
Analysis of the Characteristics of Cross-Regional Patient Groups and Differences in Hospital Service Utilization in Beijing



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Area and Data Source
2.2. Study Methods and Processes
2.2.1. Address Positioning and Aggregation of Cross-Regional Patients
2.2.2. Calculation of Distance-Related Elements
2.2.3. Hospital Patient Mobility Pattern Fitting
3. Results
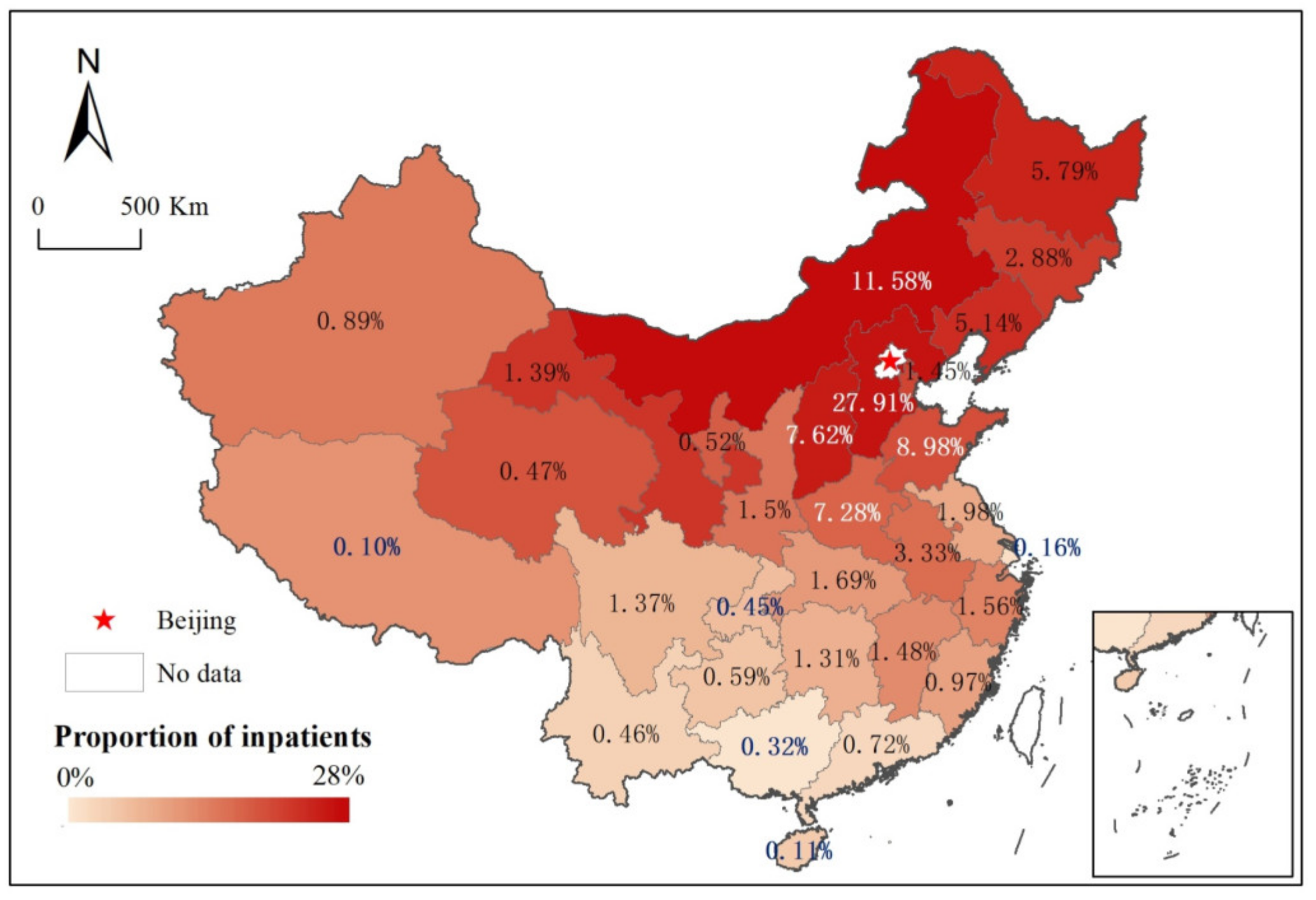
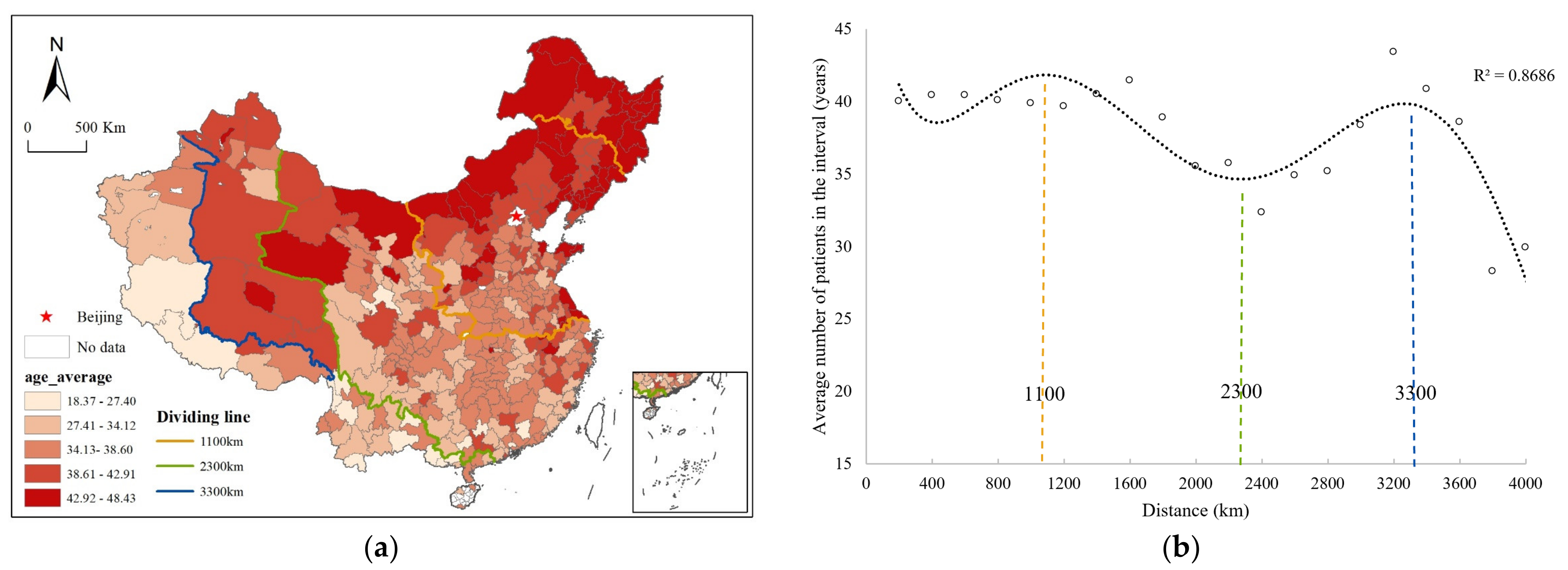
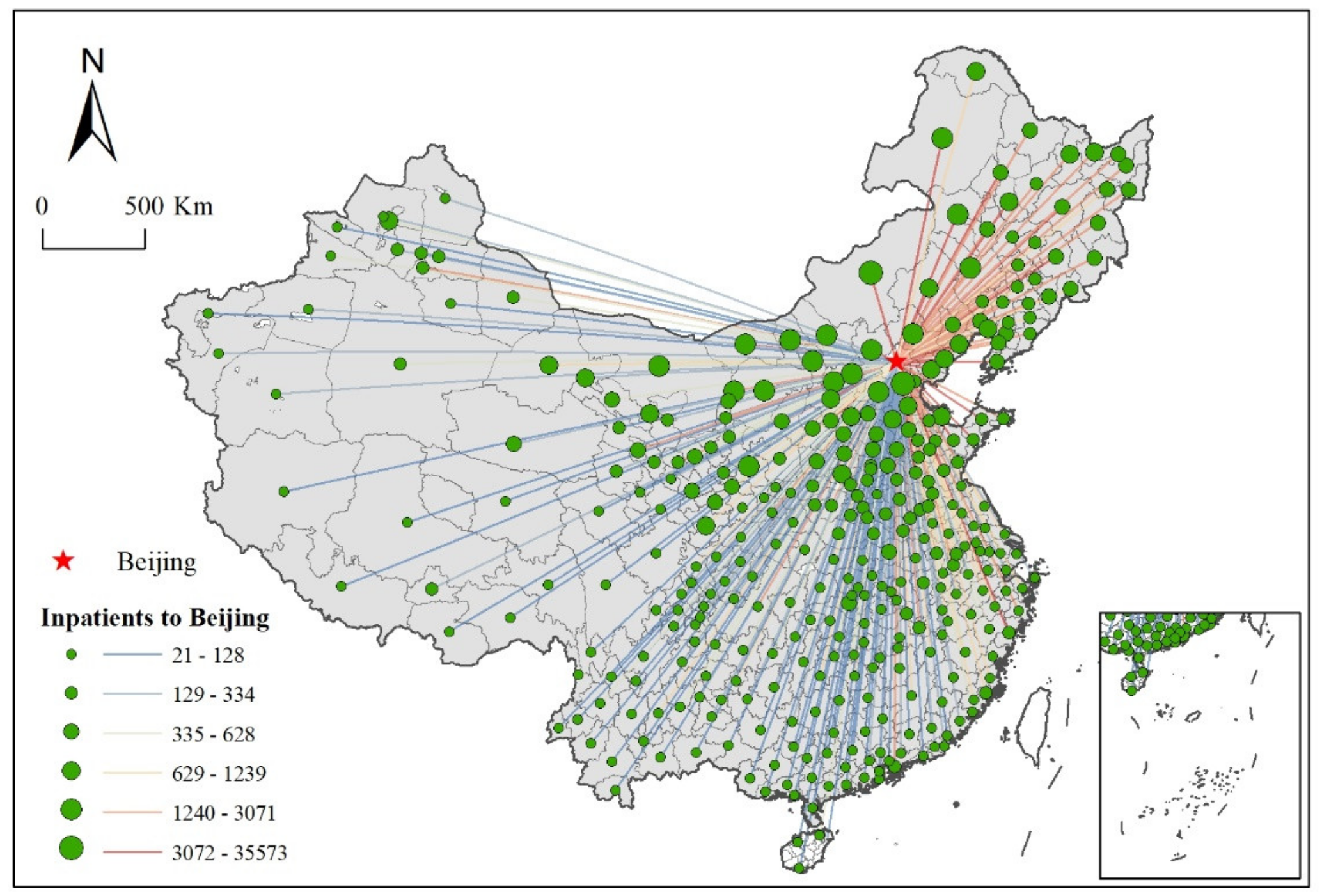
3.1. Analysis of the Characteristics of Cross-Regional Patient Groups
3.2. Differences in Cross-Regional Hospital Service Utilization
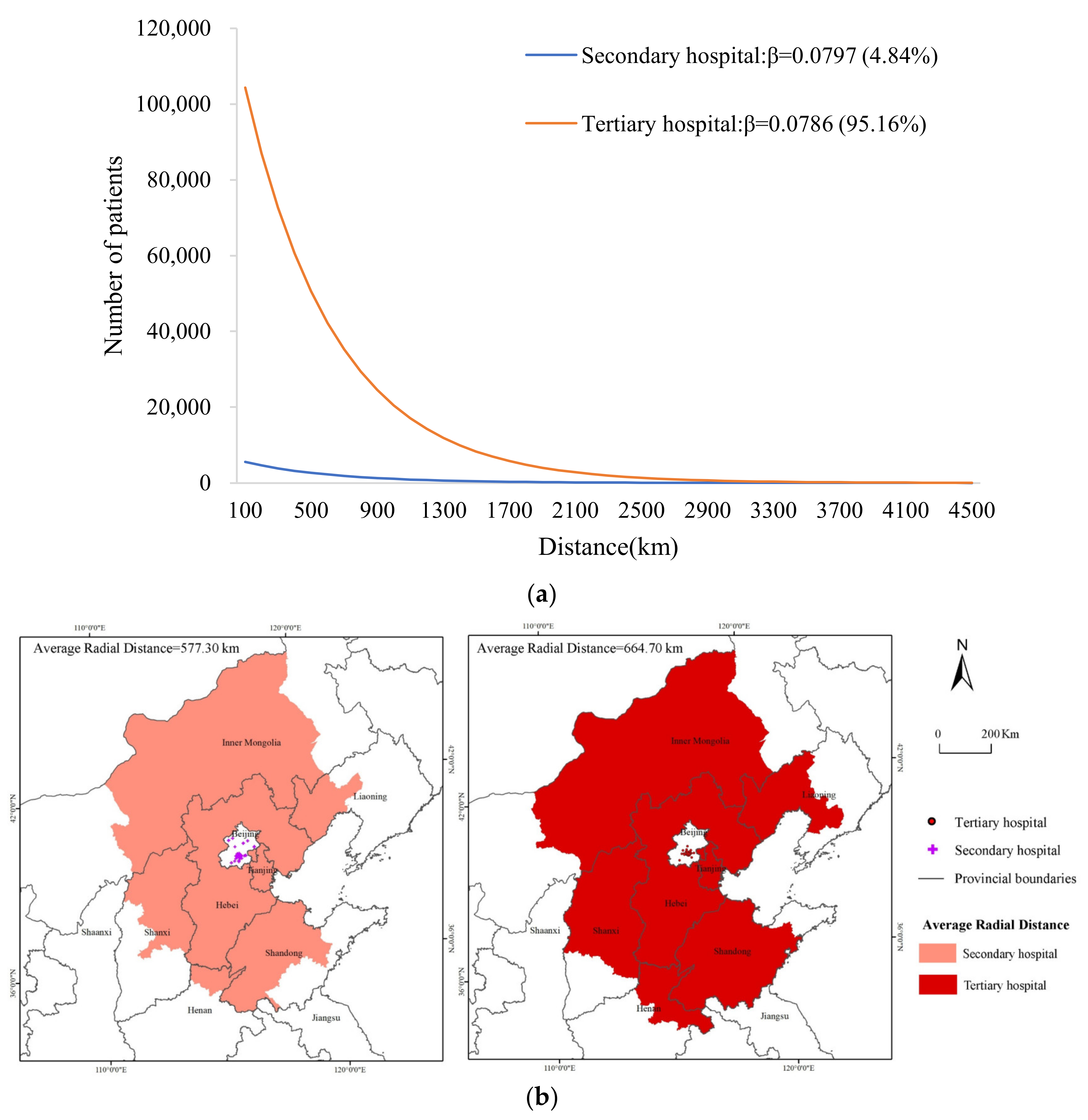
3.2.1. Cross-Regional Hospital Service Utilization at Different Levels
