Abstract
Systemic lupus erythematosus (SLE) is a chronic and multi-systemic autoimmune disease, which has a deleterious impact on patients’ psychological well-being. This paper aims to review the existing literature on empirical research on psychological outcomes of SLE and psychological interventions to improve well-being in SLE patients. A search of significant English language articles was conducted in PubMed, Medline, ScienceDirect, Scopus, and ResearchGate databases. Titles and abstracts were screened for the relevant terms, including “systemic lupus erythematosus”, “childhood-onset systemic lupus erythematosus”, “juvenile systemic lupus erythematosus”, “lupus nephritis”, and their respective synonyms along with “depression”, “anxiety”, “fatigue”, “medical adherence”, “health-related quality of life”, “self-management” or “intervention”. The articles were evaluated by independent reviewers and the lists of eligible publications were compared whilst disagreements were settled by discussion. Of the 59 publications sought for retrieval, 35 papers were shortlisted based on predefined inclusion/exclusion criteria. They were classified according to their content and the methodology applied. Research topics including “anxiety and depression in SLE” and “self-management interventions for SLE patients” were identified and are presented in this review. As the prognosis and life expectancy of SLE patients are improving, further research on the psychological outcomes of SLE and the evidence-based psychological interventions to improve patients’ well-being are justified.
1. Introduction
Systemic lupus erythematosus (SLE) is a connective tissue disease of unknown origin and multi-organ clinical presentation and unpredictable course [1]. SLE is a disease distributed worldwide, which occurs in both genders, and all racial/ethnic and age groups. However, higher rates are observed in adults, females, and non-Caucasians [2]. Genetic, environmental, and sociodemographic factors are responsible for the variable course and outcome of the disease [3]. SLE includes many symptoms, such as cutaneous, haematological, and renal disease. Clinical heterogeneity and unpredictable course and flares are characteristics of SLE [1,2,3,4,5,6].
One of the major problems in SLE patients is neuropsychiatric disease, which has one of the heaviest weights in the measurement of SLE disease activity [7]. The prevalence of neuropsychiatric systemic lupus erythematosus (NPSLE) is estimated to be between 37 and 95% [8]. NPSLE refers to a series of neurological and psychiatric symptoms directly related to SLE. Neuropsychiatric disease includes heterogeneous manifestations involving both the central and peripheral nervous systems [7]. Although in 1999 the American College of Rheumatology (ACR) proposed a set of definitions for the neuropsychiatric involvement in SLE with the intention of homogenizing the terminology, the unequivocal diagnosis remains a challenge. This is due to the multiple neuropsychiatric disease presentations and the severity of symptoms [8].
Additionally, it seems that it is not only patients who meet the criteria for the diagnosis of NPSLE who present with a whole range of psychological symptoms [7]. Even lupus patients in remission often report residual symptoms, such as chronic pain (not only organic) and fatigue [9,10]. Similarly, even successfully treated SLE patients are also at a high risk for depression and anxiety [11]. A clinically significant problem is also decreased sleep quality in this group of patients [12]. All of these symptoms are difficult to clearly diagnose and rank in order but can significantly affect the quality of life of patients with SLE [13].
Therefore, psychological symptoms represent a challenge for the treating physician in terms of diagnosis and treatment. Targeted symptomatic therapy is indicated according to the type of neuropsychiatric manifestations (e.g., antipsychotics for psychosis and anxiolytics for anxiety disorder) [14,15]. However, comprehensive care requires not only pharmacological therapy. Therefore, the role of the psychologist, as a therapist who coordinates psychological care, also appears important [16,17]. The goal of this paper is to review the current empirical research on the psychological outcomes of SLE and the efficacy of psychological interventions to improve well-being in SLE patients.
2. Methods
A scholarly literature search to identify English language peer-reviewed original publications on the psychological outcomes of SLE and the psychological interventions to improve well-being in SLE patients released between January 2007 and July 2022 was conducted across PubMed, Medline, ScienceDirect, Scopus, and ResearchGate databases. The review methodology was formally discussed and agreed upon within the research group. This review aimed to collect the evidence on the psychological impact of SLE and the efficacy of psychological interventions in SLE patients. Consequently, the goal to examine the psychological effects of lupus and the results of psychological interventions for lupus patients from the point of the diagnostic disclosure and then across the treatment trajectory was carefully addressed during the selection process. The search terms included both standardized medical subject headings and keywords, such as “systemic lupus erythematosus”, “SLE”, “childhood-onset systemic lupus erythematosus”, “cSLE”, “juvenile systemic lupus erythematosus”, “JSLE”, “lupus nephritis”, and “LN”, along with “depression”, “anxiety”, “fatigue”, “medical adherence”, “health-related quality of life”, “patient”, “self-management” or “intervention”, “psychotherapy”, “therapy”, “treatment”, “psychology”, cause”, ”factor”, “determinant”, and “variable”. The terms were intermingled with Boolean operators and the search queries were combined so that several potential search strategies could be developed to find the relevant results. Papers on the psychological outcomes of SLE were included if they presented prospective, retrospective, longitudinal, observational, or cross-sectional studies. Studies that were descriptive based on qualitative assessments or small sample size investigations without power of the test calculations were also included. Publications on the psychological interventions for lupus patients were included if they set forth single- or double-blinded and non-blinded randomized controlled trials. In turn, investigations exploring the psychological outcomes or the psychological interventions for autoimmune and rheumatologic diseases or autoimmune/rheumatologic disease patients involving a lupus subgroup were included if they highlighted the results for this subgroup. Meta-analyses, reviews, systematic reviews, scoping reviews, and “grey literature”, such as conference reports, commentaries, theses, and non-peer-reviewed publications were excluded from the review. In order to establish a more conclusive evidence of contemporary literature, citation information and published research profiles of key authors were screened for relevant publications. Three independently working researchers reviewed the titles and abstracts yielded by this comprehensive search and selected articles in accordance with the predefined inclusion and exclusion criteria. Subsequently, 65 potentially relevant articles were retrieved for further analysis. The unmasked lists of eligible publications were compared and any disagreement between reviewers was settled through a consensus discussion with a fourth reviewer. The reviewers assessed the full text of the articles retained after the title/abstract screening. Of the 59 articles initially identified through the database search and sought for retrieval, 35 papers that addressed the subject of the review and fulfilled the criteria of methodologically robust research were selected. The details of the screening process, including reasons for full-text exclusion, are delineated in Figure 1.
