
Obesity, Diabetes, and Cardiovascular Risk Burden in Systemic Lupus Erythematosus: Current Approaches and Knowledge Gaps—A Rapid Scoping Review

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Protocol and Registration
2.2. Eligibility Criteria
2.3. Information Sources
2.4. Search Strategy
2.5. Selection of Sources of Evidence
2.6. Data Charting Process
2.7. Synthesis of Results
3. Results
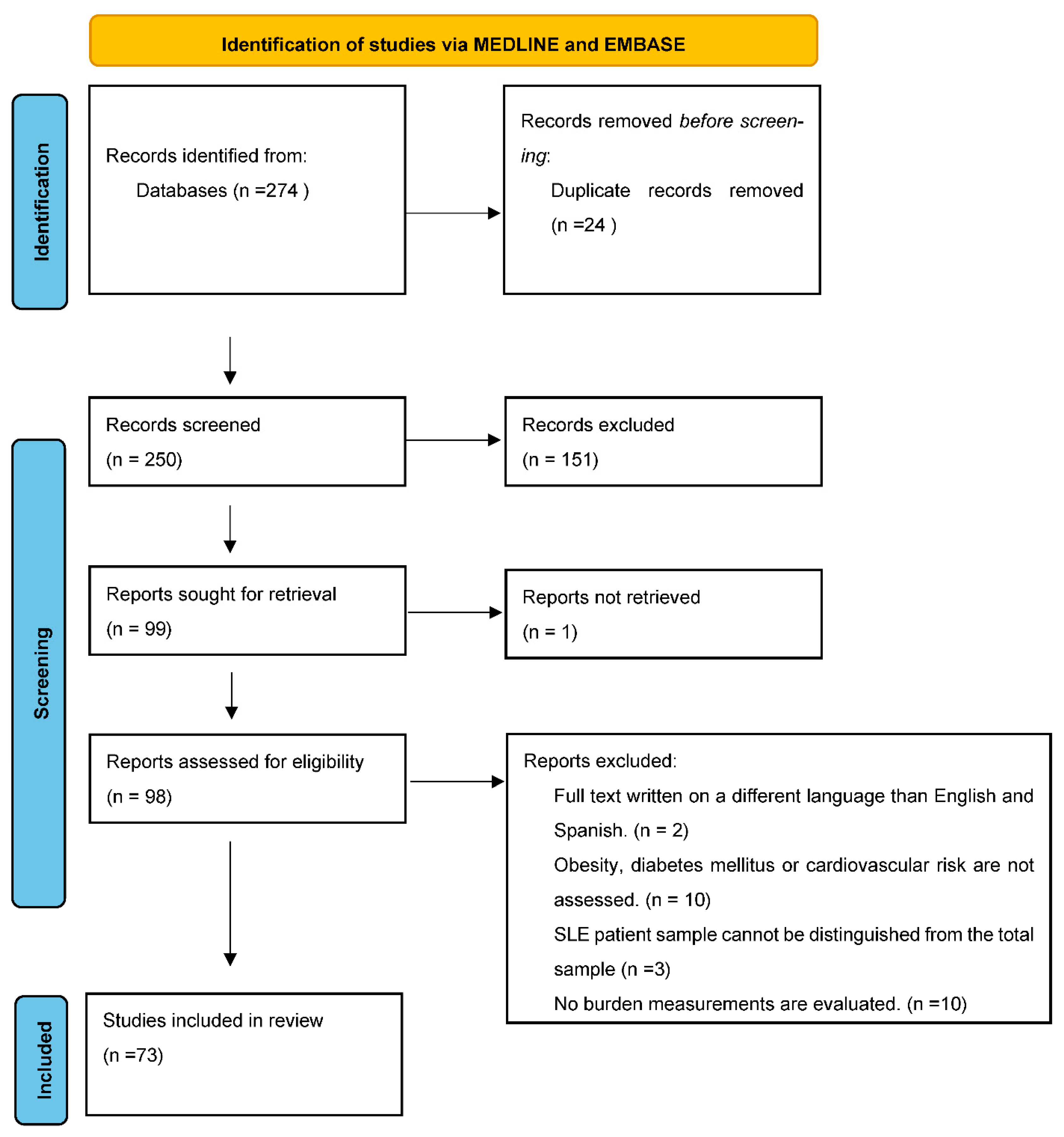
3.1. Selection of Sources of Evidence
3.2. Characteristics of Sources of Evidence
3.3. Results of Individual Sources of Evidence
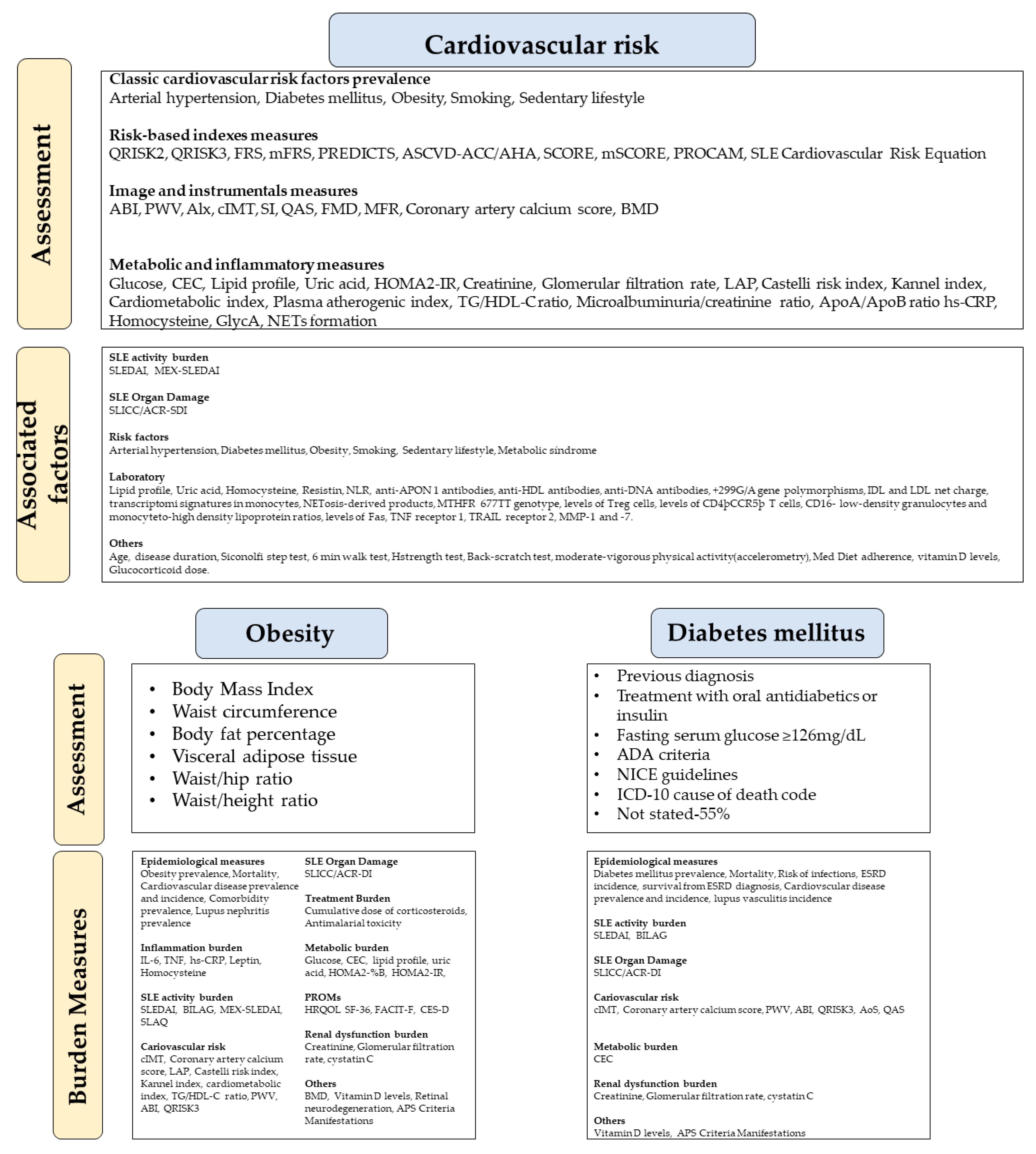
3.4. Synthesis of Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lee, Y.H.; Choi, S.J.; Ji, J.D.; Song, G.G. Overall and cause-specific mortality in systemic lupus erythematosus: An updated meta-analysis. Lupus 2016, 25, 727–734. [Google Scholar] [CrossRef] [PubMed]
- Conrad, N.; Verbeke, G.; Molenberghs, G.; Goetschalckx, L.; Callender, T.; Cambridge, G.; Mason, J.C.; Rahimi, K.; McMurray, J.J.V.; Verbakel, J.Y. Autoimmune diseases and cardiovascular risk: A population-based study on 19 autoimmune diseases and 12 cardiovascular diseases in 22 million individuals in the UK. Lancet 2022, 400, 733–743. [Google Scholar] [CrossRef]
- Romero-Díaz, J.; Acosta-Hernández, R.I.; Criales-Vera, S.; Kimura-Hayama, E.; Domínguez-Quintana, M.; Morán-Contla, R.; Núñez-Alvarez, C.; Lara-Reyes, P.; Aguilar-Salinas, C.; Sánchez-Guerrero, J. Asymptomatic Coronary Artery Calcifications in Men with Systemic Lupus Erythematosus. J. Rheumatol. 2018, 45, 663–670. [Google Scholar] [CrossRef] [PubMed]
- Andrades, C.; Fuego, C.; Manrique-Arija, S.; Fernandez-Nebro, A. Management of cardiovascular risk in systemic lupus erythematosus: A systematic review. Lupus 2017, 26, 1407–1419. [Google Scholar] [CrossRef] [PubMed]
- Fanouriakis, A.; Kostopoulou, M.; Alunno, A.; Aringer, M.; Bajema, I.; Boletis, J.; Cervera, R.; Doria, A.; Gordon, C.; Govoni, M.; et al. 2019 update of the EULAR recommendations for the management of systemic lupus erythematosus. Ann. Rheum. Dis. 2019, 78, 736–745. [Google Scholar] [CrossRef] [PubMed]
- Drosos, G.C.; Vedder, D.; Houben, E.; Boekel, L.; Atzeni, F.; Badreh, S.; Boumpas, D.T.; Brodin, N.; Bruce, I.N.; González-Gay, M.; et al. EULAR recommendations for cardiovascular risk management in rheumatic and musculoskeletal diseases, including systemic lupus erythematosus and antiphospholipid syndrome. Ann. Rheum. Dis 2022, 81, 768–779. [Google Scholar] [CrossRef]
