
Efficacy of Breast Milk Olfactory and Gustatory Interventions on Neonates’ Biobehavioral Responses to Pain during Heel Prick Procedures


Abstract
:1. Introduction
1.1. Background
1.2. Aims
2. Materials and Methods
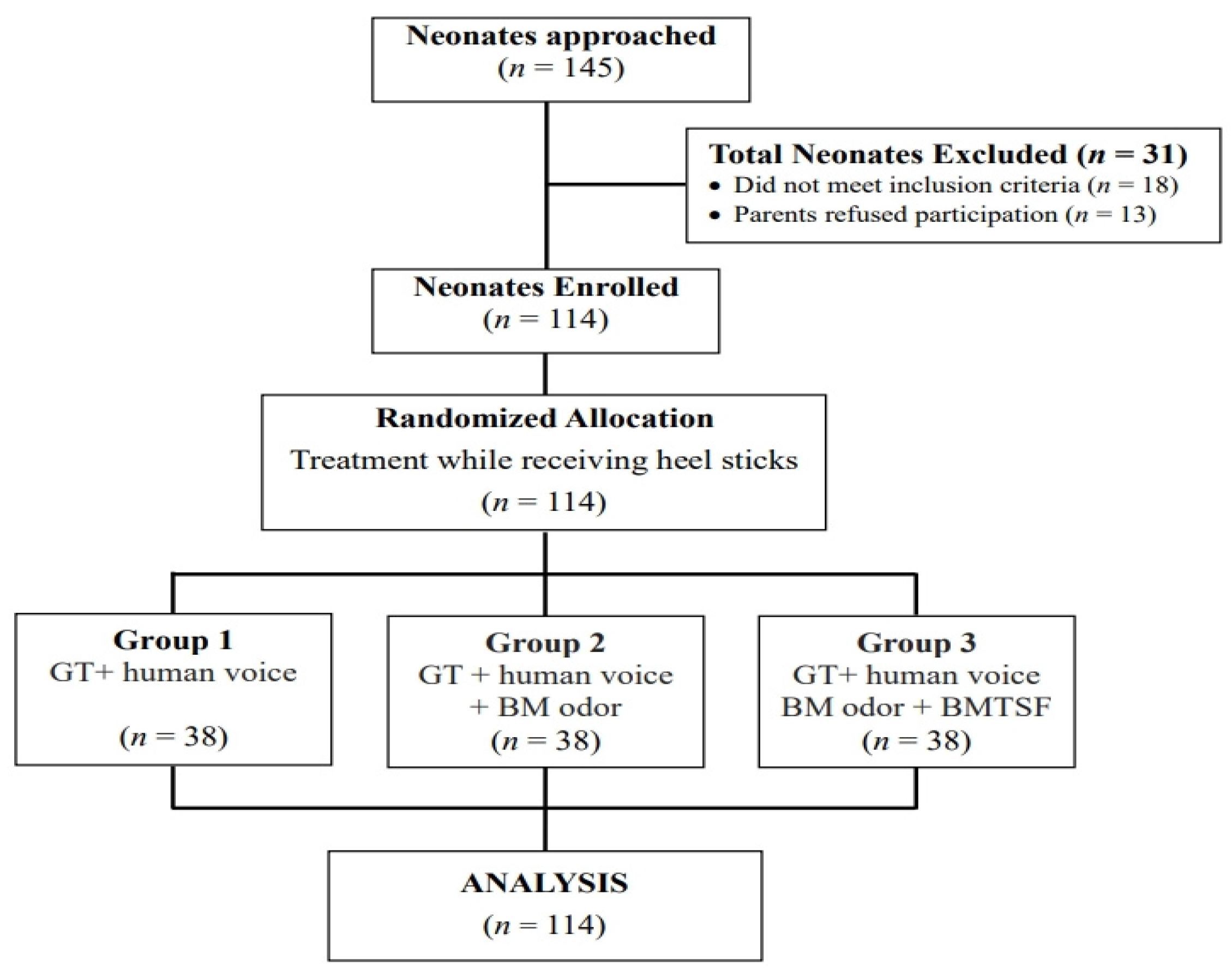
2.1. Design
2.2. Sample and Setting
2.3. Measures
2.3.1. Biological Responses to Pain
2.3.2. Behavioral Response to Pain
2.4. Data Collection
2.4.1. Heel Pricks
2.4.2. Intervention
2.4.3. Study Fidelity
2.5. Ethical Considerations
2.6. Statistical Analyses
3. Results
3.1. Characteristics of the Neonates
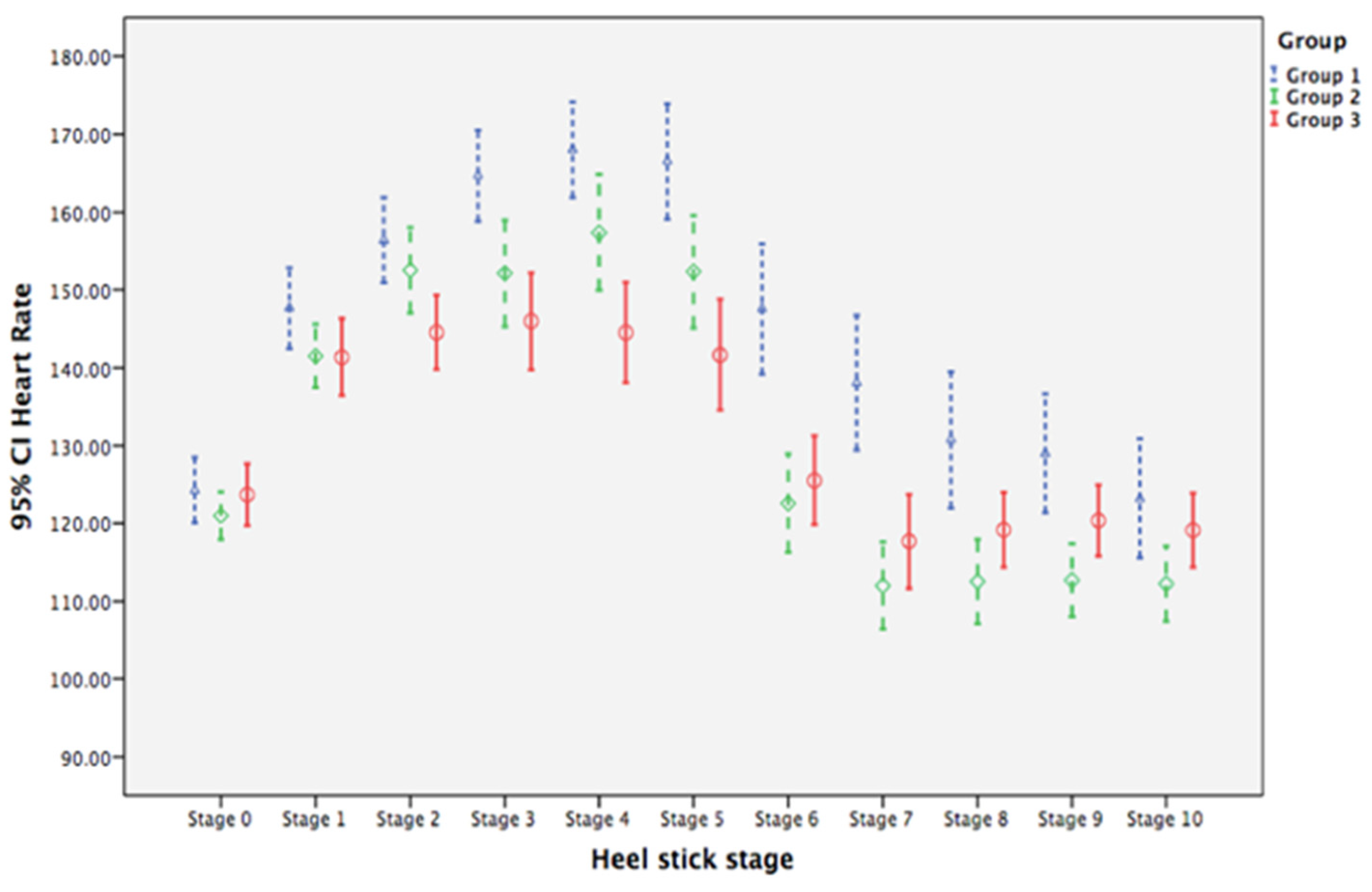
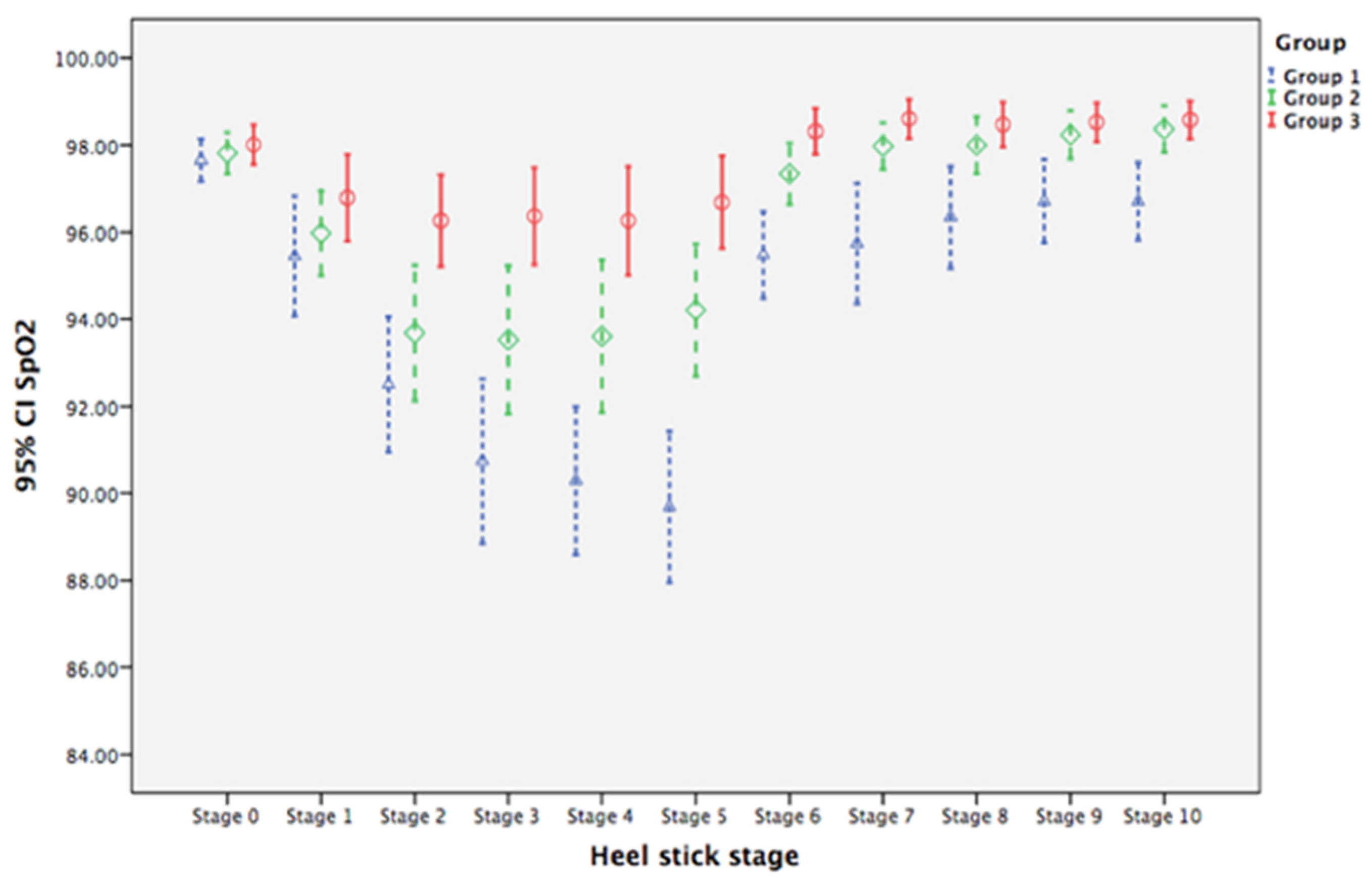
3.2. Biological Parameters of Pain
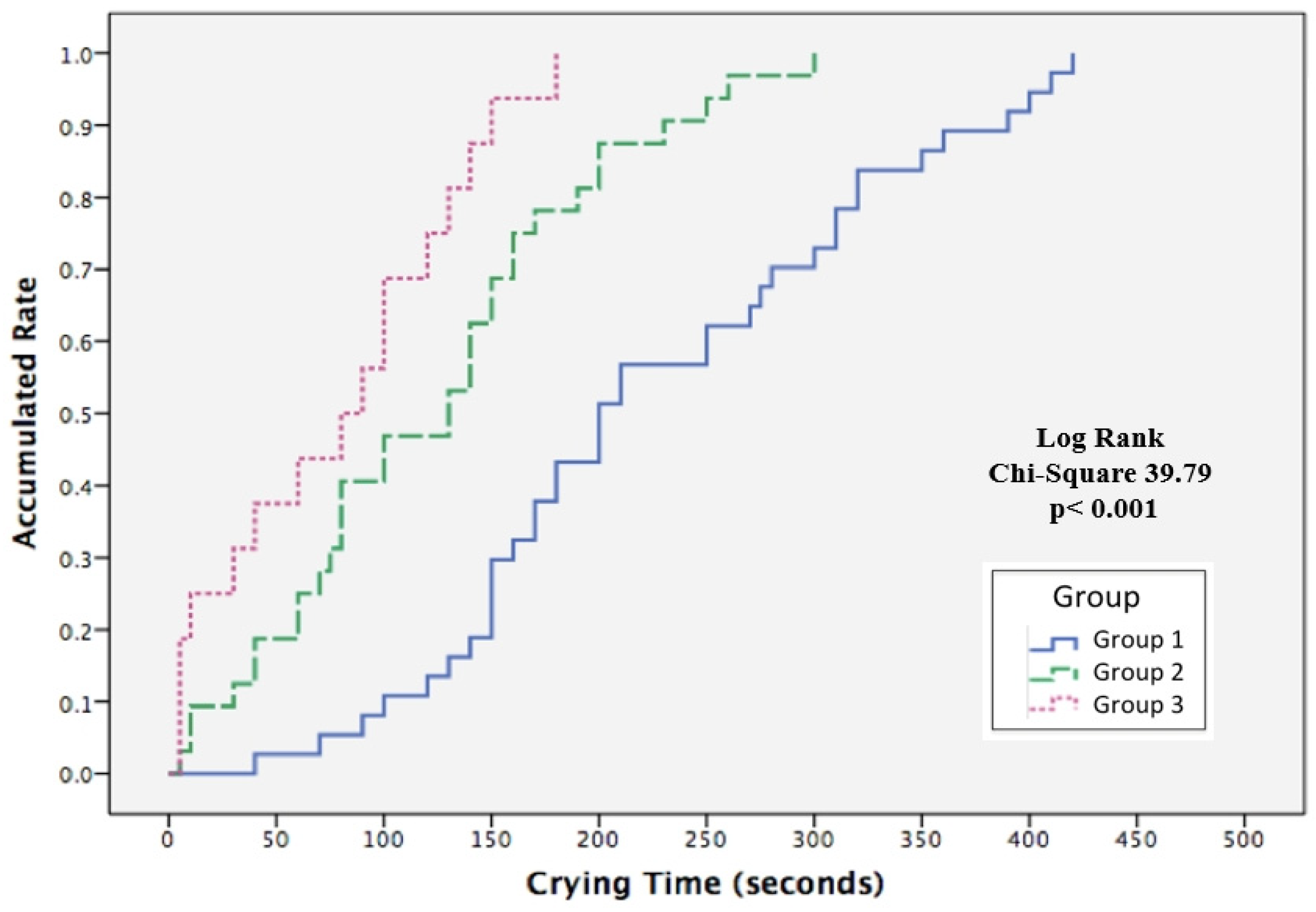
3.3. Time to Crying Cessation
4. Discussion
4.1. Clinical Implications
4.2. Strengths, Limitations, and Recommendations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Williams, M.D.; Lascelles, B.D.X. Early neonatal pain—A review of clinical and experimental implications on painful conditions later in life. Front. Pediatr. 2020, 8, 30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Friedrichsdorf, S.J.; Postier, A.; Eull, D.; Weidner, C.; Foster, L.; Gilbert, M.; Campbell, F. Pain outcomes in a US children’s hospital: A prospective cross-sectional survey. Hosp. Pediatr. 2015, 5, 18–26. [Google Scholar] [CrossRef] [Green Version]
