
Discriminating Potential Genetic Markers for Complete Response and Non-Complete Response Patients to Neoadjuvant Chemotherapy with Locally Advanced Rectal Cancer

 ,
,  , ,
, ,  and
and
Abstract
:1. Introduction
1.1. Biomarker Discovery for the Prediction of Tumor Response to Neoadjuvant Chemoradiotherapy in Locally Advanced Rectal Cancer
1.2. Patients
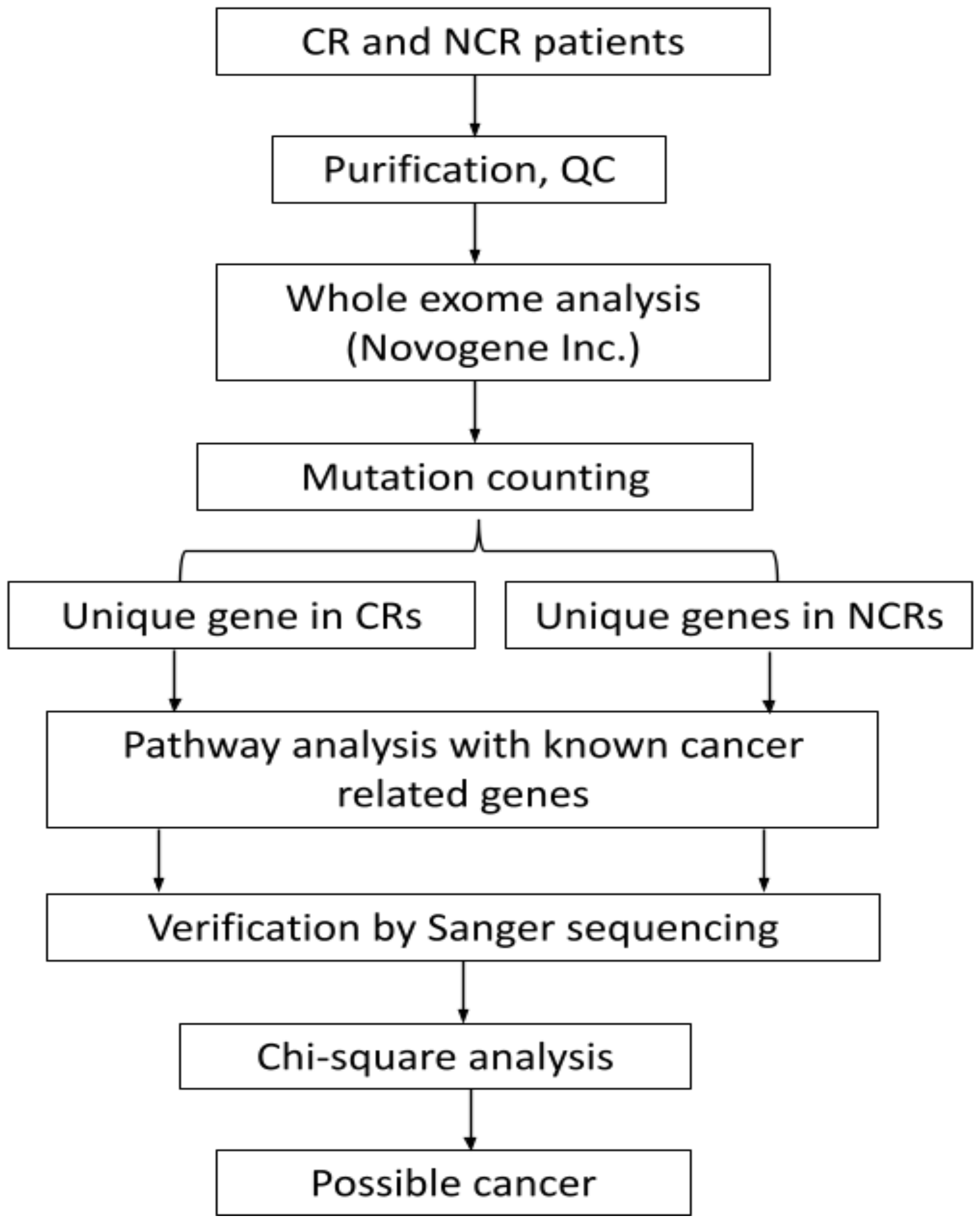
2. Materials and Methods
3. Results
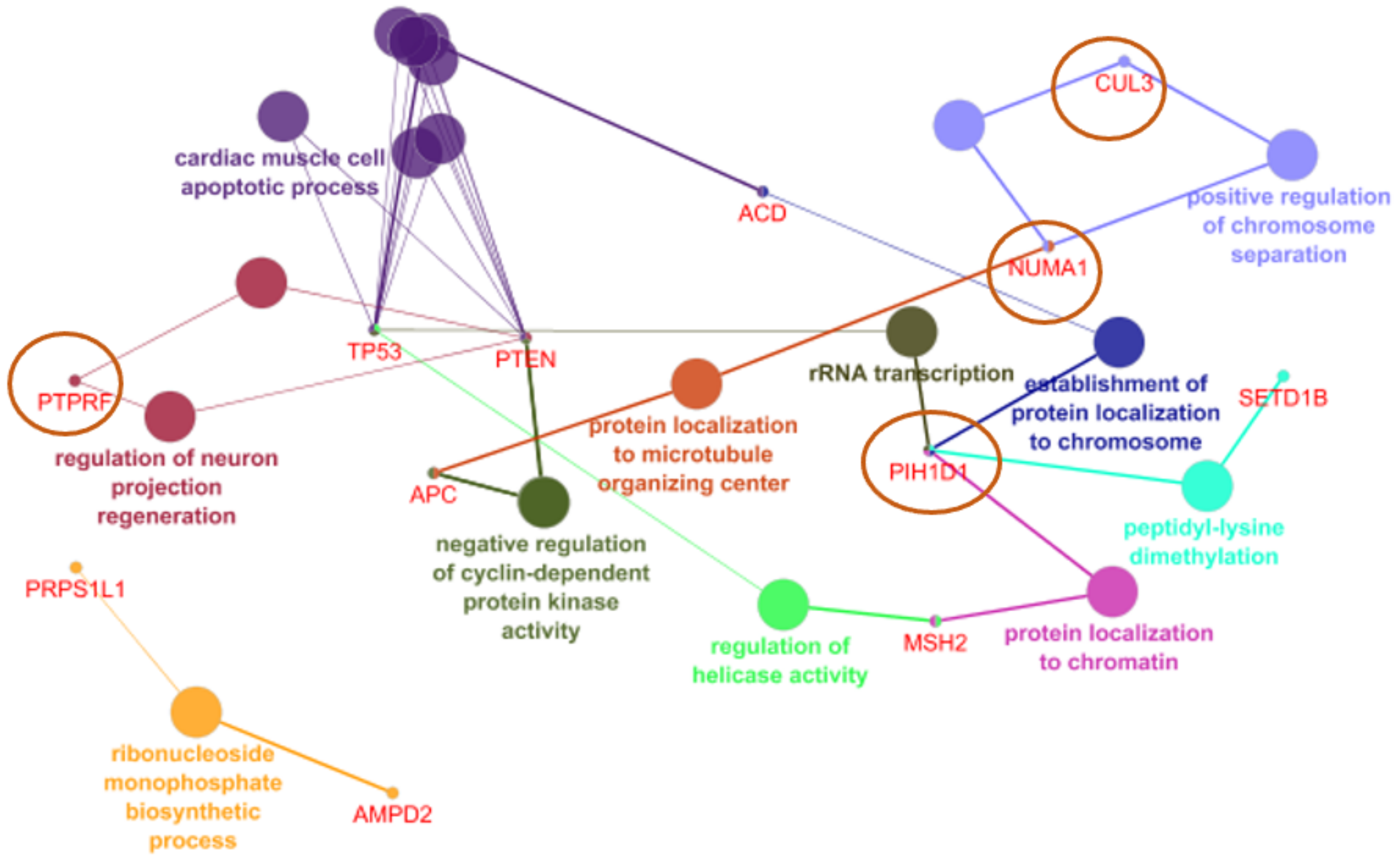
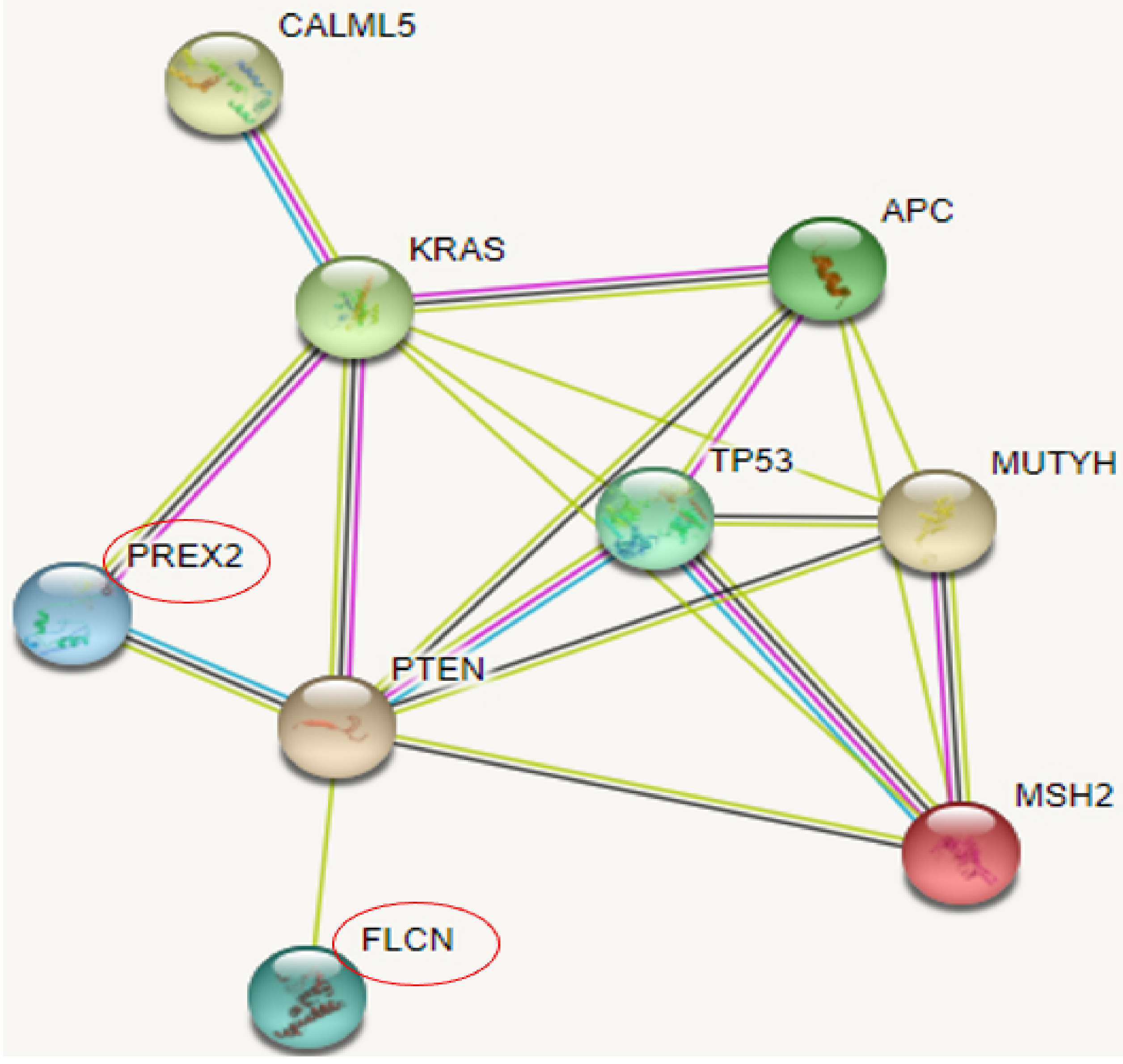
3.1. NCR Genes and Their Association with Rectal Cancer Related Genes through Pathway Analysis
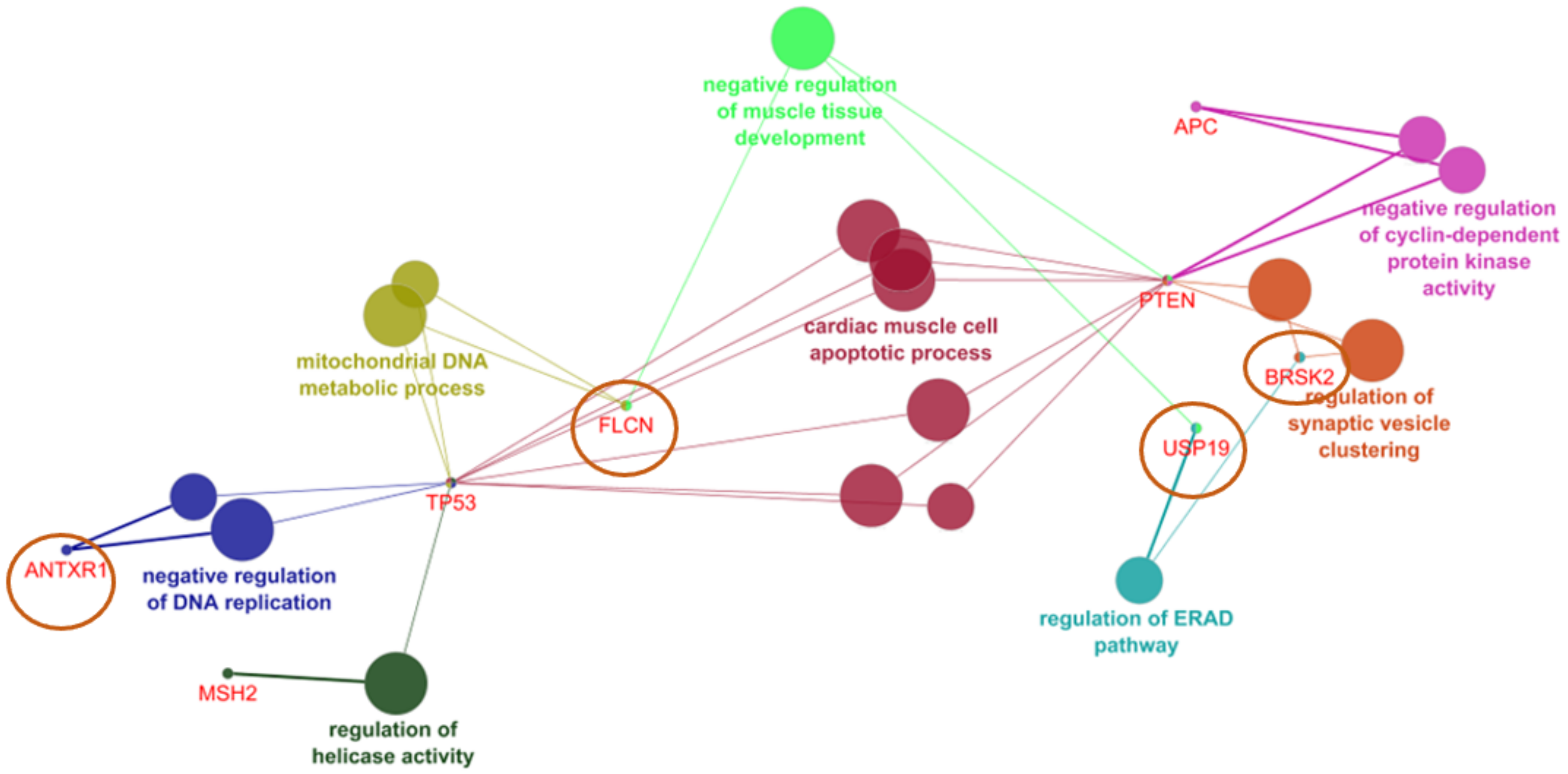
3.2. CR Genes and Their Association with Rectal Cancer Related Genes through Pathway Analysis
3.3. SNPs in the Genes, Found in CR and NCR Groups
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sauer, R.; Becker, H.; Hohenberger, W.; Rodel, C.; Wittekind, C.; Fietkau, R.; Martus, P.; Tschmelitsch, J.; Hager, E.; Hess, C.F.; et al. Preoperative versus Postoperative Chemoradiotherapy for Rectal Cancer. N. Engl. J. Med. 2004, 351, 1731–1740. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sauer, R.; Liersch, T.; Merkel, S.; Fietkau, R.; Hohenberger, W.; Hess, C.; Becker, H.; Raab, H.-R.; Villanueva, M.-T.; Witzigmann, H.; et al. Preoperative Versus Postoperative Chemoradiotherapy for Locally Advanced Rectal Cancer: Results of the German CAO/ARO/AIO-94 Randomized Phase III Trial After a Median Follow-Up of 11 Years. J. Clin. Oncol. 2012, 30, 1926–1933. [Google Scholar] [CrossRef]
- Alkan, A.; Hofving, T.; Angenete, E.; Yrlid, U. Biomarkers and cell-based models to predict the outcome of neoadjuvant therapy for rectal cancer patients. Biomark. Res. 2021, 9, 60. [Google Scholar] [CrossRef]
- Brown, C.L.; Ternent, C.A.; Thorson, A.G.; Christensen, M.A.; Blatchford, G.J.; Shashidharan, M.; Haynatzki, G.R. Response to Preoperative Chemoradiation in Stage II and III Rectal Cancer. Dis. Colon Rectum 2003, 46, 1189–1193. [Google Scholar] [CrossRef]
- Martin, S.T.; Heneghan, H.; Winter, D.C. Systematic review and meta-analysis of outcomes following pathological complete response to neoadjuvant chemoradiotherapy for rectal cancer. Br. J. Surg. 2012, 99, 918–928. [Google Scholar] [CrossRef]
