
Perceived Support Needs of School-Aged Young People on the Autism Spectrum and Their Caregivers

 , , , , , ,
, , , , , , 
Abstract
1. Introduction
1.1. Local and International Context in Determining Necessary Supports
1.2. Support Needs as a Foundation for Determining Necessary Supports
1.3. Research Aim and Objectives
2. Materials and Methods
2.1. Research Design
2.2. Participants and Recruitment
2.3. Data Collection
2.3.1. Demographic and Clinical Characteristics
2.3.2. Support Needs Interviews
2.4. Data Analysis
3. Findings
3.1. Participants
3.2. Overview of Support Needs
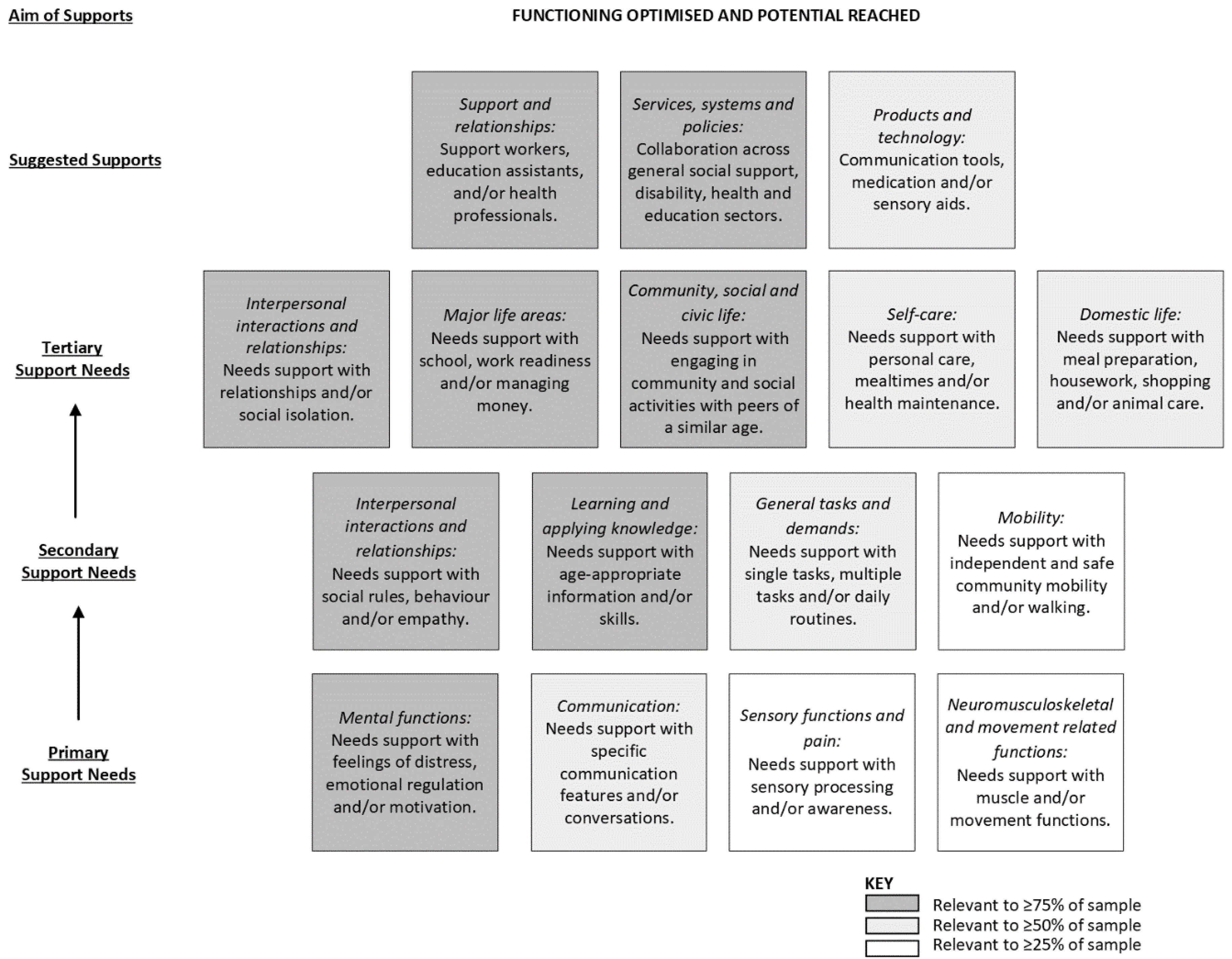
3.3. Young People
“being about (their) ability to play (their) role in society and to feel included. This includes support to transition into employment (and) possibly other roles as (they) become an adult, but also (their) genuine inclusion (not tokenistic inclusion) and (their) ability to be involved in … communities and any other hobbies that (they have) an interest in”.