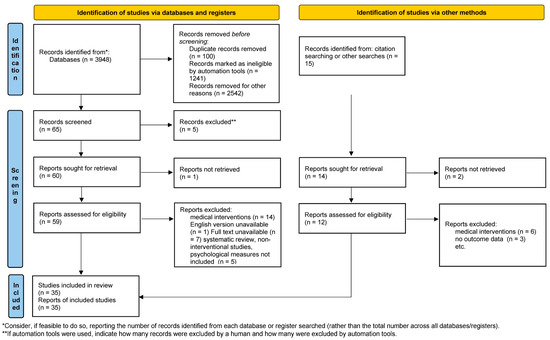
Figure 1.
PRISMA 2020 flow diagram for new systematic reviews which included searches of databases, registers and other sources. (PRISMA 2020 statement, https://www.prisma-statement.org// (accessed on 7 October 2022).
3. Results
The initial search yielded 65 articles after removing duplicate records and articles deemed ineligible. Fifty-nine of these articles were sought for retrieval whilst only 35 articles that complied with the inclusion criteria were included. Twenty-six studies focusing on the psychological outcomes of lupus involved 7302 subjects with lupus [18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43] while nine interventional studies involved 431 subjects with SLE [44,45,46,47,48,49,50,51,52]. Because of a diverse nature of retrieved investigations and the heterogeneity of data in terms of the type of intervention technique, research procedures, and outcome evaluation measures, a meta-analysis could not be performed. The papers were classified on the basis of their contents and methodology. The following research topics were identified and are presented in this review: (1) “Anxiety, depression and sleep quality”; (2) “Fatigue and pain”; (3) “Health-related quality of life (HRQOL) in SLE”; (4) “Improving HRQOL in SLE patients”; and (5) “Focusing on psychosocial adjustment to the disease”. The investigations of the psychological outcomes of SLE are presented in Table 1 while the overview of the interventional studies is demonstrated in Table 2.

Table 1.
Findings on the psychological outcomes of SLE in chronological order.
Table 2.
An overview of the interventional studies.
3.1. Anxiety, Depression and Sleep Quality
The prevalence of anxiety and depression and sleep quality in SLE was assessed in thirteen investigations in eight countries in Europe, Asia, and North America [18,19,21,22,26,27,30,34,35,38,40,42,43]. Most studies applied a cross-sectional design and used sample sizes ranging from 29 to 405 participants with an overwhelming majority (80–100%) of female participants. Studies applied a number of commonly used standardized questionnaires and tools including the Beck Depression Inventory (BDI) [19,38], the Hospital Anxiety and Depression Scale (HADS) [27,34,36,37,39,40], the Patient Health Questionnaire-9 [21], and the Hamilton Depression Rating Scale (HAMD) [18] to assess symptoms of depression and anxiety while the Pittsburgh Sleep Quality Index (K-PSQI) was used to assess sleep quality indicators [26,34,35,38]. Studies reported mixed findings as mild to severe depression was present in 15-68.7% of subjects [18,21,30]. One study, however, indicated the prevalence of depression in SLE subjects and in controls was similar [27]. According to another study, suicidal ideation could be found in as many as 14% of subjects with SLE. Suicidal ideation correlated with a younger age at diagnosis [21].
Depression was associated with anxiety, fatigue, pain intensity, symptoms of ill physical health, or medication side effects (e.g., an uptake of steroids, kidney function, or dizziness) [18,35], marital status, or ethnic background [19,21]. There were discordant findings on the relationship between depression, socioeconomic status, cognitive function, and disease activity in terms of SLEDAI scores [18,19,37,43]. A higher disease activity in terms of SLEDAI scores predicted depression [18,19,27].
An investigation on the psychological aftermath of the COVID-19 pandemic also revealed depression in SLE patients and was associated with compliance towards coronavirus prevention measures [42].
Anxiety seemed to be more common in older patients and strongly correlated with signs of the disease (e.g., alopecia, proteinuria, negative anti-P0 antibodies, poor kidney function, and fatigue) and depression [18]. Additionally, there was a positive association between anxiety and the duration of the disease (time since diagnostic disclosure) [43]. A longer duration of the disease was more anxiety-provoking only in individuals with SLE [43], but the association between the duration of the disease and anxiety in patients with JSLE could not be confirmed [21]. Furthermore, anxiety corresponded to a patient’s perception of SLE, which pertains to the patient’s perspective of and understanding of the illness (their knowledge, memories, thoughts, beliefs, and expectations about SLE) [38]. Interestingly, 19–57.4% of respondents reported anxiety whereas 57.1% complained of poor sleep [34,38]. Studies have found that poor quality of sleep in SLE patients are strongly correlated with symptoms of depression and anxiety and are predicted by older age [34,38].