- Bogaert, J.; Prenen, H. Molecular genetics of colorectal cancer. Ann. Gastroenterol. 2014, 27, 9–14. [Google Scholar]
- Jeter, J.M.; Kohlmann, W.; Gruber, S.B. Genetics of colorectal cancer. Oncology 2006, 20, 269–276; discussion 285–286, 288–289. [Google Scholar]
- Chung, D.C.; Rustgi, A.K. DNA mismatch repair and cancer. Gastroenterology 1995, 109, 1685–1699. [Google Scholar] [CrossRef]
- Weinberg, R.A. Oncogenes and tumor suppressor genes. CA Cancer J. Clin. 1994, 44, 160–170. [Google Scholar] [CrossRef]
- American Society of Clinical Oncology. Cancer Genetics and Cancer Predisposition Testing. ASCO Curriculum; American Society of Clinical Oncology: Alexandria, VA, USA, 1998; Volume 1. [Google Scholar]
- Knudson, A.G., Jr. Mutation and Cancer: Statistical Study of Retinoblastoma. Proc. Natl. Acad. Sci. USA 1971, 68, 820–823. [Google Scholar] [CrossRef] [Green Version]
- Sherr, C.J. Cancer cell cycles. Science 1996, 274, 1672–1677. [Google Scholar] [CrossRef] [Green Version]
- Markowitz, S.; Wang, J.; Myeroff, L.; Parsons, R.; Sun, L.; Lutterbaugh, J.; Fan, R.S.; Zborowska, E.; Kinzler, K.W.; Vogelstein, B.; et al. Inactivation of the type II TGF-beta receptor in colon cancer cells with microsatellite instability. Science 1995, 268, 1336–1338. [Google Scholar] [CrossRef]
- Armaghany, T.; Wilson, J.D.; Chu, Q.; Mills, G. Genetic Alterations in Colorectal Cancer. Gastrointest. Cancer Res. 2012, 5, 19–27. [Google Scholar]
- De la Chapelle, A. Genetic predisposition to colorectal cancer. Nat. Rev. Cancer 2004, 4, 769–780. [Google Scholar] [CrossRef]
- Chung, D.C. The genetic basis of colorectal cancer: Insights into critical pathways of tumorigenesis. Gastroenterology 2000, 119, 854–865. [Google Scholar] [CrossRef]
- Dienstmann, R.; Tabernero, J. Spectrum of Gene Mutations in Colorectal Cancer: Implications for Treatment. Cancer J. 2016, 22, 149–155. [Google Scholar] [CrossRef]
- Fearon, E.R. Molecular Genetics of Colorectal Cancer. Annu. Rev. Pathol. Mech. Dis. 2011, 6, 479–507. [Google Scholar] [CrossRef]
