
The Acute Effects of Single or Repeated Bouts of Vigorous-Intensity Exercise on Insulin and Glucose Metabolism during Postprandial Sedentary Behavior


Abstract
:1. Introduction
2. Materials and Methods
2.1. Trial Design
2.2. Participants
2.3. Preliminary Examination
2.4. Interventions
2.5. Outcome Measures
2.6. Statistical Methods
3. Results
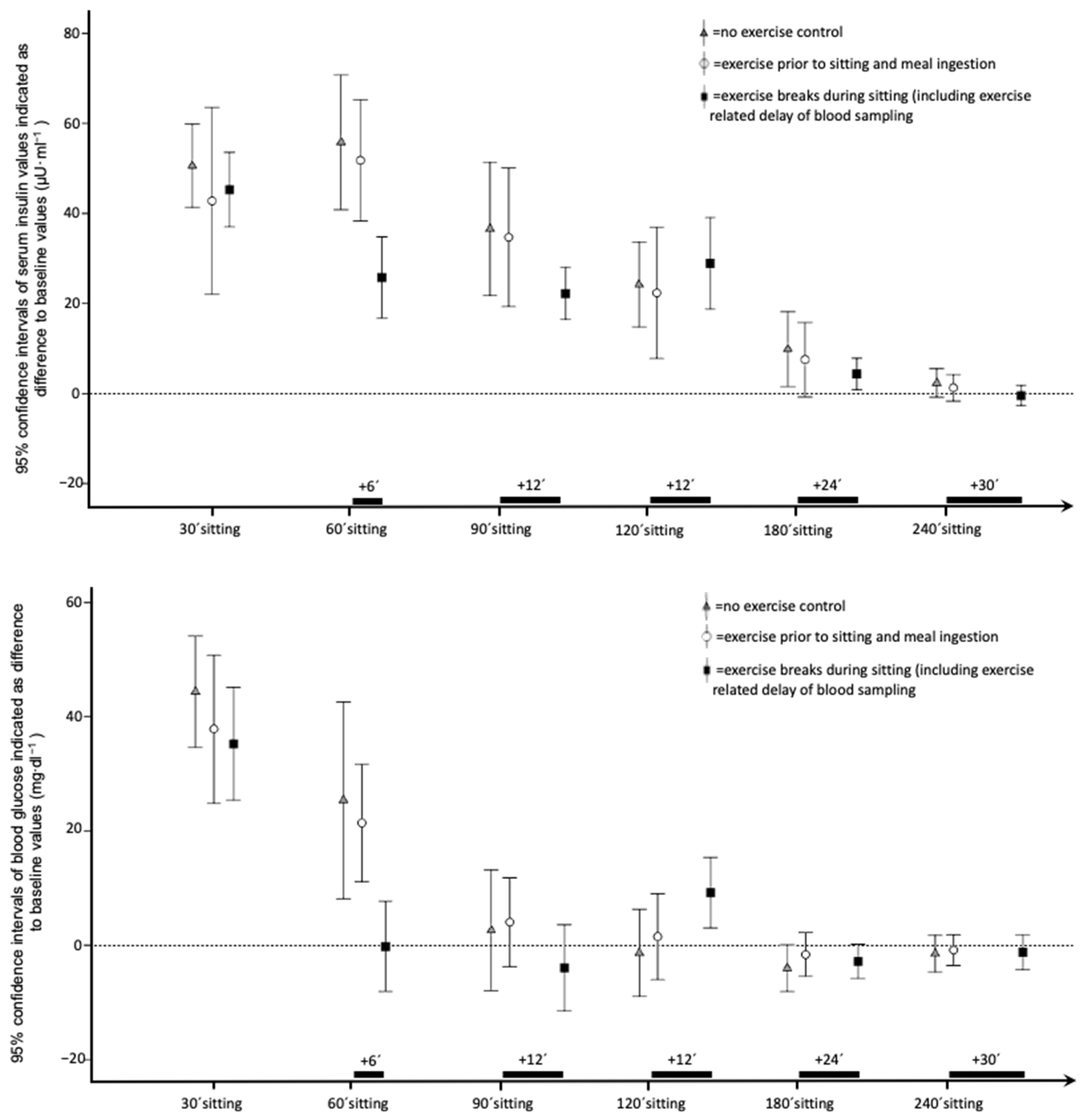
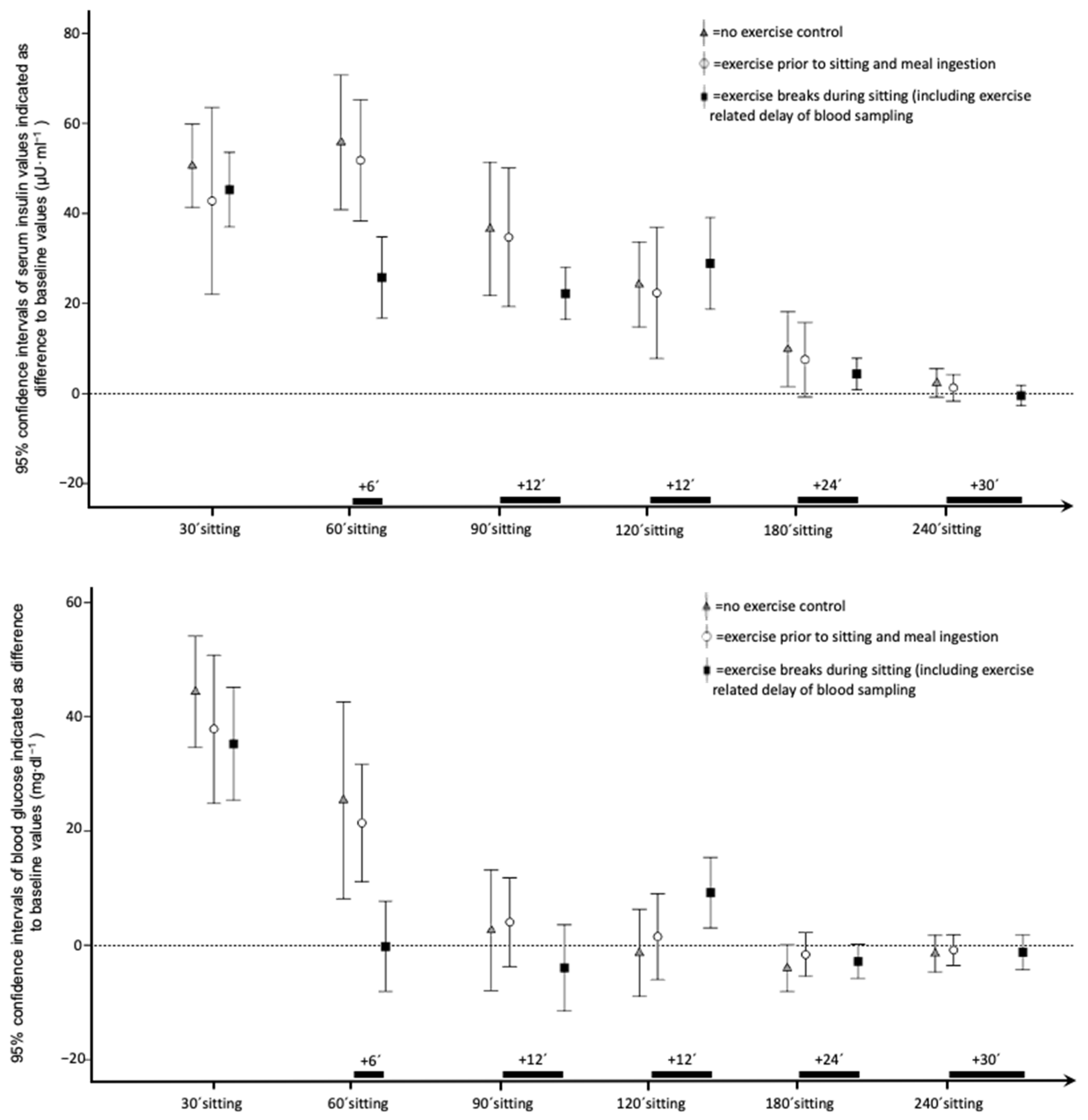
3.1. Insulin and Glucose
3.2. Cardiorespiratory Fitness and Caloric Intake
3.3. Mood and Well-Being
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Church, T.S.; Thomas, D.M.; Tudor-Locke, C.; Katzmarzyk, P.T.; Earnest, C.P.; Rodarte, R.Q.; Martin, C.K.; Blair, S.N.; Bouchard, C. Trends over 5 Decades in U.S. Occupation-Related Physical Activity and Their Associations with Obesity. PLoS ONE 2011, 6, e19657. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sedentary Behaviour Research Network. Letter to the Editor: Standardized Use of the Terms “Sedentary” and “Sedentary Behaviours”. Appl. Physiol. Nutr. Metab. 2012, 37, 540–542. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ford, E.S.; Caspersen, C.J. Sedentary Behaviour and Cardiovascular Disease: A Review of Prospective Studies. Int. J. Epidemiol. 2012, 41, 1338–1353. [Google Scholar] [CrossRef] [PubMed]
- Owen, N.; Healy, G.N.; Matthews, C.E.; Dunstan, D.W. Too Much Sitting: The Population Health Science of Sedentary Behavior. Exerc. Sport Sci. Rev. 2010, 38, 105–113. [Google Scholar] [CrossRef] [PubMed]
- Ekelund, U.; Steene-Johannessen, J.; Brown, W.J.; Fagerland, M.W.; Owen, N.; Powell, K.E.; Bauman, A.; Lee, I.-M. Does Physical Activity Attenuate, or Even Eliminate, the Detrimental Association of Sitting Time with Mortality? A Harmonised Meta-Analysis of Data from More than 1 Million Men and Women. Lancet 2016, 388, 1302–1310. [Google Scholar] [CrossRef] [Green Version]
- Sui, W.; Sui, A.; Prapavessis, H. Relationships between Indices of Sedentary Behavior and Hedonic Well-Being: A Scoping Review. Psychol. Sport Exerc. 2021, 54, 101920. [Google Scholar] [CrossRef]
- Organisation Mondiale de la Santé WHO Guidelines on Physical Activity and Sedentary Behaviour; World Health Organization: Geneva, Switzerland, 2020; ISBN 978-92-4-001512-8.