3.3.1. Exploration of Primary Support Needs
3.3.2. Exploration of Secondary Support Needs
3.3.3. Exploration of Tertiary Support Needs
3.3.4. Suggested Supports to Meet Support Needs
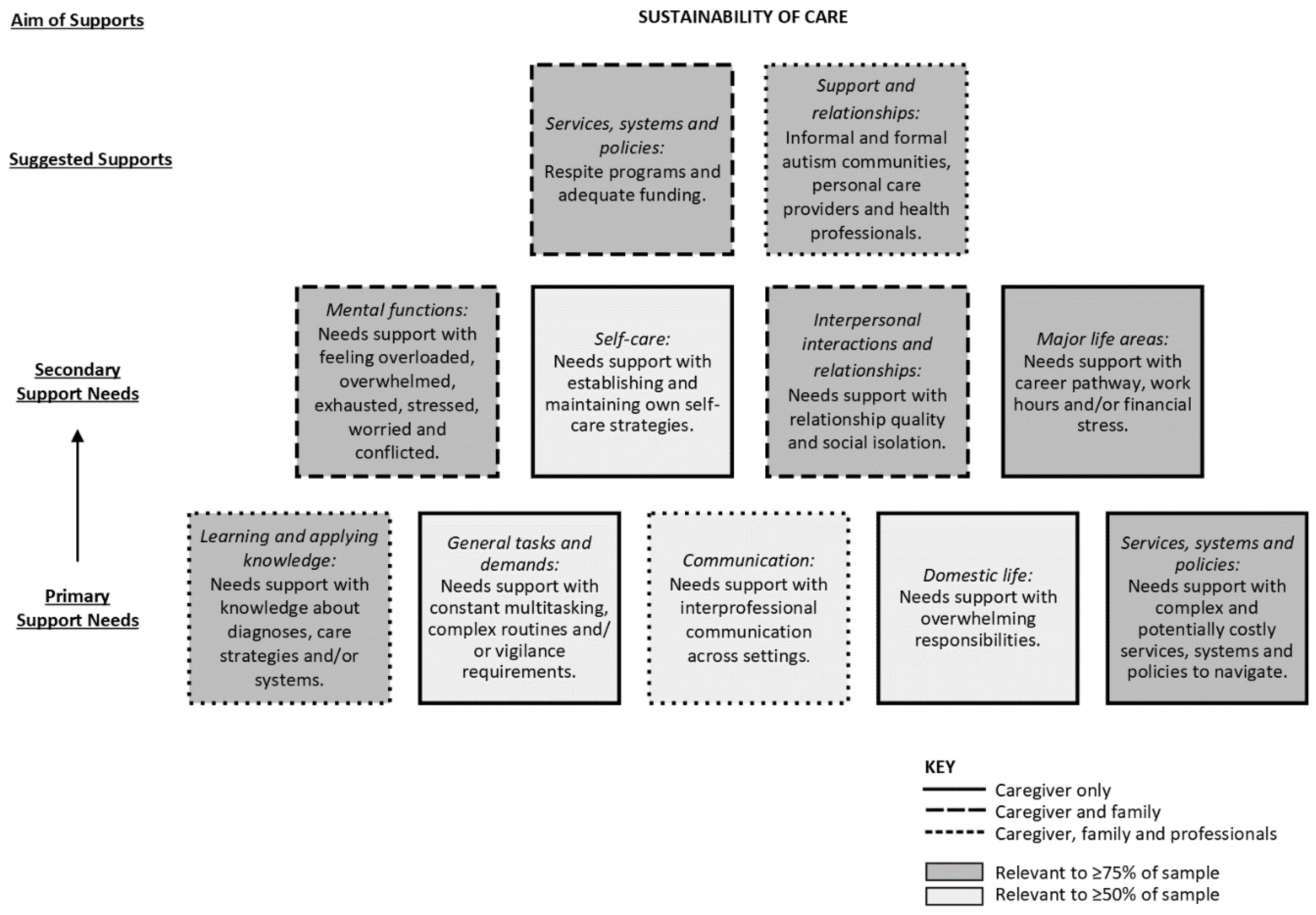
3.4. Caregiver(s) and Others
“I have little to no support. If I fall to pieces, how am I going to support my kids? Who is going to support them if I can’t? If I’m not supporting them, then they will be a burden on society forever”.