- Velho, S.; Moutinho, C.; Cirnes, L.; Albuquerque, C.; Hamelin, R.; Schmitt, F.; Carneiro, F.; Oliveira, C.; Seruca, R. BRAF, KRAS and PIK3CA mutations in colorectal serrated polyps and cancer: Primary or secondary genetic events in colorectal carcinogenesis? BMC Cancer 2008, 8, 255. [Google Scholar] [CrossRef] [Green Version]
- Powell, S.M.; Zilz, N.; Beazer-Barclay, Y.; Bryan, T.M.; Hamilton, S.R.; Thibodeau, S.N.; Vogelstein, B.; Kinzler, K.W. APC mutations occur early during colorectal tumorigenesis. Nature 1992, 359, 235–237. [Google Scholar] [CrossRef]
- Coppedè, F.; Lopomo, A.; Spisni, R.; Migliore, L. Genetic and epigenetic biomarkers for diagnosis, prognosis and treatment of colorectal cancer. World J. Gastroenterol. 2014, 20, 943–956. [Google Scholar] [CrossRef]
- Leslie, A.; Carey, F.A.; Pratt, N.R.; Steele, R.J. The colorectal adenoma–carcinoma sequence. Br. J. Surg. 2002, 89, 845–860. [Google Scholar] [CrossRef] [Green Version]
- Steele, R.J.C.; Thompson, A.M.; Hall, P.A.; Lane, D.P. The p53 tumour suppressor gene. Br. J. Surg. 1998, 85, 1460–1467. [Google Scholar] [CrossRef] [Green Version]
- Takayama, T.; Miyanishi, K.; Hayashi, T.; Sato, Y.; Niitsu, Y. Colorectal cancer: Genetics of development and metastasis. J. Gastroenterol. 2006, 41, 185–192. [Google Scholar] [CrossRef]
- Hong, S.B.; Oh, H.; Valera, V.A.; Stull, J.; Ngo, D.T.; Baba, M.; Merino, M.J.; Linehan, W.M.; Schmidt, L.S. Tumor suppressor FLCN inhibits tumorigenesis of a FLCN-null renal cancer cell line and regulates ex-pression of key molecules in TGF-beta signaling. Mol. Cancer 2010, 9, 160. [Google Scholar] [CrossRef] [Green Version]
- Wada, S.; Neinast, M.; Jang, C.; Ibrahim, Y.H.; Lee, G.; Babu, A.; Li, J.; Hoshino, A.; Rowe, G.; Rhee, J.; et al. The tumor suppressor FLCN mediates an alternate mTOR pathway to regulate browning of adipose tissue. Genes Dev. 2016, 30, 2551–2564. [Google Scholar] [CrossRef] [Green Version]
- Nahorski, M.S.; Lim, D.H.; Martin, L.; Gille, J.J.; McKay, K.; Rehal, P.K.; Ploeger, H.M.; Van Steensel, M.; Tomlinson, I.P.; Latif, F.; et al. Investigation of the Birt-Hogg-Dube tumour suppressor gene (FLCN) in familial and sporadic colorectal cancer. J. Med. Genet. 2010, 47, 385–390. [Google Scholar] [CrossRef] [Green Version]
