
Experience of Rwanda on COVID-19 Case Management: From Uncertainties to the Era of Neutralizing Monoclonal Antibodies

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Objectives
- To document the evolution of COVID-19 case management interventions since the beginning of the pandemic;
- To highlight lessons learnt in COVID-19 case management and the way forward as we promote the culture of experience sharing across the world for mutual learning and support in this global fight against the COVID-19 pandemic.
3. Methods
3.1. Study Design and Source of Information
3.2. Variables’ Definition
3.2.1. Demographic Variables
3.2.2. Clinical Variables
3.2.3. Outcomes Variables
4. Results
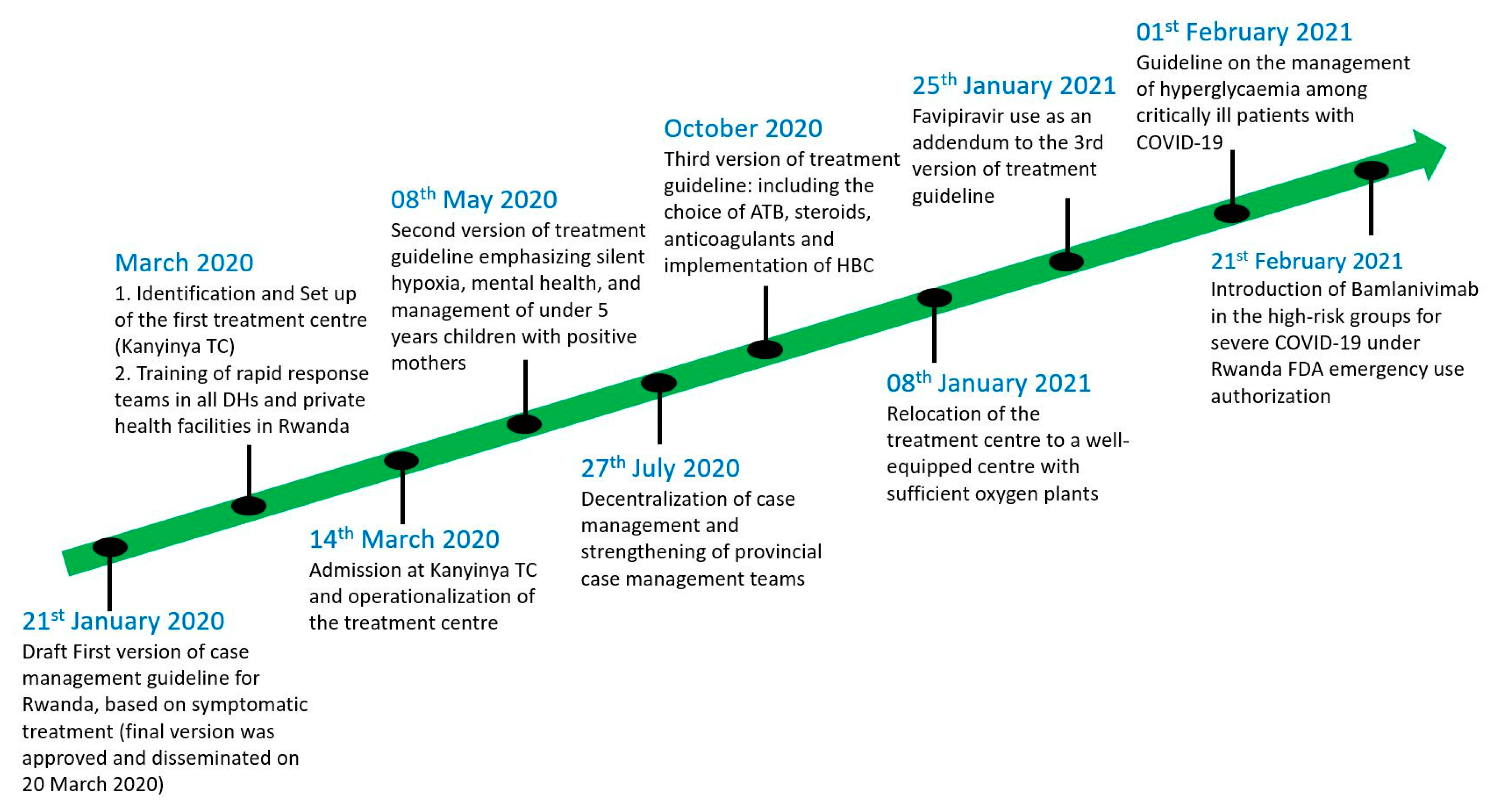
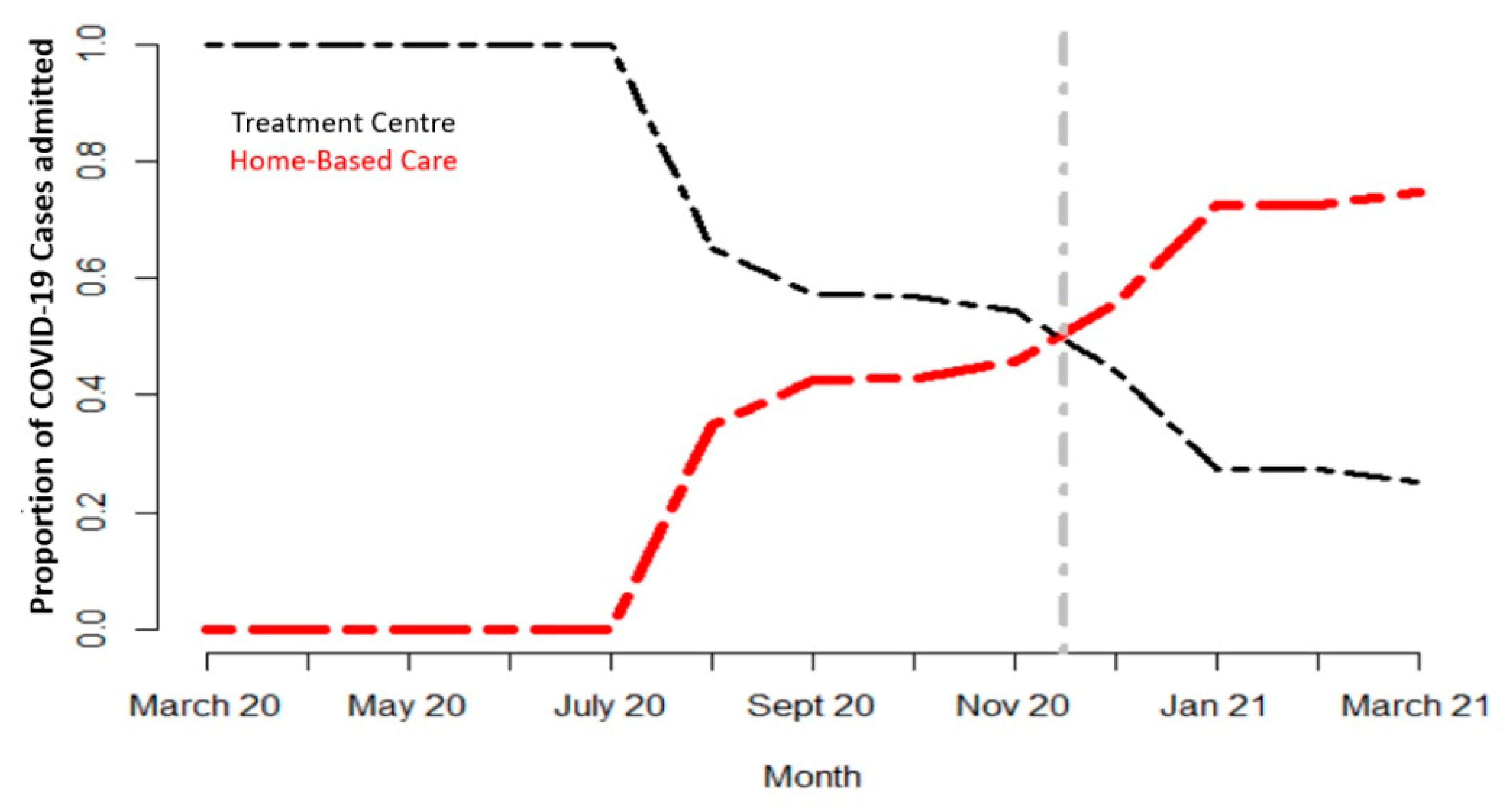
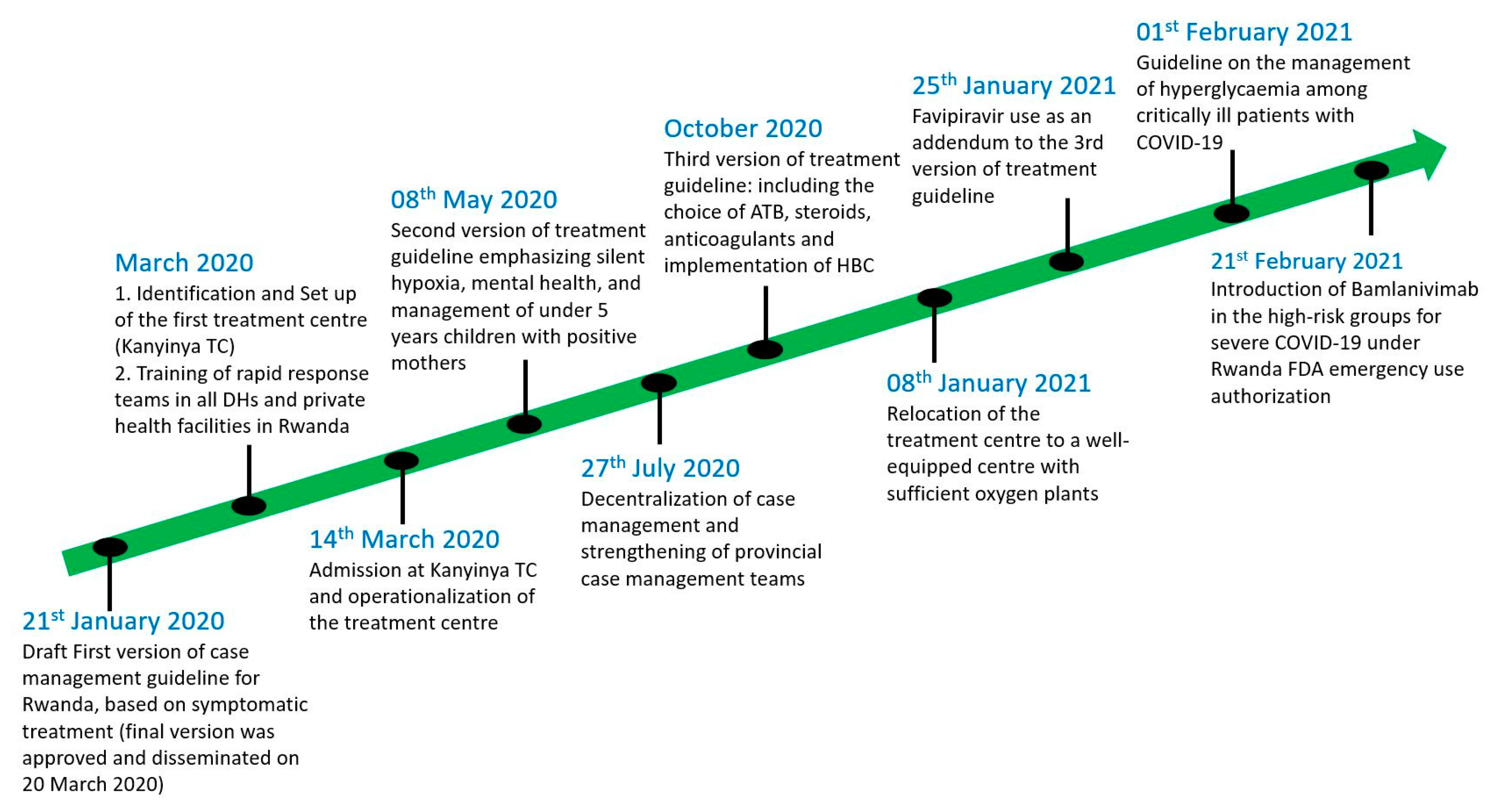
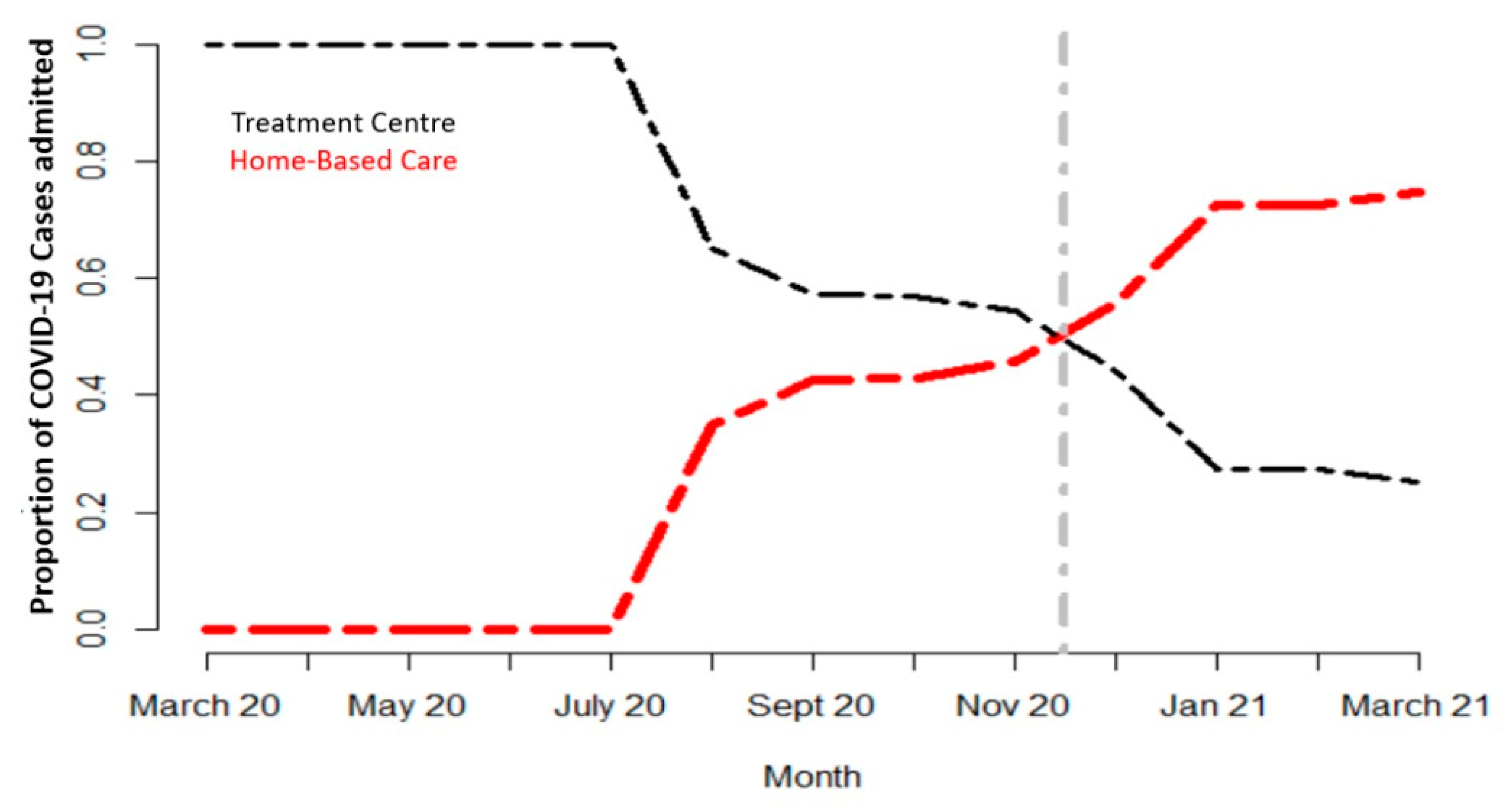
