Abstract
Various studies have indicated that persons with special needs may face several barriers to dental treatment, which increases the prevalence of oral diseases in this population. Moreover, these studies suggested that Saudis with special needs have a higher prevalence of oral diseases, such as dental caries and periodontal disease. The aim of this review is to synthesize evidence regarding the current status, trends in oral health behaviors, and oral health care utilization among these individuals, as well as to assess the quality of the literature. Furthermore, this review seeks to recommend directions for future research and oral health care policymaking. An electronic search was conducted using the following databases and registers: PubMed/Medline, Embase, ISI Web of Science, Scopus, ClinicalTrials.gov, and CENTRAL. Gray literature, which included conference proceedings and unpublished literature, was searched via the library services and Google/Google Scholar, and the quality of studies was assessed using the AXIS scale for cross-sectional studies. A total of 38 studies were included in this review, with the majority of the studies graded as ‘low’. Within the limitations of this study, it can be concluded that individuals with special needs have limited access to oral health care, poor oral health status, and a general lack of awareness in regard to oral health. Therefore, nationwide surveys should be carried out to ascertain the actual extent of the oral inequities among individuals with special needs.
1. Introduction
The contemporary concept of disability is that individuals with disabilities are differently abled persons who have a different capacity to perform functions [1]. Disability can be apparent, such as physical and sensory, or intellectual and cognitive. It usually affects a person’s movement, vision, thinking, hearing, learning, speech, communication, memorizing, and social interactions [2,3]. The World Health Organization (WHO) and World Bank 2011 reports have stated that 15% of the global population is living with some form of disability, of which a majority (80%) belongs to the developing world [4]. It has been indicated that persons with special needs may face several barriers to dental treatment, which increases the prevalence of oral diseases in this population [5]. Individuals with special needs have poor oral health and face oral inequity more frequently than those without disabilities [6]. Additionally, developmental disorders, such as Down syndrome, may alter immune responses, making the individual more susceptible to periodontal disease and peri-implantitis [7]. Efforts have been made internationally to educate and train dentists to treat individuals with special needs [8]. In Saudi Arabia, it has been estimated that 2.9% of the total population have an extreme form of disability [9]. Moreover, studies suggest that Saudis with special needs have a higher prevalence of oral disease, such as dental caries and periodontal disease [10].
Several barriers to the oral health care of individuals with special needs have been identified, including distance, lack of trained specialists, lack of awareness or education of the caregivers, and costs of the treatment [11,12,13,14,15]. Patients with intellectual disabilities may underestimate the importance of oral health care and may not know how to access oral health care opportunities. Moreover, the dental treatment of individuals with special needs may take longer and may require additional personnel and sedation or anesthesia modalities. Over the last few years, several studies and reviews have been published on the oral health of Saudis without disabilities [16,17]. However, to date, no systematic review has been published that summarizes the status of oral health, oral health behaviors, and oral health care utilization among persons with disabilities in the Saudi population. Therefore, this review aims to synthesize evidence regarding the current status, trends in oral health behaviors, and oral health care utilization among these individuals, as well as to assess the quality of the literature. Furthermore, this review aims to recommend directions for future research and oral health care policymaking.
2. Materials and Methods
2.1. Focused Question
Utilizing the Participants, Intervention, Control, and Outcomes (PICO) principal as defined in the Preferred Reporting Items in Systematic Reviews and Meta-analysis (PRISMA), the following focused question was constructed: ‘What is the oral health status, oral health behaviors, and oral health care utilization among persons with disabilities, and is it similar to those without disabilities in Saudi Arabia? Is the status of oral health, oral health behaviors, and oral health care utilization among persons with disabilities similar to those without disabilities in Saudi Arabia?’
2.2. Eligibility Criteria and Literature Search
An electronic search was conducted on the following databases and registers: PubMed/Medline, Embase, ISI Web of Science, Scopus, ClinicalTrials.gov, and CENTRAL. Gray literature, which included conference proceedings and unpublished literature, was searched via the library services and Google/Google Scholar. All clinical studies focused on the oral health status and/or self-reported oral hygiene practices (tooth brushing, flossing, fluoride use, smoking, and sugar consumption) and/or studies that assessed oral health care utilization by evaluating the dental attendance status and barriers encountered while accessing dental care services. Exclusion criteria for the study were non-English letters to the editors, commentaries, and studies (MeSH keywords are provided in Supplementary File S1). Moreover, the reference lists of the included articles were searched for additional studies. Two investigators independently conducted the literature search and any disagreements were resolved through discussion. Furthermore, we calculated the inter-examiner reliability (Kappa) score.
2.3. Data Extraction
The data from each included study were extracted using pre-calibrated data forms by two investigators independently using the Covidence platform. The data were validated by a subject matter expert. Briefly, in addition to the PICO information, the following data were extracted: study author and year, gender, intervention/observed groups, target population and the actual included population, the type and number of centers in which the samples were studied, the assessed variables, and the overall outcomes (qualitative and/or quantitative). The data from the forms were extracted into Microsoft Excel prior to validation. A qualitative meta-analysis was not feasible due to the heterogeneity of the studies.
