google Scholar] [CrossRef]
- Winding, K.M.; Munch, G.W.; Iepsen, U.W.; Van Hall, G.; Pedersen, B.K.; Mortensen, S.P. The effect on glycaemic control of low-volume high-intensity interval training versus endurance training in individuals with type 2 diabetes. Diabetes Obes. Metab. 2018, 20, 1131–1139. [Google Scholar] [CrossRef] [Green Version]
- Søgaard, D.; Lund, M.T.; Scheuer, C.M.; Dehlbaek, M.S.; Dideriksen, S.G.; Abildskov, C.V.; Christensen, K.K.; Dohlmann, T.L.; Larsen, S.; Vigelsø, A.H.; et al. High-intensity interval training improves insulin sensitivity in older individuals. Acta Physiol. 2018, 222, e13009. [Google Scholar] [CrossRef]
- Cho, Y.; Hong, N.; Kim, K.W.; Cho, S.J.; Lee, M.; Lee, Y.H.; Lee, Y.H.; Kang, E.S.; Cha, B.S.; Lee, B.W. The Effectiveness of Intermittent Fasting to Reduce Body Mass Index and Glucose Metabolism: A Systematic Review and Meta-Analysis. J. Clin. Med. 2019, 8, 1645. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Souza, J.F.T.; Dáttilo, M.; de Mello, M.T.; Tufik, S.; Antunes, H.K.M. High-Intensity Interval Training Attenuates Insulin Resistance Induced by Sleep Deprivation in Healthy Males. Front. Physiol. 2017, 8, 992. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| PICOS | Inclusion | Exclusion |
|---|---|---|
| Participant | ≥18 years old diagnosed with overweight or obesity | Age-incompatible; normal-weight; animal-based subjects |
| Intervention | HIIT + fasting | Other intervention |
| Outcome | BM; BMI; WC; PFM; FM; FFM; VO2peak; FPG; FPI | Other outcomes |
| Study | RCT | Books; opinion articles; observational studies; reviews; prospective cohort studies; studies and abstracts without adequate data |
| PICOS | Search Terms |
|---|---|
| Participant | obesity OR adult obesity OR adult with obesity OR obesity in adult OR obese OR overweight |
| Intervention | (High-Intensity Interval Training OR High Intensity Interval Training OR High-Intensity Interval Trainings OR Interval Training OR Interval Trainings OR High-Intensity Intermittent Exercise OR High-Intensity Intermittent Exercises OR Sprint Interval Training OR Sprint Interval Trainings OR high intensity sprint OR aerobic interval training OR aerobic interval trainings OR HIIT OR HIIE) AND (Fasting OR fasting OR Intermittent Fasting OR Intermittent Fastings OR Hunger Strike OR Hunger Strikes OR Time Restricted Feeding OR Time Restricted Feedings) |