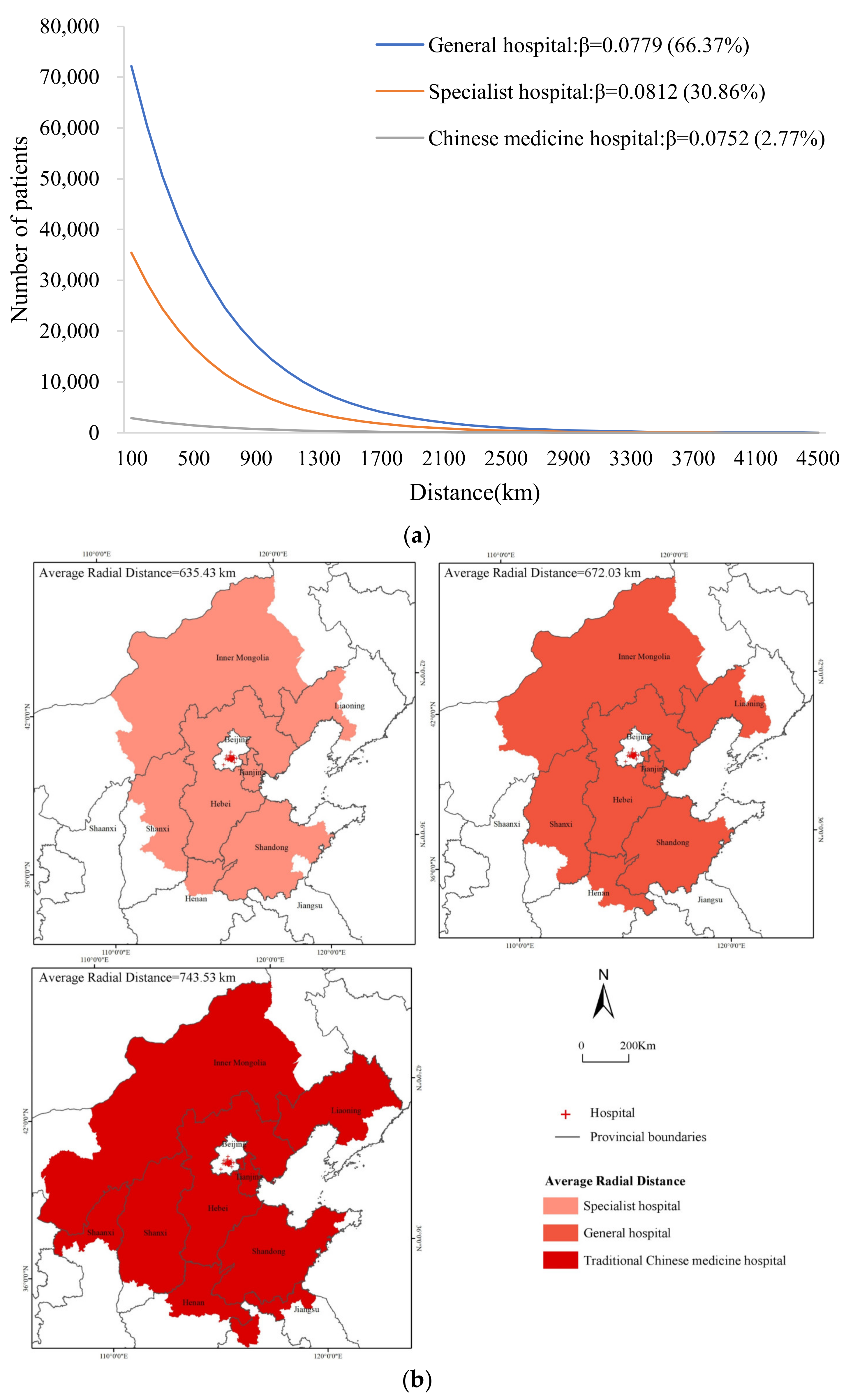
3.2.2. Cross-Regional Hospital Service Utilization of Different Types of Hospitals
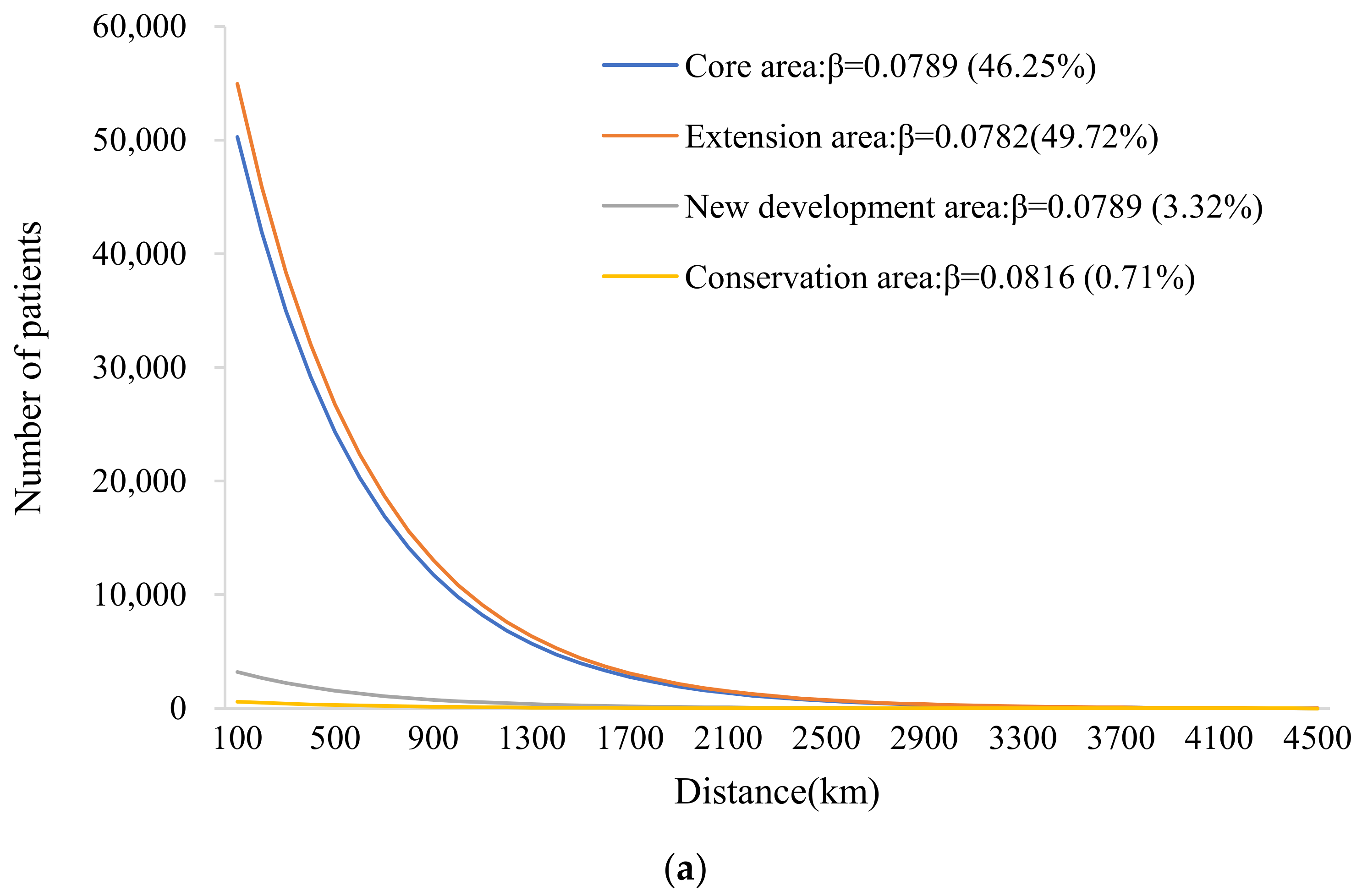
3.2.3. Cross-Regional Hospital Service Utilization in Different Functional Areas
4. Discussion
4.1. The Attractiveness of High-Quality Medical Resources to Patients of Different Ages
4.2. Several Potential Factors Affecting Patients’ Cross-Regional Mobility
4.3. The Nationality of Beijing Medical Services and the Regional Distribution of Resources
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Delil, S.; Çelik, R.N.; San, S.; Dundar, M. Clustering patient mobility patterns to assess effectiveness of health-service delivery. BMC Health Serv. Res. 2017, 17, 458. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, L.; Li, F.; Wang, C.; Chen, W.; Xie, Z.; Jin, C. Analysis on the impact of non-residents’ medical service utilization on medical services system of Shanghai. Chin. Health Res. 2014, 17, 330–333. [Google Scholar]
- Athanasakis, K.; Souliotis, K.; Kyriopoulos, E.J.; Loukidou, E.; Kritikou, P.; Kyriopoulos, J. Inequalities in access to cancer treatment: An analysis of cross-regional patient mobility in Greece. Support. Care Cancer 2012, 20, 455–460. [Google Scholar] [CrossRef] [PubMed]
- Yan, X.; Dong, D.; He, S.; Webster, C. Examining trans-provincial diagnosis of rare diseases in china: The importance of healthcare resource distribution and patient mobility. Sustainability 2020, 12, 5444. [Google Scholar] [CrossRef]
- Balia, S.; Brau, R.; Moro, D. Choice of hospital and long-distances: Evidence from Italy. Reg. Sci. Urban Econ. 2020, 81, 103502. [Google Scholar] [CrossRef]
- Peng, B.; Zhang, H.; Shi, L.; Ling, L. Migration status and healthcare seeking behaviours among the Chinese labor-force: A nationally representative study. BMJ Open 2019, 9, e031798. [Google Scholar] [CrossRef]
- Kelly, C.; Hulme, C.; Farragher, T.; Clarke, G. Are differences in travel time or distance to healthcare for adults in global north countries associated with an impact on health outcomes? A systematic review. BMJ Open 2016, 6, e013059. [Google Scholar] [CrossRef]
- Beukers, P.D.; Kemp, R.G.; Varkevisser, M. Patient hospital choice for hip replacement: Empirical evidence from the Netherlands. Eur. J. Health Econ. 2014, 15, 927–936. [Google Scholar] [CrossRef]