3.4.1. Exploration of Primary Support Needs
3.4.2. Exploration of Secondary Support Needs
3.4.3. Suggested Supports to Meet Support Needs
4. Discussion
4.1. Perceived Support Needs and Suggested Supports
4.2. Practice Implications during the Clinical Cycle
4.3. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Solmi, M.; Song, M.; Yon, D.; Lee, S.; Fombonne, E.; Kim, M.; Park, S.; Lee, M.; Hwang, J.; Keller, R. Incidence, prevalence, and global burden of autism spectrum disorder from 1990 to 2019 across 204 countries. Mol. Psychiatry 2022, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Hodges, H.; Fealko, C.; Soares, N. Autism spectrum disorder: Definition, epidemiology, causes, and clinical evaluation. Transl. Pediatr. 2020, 9 (Suppl. 1), S55. [Google Scholar] [CrossRef] [PubMed]
- O’Sullivan, B.; Worley, P. Setting priorities for rural allied health in Australia: A scoping review. Rural Remote Health 2020, 20, 5719. [Google Scholar] [CrossRef] [PubMed]
- Rogge, N.; Janssen, J. The economic costs of autism spectrum disorder: A literature review. J. Autism Dev. Disord. 2019, 49, 2873–2900. [Google Scholar] [CrossRef] [PubMed]
- Foster, M.; Henman, P.; Tilse, C.; Fleming, J.; Allen, S.; Harrington, R. ‘Reasonable and necessary’ care: The challenge of operationalising the NDIS policy principle in allocating disability care in Australia. Aust. J. Soc. Issues 2016, 51, 27–46. [Google Scholar] [CrossRef]
- McClure, J.; Leah, C. Is independence enough? Rehabilitation should include autonomy and social engagement to achieve quality of life. Clin. Rehabil. 2021, 35, 3–12. [Google Scholar] [CrossRef]
- World Health Organization. International Classification of Functioning, Disability, and Health; World Health Organization: Geneva, Switzerland, 2001. [Google Scholar]
- United Nations. Convention on the Rights of Persons with Disabilities and Optional Protocol; United Nations: New York, NY, USA, 2006. [Google Scholar]
- Bölte, S.; Mahdi, S.; de Vries, P.; Granlund, M.; Robison, J.; Shulman, C.; Swedo, S.; Tonge, B.; Wong, V.; Zwaigenbaum, L. The gestalt of functioning in autism spectrum disorder: Results of the international conference to develop final consensus International Classification of Functioning, Disability and Health core sets. Autism 2019, 23, 449–467. [Google Scholar] [CrossRef]
- Australian Government. National Disability Insurance Scheme Act; Australian Government: Canberra, Australia, 2013. [Google Scholar]
- UK Legislation. Care Act; UK Legislation: London, UK, 2014. [Google Scholar]
- Purcal, C.; Fisher, K.; Laragy, C. Analysing choice in Australian individual funding disability policies. Aust. J. Public Adm. 2014, 73, 88–102. [Google Scholar] [CrossRef]
- Verdugo, M.; Aguayo, V.; Arias, V.; García-Domínguez, L. A systematic review of the assessment of support needs in people with intellectual and developmental disabilities. Int. J. Environ. Res. Public Health 2020, 17, 9494. [Google Scholar] [CrossRef]
- Zander, E.; Bölte, S. The new DSM-5 impairment criterion: A challenge to early autism spectrum disorder diagnosis? J. Autism Dev. Disord. 2015, 45, 3634–3643. [Google Scholar] [CrossRef]
- Arnold, S.; Riches, V.; Stancliffe, R. Does a measure of support needs predict funding need better than a measure of adaptive and maladaptive behavior? Am. J. Intellect. Dev. Disabil. 2015, 120, 375–394. [Google Scholar] [CrossRef]
- Whitehouse, A.; Evans, K.; Eapen, V.; Wray, J. A National Guideline for the Assessment and Diagnosis of Autism Spectrum Disorders in Australia; Autism CRC: Brisbane, Australia, 2018. [Google Scholar]
- Oxford University Press Oxford English Dictionary. Available online: https://www.oed.com/ (accessed on 8 September 2022).