- Gwinnutt, J.M.; Wieczorek, M.; Balanescu, A.; Bischoff-Ferrari, H.A.; Boonen, A.; Cavalli, G.; de Souza, S.; de Thurah, A.; Dorner, T.E.; Moe, R.H.; et al. 2021 EULAR recommendations regarding lifestyle behaviours and work participation to prevent progression of rheumatic and musculoskeletal diseases. Ann. Rheum. Dis. 2022. [Google Scholar] [CrossRef]
- Versini, M.; Jeandel, P.Y.; Rosenthal, E.; Shoenfeld, Y. Obesity in autoimmune diseases: Not a passive bystander. Autoimmun. Rev. 2014, 13, 981–1000. [Google Scholar] [CrossRef]
- Henrot, P.; Foret, J.; Barnetche, T.; Lazaro, E.; Duffau, P.; Seneschal, J.; Schaeverbeke, T.; Truchetet, M.-E.; Richez, C. Assessment of subclinical atherosclerosis in systemic lupus erythematosus: A systematic review and meta-analysis. Jt. Bone Spine 2018, 85, 155–163. [Google Scholar] [CrossRef]
- Lu, X.; Wang, Y.; Zhang, J.; Pu, D.; Hu, N.; Luo, J.; An, Q.; He, L. Patients with systemic lupus erythematosus face a high risk of cardiovascular disease: A systematic review and Meta-analysis. Int. Immunopharmacol. 2021, 94, 107466. [Google Scholar] [CrossRef]
- Restivo, V.; Candiloro, S.; Daidone, M.; Norrito, R.; Cataldi, M.; Minutolo, G.; Caracci, F.; Fasano, S.; Ciccia, F.; Casuccio, A.; et al. Systematic review and meta-analysis of cardiovascular risk in rheumatological disease: Symptomatic and non-symptomatic events in rheumatoid arthritis and systemic lupus erythematosus. Autoimmun. Rev. 2022, 21, 102925. [Google Scholar] [CrossRef] [PubMed]
- Vazquez-Del Mercado, M.; Perez-Vazquez, F.J.; Gomez-Banuelos, E.; Chavarria-Avila, E.; Llamas-Garcia, A.; Arrona-Rios, K.I.; Diaz-Rubio, G.I.; Durán-Barragán, S.; Navarro-Hernández, R.E.; Jordán-Estrada, B.P.; et al. Subclinical parameters of arterial stiffness and arteriosclerosis correlate with QRISK3 in systemic lupus erythematosus. PLoS ONE 2018, 13, e0207520. [Google Scholar] [CrossRef] [PubMed]
- Drosos, G.C.; Konstantonis, G.; Sfikakis, P.P.; Tektonidou, M.G. Underperformance of clinical risk scores in identifying vascular ultrasound-based high cardiovascular risk in systemic lupus erythematosus. Eur. J. Prev. Cardiol. 2020, 28, 346–352. [Google Scholar] [CrossRef] [PubMed]