- Messina, G.; Forni, S.; Collini, F.; Quercioli, C.; Nante, N. Patient mobility for cardiac problems: A risk-adjusted analysis in Italy. BMC Health Serv. Res. 2013, 13, 56. [Google Scholar] [CrossRef] [Green Version]
- Berta, P.; Guerriero, C.; Levaggi, R. Hospitals’ strategic behaviours and patient mobility: Evidence from Italy. Socio-Econ. Plan. Sci. 2021, 77, 101030. [Google Scholar] [CrossRef]
- Li, Y.; Liu, L.; Chen, J.; Zhang, J. Medical travel of cardiovascular and cerebrovascular diseases inpatients in central China. Appl. Geogr. 2021, 127, 102391. [Google Scholar] [CrossRef]
- Koylu, C.; Delil, S.; Guo, D.; Celik, R.N. Analysis of big patient mobility data for identifying medical regions, spatio-temporal characteristics and care demands of patients on the move. Int. J. Health Geogr. 2018, 17, 32. [Google Scholar] [CrossRef]
- Fu, L.; Xu, K.; Liu, F.; Liang, L.; Wang, Z. Regional Disparity and Patients Mobility: Benefits and Spillover Effects of the Spatial Network Structure of the Health Services in China. Int. J. Environ. Res. Public Health 2021, 18, 1096. [Google Scholar] [CrossRef]
- Wang, C.; Wang, F.; Onega, T. Spatial behavior of cancer care utilization in distance decay in the Northeast region of the US. Travel Behav. Soc. 2021, 24, 291–302. [Google Scholar] [CrossRef]
- Liu, Z.; Yang, H.; Xiong, W.; Chen, G. Spatial Accessibilities of Medical Services at County Level Based on Optimized Two-step Floating Catchment Area Method. Sci. Geogr. Sin. 2017, 37, 728–737. [Google Scholar]
- Xiong, X.; Luo, L. Inpatient flow distribution patterns at Shanghai hospitals. Int. J. Environ. Res. Public Health 2020, 17, 2183. [Google Scholar] [CrossRef] [Green Version]
- Halás, M.; Klapka, P.; Kladivo, P. Distance-decay functions for daily travel-to-work flows. J. Transp. Geogr. 2014, 35, 107–119. [Google Scholar] [CrossRef]
- Jia, P.; Wang, F.; Xierali, I.M. Differential effects of distance decay on hospital inpatient visits among subpopulations in Florida, USA. Environ. Monit. Assess. 2019, 191, 381. [Google Scholar] [CrossRef] [Green Version]
- National Health and Family Planning Commission of China. National Report on the Services, Quality and Safety in Medical Care System (2015); People’s Medical Publishing House: Beijing, China, 2016.
