
A Cohort Study on the Effect of Parental Mind-Mindedness in Parent−Child Interaction Therapy

Abstract
:1. Introduction
The Present Study
2. Materials and Methods
2.1. Participants
2.1.1. PCIT-Home Sample
2.1.2. PCIT-Clinic Sample
2.2. Time-Limited, Home-Based PCIT and Clinic-Based PCIT: Similarities and Differences
2.3. Procedure
3. Measures
3.1. Mind-Mindedness
3.2. Dyadic Parent–Child Interaction Coding System
3.3. Eyberg Child Behavior Inventory
3.4. Strengths and Difficulties Questionnaire
3.5. Adult Self-Report
3.6. Parenting Stress Index Short Form & Dutch Parenting Stress Questionnaire
4. Statistical Approach
5. Results
5.1. Preliminary Analyses
5.2. Moderating and Group Effects of Mind-Mindedness
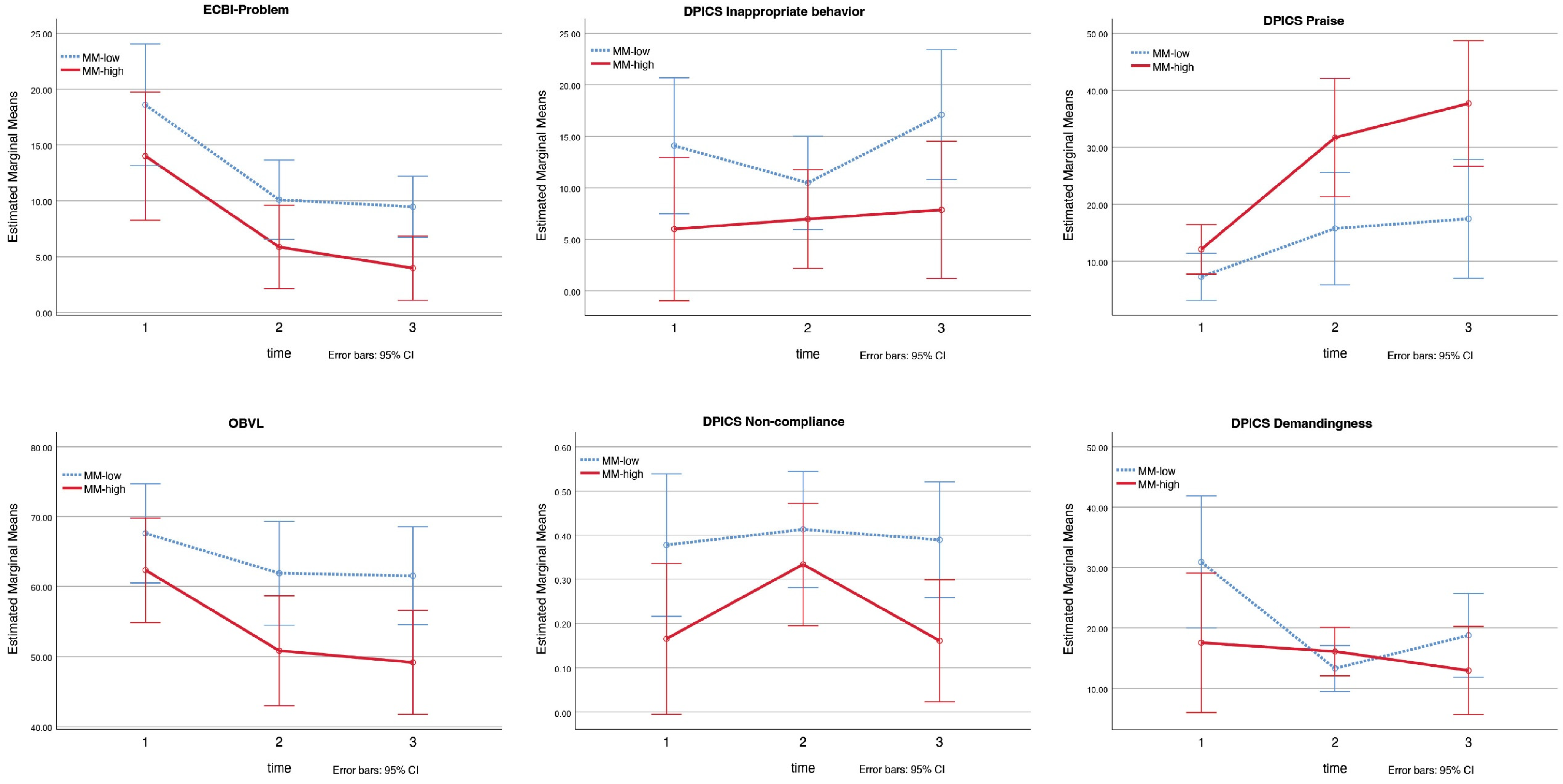
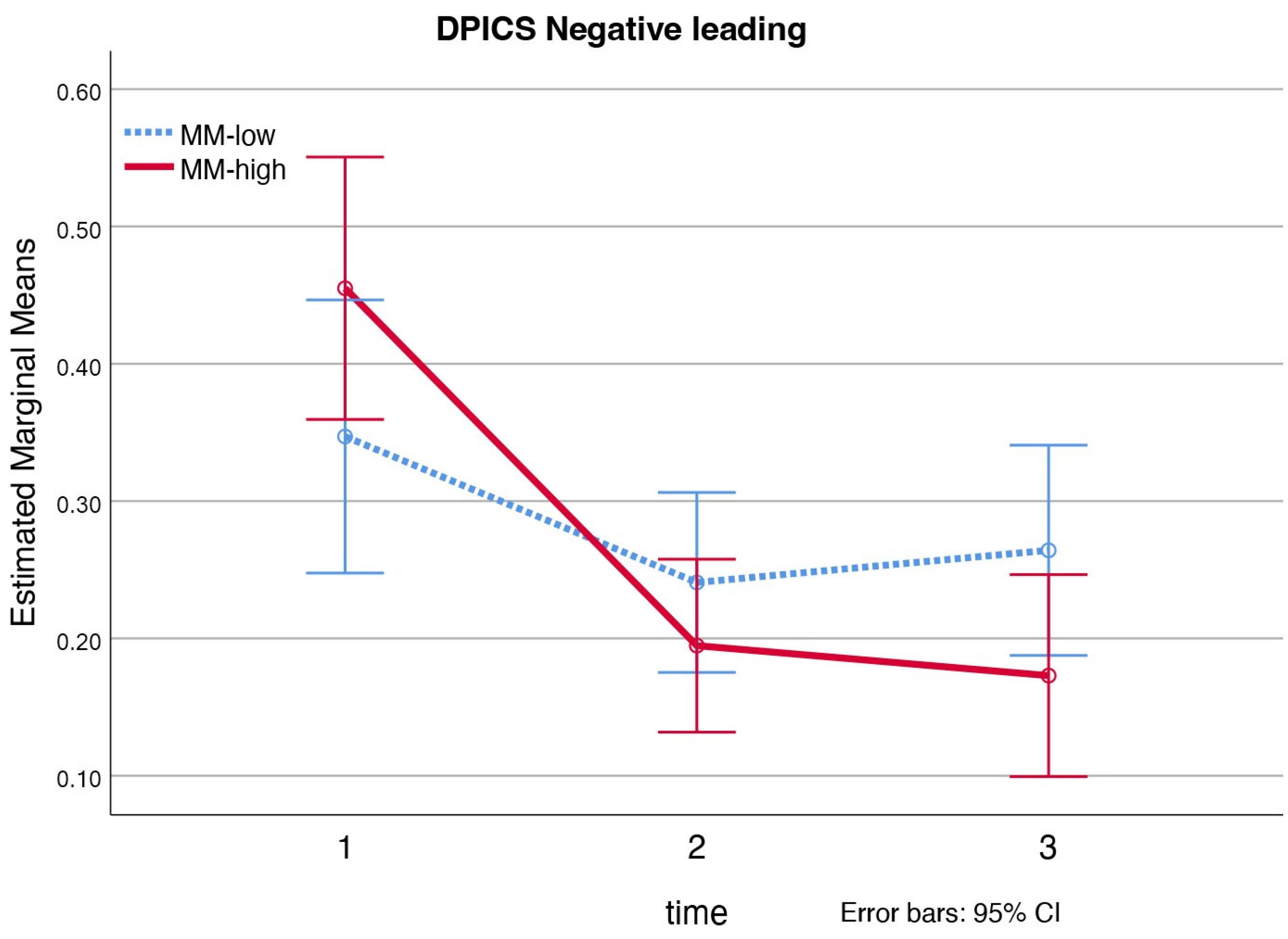
5.2.1. PCIT-Home Sample
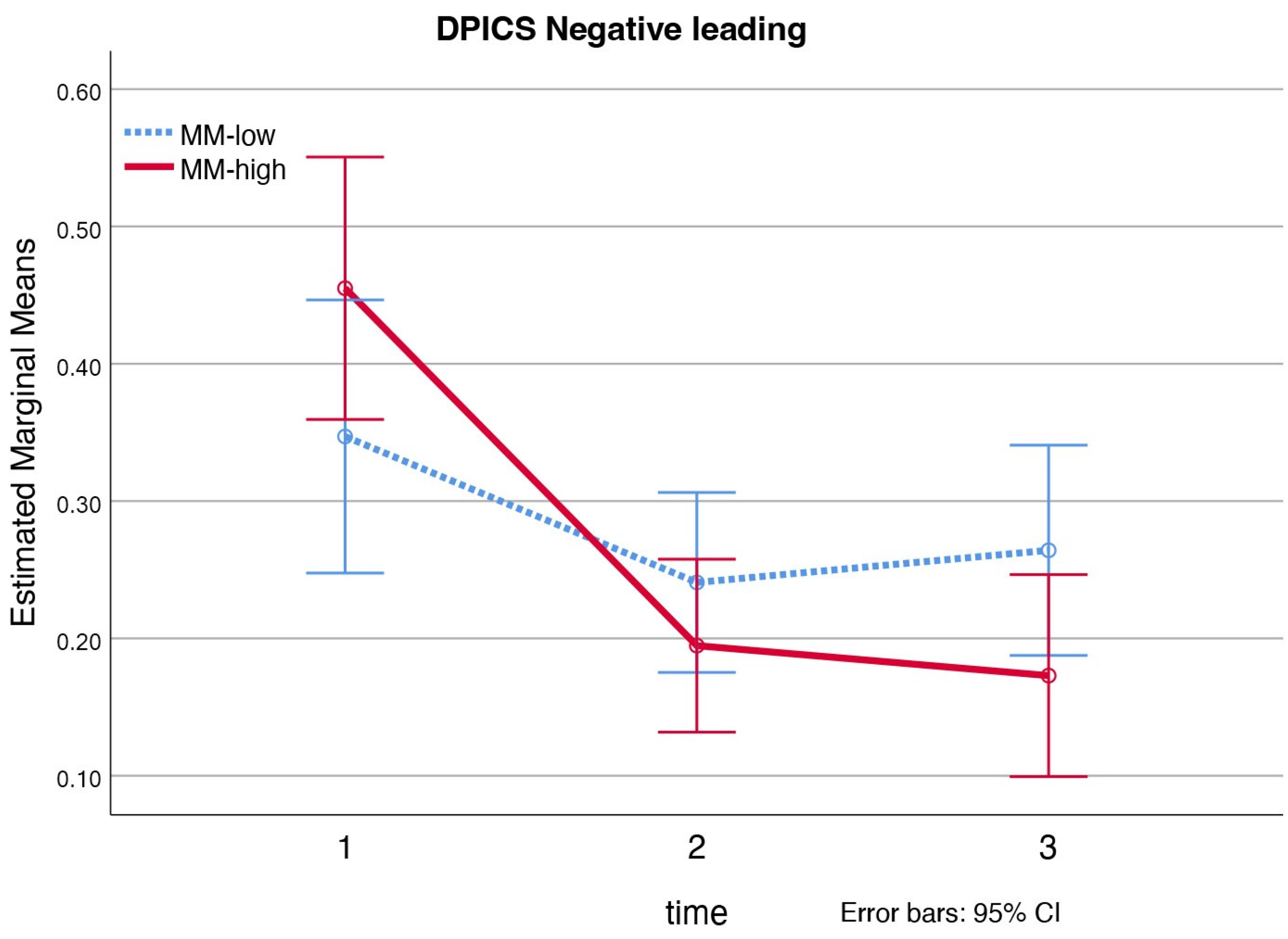
5.2.2. PCIT-Clinic Sample
5.3. Premature Attrition and Total Sessions
5.3.1. PCIT-Home Sample
5.3.2. PCIT-Clinic Sample
5.4. Sensitivity Analyses
6. Discussion
6.1. Moderating Effects
6.2. Group Effects
6.3. Premature Attrition and Total Sessions
6.4. Limitations
6.5. Recommendations for Future Research
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. Descriptive Statistics and Sensitivity Analyses

{kind=link}
{kind=link}
| Pre-Test | Post-Test | Follow-Up Test | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Variables | M | SD | Range | M | SD | Range | M | SD | Range |
| ECBI Intensity | |||||||||
| MM-low | 137.90 | 37.07 | 79.00–201.00 | 104.30 | 42.01 | 71.00–182.00 | 101.07 | 22.41 | 76.00–147.00 |
| MM-high | 113.00 | 32.20 | 65.00–164.00 | 78.18 | 18.87 | 46.00–94.01 | 79.71 | 21.80 | 42.00–102.00 |
| ECBI Problem | |||||||||
| MM-low | 18.60 | 8.13 | 6.00–31.00 | 10.10 | 6.08 | 1.00–19.00 | 9.47 | 4.93 | 5.00–20.00 |
| MM-high | 14.01 | 8.22 | 0.00–29.00 | 5.87 | 4.32 | 0.00–12.00 | 3.98 | 2.89 | 0.00–7.64 |
| OBVL | |||||||||
| MM-low | 67.60 | 9.22 | 48.00–78.00 | 61.90 | 12.78 | 40.00–79.00 | 61.53 | 10.51 | 44.00–78.00 |
| MM-high | 62.33 | 12.05 | 39.00–75.00 | 50.82 | 9.00 | 36.00–62.00 | 49.16 | 10.51 | 34.00–60.00 |
| DPICS Child | |||||||||
| Inappr. behavior | |||||||||
| MM-low | 14.10 | 12.42 | 0.00–38.00 | 10.50 | 7.69 | 4.00–30.00 | 17.10 | 11.82 | 8.00–42.00 |
| MM-high | 6.00 | 5.85 | 1.00–19.00 | 6.97 | 5.62 | 2.00–19.00 | 7.87 | 5.71 | 0.00–14.88 |
| Non-compliance | |||||||||
| MM-low | 0.38 | 0.29 | 0.00–0.88 | 0.41 | 0.17 | 0.17–0.78 | 0.39 | 0.21 | 0.16–0.75 |
| MM-high | 0.17 | 0.18 | 0.00–0.50 | 0.33 | 0.22 | 0.00–0.64 | 0.16 | 0.18 | 0.00–0.44 |
| DPICS Parent | |||||||||
| Positive following | |||||||||
| MM-low | 0.04 | 0.04 | 0.00–0.10 | 0.28 | 0.20 | 0.06–0.62 | 0.28 | 0.18 | 0.05–0.66 |
| MM-high | 0.11 | 0.07 | 0.03–0.22 | 0.32 | 0.11 | 0.15–0.51 | 0.29 | 0.16 | 0.14–0.61 |
| Negative leading | |||||||||
| MM-low | 0.43 | 0.16 | 0.28–0.75 | 0.21 | 0.15 | 0.03–0.55 | 0.20 | 0.09 | 0.04–0.35 |
| MM-high | 0.36 | 0.10 | 0.25–0.54 | 0.12 | 0.09 | 0.01–0.28 | 0.15 | 0.09 | 0.03–0.31 |
| Praise | |||||||||
| MM-low | 7.30 | 5.33 | 0.00–18.00 | 15.77 | 12.36 | 1.00–32.00 | 17.46 | 11.46 | 3.00–33 |