- Postier, A.C.; Eull, D.; Schulz, C.; Fitzgerald, M.; Symalla, B.; Watson, D.; Friedrichsdorf, S.J. Pain experience in a US children’s hospital: A point prevalence survey undertaken after the implementation of a system-wide protocol to eliminate or decrease pain caused by needles. Hosp. Pediatr. 2018, 8, 515–523. [Google Scholar] [CrossRef] [Green Version]
- Walker, S.M. Long-term effects of neonatal pain. Semin. Fetal Neonatal Med. 2019, 24, 101005. [Google Scholar] [CrossRef]
- Zunino, C.; Notejane, M.; Bernadá, M.; Rodríguez, L.; Vanoli, N.; Rojas, M.; Mimbacas, I. Pain in children and adolescents hospitalized in a center of reference. Rev. Chil. Pediatr. 2018, 89, 67–73. [Google Scholar] [CrossRef] [PubMed]
- Lago, P.; Cavicchiolo, M.E.; Mion, T.; Dal Cengio, V.; Allegro, A.; Daverio, M.; Frigo, A.C. Repeating a dose of sucrose for heel prick procedure in preterms is not effective in reducing pain: A randomised controlled trial. Eur. J. Pediatr. 2020, 179, 293–301. [Google Scholar] [CrossRef]
- Hatfield, L.A.; Murphy, N.; Karp, K.; Polomano, R.C. A systematic review of behavioral and environmental interventions for procedural pain management in preterm infants. J. Pediatr. Nurs. 2019, 44, 22–30. [Google Scholar] [CrossRef] [PubMed]
- Eriksson, M.; Campbell-Yeo, M. Assessment of pain in newborn infants. Semin. Fetal Neonatal Med. 2019, 24, 101003. [Google Scholar] [CrossRef]
- Bellieni, C.V.; Johnston, C.C. Analgesia, nil or placebo to babies, in trials that test new analgesic treatments for procedural pain. Acta Paediatr. 2016, 105, 129–136. [Google Scholar] [CrossRef]