3.2. Fatigue and Pain
Fatigue and pain in SLE were evaluated in twelve investigations carried out in eight countries in Europe, Asia, and North America [19,22,23,26,27,30,36,38,39]. The sample sizes in the respective studies ranged from 29 to 405 participants with women making up 80–100% of study participants. Most investigations were carried out by very commonly used and standardized tools, such as the Brief Pain Inventory (BPI) [22,30], the Pain Coping Questionnaire (PCQ) [30], the Pain Catastrophizing Scale (PCS) [22,30] for pain and pain coping, and the Visual Analogue Scale (VAS) [19,36,38] for pain and fatigue, while the Fatigue Severity Scale (FSS), the Vitality subscale from SF-36 [40], and the Functional Assessment Chronic Illness Therapy Fatigue (FACIT-Fatigue) [23,41] were used for fatigue. A proportion of 65–78% of respondents reported significant fatigue [30,36], and 40% of them reported clinical pain [30] and 22% pain catastrophizing [30]. SLE patients had poorer fatigue outcomes than controls [23]. Fatigue, pain intensity, and pain catastrophizing strongly predicted HRQoL and depression in individuals with SLE [26,27,36,38,39,40].
3.3. Health–Related Quality of Life in SLE
HRQoL in SLE was assessed in nineteen investigations in thirteen countries in Europe, Asia, and America. One study involved international respondents [19,20,22,24,25,28,29,31,32,33,34,35,36,37,40,41,42,43]. The total number of participants amounted to 6319 respondents while sample sizes ranged from 29 to 1803. The proportion of female respondents in the sample reached 80–100%. Most studies applied generic and disease-specific questionnaires, such as the SF-36 [19,23,26,27,31,32,33,35,36,37,39,40,41] and the LupusPRO [28,29,34], but one study applied qualitative methods [25]. Lupus was associated with poor HRQoL outcomes and both the JSLE and SLE patients had worse HRQoL than the controls [30,41,43]. Moreover, patients with SLE reported worse oral HRQoL despite better oral hygiene habits [20]. Cross-sectional and longitudinal studies have indicated that HRQoL is positively associated with self-management skills and regular physical activity [33]. Poor HRQoL scores were associated with lower educational status, smoking, sleep quality, fatigue, disability, organ involvement, pain catastrophizing, problematic support, and symptoms of depression and anxiety [21,24,30,31,32,33,34,35,37,39,41]. To add, lupus nephritis symptoms were strongly associated with poorer HRQoL outcomes controlling for age, ethnicity, gender, and country of residence [28]. Furthermore, males tended to have poorer scores than females [29]. There were inconsistent findings on the association between HRQoL in SLE, age, disease activity, pain severity, and treatment regimen [22,31]. In Feldman’study [25] on patients’ unmet needs for informative, emotional, and self-esteem support, participants reported feelings of loneliness and social isolation, and a need for informative support on SLE at the diagnostic disclosure.
3.4. Focusing on Psychosocial Adjustment to the Disease
The influence of psychological interventions for improving self-management skills and medical adherence in SLE patients was evaluated in five randomized controlled trials in China and in the U.S. [45,46,49,51,52]. The sample sizes varied from 19 to 125 while the number of respondents totaled 506. The proportion of women in each study ranged from 84–100%. The interventions addressed a plethora of aspects of psychosocial adjustment with the illness, such as: health locus of control [45], improving positive health behaviors [49,51], medical adherence [46,49,50,52], patients’ needs for social support [49], and self-efficacy [49,51]. The interventions employed digital adherence technologies [46,48,51], CBT intervention [45], stationary and social-media-based patient education [48,49,50,51], focus groups, and support groups with various meeting cadences and duration [49]. Scalzi’s study [49] found that an Internet-based educational intervention was associated with significantly enhanced medical adherence, self-efficacy, sense of agency, and empowerment scores in the experimental group compared to the controls. Xie’s [52] study captured the significant benefits of a 12 wk post-hospital transitional care intervention on positive health-behaviors, self-care, and adjustment to illness. White [51] observed insignificant improvements in the perceived lupus self-efficacy, patient activation, self-efficacy, and lower disease activity in the experimental group only. Similarly, Harry’s study [46] yielded only non-significant pre- and post-intervention differences in medical adherence in the intervention group. Nonetheless, Brown’s study 45] could not find any differences in outcome measures between two experimental groups receiving psychoeducation and cognitive behavioral treatment, and controls who did not receive treatment.
3.5. Improving HRQoL in SLE Patients
The efficacy of HRQoL interventions for SLE patients was evaluated in four randomized controlled trials carried out in Brazil, Greece, Serbia, and the U.S. [44,47,48,50]. The sample sizes varied from 21 to 62 while the total number of respondents reached 230. The lowest percentage of women in a single study reached 76% [50], but there were two studies involving only females [44,45]. Two studies focused on adolescent JSLE patients [45,46,47,48,49]. The publications described a home-based and stationary personalized physical exercise [44,47,50], the CBT approach [45], patient education, and app-supported mobile procedures [48,51] with a total duration of six to twenty-four weeks. Bogdanovic [44] demonstrated the benefits of exercise on HRQoL. Similarly, Keramiotou’s study [47] indicated a six month upper limb workout routine enhanced the HRQoL in the experimental group, but the differences between the intervention group and the treatment-as-usual control group could not be found. Moreover, Sieczkowska’s investigation [50] of a home-based exercise in SLE indicated the program was well-accepted by the study participants, but statistical differences in the HRQoL between the experimental and the control group could not be indicated.