| MM-high | 12.11 | 7.04 | 5.00–22.00 | 31.70 | 17.12 | 9.00–60.00 | 37.71 | 19.30 | 14.00–78.00 |
| Demandingness | |||||||||
| MM-low | 30.90 | 18.60 | 8.00–60.00 | 13.30 | 6.57 | 2.00–25.00 | 18.78 | 13.26 | 4.00–43.00 |
| MM-high | 17.56 | 13.45 | 2.00–48.00 | 16.10 | 4.50 | 7.00–24.00 | 12.95 | 5.49 | 5.00–19.00 |
| Pre-Test | Post-Test | Follow-Up Test | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Variables | M | SD | Range | M | SD | Range | M | SD | Range |
| ECBI Intensity | |||||||||
| MM-low | 143.25 | 26.07 | 112.00–175.00 | 95.28 | 26.57 | 53.00–154.50 | 106.40 | 28.70 | 61.00–144.00 |
| MM-high | 155.92 | 27.75 | 110.00–200.00 | 109.69 | 32.89 | 36.00–166.00 | 116.91 | 36.07 | 50.00–175.00 |
| ECBI Problem | |||||||||
| MM-low | 17.17 | 9.15 | 0.00–30.00 | 8.04 | 6.49 | 0.00–20.00 | 8.77 | 7.26 | 0.00–27.00 |
| MM-high | 18.46 | 5.74 | 10.00–29.00 | 8.94 | 7.26 | 0.00–27.00 | 8.17 | 7.65 | 0.00–26.00 |
| PSI-SF | |||||||||
| MM-low | 86.02 | 24.67 | 55.00–135.00 | 69.36 | 22.76 | 35.00–114.00 | 79.20 | 30.54 | 37.00–134.00 |
| MM-high | 90.09 | 20.34 | 62.00–134.00 | 74.00 | 24.40 | 35.00–124.00 | 66.79 | 27.93 | 25.00–129.00 |
| ASR Anx./Depr. Scale | |||||||||
| MM-low | 11.50 | 7.42 | 2.00–32.00 | 9.04 | 7.17 | 0.00–27.00 | 6.64 | 5.15 | 0.00–16.00 |
| MM-high | 8.54 | 5.97 | 0.00–21.00 | 7.17 | 4.87 | 0.00–17.00 | 5.95 | 4.02 | 0.00–14.00 |
| DPICS Child | |||||||||
| Inappr. behavior | |||||||||
| MM-low | 16.25 | 16.73 | 0.00–62.00 | 11.00 | 11.60 | 0.00–29.00 | 8.48 | 7.97 | 1.00–25.00 |
| MM-high | 21.23 | 16.04 | 2.00–51.00 | 12.08 | 16.16 | 0.00–47.00 | 8.57 | 9.24 | 0.00–30.00 |
| Non-compliance | |||||||||
| MM-low | 0.53 | 0.23 | 0.25–0.88 | 0.28 | 0.16 | 0.00–0.50 | 0.33 | 0.31 | 0.00–1.00 |
| MM-high | 0.49 | 0.21 | 0.18–0.83 | 0.35 | 0.19 | 0.10–0.83 | 0.38 | 0.24 | 0.00–0.83 |
| DPICS Parent | |||||||||
| Positive following | |||||||||
| MM-low | 0.11 | 0.10 | 0.02–0.34 | 0.20 | 0.09 | 0.03–0.31 | 0.23 | 0.16 | 0.00–0.44 |
| MM-high | 0.12 | 0.11 | 0.00–0.45 | 0.26 | 0.13 | 0.00–0.49 | 0.34 | 0.16 | 0.05–0.60 |
| Negative leading | |||||||||
| MM-low | 0.35 | 0.15 | 0.08–0.62 | 0.24 | 0.09 | 0.10–0.40 | 0.26 | 0.17 | 0.00–0.59 |
| MM-high | 0.46 | 0.18 | 0.02–0.70 | 0.19 | 0.12 | 0.03–0.45 | 0.17 | 0.08 | 0.08–0.33 |
| Praise | |||||||||
| MM-low | 12.00 | 7.93 | 1.00–28.00 | 22.08 | 18.25 | 4.00–62.00 | 15.94 | 7.87 | 3.00–28.00 |
| MM-high | 10.08 | 8.59 | 2.00–34.00 | 21.77 | 16.98 | 0.00–59.00 | 23.94 | 13.43 | 5.00–47.00 |
| Demandingness | |||||||||
| MM-low | 31.58 | 13.83 | 13.00–60.00 | 19.08 | 9.12 | 5.00–38.00 | 21.29 | 14.13 | 4.00–53.00 |
| MM-high | 40.92 | 19.37 | 11.00–78.00 | 17.77 | 7.74 | 6.00–36.00 | 18.29 | 10.92 | 4.00–47.00 |
| Intervention | Group (MM) | Interaction (MM) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| F | p | ηp2 | F | p | ηp2 | F | p | ηp2 | |
| ECBI Intensity | 1.69 | 0.202 | 0.11 | 4.94 | 0.043 | 0.26 | 0.02 | 0.981 | 0.00 |
| ECBI Problem | 1.37 | 0.271 | 0.09 | 2.11 | 0.168 | 0.13 | 0.05 | 0.955 | 0.00 |
| OBVL | 1.97 | 0.159 | 0.12 | 0.52 | 0.484 | 0.04 | 1.21 | 0.313 | 0.08 |