- Loh, R.; Stamatakis, E.; Folkerts, D.; Allgrove, J.E.; Moir, H.J. Effects of Interrupting Prolonged Sitting with Physical Activity Breaks on Blood Glucose, Insulin and Triacylglycerol Measures: A Systematic Review and Meta-Analysis. Sports Med. 2020, 50, 295–330. [Google Scholar] [CrossRef] [Green Version]
- del Pozo-Cruz, J.; García-Hermoso, A.; Alfonso-Rosa, R.M.; Alvarez-Barbosa, F.; Owen, N.; Chastin, S.; del Pozo-Cruz, B. Replacing Sedentary Time: Meta-Analysis of Objective-Assessment Studies. Am. J. Prev. Med. 2018, 55, 395–402. [Google Scholar] [CrossRef]
- Saunders, T.J.; Atkinson, H.F.; Burr, J.; MacEwen, B.; Skeaff, C.M.; Peddie, M.C. The Acute Metabolic and Vascular Impact of Interrupting Prolonged Sitting: A Systematic Review and Meta-Analysis. Sports Med. 2018, 48, 2347–2366. [Google Scholar] [CrossRef]
- Quan, M.; Xun, P.; Wu, H.; Wang, J.; Cheng, W.; Cao, M.; Zhou, T.; Huang, T.; Gao, Z.; Chen, P. Effects of Interrupting Prolonged Sitting on Postprandial Glycemia and Insulin Responses: A Network Meta-Analysis. J. Sport Health Sci. 2021, 10, 419–429. [Google Scholar] [CrossRef]
- Little, J.P.; Langley, J.; Lee, M.; Myette-Côté, E.; Jackson, G.; Durrer, C.; Gibala, M.J.; Jung, M.E. Sprint Exercise Snacks: A Novel Approach to Increase Aerobic Fitness. Eur. J. Appl. Physiol. 2019, 119, 1203–1212. [Google Scholar] [CrossRef] [PubMed]
- Shuval, K.; Finley, C.E.; Barlow, C.E.; Gabriel, K.P.; Leonard, D.; Kohl, H.W. Sedentary Behavior, Cardiorespiratory Fitness, Physical Activity, and Cardiometabolic Risk in Men: The Cooper Center Longitudinal Study. Mayo Clin. Proc. 2014, 89, 1052–1062. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, M.T.; Hamilton, D.G.; Zderic, T.W. Exercise Physiology versus Inactivity Physiology: An Essential Concept for Understanding Lipoprotein Lipase Regulation. Exerc. Sport Sci. Rev. 2004, 32, 161–166. [Google Scholar] [CrossRef] [PubMed]
- Saanijoki, T.; Nummenmaa, L.; Eskelinen, J.-J.; Savolainen, A.M.; Vahlberg, T.; Kalliokoski, K.K.; Hannukainen, J.C. Affective Responses to Repeated Sessions of High-Intensity Interval Training. Med. Sci. Sports Exerc. 2015, 47, 2604–2611. [Google Scholar] [CrossRef]
