
Returning to Work after the COVID-19 Pandemic Earthquake: A Systematic Review

 ,
, 
 and
and 
Abstract
:1. Introduction
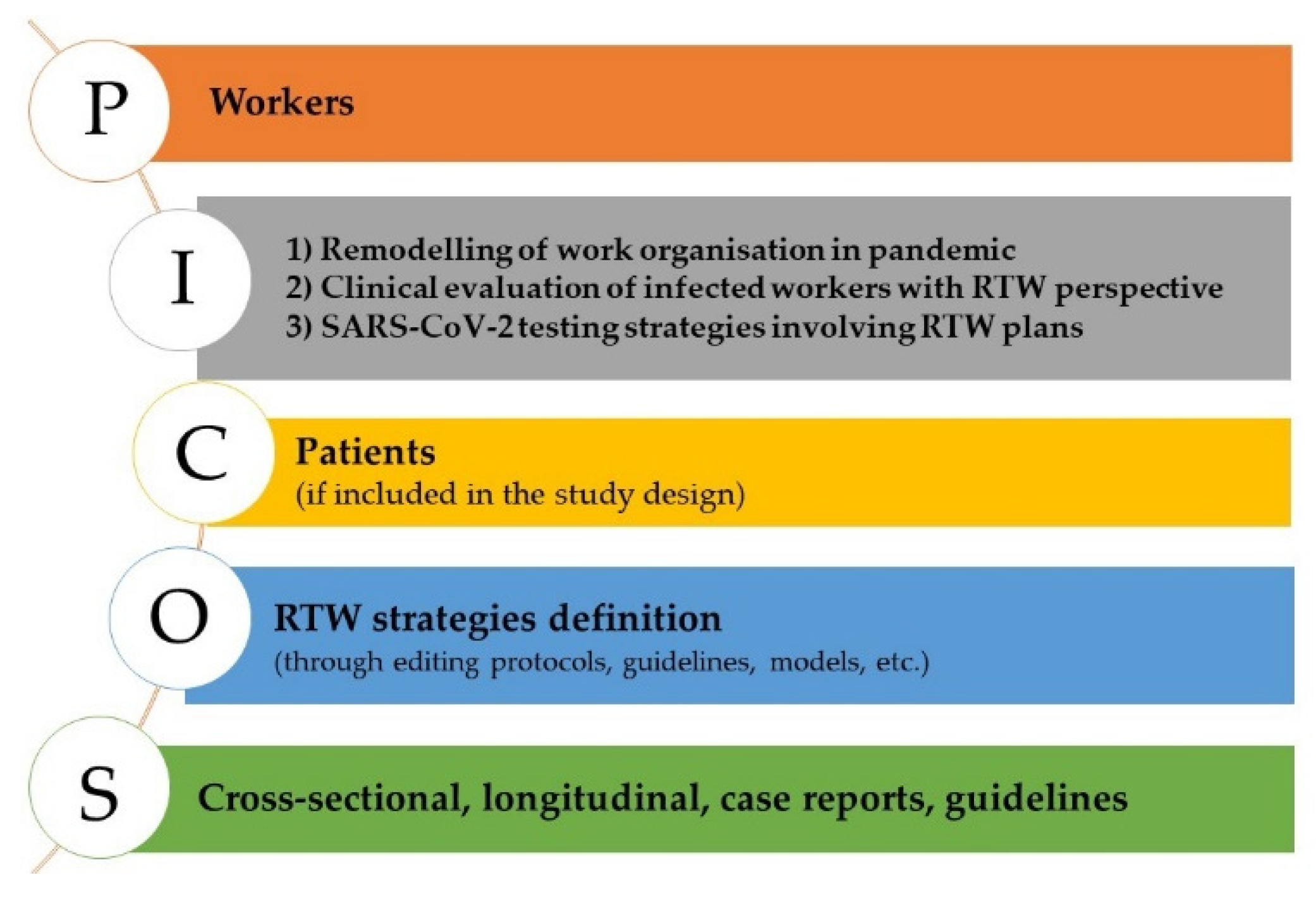
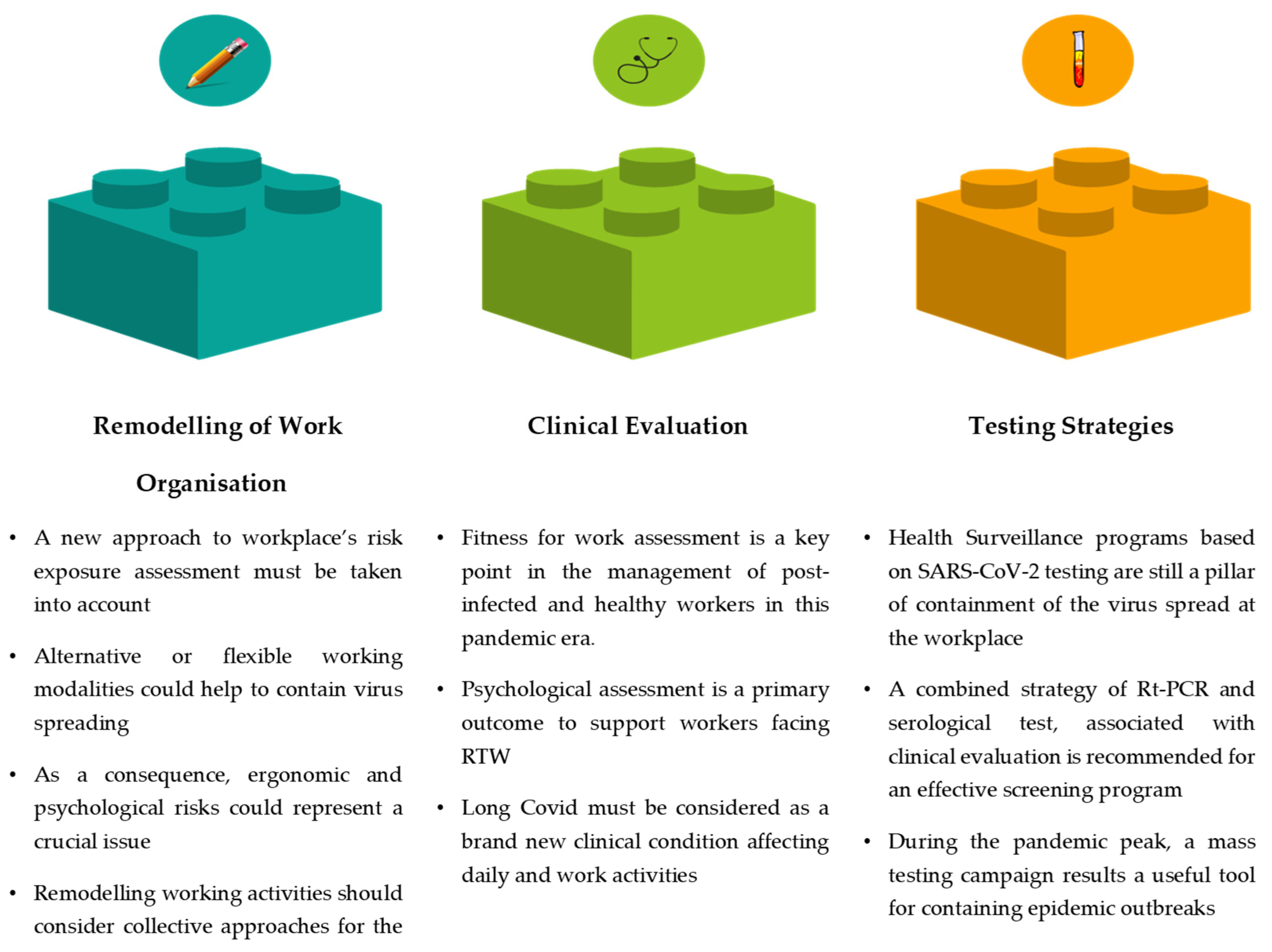
- Remodelling of work organisation;
- Clinical evaluation of workers;
- Testing strategies related to RTW.
2. Methods
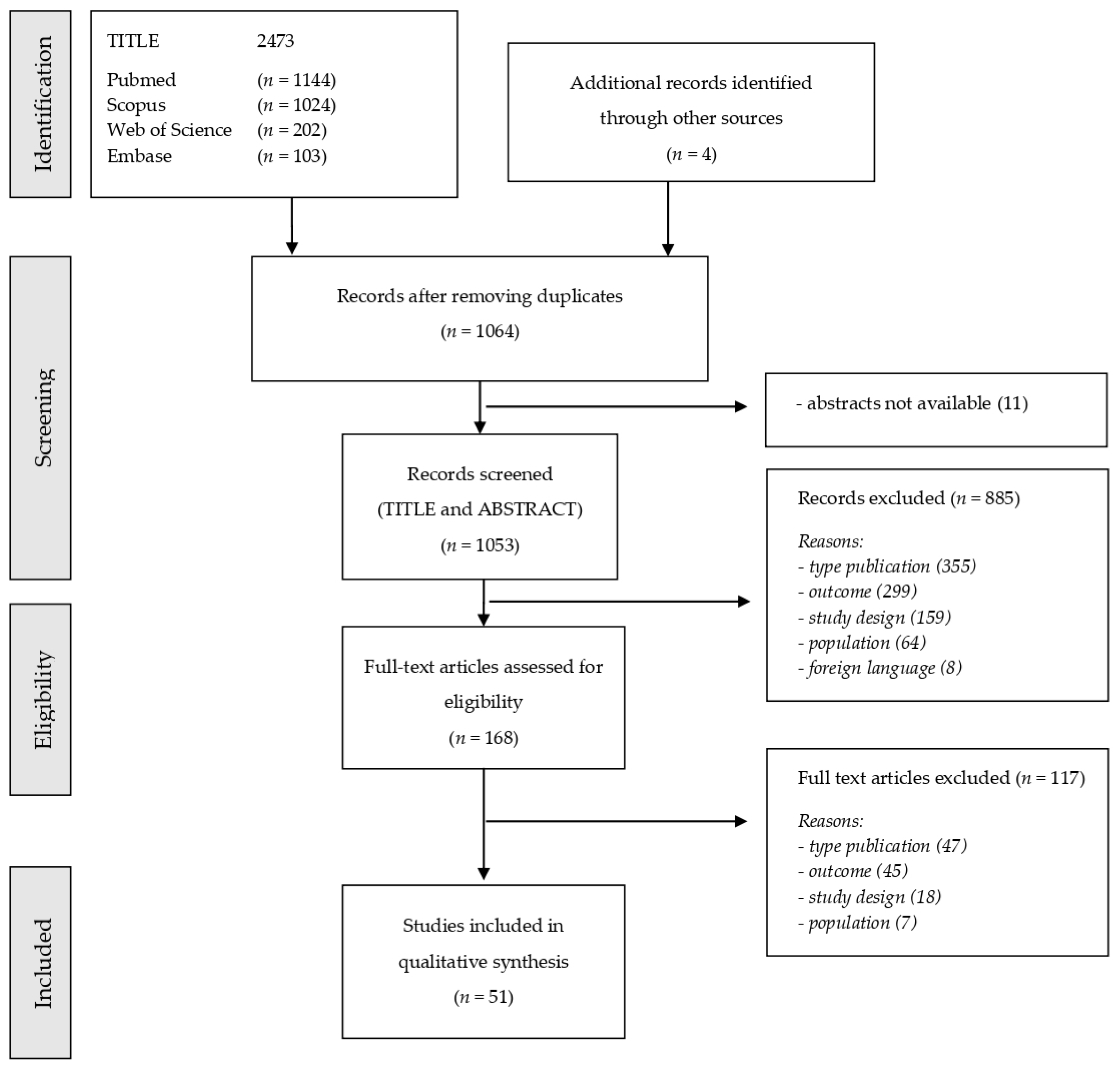
2.1. Data Sources and Searches
2.2. Study Outcomes and Selection
2.3. Data Extraction, Synthesis, and Analysis
3. Results
4. Discussion
4.1. Remodelling of Work Organisation
4.1.1. Models for RTW Management
4.1.2. Remodelling in Healthcare Settings
4.1.3. Teleworking
4.2. Evaluation of Clinical Condition, Health Surveillance and RTW
4.2.1. Psychosocial Aspects
4.2.2. Long COVID
4.2.3. Pre-Existing Medical Conditions and Vulnerable Workers
4.3. SARS-CoV-2 Testing and Return to Work
5. Strengths and limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization (WHO). Available online: https://covid19.who.int (accessed on 3 April 2022).