4.1. Set up of Quarantine, Isolation and Treatment Facilities for COVID-19 across the Country
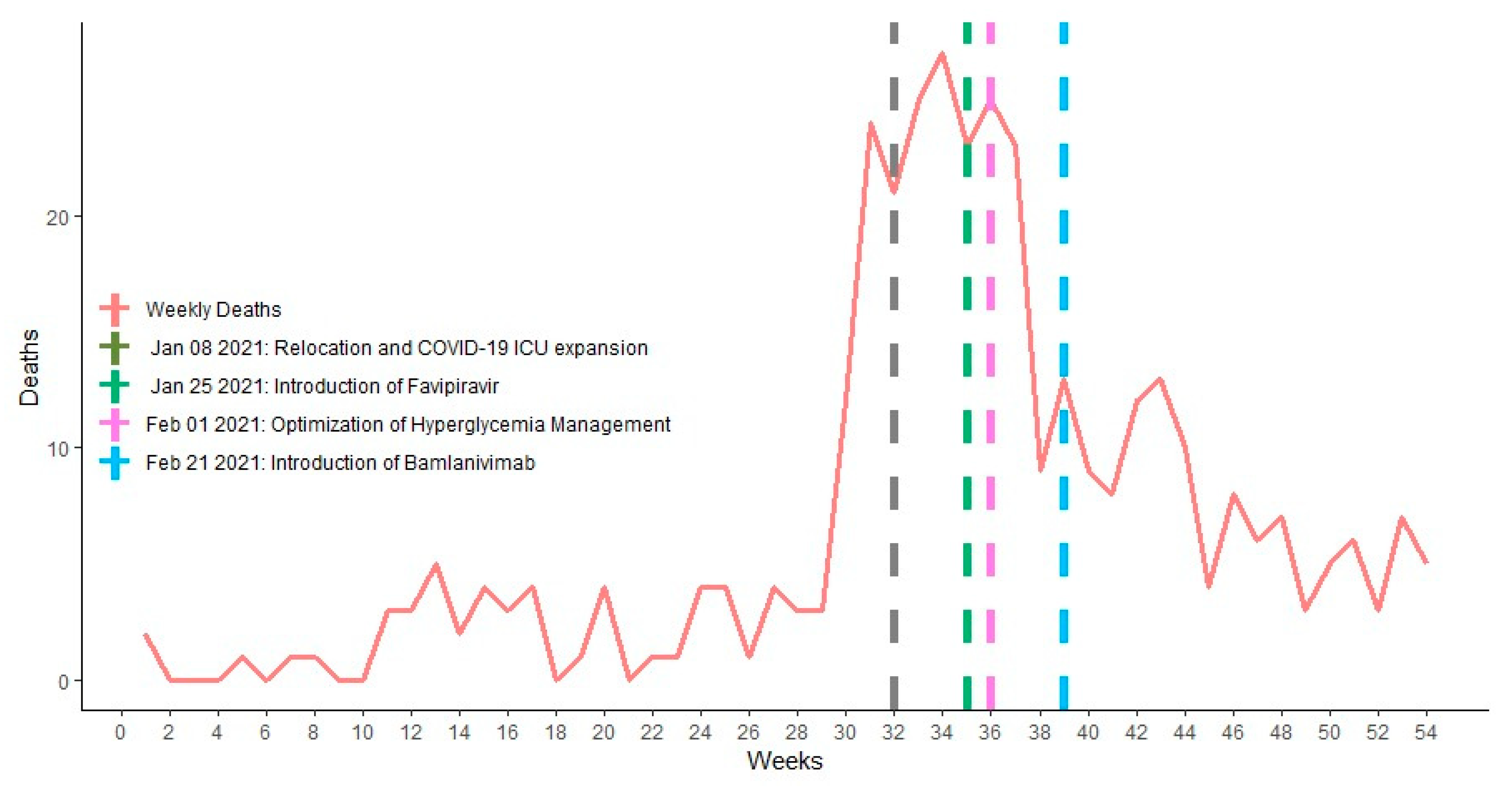
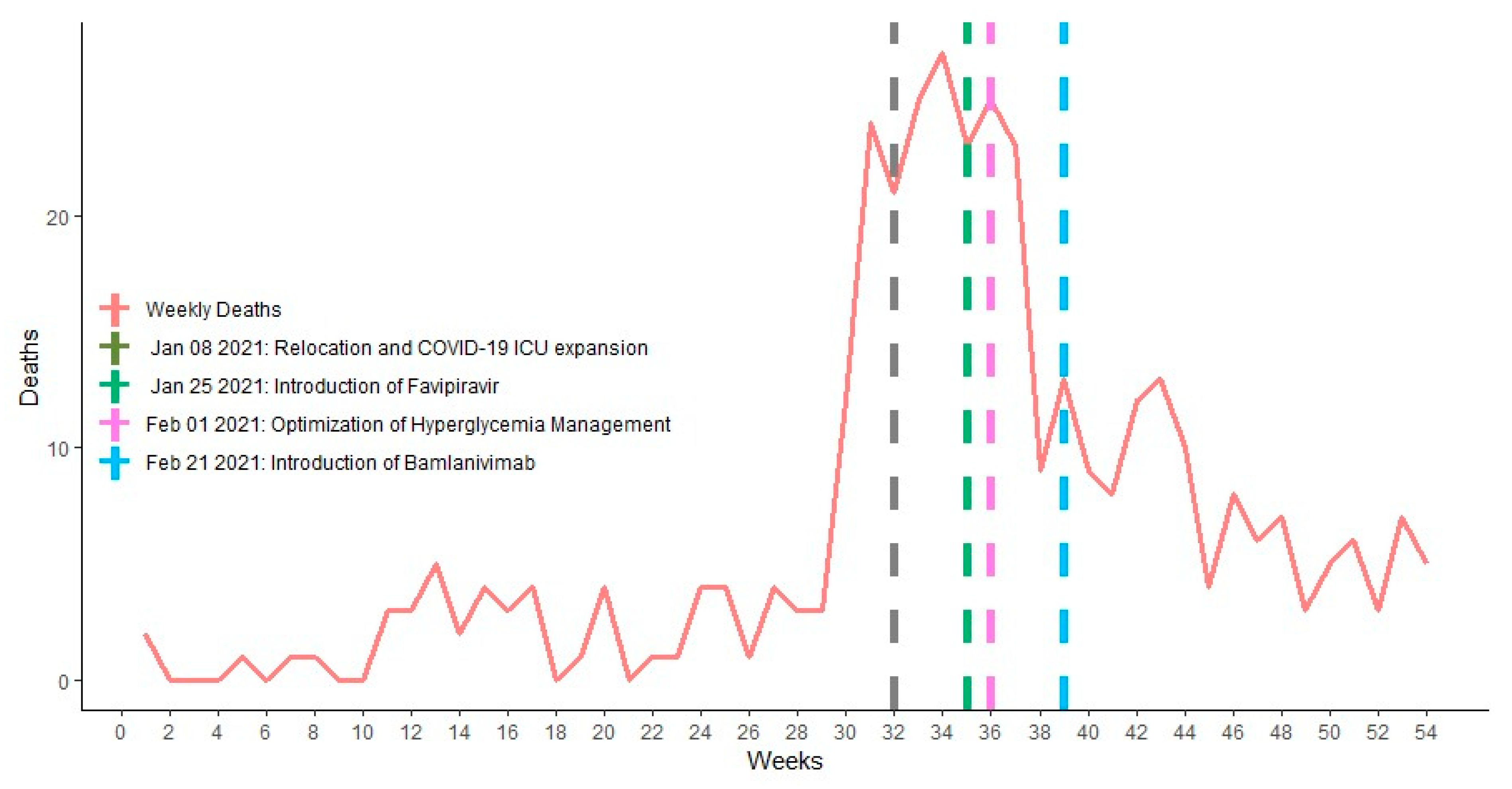
4.2. Faith in Science: The Basis of Evidence-Based Case Management in Rwanda
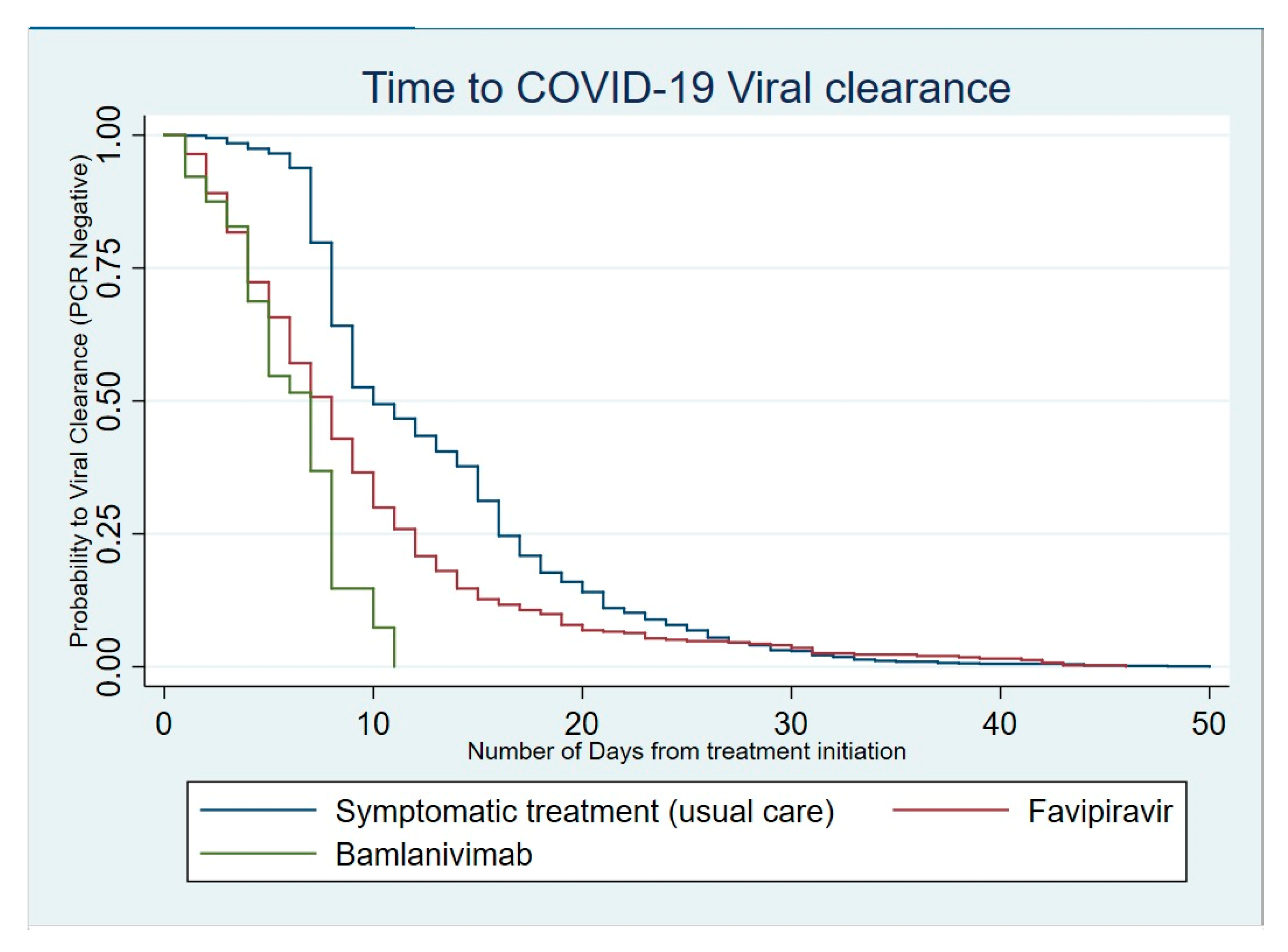