- Truong, H.T.; Dudding, T.; Blanchard, C.L.; Elsea, S.H. Frameshift mutation hotspot identified in Smith-Magenis syndrome: Case report and review of literature. BMC Med. Genet. 2010, 11, 142. [Google Scholar] [CrossRef] [Green Version]
- Cai, C.; Dang, W.; Liu, S.; Huang, L.; Li, Y.; Li, G.; Yan, S.; Jiang, C.; Song, X.; Hu, Y.; et al. Anthrax toxin receptor 1/tumor endothelial marker 8 promotes gastric cancer progression through activation of the PI3K/AKT/mTOR signaling pathway. Cancer Sci. 2020, 111, 1132–1145. [Google Scholar] [CrossRef]
- Cheng, B.; Liu, Y.; Zhao, Y.; Li, Q.; Liu, Y.; Wang, J.; Chen, Y.; Zhang, M. The role of anthrax toxin protein receptor 1 as a new mechanosensor molecule and its mechanotransduction in BMSCs under hydrostatic pressure. Sci. Rep. 2019, 9, 12642. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Debald, M.; Schildberg, F.A.; Linke, A.; Walgenbach, K.; Kuhn, W.; Hartmann, G.; Walgenbach-Bruenagel, G. Specific expression of k63-linked ubiquitination of calmodulin-like protein 5 in breast cancer of premen-opausal patients. J. Cancer Res. Clin. Oncol. 2013, 139, 2125–2132. [Google Scholar] [CrossRef] [PubMed]
- Shan, J.; Liu, Y.; Wang, Y.; Li, Y.; Yu, X.; Wu, C. GALNT14 Involves the Regulation of Multidrug Resistance in Breast Cancer Cells. Transl. Oncol. 2018, 11, 786–793. [Google Scholar] [CrossRef] [PubMed]
- Tsou, Y.-K.; Liang, K.-H.; Lin, W.-R.; Chang, H.-K.; Tseng, C.-K.; Yeh, C.-T. GALNT14 genotype as a response predictor for concurrent chemoradiotherapy in advanced esophageal squamous cell carcinoma. Oncotarget 2017, 8, 29151–29160. [Google Scholar] [CrossRef] [Green Version]
- Broughton, S.; Hercus, T.; Hardy, M.P.; McClure, B.J.; Nero, T.; Dottore, M.; Huynh, H.; Braley, H.; Barry, E.F.; Kan, W.L.; et al. Dual Mechanism of Interleukin-3 Receptor Blockade by an Anti-Cancer Antibody. Cell Rep. 2014, 8, 410–419. [Google Scholar] [CrossRef] [Green Version]
- Levin, A.; Minis, A.; Lalazar, G.; Rodríguez, J.; Steller, H. PSMD5 inactivation promotes 26S proteasome assembly during colorectal tumor progression. Cancer Res. 2018, 78, 3458–3468. [Google Scholar] [CrossRef] [Green Version]