| DPICS Child | |||||||||
| Inappr. behavior | 1.60 | 0.219 | 0.10 | 7.13 | 0.018 | 0.34 | 1.27 | 0.297 | 0.08 |
| Non-compliance | 2.84 | 0.075 | 0.17 | 8.52 | 0.011 | 0.38 | 1.45 | 0.249 | 0.09 |
| DPICS Parent | |||||||||
| Positive following | 3.80 | 0.035 | 0.21 | 0.41 | 0.532 | 0.03 | 0.15 | 0.860 | 0.01 |
| Negative leading | 1.20 | 0.315 | 0.08 | 3.53 | 0.081 | 0.20 | 0.15 | 0.862 | 0.01 |
| Praise | 5.58 | 0.009 | 0.29 | 5.13 | 0.040 | 0.27 | 3.49 | 0.044 | 0.20 |
| Demandingness | 0.20 | 0.824 | 0.01 | 4.59 | 0.050 | 0.25 | 3.65 | 0.039 | 0.21 |
References
- Lavigne, J.V.; LeBailly, S.A.; Hopkins, J.; Gouze, K.R.; Binns, H.J. The prevalence of ADHD, ODD, depression, and anxiety in a community sample of 4-year-olds. J. Clin. Child Adolesc. Psychol. 2009, 38, 315–328. [Google Scholar] [CrossRef] [PubMed]
- Loeber, R.; Burke, J.D.; Lahey, B.B.; Winters, A.; Zera, M. Oppositional defiant and conduct disorder: A review of the past 10 years, part I. J. Am. Acad. Child Adolesc. Psychiatry 2000, 39, 1468–1484. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bongers, I.L.; Koot, H.M.; van der Ende, J.; Verhulst, F.C. Developmental Trajectories of Externalizing Behaviors in Childhood and Adolescence. Child Dev. 2004, 75, 1523–1537. [Google Scholar] [CrossRef] [PubMed]
- Oldehinkel, A.J.; Ormel, J. A longitudinal perspective on childhood adversities and onset risk of various psychiatric disorders. Eur. Child Adolesc. Psychiatry 2014, 24, 641–650. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McGee, R.; Prior, M.; Williams, S.; Smart, D.; Sanson, A. The long-term significance of teacher-rated hyperactivity and reading ability in childhood: Findings from two longitudinal studies. J. Child Psychol. Psychiatry 2002, 43, 1004–1017. [Google Scholar] [CrossRef]
- Maughan, B.; Rutter, M. Antisocial children grown up. In Conduct Disorders in Childhood and Adolescence; Cambridge Child and Adolescent Psychiatry; Cambridge University Press: New York, NY, USA, 2001; pp. 507–552. [Google Scholar]
- McCord, J.; Widom, C.S.; Crowell, N.E. Juvenile Crime, Juvenile Justice; National Academy Press: Washington, DC, USA, 2001. [Google Scholar]
- Eyberg, S.M.; Nelson, M.M.; Boggs, S.R. Evidence-Based Psychosocial Treatments for Children and Adolescents With Disruptive Behavior. J. Clin. Child Adolesc. Psychol. 2008, 37, 215–237. [Google Scholar] [CrossRef]
- Zisser-Nathenson, A.R.; Herschell, A.D.; Eyberg, S.M. Parent-child interaction therapy and the treatment of disruptive behavior disorders. In Evidence-Based Psychotherapies for Children And Adolescents, 3rd ed.; The Guilford Press: New York, NY, USA, 2018; pp. 103–121. [Google Scholar]
- Ainsworth, M.D.S. Object Relations, Dependency, and Attachment: A Theoretical Review of the Infant-Mother Relationship. Child Dev. 1969, 40, 969–1025. [Google Scholar] [CrossRef]
- Patterson, G.R. Coercive Family Process; Castalia Press: Eugene, OR, USA, 1982. [Google Scholar]
- Schuhmann, E.M.; Foote, R.C.; Eyberg, S.M.; Boggs, S.R.; Algina, J. Efficacy of Parent-Child Interaction Therapy: Interim Report of a Randomized Trial with Short-Term Maintenance. J. Clin. Child Psychol. 1998, 27, 34–45. [Google Scholar] [CrossRef]