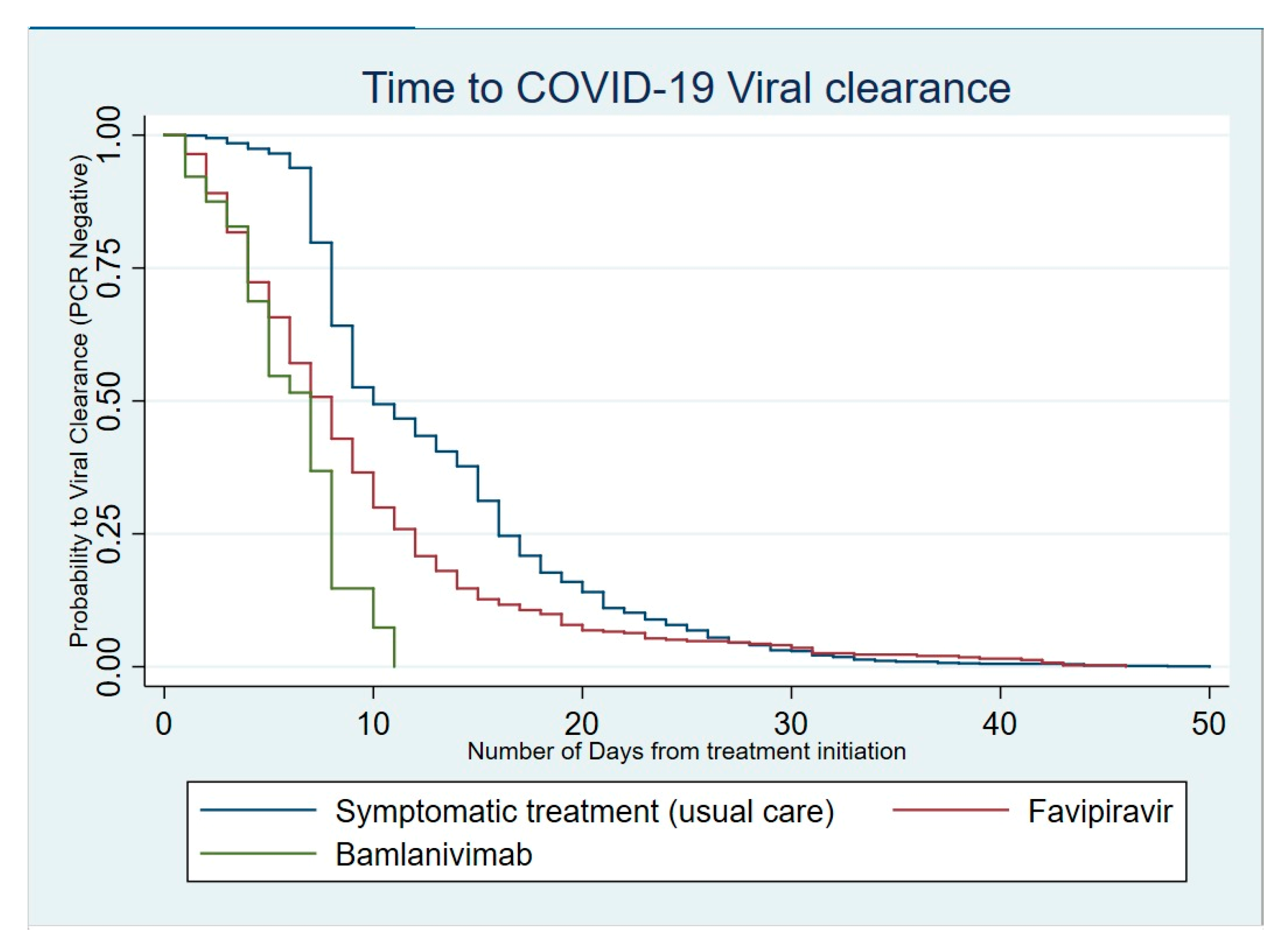
4.3. Impact of Therapeutic Strategies on the Duration of Virus Shedding
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cucinotta, D.; Vanelli, M. WHO Declares COVID-19 a Pandemic. Acta Biomed. 2020, 91, 157–160. [Google Scholar]
- Policy Responses to COVID19. IMF. Available online: https://www.imf.org/en/Topics/imf-and-covid19/Policy-Responses-to-COVID-19 (accessed on 9 June 2021).
- Severe Acute Respiratory Syndrome Coronavirus-2 (SARS-CoV-2). Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7182166/ (accessed on 9 June 2021).