- Thompson, J.; Bradley, V.; Buntinx, W.; Schalock, R.; Shogren, K.; Snell, M.; Wehmeyer, M.; Borthwick-Duffy, S.; Coulter, D.; Craig, E. Conceptualizing supports and the support needs of people with intellectual disability. Intellect. Dev. Disabil. 2009, 47, 135–146. [Google Scholar] [CrossRef]
- Heaney, C.; Israel, B. Social networks and social support In Health Behavior and Health Education: Theory, Research, and Practice, 4th ed.; Jossey-Bass: San Francisco, CA, USA, 2008; pp. 189–210. [Google Scholar]
- Arnold, S.; Riches, V.; Stancliffe, R. I-CAN: The classification and prediction of support needs. J. Appl. Res. Intellect. Disabil. 2014, 27, 97–111. [Google Scholar] [CrossRef]
- NDIS. Independent Assessment: Selection of Assessment Tools; National Disability Insurance Agency: Geelong, Australia, 2020. [Google Scholar]
- Hartley, S.; Schultz, H. Support needs of fathers and mothers of children and adolescents with autism spectrum disorder. J. Autism Dev. Disord. 2015, 45, 1636–1648. [Google Scholar] [CrossRef]
- Lai, J.; Weiss, J. Priority service needs and receipt across the lifespan for individuals with autism spectrum disorder. Autism Res. 2017, 10, 1436–1447. [Google Scholar] [CrossRef]
- Roddy, Á.; O’Neill, C. Predictors of unmet needs and family debt among children and adolescents with an autism spectrum disorder: Evidence from Ireland. Health Policy 2020, 124, 317–325. [Google Scholar] [CrossRef]
- Eggleston, M.; Thabrew, H.; Frampton, C.; Eggleston, K.; Hennig, S. Obtaining an autism spectrum disorder diagnosis and supports: New Zealand parents’ experiences. Res. Autism Spectr. Disord. 2019, 62, 18–25. [Google Scholar] [CrossRef]
- Crane, L.; Chester, J.; Goddard, L.; Henry, L.; Hill, E. Experiences of autism diagnosis: A survey of over 1000 parents in the United Kingdom. Autism 2016, 20, 153–162. [Google Scholar] [CrossRef]
- Arias, V.; Aguayo, V.; Verdugo, M.; Amor, A. Differences in the support needs of children with developmental disabilities among groups of medical and behavioral needs. PeerJ 2020, 8, e9557. [Google Scholar] [CrossRef]
- Evans, K.; van der Meer, L.; Johnston, S.; Boutrus, M.; Eggleston, M.; Thabrew, H.; Waddington, H.; Whitehouse, A. The autism diagnostic process in New Zealand: A call for action from caregivers. In The Autism Spectrum Disorder Diagnostic Process in New Zealand; van der Meer, L., Evans, K., Eds.; Autism CRC: Brisbane, Australia, 2020. [Google Scholar]
- Colombet, C.; Alcaraz, C.; de la Tribonnière, X.; Morsa, M.; Rattaz, C.; Baghdadli, A. Self-reported needs of caregivers of people with autism spectrum disorder. J. Autism Dev. Disord. 2022, 1–8. [Google Scholar] [CrossRef]
- Galpin, J.; Barratt, P.; Ashcroft, E.; Greathead, S.; Kenny, L.; Pellicano, E. ‘The dots just don’t join up’: Understanding the support needs of families of children on the autism spectrum. Autism 2018, 22, 571–584. [Google Scholar] [CrossRef] [PubMed]
- Han, E.; Tan, M.; Crane, L.; Legido-Quigley, H. A qualitative study of autism services and supports in Singapore: Perspectives of service providers, autistic adults and caregivers. Autism 2021, 25, 2279–2290. [Google Scholar] [CrossRef] [PubMed]
- Papoudi, D.; Jørgensen, C.; Guldberg, K.; Meadan, H. Perceptions, experiences, and needs of parents of culturally and linguistically diverse children with autism: A scoping review. Rev. J. Autism Dev. Disord. 2021, 8, 195–212. [Google Scholar] [CrossRef]
- Hajar, A. Theoretical foundations of phenomenography: A critical review. High. Educ. Res. Dev. 2021, 40, 1421–1436. [Google Scholar] [CrossRef]
- Sjöström, B.; Dahlgren, L. Applying phenomenography in nursing research. J. Adv. Nurs. 2002, 40, 339–345. [Google Scholar] [CrossRef]
- Harris, P.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J. A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef]