4. Discussion
Despite a progress in understanding the pathophysiology and improving the treatments for SLE, the experience of the disease and subsequent treatment impose a large burden on patients, their families, and the society. The goal of this paper was to present empirical research on the psychological outcomes of lupus and the currently used psychological interventions for individuals with the disease.
4.1. Psychological Consequences of SLE
The psychological consequences of lupus were assessed by way of popular standardized methods, such as BDI II, HADS, or SF-36. In the great majority of the reviewed studies, lupus was associated with high rates of fatigue, pain, pain catastrophizing, psychological distress, anxiety, depression, and impaired sleep. SLE patients around the world reported significantly lower scores in several HRQoL domains compared to individuals with other rheumatologic diseases and healthy controls. Despite some data inconsistencies, several indicators of QoL, such as pain and fatigue, strongly correlated with mental health indicators, such as depression and anxiety. Additionally, the relationship between HRQoL and socioeconomic variables, such as family income or educational level, was non-significant or the findings were inconsistent. However, available information on the psychological responses to illness indicated that socioeconomic disparities were strongly associated with subjective HRQoL in chronically ill children and adults [53,54]. Jolly’s study [29] illuminated the sex differences in the psychological responses to lupus. They found that men were more adversely affected by the disease than women, particularly in the social support and coping domains. Women, in turn, reported poorer outcomes in, e.g., the cognitive domain and pain. This trend may also be characteristic for other rheumatologic diseases. For example, comparative studies on the psychological aftermath of rheumatoid arthritis (RA) in males and in females [55] indicate that females with RA have significantly better scores in bodily pain, but their physical and mental health are worse. In fact, emerging evidence in medical psychology suggests that male and female psychological reactions to chronic diseases differ [56,57]. For example, the investigations on Parkinson’s disease indicated the female gender was associated with lower scores both in physical and in emotional functioning while males had poorer outcomes in the cognitive domains of HRQoL [58]. These findings highlighted a need to explore the gender differences in the psychological response to a chronic illness and the importance of personalized support for chronic conditions.
4.2. Interventions to Improve Patients’ HRQoL and Well-Being
The current paper also analyzed the psychological interventions for lupus patients. Overall, the quality of the interventional studies assessed was high as all of them used a randomized controlled trial design to determine the outcomes with three publications on an experimental control group design. Three observations demonstrated significant post-intervention improvements in the experimental group compared with the controls. Importantly, the results of Xie’s study [52] highlighted the significance of early intervention and the role of transitional care in the process of adjusting to a chronic disease and living a happy life with lupus.
4.3. The Effect of Physical Fitness Interventions on HRQoL, Depression, and General Well-Being
Three studies included in the current review analyzed the effect of physical fitness interventions on HRQoL, depression, and general well-being [44,47,50]. Although only modest statistical differences between the experimental group and the controls could be detected, exercise led to improvements in the respondents’ well-being and the vital mental health indicators in the study participants. These outcomes are consistent with previous findings on the impact of structured physical activity on well-being and HRQoL in individuals with a chronic disease [59]. It may be concluded that regular low impact cardio workouts, which improve mobility and build stamina but are easy on the joints, can be recommended for SLE patients and could be combined with pharmacological treatment. Future investigations should include larger samples and the interventions should be longer to evoke the lingering beneficial effects for patients’ health.
This review has some limitations. First, only a small number of interventions presented in this review depicted the so-called “talk therapies” to elicit change and increase well-being. Nonetheless, the term “psychological intervention” has not been precisely defined yet and continues to attract attention in the literature [60,61]. In this review, “psychological intervention” pertained to treatment procedures that aim to enhance patients’ psychological well-being and various aspects of health-related quality of life. To add, the observations collected here varied in terms of sample size, experimental procedure, approaches, and outcome measures.
Second, although the methodological aspects related to experimental design were duly considered in the presented interventions, their outcomes may have resulted from a number of variables that were not considered, such as cultural, religious background, or permanent urban/rural residence. Since these factors may also impede or facilitate participation in psychological interventions, they should be carefully investigated because of stigma towards mental health services and towards patients. Consequently, the process of the implementation of psychological interventions should be investigated at the level of the healthcare provider (HCP), patient, and at the organizational/corporate level to stimulate inclusion mechanisms and patient-HCP partnership.
From a methodological point of view, future randomized controlled trials should include placebo groups as an addition to multiple experimental group designs to objectivize the interpretation of the results.
Third, although cognitive symptoms of lupus such as “brain fog” are very well-known, only very few epidemiological studies or interventions identified in the review addressed research themes related to cognitive dysfunction in the course of SLE and NPSLE [62]. Hence, continued research is needed towards developing neurorehabilitation procedures to mitigate the negative effects of the disease and enhance patients’ cognitive, social, and vocational skills. All in all, this review contributes to the existing literature on the psychological aspects of SLE as valuable adjuncts to medical care and highlights the possibilities for continued research on the topic.