- Wei, Y.; Guan, J.; Ning, X.; Li, Y.; Wei, L.; Shen, S.; Zhang, R.; Zhao, Y.; Shen, H.; Chen, F. Global COVID-19 pandemic waves: Limited lessons learned worldwide over the past year. Engineering, 2021; in press. [Google Scholar] [CrossRef]
- Alwan, N.A.; Burgess, R.A.; Ashworth, S.; Beale, R.; Bhadelia, N.; Bogaert, D.; Dowd, J.; Eckerle, I.; Goldman, L.R.; Greenhalgh, T.; et al. Scientific consensus on the COVID-19 pandemic: We need to act now. Lancet 2020, 396, e71–e72. [Google Scholar] [CrossRef]
- Marziano, V.; Guzzetta, G.; Rondinone, B.M.; Boccuni, F.; Riccardo, F.; Bella, A.; Poletti, P.; Trentini, F.; Pezzotti, P.; Brusaferro, S.; et al. Retrospective analysis of the Italian exit strategy from COVID-19 lockdown. Proc. Natl. Acad. Sci. USA 2021, 118, e2019617118. [Google Scholar] [CrossRef] [PubMed]
- Sugerman-Brozan, J. Health Technical Committee of the Massachusetts Coalition for Occupational Safety and Health. Measures to Protect the Health and Safety of Massachusetts Employees Who Must Work at the Workplace During the SARS-CoV-2 Pandemic. New Solut. 2020, 30, 249–253. [Google Scholar] [CrossRef] [PubMed]
- Marcone, V. Reduction of Contagion Risks by SARS-Cov-2 (COVID-19) in Air-Conditioned Work Environments. Pain Physician 2020, 23, S475–S482. [Google Scholar] [CrossRef] [PubMed]
- Garzillo, E.M.; Monaco, M.G.L.; Spacone, A.; Inglese, E.; Lamberti, M.; Pompei, D. SARS-CoV-2 emergency in the workplace: Are companies ready to protect their workers? A cross-sectional survey. Int. J. Occup. Saf. Ergon. 2020, 11, 1–8. [Google Scholar] [CrossRef]
- Rueda-Garrido, J.C.; Vicente-Herrero, M.T.; Del Campo, M.T.; Reinoso-Barbero, L.; de la Hoz, R.E.; Delclos, G.L.; Kales, S.N.; Fernandez-Montero, A. Return to work guidelines for the COVID-19 pandemic. Occup. Med. 2020, 17, 300–305. [Google Scholar] [CrossRef]
- Shi, L.; Lu, Z.-A.; Que, J.-Y.; Huang, X.-L.; Lu, Q.-D.; Liu, L.; Zheng, Y.-B.; Liu, W.-J.; Ran, M.-S.; Yuan, K.; et al. Long-Term Impact of COVID-19 on Mental Health among the General Public: A Nationwide Longitudinal Study in China. Int. J. Environ. Res. Public Health 2021, 18, 8790. [Google Scholar] [CrossRef]
- Torres, A.E.; Ozog, D.M.; Hruza, G.J. Coronavirus Disease 2019 and Dermatology Practice Changes. Dermatol. Clin. 2021, 39, 587–597. [Google Scholar] [CrossRef]
- Rizk, H.G.; Strange, C.; Atallah, S.; Massingale, S.; Clendaniel, R. Coronavirus Disease 2019 Return to Work Guidance and Recommendations for Vestibular Clinicians. Ear Hear. 2020, 41, 693–696. [Google Scholar] [CrossRef]
- Lakkireddy, D.R.; Chung, M.K.; Deering, T.F.; Gopinathannair, R.; Albert, C.M.; Epstein, L.M.; Harding, C.V.; Hurwitz, J.L.; Jeffery, C.C.; Krahn, A.D.; et al. Guidance for Rebooting Electrophysiology Through the COVID-19 Pandemic From the Heart Rhythm Society and the American Heart Association Electrocardiography and Arrhythmias Committee of the Council on Clinical Cardiology: Endorsed by the American College of Cardiology. JACC Clin. Electrophysiol. 2020, 6, 1053–1066. [Google Scholar] [CrossRef] [PubMed]
- Benito, D.A.; Pasick, L.J.; Mulcahy, C.F.; Rajasekaran, K.; Todd-Hesham, H.; Joshi, A.S.; Goodman, J.F.; Thakkar, P. Local spikes in COVID-19 cases: Recommendations for maintaining otolaryngology clinic operations. Am. J. Otolaryngol. 2020, 41, 102688. [Google Scholar] [CrossRef] [PubMed]
- Geneid, A.; Nawka, T.; Schindler, A.; Oguz, H.; Chrobok, V.; Calcinoni, O.; Am Zehnhoff-Dinnesen, A.; Neumann, K.; Farahat, M.; Abou-Elsaad, T.; et al. Union of the European Phoniatricians’ position statement on the exit strategy of phoniatric and laryngological services: Staying safe and getting back to normal after the peak of coronavirus disease 2019 (issued on 25th May 2020). J. Laryngol. Otol. 2020, 134, 661–664. [Google Scholar] [CrossRef] [PubMed]
- Soffin, E.M.; Reisener, M.J.; Sama, A.A.; Beckman, J.D.; Liguori, G.A.; Lebl, D.R.; Girardi, F.P.; Cammisa, F.P.; Hughes, A.P. Essential Spine Surgery During the COVID-19 Pandemic: A Comprehensive Framework for Clinical Practice from a Specialty Orthopedic Hospital in New York City. HSS J. 2020, 16 (Suppl. 1), 29–35. [Google Scholar] [CrossRef] [PubMed]
- Nobel, T.B.; Marin, M.; Divino, C.M. Lessons in flexibility from a general surgery program at the epicenter of the pandemic in New York City. Surgery 2020, 168, 11–13. [Google Scholar] [CrossRef]
- Juprasert, J.M.; Gray, K.D.; Moore, M.D.; Obeid, L.; Peters, A.W.; Fehling, D.; Fahey, T.J., 3rd; Yeo, H.L. Restructuring of a General Surgery Residency Program in an Epicenter of the Coronavirus Disease 2019 Pandemic: Lessons From New York City. JAMA Surg. 2020, 155, 870–875. [Google Scholar] [CrossRef]
- de Amorim, L.M.; Maske, T.T.; Ferreira, S.H.; Dos Santos, R.B.; Feldens, C.A.; Kramer, P.F. New Post-COVID-19 Biosafety Protocols in Pediatric Dentistry. Pesqui Bras. Odontopediatria Clín. Integr. 2020, 20 (Suppl. 1). [Google Scholar] [CrossRef]
- Moura-Neto, J.A.; Palma, L.M.P.; Marchiori, G.F.; Stucchi, R.S.B.; Misael, A.M.; D’Avila, R.; Silva, D.R.D.; Andreoli, M.C.C.; Kraychete, A.; Bastos, K.; et al. Recommendations from the Brazilian Society of Nephrology for approaching Covid-19 Diagnostic Testing in Dialysis Units. J. Bras. Nefrol. 2020, 42 (Suppl. 1), 4–8. [Google Scholar] [CrossRef]
- Jin, S.; He, Y.; Yang, K.; Gan, Q.; Huang, W.; Wang, X.; Meng, C.; Wang, H. The Resumption of Sports Medicine During the COVID-19 Post-Epidemic Period: Experiences from Wuhan, People’s Republic of China. J. Bone Joint Surg. Am. 2021, 103, 10–14. [Google Scholar] [CrossRef]
- Wilson, K.C.; Kaminsky, D.A.; Michaud, G.; Sharma, S.; Nici, L.; Folz, R.J.; Barjaktarevic, I.; Bhakta, N.R.; Cheng, G.; Chupp, G.L.; et al. Restoring Pulmonary and Sleep Services as the COVID-19 Pandemic Lessens. From an Association of Pulmonary, Critical Care, and Sleep Division Directors and American Thoracic Society-coordinated Task Force. Ann. Am. Thorac. Soc. 2020, 17, 1343–1351. [Google Scholar] [CrossRef]
- Sunandar, H.; Ramdhan, D.K. Preventing and Controlling COVID-19: A Practical-Based Review in Offshore Workplace. Kesmas Jurnal Kesehatan Masyarakat Nasional 2021, 16, 97–101. [Google Scholar] [CrossRef]
- Callander, D.; Meunier, É.; DeVeau, R.; Grov, C.; Donovan, B.; Minichiello, V.; Singham Goodwin, A.; Duncan, D.T. Sex workers are returning to work and require enhanced support in the face of COVID-19: Results from a longitudinal analysis of online sex work activity and a content analysis of safer sex work guidelines. Sex Health 2020, 17, 384–386. [Google Scholar] [CrossRef] [PubMed]
- Simić, N.; Stefanović, M.; Petrović, G.; Stanković, A. Use of the risk analysis approach n the Serbian army integration process against Covid-19. Oper. Res. Eng. Sci. Theor. Appl. 2021, 4, 67–71. [Google Scholar] [CrossRef]
- Falorca, J.F. Envisioning a strategic framework to streamline building operation, sustainability and users’ disease control. J. Facil. Manag. 2021, 19, 195–227. [Google Scholar] [CrossRef]
- Iavicoli, S.; Boccuni, F.; Buresti, G.; Gagliardi, D.; Persechino, B.; Valenti, A.; Rondinone, B.M. Risk assessment at work and prevention strategies on COVID-19 in Italy. PLoS ONE 2021, 16, e0248874. [Google Scholar] [CrossRef]
- Carvalhais, C.; Querido, M.; Pereira, C.C.; Santos, J. Biological risk assessment: A challenge for occupational safety and health practitioners during the COVID-19 (SARS-CoV-2) pandemic. Work 2021, 69, 3–13. [Google Scholar] [CrossRef]
- Binnicker, M.J. Can the Severe Acute Respirat.tory Syndrome Coronavirus 2 Polymerase Chain Reaction Cycle Threshold Value and Time From Symptom Onset to Testing Predict Infectivity? Clin. Infect. Dis. 2020, 71, 2667–2668. [Google Scholar] [CrossRef]
- Longtin, Y.; Charest, H.; Quach, C.; Savard, P.; Baz, M.; Boivin, G.; Farfard, J.; Villeneuve, J.; Roger, M.; De Serres, G. Infectivity of healthcare workers diagnosed with coronavirus disease 2019 (COVID-19) approximately 2 weeks after onset of symptoms: A cross-sectional study. Infect. Control. Hosp. Epidemiol. 2021, 11, 102–104. [Google Scholar] [CrossRef]
- Stewart-Patterson, C.; Bourgeois, R.; Martin, D.W. The Importance of Keeping Patients with Post-Acute Sequelae of SARS-CoV-2 Infection (Long COVID) Engaged in Work. Am. Fam. Physician 2021, 103, 710. [Google Scholar]
- Cavasin, D.; Paladino, M.E.; Riva, M.A.; Persico, G.; Belingheri, M. Prolonged PCR Positivity Stigma and Return-To-Work After SARS-CoV-2 Infection. J. Occup. Environ. Med. 2021, 63, e100–e101. [Google Scholar] [CrossRef]
- Chua, K.Y.; Holmes, N.E.; Kwong, J. Prolonged PCR positivity in health care workers with COVID-19: Implications for practice guidelines. Med. J. Aust 2020, 213, 430–430.e1. [Google Scholar] [CrossRef] [PubMed]
- Henderson, D.K.; Weber, D.J.; Babcock, H.; Hayden, M.K.; Malani, A.; Wright, S.B.; Murthy, A.R.; Guzman-Cottrill, J.; Haessler, S.; Rock, C.; et al. The perplexing problem of persistently PCR-positive personnel. Infect. Control. Hosp. Epidemiol. 2021, 42, 203–204. [Google Scholar] [CrossRef] [PubMed]
- Caban-Martinez, A.J.; Schaefer-Solle, N.; Santiago, K.; Louzado-Feliciano, P.; Brotons, A.; Gonzalez, M.; Issenberg, S.B.; Kobetz, E. Epidemiology of SARS-CoV-2 antibodies among firefighters/paramedics of a US fire department: A cross-sectional study. Occup. Environ. Med. 2020, 77, 857–861. [Google Scholar] [CrossRef] [PubMed]