- Sivakumaran, J.; Harvey, P.; Omar, A.; Tayer-Shifman, O.; Urowitz, M.B.; Gladman, D.D.; Anderson, N.; Su, J.; Touma, Z. Assessment of cardiovascular risk tools as predictors of cardiovascular disease events in systemic lupus erythematosus. Lupus Sci. Med. 2021, 8, e000448. [Google Scholar] [CrossRef]
- Teh, P.; Zakhary, B.; Sandhu, V.K. The impact of obesity on SLE disease activity: Findings from the Southern California Lupus Registry (SCOLR). Clin. Rheumatol. 2019, 38, 597–600. [Google Scholar] [CrossRef] [PubMed]
- Peters, M.D.J.; Godfrey, C.; McInerney, P.; Munn, Z.; Tricco, A.C.; Khalil, H. Chapter 11: Scoping Reviews (2020 version). In JBI Manual for Evidence Synthesis; Aromataris, E., Munn, Z., Eds.; JJBI: Adelaide, Australia, 2020; Available online: https://synthesismanual.jbi.global (accessed on 20 January 2022).
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef]
- Chew, C.; Reynolds, J.A.; Lertratanakul, A.; Wu, P.; Urowitz, M.; Gladman, D.D.; Fortin, P.R.; Bae, S.-C.; Gordon, C.; Clarke, A.E.; et al. Lower vitamin D is associated with metabolic syndrome and insulin resistance in systemic lupus: Data from an international inception cohort. Rheumatology 2021, 60, 4737–4747. [Google Scholar] [CrossRef]
- Patterson, S.L.; Schmajuk, G.; Jafri, K.; Yazdany, J.; Katz, P. Obesity is Independently Associated with Worse Patient-Reported Outcomes in Women with Systemic Lupus Erythematosus. Arthritis Care Res. 2019, 71, 126–133. [Google Scholar] [CrossRef]
- Li, Z.; Shang, J.; Zeng, S.; Wu, H.; Zhou, Y.; Xu, H. Altered body composition and increased visceral adipose tissue in premenopausal and late postmenopausal patients with SLE. Clin. Rheumatol. 2019, 38, 3117–3127. [Google Scholar] [CrossRef]
- Baragetti, A.; Ramirez, G.; Magnoni, M.; Garlaschelli, K.; Grigore, L.; Berteotti, M.; Scotti, I.; Bozzolo, E.; Berti, A.; Camici, P.; et al. Disease trends over time and CD4 + CCR5 + T-cells expansion predict carotid atherosclerosis development in patients with systemic lupus erythematosus. Nutr. Metab. Cardiovasc. Dis. 2018, 28, 53–63. [Google Scholar] [CrossRef]
- Wigren, M.; Svenungsson, E.; Mattisson, I.Y.; Gustafsson, J.T.; Gunnarsson, I.; Zickert, A.; Elvin, K.; Jensen-Urstad, K.; Bengtsson, A.; Gullstrand, B.; et al. Cardiovascular disease in systemic lupus erythematosus is associated with increased levels of biomarkers reflecting receptor-activated apoptosis. Atherosclerosis 2018, 270, 1–7. [Google Scholar] [CrossRef]