- Marchetti, G.; Vittori, A.; Tortora, V.; Bishop, M.; Lofino, G.; Pardi, V.; Picardo, S. Prevalence of pain in the departments of surgery and oncohematology of a paediatric hospital that has joined the project “Towards pain free hospital”. Clin. Ter. 2016, 167, 156–160. [Google Scholar] [CrossRef]
- Eccleston, C.; Fisher, E.; Howard, R.F.; Slater, R.; Forgeron, P.; Palermo, T.M.; Birnie, K.A.; Anderson, B.J.; Chambers, C.T.; Crombez, G.; et al. Delivering transformative action in paediatric pain: A lancet child & adolescent health commission. Lancet Child Adolesc. Health 2020, 5, 47–87. [Google Scholar] [CrossRef]
- Stadtlander, L. Understanding infant pain. Int. J. Childbirth Educ. 2018, 33, 6–8. [Google Scholar]
- Rad, Z.A.; Aziznejadroshan, P.; Amiri, A.S.; Ahangar, H.G.; Valizadehchari, Z. The effect of inhaling mother’s breast milk odor on the behavioral responses to pain caused by hepatitis B vaccine in preterm infants: A randomized clinical trial. BMC Pediatr. 2021, 21, 61. [Google Scholar] [CrossRef]
- Stevens, B.; Yamada, J.; Ohlsson, A.; Haliburton, S.; Shorkey, A. Sucrose for analgesia in newborn infants undergoing painful procedures. Cochrane Database Syst. Rev. 2016, 7, Cd001069. [Google Scholar] [CrossRef]
- Liaw, J.J.; Yang, L.; Wang, K.W.K.; Chen, C.M.; Chang, Y.C.; Yin, T. Non-nutritive sucking and facilitated tucking relieve preterm infant pain during heel-stick procedures: A prospective, randomised controlled crossover trial. Int. J. Nurs. Stud. 2012, 49, 300–309. [Google Scholar] [CrossRef] [PubMed]