- Krsak, M.; Johnson, S.C.; Poeschla, E.M. COVID-19 Serosurveillance May Facilitate Return-to-Work Decisions. Am. J. Trop. Med. Hyg. 2020, 102, 1189–1190. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ray, S.; Chawla, N.; Gupta, A.; Maramaraj, K.K.; Kumar, S.; Anand, K.B. Return to work strategy with antibody-based tests in COVID19: An observational study from a metropolitan area, India. J. Mar. Med. Soc. 2020, 22, 46–50. [Google Scholar] [CrossRef]
- Saretto, G.; Bozzi, C. A proposal for the management of health surveillance and monitoring procedures in relation to the risks posed by SARS-COV-2 to hospital and nursing home workers, based on strategies implemented in the facilities of the Fondazione Opera San Camillo. G Ital. Med. Lav. Ergon. 2021, 43, 99–110. [Google Scholar]
- Leso, V.; Fontana, L.; Iavicoli, I. Susceptibility to Coronavirus (COVID-19) in Occupational Settings: The Complex Interplay between Individual and Workplace Factors. Int. J. Environ. Res. Public Health 2021, 18, 1030. [Google Scholar] [CrossRef]
- Huyck, K.L.; McDonough, C.M.; Kennedy, D.D.; Phillips, P.; Haig, A.J. Return to Work in the Pandemic—Considerations beyond Infection. PM R 2021, 13, 1044–1049. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. J. Clin. Epidemiol. 2009, 62, 1006–1012. [Google Scholar] [CrossRef]
- Schardt, C.; Adams, M.B.; Owens, T.; Keitz, S.; Fontelo, P. Utilization of the PICO framework to improve searching PubMed for clinical questions. BMC Med. Inform. Decis. Mak. 2007, 7, 16. [Google Scholar] [CrossRef] [Green Version]
- Available online: https://www.zotero.org/ (accessed on 11 January 2022).
- Available online: https://www.rayyan.ai/ (accessed on 11 January 2022).
- Microsoft Corporation. Microsoft Excel [Internet]. 2018. Available online: https://office.microsoft.com/excel (accessed on 15 March 2022).
- VOSVIEWER. Available online: https://www.vosviewer.com (accessed on 3 April 2022).
- Barriga Medina, H.R.; Campoverde Aguirre, R.; Coello-Montecel, D.; Ochoa Pacheco, P.; Paredes-Aguirre, M.I. The Influence of Work-Family Conflict on Burnout during the COVID-19 Pandemic: The Effect of Teleworking Overload. Int. J. Environ. Res. Public Health 2021, 18, 10302. [Google Scholar] [CrossRef] [PubMed]
- Brosseau, L.M.; Rosen, J.; Harrison, R. Selecting Controls for Minimizing SARS-CoV-2 Aerosol Transmission in Workplaces and Conserving Respiratory Protective Equipment Supplies. Ann. Work Expo Health 2021, 65, 53–62. [Google Scholar] [CrossRef] [PubMed]
- Calderwood, M.S.; Deloney, V.M.; Anderson, D.J.; Cheng, V.C.; Gohil, S.; Kwon, J.H.; Mody, L.; Monsees, E.; Vaughn, V.M.; Wiemken, T.L.; et al. Policies and practices of SHEA Research Network hospitals during the COVID-19 pandemic. Infect. Control. Hosp. Epidemiol. 2020, 41, 1127–1135. [Google Scholar] [CrossRef]
- Expósito-Delgado, A.J.; Ausina-Márquez, V.; Mateos-Moreno, M.V.; Martínez-Sanz, E.; Del Carmen Trullols-Casas, M.; Llamas-Ortuño, M.E.; Blanco-González, J.M.; Almerich-Torres, T.; Bravo, M.; Martínez-Beneyto, Y. Delivery of Health Care by Spanish Dental Hygienists in Private and Public Dental Services during the COVID-19 De-Escalation Phase (June 2020): A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2021, 18, 8298. [Google Scholar] [CrossRef]
- Ge, Y.; Zhang, W.B.; Wang, J.; Liu, M.; Ren, Z.; Zhang, X.; Zhou, C.; Tian, Z. Effect of different resumption strategies to flatten the potential COVID-19 outbreaks amid society reopens: A modeling study in China. BMC Public Health 2021, 21, 604. [Google Scholar] [CrossRef] [PubMed]
- Gross, D.P.; Asante, A.; Pawluk, J.; Niemeläinen, R. A Descriptive Study of the Implementation of Remote Occupational Rehabilitation Services Due to the COVID-19 Pandemic within a Workers’ Compensation Context. J. Occup. Rehabil. 2021, 31, 444–453. [Google Scholar] [CrossRef]
- Lichtman, A.; Greenblatt, E.; Malenfant, J.; Kuo, A. Universal symptom monitoring to address presenteeism in healthcare workers. Am. J. Infect. Control 2021, 49, 1021–1023. [Google Scholar] [CrossRef] [PubMed]
- Lu, Y.; Wu, J.; Peng, J.; Lu, L. The perceived impact of the Covid-19 epidemic: Evidence from a sample of 4807 SMEs in Sichuan Province, China. Environ. Hazards 2020, 19, 323–340. [Google Scholar] [CrossRef]
- Marzban, S.; Durakovic, I.; Candido, C.; Mackey, M. Learning to work from home: Experience of Australian workers and organizational representatives during the first Covid-19 lockdowns. J. Corp Real Estate 2021, 3, 203–222. [Google Scholar] [CrossRef]
- Onesti, C.E.; Rugo, H.S.; Generali, D.; Peeters, M.; Zaman, K.; Wildiers, H.; Harbeck, N.; Martin, M.; Cristofanilli, M.; Cortes, J.; et al. Oncological care organisation during COVID-19 outbreak. ESMO Open 2020, 5, e000853. [Google Scholar] [CrossRef]
- Pratama, M.R.; Supriyadi, A.; Sari, N. Assessment of Precautionary Measures against COVID-19 in Indonesian Workplaces. Int. J. Public Health Sci. 2021, 10, 281–288. [Google Scholar] [CrossRef]
- Robinson, J.; Kengatharan, N. Exploring the effect of Covid-19 on Small and Medium Enterprises: Early Evidence from Sri Lanka. J. Appl. Econ. Bus. Res. 2020, 10, 115–125. [Google Scholar]
- Salgarello, S.; Salvadori, M.; Mazzoleni, F.; Francinelli, J.; Bertoletti, P.; Audino, E.; Garo, M.L. The New Normalcy in Dentistry after the COVID-19 Pandemic: An Italian Cross-Sectional Survey. Dent. J. 2021, 9, 86. [Google Scholar] [CrossRef] [PubMed]
- Soneru, C.N.; Fernandez, A.M.; Bradford, V.; Staffa, S.J.; Raman, V.T.; Cravero, J.; Zurakowski, D.; Meier, P.M. Pediatric Anesthesia COVID-19 Collaborative. A survey of the global impact of COVID-19 on the practice of pediatric anesthesia: A study from the pediatric anesthesia COVID-19 Collaborative Group. Paediatr Anaesth. 2021, 31, 720–729. [Google Scholar] [CrossRef] [PubMed]
- Taylor, T.K.; Das, R.; Mueller, K.; Pransky, G.; Christian, J.; Orford, R.; Blink, R. Safely Returning America to Work: Part I: General Guidance for Employers. J. Occup. Environ. Med. 2020, 62, 771–779. [Google Scholar] [CrossRef]
- Taylor, T.K.; Das, R.; Mueller, K.L.; Pransky, G.S.; Harber, P.; McLellan, R.K.; Hartenbaum, N.P.; Behrman, A.J.; Roy, D.R.; Blink, R.C. Safely Returning America to Work Part II: Industry-Specific Guidance. J. Occup. Environ. Med. 2021, 63, e373–e391. [Google Scholar] [CrossRef]
- Tkatek, S.; Belmzoukia, A.; Nafai, S.; Abouchabaka, J.; Ibnou-Ratib, Y. Putting the world back to work: An expert system using big data and artificial intelligence in combating the spread of COVID-19 and similar contagious diseases. Work 2020, 67, 557–572. [Google Scholar] [CrossRef]
- Zhang, Q.; Wu, Y.; Li, M.; Li, L. Epidemic Prevention During Work Resumption: A Case Study of One Chinese Company’s Experience. Front. Public Health 2021, 21, 596332. [Google Scholar] [CrossRef]
- Zhao, J.; Jia, J.; Qian, Y.; Zhong, L.; Wang, J.; Cai, Y. COVID-19 in Shanghai: IPC Policy Exploration in Support of Work Resumption Through System Dynamics Modeling. Risk Manag. Healthc. Policy 2020, 13, 1951–1963. [Google Scholar] [CrossRef]
- Du, Y.; Liu, H. Analysis of the Influence of Psychological Contract on Employee Safety Behaviors against COVID-19. Int. J. Environ. Res. Public Health 2020, 17, 6747. [Google Scholar] [CrossRef]
- Frontera, J.A.; Yang, D.; Lewis, A.; Patel, P.; Medicherla, C.; Arena, V.; Fang, T.; Andino, A.; Snyder, T.; Madhavan, M.; et al. A prospective study of long-term outcomes among hospitalized COVID-19 patients with and without neurological complications. J. Neurol. Sci. 2021, 15, 117486. [Google Scholar] [CrossRef] [PubMed]
- Ganz-Lord, F.A.; Segal, K.R.; Rinke, M.L. COVID-19 symptoms, duration, and prevalence among healthcare workers in the New York metropolitan area. Infect. Control. Hosp. Epidemiol. 2021, 42, 917–923. [Google Scholar] [CrossRef] [PubMed]
- Griffiths, D.; Sheehan, L.; van Vreden, C.; Whiteford, P.; Collie, A. Returning to the Workplace during the COVID-19 Pandemic: The Concerns of Australian Workers. J. Occup. Rehabil. 2021, 31, 711–720. [Google Scholar] [CrossRef] [PubMed]
- Ladak, K.; Winthrop, K.; Marshall, J.K.; Gelfand, J.; Pope, J. Counselling patients for return to work on immunosuppression: Practices of Canadian specialists during the COVID-19 pandemic. Clin. Exp. Rheumatol. 2021, 39, 874–878. [Google Scholar] [PubMed]
- Lai, R.; Tan, L.; Lai, X.; Zhang, X.; Zhou, Q. Help-Seeking Behavior of Returning to Work in Healthcare Workers and its Influencing Factors During COVID-19 Subsiding. J. Occup. Environ. Med. 2020, 62, 898–903. [Google Scholar] [CrossRef]
- Liu, X.; Cheng, A.S.; Zeng, Y.; Zhang, X.; Peng, X.; Hu, H.; Li, H.; Feuerstein, M. Fears of COVID-19 and cancer recurrence related to work sustainability among male cancer survivors. J. Mens Health 2021, 17, 49–54. [Google Scholar]
- Liu, Z.; Van Egdom, D.; Flin, R.; Spitzmueller, C.; Adepoju, O.; Krishnamoorti, R. I Don’t Want to Go Back: Examining the Return to Physical Workspaces During COVID-19. J. Occup. Environ. Med. 2020, 62, 953–958. [Google Scholar] [CrossRef]
- Ly, D.P. Age, disability, and household composition of nurses and physicians who are not in the labor force. PLoS ONE 2021, 16, e0247967. [Google Scholar] [CrossRef]
- Mehrsafar, A.H.; Moghadam Zadeh, A.; Jaenes Sánchez, J.C.; Gazerani, P. Competitive anxiety or Coronavirus anxiety? The psychophysiological responses of professional football players after returning to competition during the COVID-19 pandemic. Psychoneuroendocrinology 2021, 129, 105269. [Google Scholar] [CrossRef]