5. Conclusions
- Current studies should be revisited with the emergence of stronger evidence for the efficacy of specific psychological intervention procedures. The impact of intervention procedures may be mediated by respondents’ cultural and religious background or permanent urban/rural residence. Hence, these factors should be carefully considered while developing experimental designs.
- Evidence-based research is needed on effective psychological interventions for cognitive dysfunction in SLE and neurorehabilitation to ameliorate its adverse effects.
Author Contributions
Conceptualization, K.W.-B. and E.M.; methodology, K.W.-B., E.M., D.S., P.K., G.T. and W.S.; formal analysis, K.W.-B., E.M., D.S., P.K., G.T. and W.S.; investigation, K.W.-B., E.M., D.S., P.K., G.T. and W.S.; writing—original draft preparation, K.W.-B., E.M., D.S., P.K. and W.S.; writing—review and editing, K.W.-B., D.S., P.K., G.T. and W.S.; supervision, W.S. All authors have read and agreed to the published version of the manuscript.
Funding
Paper has been supported by the grant from Medical University of Silesia PCN-1-213/N/9.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Manson, J.J.; Rahman, A. Systemic lupus erythematosus. Orphanet J. Rare Dis. 2006, 1, 6. [Google Scholar] [CrossRef]
- Stojan, G.; Petri, M. Epidemiology of systemic lupus erythematosus: An update. Curr. Opin. Rheumatol. 2018, 30, 144–150. [Google Scholar] [CrossRef]
- Dörner, T.; Furie, R. Novel paradigms in systemic lupus erythematosus. Lancet 2019, 393, 2344–2358. [Google Scholar] [CrossRef]
- Kiriakidou, M.; Ching, C.L. Systemic Lupus Erythematosus. Ann. Intern. Med. 2020, 172, ITC81–ITC96. [Google Scholar] [CrossRef]
- Leone, P.; Prete, M.; Malerba, E.; Bray, A.; Susca, N.; Ingravallo, G.; Racanelli, V. Lupus Vasculitis: An Overview. Biomedicines 2021, 9, 1626. [Google Scholar] [CrossRef]
- Pons-Estel, G.J.; Ugarte-Gil, M.F.; Alarcón, G.S. Epidemiology of systemic lupus erythematosus. Expert Rev. Clin. Immunol. 2017, 13, 799–814. [Google Scholar] [CrossRef]
- Fanouriakis, A.; Tziolos, N.; Bertsias, G.; Boumpas, D.T. Update οn the diagnosis and management of systemic lupus erythematosus. Ann. Rheum. Dis. 2021, 80, 14–25. [Google Scholar] [CrossRef]
- Carrión-Barberà, I.; Salman-Monte, T.C.; Vílchez-Oya, F.; Monfort, J. Neuropsychiatric involvement in systemic lupus erythematosus: A review. Autoimmun. Rev. 2021, 20, 102780. [Google Scholar] [CrossRef]
- The American College of Rheumatology nomenclature and case definitions for neuropsychiatric lupus syndromes. Arthritis Rheum. 1999, 42, 599–608. [CrossRef]
- Goldenberg, D.L. The Interface of Pain and Mood Disturbances in the Rheumatic Diseases. Semin. Arthritis Rheum. 2010, 40, 15–31. [Google Scholar] [CrossRef]
- Staud, R. Peripheral and Central Mechanisms of Fatigue in Inflammatory and Noninflammatory Rheumatic Diseases. Curr. Rheumatol. Rep. 2012, 14, 539–548. [Google Scholar] [CrossRef]
- Zhang, L.; Fu, T.; Yin, R.; Zhang, Q.; Shen, B. Prevalence of depression and anxiety in systemic lupus erythematosus: A systematic review and meta-analysis. BMC Psychiatry 2017, 17, 70. [Google Scholar] [CrossRef]
- Wu, L.; Shi, P.-L.; Tao, S.-S.; Tao, J.-H.; Wu, G.-C. Decreased sleep quality in patients with systemic lupus erythematosus: A meta-analysis. Clin. Rheumatol. 2021, 40, 913–922. [Google Scholar] [CrossRef]
- Fanouriakis, A.; Kostopoulou, M.; Alunno, A.; Aringer, M.; Bajema, I.; Boletis, J.N.; Cervera, R.; Doria, A.; Gordon, C.; Govoni, M.; et al. 2019 update of the EULAR recommendations for the management of systemic lupus erythematosus. Ann. Rheum. Dis. 2019, 78, 736–745. [Google Scholar] [CrossRef]
- Shi, Y.; Li, M.; Liu, L.; Wang, Z.; Wang, Y.; Zhao, J.; Tian, X.; Li, M.; Zeng, X. Relationship between disease activity, organ damage and health-related quality of life in patients with systemic lupus erythematosus: A systemic review and meta-analysis. Autoimmun. Rev. 2021, 20, 102691. [Google Scholar] [CrossRef]
- Checa, C.M.; Zirkzee, E.J.; Huizinga, T.W.; Steup-Beekman, G.M. Management of Neuropsychiatric Systemic Lupus Erythematosus: Current Approaches and Future Perspectives. Drugs 2016, 76, 459–483. [Google Scholar] [CrossRef]