- Hisamatsu, T.; McGuire, M.; Wu, S.Y.; Rupaimoole, R.; Pradeep, S.; Bayraktar, E.; Noh, K.; Hu, W.; Hansen, J.M.; Lyons, Y.; et al. PRKRA/PACT Expression Promotes Chemoresistance of Mucinous Ovarian Cancer. Mol. Cancer Ther. 2019, 18, 162–172. [Google Scholar] [CrossRef] [Green Version]
- Neilsen, B.; Frodyma, D.E.; Lewis, R.E.; Fisher, K.W. KSR as a therapeutic target for Ras-dependent cancers. Expert Opin. Ther. Targets 2017, 21, 499–509. [Google Scholar] [CrossRef]
- Quadri, H.S.; Aiken, T.J.; Allgaeuer, M.; Moravec, R.; Altekruse, S.; Hussain, S.P.; Miettinen, M.M.; Hewitt, S.M.; Rudloff, U. Expression of the scaffold connector enhancer of kinase suppressor of Ras 1 (CNKSR1) is correlated with clinical outcome in pancreatic cancer. BMC Cancer 2017, 17, 495. [Google Scholar] [CrossRef] [Green Version]
- Chen, H.-Y.; Chen, R.-H. Cullin 3 Ubiquitin Ligases in Cancer Biology: Functions and Therapeutic Implications. Front. Oncol. 2016, 6, 113. [Google Scholar] [CrossRef] [Green Version]
- Chen, R.-H. Cullin 3 and Its Role in Tumorigenesis. Adv. Exp. Med. Biol. 2020, 1217, 187–210. [Google Scholar] [CrossRef]
- Zhang, Y.; Fan, H.; Fang, S.; Wang, L.; Chen, L.; Jin, Y.; Jiang, W.; Lin, Z.; Shi, Y.; Zhan, C.; et al. Mutations and expression of the NFE2L2/KEAP1/CUL3 pathway in Chinese patients with lung squamous cell carcinoma. J. Thorac. Dis. 2016, 8, 1639–1644. [Google Scholar] [CrossRef] [Green Version]
- Kakihara, Y.; Kiguchi, T.; Ohazama, A.; Saeki, M. R2TP/PAQosome as a promising chemotherapeutic target in cancer. Jpn. Dent. Sci. Rev. 2020, 56, 38–42. [Google Scholar] [CrossRef]
- Kamano, Y.; Saeki, M.; Egusa, H.; Kakihara, Y.; Houry, W.A.; Yatani, H.; Kamisaki, Y. PIH1D1 interacts with mTOR complex 1 and enhances ribosome RNA transcription. FEBS Lett. 2013, 587, 3303–3308. [Google Scholar] [CrossRef] [Green Version]
- Du, Y.; Lu, F.; Li, P.; Ye, J.; Ji, M.; Ma, D.; Ji, C. SMG1 Acts as a Novel Potential Tumor Suppressor with Epigenetic Inactivation in Acute Myeloid Leukemia. Int. J. Mol. Sci. 2014, 15, 17065–17076. [Google Scholar] [CrossRef]
- Bokhari, A.; Jonchere, V.; Lagrange, A.; Bertrand, R.; Svrcek, M.; Marisa, L.; Buhard, O.; Greene, M.; Demidova, A.; Jia, J.; et al. Targeting nonsense-mediated mRNA decay in colorectal cancers with microsatellite instability. Oncogenesis 2018, 7, 70. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient Info | Number | |