- Mohammadi, F.; Radfar, M.; Hemmati Maslak Pak, M. Workplace challenges and nurses recovered from COVID-19. Nurs. Ethics 2021, 13, 9697330211020439. [Google Scholar] [CrossRef]
- Rex, D.K.; Vemulapalli, K.C.; Lahr, R.E.; McHenry, L.; Sherman, S.; Al-Haddad, M. Endoscopy Staff Are Concerned About Acquiring Coronavirus Disease 2019 Infection When Resuming Elective Endoscopy. Gastroenterology 2020, 159, 1167–1169.e3. [Google Scholar] [CrossRef] [PubMed]
- Rumrill, P.; Rumrill, S.; Sheppard-Jones, K.; Rumrill, A.; Graham-Smith, M.; Curry, B.; Wiley, L.; Fisher, E.; Kabeya, A.; Adams, C.; et al. Identifying the Job Accommodation Needs of American Workers with Mid-career Neurological Disabilities: A Multiple Case Study Investigation. J. Vocat Rehabil. 2021, 55, 115–129. [Google Scholar] [CrossRef]
- Tan, W.; Hao, F.; McIntyre, R.S.; Jiang, L.; Jiang, X.; Zhang, L.; Zhao, X.; Zou, Y.; Hu, Y.; Luo, X.; et al. Is returning to work during the COVID-19 pandemic stressful? A study on immediate mental health status and psychoneuroimmunity prevention measures of Chinese workforce. Brain Behav. Immun. 2020, 87, 84–92. [Google Scholar] [CrossRef] [PubMed]
- Vanichkachorn, G.; Newcomb, R.; Cowl, C.T.; Murad, M.H.; Breeher, L.; Miller, S.; Trenary, M.; Neveau, D.; Higgins, S. Post-COVID-19 Syndrome (Long Haul Syndrome): Description of a Multidisciplinary Clinic at Mayo Clinic and Characteristics of the Initial Patient Cohort. Mayo Clin. Proc. 2021, 96, 1782–1791. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Zhang, Y.; Guan, Y.; Ding, W.; Meng, Y.; Hu, H.; Liu, Z.; Zeng, X.; Wang, M. A nationwide evaluation of the prevalence of and risk factors associated with anxiety, depression and insomnia symptoms during the return-to-work period of coronavirus disease 2019 in China. Soc. Psychiatry Psychiatr Epidemiol. 2021, 56, 2275–2286. [Google Scholar] [CrossRef]
- Yang, Q.; Huo, J.; Li, J.; Jiang, Y. Research on the influence of the COVID-19 epidemic on work stress of returning workers in China: A study based on empirical analyses of industrial enterprises. Work 2020, 67, 67–79. [Google Scholar] [CrossRef]
- Yuan, Z.; Ye, Z.; Zhong, M. Plug back into work, safely: Job reattachment, leader safety commitment, and job engagement in the COVID-19 pandemic. J. Appl. Psychol. 2021, 106, 62–70. [Google Scholar] [CrossRef]
- Zanghì, A.; D’Amico, E.; Luca, M.; Ciaorella, M.; Basile, L.; Patti, F. Mental health status of relapsing-remitting multiple sclerosis Italian patients returning to work soon after the easing of lockdown during COVID-19 pandemic: A monocentric experience. Mult. Scler. Relat. Disord. 2020, 46, 102561. [Google Scholar] [CrossRef]
- Zheng, N.; Zhang, T.; Liu, Y.; Zhu, X.Q. Investigation of the Status of Nurses Returning to Work After Recovering From COVID-19 and Influencing Factors. J. Nurs. Care Qual. 2021, 36, E1–E6. [Google Scholar] [CrossRef]
- Cariani, L.; Orena, B.S.; Ambrogi, F.; Gambazza, S.; Maraschini, A.; Dodaro, A.; Oggioni, M.; Orlandi, A.; Pirrone, A.; Uceda Renteria, S.; et al. Time Length of Negativization and Cycle Threshold Values in 182 Healthcare Workers with Covid-19 in Milan, Italy: An Observational Cohort Study. Int. J. Environ. Res. Public Health 2020, 17, 5313. [Google Scholar] [CrossRef]
- Domeracki, S.; Clapp, R.N.; Taylor, K.; Lu, C.M.; Lampiris, H.; Blanc, P.D. Cycle Threshold to Test Positivity in COVID-19 for Return to Work Clearance in Health Care Workers. J. Occup. Environ. Med. 2020, 62, 889–891. [Google Scholar] [CrossRef] [PubMed]
- Garzaro, G.; Clari, M.; Ciocan, C.; Grillo, E.; Mansour, I.; Godono, A.; Borgna, L.G.; Sciannameo, V.; Costa, G.; Raciti, I.M.; et al. COVID-19 infection and diffusion among the healthcare workforce in a large university-hospital in northwest Italy. Med. Lav. 2020, 111, 184–194. [Google Scholar] [CrossRef] [PubMed]
- Gombar, S.; Chang, M.; Hogan, C.A.; Zehnder, J.; Boyd, S.; Pinsky, B.A.; Shah, N.H. Persistent detection of SARS-CoV-2 RNA in patients and healthcare workers with COVID-19. J. Clin. Virol. 2020, 129, 04477. [Google Scholar] [CrossRef] [PubMed]
- González Martin-Moro, J.; Chamorro Gómez, M.; Dávila Fernández, G.; Elices Apellaniz, A.; Fernández Hortelano, A.; Guzmán Almagro, E.; Herranz Varela, A.; Izquierdo Rodríguez, C.; Molina Montes, B.; Sánchez Moreno, G.V.; et al. Survival analysis of time to SARS-CoV-2 PCR negativisation to optimise PCR prescription in health workers: The Henares COVID-19 healthcare workers cohort study. Occup. Environ. Med. 2021, 78, 638–642. [Google Scholar] [CrossRef]
- Guarnieri, V.; Moriondo, M.; Giovannini, M.; Lodi, L.; Ricci, S.; Pisano, L.; Barbacci, P.; Bini, C.; Indolfi, G.; Zanobini, A.; et al. Surveillance on Healthcare Workers During the First Wave of SARS-CoV-2 Pandemic in Italy: The Experience of a Tertiary Care Pediatric Hospital. Front. Public Health 2021, 9, 644702. [Google Scholar] [CrossRef]
- Pan, S.C.; Hsu, M.C.; Chang, H.H.; Wang, J.T.; Lai, Y.L.; Chen, P.C.; Chang, S.Y.; Sheng, W.H.; Chen, Y.C.; Chen, S.C.; et al. Prospective health surveillance for COVID-19 among health care workers at a university medical center in Taiwan, January to June 2020. J. Formos Med. Assoc. 2021, 23, S0929–S6646. [Google Scholar] [CrossRef]
- Porru, S.; Carta, A.; Monaco, M.G.L.; Verlato, G.; Battaggia, A.; Parpaiola, M.; Lo Cascio, G.; Pegoraro, M.; Militello, V.; Moretti, F.; et al. Health Surveillance and Response to SARS-CoV-2 Mass Testing in Health Workers of a Large Italian Hospital in Verona, Veneto. Int. J. Environ. Res. Public Health 2020, 17, 5104. [Google Scholar] [CrossRef]
- Rivett, L.; Sridhar, S.; Sparkes, D.; Routledge, M.; Jones, N.K.; Forrest, S.; Young, J.; Pereira-Dias, J.; Hamilton, W.L.; Ferris, M.; et al. Screening of healthcare workers for SARS-CoV-2 highlights the role of asymptomatic carriage in COVID-19 transmission. Elife 2020, 9, e58728. [Google Scholar] [CrossRef]
- Shenoy, E.S.; West, L.R.; Hooper, D.C.; Sheehan, R.R.; Hashimoto, D.; Boukus, E.R.; Aurora, M.N.; McEvoy, D.S.; Klompas, M. Healthcare worker infection with SARS-CoV-2 and test-based return to work. Infect. Control. Hosp. Epidemiol. 2020, 41, 1464–1466. [Google Scholar] [CrossRef]
- Tripathy, D.; Roy, A.K.; Khanna, R.C.; Jalali, S.; Panigrahy, B.; Parija, D.C.; Rath, S. Point-of-care rapid antigen testing for COVID-19 at a tertiary eye care facility: Role in commencement of elective surgeries, contact tracing and implementation of back-to-work policy. Indian J. Ophthalmol. 2021, 69, 964–970. [Google Scholar] [CrossRef]
- Villarreal, J.; Nieto, S.V.; Vázquez, F.; Del Campo, M.T.; Mahillo, I.; de la Hoz, R.E. Time to a Negative SARS-CoV-2 PCR Predicts Delayed Return to Work After Medical Leave in COVID-19 Infected Health Care Workers. J. Occup. Environ. Med. 2021, 63, 970–974. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Li, G.; He, J.; Cao, D.; Tian, J. The Smart Safeguard System for COVID-19 to prevent cluster-infection in workplaces. J. Infect. Public Health 2021, 14, 1042–1044. [Google Scholar] [CrossRef] [PubMed]
- Niu, Q.; Nagata, T.; Fukutani, N.; Tezuka, M.; Shimoura, K.; Nagai-Tanima, M.; Aoyama, T. Health effects of immediate telework introduction during the COVID-19 era in Japan: A cross-sectional study. PLoS ONE 2021, 8, e0256530. [Google Scholar] [CrossRef] [PubMed]
- Wood, S.J.; Michaelides, G.; Inceoglu, I.; Hurren, E.T.; Daniels, K.; Niven, K. Homeworking, Well-Being and the COVID-19 Pandemic: A Diary Study. Int. J. Environ. Res. Public Health 2021, 18, 7575. [Google Scholar] [CrossRef] [PubMed]
- Radonić, M.; Vukmirović, V.; Milosavljević, M. The Impact of Hybrid Workplace Models on Intangible Assets: The Case of an Emerging Country. Amfiteatru Econ. 2021, 23, 770–786. [Google Scholar]
- World Health Organization. Telemedicine: Opportunities and developments in Member States: Report on the second global survey on eHealth 2009. (Global Observatory for eHealth Series, 2). 2010. Available online: https://www.who.int/goe/publications/goe_telemedicine_2010.pdf (accessed on 30 January 2022).
- Ashry, A.H.; Alsawy, M.F. Doctor-patient distancing: An early experience of telemedicine for postoperative neurosurgical care in the time of COVID-19. Egypt J. Neurol. Psychiatr. Neurosurg. 2020, 56, 80. [Google Scholar] [CrossRef]
- Salazar, M.Á.; Chavez-Galan, L.; Castorena-Maldonado, A.; Mateo-Alonso, M.; Diaz-Vazquez, N.O.; Vega-Martínez, A.M.; Martínez-Orozco, J.A.; Becerril-Vargas, E.; Sosa-Gómez, F.M.; Patiño-Gallegos, H.; et al. Low Incidence and Mortality by SARS-CoV-2 Infection Among Healthcare Workers in a Health National Center in Mexico: Successful Establishment of an Occupational Medicine Program. Front. Public Health 2021, 13, 651144. [Google Scholar] [CrossRef]
- Trivedy, C.; Mills, I.; Dhanoya, O. The impact of the risk of COVID-19 on Black, Asian and Minority Ethnic (BAME) members of the UK dental profession. Br. Dent. J. 2020, 228, 919–922. [Google Scholar] [CrossRef]
- Banaee, S.; Claiborne, D.M.; Akpinar-Elci, M. Occupational health practices among dental care professionals before and during the COVID-19 pandemic. Work 2021, 68, 993–1000. [Google Scholar] [CrossRef]
- Manucci, M. How People Come Back to Workplaces during the Pandemic: Three dimensions of intervention for new emotional performance conditions. Hum. Resour. Dev. Int. 2021, 4, 446–453. [Google Scholar] [CrossRef]