| Study | randomized controlled trial OR randomized OR placebo |
| Outcome | body weight OR body mass OR BMI OR body mass index OR body fat percent OR percent fat mass OR body fat mass OR fat-free mass OR lean body mass OR VO2peak OR fasting plasma glucose OR fasting plasma insulin |
| Study | Country | Sample Size | Age Years | Types of Sport | HIIT Intervention | Fasting Intervention | Frequency | Duration | Control | Outcomes |
|---|---|---|---|---|---|---|---|---|---|---|
| Francois 2018 | USA | 23 | 46 ± 12 | Bicycle | Exercise: 90%HRmax for 3 min; Intermittent: 50%HRmax for 3 min; 6–10 times | LCD (1000–1200 kcal/day) | HIIT: 7 times/week Fasting: 7 times/week | 13 days | Only maintain LCD | BM; BMI; VO2peak; FM; PFM; FFM; FPG; FPI |
| Gilbertson 2019 | USA | 24 | 48.3 ± 13 | Bicycle | Exercise: 90%HRmax for 3 min; Intermittent: 50%HRmax for 3 min; 6–10 times | LCD (1000–1200 kcal/day) | HIIT: 7 times/week Fasting: 7 times/week | 2 weeks | Only maintain LCD | BM; BMI; WC; VO2peak; FM; PFM; FFM; FPG; FPI |
| Gillen 2013 | Canada | 16 | 27 ± 8 | Bicycle | Exercise: 90%HRmax for 60 s; Intermittent: rest or pedal slowly at a resistance of 50 W for 60 s; 10 times | Keeping overnight fasting before exercise | HIIT: 3 times/week Fasting:3 times/week | 6 weeks | Meal at 60min before HIIT | BM; FM; PFM; FPG; FPI |
| Gyorkos | USA | 12 | 18–60 | Bicycle | Exercise: 90%HRmax for 60 s; Intermittent: active recovery for 60 s; 10 times | A carbohydrate-restricted Paleolithic-based diet | HIIT: 3 times/week Fasting: 7 times/week | 4 weeks | Only maintain a carbohydrate-restricted Paleolithic-based diet | BM; BMI; WC; PFM; VO2peak; FPG;FPI |
| Heiston 2020 | USA | 25 | 47.1 ± 12 | Bicycle | Exercise: 90%HRmax for 3 min; Intermittent: 50%HRmax for 3 min; 6–10 times | LCD (1000–1200 kcal/day) | HIIT: 7 times/week Fasting: 7 times/week | 13 days | Only maintain LCD | BM; BMI; WC; VO2peak; PFM; FFM; FPG; FPI |