- World Health Organization. Coronavirus (COVID-19) Events as They Happen. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/events-as-they-happen (accessed on 9 June 2021).
- Rwanda Biomedical Centre. Situation Report on COVID-19. Available online: https://www.rbc.gov.rw/index.php?id=717&L=0 (accessed on 9 June 2021).
- Interleukin-6 Receptor Antagonists in Critically Ill Patients with COVID-19 | NEJM. Available online: https://www.nejm.org/doi/full/10.1056/NEJMoa2100433 (accessed on 9 June 2021).
- The RECOVERY Collaborative Group. Dexamethasone in Hospitalized Patients with COVID-19. N. Engl. J. Med. 2021, 384, 693–704. [Google Scholar] [CrossRef] [PubMed]
- Information on COVID-19 Treatment, Prevention and Research. COVID-19 Treatment Guidelines. Available online: https://www.covid19treatmentguidelines.nih.gov/ (accessed on 9 June 2021).
- Therapeutic Management. COVID-19 Treatment Guidelines. Available online: https://www.covid19treatmentguidelines.nih.gov/therapeutic-management/ (accessed on 9 June 2021).
- WHO Applauds Rwanda’s Ebola Preparedness Efforts. Available online: https://www.who.int/news/item/24-07-2019-who-applauds-rwanda-s-ebola-preparedness-efforts (accessed on 9 June 2021).
- Rwanda Uses Ebola Experience to Combat COVID-19. Available online: https://www.aa.com.tr/en/africa/rwanda-uses-ebola-experience-to-combat-covid-19/1813902 (accessed on 9 June 2021).
- WHO COVID-19 Case Definition. Available online: https://www.who.int/publications-detail-redirect/WHO-2019-nCoV-Surveillance_Case_Definition-2020.2 (accessed on 9 June 2021).
- Rwanda Ministry of Health, Rwanda Biomedical Center. COVID-19 Clinical Guideline for Rwanda, 1st ed.; 2020. Available online: https://www.moh.gov.rw/fileadmin/user_upload/Moh/Publications/Guidelines_Protocols/Covid_-19_Clinical_Management_Guideline.pdf (accessed on 9 June 2021).
- Rwanda Ministry of Health, Rwanda Biomedical Center. COVID-19 Clinical Guideline for Rwanda, 2nd ed.; 2020. Available online: https://rbc.gov.rw/fileadmin/user_upload/annoucement/4th%20Clinical%20management%20guidelines%20COVID19.pdf?download=false (accessed on 9 June 2021).
- COVID-19 Clinical Management Guidelines. Available online: https://www.rbc.gov.rw/fileadmin/user_upload/guide/Guidelines/COVID-19%20Clinical%20Managment%20guidelines.pdf (accessed on 9 June 2021).
- Joshi, S.; Parkar, J.; Ansari, A.; Vora, A.; Talwar, D.; Tiwaskar, M.; Patil, S.; Barkate, H. Role of favipiravir in the treatment of COVID-19. Int. J. Infect. Dis. 2021, 102, 501–508. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. COVID-19 Clinical Management: Living Guidance; World Health Organization: Geneva, Switzerland, 2021; Available online: https://apps.who.int/iris/handle/10665/338882 (accessed on 25 January 2021).
- Clinical management of severe acute respiratory infection when novel coronavirus (nCoV) infection is suspected. WHO Interim guidance. Available online: https://apps.who.int/iris/bitstream/handle/10665/332299/WHO-2019-nCoV-Clinical-2020.1-eng.pdf (accessed on 10 June 2021).
- Barasa, E.; Kairu, A.; Ng’ang’a, W.; Maritim, M.; Were, V.; Akech, S.; Mwangangi, M. Examining unit costs for COVID-19 case management in Kenya. BMJ Global Health. BMJ Glob. Health 2021, 6, e004159. [Google Scholar] [CrossRef] [PubMed]
- Home Care for Patients with Suspected or Confirmed COVID-19 and Management of Their Contacts. WHO Interim Guidance. Available online: https://apps.who.int/iris/bitstream/handle/10665/333782/WHO-2019-nCoV-IPC-HomeCare-2020.4-eng.pdf (accessed on 10 June 2021).
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Driouich, J.-S.; Cochin, M.; Lingas, G.; Moureau, G.; Touret, F.; Petit, P.-R.; Piorkowski, G.; Barthélémy, K.; Laprie, C.; Coutard, B.; et al. Favipiravir antiviral efficacy against SARS-CoV-2 in a hamster model. Nat. Commun. 2021, 12, 1735. [Google Scholar] [CrossRef] [PubMed]
- Bosaeed, M.; Alharbi, A.; Hussein, M.; Abalkhail, M.; Sultana, K.; Musattat, A.; Alqahtani, H.; Alshamrani, M.; Mahmoud, E.; Alothman, A.; et al. Multicentre randomised double-blinded placebo-controlled trial of favipiravir in adults with mild COVID-19. BMJ Open 2021, 11, e047495. [Google Scholar] [CrossRef] [PubMed]
- Agrawal, U.; Raju, R.; Udwadia, Z.F. Favipiravir: A new and emerging antiviral option in COVID-19. Med. J. Armed. Forces India 2020, 76, 370–376. [Google Scholar] [CrossRef] [PubMed]
- Fact Sheet for Health Care Providers Emergency Use Authorization (EUA) of Bamlanivimab. Available online: https://www.fda.gov/media/143603/download (accessed on 15 February 2021).