- Ranjbar, A.; Bernstein, C.; Shariat, M.; Ranjbar, H. Comparison of facilitated tucking and oral dextrose in reducing the pain of heel stick in preterm infants: A randomized clinical trial. BMC Pediatr. 2020, 20, 2–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cirik, V.A.; Efe, E. The effect of expressed breast milk, swaddling and facilitated tucking methods in reducing the pain caused by orogastric tube insertion in preterm infants: A randomized controlled trial. Int. J. Nurs. Stud. 2020, 104, 103532. [Google Scholar] [CrossRef] [PubMed]
- Wu, H.P.; Yin, T.; Hsieh, K.H.; Lan, H.Y.; Feng, R.C.; Chang, Y.C.; Liaw, J.J. Integration of different sensory interventions from mother’s breast milk for preterm infant pain during peripheral venipuncture procedures: A prospective randomized controlled trial. J. Nurs. Sch. 2020, 52, 75–84. [Google Scholar] [CrossRef] [PubMed]
- Gao, H.; Xu, G.; Li, F.; Lv, H.; Rong, H.; Mi, Y.; Li, M. Effect of combined pharmacological, behavioral, and physical interventions for procedural pain on salivary cortisol and neurobehavioral development in preterm infants: A randomized controlled trial. Pain 2021, 162, 253–262. [Google Scholar] [CrossRef]
- World Health Organization. Breastfeeding. 2018. Available online: https://www.who.int/nutrition/topics/exclusive_breastfeeding/en/ (accessed on 20 July 2021).