| Malin 2020 | USA | 26 | 47.3 ± 12.2 | Bicycle | Exercise: 90%HRmax for 3 min; Intermittent: 50%HRmax for 3 min; 6–10 times | LCD (1000–1200 kcal/day) | HIIT:7 times/week Fasting: 7 times/week | 13 days | Only maintain LCD | BM; BMI; WC; PFM; FM; FFM; VO2peak |
| Pedersen 2019 | Denmark | 55 | 45–75 | Bicycle | Exercise: 85–90%VO2peak for 1–4 min; Intermittent: 65–70%VO2peak for 1–3 min 4 times | LCD (800–1000 kcal/day) | HIIT: 3 times/week Fasting: 7 times/week | 1 years | Only maintain HIIT | BM; BMI; FM; FFM; WC; VO2peak; |
| Sartor 2010 | UK | 19 | 39 ± 12 | Bicycle | Exercise: 90%VO2peak for 4 min; Intermittent: rest for 2–3 min; 10 times | A moderately low-carbohydrate and high-unsaturated fat diet | HIIT: 3 times/week Fasting: 7 time/week | 2 weeks | Only maintain fasting intervention | BM; FM; FFM; FPG; FPI; |
| Sun 2019 | China | 30 | 21.2 ± 3.3 | Bicycle | Exercise: Sprint phases for 6 s; Intermittent: passive recovery for 9 s; 10 times | A low-carbohydrate diet | HIIT: 5 times/week Fasting: 7 times/week | 4 weeks | Maintain normal dietary habits and normal exercise habits | BM; BMI; VO2peak; WC; FPG; |
| Outcomes | Intervention | N | ES (95% CI) | Heterogeneity | p | |
|---|---|---|---|---|---|---|
| I2 (%) | p | |||||
| Body mass | Long term | 4 | MD: −4.28 | 0 | 0.45 | 0.008 |
| (−7.44, −1.13) | ||||||
| Short term | 4 | MD: 2.91 | 0 | 1 | 0.39 | |
| (−3.78, 9.06) | ||||||
| Long interval | 6 | MD: −2.93 | 7 | 0.37 | 0.16 | |
| (−6.99, 1.13) | ||||||
| Short interval | 3 | MD: −0.81 | 0 | 0.91 | 0.77 | |
| (−6.20, 4.58) | ||||||
| LCD | 6 | MD: −2.31 | 12 | 0.34 | 0.3 | |
| (−6.69, 2.07) | ||||||
| Low-carbohydrate diet | 3 | MD: −1.02 | 0 | 0.96 | 0.71 | |
| (−6.5, 4.45) | ||||||
| BMI | Long term | 3 | MD: −1.56 | 0 | 0.39 | 0.01 |
| (−2.76, −0.36) | ||||||
| Short term | 4 | MD: 0.36 | 0 | 0.98 | 0.78 | |
| (−2.22, 2.94) | ||||||
| Long interval | 5 | MD: −1.23 | 0 | 0.7 | 0.03 | |
| (−2.55, 0.09) | ||||||
| Short interval | 2 | MD: −1.43 | 40 | 0.2 | 0.29 | |
| (−4.08, 1.22) | ||||||