- Sarihasan, I.; Oláh, J.; Al-Dalahmeh, M.; Yousuf, A.; Dajnoki, K. Determining the importance of high-reliability healthcare organizations during the Covid-19 pandemic: Evidence from healthcare workers in Turkey. Probl. Perspect. Manag. 2021, 19, 345–355. [Google Scholar] [CrossRef]
- Sizemore, L.M.; Peganoff-O’Brien, S.; Skubik-Peplaski, C. Interference: COVID-19 and the Impact on Potential and Performance in Healthcare. Work 2021, 69, 767–774. [Google Scholar] [CrossRef] [PubMed]
- Trivedi, A.; Fontelera, M.; Ishak, N.; Lai, A.; Win, K.N.; Ismail, K.; Koh, D. Healthcare workers’ preparedness and response during COVID-19 pandemic. Proc. Singap. Healthc. 2021. [Google Scholar] [CrossRef]
- Soriano, J.B.; Murthy, S.; Marshall, J.C.; Relan, P.; Diaz, J.V. WHO Clinical Case Definition Working Group on Post-COVID-19 Condition. A clinical case definition of post-COVID-19 condition by a Delphi consensus. Lancet Infect. Dis. 2021, 21, S1473–S3099. [Google Scholar] [CrossRef]
- Asadi-Pooya, A.A.; Akbari, A.; Emami, A.; Lotfi, M.; Rostamihosseinkhani, M.; Nemati, H.; Barzegar, Z.; Kabiri, M.; Zeraatpisheh, Z.; Farjoud-Kouhanjani, M.; et al. Long COVID syndrome-associated brain fog. J. Med. Virol. 2021, 21, 979–984. [Google Scholar] [CrossRef] [PubMed]
- Fan, C.Y.; Fann, J.C.; Yang, M.C.; Lin, T.Y.; Chen, H.H.; Liu, J.T.; Yang, K.C. Estimating global burden of COVID-19 with disability-adjusted life years and value of statistical life metrics. J. Formos. Med. Assoc. 2021, 120 (Suppl. 1), S106–S117. [Google Scholar] [CrossRef]
- Brown, N.; Nicholson, J.; Campbell, F.K.; Patel, M.; Knight, R.; Moore, S. COVID-19 Post-lockdown: Perspectives, implications and strategies for disabled staff. Alter-Eur. J. Disabil. Res. 2021, 15, 262–269. [Google Scholar] [CrossRef]
- Jones, J.M.; Saeed, H.; Katz, M.S.; Lustberg, M.B.; Forster, V.J.; Nekhlyudov, L. Readdressing the Needs of Cancer Survivors During COVID-19: A Path Forward. J. Natl. Cancer Inst. 2021, 113, 955–961. [Google Scholar] [CrossRef]
- Scheid, J.L.; Lupien, S.P.; Ford, G.S.; West, S.L. Commentary: Physiological and Psychological Impact of Face Mask Usage during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2020, 17, 6655. [Google Scholar] [CrossRef]
- Iddins, B.O.; Waugh, M.H.; Buck, B.; Cato, T.; Graham, D.E.; Attia, K.; Jones, D.; Partin, A.; Shourbaji, R.; Wesh, C. Benchmarking SARS CoV-2 Infection in the Workplace to Support Continuity of Operations. J. Occup. Environ. Med. 2021, 63, 548–556. [Google Scholar] [CrossRef]
- Oliveira, B.A.; Oliveira, L.C.; Sabino, E.C.; Okay, T.S. SARS-CoV-2 and the COVID-19 disease: A mini review on diagnostic methods. Rev. Inst. Med. Trop. Sao Paulo 2020, 62, e44. [Google Scholar] [CrossRef] [PubMed]
- Makoah, N.A.; Tipih, T.; Litabe, M.M.; Brink, M.; Sempa, J.B.; Goedhals, D.; Burt, F.J. A systematic review and meta-analysis of the sensitivity of antibody tests for the laboratory confirmation of COVID-19. Future Virol. 2021, 17, 119–139. [Google Scholar] [CrossRef] [PubMed]
- Rostami, A.; Sepidarkish, M.; Leeflang, M.M.G.; Riahi, S.M.; Nourollahpour Shiadeh, M.; Esfandyari, S.; Mokdad, A.H.; Hotez, P.J.; Gasser, R.B. SARS-CoV-2 seroprevalence worldwide: A systematic review and meta-analysis. Clin. Microbiol. Infect. 2021, 27, 331–340. [Google Scholar] [CrossRef] [PubMed]
- Böger, B.; Fachi, M.M.; Vilhena, R.O.; Cobre, A.F.; Tonin, F.S.; Pontarolo, R. Systematic review with meta-analysis of the accuracy of diagnostic tests for COVID-19. Am. J. Infect. Control. 2021, 49, 21–29. [Google Scholar] [CrossRef] [PubMed]
- Gao, Z.; Xu, Y.; Sun, C.; Wang, X.; Guo, Y.; Qiu, S.; Ma, K. A systematic review of asymptomatic infections with COVID-19. J. Microbiol. Immunol. Infect. 2021, 54, 12–16. [Google Scholar] [CrossRef]
- Lucan, S.C.; Goodwin, S.K.; Lozano, M.; Pak, S.; Freitas, M. Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) testing for essential food production workers: Evolving thinking, pilot testing, and lessons learned. Public Health 2021, 197, 56–62. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Authors, Year | Country | Setting | Sample Size | Study Design | Aim of the Study | Main Findings |
|---|---|---|---|---|---|---|
| Barriga Medina HR et al., 2021 [46] | Ecuador | Teleworkers in Guayaquil, Ecuador. | 1044 Teleworkers | Cross-sectional | To analyse the impact of work-family conflict on burnout and work overload in teleworkers during the COVID-19 pandemic. | Teleworkers are involved in high levels of work-family conflict; the impact of the work-family conflict manifested primarily in greater exhaustion; no effect of teleworking overlwork-familywork–family conflict and burnout relationship. |
| Brosseau LM et al., 2020 [47] | USA | Healthcare (Ophthalmologist) and Non-Healthcare settings (transportation and warehouse workers, police patrol officer) | N/A | Modelling study | To describe how a control banding model is applicable to the current COVID-19 pandemic and illustrate, using several case examples, how decisions about workplace controls for aerosol transmission are facilitated by this model and can inform the safe reopening of workplaces. | The using control banding for workers at high risk of exposure in the Return to Work (RTW) phase is unhelpful to develop effective infection and disease prevention programs. |
| Calderwood MS et al., 2020 [48] | USA | USA and International Healthcare Facilities | 95 Healthcare Facilities | Cross-sectional | To obtain an aggregated picture of healthcare facilities’ approaches to mitigating COVID-19 transmission risk. | Variation in the isolation precautions used for specific procedures during the COVID-19 pandemic was higher than expected among healthcare facilities dealing with other viral respiratory pathogens. Moreover, the authors reported that healthcare facilities followed the Centers for Disease Control and Prevention (CDC) non-test-based return-to-work criteria for more than a half (52%) |
| Expósito-Delgado et al., 2021 [49] | Spain | Spanish dental hygienists | 517 Dental Hygienists | Cross-sectional | To describe dental hygienists’ work status and employment patterns during RTW | 86.2% followed the official recommendations to avoid contagion; 63.8% agreed with the gradual RTW by limiting the use of the aerosols; private dental hygienists identified more with RTW without restrictions (14.5%) versus those working for public service (1.2%) |
| Ge Y et al., 2021 [50] | China | China’s Business Enterprises | Not specified | Modelling study | To investigate the effects of different resumption strategies on COVID-19 transmission using a Susceptible–Exposed–Infectious–Removed (SEIR) model. | The hierarchy-based reopen strategy performed best when current pandemic prevention measures were maintained save for lockdown, reducing the peak number of active cases (50%) and cumulative cases (44%) |
| Gross DP et al., 2020 [51] | Canada | Workers’ Compensation Board of Alberta | 4516 Injured Workers | Cross-sectional | To describe the transition to remote occupational rehabilitation services in response to the COVID-19 pandemic. | Workers using remote assessments were significantly less likely to be judged as ready to return to pre-accident functional work levels and more likely to be recommended modified work duties. The number of completed rehabilitation programs also reduced. |
| Lichtman A et al., 2021 [52] | USA | Healthcare Settings in California | 5035 Health Workers (HWs) | Modelling study | To outline an effective strategy for rapid implementation of a symptom monitoring system to integrate into an adaptable model | 1318 HWs had been identified as being symptomatic with testing indication. A total of 82% reported not currently staying home from work due to illness or quarantine, consistent with the high rates of ‘presenteeism’ reported in HWs. |
| Lu Y et al., 2020 [53] | China | Small and Medium Enterprises (SME) in Sichuan’s | 4087 workers | Cross-sectional | To assess the challenges associated with work resumption and the related policy requirements. | SMEs were unable to resume work for several reasons, including a shortage of pandemic mitigation materials, the inability of employees to RTW, disrupted supply chains, and reduced market demand. |
| Marzban S et al., 2021 [54] | Australia | 28 Australian organisations | 301 employees | Cross-sectional | To describe the homeworking experience during the Australian lockdown in the middle of the COVID-19 pandemic, and to inform organisations, employees and the design of the workspaces post-2020. | Organisations reported a homeworking increase (more than 50%) and indicated employees’ productivity as the biggest concern in remote working. Employees were more concerned about their social interactions, internet connectivity, and increased workload challenges and disclosed that face-to-face interactions with their colleagues were the most important reason to return to the office. |
| Onesti CE et al., 2021 [55] | USA/Europe | Oncological Centres in Europe and USA | 30 Oncological Units | Cross-sectional | To assess how oncology centres reacted to the health crisis related to the COVID-19 pandemic to improve oncological care and implement preventive measures. | Triage for patients with cancer was conducted before a hospital or clinic visit (90.5%), before daycare admissions (95.2%), and before overnight hospitalisation. Separated pathways for COVID-19-positive/-negative patients were organised, and permission for caregivers to attend clinic visits was limited. Telemedicine was implemented in 76.2% of the centres. RTW policies required a negative swab test in 76.2% of the centres |