- Engeroff, T.; Füzéki, E.; Vogt, L.; Banzer, W. Breaking up Sedentary Time, Physical Activity and Lipoprotein Metabolism. J. Sci. Med. Sport 2017, 20, 678–683. [Google Scholar] [CrossRef]
- Miyashita, M.; Burns, S.F.; Stensel, D.J. Accumulating Short Bouts of Brisk Walking Reduces Postprandial Plasma Triacylglycerol Concentrations and Resting Blood Pressure in Healthy Young Men. Am. J. Clin. Nutr. 2008, 88, 1225–1231. [Google Scholar] [CrossRef]
- Pescatello, L.S. American College of Sports Medicine ACSM’s Guidelines for Exercise Testing and Prescription; Wolters Kluwer/Lippincott Williams & Wilkins Health: Philadelphia, PA, USA, 2014; ISBN 978-1-60913-605-5. [Google Scholar]
- Stehle, P. The Nutrition Report 2012 Summary. EJNFS 2014, 4, 14–62. [Google Scholar] [CrossRef]
- Abele-Brehm, A.; Brehm, W. Zur Konzeptualisierung und Messung von Befindlichkeit. Die Entwicklung der “Befindlichkeitsska-Len”. Diagnostica 1986, 32, 209–228. [Google Scholar]
- Ziemainz, H.; Peters, S. Die Messung aktuellen Wohlbefindens im Gesundheitssport: Ein kritisches Review. Sportwiss 2010, 40, 174–181. [Google Scholar] [CrossRef]
- Jawień, W. Searching for an Optimal AUC Estimation Method: A Never-Ending Task? J. Pharmacokinet. Pharmacodyn. 2014, 41, 655–673. [Google Scholar] [CrossRef] [Green Version]
- Stephens, B.R.; Granados, K.; Zderic, T.W.; Hamilton, M.T.; Braun, B. Effects of 1 Day of Inactivity on Insulin Action in Healthy Men and Women: Interaction with Energy Intake. Metabolism 2011, 60, 941–949. [Google Scholar] [CrossRef] [PubMed]
- Dawson, B.; Straton, S.; Randall, N. Oxygen Consumption during Recovery from Prolonged Submaximal Cycling below the Anaerobic Threshold. J. Sports Med. Phys. Fit. 1996, 36, 77–84. [Google Scholar]
- Chad, K.E.; Wenger, H.A. The Effect of Exercise Duration on the Exercise and Post-Exercise Oxygen Consumption. Can. J. Sport Sci. 1988, 13, 204–207. [Google Scholar] [PubMed]
- Yeung, R.R. The Acute Effects of Exercise on Mood State. J. Psychosom. Res. 1996, 40, 123–141. [Google Scholar] [CrossRef]