- Fangtham, M.; Kasturi, S.; Bannuru, R.R.; Nash, J.L.; Wang, C. Non-pharmacologic therapies for systemic lupus erythematosus. Lupus 2019, 28, 703–712. [Google Scholar] [CrossRef]
- Bai, R.; Liu, S.; Zhao, Y.; Cheng, Y.; Li, S.; Lai, A.; Xie, Z.; Xu, X.; Lu, Z.; Xu, J. Depressive and Anxiety Disorders in Systemic Lupus Erythematosus Patients without Major Neuropsychiatric Manifestations. J. Immunol. Res. 2016, 2016, 2829018. [Google Scholar] [CrossRef]
- Chalhoub, N.E.; Luggen, M.E. Depression-, Pain-, and Health-Related Quality of Life in Patients with Systemic Lupus Erythematosus. Int. J. Rheumatol. 2022, 2022, 6290736. [Google Scholar] [CrossRef]
- Corrêa, J.D.; A Branco, L.G.; Calderaro, D.C.; Mendonça, S.M.S.; Travassos, D.; A Ferreira, G.; Teixeira, A.L.; Abreu, L.G.; A Silva, T. Impact of systemic lupus erythematosus on oral health-related quality of life. Lupus 2018, 27, 283–289. [Google Scholar] [CrossRef]
- Davis, A.M.; Graham, T.B.; Zhu, Y.; McPheeters, M.L. Depression and medication nonadherence in childhood-onset systemic lupus erythematosus. Lupus 2018, 27, 1532–1541. [Google Scholar] [CrossRef]
- Donnelly, C.; Cunningham, N.; Jones, J.; Ji, L.; I Brunner, H.; Kashikar-Zuck, S. Fatigue and depression predict reduced health-related quality of life in childhood-onset lupus. Lupus 2018, 27, 124–133. [Google Scholar] [CrossRef] [PubMed]
- Elefante, E.; Tani, C.; Stagnaro, C.; Ferro, F.; Parma, A.; Carli, L.; Signorini, V.; Zucchi, D.; Peta, U.; Santoni, A.; et al. Impact of fatigue on health-related quality of life and illness perception in a monocentric cohort of patients with systemic lupus erythematosus. RMD Open 2020, 6, e001133. [Google Scholar] [CrossRef]
- Elera-Fitzcarrald, C.; Alva, M.; Gamboa-Cárdenas, R.; Mora-Trujillo, C.S.; Zevallos, F.; García-Poma, A.; Medina, M.; Rodriguez-Bellido, Z.; A Perich-Campos, R.; A Pastor-Asurza, C.; et al. Factors associated with health-related quality of life in Peruvian patients with systemic lupus erythematosus. Lupus 2018, 27, 913–919. [Google Scholar] [CrossRef] [PubMed]
- Feldman, C.H.; Bermas, B.L.; Zibit, M.; Fraser, P.; Todd, D.J.; Fortin, P.R.; Massarotti, E.; Costenbader, K.H. Designing an intervention for women with systemic lupus erythematosus from medically underserved areas to improve care: A qualitative study. Lupus 2013, 22, 52–62. [Google Scholar] [CrossRef]
- Figueiredo-Braga, M.; Cornaby, C.; Bernardes, M.; Figueiredo, M.; Mesquita, C.D.S.; Costa, L.; Poole, B.D. Correlation between physical markers and psychiatric health in a Portuguese systemic lupus erythematosus cohort: The role of suffering in chronic autoimmune disease. PLoS ONE 2018, 13, e0195579. [Google Scholar] [CrossRef]
- Figueiredo-Braga, M.; Silva, B.; Ganhão, S.; Aguiar, F.; Cornaby, C.; Brito, I.; Poole, B.D. Kidney Function, Age, and Education as Contributors to Depression and Anxiety in Juvenile Systemic Lupus Erythematosus. Eur. J. Investig. Health Psychol. Educ. 2021, 11, 1503–1515. [Google Scholar] [CrossRef]
- Jolly, M.; Toloza, S.; Goker, B.; E Clarke, A.; Navarra, S.V.; Wallace, D.; Weisman, M.; Mok, C.C. Disease-specific quality of life in patients with lupus nephritis. Lupus 2018, 27, 257–264. [Google Scholar] [CrossRef]
- Jolly, M.; Sequeira, W.; Block, J.A.; Toloza, S.; Bertoli, A.; Blazevic, I.; Vila, L.M.; Moldovan, I.; Torralba, K.D.; Mazzoni, D.; et al. Sex Differences in Quality of Life in Patients with Systemic Lupus Erythematosus. Arthritis Care Res. 2019, 71, 1647–1652. [Google Scholar] [CrossRef]
- Jones, J.T.; Cunningham, N.; Kashikar-Zuck, S.; Brunner, H.I. Pain, Fatigue, and Psychological Impact on Health-Related Quality of Life in Childhood-Onset Lupus. Arthritis Care Res. 2016, 68, 73–80. [Google Scholar] [CrossRef]
- Kiani, A.N.; Strand, V.; Fang, H.; Jaranilla, J.; Petri, M. Predictors of self-reported health-related quality of life in systemic lupus erythematosus. Rheumatology 2013, 52, 1651–1657. [Google Scholar] [CrossRef] [PubMed]
- Louthrenoo, W.; Kasitanon, N.; Morand, E.; Kandane-Rathnayake, R. Comparison of performance of specific (SLEQOL) and generic (SF36) health-related quality of life questionnaires and their associations with disease status of systemic lupus erythematosus: A longitudinal study. Arthritis Res. Ther. 2020, 22, 8. [Google Scholar] [CrossRef] [PubMed]