| Pratama MR et al., 2021 [56] | Indonesia | Indonesian Companies (Healthcare excluded) | 106 Participants | Cross-sectional | To assess the measures taken against the COVID-19 pandemic in workplaces. | Almost all enrolled participants have already developed the specific COVID-19 policy. A total of 91% reported a specific emergency response team and communication centre for COVID-19 at the workplace, but only 42.7% performed an emergency drill for COVID-19 cases. A total of 95.1% of the participants implemented flexible worksites and work hours to maximise the physical distancing among the workers. |
| Robinson J et al., 2020 [57] | Sri Lanka | Small and Medium Enterprises (SME) | 14 SME operators | Cross-sectional | To explore the effects of the COVID-19 pandemic on SMEs in Sri Lanka | Some managers’ practices, such as a four-day workweek, work sharing, half-time working, etc., might help the SMEs to remain open; in addition to management local actions, Government should establish health and safety measures to ensure minimal virus diffusion at the workplace, formulating the right policies and guidelines to support the SMEs. |
| Salgarello S et al., 2021 [58] | Italy | Italian Dentists | 1028 Dentists | Cross-sectional | To understand the procedures that were adopted in the second phase of the COVID-19 pandemic and to evaluate the dentists’ expectations and concerns about returning to normalcy | A total of 83% of Italian dentists fully restarted their activities after the lockdown, with a resumption significantly marked in northern and central Italy than in the south. Over 80% adopted the recommended precautional guidelines, modifying them according to the specific dental treatment. Additionally, 50% were confident in returning to normalcy after the COVID-19 crisis |
| Soneru et al., 2021 [59] | USA | Paediatric Anaesthesiology Staff Worldwide | 63 Institutions | Cross-sectional | To determine how COVID-19 directly impacted paediatric anaesthesia practices during September/October 2020 | N95 masks were available to anaesthesia teams at 91% of institutions. COVID-19 testing criteria of anaesthesia staff and RTW guidelines varied by institution. Structured simulation training aimed at improving COVID-19 safety and patient care at 62% of institutions. A total of 31% declared a voluntary option to not work with COVID-19-positive cases |
| Taylor TK et al., 2020 [60] | USA | ACOEM | N/A | Guideline | To provide RTW guidance for employers and the OPs supporting businesses in implementing safe strategies—Part I: General Guidance for Employers. | Transition phase analysis: RTW policies proposal. Employers will need to facilitate the safe return of employees through evaluation, testing, work modifications, and the development of appropriate workplace policies. |
| Taylor TK et al., 2021 [61] | USA | ACOEM | N/A | Guideline | To provide RTW guidance for both employers and the OPS who will be supporting businesses in implementing safety measures —Part II: Industry-Specific Guidance. | Special considerations for the food industry, general office settings/warehouses, retail, healthcare, long-term care facilities, transportation and travel, construction, marine and offshore industries |
| Tkatek S et al., 2020 [62] | Morocco | Morocco’s Research Team System Expert | N/A | Modelling study | To develop an expert system that combines several solutions to combat COVID-19 | The authors developed a methodology based on a new expert system allowing them to explore, monitor, forecast, and optimise the data collected to assist in stopping the spread of COVID-19 and make an efficient decision regarding RTW. |
| Zhang Q et al., 2021 [63] | China | A Chinese enterprise | 500 Employees | Case Model Study | To elaborate pandemic prevention measures in a Chinese company during the RTW stage. | Description of RTW measures (i.e., Employee Information Report, Flexible Work Resumption, Health Education); the authors underlined three preconditions that could influence the RTW phase (social culture; national/local OSH-regulation and temporary guidelines for pandemic prevention; OSH practice, resources, and physical environment at the company level) |
| Zhao et al., 2020 [64] | China | National Health Commission of the People’s Republic of China; the Shanghai Municipal Health Commission | Not specified | Modelling study | To estimate the COVD-19 transmission dynamics under various COVID-19 prevention and control policies and offer evidence-based outcomes for RTW policies. | The authors highlighted 4 RTW policy approaches to prevent a secondary COVID-19 outbreak. The combination of quarantined and staged approaches is the most conservative and safest policy from a disease control perspective. The dynamic systems model designed in the study can serve as a tool to test various RTW policies, facilitating decision-making in responses to combating the COVID-19 pandemic. |
| Authors, Year | Country | Setting | Sample Size | Study Design | Aim of the Study | Main Findings |
|---|---|---|---|---|---|---|
| Du Y et al., 2020 [65] | China | Manufacturing and Service Industries | 402 Workers | Cross-sectional | To explore the impact of the psychological contract on employees’ safety behaviour and provide preventive suggestions for combating the global spread of COVID-19. | The psychological contract and perceived insider status positively promote employees’ safety behaviour, while job burnout negatively affects it. The results show that employees’ conscious participation in safety behaviour plays an irreplaceable role in preventing COVID-19 and the safety of work resumption. |
| Frontera et al., 2021 [66] | USA | 4 New York City hospitals | 606 patients | Cohort study | Primary aim: To compare global functional outcomes between COVID-19 hospital survivors with and without neurological complications. Secondary purpose: To assess activities of daily living, Return to Work (RTW), cognitive function, anxiety, depression, fatigue and sleep abnormalities in COVID-19 hospital survivors with and without neurological complications | Patients with neurological complications were less likely to RTW than controls. Long-term functional outcomes would be worse among patients with neurological complications compared to age, gender and severity of illness-matched COVID-19 rules without neurological complications. |
| Ganz-Lord FA et al., 2020 [67] | USA | Montefiore Medical Center (New York City) | 1698 Health Workers (HWs) | Cohort study | To evaluate symptoms, workforce implications, and testing patterns related to the COVID-19 pandemic among HWs. | From symptom onset until RTW, the median time for HWs who did not require hospitalisation was 15 days. Shortness of breath, fever, sore throat, and diarrhoea were significantly associated with longer durations from symptom onset to RTW. Among symptomatic HWs who had Real-time Polymerase Chain Reaction (Rt-PCR) testing during the study period, 51.9% tested positive. |
| Griffiths D et al., 2021 [68] | Australia | Australian Workers | 1169 Workers | Cross-sectional | To determine the nature and prevalence of workers’ concerns regarding workplace reopening and to identify characteristics of workers and industries where particular concerns are more common | 82.4% of workers reported concerns about workplace infection risk (common for HWs, retail, and accommodation/food service industries), and 53.4% reported concerns about work and home life (common for female workers, partners/spouses with dependent children). The prevalence of concerns is related to work and responsibilities at home. Actions that reduce the risk of workplace transmission, coupled with effective communication of infection controls, may alleviate worker concerns whilst recognising workers’ family and social circumstances. |
| Ladak et al., 2021 [69] | Canada | Canadian Rheumatology, Gastroenterology and Dermatology Associations | 151 Physicians | Cross-sectional | To determine how physicians who frequently prescribe immunosuppressive medications are counselling patients on RTW before widespread vaccine distribution | 94% were asked for RTW advice, and 33% felt informed enough to provide counselling. When patients requested a medical note, physicians provided one 25% of the time; among the most associated with notes were patient comorbidities, high-risk work, and vulnerable co-inhabitants. Conventional synthetic and biologic immunosuppressants did not prompt most physicians to provide a message. Respondents considered patient perspectives and workplace factors. |
| Lai R et al., 2020 [70] | China | Wuhan’s Hospital | 861 HWs | Cross-sectional | To explore the level and influencing factors of help-seeking behaviour of returning to work in HWs. | More help-seeking was reported in HWs who had encountered problems after return, worked in a hospital before RTW, received Computerised Tomography scans and blood routine examination, had relatives or friends diagnosed or suspected as COVID-19, not a doctor, higher education and title, elder age, and single status. |