- Thomas, R.; Zimmer-Gembeck, M.J. Behavioral Outcomes of Parent-Child Interaction Therapy and Triple P—Positive Parenting Program: A Review and Meta-Analysis. J. Abnorm. Child Psychol. 2007, 35, 475–495. [Google Scholar] [CrossRef]
- MacMillan, H.L.; Wathen, C.N.; Barlow, J.; Fergusson, D.M.; Leventhal, J.M.; Taussig, H.N. Interventions to prevent child maltreatment and associated impairment. Lancet 2009, 373, 250–266. [Google Scholar] [CrossRef]
- Thomas, R.; Zimmer-Gembeck, M.J. Accumulating Evidence for Parent-Child Interaction Therapy in the Prevention of Child Maltreatment. Child Dev. 2011, 82, 177–192. [Google Scholar] [CrossRef] [PubMed]
- Thomas, R.; Zimmer-Gembeck, M.J. Parent–Child Interaction Therapy. Child Maltreat. 2012, 17, 253–266. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abrahamse, M.E.; Niec, L.N.; Junger, M.; Boer, F.; Lindauer, R.J.L. Risk factors for attrition from an evidence-based parenting program: Findings from the Netherlands. Child. Youth Serv. Rev. 2016, 64, 42–50. [Google Scholar] [CrossRef]
- Boggs, S.R.; Eyberg, S.M.; Edwards, D.L.; Rayfield, A.; Jacobs, J.; Bagner, D.; Hood, K.K. Outcomes of Parent-Child Interaction Therapy: A Comparison of Treatment Completers and Study Dropouts One to Three Years Later. Child Fam. Behav. Ther. 2005, 26, 1–22. [Google Scholar] [CrossRef]
- Chen, Y.-C.; Fortson, B.L. Predictors of treatment attrition and treatment length in Parent-Child Interaction Therapy in Taiwanese families. Child. Youth Serv. Rev. 2015, 59, 28–37. [Google Scholar] [CrossRef]
- Lanier, P.; Kohl, P.L.; Benz, J.; Swinger, D.; Moussette, P.; Drake, B. Parent–Child Interaction Therapy in a Community Setting: Examining Outcomes, Attrition, and Treatment Setting. Res. Soc. Work. Pract. 2011, 21, 689–698. [Google Scholar] [CrossRef] [Green Version]
- Fowles, T.R.; Masse, J.J.; McGoron, L.; Beveridge, R.M.; Williamson, A.A.; Smith, M.A.; Parrish, B.P. Home-Based vs. Clinic-Based Parent–Child Interaction Therapy: Comparative Effectiveness in the Context of Dissemination and Implementation. J. Child Fam. Stud. 2017, 27, 1115–1129. [Google Scholar] [CrossRef]
- Heinrichs, N.; Bertram, H.; Kuschel, A.; Hahlweg, K. Parent Recruitment and Retention in a Universal Prevention Program for Child Behavior and Emotional Problems: Barriers to Research and Program Participation. Prev. Sci. 2005, 6, 275–286. [Google Scholar] [CrossRef]
- Kazdin, A.E.; Holland, L.; Crowley, M. Family experience of barriers to treatment and premature termination from child therapy. J. Consult. Clin. Psychol. 1997, 65, 453–463. [Google Scholar] [CrossRef]
- Lavigne, J.V.; LeBailly, S.A.; Gouze, K.R.; Binns, H.J.; Keller, J.; Pate, L. Predictors and Correlates of Completing Behavioral Parent Training for the Treatment of Oppositional Defiant Disorder in Pediatric Primary Care. Behav. Ther. 2010, 41, 198–211. [Google Scholar] [CrossRef] [Green Version]
- Masse, J.J.; Quetsch, L.B.; McNeil, C.B. Taking PRIDE in Your Home: Implementing Home-Based Parent–Child Interaction Therapy (PCIT) with Fidelity. In Handbook of Parent-Child Interaction Therapy; Springer Nature: Cham, Switzerland, 2018; pp. 161–181. [Google Scholar]