- Giurgiu, M.; Koch, E.D.; Plotnikoff, R.C.; Ebner-Priemer, U.W.; Reichert, M. Breaking up Sedentary Behavior Optimally to Enhance Mood. Med. Sci. Sports Exerc. 2020, 52, 457–465. [Google Scholar] [CrossRef]
- Bergouignan, A.; Legget, K.T.; De Jong, N.; Kealey, E.; Nikolovski, J.; Groppel, J.L.; Jordan, C.; O’Day, R.; Hill, J.O.; Bessesen, D.H. Effect of Frequent Interruptions of Prolonged Sitting on Self-Perceived Levels of Energy, Mood, Food Cravings and Cognitive Function. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 113. [Google Scholar] [CrossRef] [Green Version]
- De Jong, N.; Debache, I.; Pan, Z.; Garnotel, M.; Lyden, K.; Sueur, C.; Simon, C.; Bessesen, D.; Bergouignan, A. Breaking up Sedentary Time in Overweight/Obese Adults on Work Days and Non-Work Days: Results from a Feasibility Study. Int. J. Environ. Res. Public Health 2018, 15, 2566. [Google Scholar] [CrossRef] [Green Version]
- Hacker, S.; Banzer, W.; Vogt, L.; Engeroff, T. Acute Effects of Aerobic Exercise on Cognitive Attention and Memory Performance: An Investigation on Duration-Based Dose-Response Relations and the Impact of Increased Arousal Levels. J. Clin. Med. 2020, 9, 1380. [Google Scholar] [CrossRef]

{kind=link}
| Anthropometrics | n = 18 | Mean Values ± Standard Deviation 95% Confidence Interval |
|---|---|---|
| Age (Years) | 25.6 ± 2.6 24.3–26.9 | |
| Height (Meter, m) | 1.66 ± 0.07 1.63–1.69 | |
| Weight (Kilogram, kg) | 59.5 ± 9.0 55.0–64.0 | |
| Body Mass Index (BMI, kg/m2) | 21.5 ± 2.0 20.5–22.5 (Minimum: 17.5; Maximum: 25.6) | |
| Fasting Glucose (Milligrams per deciliter, mg·dL−1) | 75.8 ± 6.8 79.6–72.0 | |
| HOMA-IR | 1.0 ± 0.3 0.8–1.2 | |
| Cardiopulmonary Exercise Testing | 70% VO2max | VO2max |
| VO2 (Liters per minute, L/min) | 1.7303 ± 0.2993 1.5815–1.8791 | 2.4475 ± 0.3811 2.2580–2.6370 |
| VO2 (Milliliters per kilogram bodyweight per minute, mL/kg/min) | 29.2 ± 3.6 27.4–31.0 | 41.3 ± 4.2 39.2–43.4 |
| VCO2 (Liters per minute, L/min) | 1.8109 ± 0.3242 1.6497–1.9722 | 3.1850 ± 0.4210 2.9757–3.3944 |
| Respiratory Quotient (VCO2/VO2) | 1.05 ± 0.05 1.02–1.7 | 1.31 ± 0.05 1.28–1.33 |
| Heart rate (beats per minute) | 161 ± 9 156–165 | 190 ± 9 186–194 |
| Power (Watt) | 140 ± 28 127–154 | 249 ± 31 233–264 |