- Maitre, N.L.; Key, A.P.; Slaughter, J.C.; Yoder, P.J.; Neel, M.L.; Richard, C.; Wallace, M.T.; Murray, M.M. Neonatal multisensory processing in preterm and term infants predicts sensory reactivity and internalizing tendencies in early childhood. Brain Topogr. 2020, 33, 586–599. [Google Scholar] [CrossRef]
- Bennett, A.J.; Hopkins, W.D.; Feldmann, T.; Gazzola, V.; Giedd, J.; Lamb, M.E.; Tottenham, N. Neural foundation of variability in attachment. In The Cultural Nature of Attachment and Contextualizing Relationships and Development; Keller, H., Bard, K.A., Eds.; MIT Press: Cambridge, MA, USA, 2017. [Google Scholar]
- Boix-Amorós, A.; Collado, M.C.; Van’t Land, B.; Calvert, A.; Le Doare, K.; Garssen, J.; Munblit, D. Reviewing the evidence on breast milk composition and immunological outcomes. Nutr. Rev. 2019, 77, 541–556. [Google Scholar] [CrossRef]
- Garwolińska, D.; Namieśnik, J.; Kot-Wasik, A.; Hewelt-Belka, W. Chemistry of human breast milk—A comprehensive review of the composition and role of milk metabolites in child development. J. Agric. Food Chem. 2018, 66, 11881–11896. [Google Scholar] [CrossRef]
- Grote, V.; Verduci, E.; Scaglioni, S.; Vecchi, F.; Contarini, G.; Giovannini, M.; Agostoni, C. Breast milk composition and infant nutrient intakes during the first 12 months of life. Eur. J. Clin. Nutr. 2016, 70, 250–256. [Google Scholar] [CrossRef] [Green Version]
- Baudesson de Chanville, A.; Brevaut-Malaty, V.; Garbi, A.; Tosello, B.; Baumstarck, K.; Gire, C.; Cozannet, R.L. Analgesic effect of maternal human milk odor on premature neonates: A randomized controlled trial. J. Hum. Lact. 2017, 33, 300–308. [Google Scholar] [CrossRef] [PubMed]
- Neshat, H.; Jebreili, M.; Seyyedrasouli, A.; Ghojazade, M.; Hosseini, M.B.; Hamishehkar, H. Effects of breast milk and vanilla odors on premature neonate’s heart rate and blood oxygen saturation during and after venipuncture. Pediatr. Neonatol. 2016, 57, 225–231. [Google Scholar] [CrossRef] [Green Version]
- Erkul, M.; Efe, E. Efficacy of breastfeeding on babies’ pain during vaccinations. Breastfeed. Med. 2017, 12, 110–115. [Google Scholar] [CrossRef] [PubMed]
- Locatelli, C.; Bellieni, C.V. Sensorial saturation and neonatal pain: A review. J. Matern. Fetal Neonatal Med. 2018, 31, 3209–3213. [Google Scholar] [CrossRef]
- Melzack, R.; Wall, P.D. Pain mechanisms: A new theory. Science 1965, 150, 971–979. [Google Scholar] [CrossRef]
- Kahraman, A.; Gümüş, M.; Akar, M.; Sipahi, M.; Yılmaz, H.B.; Başbakkal, Z. The effects of auditory interventions on pain and comfort in premature newborns in the neonatal intensive care unit; a randomised controlled trial. Intensive Crit. Care Nurs. 2020, 61, 102904. [Google Scholar] [CrossRef] [PubMed]
- Fitri, S.Y.R.; Lusmilasari, L.; Juffrie, M.; Bellieni, C.V. Modified sensory stimulation using breastmilk for reducing pain intensity in neonates in Indonesia: A randomized controlled trial. J. Pediatr. Nurs. 2020, 53, 199–203. [Google Scholar] [CrossRef] [PubMed]
- Küçük Alemdar, D.; Kardaş Özdemir, F. Effects of having preterm infants smell amniotic fluid, mother’s milk, and mother’s odor during heel stick procedure on pain, physiological parameters, and crying duration. Breastfeed. Med. 2017, 12, 297–304. [Google Scholar] [CrossRef] [PubMed]
- Mangat, A.K.; Oei, J.L.; Chen, K.; Quah-Smith, I.; Schmölzer, G.M. A review of non-pharmacological treatments for pain management in newborn infants. Children 2018, 5, 130. [Google Scholar] [CrossRef] [Green Version]
- Grant, S. The CONSORT-SPI 2018 extension: A new guideline for reporting social and psychological intervention trials. Addiction 2018, 114, 4–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sealed Envelope. Randomisation and Online Databases for Clinical Trials. 2017. Available online: https://www.sealedenvelope.com/simple-randomiser/v1/lists (accessed on 1 June 2017).