- Masse, J.J.; McNeil, C.B. In-Home Parent-Child Interaction Therapy: Clinical Considerations. Child Fam. Behav. Ther. 2008, 30, 127–135. [Google Scholar] [CrossRef]
- Bagner, D.M.; Rodríguez, G.M.; Blake, C.A.; Rosa-Olivares, J. Home-Based Preventive Parenting Intervention for at-Risk Infants and Their Families: An Open Trial. Cogn. Behav. Pract. 2013, 20, 334–348. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bagner, D.M.; Coxe, S.; Hungerford, G.M.; Garcia, D.; Barroso, N.E.; Hernandez, J.; Rosa-Olivares, J. Behavioral Parent Training in Infancy: A Window of Opportunity for High-Risk Families. J. Abnorm. Child Psychol. 2015, 44, 901–912. [Google Scholar] [CrossRef] [Green Version]
- Galanter, R.; Self-Brown, S.; Valente, J.R.; Dorsey, S.; Whitaker, D.J.; Bertuglia-Haley, M.; Prieto, M. Effectiveness of Parent–Child Interaction Therapy Delivered to At-Risk Families in the Home Setting. Child Fam. Behav. Ther. 2012, 34, 177–196. [Google Scholar] [CrossRef]
- Timmer, S.G.; Zebell, N.M.; Culver, M.A.; Urquiza, A.J. Efficacy of Adjunct In-Home Coaching to Improve Outcomes in Parent—Child Interaction Therapy. Res. Soc. Work. Pract. 2009, 20, 36–45. [Google Scholar] [CrossRef]
- Villodas, M.T.; Moses, J.O.; Cromer, K.D.; Mendez, L.; Magariño, L.S.; Villodas, F.M.; Bagner, D.M. Feasibility and promise of community providers implementing home-based parent-child interaction therapy for families investigated for child abuse: A pilot randomized controlled trial. Child Abus. Negl. 2021, 117, 105063. [Google Scholar] [CrossRef] [PubMed]
- Bakermans-Kranenburg, M.J.; van Ijzendoorn, M.H.; Juffer, F. Less is more: Meta-analyses of sensitivity and attachment interventions in early childhood. Psychol. Bull. 2003, 129, 195–215. [Google Scholar] [CrossRef]
- Abrahamse, M.E.; Tsang, V.M.W.; Lindauer, R.J.L. Home-Based Parent–Child Interaction Therapy to Prevent Child Maltreatment: A Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2021, 18, 8244. [Google Scholar] [CrossRef]
- Sharp, C.; Fonagy, P. The Parent’s Capacity to Treat the Child as a Psychological Agent: Constructs, Measures and Implications for Developmental Psychopathology. Soc. Dev. 2008, 17, 737–754. [Google Scholar] [CrossRef] [Green Version]
- McNeil, C.B.; Hembree-Kigin, T.L. Parent-Child Interaction Therapy, 2nd ed.; Springer: New York, NY, USA, 2010. [Google Scholar]
- Meins, E. Security of Attachment and the Social Development of Cognition; Psychology Press: Hove, UK, 1997. [Google Scholar]
- Meins, E. Sensitivity, security and internal working models: Bridging the transmission gap. Attach. Hum. Dev. 1999, 1, 325–342. [Google Scholar] [CrossRef]
- Meins, E. Sensitive attunement to infants’ internal states: Operationalizing the construct of mind-mindedness. Attach. Hum. Dev. 2013, 15, 524–544. [Google Scholar] [CrossRef] [PubMed]
- Meins, E.; Fernyhough, C. Mind-Mindedness Coding Manual, Version 2.2; Unpublished manuscript; Durham University: Durham, UK, 2015. [Google Scholar]