2.4. Quality Assessment
The quality of the studies was determined by using the critical appraisal tool to assess the quality of cross-sectional studies (AXIS) [18]. Briefly, various aspects of introduction, methodology, results, discussion and other sections of studies were assessed. Any disagreements were solved by discussion.
3. Results of the Literature Search
The initial literature search resulted in 1657 items. After the removal of 1200 items, the titles and abstracts of 457 articles were read to determine eligibility. Ultimately, the full texts of 53 research articles were downloaded for potential inclusion. Of these, 15 articles were excluded and are listed in Supplementary Table S1, along with the reasons for their exclusion (Supplementary Table S1). Therefore, 38 studies were included in this review [10,11,12,13,14,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51]. No additional studies were found upon hand searching or searching the gray literature. The inter-examiner reliability (Kappa) score was calculated as 0.89. The literature search process is presented in Figure 1.
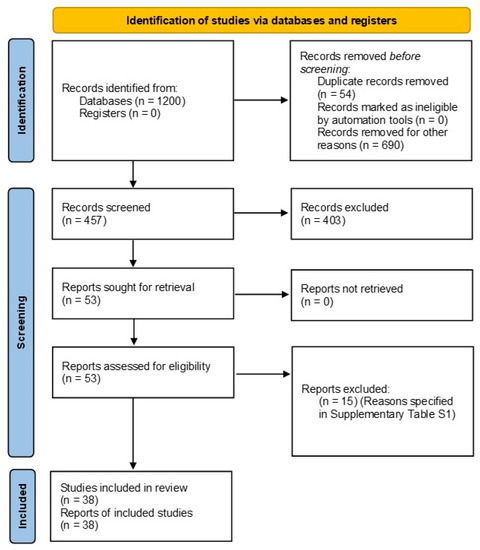
Figure 1.
Prisma flow diagram of the search methodology employed for this review.
4. General Characteristics of Studies
Thirty-five studies were cross-sectional [10,11,12,13,14,19,20,21,22,23,24,25,26,27,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,46,47,48,50,51], one was a longitudinal study [45], and two were retrospective studies [28,49]. Twenty-two studies were conducted in or near Riyadh [10,11,13,14,19,20,21,22,23,24,26,27,28,29,32,33,34,35,38,46,49,51]. Populations with special needs in the following cities were also studied: Al-Hofuf [11], Makkah [25], Khobar [30,50], Dammam [12,30,34], Qatif [30,39,44], AlMadinah Munawwarah [31], the Abha/Albaha province [34,36], Jeddah [37], Taif [40,42], Al-Kharj [41,45], the Aseer region [43], Makkah [47], Al-Qassim [48], Dhahran [50], Anak [50], Dareen [50], UmulSahik [50], and Al-Nabia [50]. In 13 studies, the target population was selected from multiple institutions or schools [10,12,13,20,21,26,27,30,33,39,43,44,46], while in the remaining studies the sample population was either from a single institution or the exact number was not stated. The sample sizes of included studies ranged between 23 and 819 participants [10,11,12,13,14,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50]. Overall, 942 participants with Down syndrome, 1070 with autism spectrum disorder, 564 with cerebral palsy, 466 with a visual impairment, 785 with a hearing and/or speech impairment, 656 with intellectual disabilities, 111 with learning disabilities, 30 with epilepsy, 221 that were medically compromised, and 128 with unclassified disabilities were included. Therefore, in this systematic review, data from 4441 individuals with special needs were included [10,11,12,13,14,15,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50]. The ages of the included participants ranged between 3 and 60 years, with the majority of the studies focusing on children with special needs. Four studies did not report the gender of the included participants [12,34,43,46], and in four other studies, no female participants were included [30,36,38,45]. The complete record of the general characteristics is provided in Table 1.

Table 1.
List of studies about oral health status, oral health behavior, and oral health care utilization.
5. Overall Outcomes of Studies
The most frequently measured oral health outcome was dental caries [12,14,24,25,29,30,31,32,35,36,37,38,41,42,43,45,46,47,48,49]. The included studies showed a high prevalence of dental caries in the majority of the population with special needs or disabilities. It was also observed that in the majority of individuals with special needs, there was a high prevalence of gingival and periodontal disease [28,29,35,39,41,43,50].
Three studies showed a significantly higher prevalence of gingival inflammation and dental caries in children with special needs (ASD, hearing impairment, and visual impairment) [28,29,30] and that children with visual impairment, hearing impairment, and cerebral palsy are more likely to experience dental trauma [20,33,40]. Moreover, there was a higher need for orthodontic treatment in patients with Down syndrome (66–81.9%) due to Class III malocclusions [19,22,23,43]. Children with intellectual disabilities had a higher prevalence of dental caries than children with blindness or deafness [24], and people with intellectual disabilities and cerebral palsy had a higher risk and prevalence of dental caries, compared to people with other physical or mental disabilities [25].