- Wang, M.; Bao, H.X. Behavioural insights into housing relocation decisions: The effects of the Beijing Olympics. Habitat Int. 2015, 47, 20–28. [Google Scholar] [CrossRef] [Green Version]
- Smith, S.L.J. Tourism Analysis: A Handbook; Longman: Harlow, UK, 1989. [Google Scholar]
- Kang, C.; Sobolevsky, S.; Liu, Y.; Ratti, C. Exploring human movements in Singapore: A comparative analysis based on mobile phone and taxicab usages. In Proceedings of the 2nd ACMSIGKDD International Workshop on Urban Computing, Chicago, IL, USA, 11–14 August 2013. [Google Scholar]
- Shen, Y.; Li, L. The influence of medical facility accessibility on residents’ health seeking behaviors from the perspective of age stratification: A case study of Shanghai Chongming island. Appl. Geogr. 2021, 36, 46–54. [Google Scholar]
- Meng, Q.; Yin, D.; Mills, A.; Abbasi, K. China’s Health System Reforms: Ten Years of Progress: China’s encouraging commitment to health. BMJ 2019, 365, l4178. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Factor | OLS Model | GWR Model | ||
|---|---|---|---|---|
| β | t | |||
| Availability | −0.477 *** | −7.943 | −0.331 ** | 1.750 |
| Affordability | 0.024 | 0.528 | 0.057 | 0.647 |
| Accessibility | −0.477 *** | −10.383 | −0.743 ** | 2.451 |
| Economic level | 0.418 *** | 7.524 | 0.333 ** | 2.417 |
| R2 | 0.324 | 0.814 | ||
| Adj. R2 | 0.316 | 0.771 | ||
| AICc | 846.274 | 554.770 | ||
| Residual squares | 230.401 | 63.311 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang, Y.; Wang, Y. Analysis of the Characteristics of Cross-Regional Patient Groups and Differences in Hospital Service Utilization in Beijing. Int. J. Environ. Res. Public Health 2022, 19, 3227. https://doi.org/10.3390/ijerph19063227
Yang Y, Wang Y. Analysis of the Characteristics of Cross-Regional Patient Groups and Differences in Hospital Service Utilization in Beijing. International Journal of Environmental Research and Public Health. 2022; 19(6):3227. https://doi.org/10.3390/ijerph19063227
Chicago/Turabian StyleYang, Yu, and Yong Wang. 2022. "Analysis of the Characteristics of Cross-Regional Patient Groups and Differences in Hospital Service Utilization in Beijing" International Journal of Environmental Research and Public Health 19, no. 6: 3227. https://doi.org/10.3390/ijerph19063227
APA StyleYang, Y., & Wang, Y. (2022). Analysis of the Characteristics of Cross-Regional Patient Groups and Differences in Hospital Service Utilization in Beijing. International Journal of Environmental Research and Public Health, 19(6), 3227. https://doi.org/10.3390/ijerph19063227