- McMahon, C.A.; Bernier, A. Twenty years of research on parental mind-mindedness: Empirical findings, theoretical and methodological challenges, and new directions. Dev. Rev. 2017, 46, 54–80. [Google Scholar] [CrossRef]
- Zeegers, M.A.J.; Colonnesi, C.; Stams, G.-J.J.M.; Meins, E. Mind matters: A meta-analysis on parental mentalization and sensitivity as predictors of infant–parent attachment. Psychol. Bull. 2017, 143, 1245–1272. [Google Scholar] [CrossRef] [PubMed]
- Bernier, A.; McMahon, C.A.; Perrier, R. Maternal mind-mindedness and children’s school readiness: A longitudinal study of developmental processes. Dev. Psychol. 2017, 53, 210–221. [Google Scholar] [CrossRef] [Green Version]
- Meins, E.; Fernyhough, C.; Arnott, B.; Leekam, S.R.; de Rosnay, M. Mind-Mindedness and Theory of Mind: Mediating Roles of Language and Perspectival Symbolic Play. Child Dev. 2013, 84, 1777–1790. [Google Scholar] [CrossRef] [Green Version]
- Centifanti, L.C.M.; Meins, E.; Fernyhough, C. Callous-unemotional traits and impulsivity: Distinct longitudinal relations with mind-mindedness and understanding of others. J. Child Psychol. Psychiatry 2016, 57, 84–92. [Google Scholar] [CrossRef] [Green Version]
- Easterbrooks, M.A.; Crossman, M.K.; Caruso, A.; Raskin, M.; Miranda-Julian, C. Maternal mind–mindedness and toddler behavior problems: The moderating role of maternal trauma and posttraumatic stress. Dev. Psychopathol. 2017, 29, 1431–1442. [Google Scholar] [CrossRef] [Green Version]
- Hughes, C.; Aldercotte, A.; Foley, S. Maternal Mind-Mindedness Provides a Buffer for Pre-Adolescents at Risk for Disruptive Behavior. J. Abnorm. Child Psychol. 2016, 45, 225–235. [Google Scholar] [CrossRef] [Green Version]
- Meins, E.; Centifanti, L.C.M.; Fernyhough, C.; Fishburn, S. Maternal Mind-Mindedness and Children’s Behavioral Difficulties: Mitigating the Impact of Low Socioeconomic Status. J. Abnorm. Child Psychol. 2013, 41, 543–553. [Google Scholar] [CrossRef] [Green Version]
- Walker, T.M.; Wheatcroft, R.; Camic, P.M. Mind-mindedness in parents of pre-schoolers: A comparison between clinical and community samples. Clin. Child Psychol. Psychiatry 2011, 17, 318–335. [Google Scholar] [CrossRef]
- Colonnesi, C.; Wissink, I.B.; Noom, M.J.; Asscher, J.J.; Hoeve, M.; Stams, G.J.J.M.; Polderman, N.; Kellaert-Knol, M.G. Basic Trust. Res. Soc. Work. Pract. 2012, 23, 179–188. [Google Scholar] [CrossRef]
- Zeegers, M.A.J.; Colonnesi, C.; Noom, M.J.; Polderman, N.; Stams, G.-J.J.M. Remediating Child Attachment Insecurity: Evaluating the Basic Trust Intervention in Adoptive Families. Res. Soc. Work. Pract. 2019, 30, 736–749. [Google Scholar] [CrossRef] [Green Version]
- Konijn, C.; Colonnesi, C.; Kroneman, L.; Liefferink, N.; Lindauer, R.J.L.; Stams, G.-J.J.M. ‘Caring for children who have experienced trauma’—an evaluation of a training for foster parents. Eur. J. Psychotraumatol. 2020, 11, 1756563. [Google Scholar] [CrossRef] [PubMed]
- Statistics Netherlands. Overview Definition for People with a Foreign Background. 2021. Available online: https://www.cbs.nl/en-gb/onze-diensten/methods/definitions/migration-background (accessed on 14 January 2021).