- -
- Oral health behavior:
Overall, there was a low frequency of tooth brushing (less than twice a day) and flossing among the participants [11,25,26,27,30,31,34,35,50]. When dietary habits were studied, sugar consumption was high and was associated with a high caries rate [12,25,27,42]. In one study, sugar consumption was low and this was associated with the overall positive parental attitude towards oral health [39]. One study showed that obesity may act as a co-factor in aggravating the dental caries prevalence in children with special needs [42]. In the studies included, there was variability in the brushing habits of persons with disabilities. Murshid et al. observed that up to 60% of participants with ASD could not brush their teeth by themselves [27] and 85.2% needed help during brushing [12]. Moreover, there were statistically significant differences between those with and without visual impairment in terms of tooth brushing (p = 0.043) [29], whilst two studies did not find significant differences in brushing habits among persons with and without disabilities [30,50]. In another study, nearly 50% of caregivers or parents helped their children with disabilities with brushing, but this did not have a statistically significant effect on periodontal disease or plaque accumulation. Plaque accumulation and gingival inflammation were significantly associated with reduced brushing practices (=0.004 and <0.0001, respectively) [39]. Ashour et al. observed that dental caries prevalence decreased with the use of fluoridated dentifrice [25].
Smoking and Substance Abuse
Only two studies explored the effect of smoking on the oral health of persons with disabilities [30,50], and one study found a significantly higher prevalence of periodontal disease in cigarette smokers [50]. No other type of substance abuse was studied.
- -
- Oral health care attendance and barriers:
A study showed that 26.3% of children with special needs have never visited a dentist [13], and the most prevalent reasons for this included: the inability or difficulty of the children to adjust to the environment of the dental clinic (43.4%), parents being too busy with providing medical care to their children (30.1%), and inaccessibility of dental clinics (26.5%). In another study, it was observed that 51.3% of individuals with disabilities had not seen a dentist for more than a year and 84.7% visited a dentist only for emergency treatment. Fear of the dentist was found to be the most common factor impeding dental care to persons with disabilities (52.1%), followed by cost (48.7%), inability to sit in the dental chair (28.2%), transportation issues (26.9%), distance (18.5%), and the lack of skill of the dentist (16.5%) [11]. In other studies, only 28.2% of children with ASD had visited the dentist and this was only in cases of an emergency [26,27]. Al-Qahtani et al. found that 40% of the included sample size of children with disabilities had never visited the dentist before [30]. Two studies also showed that almost half (46.6% to 49.2%) of the participants had never visited the dentist [12,35], and Alsheri et al. found that dental pain was the main reason for visiting a dental clinic [10]. Common barriers to dental care stated by caregivers included distance, transportation difficulties, unsuitable clinic environment care, medical issues, lack of medical insurance or coverage, previous bad experience at the dental clinic, and lack of time [44,51].
6. Results of the Quality Assessment
All studies included an adequate objective, justification of the study design, and justification of the results [10,11,12,13,14,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51]. Seven studies included a statistically calculated or a pre-determined sample size [19,20,21,24,29,35,40], nineteen studies adequately described the included target population [12,19,20,21,22,26,27,29,30,34,35,36,37,38,40,42,44,48,50], and thirty studies included an appropriate population base [10,11,13,14,19,20,21,22,23,24,26,27,29,30,31,33,34,35,36,37,38,39,40,41,42,44,45,46,47,48,49,50]. Non-responders were addressed in only two studies [29,37]. Outcomes were adequately measured in 35 studies [10,11,12,13,14,19,20,21,22,23,24,25,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50]. In 17 studies, the piloting or validation of the measurement instrument was carried out [10,11,13,14,21,22,23,24,27,28,30,32,34,35,37,39,40,42,44,45,46,47,48,49,50]. Statistical results were described adequately in 14 studies [12,25,26,27,29,30,34,35,36,37,39,40,42,44]. The basic data were described adequately in 32 studies [10,11,12,13,14,19,20,21,22,23,24,25,26,27,28,29,30,32,34,35,36,38,39,40,41,42,43,44,45,46,47,48,49,50]. The methodology to address the response rate was described in only four studies [15,26,29,41], and non-responder information was provided in only one study [15]. Outcomes were adequately reported in 33 studies [10,11,13,14,20,21,22,23,24,25,26,27,28,29,30,32,33,34,35,36,37,38,39,40,43,44,45,46,47,48,49,50]; in the discussion section, 37 studies justified the results adequately [10,11,12,13,14,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50] and limitations where identified in 16 studies [12,22,25,26,27,28,29,30,31,33,34,36,39,40,51]. Funding information was provided in 11 studies [12,22,29,30,33,36,37,39,40,41,48,51]. Funding or ethical information was provided in 23 studies [11,13,14,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,39,40,42,44]. Eighteen studies received a grading of ‘low’ [10,11,13,14,23,24,28,31,33,38,41,43,45,46,47,48,49,50], the same number of studies received an overall grade of ‘moderate’ [12,15,19,20,21,22,25,26,27,30,34,35,36,37,51], and three studies received a grade of ‘high’ [29,39,40]. The detailed results of the quality assessment are presented in Table 2.