| LCD | 5 | MD: −1.23 | 0 | 0.7 | 0.03 | |
| (−2.55, 0.09) | ||||||
| Low-carbohydrate diet | 2 | MD: −1.43 | 40 | 0.2 | 0.29 | |
| (−4.08, 1.22) | ||||||
| WC | Long term | 3 | MD: −5.14 | 0 | 0.7 | 0.002 |
| (−8.33, −1.96) | ||||||
| Short term | 3 | MD: −1.73 | 0 | 0.76 | 0.55 | |
| (−7.43, 3.97) | ||||||
| Long interval | 4 | MD: −4.22 | 0 | 0.65 | 0.01 | |
| (−7.54, −0.89) | ||||||
| Short interval | 2 | MD: −4.6 | 0 | 0.42 | 0.07 | |
| (−9.66, 0.46) | ||||||
| LCD | 4 | MD: −4.22 | 0 | 0.65 | 0.01 | |
| (−7.54, −0.89) | ||||||
| Low-carbohydrate diet | 2 | MD: −4.6 | 0 | 0.42 | 0.07 | |
| (−9.66, 0.46) | ||||||
| BFP | Long term | 3 | MD: −1.04 | 0 | 0.67 | 0.26 |
| (−2.84, 0.76) | ||||||
| Short term | 3 | MD: −1.05 | 0 | 0.58 | 0.31 | |
| (−3.09, 0.98) | ||||||
| Long interval | 4 | MD: −1.08 | 0 | 0.78 | 0.14 | |
| (−2.5, 0.35) | ||||||
| Short interval | 2 | MD: −0.78 | 0 | 0.37 | 0.72 | |
| (−5.02, 3.46) | ||||||
| LCD | 5 | MD: −0.96 | 0 | 0.8 | 0.18 | |
| (−2.35, 0.43) | ||||||
| Low-carbohydrate diet | 1 | MD: −2.4 | NA | NA | 0.4 | |
| (−7.95, 3.15) | ||||||
| FM | Long term | 2 | MD: −2.47 | 2 | 0.31 | 0.01 |
| (−4.45, −0.5) | ||||||
| Short term | 3 | MD: 0.65 | 0 | 0.86 | 0.8 | |
| (−4.42, 5.71) | ||||||
| Long interval | 5 | MD: −2.33 | 0 | 0.69 | 0.007 | |
| (−4.02, −0.63) | ||||||
| Short interval | 1 | MD: 2 | NA | NA | 0.66 | |
| (−6.94, 10.94) | ||||||
| LCD | 5 | MD: −2.45 | 0 | 0.54 | 0.01 | |
| (−4.17, −0.73) | ||||||
| Low-carbohydrate diet | 1 | MD: −2 | NA | NA | 0.65 | |
| (−10.59, 6.59) | ||||||
| FFM | Long term | 2 | MD: −2.28 | 0 | 0.58 | 0.28 |
| (−6.38, 1.82) | ||||||
| Short term | 5 | MD: 1.57 | 0 | 0.99 | 0.28 | |
| (−1.27, 4.41) | ||||||
| Long interval | 6 | MD: 0.48 | 0 | 0.74 | 0.7 | |
| (−2.01, 2.98) | ||||||
| Short interval | 1 | MD: −0.8 | NA | NA | 0.81 | |
| (−7.41, 5.81) | ||||||
| LCD | 6 | MD: 0.16 | 0 | 0.77 | 0.9 | |
| (−2.24, 2.57) | ||||||
| Low-carbohydrate diet | 1 | MD: 3 | NA | NA | 0.55 | |
| (−6.82, 12.82) | ||||||
| VO2peak | Long term | 3 | SMD: 0.67 | 58 | 0.09 | 0.04 |
| (0.03, 1.32) | ||||||
| Short term | 4 | SMD: 0.85 | 29 | 0.24 | 0.0006 | |