- Barnett, D.; Manly, J.T.; Cicchetti, D. Defining child maltreatment: The interface between policy and research. Child Abus. Child Dev. Soc. Policy 1993, 8, 7–73. [Google Scholar]
- Eyberg, S.M.; Funderburk, B. Parent-Child Interaction Therapy Protocol; PCIT International: Gainesville, FL, USA, 2011. [Google Scholar]
- Eyberg, S.M.; Nelson, M.M.; Ginn, N.C.; Bhuiyan, N.N.; Boggs, S.R. Manual for the Dyadic Parent–Child. Interaction Coding System; PCIT International: Gainesville, FL, USA, 2013. [Google Scholar]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef] [Green Version]
- Colonnesi, C.; van Polanen, M.; Tavecchio, L.W.C.; Fukkink, R.G. Mind-Mindedness of Male and Female Caregivers in Childcare and the Relation to Sensitivity and Attachment: An Exploratory Study. Infant Behav. Dev. 2017, 48, 134–146. [Google Scholar] [CrossRef]
- Fernandez, M.A.; Eyberg, S.M. Predicting Treatment and Follow-up Attrition in Parent–Child Interaction Therapy. J. Abnorm. Child Psychol. 2008, 37, 431–441. [Google Scholar] [CrossRef]
- Werba, B.E.; Eyberg, S.M.; Boggs, S.R.; Algina, J. Predicting Outcome in Parent-Child Interaction Therapy. Behav. Modif. 2016, 30, 618–646. [Google Scholar] [CrossRef]
- Eyberg, S.M.; Pincus, D.B. Eyberg Child Behavior Inventory and Sutter-Eyberg Behavior Inventory-Revised: Professional Manual; Psychological Assessment Resources: Odessa, FL, USA, 1999. [Google Scholar]
- Abrahamse, M.E.; Junger, M.; Leijten, P.H.O.; Lindeboom, R.; Boer, F.; Lindauer, R.J.L. Psychometric properties of the Dutch Eyberg Child Behavior Inventory (ECBI) in a community sample and a multi-ethnic clinical sample. J. Psychopathol. Behav. Assess. 2015, 37, 679–691. [Google Scholar] [CrossRef] [Green Version]
- Weeland, J.; van Aar, J.; Overbeek, G. Dutch Norms for the Eyberg Child Behavior Inventory: Comparisons with other Western Countries. J. Psychopathol. Behav. Assess. 2017, 40, 224–234. [Google Scholar] [CrossRef] [Green Version]
- Goodman, R. The Strengths and Difficulties Questionnaire: A Research Note. J. Child Psychol. Psychiatry 1997, 38, 581–586. [Google Scholar] [CrossRef] [PubMed]
- Goodman, R. Psychometric Properties of the Strengths and Difficulties Questionnaire. J. Am. Acad. Child Adolesc. Psychiatry 2001, 40, 1337–1345. [Google Scholar] [CrossRef] [PubMed]
- Achenbach, T.M.; Rescorla, L.A. Manual for the ASEBA Adult Forms and Profiles; University of Vermont, Research Center for Children, Youth, and Families: Burlington, VT, USA, 2003. [Google Scholar]
- Vermulst, A.; Kroes, G.; De Meyer, R.; Nguyen, L.; Veerman, J.W. Handleiding OBVL (Manual Parenting Stress Questionnaire); Praktikon: Nijmegen, The Netherlands, 2015. [Google Scholar]
- Abidin, R.R. Parenting Stress Index: Professional Manual, 3rd ed.; Psychological Assessment Resources: Odessa, FL, USA, 1995. [Google Scholar]
- De Brock, A.J.L.L.; Vermulst, A.A.; Gerris, J.R.M.; Abidin, R.R. Nijmeegse Ouderlijke Stress Index [Parenting Stress Index]; Swets & Zeitlinger: Lisse, The Netherlands, 1992. [Google Scholar]
- Graham, J.W. Missing Data Analysis: Making It Work in the Real World. Annu. Rev. Psychol. 2009, 60, 549–576. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Field, A. Discovering Statistics Using IBM SPSS Statistics, 4th ed.; SAGE Publications: London, UK, 2013. [Google Scholar]
- Tabachnick, B.G.; Fidell, L.S. Using Multivariate Statistics, 7th ed.; Pearson: New York City, NY, USA, 2013. [Google Scholar]
- Kwak, S.K.; Kim, J.H. Statistical data preparation: Management of missing values and outliers. Korean J. Anesthesiol. 2017, 70, 407–411. [Google Scholar] [CrossRef] [PubMed]
- Faul, F.; Erdfelder, E.; Lang, A.-G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- Niec, L.N. Handbook of Parent-Child Interaction Therapy: Innovations and Applications for Research and Practice; Springer: Berlin/Heidelberg, Germany, 2018. [Google Scholar]
- Camisasca, E.; Procaccia, R.; Miragoli, S.; Valtolina, G.G.; Di Blasio, P. Maternal mind-mindedness as a linking mechanism between childbirth-related posttraumatic stress symptoms and parenting stress. Health Care Women Int. 2017, 38, 593–612. [Google Scholar] [CrossRef]
- McMahon, C.A.; Meins, E. Mind-mindedness, parenting stress, and emotional availability in mothers of preschoolers. Early Child. Res. Q. 2012, 27, 245–252. [Google Scholar] [CrossRef]
- Colonnesi, C.; Konijn, C.; Kroneman, L.; Lindauer, R.J.L.; Stams, G.J.J.M. Mind-mindedness in out-of-home Care for Children: Implications for caregivers and child. Curr. Psychol. 2021, 40, 1–13. [Google Scholar] [CrossRef]
- Fishburn, S.; Meins, E.; Greenhow, S.; Jones, C.; Hackett, S.; Biehal, N.; Baldwin, H.; Cusworth, L.; Wade, J. Mind-mindedness in parents of looked-after children. Dev. Psychol. 2017, 53, 1954–1965. [Google Scholar] [CrossRef] [Green Version]
- Zimmer-Gembeck, M.J.; Kerin, J.L.; Webb, H.J.; Gardner, A.A.; Campbell, S.M.; Swan, K.; Timmer, S.G. Improved Perceptions of Emotion Regulation and Reflective Functioning in Parents: Two Additional Positive Outcomes of Parent-Child Interaction Therapy. Behav. Ther. 2019, 50, 340–352. [Google Scholar] [CrossRef]
- Fishburn, S. ‘Thinking about Parenting’—The Role of Mind-Mindedness and Parental Cognitions in Parental Behaviour and Child Developmental Outcomes. Ph.D. Thesis, University of York, York, UK, 2017. [Google Scholar]