- Mazzoni, D.; Cicognani, E.; Prati, G. Health-related quality of life in systemic lupus erythematosus: A longitudinal study on the impact of problematic support and self-efficacy. Lupus 2016, 26, 125–131. [Google Scholar] [CrossRef]
- Mirbagher, L.; Gholamrezaei, A.; Hosseini, N.; Bonakdar, Z.S. Sleep quality in women with systemic lupus erythematosus: Contributing factors and effects on health-related quality of life. Int. J. Rheum. Dis. 2016, 19, 305–311. [Google Scholar] [CrossRef]
- Mok, C.C.; Chan, K.L.; Ho, L.Y. Association of depressive/anxiety symptoms with quality of life and work ability in patients with systemic lupus erythematosus. Clin. Exp. Rheumatol. 2016, 34, 389–395. [Google Scholar]
- Monahan, R.C.; de Voorde, L.J.B.-V.; Eikenboom, J.; Fronczek, R.; Kloppenburg, M.; Middelkoop, H.A.; Terwindt, G.M.; van der Wee, N.J.; Huizinga, T.W.; Steup-Beekman, G.M. Fatigue in patients with systemic lupus erythematosus and neuropsychiatric symptoms is associated with anxiety and depression rather than inflammatory disease activity. Lupus 2021, 30, 1124–1132. [Google Scholar] [CrossRef]
- Moon, S.-J.; Kang, K.Y.; Kwok, S.-K.; Ju, J.H.; Hong, Y.-S.; Park, S.-H.; Jeon, C.H.; Choi, S.T.; Song, J.-S.; Min, J.-K. Differences in quality of life determinants according to the presence of fibromyalgia in middle-aged female patients with systemic lupus erythematosus: A multicenter, cross-sectional, single-ethnicity cohort. Int. J. Rheum. Dis. 2018, 21, 1173–1184. [Google Scholar] [CrossRef]
- Nowicka-Sauer, K.; Hajduk, A.; Kujawska-Danecka, H.; Banaszkiewicz, D.; Smolenska, Z.; Czuszyńska, Z.; Siebert, J. Illness perception is significantly determined by depression and anxiety in systemic lupus erythematosus. Lupus 2018, 27, 454–460. [Google Scholar] [CrossRef]
- Pettersson, S.; Lövgren, M.; Eriksson, L.; Moberg, C.; Svenungsson, E.; Gunnarsson, I.; Henriksson, E.W. An exploration of patient-reported symptoms in systemic lupus erythematosus and the relationship to health-related quality of life. Scand. J. Rheumatol. 2012, 41, 383–390. [Google Scholar] [CrossRef]
- Pettersson, S.; Boström, C.; Eriksson, K.; Svenungsson, E.; Gunnarsson, I.; Henriksson, E.W. Lifestyle habits and fatigue among people with systemic lupus erythematosus and matched population controls. Lupus 2015, 24, 955–965. [Google Scholar] [CrossRef]
- Piga, M.; Congia, M.; Gabba, A.; Figus, F.; Floris, A.; Mathieu, A.; Cauli, A. Musculoskeletal manifestations as determinants of quality of life impairment in patients with systemic lupus erythematosus. Lupus 2018, 27, 190–198. [Google Scholar] [CrossRef] [PubMed]
- A Tee, C.; O Salido, E.; Reyes, P.W.C.; Ho, R.C.; Tee, M.L. Psychological State and Associated Factors During the 2019 Coronavirus Disease (COVID-19) Pandemic Among Filipinos with Rheumatoid Arthritis or Systemic Lupus Erythematosus. Open Access Rheumatol. Res. Rev. 2020, 12, 215–222. [Google Scholar] [CrossRef]
- Yilmaz-Oner, S.; Oner, C.; Dogukan, F.M.; Moses, T.F.; Demir, K.; Tekayev, N.; Yilmaz, N.; Tuglular, S.; Direskeneli, H. Anxiety and depression predict quality of life in Turkish patients with systemic lupus erythematosus. Clin. Exp. Rheumatol. 2015, 33, 360–365. [Google Scholar] [PubMed]
- Bogdanovic, G.; Stojanovich, L.; Djokovic, A.; Stanisavljevic, N. Physical Activity Program Is Helpful for Improving Quality of Life in Patients with Systemic Lupus Erythematosus. Tohoku J. Exp. Med. 2015, 237, 193–199. [Google Scholar] [CrossRef]
- Brown, R.T.; Shaftman, S.R.; Tilley, B.C.; Anthony, K.K.; Bonner, M.J.; Kral, M.C.; Maxson, B.; Mee, L.; Vogler, L.B.; Schanberg, L.E.; et al. The Health Education for Lupus Study: A Randomized Controlled Cognitive-Behavioral Intervention Targeting Psychosocial Adjustment and Quality of Life in Adolescent Females with Systemic Lupus Erythematosus. Am. J. Med Sci. 2012, 344, 274–282. [Google Scholar] [CrossRef]
- Harry, O.; Crosby, L.E.; Mara, C.; Ting, T.V.; Huggins, J.L.; Modi, A.C. Feasibility and acceptability of an innovative adherence intervention for young adults with childhood-onset systemic Lupus Erythematosus. Pediatr. Rheumatol. 2020, 18, 36. [Google Scholar] [CrossRef]
- Keramiotou, K.; Anagnostou, C.; Kataxaki, E.; Galanos, A.; Sfikakis, P.P.; Tektonidou, M.G. The impact of upper limb exercise on function, daily activities and quality of life in systemic lupus erythematosus: A pilot randomised controlled trial. RMD Open 2020, 6, e001141. [Google Scholar] [CrossRef]