| Liu X et al., 2021 [71] | China | Hunan Cancer Hospital in Changsha | 121 employed male cancer survivors | Cross-sectional | To explore whether fear of COVID-19 and fear of cancer recurrence are related to the likelihood of remaining at work following treatment in male cancer survivors. | Fear of COVID-19 and fear of cancer recurrence were negatively correlated with work sustainability. Significant interaction effects were observed between fear of COVID-19 and fear of cancer recurrence. Advanced disease stage, radiation therapy, and recently completed cancer treatment were all factors related to lower work sustainability scores. |
| Liu Z et al., 2020 [72] | USA | Industry Associations in the Energy Sector | 333 Workers | Cross-sectional | To inform employers’ and policy makers’ decision making around the RTW during COVID-19. | Women, non-Caucasians, and employees living in multi-generational households were less willing to RTW. Childcare concerns were negatively related to willingness to return, whereas organisational strategies for mitigating COVID-19 transmission at work were positively associated with willingness to return. |
| Ly DP, 2021 [73] | USA | American Community Survey 2014–2018 5-year file | 189,521 nurses; 51,834 physicians | Cross-sectional | To analyse age, disability, and household composition of nurses and physicians not in the workforce, highlighting the higher risk of COVID-19 related morbidity and mortality if exposed. | Over ¾ of nurses and physicians not in the labour force are aged 55, and about 15% have a disability. For female nurses and physicians not in the labour force, over half of those ages 20–54 had a child under 15 at home, and over half of those ages, 65+ had another adult 65 and over at home. These characteristics may present challenges and risks to returning. |
| Mehrsafar et al., 2021 [74] | Iran | Iranian Football League | 90 Professional Football Players | Cross-sectional | To examine the relationship between competitive anxiety, fear/anxiety of COVID-19, and autonomic and endocrine stress responses in professional football players after returning to competition during the COVID-19 pandemic. | Somatic–cognitive anxiety is correlated with fear/anxiety of COVID-19 and the competition responses of salivary alpha-amylase and salivary cortisol. |
| Mohammadi F et al., 2021 [75] | Iran | Urmia Hospitals | 14 Nurses | Cross-sectional | To determine the workplace challenges faced by nurses who had recovered from COVID-19. | The authors overviewed the challenges faced by the nurses after their RTW, such as declined ethical values, fear of re-infection, forgotten patients, gradually leaving the job, and corona-phobia. |
| Rex DK et al., 2020 [76] | USA | Endoscopy staff | 106 HWs | Cross-sectional | To investigate the concerns of endoscopy staff regarding their risk of acquiring COVID-19 by returning to work. | Assuming no change in infection control measures, 66% were very or somewhat concerned about RTW. Four respondents preferred daily COVID-19 testing, 49 preferred weekly tests, and 47 said it did not matter. Assuming pre-COVID-19 infection control measures, endoscopists were more often unwilling to RTW compared to nonphysician staff (80% vs. 30%). After instituting new protective measures viewed as critical, 35% remained very or somewhat concerned. Wearing masks has resulted in the best preventive practice for 100% of endoscopists. |
| Rumrill P et al., 2021 [77] | USA | U.S. Dept. of Labor Office of Disability Employment Policy | 4 Disable Workers | Cross-sectional | To demonstrate the use of a psychometrically sound assessment instrument and resource-driven planning procedure to help workers with disabilities resume or retain their employment. | Regarding RTW, for employees with neurological disabilities in the post-COVID-19 era, one potentially positive outcome of the pandemic may be that home-working will be more readily available, not only as a reasonable accommodation but also as an alternative for more significant numbers of employees than ever before. |
| Tan W et al., 2020 [78] | China | Chongqing enterprises | 1323 Workers | Cross-sectional | To quantify the immediate psychological effects and identify preventive measures that determine the mental health of the workforce members returning to work. | RTW had not caused a high level of psychiatric symptoms, probably due to confidence instilled by psychoneuroimmunity prevention measures before the resumption of work. Low prevalence of anxiety, depression, stress and insomnia is reported, while 10.8% of workers received a Post-Traumatic Stress Disorder (PTSD) diagnosis after RTW. The severity of psychiatric symptoms was associated with marital status, presence of a physical sign, poor physical health and viewing RTW as a health hazard. There were no significant differences in the severity of psychiatric symptoms between workers/technicians and executives/managers; >95% reported psychoneuroimmunity prevention measures and were associated with less severe psychiatric symptoms. |
| Vanichkachorn G et al., 2021 [79] | USA | COVID-19 Activity Rehabilitation Program at Mayo Clinic | 100 Patients | Cohort study | To describe characteristics of a series of patients reporting prolonged symptoms after infection with coronavirus. | Only 1 in 3 patients had returned to unrestricted work duty at the time of analysis. More than one-third of patients (34%) reported difficulties performing basic activities of daily living. Most of them required physical therapy, occupational therapy, or brain rehabilitation. |
| Wang S et al., 2021 [80] | China | Multicenter, Nationwide | 42,000 Workers | Cross-sectional | To evaluate the prevalence of and risk factors associated with anxiety, depression, and insomnia symptoms during the RTW period in China. | Generally, 18.3, 14.9, and 17.9% of the participants had anxiety, depression, and insomnia symptoms, respectively, and 2.2–2.7% had severe symptoms. Engaging in outside activity once in ≥ 30 days and age 50–64 years were common risk factors for anxiety, depression and insomnia symptoms. Living in Hubei Province was a common risk factor for anxiety and insomnia symptoms. Working as frontline medical staff was another risk factor for anxiety symptoms. |
| Yang Q et al., 2020 [81] | China | Industrial Enterprises | 526 Workers | Cross-sectional | To explore the impact of psychosocial stress caused by the COVID-19 pandemic on the work stress of returned workers and the boundary conditions for reducing work stress from the perspectives of perceived organisational support, perceived social support and pandemic awareness. | Psychosocial stress had a significant positive effect on employees’ work stress, whether in severe pandemic areas or non-severe pandemic areas; perceived organisational support can alleviate the impact of psychosocial stress on work stress. The moderating effect of pandemic awareness was only established in non-severe pandemic areas. |
| Yuan Z et al., 2021 [82] | China | Wuhan’s workers | 485 participants | Cross-sectional | To investigate job reattachment as an antecedent of job engagement | Job reattachment in preparation for returning to work was related to greater levels of job engagement, which was associated with lower levels of work withdrawal and higher levels of personal protective equipment use and task performance. |
| Zanghì A et al., 2020 [83] | Italy | Tertiary Multiple Sclerosis Center in Catania, Italy | 672 Patients | Cross-sectional | To assess the mental health status and RTW of multiple sclerosis patients. | RTW was associated with the presence of psychiatric concerns higher in patients who have started/switched disease-modifying treatment in the last 12 months or those with higher levels of disability. A total of 31.8% of patients resulted in clinically significant PTSD-like symptoms. Moderate-to-severe anxiety was reported by 48.6% of patients, while moderate-to-severe depression and moderate-to-severe stress were, respectively, reported by 22% and 50.9% of patients. |
| Zheng N et al., 2021 [84] | China | Healthcare setting in Hubei Province | 83 Nurses | Cross-sectional | To understand the adaptation status of nurses after recovering from COVID-19 during RTW. | The working adaptation status of infected nurses resulted in a medium level; they had difficulties adapting to the fast pace of work after RTW and decreased concentration on their work. Age, marital status, hospital grade and type, work department, job title, and educational background had no significant effects on nurses’ job adaptability after RTW. |
| Authors, Year | Country | Setting | Sample Size | Study Design | Aim of the Study | Main Findings |
|---|---|---|---|---|---|---|
| Cariani L et al., 2020 [85] | Italy | Ca’ Granda Ospedale Maggiore Policlinico in Milan, Italy | 182 health workers (HWs) | Cohort study | To evaluate the time length of negativisation from HWs’ symptoms onset significant variations in cycle threshold (Ct) values and gene positivity among positive individuals who returned to work. | The median time length of negativisation was four weeks (35% symptomatic Vs 40% asymptomatic). Three-gene positivity had the most significant variability and increasing Ct values from single- to three-gene positivity among all age groups was observed. Self-isolation of longer than two weeks and prolonged follow-up periods could be the most suitable to reduce the SARS-CoV-2 spread. |