- Harris, P.; Taylor, R.; Minor, B.; Elliott, V.; Fernandez, M.; O’Neal, L.; McLeod, L.; Delacqua, G.; Delacqua, F.; Kirby, J. The REDCap consortium: Building an international community of software platform partners. J. Biomed. Inform. 2019, 95, 103208. [Google Scholar] [CrossRef]
- EuroQol Research Foundation. EQ-5D-5L User Guide (Version 3); EuroQol Research Foundation: Rotterdam, The Netherlands, 2019. [Google Scholar]
- The International Wellbeing Group. Personal Wellbeing Index—Adult (English) Manual, 5th ed.; Centre on Quality of Life, Deakin University: Melbourne, Australia, 2013. [Google Scholar]
- Feng, Y.; Kohlmann, T.; Janssen, M.; Buchholz, I. Psychometric properties of the EQ-5D-5L: A systematic review of the literature. Qual. Life Res. 2021, 30, 647–673. [Google Scholar] [CrossRef]
- Grodberg, D.; Weinger, P.; Kolevzon, A.; Soorya, L.; Buxbaum, J. Brief report: The Autism Mental Status Examination: Development of a brief autism-focused exam. J. Autism Dev. Disord. 2012, 42, 455–459. [Google Scholar] [CrossRef]
- Cederlund, M. Autism Mental Status Examination (AMSE): A valid instrument in the evaluation of pre-school children with suspected autism spectrum disorders? J. Autism Dev. Disord. 2019, 49, 2965–2979. [Google Scholar] [CrossRef]
- Sparrow, S.; Cicchetti, D.; Saulnier, C. Vineland Adaptive Behaviour Scales, 3rd ed.; Pearson Inc.: San Antonio, TX, USA, 2016. [Google Scholar]
- D’Arcy, E.; Wallace, K.; Chamberlain, A.; Evans, K.; Milbourn, B.; Bölte, S.; Whitehouse, A.; Girdler, S. Content validation of common measures of functioning for young children against the International Classification of Functioning, Disability and Health and Code and Core Sets relevant to neurodevelopmental conditions. Autism 2022, 26, 928–939. [Google Scholar] [CrossRef]
- Hayden-Evans, M.; Milbourn, B.; D’Arcy, E.; Chamberlain, A.; Afsharnejad, B.; Evans, K.; Whitehouse, A.; Bölte, S.; Girdler, S. An evaluation of the overall utility of measures of functioning suitable for school-aged children on the autism spectrum: A scoping review. Int. J. Environ. Res. Public Health 2022, 19, 14114. [Google Scholar] [CrossRef]
- Australian Bureau of Statistics. Australian Statistical Geography Standard (ASGS): Volume 5—Remoteness Structure, [1270.0.55.005]. July 2016. Available online: https://www.abs.gov.au/AUSSTATS/abs@.nsf/Lookup/1270.0.55.005Main+Features1July%202016?OpenDocument (accessed on 30 September 2022).
- Australian Bureau of Statistics. Census of Population and Housing: Socio-Economic Indexes for Areas (SEIFA), Australia, [2033.0.55.001]. 2016. Available online: https://www.abs.gov.au/ausstats/abs@.nsf/Lookup/by%20Subject/2033.0.55.001~2016~Main%20Features~IRSAD~20 (accessed on 30 September 2022).
- IBM Corp. IBM SPSS Statistics for Windows, Version 27.0; IBM Corp.: Armonk, NY, USA, 2020.
- QSR International. NVivo, Version 12; QSR International: Doncaster, Australia, 2020.
- Krefting, L. Rigor in qualitative research: The assessment of trustworthiness. Am. J. Occup. Ther. 1991, 45, 214–222. [Google Scholar] [CrossRef]
- McCaffrey, N.; Kaambwa, B.; Currow, D.; Ratcliffe, J. Health-related quality of life measured using the EQ-5D–5L: South Australian population norms. Health Qual. Life Outcomes 2016, 14, 133. [Google Scholar] [CrossRef]
- Australian Unity. Australian Unity Wellbeing Index: Commemorative Report; Deakin University: Melbourne, Australia, 2021. [Google Scholar]
- Steinhausen, H.; Mohr Jensen, C.; Lauritsen, M. A systematic review and meta-analysis of the long-term overall outcome of autism spectrum disorders in adolescence and adulthood. Acta Psychiatr. Scand. 2016, 133, 445–452. [Google Scholar] [CrossRef]
- Mason, D.; Capp, S.; Stewart, G.; Kempton, M.; Glaser, K.; Howlin, P.; Happé, F. A meta-analysis of outcome studies of autistic adults: Quantifying effect size, quality, and meta-regression. J. Autism Dev. Disord. 2021, 51, 3165–3179. [Google Scholar] [CrossRef]
- D’Arcy, E.; Burnett, T.; Capstick, E.; Elder, C.; Slee, O.; Girdler, S.; Scott, M.; Milbourn, B. The well-being and support needs of Australian caregivers of neurodiverse children. J. Autism Dev. Disord. 2022; under review. [Google Scholar]