- Illingworth, G.; MacLean, M.; Wiggs, L. Maternal mind-mindedness: Stability over time and consistency across relationships. Eur. J. Dev. Psychol. 2015, 13, 488–503. [Google Scholar] [CrossRef] [Green Version]
- Lundy, B.L. Paternal and Maternal Mind-mindedness and Preschoolers' Theory of Mind: The Mediating Role of Interactional Attunement. Soc. Dev. 2013, 22, 58–74. [Google Scholar] [CrossRef]
- Colonnesi, C.; Zeegers, M.A.J.; Majdandžić, M.; van Steensel, F.J.A.; Bögels, S.M. Fathers’ and Mothers’ Early Mind-Mindedness Predicts Social Competence and Behavior Problems in Childhood. J. Abnorm. Child Psychol. 2019, 47, 1421–1435. [Google Scholar] [CrossRef] [PubMed] [Green Version]

| PCIT-Home (n = 19) | PCIT-Clinic (n = 25) | |||||
|---|---|---|---|---|---|---|
| n (%*) | M | SD | n (%*) | M | SD | |
| Child characteristics | ||||||
| Age (months) | 67.21 | 19.17 | 57.88 | 12.45 | ||
| Gender (male) | 13 (68.4) | 18 (72.0) | ||||
| Country of birth (Netherlands) | 17 (89.5) | 24 (96.0) | ||||
| Ethnicity (Dutch) | 11 (57.9) | 20 (80.0) | ||||
| Maltreatment history (reported in client file) | 14 (73.7) | 16 (64.0) | ||||
| Conduct problems (SDQ) | 4.15 | 1.82 | 4.86 | 2.39 | ||
| Hyperactivity/inattention problems (SDQ) | 7.67 | 1.78 | 6.55 | 2.73 | ||
| Family characteristics | ||||||
| Age mother (years) | - | - | 36.78 | 6.18 | ||
| Country of birth mother (Netherlands) | 12 (63.2) | 20 (80.0) | ||||
| Family status (single mother) | 8 (42.1) | 10 (40.0) | ||||
| First-time mothers | - | 12 (48%) | ||||
| Educational level mother | ||||||
| Lower education | 8 (44.4) | 13 (52.0) | ||||
| Medium education | 2 (11.1) | 2 (8.0) | ||||
| Higher education | 8 (44.4) | 6 (24.0) | ||||
| Relation to child | ||||||
| Biological mother | 13 (68.4) | 25 (100) | ||||
| Foster mother | 6 (31.6) | 0 (0.0) | ||||
| Family income (<€1.000 per month) | 1 (5.3) | 3 (12.0) | ||||
| Intervention | Group (MM) | Interaction (MM) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| F | p | ηp2 | F | p | ηp2 | F | p | ηp2 | |
| ECBI Intensity | 18.33 | 0.000 | 0.52 | 4.18 | 0.057 | 0.20 | 0.07 | 0.932 | 0.00 |
| ECBI Problem | 23.05 | 0.000 | 0.58 | 4.81 | 0.043 | 0.22 | 0.09 | 0.914 | 0.01 |
| OBVL | 16.83 | 0.000 | 0.50 | 4.56 | 0.048 | 0.21 | 2.15 | 0.132 | 0.13 |
| DPICS Child | |||||||||
| Inappr. behavior | 1.06 | 0.357 | 0.06 | 6.62 | 0.020 | 0.28 | 0.67 | 0.520 | 0.04 |
| Non-compliance | 1.32 | 0.280 | 0.07 | 10.47 | 0.005 | 0.38 | 0.66 | 0.521 | 0.04 |
| DPICS Parent | |||||||||
| Positive following | 20.76 | 0.000 | 0.55 | 0.74 | 0.402 | 0.04 | 0.25 | 0.778 | 0.02 |
| Negative leading | 27.69 | 0.000 | 0.62 | 3.53 | 0.078 | 0.17 | 0.15 | 0.863 | 0.01 |
| Praise | 17.93 | 0.000 | 0.51 | 8.43 | 0.010 | 0.33 | 3.21 | 0.053 | 0.16 |
| Demandingness | 6.32 | 0.005 | 0.27 | 1.72 | 0.207 | 0.09 | 3.82 | 0.032 | 0.18 |
| Intervention | Group (MM) | Interaction (MM) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| F | p | ηp2 | F | p | ηp2 | F | p | ηp2 | |
| ECBI Intensity | 23.19 | 0.000 | 0.50 | 2.16 | 0.155 | 0.09 | 0.04 | 0.965 | 0.00 |
| ECBI Problem | 28.74 | 0.000 | 0.56 | 0.05 | 0.829 | 0.00 | 0.25 | 0.782 | 0.01 |
| PSI-SF | 6.02 | 0.005 | 0.21 | 0.02 | 0.880 | 0.00 | 1.71 | 0.193 | 0.07 |
| ASR Anx./Depr. Scale | 6.83 | 0.003 | 0.29 | 0.82 | 0.376 | 0.38 | 0.64 | 0.534 | 0.03 |
| DPICS Child | |||||||||
| Inappr. behavior | 5.17 | 0.009 | 0.18 | 0.28 | 0.600 | 0.02 | 0.31 | 0.732 | 0.01 |
| Non-compliance | 4.84 | 0.012 | 0.17 | 0.30 | 0.592 | 0.01 | 0.34 | 0.717 | 0.01 |
| DPICS Parent | |||||||||
| Positive following | 13.97 | 0.000 | 0.38 | 3.32 | 0.082 | 0.13 | 1.33 | 0.274 | 0.06 |
| Negative leading | 22.07 | 0.000 | 0.49 | 0.06 | 0.812 | 0.00 | 5.40 | 0.008 | 0.19 |
| Praise | 6.48 | 0.003 | 0.22 | 0.28 | 0.599 | 0.01 | 1.37 | 0.265 | 0.06 |
| Demandingness | 22.42 | 0.000 | 0.49 | 0.18 | 0.678 | 0.01 | 2.55 | 0.089 | 0.10 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Meynen, M.; Colonnesi, C.; Abrahamse, M.E.; Hein, I.; Stams, G.-J.J.M.; Lindauer, R.J.L.L. A Cohort Study on the Effect of Parental Mind-Mindedness in Parent−Child Interaction Therapy. Int. J. Environ. Res. Public Health 2022, 19, 4533. https://doi.org/10.3390/ijerph19084533
Meynen M, Colonnesi C, Abrahamse ME, Hein I, Stams G-JJM, Lindauer RJLL. A Cohort Study on the Effect of Parental Mind-Mindedness in Parent−Child Interaction Therapy. International Journal of Environmental Research and Public Health. 2022; 19(8):4533. https://doi.org/10.3390/ijerph19084533
Chicago/Turabian StyleMeynen, Merlijn, Cristina Colonnesi, Mariëlle E. Abrahamse, Irma Hein, Geert-Jan J. M. Stams, and Ramón J. L. L. Lindauer. 2022. "A Cohort Study on the Effect of Parental Mind-Mindedness in Parent−Child Interaction Therapy" International Journal of Environmental Research and Public Health 19, no. 8: 4533. https://doi.org/10.3390/ijerph19084533
APA StyleMeynen, M., Colonnesi, C., Abrahamse, M. E., Hein, I., Stams, G.-J. J. M., & Lindauer, R. J. L. L. (2022). A Cohort Study on the Effect of Parental Mind-Mindedness in Parent−Child Interaction Therapy. International Journal of Environmental Research and Public Health, 19(8), 4533. https://doi.org/10.3390/ijerph19084533