| (0.37, 1.34) | ||||||
| Long interval | 5 | SMD: 0.77 | 13 | 0.33 | 0.0001 | |
| (0.41, 1.13) | ||||||
| Short interval | 2 | SMD: 0.89 | 77 | 0.04 | 0.15 | |
| (−0.32, 2.09) | ||||||
| LCD | 5 | SMD: 0.77 | 13 | 0.33 | 0.0001 | |
| (0.41, 1.13) | ||||||
| Low-carbohydrate diet | 2 | SMD: 0.89 | 77 | 0.04 | 0.15 | |
| (−0.32, 2.09) | ||||||
| FPG | Long term | 3 | SMD: −0.61 | 0 | 0.42 | 0.01 |
| (−1.09, −0.13) | ||||||
| Short term | 4 | SMD: 0.22 | 0 | 0.84 | 0.22 | |
| (−0.19, 0.63) | ||||||
| Long interval | 4 | SMD: 0.22 | 0 | 0.84 | 0.22 | |
| (−0.19, 0.63) | ||||||
| Short interval | 3 | SMD: −0.61 | 0 | 0.42 | 0.01 | |
| (−1.09, −0.13) | ||||||
| LCD | 4 | SMD: 0.23 | 0 | 0.84 | 0.29 | |
| (−0.19, 0.65) | ||||||
| Low-carbohydrate diet | 3 | SMD: −0.58 | 4 | 0.35 | 0.02 | |
| (−1.06, −0.09) | ||||||
| FPI | Long term | 2 | SMD: −0.05 | 0 | 0.97 | 0.87 |
| (−0.67, 0.57) | ||||||
| Short term | 4 | SMD: 0.21 | 0 | 0.7 | 0.32 | |
| (−0.2, 0.62) | ||||||
| Long interval | 4 | SMD: 0.21 | 0 | 0.7 | 0.32 | |
| (−0.2, 0.62) | ||||||
| Short interval | 2 | SMD: −0.05 | 0 | 0.97 | 0.87 | |
| (−0.67, 0.57) | ||||||
| LCD | 4 | SMD: 0.17 | 0 | 0.64 | 0.43 | |
| (−0.25, 0.59) | ||||||
| Low-carbohydrate diet | 2 | SMD: 0.05 | 0 | 0.74 | 0.87 | |
| (−0.55, 0.65) | ||||||
| Patient or population: patients with overweight and obese adults Settings: HIIT + fasting compared to other intervention in the treatment of overweight and obese adults Intervention: HIIT + fasting Comparison: HIIT alone or fasting alone or normal intervention | ||||
| Outcomes | Illustrative comparative risks * (95% CI) | Relative effect (95% CI) | No of Participants (studies) | Quality of the evidence (GRADE) |
| Corresponding risk | ||||
| HIIT + fasting | ||||
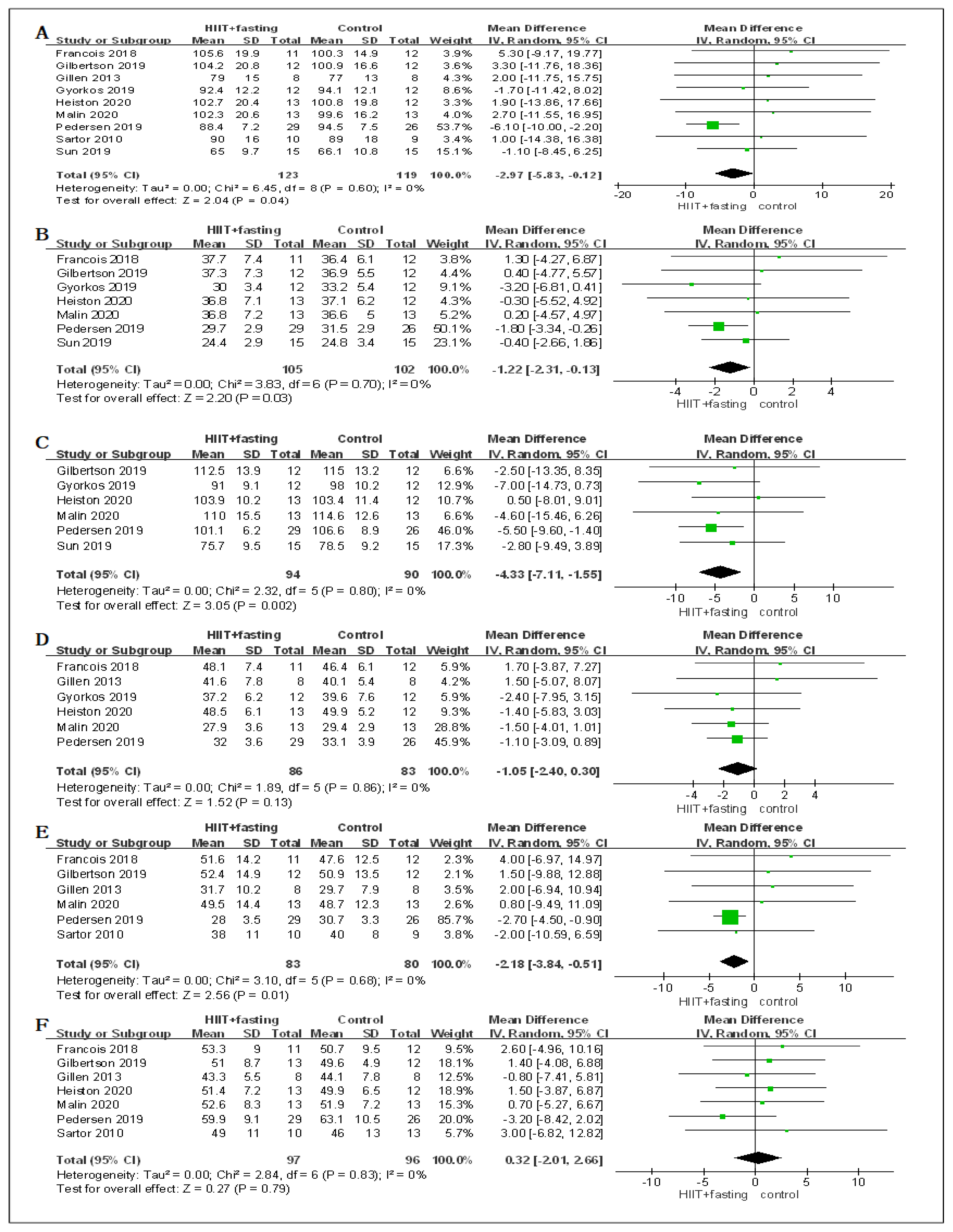
| Body mass | The mean body mass in the intervention groups was 2.97 lower (5.83 to 0.12 lower) | 242 (9 studies) | ⊕⊝⊝⊝ very low 1,2,3 | |
| BMI | The mean BMI in the intervention groups was 1.22 lower (2.31 to 0.13 lower) | 207 (7 studies) | ⊕⊝⊝⊝ very low 1,2,3 | |