- López, P.; Rodríguez-Carrio, J.; Martínez-Zapico, A.; Pérez-Álvarez, Á.I.; Suárez-Díaz, S.; Mozo, L.; Benavente, L.; Caminal-Montero, L.; Suárez, A. Low-density granulocytes and monocytes as biomarkers of cardiovascular risk in systemic lupus erythematosus. Rheumatology 2020, 59, 1752–1764. [Google Scholar] [CrossRef] [PubMed]
- Casey, K.A.; Smith, M.A.; Sinibaldi, D.; Seto, N.L.; Playford, M.P.; Wang, X.; Carlucci, P.M.; Wang, L.; Illei, G.; Yu, B.; et al. Modulation of Cardiometabolic Disease Markers by Type I Interferon Inhibition in Systemic Lupus Erythematosus. Arthritis Rheumatol. 2021, 73, 459–471. [Google Scholar] [CrossRef] [PubMed]
- Bortoluzzi, A.; Chighizola, C.B.; Fredi, M.; Raschi, E.; Bodio, C.; Privitera, D.; Gonelli, A.; Silvagni, E.; Govoni, M.; Cavazzana, I.; et al. The IMMENSE Study: The Interplay between iMMune and ENdothelial Cells in Mediating Cardiovascular Risk in Systemic Lupus Erythematosus. Front. Immunol. 2020, 11, 572876. [Google Scholar] [CrossRef] [PubMed]
- Zhu, L.; Singh, M.; Lele, S.; Sahakian, L.; Grossman, J.; Hahn, B.; McMahon, M. Assessing the validity of QRISK3 in predicting cardiovascular events in systemic lupus erythematosus. Lupus Sci. Med. 2022, 9, e000564. [Google Scholar] [CrossRef] [PubMed]
- Jafri, K.; Ogdie, A.; Qasim, A.; Patterson, S.L.; Gianfrancesco, M.; Izadi, Z.; Katz, P.; Yazdany, J.; Schmajuk, G. Discordance of the Framingham cardiovascular risk score and the 2013 American College of Cardiology/American Heart Association risk score in systemic lupus erythematosus and rheumatoid arthritis. Clin. Rheumatol. 2018, 37, 467–474. [Google Scholar] [CrossRef]
- Borg, A.; Gomez, A.; Cederlund, A.; Cobar, F.; Qiu, V.; Lindblom, J.; Emamikia, S.; Enman, Y.; Pettersson, S.; Parodis, I. Contribution of abnormal BMI to adverse health-related quality of life outcomes after a 52-week therapy in patients with SLE. Rheumatology 2021, 60, 4205–4217. [Google Scholar] [CrossRef]
- Sola-Rodríguez, S.; Gavilán-Carrera, B.; Vargas-Hitos, J.A.; Sabio, J.M.; Morillas-De-Laguno, P.; Soriano-Maldonado, A. Physical Fitness and Body Composition in Women with Systemic Lupus Erythematosus. Medicina 2019, 55, 57. [Google Scholar] [CrossRef]
- Sola-Rodríguez, S.; Vargas-Hitos, J.A.; Gavilán-Carrera, B.; Rosales-Castillo, A.; Ríos-Fernández, R.; Sabio, J.M.; Soriano-Maldonado, A. Physical Fitness Attenuates the Impact of Higher Body Mass and Adiposity on Inflammation in Women with Systemic Lupus Erythematosus. Front. Immunol. 2021, 12, 729672. [Google Scholar] [CrossRef]