- MacKenzie, K.; Eack, S. Interventions to improve outcomes for parents of children with autism spectrum disorder: A meta-analysis. J. Autism Dev. Disord. 2022, 52, 2859–2883. [Google Scholar] [CrossRef]
- Taylor, J.; Hodapp, R.; Burke, M.; Waitz-Kudla, S.; Rabideau, C. Training parents of youth with autism spectrum disorder to advocate for adult disability services: Results from a pilot randomized controlled trial. J. Autism Dev. Disord. 2017, 47, 846–857. [Google Scholar] [CrossRef]
- Jonsson, U.; Coco, C.; Fridell, A.; Brown, S.; Berggren, S.; Hirvikoski, T.; Bölte, S. Proof of concept: The TRANSITION program for young adults with autism spectrum disorder and/or attention deficit hyperactivity disorder. Scand. J. Occup. Ther. 2021, 28, 78–90. [Google Scholar] [CrossRef]
- American Occupational Therapy Association. Occupational therapy practice framework: Domain and process (3rd ed.). Am. J. Occup. Ther. 2020, 74 (Suppl. 2), 7412410010p1–7412410010p87. [Google Scholar] [CrossRef]
- Woodman, J.; Simon, A.; Hauari, H.; Gilbert, R. A scoping review of ‘think-family’approaches in healthcare settings. J. Public Health 2020, 42, 21–37. [Google Scholar] [CrossRef]
- Chamberlain, A.; D’Arcy, E.; Whitehouse, A.; Wallace, K.; Hayden-Evans, M.; Girdler, S.; Milbourn, B.; Bölte, S.; Evans, K. Reliability, validity and acceptability of the PEDI-CAT with ASD scales for Australian children and youth on the autism spectrum. J. Autism Dev. Disord. 2022; under review. [Google Scholar]
- D’Arcy, E.; Evans, K.; Afsharnejad, B.; Milbourn, B.; Whitehouse, A.; Bölte, S.; Girdler, S. Australian clinicians when choosing an assessment of functioning tool for children with neurodevelopmental conditions. Adv. Neurodev. Disord. 2022. [Google Scholar] [CrossRef]
- World Health Organization. Framework for Action on Interprofessional Education and Collaborative Practice; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- Portney, L.; Watkins, M. Foundations of Clinical Research: Applications to Practice, 3rd ed.; F.A. Davis Company: Philadelphia, PA, USA, 2015. [Google Scholar]
- Whitehouse, A.; Varcin, K.; Waddington, H.; Sulek, R.; Bent, C.; Ashburner, J.; Eapen, V.; Goodall, E.; Hudry, K.; Roberts, J. Interventions for Children on the Autism Spectrum: A Synthesis of Research Evidence; Autism CRC: Brisbane, Australia, 2021. [Google Scholar]
- Novak, I.; McIntyre, S. The effect of education with workplace supports on practitioners’ evidence-based practice knowledge and implementation behaviours. Aust. Occup. Ther. J. 2010, 57, 386–393. [Google Scholar] [CrossRef] [PubMed]
- McColl, M.; Paterson, M.; Davies, D.; Doubt, L.; Law, M. Validity and community utility of the Canadian Occupational Performance Measure. Can. J. Occup. Ther. 2000, 67, 22–30. [Google Scholar] [CrossRef] [PubMed]
- Steenbeek, D.; Ketelaar, M.; Galama, K.; Gorter, J. Goal attainment scaling in paediatric rehabilitation: A critical review of the literature. Dev. Med. Child Neurol. 2007, 49, 550–556. [Google Scholar] [CrossRef]
- Thompson, C.; Falkmer, T.; Evans, K.; Bölte, S.; Girdler, S. A realist evaluation of peer mentoring support for university students with autism. Br. J. Spec. Educ. 2018, 45, 412–434. [Google Scholar] [CrossRef]
- Willis, C.; Reid, S.; Elliott, C.; Rosenberg, M.; Nyquist, A.; Jahnsen, R.; Girdler, S. A realist evaluation of a physical activity participation intervention for children and youth with disabilities: What works, for whom, in what circumstances, and how? BMC Pediatr. 2018, 18, 113. [Google Scholar] [CrossRef]
- Afsharnejad, B.; Falkmer, M.; Black, M.; Alach, T.; Lenhard, F.; Fridell, A.; Coco, C.; Milne, K.; Bölte, S.; Girdler, S. KONTAKT® social skills group training for Australian adolescents with autism spectrum disorder: A randomized controlled trial. Eur. Child Adolesc. Psychiatry 2022, 31, 1695–1713. [Google Scholar] [CrossRef]