Table 2.
Quality assessment.
7. Discussion
Children and young adults with disability and special education needs are known to have poorer oral health and greater unmet dental needs, compared to that of the general child population [52]. In addition to receiving high-quality clinical care, improving the oral health of people with disabilities necessitates that they have adequate access to dental care. Before recommending solutions, an awareness of the obstacles that people with disabilities face when trying to access dental treatment is required.
The government of Saudi Arabia has planned to modernize health care by 2030. The main aim of this agenda is to promote healthy lives. An action plan specifically for the aforementioned program is the “Health Sector Transformation Program” [53]. Its goal is to improve the accessibility of health care services to the entire population and deliver people-centered services by providing quality services along with disease prevention and promotion [54]. Therefore, the goal of this systematic review is to summarize and analyze the literature that has been published, focusing on oral health care (including the barriers, access, and utilization of oral health services) among people with special needs in Saudi Arabia. Additionally, this study also aims to describe the current oral health status of people with disabilities.
This study observed that the majority of research participants had poor oral hygiene practices and were dependent on caretakers to maintain proper oral hygiene and access oral health care services. As a result, caregiver training and education should be considered to support preventative approaches to oral disease [55]. Previous studies have indicated that training health care workers to treat individuals with special needs improves their ability to provide health care and may improve outcomes, when compared to those providers with no such training [56].
Over the last few decades, there have been significant advances in medical care for persons with special needs, leading to greater life expectancy. Therefore, oral health provisions for people with special needs need to be tailored and made accessible. Dental care is recognized as an integral component of the basic health requirements of children and adults with special needs [57]. Globally, one in every ten individuals live with disability, and the majority lack access to dental care [58]. Although disability in Saudi Arabia is a major concern, both socially and economically, there is very limited literature available to analyze the situation in detail [59].
Over the years, approximately 4–8% of Saudi Arabia’s population has become disabled, but only a small percentage receives proper health care services [44]. In Saudi Arabia, according to the General Authority for Statistics, 2.9% of the population is living with an extreme form of disability [9]. Therefore, there is a need a for comprehensive guidelines and policy to make dental care accessible for Saudis with special needs. Results from this review suggest that there are several gaps in the research that need to be overcome to achieve this goal. Arguably the biggest deficiency in the literature concerning dental care of the Saudi population with special needs, is the lack of national-level surveys assessing access to dental care, oral health status, and knowledge of caregivers [60,61]. This is indicated by more than two-thirds of studies being conducted in one city, Riyadh [10,11,13,14,15,19,20,21,22,23,24,25,26,27,28,32,33,35,38,46,49]. Participants from smaller cities and towns need to be studied to gauge a more representative view of the national situation. The lack of representation is shown by the majority of studies conducted in single institutions. Furthermore, the majority of the studies that did carry out multi-center surveys, did not include individuals with special needs from mainstream schools. Since special needs schools are more likely to provide an oral and systemic health care regimen personalized to the disabilities of the patient, the outcomes of the studies could have been influenced. Future studies should include both individuals with special needs living or studying in specialized institutes and those studying in mainstream schools.
An important observation made in this review are the barriers and difficulties faced by individuals with special needs in receiving dental care. Surveys in rural areas would reveal additional data regarding issues, such as distance and lack of dental clinics. Furthermore, more detailed studies should be conducted regarding the skills of general dental practitioners in treating individuals with special needs. We also recommend establishing continuing education or specialist programs that train dentists in special care dentistry. A glaring omission in the literature is a lack of studies focusing on adults with special needs, with only three studies [34,38,50] focusing on adults. With increasing age, psychomotor issues, lack of parental assistance, and poor oral hygiene, adults with special needs are expected to have a higher prevalence of periodontal disease and dental caries, which can add to the difficulties encountered by these individuals. Therefore, specialized dental programs aimed at adults with special needs should be initiated.
There are several recommendations that could be made to attempt to improve the oral health care of individuals with special needs in Saudi Arabia. Firstly, there needs to be specialized training programs in special care dentistry. Similar training for dental therapists, hygienists and assistants should be conducted. The oral health care for children with special needs should be accessible. One way to do this would be to create mobile dental hygiene services that can visit special needs centers. Oral health education programs need to be implemented in special needs centers and among children with special needs in mainstream schools. Dental outreach programs focusing on the population with special needs should be mandated among dental students. Doing so may not only make dental care accessible for patients but also familiarize future clinicians with providing dental care to these patients. Special care dentistry should be emphasized in the dental curriculum, dental offices and clinics should be designed appropriately to cater for people with special needs (focus on ramps and elevators for ease of access), and conscious sedation should be available and used where appropriate. To date, there has not been a guideline published in regard to the provision of general anesthesia or conscious sedation to patients with special needs and disabilities.