- Sola-Rodríguez, S.; Vargas-Hitos, J.; Gavilán-Carrera, B.; Rosales-Castillo, A.; Sabio, J.; Hernández-Martínez, A.; Martínez-Rosales, E.; Ortego-Centeno, N.; Soriano-Maldonado, A. Relative Handgrip Strength as Marker of Cardiometabolic Risk in Women with Systemic Lupus Erythematosus. Int. J. Environ. Res. Public Health 2021, 18, 4630. [Google Scholar] [CrossRef]
- Legge, A.; Blanchard, C.; Hanly, J.G. Physical activity, sedentary behaviour and their associations with cardiovascular risk in systemic lupus erythematosus. Rheumatology 2020, 59, 1128–1136. [Google Scholar] [CrossRef] [PubMed]
- Tziomalos, K.; Gkougkourelas, I.; Sarantopoulos, A.; Bekiari, E.; Makri, E.; Raptis, N.; Tselios, K.; Pantoura, M.; Hatzitolios, A.I.; Boura, P. Arterial stiffness and peripheral arterial disease in patients with systemic lupus erythematosus. Rheumatol. Int. 2017, 37, 293–298. [Google Scholar] [CrossRef] [PubMed]
- Di Battista, M.; Tani, C.; Elefante, E.; Chimera, D.; Carli, L.; Ferro, F.; Stagnaro, C.; Mosca, M. Framingham, ACC/AHA or QRISK3: Which is the best in systemic lupus erythematosus cardiovascular risk estimation? Clin. Exp. Rheumatol. 2020, 38, 602–608. [Google Scholar]
- Garcia-Garcia, P.; Castejon, R.; Tutor-Ureta, P.; Silvestre, R.A.; Mellor-Pita, S.; Jimenez-Ortiz, C.; Yebra-Bango, M. Serum cystatin C is associated with kidney function but not with cardiovascular risk factors or subclinical atherosclerosis in patients with Systemic Lupus Erythematosus. Clin. Rheumatol. 2017, 36, 2709–2717. [Google Scholar] [CrossRef] [PubMed]
- Ammar, W.; Taha, M.; Baligh, E.; Osama, D. Assessment of vascular stiffness using different modalities in patients with systemic lupus erythematosus: A case control study. Egypt. Heart J. 2020, 72, 24. [Google Scholar] [CrossRef]
- Shaaban, A.; Helmy, M.; Barakat, M.; Elneily, D.; Ahmed, O. Serum resistin, insulin resistance and carotid intima-media thickness as an indication of subclinical atherosclerosis in systemic lupus erythematosus patients. Egypt. Rheumatol. 2021, 43, 319–323. [Google Scholar] [CrossRef]
- Sánchez-Pérez, H.; Tejera-Segura, B.; De Vera-González, A.; Delgado, A.G.; Olmos, J.M.; Hernandez, J.L.; Corrales, A.; López-Mejías, R.; González-Gay, M.A.; Ferraz-Amaro, I. Insulin resistance in systemic lupus erythematosus patients: Contributing factors and relationship with subclinical atherosclerosis. Clin. Exp. Rheumatol. 2017, 35, 885–892. [Google Scholar]