- Khan, F.; Granville, N.; Malkani, R.; Chathampally, Y. Health-Related Quality of Life Improvements in Systemic Lupus Erythematosus Derived from a Digital Therapeutic Plus Tele-Health Coaching Intervention: Randomized Controlled Pilot Trial. J. Med. Internet Res. 2020, 22, e23868. [Google Scholar] [CrossRef]
- Scalzi, L.V.; Hollenbeak, C.S.; Mascuilli, E.; Olsen, N. Improvement of medication adherence in adolescents and young adults with SLE using web-based education with and without a social media intervention, a pilot study. Pediatr. Rheumatol. 2018, 16, 18. [Google Scholar] [CrossRef]
- Sieczkowska, S.M.; Astley, C.; Marques, I.G.; Iraha, A.Y.; Franco, T.C.; Ihara, B.P.; Lavorato, S.S.M.; Lindoso, L.; Setoue, D.N.D.; Tanigava, N.Y.; et al. A home-based exercise program during COVID-19 pandemic: Perceptions and acceptability of juvenile systemic lupus erythematosus and juvenile idiopathic arthritis adolescents. Lupus 2022, 31, 443–456. [Google Scholar] [CrossRef]
- White, A.A.; Ba, A.; Faith, T.D.; Ramakrishnan, V.; Dismuke-Greer, C.L.; Oates, J.C.; Williams, E.M. The Care-coordination Approach to Learning Lupus Self-Management: A patient navigator intervention for systemic lupus inpatients. Lupus Sci. Med. 2021, 8, e000482. [Google Scholar] [CrossRef] [PubMed]
- Xie, X.; Song, Y.; Yang, H.; Nie, A.; Chen, H.; Li, J.-P. Effects of transitional care on self-care, readmission rates, and quality of life in adult patients with systemic lupus erythematosus: A randomized controlled trial. Arthritis Res. Ther. 2018, 20, 184. [Google Scholar] [CrossRef] [PubMed]
- Díaz-Toro, F.; Verdejo, H.E.; Castro, P.F. Socioeconomic Inequalities in Heart Failure. Heart Fail. Clin. 2015, 11, 507–513. [Google Scholar] [CrossRef] [PubMed]
- Didsbury, M.S.; Kim, S.; Medway, M.M.; Tong, A.; McTaggart, S.J.; Walker, A.M.; White, S.; Mackie, F.E.; Wong, G.; Kara, T.; et al. Socio-economic status and quality of life in children with chronic disease: A systematic review. J. Paediatr. Child Health 2016, 52, 1062–1069. [Google Scholar] [CrossRef]
- Matcham, F.; Scott, I.C.; Rayner, L.; Hotopf, M.; Kingsley, G.H.; Norton, S.; Scott, D.L.; Steer, S. The impact of rheumatoid arthritis on quality-of-life assessed using the SF-36: A systematic review and meta-analysis. Semin. Arthritis Rheum. 2014, 44, 123–130. [Google Scholar] [CrossRef]
- Yu, T.; Enkh-Amgalan, N.; Zorigt, G.; Hsu, Y.-J.; Chen, H.-J.; Yang, H.-Y. Gender differences and burden of chronic conditions: Impact on quality of life among the elderly in Taiwan. Aging 2019, 31, 1625–1633. [Google Scholar] [CrossRef]
- Gemmell, L.A.; Terhorst, L.; Jhamb, M.; Unruh, M.; Myaskovsky, L.; Kester, L.; Steel, J.L. Gender and Racial Differences in Stress, Coping, and Health-Related Quality of Life in Chronic Kidney Disease. J. Pain Symptom Manag. 2016, 52, 806–812. [Google Scholar] [CrossRef]
- Crispino, P.; Gino, M.; Barbagelata, E.; Ciarambino, T.; Politi, C.; Ambrosino, I.; Ragusa, R.; Marranzano, M.; Biondi, A.; Vacante, M. Gender Differences and Quality of Life in Parkinson’s Disease. Int. J. Environ. Res. Public Health 2020, 18, 198. [Google Scholar] [CrossRef]
- Pedersen, B.K.; Saltin, B. Exercise as medicine–Evidence for prescribing exercise as therapy in 26 different chronic diseases. Scand. J. Med. Sci. Sports 2015, 25, 1–72. [Google Scholar] [CrossRef]
- Hodges, L.J.; Walker, J.; Kleiboer, A.M.; Ramirez, A.J.; Richardson, A.; Velikova, G.; Sharpe, M. What is a psychological intervention? A metareview and practical proposal. Psycho-Oncology 2011, 20, 470–478. [Google Scholar] [CrossRef]
- Ranchor, A.V.; Fleer, J.; Sanderman, R.; Van Der Ploeg, K.M.; Coyne, J.C.; Schroevers, M. Psychological interventions for cancer survivors and cancer patients in the palliative phase. Cochrane Database Syst. Rev. 2017, 2017. [Google Scholar] [CrossRef]
- Seet, D.; Allameen, N.A.; Tay, S.H.; Cho, J.; Mak, A. Cognitive Dysfunction in Systemic Lupus Erythematosus: Immunopathology, Clinical Manifestations, Neuroimaging and Management. Rheumatol. Ther. 2021, 8, 651–679. [Google Scholar] [CrossRef] [PubMed]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).