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.G. Statistical power analyses using G*Power 3.1: Tests for correlation and regression analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef] [Green Version]
- Yin, T.; Yang, L.; Lee, T.Y.; Li, C.C.; Hua, Y.M.; Liaw, J.J. Development of atraumatic heel-stick procedures by combined treatment with non-nutritive sucking, oral sucrose, and facilitated tucking: A randomised, controlled trial. Int. J. Nurs. Stud. 2015, 52, 1288–1299. [Google Scholar] [CrossRef]
- Ballinger, G.A. Using generalized estimating equations for longitudinal data analysis. Organ. Res. Methods 2004, 7, 127–150. [Google Scholar] [CrossRef]
- Bewick, V.; Cheek, L.; Ball, J. Statistics review 12: Survival analysis. Crit. Care 2004, 8, 389–394. [Google Scholar] [CrossRef] [Green Version]
- De Clifford-Faugere, G.; Lavallée, A.; Khadra, C.; Ballard, A.; Colson, S.; Aita, M. Systematic review and meta-analysis of olfactive stimulation interventions to manage procedural pain in preterm and full-term neonates. Int. J. Nurs. Stud. 2020, 110, 103697. [Google Scholar] [CrossRef]
- Zhang, S.; Su, F.; Li, J.; Chen, W. The analgesic effects of maternal milk odor on newborns: A meta-analysis. Breastfeed. Med. 2018, 13, 327–334. [Google Scholar] [CrossRef] [PubMed]
- Tasci, B.; Kuzlu Ayyildiz, T. The calming effect of maternal breast milk odor on term infant: A randomized controlled trial. Breastfeed. Med. 2020, 15, 724–730. [Google Scholar] [CrossRef]
- Bhurtel, R.; Yadav, U.; Chaudhary, R.; Shah, S.; Poudel, P.; Pokhrel, R.P.; Sharma, S. Effect of breastfeeding on relieving pain during immunization in infant. Kathmandu Univ. Med. J. 2020, 72, 376–380. [Google Scholar]
- Kumar, P.; Sharma, R.; Rathour, S.; Karol, S.; Karol, M. Effectiveness of various nonpharmacological analgesic methods in newborns. Clin. Exp. Pediatr. 2020, 63, 25. [Google Scholar] [CrossRef]
- Yilmaz, D.; Inal, S. Effects of three different methods used during heel lance procedures on pain level in term neonates. Jpn. J. Nurs. Sci. 2020, 17, e12338. [Google Scholar] [CrossRef]
- Bloomfield, F.H.; Alexander, T.; Muelbert, M.; Beker, F. Smell and taste in the preterm infant. Early Hum. Dev. 2017, 114, 31–34. [Google Scholar] [CrossRef] [Green Version]
- Zurita-Cruz, J.N.; Rivas-Ruiz, R.; Gordillo-Alvarez, V.; Villasis-Keever, M.Á. Breastfeeding for acute pain control on infants: A randomized controlled trial. Nutr. Hosp. 2017, 34, 301–307. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peng, H.F.; Yin, T.; Yang, L.; Wang, C.; Chang, Y.C.; Jeng, M.J.; Liaw, J.J. Non-nutritive sucking, oral breast milk, and facilitated tucking relieve preterm infant pain during heel-stick procedures: A prospective, randomized controlled trial. Int. J. Nurs. Stud. 2018, 77, 162–170. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Group 1 (CC) | Group 2 (CC+BMO) | Group 3 (CC+BMO+BMTSF) | p | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| (n = 38) | n = 38 | n = 38 | |||||||||||
| Mean | SD | n | % | Mean | SD | n | % | Mean | SD | n | % | ||
| Baseline Measures | |||||||||||||
| Gestational age (weeks) | 39.36 | 0.99 | 38.98 | 1.04 | 38.89 | 0.99 | 0.066 1 | ||||||
| Birth weight (g) | 3120.92 | 355.69 | 3105.39 | 385.47 | 3066.45 | 345.80 | 0.836 1 | ||||||
| Delivery type | 0.128 2 | ||||||||||||
| Normal spontaneous | 30 | 78.95 | 22 | 57.89 | 24 | 63.16 | |||||||
| Caesarean | 8 | 21.05 | 16 | 42.11 | 14 | 36.84 | |||||||
| Sex | 0.656 2 | ||||||||||||
| Male | 17 | 44.74 | 21 | 55.26 | 19 | 50.00 | |||||||
| Female | 21 | 55.26 | 17 | 44.74 | 19 | 50.00 | |||||||
| Apgar score: 1 min | 7.82 | 0.39 | 7.84 | 0.37 | 7.87 | 0.34 | 0.822 1 | ||||||