| Domeracki S et al., 2020 [86] | USA | San Francisco Veterans Affairs Health Care System | 12 HWs | Cross-sectional | To ascertain whether real-time polymerase chain reaction (Rt-PCR) cycle amplifications until detection, the cycle threshold (Ct), could help inform RTW strategies for HWs recovering from COVID-19 infection. | Time elapsed until Rt-PCR test-based RTW clearance ranged from 7 to 57 days (median, 34.5 days). Lower initial Ct correlated with the total time elapsed until clearance. Thus, considering the Rt-PCR Ct, which correlates with the estimated viral load, may help inform return to work (RTW) planning and decision making. |
| Garzaro G. et al., 2020 [87] | Italy | Città della Salute e della Scienza di Torino University- Hospital in Turin, Italy | 2,411 HWs | Cross sectional | To evaluate the early impact of structured risk management for exposed COVID-19 HWs and describe how their characteristics contributed to infection and diffusion. | Among 830 HWs who were at ‘high/medium risk’, 9.6% tested positive. Physicians and non-medical services resulted in an increased risk. Patient care did not increase the risk but sharing the work environment did. HWs with management positions were the main source of infection due to the high number of interactions. |
| Gombar S at al., 2020 [88] | USA | Stanford Healthcare | 63 HWs / 87 patients | Cohort study | To understand the appropriate length of symptom to determine RTW and contact precaution strategies. | The average time to transition from Rt-PCR positive to negative was 24 days after symptom onset. A total of 20% of individuals remain Rt-PCR positive for more than one month from symptom onset, and 10% of the patients did not have a negative test until after 33 days had passed. These findings suggest that the fixed length of time before returning to work be revised to over one month. |
| González Martin -Moro G et al., 2021 [89] | Spain | Henares University Hospital in Coslada, Madrid, Spain | 374 HWs | Cohort study | To determine the most efficient time to perform Rt-PCR prior HWs resumption. | The median time to negativisation was 25 days from symptom onset (IQR 20–35 days). Some clinical variables (dyspnoea, cough) were correlated with longer times to negativisation and may be considered in developing RTW protocols. Rt-PCR during the first three weeks leads to a high percentage of positive results. In the presence of respiratory symptoms, negativisation took nearly one week more. |
| Guarnieri V et al., 2021 [90] | Italy | Meyer Children’s University Hospital in Florence, Italy | 1690 HWs: Screening 1472 Contacts 188 RTW 30 | Cross-sectional | To describe a healthcare surveillance experience based on a combined screening consisting of Rt-PCR on nasopharyngeal swabs and rapid serologic tests for SARS-CoV-2. | A total of 13/1690 without clinical manifestations was found positive for SARS-CoV-2 using Rt-PCR: 8/1472 were found positive during the screening, 1/188 during contact with a positive individual, while 4/30 were found positive on the day of re-admission at work after an influenza-like illness. Concerning working areas, most Rt-PCR positivity and se*rologic positivity were found in non-COVID-19 dedicated areas. No cases were registered among non-patient-facing workers. Nurses and residents represented, respectively, the working roles with the highest and lowest percentage of Rt-PCR positivity. |
| Pan SC et al., 2021 [91] | Taiwan | National Taiwan University Hospital in Taipei, Taiwan | 14,210 HWs | Cohort study | To describe experience implementing specific infection prevention and control policy and practice during the first six months of the pandemic. | Among 14,210 HWs, there were 367 (2.6%) incident events (with one or more predefined symptoms during a reporting interval). A total of 283 HWs were tested for COVID-19; 179 had predefined symptoms, and 104 were asymptomatic. Many of the tests (59.7%) were performed as part of the Extended COVID-19 Screening Program. Hospital-wide web-based health surveillance integrated with a risk-based management algorithm and molecular testing of asymptomatic HWs allowed authors to rapidly identify workers at risk of infection and prevent spread to other HWs and patients. |
| Porru S et al., 2020 [92] | Italy | University Hospital of Verona, Italy | 5942 HWs | Cross-sectional | To report a SARS-CoV-2mass test experience among HWs population, as part of risk assessment and management pandemic program. | Positive tests were returned for 238 workers, similarly in COVID and non-COVID units. The SARS-CoV-2 risk was not affected by gender, age, or job type, whereas work setting and occupation were both predictors of infection. The risk was higher in medical wards and health services and lower in surgical wards and administration areas. Mass screening improved risk assessment, limited SARS-CoV-2 diffusion, and allowed resumption to work for infected HW. |
| Rivett L et al., 2020 [93] | U.K. | Cambridge University Hospitals NHS Foundation Trust, UK | 1032 HWs | Cross-sectional | To highlight challenges to the roll-out of expanded screening programs. | A total of 1032 asymptomatic HWs were screened for SARS-CoV-2 over three weeks. Symptomatic staff and symptomatic household contacts were additionally tested. Thirty HWs in the asymptomatic screening group tested positive; 57% were truly asymptomatic/paucisymptomatic, while about 40% had experienced symptoms >7 days before testing. Clusters of HWs infection were discovered on two independent wards. These data supported the utility of comprehensive screening of HWs, with minimal or no symptoms, for protecting patients and hospital staff. |
| Shenoy ES et al., 2020 [94] | USA | Massachusetts General Brigham (MGB), USA | 8930 Employees | Cohort study | To evaluate average intervals until test-based clearance and the number of excesses lost workdays using test-based authorisation. | One thousand and forty-nine employees were positive for SARS-CoV-2; 37 (3.5%) were hospitalised within seven days of their positive test. The median number of days from the first positive to the first negative was 17 (range 2-38 days). Of the 425 HWs with positive SARS-CoV-2 test results, 263 (61.9%) had a sequential second negative NP. The median number of days from the first positive to the second negative was 19 (range 6–37). If test-based criteria are used for RTW, the authors recommend establishing a minimum duration of days before the clearance test. Test-based clearance accounted for an additional 4,097 days of cumulative lost work time, corresponding to a mean of 7.2 extra days of work lost per employee than would have been accrued using the time plus symptom-based clearance method. Thus, switching to time plus symptom-based clearance criteria could allow an earlier RTW for most workers and aid in workforce preservation. |
| Tripathy D et al., 2021 [95] | India | Tertiary eye care facility in Odisha, India | 87 HWs /224 patients | Cohort study | To report the use and impact of a point-of-care Rapid Antigen Test in facilitating commencement of elective surgeries and contact tracing of exposed HWs and implement RTW policy. | The overall positivity rate was around 7%. Asymptomatic patients screened preoperatively had a lower positivity rate at about 3% than the staff (who were either known contacts or were symptomatic) at around 17%. Contact tracing found three-quarters of the staff at low risk and only one quarter at medium or high risk. Rapid Antigenic Tests may be routinely considered for indication-based preoperative screening of asymptomatic patients and on-campus screening, contact tracing and implementation of RTW policies for HWs. |
| Villarreal J et al., 2021 [96] | Spain | Fundacion Jimenez Dıaz University Hospital in Madrid, Spain | 375 HWs | Cohort study | To investigate whether HWs’ RTW after COVID-19 was associated with time to a negative viral detection test. | A delayed RTW was associated with longer intervals (>30 days) to a negative Rt-PCR after symptom onset and age, sex, and nursing staff and clinical support services compared to physicians. A predictive model based on those variables is proposed. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Garzillo, E.M.; Cioffi, A.; Carta, A.; Monaco, M.G.L. Returning to Work after the COVID-19 Pandemic Earthquake: A Systematic Review. Int. J. Environ. Res. Public Health 2022, 19, 4538. https://doi.org/10.3390/ijerph19084538
Garzillo EM, Cioffi A, Carta A, Monaco MGL. Returning to Work after the COVID-19 Pandemic Earthquake: A Systematic Review. International Journal of Environmental Research and Public Health. 2022; 19(8):4538. https://doi.org/10.3390/ijerph19084538
Chicago/Turabian StyleGarzillo, Elpidio Maria, Arcangelo Cioffi, Angela Carta, and Maria Grazia Lourdes Monaco. 2022. "Returning to Work after the COVID-19 Pandemic Earthquake: A Systematic Review" International Journal of Environmental Research and Public Health 19, no. 8: 4538. https://doi.org/10.3390/ijerph19084538
APA StyleGarzillo, E. M., Cioffi, A., Carta, A., & Monaco, M. G. L. (2022). Returning to Work after the COVID-19 Pandemic Earthquake: A Systematic Review. International Journal of Environmental Research and Public Health, 19(8), 4538. https://doi.org/10.3390/ijerph19084538