The included studies had several limitations. As shown in the quality assessment results, the majority of the studies were graded as ‘low’. The majority of the studies did not have a control group comparing the oral health issues of individuals with special needs to those without them. Furthermore, the majority of the studies failed to carry out randomization of the included sample size. Additionally, due to ethical reasons, it is difficult to blind patients, participants, or caregivers. Therefore, performing randomized controlled trials would be considered unethical, which adds a further limitation to future studies. The authors plan to conduct systematic reviews, focusing on oral health status in Saudi individuals with specific disabilities and special needs.
8. Conclusions
Within the limitations of this study, it can be concluded that individuals with special needs have limited access to oral health care, poor oral health status, and a general lack of awareness about oral health. Furthermore, the differences in the age and overall health of individuals with special needs make it difficult to present an overall assessment of oral health behaviors and oral health care utilization among persons with disabilities in Saudi Arabia. Standardized nationwide surveys should be carried out to ascertain the actual extent of the oral inequities among individuals with special needs.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/ijerph192416633/s1, Supplementary File S1: MeSH words. PRISMA checklist. Table S1. Excluded studies.
Author Contributions
Conceptualization, F.Y.I.A. and E.K.; methodology, F.Y.I.A. and E.K.; software and data extraction validation, E.K. and F.Y.I.A.; overall validation, M.T. and F.Y.I.A.; writing—original draft preparation, F.Y.I.A.; manuscript writing F.Y.I.A., M.T. and E.K.; writing—review and editing, M.T. and E.K.; supervision, M.T. and E.K.; project administration, M.T. and E.K.; All authors have read and agreed to the published version of the manuscript.
Funding
This work was supported by the Deanship of Scientific Research, Vice Presidency for Graduate Studies and Scientific Research, King Faisal University, Saudi Arabia [Grant No. 1039].
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Study data are available from the corresponding author on request.
Acknowledgments
The authors would like to acknowledge the University of Western Australia and the King Faisal University for their ongoing support.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Khayatzadeh-Mahani, A.; Wittevrongel, K.; Nicholas, D.B.; Zwicker, J.D. Prioritizing barriers and solutions to improve employment for persons with developmental disabilities. Disabil. Rehabilit. 2020, 42, 2696–2706. [Google Scholar] [CrossRef] [PubMed]
- Wilson, N.J.; Lin, Z.; Villarosa, A.; Lewis, P.; Philip, P.; Sumar, B.; George, A. Countering the poor oral health of people with intellectual and developmental disability: A scoping literature review. BMC Public Health 2019, 19, 1530. [Google Scholar] [CrossRef] [PubMed]
- Cougnard, A.; Goumilloux, R.; Monello, F.; Verdoux, H. Time between schizophrenia onset and first request for disability status in France and associated patient characteristics. Psychiatr. Serv. 2007, 58, 1427–1432. [Google Scholar] [CrossRef]
- Nations, U. Disability and Development Report. In Realizing the Sustainable Development Goals by, for and with Persons with Disabilities 2018; United Nations, Department of Economic and Social Affairs: New York, NY, USA, 2019. [Google Scholar]
- Lim, M.A.W.T.; Liberali, S.A.C.; Calache, H.; Parashos, P.; Borromeo, G.L. Perceived barriers encountered by oral health professionals in the Australian public dental system providing dental treatment to individuals with special needs. Spec. Care Dent. 2021, 41, 381–390. [Google Scholar] [CrossRef]
- Pradhan, A.; Slade, G.D.; Spencer, A.J. Access to dental care among adults with physical and intellectual disabilities: Residence factors. Aust. Dent. J. 2009, 54, 204–211. [Google Scholar] [CrossRef] [PubMed]