- Tugwell, P.; Kelly, M.; Noyes, J.; Kane, R.; Chang, C.; Uhl, S.; Robinson, K.; Springs, S.; Butler, M.; Guise, J. AHRQ Series on complex intervention systematic reviews—Paper 1: An introduction to a series of articles that provide guidance and tools for reviews of complex interventions. J. Clin. Epidemiol. 2017, 90, 6–10. [Google Scholar] [CrossRef]
- Fletcher-Watson, S.; Brook, K.; Hallett, S.; Murray, F.; Crompton, C. Inclusive practices for neurodevelopmental research. Curr. Dev. Disord. Rep. 2021, 8, 88–97. [Google Scholar] [CrossRef]
- Graham, I.; McCutcheon, C.; Kothari, A. Exploring the frontiers of research co-production: The Integrated Knowledge Translation Research Network concept papers. Health Res. Policy Syst. 2019, 17, 88. [Google Scholar] [CrossRef]
- D’Arcy, E.; Evans, K.; Afsharnejad, B.; Milbourn, B.; Bölte, S.; Girdler, S. Assessing functioning for individuals with neurodevelopmental conditions: Current clinical practice in Australia. Aust. Occup. Ther. J. 2022, 1–18. [Google Scholar] [CrossRef]
- Khetani, M.; Coster, W.; Law, M.; Bedell, G. Young Children’s Partcipation and Environment Measure (YC-PEM): User Guide; CanChild, McMaster University: Hamilton, ON, Canada, 2013. [Google Scholar]
- Coster, W.; Law, M.; Bedell, G. Partcipation and Environment Measure for Children and Youth (PEM-CY): Form & User’s Guide; CanChild, McMaster University: Hamilton, ON, Canada, 2010. [Google Scholar]
- McGrath, R. The VIA Assessment Suite for Adults: Development and Initial Evaluation—Technical Report; VIA Institute on Character: Cincinnati, OH, USA, 2019. [Google Scholar]
- Beach Center on Disability. Beach Center Family Quality of Life Scale: Psychometric Characteristics and Scoring Key; University of Kansas: Lawrence, KS, USA, 2015. [Google Scholar]
- Haley, S.; Coster, W.; Dumas, H.; Fragala-Pinkham, M.; Moed, R.; Kramer, J.; Ni, P.; Feng, T.; Kao, Y.; Ludlow, L. Pediatric Evaluation of Disability Inventory: Development, Standardization and Administration Manual (Version 1.4.3); Boston University: Boston, MA, USA, 2019. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Demographic and Clinical Characteristics | M (SD) | n (%) |
|---|---|---|
| Young People | ||
| Age (years) | 10.82 (3.09) | |
| Gender | ||
| Male | 42 (61.76) | |
| Female | 26 (38.24) | |
| School Level | ||
| Lower primary (pre-primary to Year 3) | 25 (36.76) | |
| Upper primary (year 4 to 6) | 20 (29.41) | |
| Lower secondary (year 7 to 9) | 17 (25.00) | |
| Upper secondary (year 10 to 12) | 6 (8.82) | |
| Autism Diagnosis | ||
| Autism Spectrum Disorder | 57 (83.82) | |
| SCI Level 1 | 21 (38.89) | |
| SCI Level 2 | 25 (46.30) | |
| SCI Level 3 | 8 (14.81) | |
| RRB Level 1 | 26 (48.15) | |
| RRB Level 2 | 22 (40.74) | |
| RRB Level 3 | 6 (11.11) | |
| Asperger’s Syndrome | 2 (2.94) | |
| Autistic Disorder | 8 (11.76) | |
| Not Specified | 1 (1.47) | |
| Age of Initial Autism Diagnosis (years) | 5.70 (2.94) | |
| Autistic Signs and Symptoms (AMSE ≥ 5 threshold) | 5.12 (2.39) | 45 (68.18) |
| Co-Occurring Diagnosis | ||
| Attention Deficit/Hyperactivity Disorder | 25 (36.76) | |
| Communication Disorder | 13 (19.12) | |
| Global Developmental and/or Motor disorder | 12 (17.65) | |
| Intellectual disability | 15 (22.06) | |
| Vineland-3 | ||
| Adaptive Behavior Composite | 65.55 (14.76) | |
| Communication | 64.82 (18.60) | |
| Daily living skills | 71.36 (20.06) | |
| Socialization | 62.49 (17.61) | |
| Motor skills | 79.97 (18.43) | |
| Maladaptive Behavior (Internalizing) | 21.55 (1.61) | |
| Maladaptive Behavior (Externalizing) | 19.36 (2.50) | |
| Caregivers | ||
| Age (years) | 42.77 (7.52) | |
| Gender | ||
| Male | 3 (4.29) | |
| Female | 67 (95.71) | |
| Relationship | ||
| Parent | 66 (98.51) | |
| Grandparent | 1 (1.49) | |
| Health and Wellbeing 1 | ||
| EQ-5D-5L Visual Analogue Scale | 67.81 (19.39) | |
| Personal Wellbeing Index | 59.01 (22.73) | |
| Families | ||
| Family history of neurodevelopmental conditions | ||
| No | 31 (53.45) | |