- Pesqueda-Cendejas, K.; Parra-Rojas, I.; Mora-García, P.E.; Montoya-Buelna, M.; Ruiz-Ballesteros, A.I.; Meza-Meza, M.R.; Campos-López, B.; Rivera-Escoto, M.; Vizmanos-Lamotte, B.; Cerpa-Cruz, S.; et al. CRP Serum Levels Are Associated with High Cardiometabolic Risk and Clinical Disease Activity in Systemic Lupus Erythematosus Patients. J. Clin. Med. 2022, 11, 1849. [Google Scholar] [CrossRef]
- Čypienė, A.; Dadonienė, J.; Miltinienė, D.; Rinkūnienė, E.; Rugienė, R.; Stropuvienė, S.; Badarienė, J.; Laucevičius, A. The fact not to ignore: Mean blood pressure is the main predictor of increased arterial stiffness in patients with systemic rheumatic diseases. Adv. Med Sci. 2017, 62, 223–229. [Google Scholar] [CrossRef]
- López, P.; Rodríguez-Carrio, J.; Martínez-Zapico, A.; Pérez-Álvarez, Á.I.; López-Mejías, R.; Benavente, L.; Mozo, L.; Caminal-Montero, L.; González-Gay, M.A.; Suárez, A. Serum Levels of Anti-PON1 and Anti-HDL Antibodies as Potential Biomarkers of Premature Atherosclerosis in Systemic Lupus Erythematosus. Thromb. Haemost. 2017, 117, 2194–2206. [Google Scholar] [CrossRef]
- Rodríguez, M.; Guardiola, M.; Oliva, I.; Vallvé, J.C.; Ferré, R.; Masana, L.; Parra, S.; Ribalta, J.; Castro, A. Low-density lipoprotein net charge is a risk factor for atherosclerosis in lupus patients independent of lipid concentrations. Int. J. Rheum. Dis. 2019, 22, 480–487. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.-F.; Ding, F.-M.; Ye, Y.-C.; Zhang, S.-Y. Relationship between Neutrophil-to-Lymphocyte Ratio and Pulse Wave Velocity in Young Patients with Systemic Lupus Erythematosus. Chin. Med. J. 2018, 131, 10–15. [Google Scholar] [CrossRef] [PubMed]
- Giannelou, M.; Nezos, A.; Fragkioudaki, S.; Kasara, D.; Maselou, K.; Drakoulis, N.; Ioakeimidis, D.; Moutsopoulos, H.M.; Mavragani, C.P. Contribution of MTHFR gene variants in lupus related subclinical atherosclerosis. Clin. Immunol. 2018, 193, 110–117. [Google Scholar] [CrossRef] [PubMed]
- García-Carrasco, M.; Soto-Santillán, P.; Mendoza-Pinto, C.; González-Ramírez, R.; López-Carmona, A.L.; Munguía-Realpozo, P.; Etchegaray-Morales, I.; Méndez-Martínez, S.; Gálvez-Romero, J.L.; López-Colombo, A.; et al. The Role of Circulating Regulatory T Cell Levels on Subclinical Atherosclerosis and Cardiovascular Risk Factors in Women with Systemic Lupus Erythematosus. Mediat. Inflamm. 2018, 2018, 3271572. [Google Scholar] [CrossRef] [PubMed]