| Metabolic Equivalent of Task (Kilocalories per kilogram bodyweight per hour, kcal/(kg·h) | 9.27 ± 1.16 8.70–9.84 | 13.11 ± 1.36 12.43–13.79 |
| Energy Expenditure for 30 min exercise at 70% VO2max: | ||
| Energy Expenditure (Kilocalories, kcal) | 261.68 ± 45.40 239.10–284.26 | 370.58 ± 57.71 341.88–399.27 |
| Carbohydrate Oxidation (Grams) | 30.69 ± 12.66 24.40–37.00 | 62.80 ± 11.82 56.93–68.68 |
| Fat Oxidation (Grams) | 5.77 ± 4.58 3.50–8.05 | 0.44 ± 1.32 0.21–1.10 |
| Trial Condition (4 h Sitting with) | Two Factorial Repeated Measures ANCOVA A: Within Subject Effect of Trial Condition B: Interaction Effect C: Between Participants Effect of Caloric Intake | |||
|---|---|---|---|---|
| Exercise Breaks | Exercise Prior to Sitting | No Exercise | ||
| Insulin | ||||
| Baseline | 6.8 ± 2.7 | 6.5 ± 2.3 | 6.3 ± 2.4 | A: p = 0.414; F = 0.91; df = 1.87 B: p = 0.265; F = 1.39; df = 1.87 C: p = 0.844; F = 0.40; df = 1.00 |
| Maximal difference to baseline | 46.8 ± 14.9 *# | 61.9 ± 37.7 | 62.9 ± 27.1 | A: p = 0.012; F = 5.36; df = 1.85 B: p = 0.001; F= 8.60; df = 1.85 C: p < 0.000; F = 26.09; df = 1.00 |
| Minimal difference to baseline | −0.2 ± 4.6 | 1.2 ± 5.58 | 1.8 ± 6.0 | A: p = 0.728; F= 0.32; df = 2.00 B: p = 0.104; F= 2.65; df = 2.00 C: p < 0.000; F = 43.96; df = 1.00 |
| Incremental area under the curve | 4057.2 ± 2079.8 *# | 5346.7 ± 5000.7 | 6037.0 ± 3571.0 | A: p = 0.003; F= 7.23; df = 1.93 B: p < 0.000; F= 11.14; df = 1.93 C: p < 0.000; F= 75.70; df = 1.00 |
| Glucose | ||||
| Baseline | 76.7 ± 6.0 | 76.1 ± 6.5 | 76.6 ± 6.6 | A: p = 0.747; F = 0.24; df = 1.68 B: p = 0.815; F = 0.16; df = 1.68 C: p = 0.619; F = 0.26; df = 1.00 |
| Maximal difference to baseline | 35.4 ± 16.2 | 42.3 ± 23.0 | 47.0 ± 22.2 | A: p = 0.282; F = 1.32; df = 1.94 B: p = 0.080; F = 2.76; df = 1.94 C: p < 0.000; F = 23.08; df = 1.00 |
| Minimal difference to baseline | −11.6 ± 10.8 | −9.2 ± 7.3 | −11.3 ± 10.1 | A: p = 0.279; F = 1.33: df = 1.84 B: p = 0.380; F = 0.98; df = 1.84 C: p = 0.092; F = 3.21; df = 1.00 |
| Incremental area under the curve | 957.9 ± 1735.0 | 2144.0 ± 2399.4 | 1828.3 ± 2956.9 | A: p = 0.894; F = 0.71; df = 1.57 B: p = 0.475; F = 0.70; df = 1.57 C: p < 0.000; F = 25.27; df = 1.00 |