|---|---|---|
| Reaction to radiotherapy | CR | 14 |
| NCR | 15 | |
| Gender | Male | 23 |
| Female | 6 | |
| Age group (Years) | Under 40 | 1 |
| 40–49 | 2 | |
| 50–59 | 9 | |
| 60–69 | 8 | |
| 70–79 | 4 | |
| Over 80 | 5 |
| Unique Genes in CRs |
| Only occurred in CRs: USP19, RPUSD3 |
| More commonly mutated in CRs: PREX2, IRGM, TTLL3, HELT, FLCN, EDDM3B, WARS2, PDE4A, KIAA0895L, GLIS1, OR11A1, DCAF4, DHFRL1, C17orf96, ALDH5A1, ANTXR1, ACBD5, ELF1, DCTN4, NAV1, RAI14, CALML5, BRSK2 |
| Unique Genes in NCRs |
| Only occurred in NCRs: OR5L1, MRM1, GALNT14, THEMIS, SLC5A11, PTPRF, OR5L2, MED12L, KRTAP19-8, KNOP1, HIP1, DAZL |
| More commonly mutated in NCRs: IL3RA, AMER2, GPA33, ZNF546, PSMD5, CLEC3A, ZNF552, YDJC, SMG1, SAMD7, NCBP3, HPS1, TIMM21, RBP1, SLC4A1AP, PRPS1L1, PSG8, PLSCR4, PRKRA, LRRC8B, LY6G5B, OR5I1, OR7D4, NUMA1, FILIP1L, ERC1, CPD, C2orf61, CD8B, CNKSR1, AVL9, ACD, FAAH, AMPD2, CUL3, PIH1D1, FCRL3 |
| Group | Gene | SNP | AA Change | GNOMAD_All | GNOMAD_EAS | NCBI-KR | SIFT | PPH2 | CR | NCR | Chi-sq (p < 0.05) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| CR | USP19 | rs199572044 | L305P | 0.00002628 | 0.0007692 | 0.0017 | 0.002, D | 0.925, P | 1 | NA | 0.483 |
| rs11552724 | D36H | 0.07581 | 0.03814 | 0.0606 | 0.042, D | 0.919, P | 3 | NA | 0.10 | ||
| rs144742940 | G59D | 0.0008365 | 0.02230 | 0.0623 | 0.448, T | 0.207, B | 3 | NA | 0.10 | ||
| PREX2 | rs141504768 | V678L | 0.0057 | 0.0823 | 0.0717 | 0.124, T | 0.044, B | 5 | 2 | 0.22 | |
| rs61753703 | R1394W | 0.006858 | 0.0334 | 0.0246 | 0.0, D | 1.0, D | 2 | 2 | 1.0 | ||
| rs61753704 | S1488L | 0.0178 | 0.1671 | 0.1832 | 0.038, D | 0.999, D | 4 | 1 | 0.17 | ||
| FLCN | rs3744124 | G303R | 0.07370 | 0.1792 | 0.2124 | 0.377, T | 0.002, B | 9 | 2 | 0.008 | |
| ANTXR1 | rs28365986 | R7K | 0.01144 | 0.1094 | 0.1453 | 0.467, T | 0.009, B | 9 | 1 | 0.002 | |
| NA | Y278H | NA | NA | NA | 0.532, T | 0.999, D | 1 | NA | 0.483 | ||
| CALML5 | rs10904516 | K74R | 0.3704 | 0.3016 | 0.2906 | 1.0, T | 0.76, P | 11 | 4 | 0.009 | |
| rs11546426 | S58G | 0.3147 | 0.2015 | 0.1939 | 0.015, D | 0.007, B | 4 | 4 | 1.0 | ||