- Najeeb, S.; Khurshid, Z.; Siddiqui, F.; Zohaib, S.; Zafar, M.S. Outcomes of dental implant therapy in patients with down syndrome: A systematic review. J. Evid. Based Dent. Prac. 2017, 17, 317–323. [Google Scholar] [CrossRef] [PubMed]
- Dao, L.P.; Zwetchkenbaum, S.; Inglehart, M.R. General dentists and special needs patients: Does dental education matter? J. Dent. Educ. 2005, 69, 1107–1115. [Google Scholar] [CrossRef] [PubMed]
- General Authority for Statistics. 2.9% of Saudi Population Have Disability with (Extreme) Difficulty; General Authority for Statistics: Riyadh, Saudi Arabia, 2017. [Google Scholar]
- Alshehri, M.; Alghamdi, N.; Abdellatif, H. Assessment of oral health knowledge, status and awareness among visually impaired children in Saudi Arabia. J. Dent. Health Oral Disord. Ther. 2018, 9, 215–220. [Google Scholar]
- Al-Shehri, S.A.M. Access to dental care for persons with disabilities in Saudi Arabia (Caregivers’ perspective). J. Disabil. Oral Health 2012, 13, 51. [Google Scholar]
- Kotha, S.B.; AlFaraj, N.S.M.; Ramdan, T.H.; Alsalam, M.A.; Al Ameer, M.J.; Almuzin, Z.M. Associations between diet, dietary and oral hygiene habits with caries occurrence and severity in children with autism at Dammam City, Saudi Arabia. Open Access Maced. J. Med. Sci. 2018, 6, 1104. [Google Scholar] [CrossRef]
- Wyne, A.H. Attitude of parents of disabled children towards dental visits in Riyadh, Saudi Arabia. Odontostomatol. Trop. 2007, 30, 17–23. [Google Scholar] [PubMed]
- Alhammad, N.S.; Wyne, A.H. Caries experience and oral hygiene status of cerebral palsy children in Riyadh. Odontostomatol. Trop. 2010, 33, 5–9. [Google Scholar] [PubMed]
- Wyne, A.H.; Al-Hammad, N.S.; Splieth, C.H. Oral health comprehension in parents of Saudi cerebral palsy children. Saudi Dent. J. 2017, 29, 156–160. [Google Scholar] [CrossRef] [PubMed]
- Al-Ansari, A.A. Prevalence, severity, and secular trends of dental caries among various Saudi populations: A literature review. Saudi J. Med. Med. Sci. 2014, 2, 142. [Google Scholar] [CrossRef]
- Idrees, M.M.; Azzeghaiby, S.N.; Hammad, M.M.; Kujan, O.B. Prevalence and severity of plaque-induced gingivitis in a Saudi adult population. Saudi Med. J. 2014, 35, 1373. [Google Scholar]
- Downes, M.J.; Brennan, M.L.; Williams, H.C.; Dean, R.S. Development of a critical appraisal tool to assess the quality of cross-sectional studies (AXIS). BMJ Open 2016, 6, e011458. [Google Scholar] [CrossRef]
- Al-Sarheed, M.; Bedi, R.; Hunt, N.P. Orthodontic treatment need and self-perception of 11–16-year-old Saudi Arabian children with a sensory impairment attending special schools. J. Orthod. 2014, 30, 39–44. [Google Scholar] [CrossRef]
- AlSarheed, M.; Bedi, R.; Hunt, N.P. Traumatised permanent teeth in 11–16-year-old Saudi Arabian children with a sensory impairment attending special schools. Dent. Traumatol. 2003, 19, 123–125. [Google Scholar] [CrossRef]
- Al-Sarheed, M.; Bedi, R.; Hunt, N.P. The views and attitudes of parents of children with a sensory impairment towards orthodontic care. Eur. J. Orthod. 2004, 26, 87–91. [Google Scholar] [CrossRef][Green Version]
- Alkawari, H. Down Syndrome Children, Malocclusion Characteristics and the Need for Orthodontic Treatment Needs (IOTN): A Cross-Sectional Study. Children 2021, 8, 888. [Google Scholar] [CrossRef]
- Alkhadra, T. Characteristic of Malocclusion among Saudi Special Need Group Children. J. Contemp. Dent. Pract. 2017, 18, 959–963. [Google Scholar] [CrossRef]
- Al-Qahtani, Z.; Wyne, A.H. Caries experience and oral hygiene status of blind, deaf and mentally retarded female children in Riyadh, Saudi Arabia. Odontostomatol Trop. 2004, 27, 37–40. [Google Scholar] [PubMed]
- Ashour, N.A.; Ashour, A.A.; Basha, S. Association between body mass index and dental caries among special care female children in Makkah City. Ann. Saudi Med. 2018, 38, 28–35. [Google Scholar] [CrossRef]
- Murshid, E.Z. Parents’ dental knowledge and oral hygiene habits in Saudi children with autism spectrum disorder. Glob. J. Med. Res. 2014, 14, 11–18. [Google Scholar]
- Murshid, E.Z. Diet, oral hygiene practices and dental health in autistic children in Riyadh, Saudi Arabia. Oral Health Dent. Manag. 2014, 13, 91–96. [Google Scholar] [PubMed]