| Mood and Well-Being | ||||
| Positive Outcomes | Repeated measures ANCOVA Within subject effect of intervention (df = 2) | |||
| Arousal | 12.4 ± 3.2 * | 11.6 ± 4.7 | 9.9 ± 3.3 | p = 0.05; F = 3.27 |
| Elevated Mood | 15.8 ± 3.5 | 15.2 ± 4.4 | 13.2 ± 4.2 | p = 0.058; F = 3.10 |
| Thoughtfulness | 8.3 ± 2.3 | 8.6 ± 2.8 | 8.9 ± 3.8 | p = 0.637; F = 0.46 |
| Peace of Mind | 14.7 ± 3.5 | 15.2 ± 3.4 * | 12.8 ± 4.4 | p = 0.022; F = 4.25 |
| Negative Outcomes: | ||||
| Anger | 6.4 ± 1.8 | 6.1 ± 1.8 | 7.4 ± 2.8 | p = 0.105; F = 2.41 |
| Agitation | 8.6 ± 3.3 * | 8.7 ± 2.5 * | 11.4 ± 4.9 | p = 0.003; F = 6.74 |
| Depression | 6.4 ± 1.8 * | 7.4 ± 3.0 | 8.7 ± 3.6 | p = 0.033; F = 3.76 |
| Lack of Energy | 11.9 ± 4.0 | 14.3 ± 5.4 | 15.2 ± 6.1 | p = 0.056; F = 3.14 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Engeroff, T.; Füzeki, E.; Vogt, L.; Banzer, W. The Acute Effects of Single or Repeated Bouts of Vigorous-Intensity Exercise on Insulin and Glucose Metabolism during Postprandial Sedentary Behavior. Int. J. Environ. Res. Public Health 2022, 19, 4422. https://doi.org/10.3390/ijerph19084422
Engeroff T, Füzeki E, Vogt L, Banzer W. The Acute Effects of Single or Repeated Bouts of Vigorous-Intensity Exercise on Insulin and Glucose Metabolism during Postprandial Sedentary Behavior. International Journal of Environmental Research and Public Health. 2022; 19(8):4422. https://doi.org/10.3390/ijerph19084422
Chicago/Turabian StyleEngeroff, Tobias, Eszter Füzeki, Lutz Vogt, and Winfried Banzer. 2022. "The Acute Effects of Single or Repeated Bouts of Vigorous-Intensity Exercise on Insulin and Glucose Metabolism during Postprandial Sedentary Behavior" International Journal of Environmental Research and Public Health 19, no. 8: 4422. https://doi.org/10.3390/ijerph19084422
APA StyleEngeroff, T., Füzeki, E., Vogt, L., & Banzer, W. (2022). The Acute Effects of Single or Repeated Bouts of Vigorous-Intensity Exercise on Insulin and Glucose Metabolism during Postprandial Sedentary Behavior. International Journal of Environmental Research and Public Health, 19(8), 4422. https://doi.org/10.3390/ijerph19084422