| Apgar score: 5 min | 9.00 | 0.00 | 8.97 | 0.16 | 8.97 | 0.16 | 0.604 1 | ||||||
| Times of painful experiences | 2.53 | 0.56 | 2.39 | 0.50 | 2.37 | 0.49 | 0.419 1 | ||||||
| Oxygen saturation (%) | 97.65 | 1.50 | 97.82 | 1.46 | 98.01 | 1.38 | 0.543 1 | ||||||
| Heart rate (bpm) | 124.27 | 12.79 | 120.99 | 9.34 | 123.70 | 12.14 | 0.596 1 | ||||||
| Heel-prick duration (s) | 163.68 | 71.08 | 160.53 | 68.60 | 145.66 | 63.08 | 0.468 1 | ||||||
| Variable | B | SE | Wald χ2 | p | 95% CI | |
|---|---|---|---|---|---|---|
| Lower | Upper | |||||
| Group Effects | ||||||
| Group 3 vs. Group 1 | −0.568 | 2.823 | 0.041 | 0.840 | −6.102 | 4.965 |
| Group 2 vs. Group 1 | −3.279 | 2.535 | 1.673 | 0.196 | −8.248 | 1.690 |
| Stage Effects | ||||||
| Stage 10 vs. Stage 0 | −1.084 | 3.445 | 0.099 | 0.753 | −7.837 | 5.669 |
| Stage 9 vs. Stage 0 | 4.732 | 3.854 | 1.507 | 0.220 | −2.822 | 12.285 |
| Stage 8 vs. Stage 0 | 6.468 | 4.350 | 2.211 | 0.137 | −2.058 | 14.995 |
| Stage 7 vs. Stage 0 | 13.784 | 4.531 | 9.256 | 0.002 | 4.904 | 22.664 |
| Stage 6 vs. Stage 0 | 23.284 | 4.325 | 28.987 | <0.001 | 14.808 | 31.761 |
| Stage 5 vs. Stage 0 | 42.258 | 3.849 | 120.557 | <0.001 | 34.715 | 49.801 |
| Stage 4 vs. Stage 0 | 43.758 | 3.157 | 192.061 | <0.001 | 37.569 | 49.946 |
| Stage 3 vs. Stage 0 | 40.416 | 3.292 | 150.740 | <0.001 | 33.964 | 46.868 |
| Stage 2 vs. Stage 0 | 32.126 | 3.028 | 112.592 | <0.001 | 26.192 | 38.060 |
| Stage 1 vs. Stage 0 | 23.389 | 2.640 | 78.510 | <0.001 | 18.216 | 28.563 |
| Interaction Effects | ||||||
| Group 2 × Stage | ||||||
| Group 2 × Stage 10 | −7.668 | 3.978 | 3.717 | 0.054 | −15.464 | 0.127 |
| Group 2 × Stage 9 | −13.037 | 4.2518 | 9.405 | 0.002 | −21.369 | −4.705 |
| Group 2 × Stage 8 | −14.932 | 4.836 | 9.534 | 0.002 | −24.409 | −5.454 |
| Group 2 × Stage 7 | −22.774 | 5.119 | 19.792 | <0.001 | −32.807 | −12.740 |
| Group 2 × Stage 6 | −21.695 | 5.108 | 18.041 | <0.001 | −31.706 | −11.684 |
| Group 2 × Stage 5 | −10.905 | 5.204 | 4.391 | 0.036 | −21.106 | −0.705 |
| Group 2 × Stage 4 | −7.379 | 4.837 | 2.327 | 0.127 | −16.859 | 2.101 |
| Group 2 × Stage 3 | −9.274 | 4.7261 | 3.850 | 0.050 | −18.537 | −0.011 |
| Group 2 × Stage 2 | −0.589 | 4.062 | 0.021 | 0.885 | −8.552 | 7.373 |
| Group 2 × Stage 1 | −2.853 | 3.370 | 0.716 | 0.397 | −9.458 | 3.753 |
| Group 3 × Stage | ||||||
| Group 3 × Stage 10 | −3.511 | 3.876 | 0.820 | 0.365 | −11.108 | 4.087 |
| Group 3 × Stage 9 | −8.063 | 4.128 | 3.816 | 0.051 | −16.153 | 0.027 |
| Group 3 × Stage 8 | −11.011 | 4.634 | 5.646 | 0.017 | −20.092 | −1.929 |
| Group 3 × Stage 7 | −19.800 | 4.909 | 16.268 | <0.001 | −29.422 | −10.178 |
| Group 3 × Stage 6 | −21.458 | 4.716 | 20.706 | <0.001 | −30.700 | −12.216 |
| Group 3 × Stage 5 | −24.300 | 4.843 | 25.178 | <0.001 | −33.792 | −14.808 |
| Group 3 × Stage 4 | −22.932 | 4.101 | 31.270 | <0.001 | −30.969 | −14.894 |
| Group 3 × Stage 3 | −18.142 | 4.146 | 19.149 | <0.001 | −26.268 | −10.016 |
| Group 3 × Stage 2 | −11.274 | 3.783 | 8.882 | 0.003 | −18.688 | −3.860 |
| Group 3 × Stage 1 | −5.721 | 3.544 | 2.606 | 0.106 | −12.667 | 1.225 |
| Variable | B | SE | Wald χ2 | p | 95% CI | |
|---|---|---|---|---|---|---|
| Lower | Upper | |||||
| Group Effects | ||||||
| Group 3 vs. Group 1 | 0.358 | 0.327 | 1.201 | 0.273 | −0.282 | 0.998 |
| Group 2 vs. Group 1 | 0.163 | 0.335 | 0.237 | 0.626 | −0.494 | 0.820 |
| Stage Effects | ||||||
| Stage 10 vs. Stage 0 | −0.942 | 0.437 | 4.638 | 0.031 | −1.799 | −0.085 |
| Stage 9 vs. Stage 0 | −0.942 | 0.474 | 3.957 | 0.047 | −1.870 | −0.014 |
| Stage 8 vs. Stage 0 | −1.311 | 0.580 | 5.112 | 0.024 | −2.447 | −0.174 |
| Stage 7 vs. Stage 0 | −1.916 | 0.688 | 7.749 | 0.005 | −3.265 | −0.567 |
| Stage 6 vs. Stage 0 | −2.179 | 0.463 | 22.186 | <0.001 | −3.086 | −1.272 |