| BRSK2 | rs4963048 | T760A | 0.688 | 0.4424 | 0.3690 | 1.0, T | 0.0, B | 12 | 4 | 0.003 | |
| rs752637187 | A213S | 0.00001314 | 0.0003849 | NA | 0.247, T | 0.993, D | 1 | NA | 0.483 | ||
| DCTN4 | rs11954652 | F349L | 0.2029 | 0.2454 | 0.2290 | 1.0, T | 0.0, B | 10 | 3 | 0.009 | |
| NCR | GALNT14 | rs2288101 | Q449K | 0.2141 | 0.2220 | 0.1890 | 0.921, T | 0.962, D | NA | 5 | 0.042 |
| rs188727997 | P74L | 0.00003286 | 0.00 | NA | 0.007, D | 0.977, D | NA | 1 | 1.0 | ||
| PTPRF | rs3748800 | D562N | 0.000632 | 0.01612 | 0.0342 | 0.434, T | 1.0, D | NA | 2 | 0.483 | |
| rs540407495 | E1171K | 0.00001971 | 0.0005767 | 0.00513 | 0.617, T | 0.032, B | NA | 1 | 1.0 | ||
| rs368723795 | R1207W | 0.00003942 | 0.00 | 0.00102 | 0.004, D | 0.988, D | NA | 1 | 1.0 | ||
| rs17849101 | R635C | 0.0005256 | 0.01424 | 0.01029 | 0.003, D | 1.0, D | NA | 1 | 1.0 | ||
| IL3RA | rs17883366 | V323L | 0.1410 | 0.09604 | NA | 1.0, T | 0.0, B | NA | 5 | 0.042 | |
| rs201668157 | F281L | 0.00005934 | 0.001553 | NA | 0.78, T | 0.008, B | NA | 1 | 1.0 | ||
| PSMD5 | rs2297575 | E21G | 0.02510 | 0.1991 | 0.1778 | 0.038, D | 0.749, P | 2 | 9 | 0.021 | |
| PRKRA | rs77419724 | I113N | 0.1372 | 0.0797 | 0.158 | 0.013, D | 0.996, D | 2 | 7 | 0.109 | |
| rs9406386 | M1L | 0.0473 | 0.0305 | 0.157 | 0.0, D | 0.0, B | 2 | 7 | 0.109 | ||
| NUMA1 | rs117729282 | L344V | 0.001064 | 0.01830 | 0.0297 | 0.326, T | 0.998, D | NA | 2 | 0.483 | |
| rs3750913 | A794G | 0.02866 | 0.0741 | 0.05631 | 0.073, T | 0.117, B | 1 | 3 | 0.598 | ||
| rs74985106 | R1681C | 0.01552 | 0.0159 | 0.0185 | 0.003, D | 1.0, D | NA | 1 | 1.0 | ||
| rs151173629 | A96V | 0.0001446 | 0.00 | 0.002 | 0.009, D | 1.0, D | NA | 1 | 1.0 | ||
| CNKSR1 | rs1045105 | H687N | 0.1185 | 0.0883 | 0.1116 | 0.658, T | 0.0, B | NA | 4 | 0.10 | |
| rs2297710 | P350Q | 0.0052 | 0.08190 | 0.0626 | 0.267, T | 0.971, D | 3 | 4 | 1.00 | ||
| ACD | rs6979 | V515A | 0.5950 | 0.1533 | 0.1269 | 1.0, T | 0.0, B | 3 | 7 | 0.245 | |
| CUL3 | rs3738952 | V567I | 0.0905 | 0.2657 | 0.3269 | 0.195, T | 0.0, B | 3 | 11 | 0.009 | |
| rs190453078 | R46H | 0.0000616 | 0.00 | NA | 0.175, T | 0.996, D | NA | 1 | 1.0 | ||
| PIH1D1 | rs13394 | V224I | 0.7767 | 0.3938 | 0.3288 | 1.0, T | 0.0, B | 4 | 11 | 0.027 | |