| Yes | 27 (46.55) | |
| Cultural Diversity | ||
| First Nations 2 | 1 (1.52) | |
| Belongs to a specific cultural group 3 | 13 (19.12) | |
| Language other than English at home 4 | 8 (11.76) | |
| State Location | ||
| New South Wales | 14 (20.90) | |
| Queensland | 7 (10.45) | |
| Victoria | 25 (37.31) | |
| Western Australia | 21 (31.34) | |
| Geographical Location | ||
| Major city | 60 (89.55) | |
| Inner or outer regional center | 7 (10.45) |
| ICF Domain and Chapter | n (%) |
|---|---|
| Body Functions | 66 (97.06) |
| b1. Mental functions 1 | 66 (97.06) |
| b2. Sensory functions and pain | 30 (44.12) |
| b3. Voice and speech functions 2 | 1 (1.47) |
| b4. Functions of the cardiovascular, hematological, immunological and respiratory systems | 6 (8.82) |
| b5. Functions of the digestive, metabolic and endocrine systems | 5 (7.35) |
| b7. Neuromusculoskeletal and movement related functions | 26 (38.24) |
| Activities and Participation | 68 (100.00) |
| d1. Learning and applying knowledge | 54 (79.41) |
| d2. General tasks and demands | 44 (64.71) |
| d3. Communication | 49 (72.06) |
| d4. Mobility | 19 (27.94) |
| d5. Self-care | 46 (67.65) |
| d6. Domestic life | 43 (63.24) |
| d7. Interpersonal interactions and relationships | 64 (94.12) |
| d8. Major life areas | 61 (89.71) |
| d9. Community, social and civic life | 54 (79.41) |
| Environmental Factors | 68 (100.00) |
| e1. Products and technology | 45 (66.18) |
| e2. Natural environment and human-made changes to environment | 14 (20.59) |
| e3. Support and relationships | 68 (100.00) |
| e4. Attitude | 8 (11.76) |
| e5. Services, systems and policies | 59 (86.76) |
| Activity Category | Home | Community |
|---|---|---|
| Play | Backyard games Card games Electronic device games | Riding bicycle or walking in neighborhood Visiting playgrounds Swimming in public pools Play dates |
| Hobbies | Listening to music Making crafts Telling stories | Outing to shopping centers Watching a movie at the cinema Interest based classes (e.g., art, drama, music) |
| Sports | Backyard sports (e.g., shooting basketball goals) | Group lessons (e.g., ballet, gymnastics, swimming, taekwondo, yoga) Team sports (e.g., soccer, tennis) Autism or disability specific sports program |
| Informal associations | Not applicable | Youth clubs (e.g., Scouts) Activity based social skills groups (e.g., coding, cooking, Lego, Minecraft, theatre, writing) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Evans, K.; Whitehouse, A.J.O.; D’Arcy, E.; Hayden-Evans, M.; Wallace, K.; Kuzminski, R.; Thorpe, R.; Girdler, S.; Milbourn, B.; Bölte, S.; et al. Perceived Support Needs of School-Aged Young People on the Autism Spectrum and Their Caregivers. Int. J. Environ. Res. Public Health 2022, 19, 15605. https://doi.org/10.3390/ijerph192315605
Evans K, Whitehouse AJO, D’Arcy E, Hayden-Evans M, Wallace K, Kuzminski R, Thorpe R, Girdler S, Milbourn B, Bölte S, et al. Perceived Support Needs of School-Aged Young People on the Autism Spectrum and Their Caregivers. International Journal of Environmental Research and Public Health. 2022; 19(23):15605. https://doi.org/10.3390/ijerph192315605
Chicago/Turabian StyleEvans, Kiah, Andrew J. O. Whitehouse, Emily D’Arcy, Maya Hayden-Evans, Kerry Wallace, Rebecca Kuzminski, Rebecca Thorpe, Sonya Girdler, Benjamin Milbourn, Sven Bölte, and et al. 2022. "Perceived Support Needs of School-Aged Young People on the Autism Spectrum and Their Caregivers" International Journal of Environmental Research and Public Health 19, no. 23: 15605. https://doi.org/10.3390/ijerph192315605
APA StyleEvans, K., Whitehouse, A. J. O., D’Arcy, E., Hayden-Evans, M., Wallace, K., Kuzminski, R., Thorpe, R., Girdler, S., Milbourn, B., Bölte, S., & Chamberlain, A. (2022). Perceived Support Needs of School-Aged Young People on the Autism Spectrum and Their Caregivers. International Journal of Environmental Research and Public Health, 19(23), 15605. https://doi.org/10.3390/ijerph192315605