- Diab, H.M.; Motlaq, S.S.; Alsharare, A.; Alshammery, A.; Alshammery, N.; Khawja, S.G.; Shah, A.H. Comparison of gingival health and salivary parameters among autistic and non-autistic school children in Riyadh. J. Clin. Diagn. Res. 2016, 10, ZC110. [Google Scholar] [CrossRef]
- AlSadhan, S.A.; Al-Jobair, A.M.; Bafaqeeh, M.; Abusharifa, H.; Alagla, M. Dental and medical health status and oral health knowledge among visually impaired and sighted female schoolchildren in Riyadh: A comparative study. BMC Oral Health 2017, 17, 154. [Google Scholar] [CrossRef]
- Al-Qahtani, Y.; Al-Naser, H.; Al-Nahawi, D.; Al-Tuwaijri, F.; Al-Abdullati, M.; Al-Jewair, T. Dental caries prevalence and severity among deaf and hearing-impaired male students in Eastern Saudi Arabia. Adv. Dent. Oral Health 2017, 5, 1–6. [Google Scholar]
- Alhazmi, A.; Alshinqiti, I.; Aloufi, F.; Alhejali, A.; Alsulaimani, W.; Alharbi, M. Oral health knowledge, practice, oral hygiene status and dental caries prevalence among visually impaired student in Alnoor Institute of Almadinah Almunawwarah at Saudi Arabia. Int. J. Dent. Sci. Res. 2014, 2, 149–153. [Google Scholar] [CrossRef][Green Version]
- Wyne, A.H.; Al-Hammad, N.S.; Splieth, C.H. Dental caries and related risk factors in Saudi cerebral palsy children. Neurosci. J. 2017, 22, 282–286. [Google Scholar] [CrossRef]
- Al-Sehaibany, F.S. Occurrence of traumatic dental injuries among preschool children with Autism Spectrum Disorder. Pak. J. Med. Sci. 2018, 34, 859. [Google Scholar] [CrossRef] [PubMed]
- Mustafa, M.; Asiri, F.Y.I.; AlGhannam, S.; AlQarni, I.A.M.; AlAteeg, M.A.; Anil, S. Extent of awareness regarding oral health and dental treatment needs among individuals with hearing and speech impairments in Saudi Arabia. J. Int. Soc. Prev. Community Dent. 2018, 8, 70. [Google Scholar] [CrossRef] [PubMed]
- Alkahtani, F.H.; Baseer, M.A.; Ingle, N.A.; Assery, M.K.; Al Sanea, J.A.; AlSaffan, A.D.; Al-Shammery, A. Oral health status, treatment needs and oral health related quality of life among hearing impaired adults in Riyadh City, Saudi Arabia. J. Contemp. Dent. Pract. 2019, 20, 744. [Google Scholar]
- Alzahrani, A.A.H. Parent perspectives on perceived dental pain and dental caries in Saudi schoolchildren with intellectual disability. Spec. Care Dent. 2019, 39, 310–318. [Google Scholar] [CrossRef] [PubMed]
- Alaki, S.M.; Bakry, N.S. Dental pain in children with intellectual disabilities: Caregivers’ perspective. Int. J. Dent. 2012, 2012, 701608. [Google Scholar] [CrossRef][Green Version]
- Gufran, K.; Alqutaym, O.S.; Alqahtani, A.A.M.; Alqarni, A.M.; Hattan, E.A.E.; Alqahtani, R.O. Prevalence of dental caries and periodontal status among Down’s syndrome population in Riyadh City. J. Pharm. Bioallied Sci. 2019, 11, S252. [Google Scholar] [CrossRef] [PubMed]
- AlHumaid, J.; Gaffar, B.; AlYousef, Y.; Alshuraim, F.; Alhareky, M.; El Tantawi, M. Oral health of children with autism: The influence of parental attitudes and willingness in providing care. Sci. World J. 2020, 2020, 8329426. [Google Scholar] [CrossRef] [PubMed]
- Basha, S.; Mohamed, R.N.; Al-Thomali, Y.; Ashour, A.A.; Zahrani, F.S.A.; Almutair, N.E. Traumatic dental injuries in special health care needs children and association with obesity. Ann. Saudi Med. 2021, 41, 51–58. [Google Scholar] [CrossRef]
- Shah, A.; Bindayel, N.; AlOlaywi, F.; Sheehan, S.; AlQahtani, H.; AlShalwi, A. Oral health status of a group at a special needs centre in AlKharj, Saudi Arabia. J. Disabil. Oral Health 2015, 16, 79–85. [Google Scholar]
- Mohamed, R.; Basha, S.; Al-Thomali, Y.; AlZahrani, F.; Ashour, A.; Almutair, N. Association between dental caries and obesity among children with special health care needs. Oral Health Prev. Dent. 2021, 19, 101–106. [Google Scholar]
- Sandeepa, N.C.; Al Hagbani, S.A.; Alhammad, F.A.; Al Shahrani, A.S.; Al Asmari, S.E. Oral health status of Down’s syndrome patients in Aseer, Saudi Arabia. J. Pharm. Bioallied Sci. 2021, 13, S656. [Google Scholar] [CrossRef] [PubMed]