| rs2293013 | G10E | 0.6973 | 0.3880 | 0.3286 | 1.0, T | 0.0, B | 4 | 11 | 0.027 | ||
| rs2293012 | M9L | 0.6973 | 0.3894 | 0.3286 | 1.0, T | 0.0, B | 4 | 12 | 0.009 | ||
| SMG1 | rs147586756 | T1060I | 0.00212 | 0.05399 | 0.04778 | 0.026, D | 0.037, B | NA | 3 | 0.224 | |
| rs12051350 | A35T | 0.01738 | 0.1287 | 0.0778 | 0.133, T | 0.016, B | 1 | 5 | 0.169 | ||
| rs34960798 | Q2730E | 0.00001314 | 0.0003852 | 0.000342 | 1.0, T | 0.055, B | NA | 1 | 1.0 | ||
| rs777224856 | A2020T | 0.0000065 | 0.0001923 | 0.001027 | 0.335, T | 0.996, D | NA | 1 | 1.0 | ||
| GPA33 | rs2274531 | D20N | 0.08856 | 0.1601 | 0.1478 | 1.0, T | 0.0, B | 1 | 7 | 0.035 | |
| AMPD | rs28362581 | A82T | 0.1352 | 0.3146 | 0.2447 | 0.004, D | 0.059, B | 3 | 10 | 0.025 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bagaria, J.; Kim, K.-O.; Bagyinszky, E.; An, S.S.A.; Baek, J.-H. Discriminating Potential Genetic Markers for Complete Response and Non-Complete Response Patients to Neoadjuvant Chemotherapy with Locally Advanced Rectal Cancer. Int. J. Environ. Res. Public Health 2022, 19, 4008. https://doi.org/10.3390/ijerph19074008
Bagaria J, Kim K-O, Bagyinszky E, An SSA, Baek J-H. Discriminating Potential Genetic Markers for Complete Response and Non-Complete Response Patients to Neoadjuvant Chemotherapy with Locally Advanced Rectal Cancer. International Journal of Environmental Research and Public Health. 2022; 19(7):4008. https://doi.org/10.3390/ijerph19074008
Chicago/Turabian StyleBagaria, Jaya, Kyung-Ok Kim, Eva Bagyinszky, Seong Soo A. An, and Jeong-Heum Baek. 2022. "Discriminating Potential Genetic Markers for Complete Response and Non-Complete Response Patients to Neoadjuvant Chemotherapy with Locally Advanced Rectal Cancer" International Journal of Environmental Research and Public Health 19, no. 7: 4008. https://doi.org/10.3390/ijerph19074008
APA StyleBagaria, J., Kim, K.-O., Bagyinszky, E., An, S. S. A., & Baek, J.-H. (2022). Discriminating Potential Genetic Markers for Complete Response and Non-Complete Response Patients to Neoadjuvant Chemotherapy with Locally Advanced Rectal Cancer. International Journal of Environmental Research and Public Health, 19(7), 4008. https://doi.org/10.3390/ijerph19074008