| WC | The mean wc in the intervention groups was 4.33 lower (7.11 to 1.55 lower) | 184 (6 studies) | ⊕⊝⊝⊝ very low 1,2,3 | |
| PFM | The mean percentage fat mass in the intervention groups was 1.05 lower (2.4 lower to 0.3 higher) | 169 (6 studies) | ⊕⊝⊝⊝ very low 1,2,3,4 | |
| FM | The mean fat mass in the intervention groups was 2.18 lower (3.84 to 0.51 lower) | 163 (6 studies) | ⊕⊝⊝⊝ very low 1,2,3 | |
| FFM | The mean free fat mass in the intervention groups was 0.32 higher (2.01 lower to 2.66 higher) | 193 (7 studies) | ⊕⊝⊝⊝ very low 1,2,3,4 | |
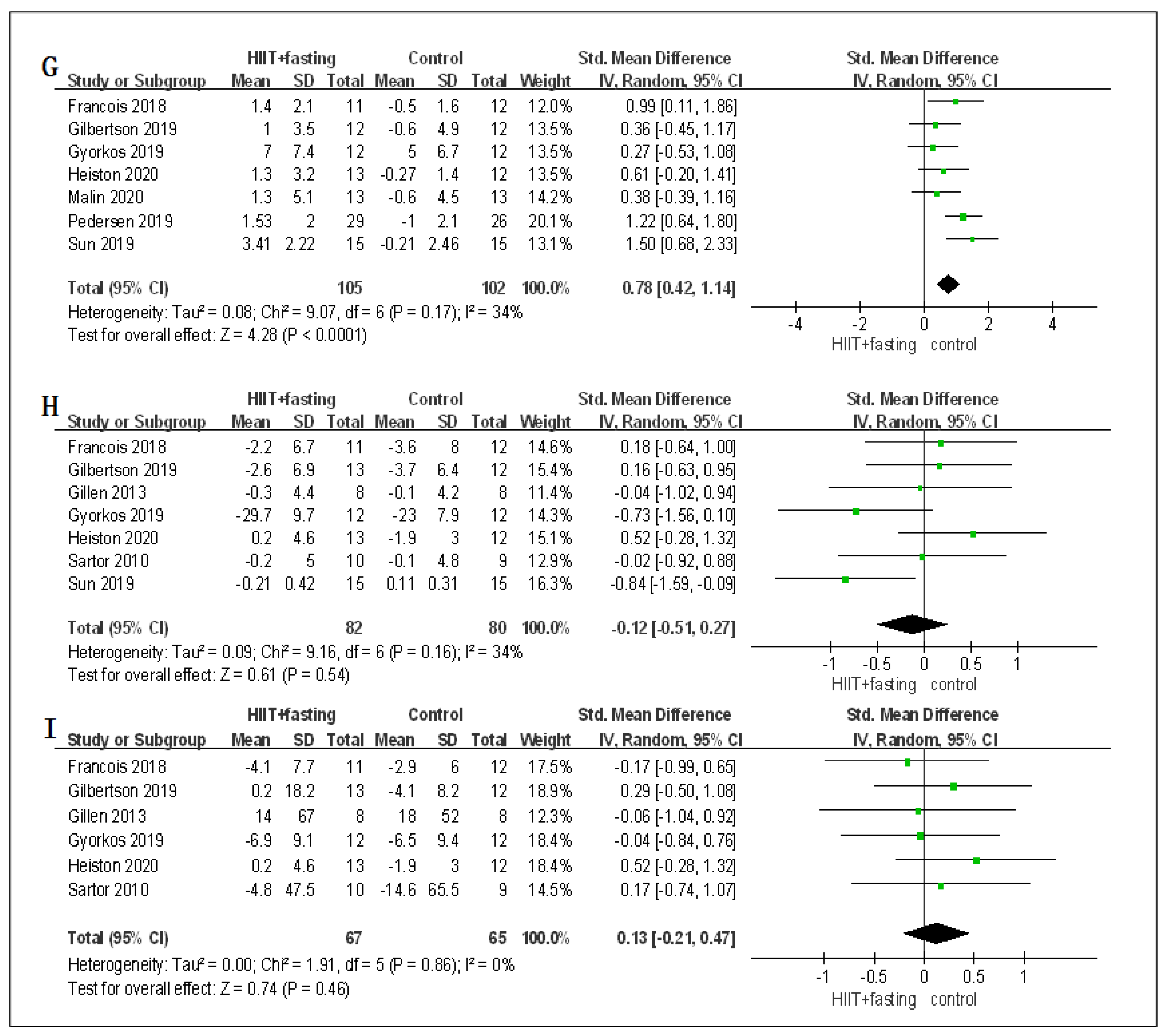
| VO2peak | The mean vo2 in the intervention groups was 0.78 SD higher (0.42 to 1.14 higher) | 207 (7 studies) | ⊕⊝⊝⊝ very low 1,2,3 | |
| FPG | The mean fpg in the intervention groups was 0.12 SD lower (0.51 lower to 0.27 higher) | 162 (7 studies) | ⊕⊝⊝⊝ very low 1,2,3,4 | |
| FPI | The mean fpi in the intervention groups was 0.13 SD higher (0.21 lower to 0.47 higher) | 132 (6 studies) | ⊕⊝⊝⊝ very low 1,2,3,4 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guo, Z.; Cai, J.; Wu, Z.; Gong, W. Effect of High-Intensity Interval Training Combined with Fasting in the Treatment of Overweight and Obese Adults: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2022, 19, 4638. https://doi.org/10.3390/ijerph19084638
Guo Z, Cai J, Wu Z, Gong W. Effect of High-Intensity Interval Training Combined with Fasting in the Treatment of Overweight and Obese Adults: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2022; 19(8):4638. https://doi.org/10.3390/ijerph19084638
Chicago/Turabian StyleGuo, Zhicheng, Jianguang Cai, Ziqiang Wu, and Weiqi Gong. 2022. "Effect of High-Intensity Interval Training Combined with Fasting in the Treatment of Overweight and Obese Adults: A Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 19, no. 8: 4638. https://doi.org/10.3390/ijerph19084638
APA StyleGuo, Z., Cai, J., Wu, Z., & Gong, W. (2022). Effect of High-Intensity Interval Training Combined with Fasting in the Treatment of Overweight and Obese Adults: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health, 19(8), 4638. https://doi.org/10.3390/ijerph19084638