- ACTIV-3/TICO LY-CoV555 Study Group; Lundgren, J.D.; Grund, B.; Barkauskas, C.E.; Holland, T.L.; Gottlieb, R.L.; Sandkovsky, U.; Brown, S.M.; Knowlton, K.U.; Self, W.H.; et al. A Neutralizing Monoclonal Antibody for Hospitalized Patients with COVID-19. N. Engl. J. Med. 2021, 384, 905–914. [Google Scholar] [PubMed]
- Gottlieb, R.L.; Nirula, A.; Chen, P.; Boscia, J.; Heller, B.; Morris, J.; Huhn, G.; Cardona, J.; Mocherla, B.; Stosor, V.; et al. Effect of Bamlanivimab as Monotherapy or in Combination with Etesevimab on Viral Load in Patients with Mild to Moderate COVID-19: A Randomized Clinical Trial. JAMA 2021, 325, 632–644. [Google Scholar] [CrossRef] [PubMed]
- Tjordan_Drupal. FDA Revokes Emergency Use Authorization for Monoclonal Antibody Bamlanivimab|AHA News. Available online: https://www.aha.org/news/headline/2021-04-19-fda-revokes-emergency-use-authorization-monoclonal-antibody-bamlanivimab (accessed on 11 June 2021).
- Taylor, P.C.; Adams, A.C.; Hufford, M.M.; de la Torre, I.; Winthrop, K.; Gottlieb, R.L. Neutralizing monoclonal antibodies for treatment of COVID-19. Nat. Rev. Immunol. 2021, 21, 382–393. [Google Scholar] [CrossRef] [PubMed]
- Evaluation of COVID-19 Vaccine Effectiveness. Available online: https://www.who.int/publications-detail-redirect/WHO-2019-nCoV-vaccine_effectiveness-measurement-2021.1 (accessed on 11 June 2021).
- Biccard, B.M.; Gopalan, P.D.; Miller, M.; Michell, W.L.; Thomson, D.; Ademuyiwa, A.; Aniteye, E.; Calligaro, G.; Chaibou, M.S.; Dhufera, H.T.; et al. Patient care and clinical outcomes for patients with COVID-19 infection admitted to African high-care or intensive care units (ACCCOS): A multicentre, prospective, observational cohort study. Lancet 2021, 397, 1885–1894. [Google Scholar] [CrossRef]
- Corti, D.; Purcell, L.A.; Snell, G.; Veesler, D. Tackling COVID-19 with neutralizing monoclonal antibodies. Cell 2021, 184, 3086–3108. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Mean of Length of Hospital Stay | Mortality Rate | Time to Viral Clearance Median (IQR) | HR | 95% CI | p-Value | |
|---|---|---|---|---|---|---|
| Treatment groups | ||||||
| Symptomatic treatment | 9.4 | 6 (6–10) | Ref | |||
| Favipiravir | 9.1 | 7 (4–11) | 1.97 | (1.74–2.23) | 0.000 | |
| Bamlanivimab | 5.4 | 3/67 (4.4%) | 6 (4–9) | 5.56 | (4.07–7.58) | 0.000 |
| Sex | ||||||
| Female | 10.0 | 6 (6–14) | Ref | |||
| Male | 9.0 | 6 (6–9) | 1.15 | (1.04–1.27) | 0.007 | |
| Age | 0.996 | (0.993–0.999) | 0.012 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nkeshimana, M.; Igiraneza, D.; Turatsinze, D.; Niyonsenga, O.; Abimana, D.; Iradukunda, C.; Bizimana, E.; Muragizi, J.; Mumporeze, L.; Lussungu, L.; et al. Experience of Rwanda on COVID-19 Case Management: From Uncertainties to the Era of Neutralizing Monoclonal Antibodies. Int. J. Environ. Res. Public Health 2022, 19, 1023. https://doi.org/10.3390/ijerph19031023
Nkeshimana M, Igiraneza D, Turatsinze D, Niyonsenga O, Abimana D, Iradukunda C, Bizimana E, Muragizi J, Mumporeze L, Lussungu L, et al. Experience of Rwanda on COVID-19 Case Management: From Uncertainties to the Era of Neutralizing Monoclonal Antibodies. International Journal of Environmental Research and Public Health. 2022; 19(3):1023. https://doi.org/10.3390/ijerph19031023
Chicago/Turabian StyleNkeshimana, Menelas, Deborah Igiraneza, David Turatsinze, Otto Niyonsenga, Deborah Abimana, Cyprien Iradukunda, Emmanuel Bizimana, Jean Muragizi, Lise Mumporeze, Laurent Lussungu, and et al. 2022. "Experience of Rwanda on COVID-19 Case Management: From Uncertainties to the Era of Neutralizing Monoclonal Antibodies" International Journal of Environmental Research and Public Health 19, no. 3: 1023. https://doi.org/10.3390/ijerph19031023
APA StyleNkeshimana, M., Igiraneza, D., Turatsinze, D., Niyonsenga, O., Abimana, D., Iradukunda, C., Bizimana, E., Muragizi, J., Mumporeze, L., Lussungu, L., Mugisha, H., Mgamb, E., Bigirimana, N., Rwagasore, E., Gatare, S., Mugabo, H., Nsekuye, O., Semakula, M., Sendegeya, A., ... Nsanzimana, S. (2022). Experience of Rwanda on COVID-19 Case Management: From Uncertainties to the Era of Neutralizing Monoclonal Antibodies. International Journal of Environmental Research and Public Health, 19(3), 1023. https://doi.org/10.3390/ijerph19031023