| Stage 5 vs. Stage 0 | −7.968 | 0.870 | 83.917 | <0.001 | −9.673 | −6.264 |
| Stage 4 vs. Stage 0 | −7.363 | 0.797 | 85.260 | <0.001 | −8.926 | −5.800 |
| Stage 3 vs. Stage 0 | −6.916 | 0.896 | 59.519 | <0.001 | −8.673 | −5.159 |
| Stage 2 vs. Stage 0 | −5.153 | 0.738 | 48.778 | <0.001 | −6.599 | −3.707 |
| Stage 1 vs. Stage 0 | −2.205 | 0.538 | 16.799 | <0.001 | −3.260 | −1.151 |
| Interaction Effects | ||||||
| Group 2 × Stage | ||||||
| Group 2 × Stage 10 | 1.495 | 0.504 | 8.810 | 0.003 | 0.508 | 2.482 |
| Group 2 × Stage 9 | 1.363 | 0.517 | 6.965 | 0.008 | 0.351 | 2.376 |
| Group 2 × Stage 8 | 1.495 | 0.637 | 5.508 | 0.019 | 0.246 | 2.743 |
| Group 2 × Stage 7 | 2.074 | 0.734 | 7.982 | 0.005 | 0.635 | 3.512 |
| Group 2 × Stage 6 | 1.705 | 0.541 | 9.956 | 0.002 | 0.646 | 2.765 |
| Group 2 × Stage 5 | 4.363 | 1.0856 | 16.154 | <0.001 | 2.235 | 6.491 |
| Group 2 × Stage 4 | 3.153 | 1.0889 | 8.382 | 0.004 | 1.018 | 5.287 |
| Group 2 × Stage 3 | 2.626 | 1.1474 | 5.239 | 0.022 | 0.377 | 4.875 |
| Group 2 × Stage 2 | 1.021 | 1.0021 | 1.038 | 0.308 | −0.943 | 2.985 |
| Group 2 × Stage 1 | 0.363 | 0.6773 | 0.288 | 0.592 | −0.964 | 1.691 |
| Group 3 × Stage | ||||||
| Group 3 × Stage 10 | 1.511 | 0.470 | 10.323 | 0.001 | 0.589 | 2.432 |
| Group 3 × Stage 9 | 1.458 | 0.501 | 8.457 | 0.004 | 0.475 | 2.440 |
| Group 3 × Stage 8 | 1.774 | 0.601 | 8.714 | 0.003 | 0.596 | 2.951 |
| Group 3 × Stage 7 | 2.511 | 0.715 | 12.321 | <0.001 | 1.109 | 3.912 |
| Group 3 × Stage 6 | 2.484 | 0.498 | 24.850 | <0.001 | 1.507 | 3.461 |
| Group 3 × Stage 5 | 6.642 | 0.986 | 45.398 | <0.001 | 4.710 | 8.574 |
| Group 3 × Stage 4 | 5.616 | 0.948 | 35.124 | <0.001 | 3.759 | 7.473 |
| Group 3 × Stage 3 | 5.274 | 0.996 | 28.056 | <0.001 | 3.322 | 7.225 |
| Group 3 × Stage 2 | 3.405 | 0.868 | 15.409 | <0.001 | 1.705 | 5.105 |
| Group 3 × Stage 1 | 0.984 | 0.685 | 2.064 | 0.151 | −0.359 | 2.327 |
| Variable | B | SE | Wald χ2 | p | HR | 95% CI | |
|---|---|---|---|---|---|---|---|
| Lower | Upper | ||||||
| Group Effects | |||||||
| Group 2 vs. Group 1 | 1.104 | 0.276 | 15.982 | <0.001 | 3.016 | 1.755 | 5.182 |
| Group 3 vs. Group 1 | 1.866 | 0.355 | 27.689 | <0.001 | 6.466 | 3.226 | 12.958 |
| Infant Characteristics | |||||||
| Gestational age | −0.323 | 0.125 | 6.692 | 0.010 | 0.724 | 0.567 | 0.925 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, C.-H.; Liaw, J.-J.; Chen, Y.-T.; Yin, T.; Yang, L.; Lan, H.-Y. Efficacy of Breast Milk Olfactory and Gustatory Interventions on Neonates’ Biobehavioral Responses to Pain during Heel Prick Procedures. Int. J. Environ. Res. Public Health 2022, 19, 1240. https://doi.org/10.3390/ijerph19031240
Lin C-H, Liaw J-J, Chen Y-T, Yin T, Yang L, Lan H-Y. Efficacy of Breast Milk Olfactory and Gustatory Interventions on Neonates’ Biobehavioral Responses to Pain during Heel Prick Procedures. International Journal of Environmental Research and Public Health. 2022; 19(3):1240. https://doi.org/10.3390/ijerph19031240
Chicago/Turabian StyleLin, Chiao-Hsuan, Jen-Jiuan Liaw, Yu-Ting Chen, Ti Yin, Luke Yang, and Hsiang-Yun Lan. 2022. "Efficacy of Breast Milk Olfactory and Gustatory Interventions on Neonates’ Biobehavioral Responses to Pain during Heel Prick Procedures" International Journal of Environmental Research and Public Health 19, no. 3: 1240. https://doi.org/10.3390/ijerph19031240
APA StyleLin, C.-H., Liaw, J.-J., Chen, Y.-T., Yin, T., Yang, L., & Lan, H.-Y. (2022). Efficacy of Breast Milk Olfactory and Gustatory Interventions on Neonates’ Biobehavioral Responses to Pain during Heel Prick Procedures. International Journal of Environmental Research and Public Health, 19(3), 1240. https://doi.org/10.3390/ijerph19031240