- Alfaraj, A.; Halawany, H.S.; Al-Hinai, M.T.; Al-Badr, A.H.; Alalshaikh, M.; Al-Khalifa, K.S. Barriers to Dental Care in Individuals with Special Healthcare Needs in Qatif, Saudi Arabia: A Caregiver’s Perspective. Patient Prefer. Adher. 2021, 15, 69. [Google Scholar] [CrossRef] [PubMed]
- Shah, A.H.; Wyne, A.H.; Asiri, F.Y.; Gulzar, S.; Sheehan, S.A.; Alghmlas, A.S.; Alomari, O.; AlJameel, A.H. Effectiveness of Preventive Oral Health Measures among Special Care School Children (boys) in Al-Kharj, Saudi Arabia. J. Clin. Diagn. Res. 2020, 14, ZC36–ZC40. [Google Scholar] [CrossRef]
- Al-damri, H.; Al-humaid, R.; Al-shehri, S.; Al-otaibi, S.; Abdulwahid, A. A comparison of DMF index and oral hygiene index between Downs syndrome subjects and a control group in Riyadh. Oral Health Care 2017, 2, 1–3. [Google Scholar] [CrossRef]
- Alzughaibi, O.S.; Filimban, L.A.; Arafa, A.A. Assessment of Salivary Immunoglobulin A, α-amylase, pH and Flow-rate Effects on Dental Caries Experience of Down’s Syndrome Children in Makkah, Saudi Arabia. Int. J. Health Sci. Res. 2017, 143–149. [Google Scholar]
- Al-Otaibi, S.M.; Rizk, H.; Riyaz, M.A. Prevalence of dental caries, salivary streptococcus mutans, lactobacilli count, pH level and buffering capacity among children with down’s syndrome in al-qassim region, KSA. Int. J. Contemp. Med. Res. 2016, 3, 2793–2797. [Google Scholar]
- Brown, A. Caries prevalence and treatment needs of healthy and medically compromised children at a tertiary care institution in Saudi Arabia. East. Mediterr. Health J. 2009, 15, 378–386. [Google Scholar] [CrossRef]
- El Tantawi, M.; AlAgl, A. Disability and the impact of need for periodontal care on quality of life: A cross-sectional study. J. Int. Med. Res. 2017, 45, 1949–1960. [Google Scholar] [CrossRef]
- Alshihri, A.A.; Al-Askar, M.H.; Aldossary, M.S. Barriers to Professional Dental Care among Children with Autism Spectrum Disorder. J. Autism. Dev. Disord. 2021, 51, 2988–2994. [Google Scholar] [CrossRef]
- Carter, A.; Clarke, L.; Stevens, C. Dental health for children with special educational needs and disability. Paediatr. Child Health 2022, 32, 290–296. [Google Scholar] [CrossRef]
- Alharbi, M.F. An analysis of the Saudi health-care system’s readiness to change in the context of the Saudi National Health-care Plan in Vision 2030. Int. J. Health Sci. 2018, 12, 83. [Google Scholar]
- Chowdhury, S.; Mok, D.; Leenen, L. Transformation of health care and the new model of care in Saudi Arabia: Kingdom’s Vision 2030. J. Med. Life 2021, 14, 347. [Google Scholar] [PubMed]
- Baskaradoss, J.K.; AlSumait, A.; Behbehani, E.; Qudeimat, M.A. Association between the caregivers’ oral health literacy and the oral health of children and youth with special health care needs. PLoS ONE 2022, 17, e0263153. [Google Scholar] [CrossRef] [PubMed]
- Mac Giolla Phadraig, C.; Guerin, S.; Nunn, J. Train the trainer? A randomized controlled trial of a multi-tiered oral health education programme in community-based residential services for adults with intellectual disability. Community Dent. Oral Epidemiol. 2013, 41, 182–192. [Google Scholar] [CrossRef] [PubMed]
- Federation, FDI World Dental. FDI/IADH policy statement on Oral health and dental care of people with disabilities: Adopted by the FDI General Assembly, September 2016, Poznan, Poland. Int. Dent. J. 2017, 67, 16–17. [Google Scholar] [CrossRef]
- Leal Rocha, L.; Vieira de Lima Saintrain, M.; Pimentel Gomes Fernandes Vieira-Meyer, A. Access to Dental Public Services by Disabled Persons. BMC Oral Health 2015, 15, 35. [Google Scholar] [CrossRef]
- Al-Jadid, M.S. Disability in Saudi Arabia. Saudi Med. J. 2013, 34, 453–460. [Google Scholar]
- Bindawas, S.M.; Vennu, V. The national and regional prevalence rates of disability, type, of disability and severity in Saudi Arabia—Analysis of 2016 demographic survey data. Int. J. Environ. Res. Public Health 2018, 15, 419. [Google Scholar] [CrossRef]
- Asma’a, A.F.; Alsalhani, A.B.; Idrees, M.M.; Alshehri, M.A.; Nassani, M.Z.; Kujan, O.B. Knowledge, attitudes, and practice behavior of dental hygienists regarding the impact of systemic diseases on oral health. Saudi Med. J. 2018, 39, 1139. [Google Scholar]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).