- Mellor-Pita, S.; Tutor-Ureta, P.; Rosado, S.; Alkadi, K.; Granado, F.; Jimenez-Ortiz, C.; Castejon, R. Calcium and vitamin D supplement intake may increase arterial stiffness in systemic lupus erythematosus patients. Clin. Rheumatol. 2019, 38, 1177–1186. [Google Scholar] [CrossRef]
- Quevedo-Abeledo, J.C.; Rúa-Figueroa, Í.; Sánchez-Pérez, H.; Tejera-Segura, B.; de Vera-González, A.; González-Delgado, A.; Llorca, J.; González-Gay, M.; Ferraz-Amaro, I. Disease Damage Influences Cardiovascular Risk Reclassification Based on Carotid Ultrasound in Patients with Systemic Lupus Erythematosus. J. Rheumatol. 2019, 46, 483–491. [Google Scholar] [CrossRef]
- Petri, M.A.; Barr, E.; Magder, L.S. Development of a systemic lupus erythematosus cardiovascular risk equation. Lupus Sci. Med. 2019, 6, e000346. [Google Scholar] [CrossRef]
- Przywara-Chowaniec, B.; Blachut, D.; Harpula, J.; Beres, M.; Nowak, A.; Nowalany-Kozielska, E. Systemic Lupus Erythematosus, Its Impact on Selected Cardiovascular Risk Factors, and Correlation with Duration of Illness: A Pilot Study. Cardiol. Res. Pract. 2020, 2020, 7025329. [Google Scholar] [CrossRef]
- Fernandez-Garces, M.; Haro, G.; Mico, M.L. Predisposing factors to nonfatal cardiovascular events in women with systemic lupus erythematosus. An observational, cross-sectional, multicenter study in Spain from the risk/systemic lupus erythematosus thematic network. Medicine 2019, 98, e17489. [Google Scholar] [CrossRef]
- Masson, W.; Rossi, E.; Mora-Crespo, L.M.; Cornejo-Peña, G.; Pessio, C.; Gago, M.; Alvarado, R.N.; Scolnik, M. Cardiovascular risk stratification and appropriate use of statins in patients with systemic lupus erythematosus according to different strategies. Clin. Rheumatol. 2020, 39, 455–462. [Google Scholar] [CrossRef]
- Salvetti, M.; Paini, A.; Andreoli, L.; Stassaldi, D.; Aggiusti, C.; Bertacchini, F.; Rosei, C.A.; Piantoni, S.; Franceschini, F.; Tincani, A.; et al. Cardiovascular target organ damage in premenopausal systemic lupus erythematosus patients and in controls: Are there any differences? Eur. J. Intern. Med. 2020, 73, 76–82. [Google Scholar] [CrossRef] [PubMed]
- Patiño-Trives, A.M.; Pérez-Sánchez, C.; Pérez-Sánchez, L.; Luque-Tévar, M.; Ábalos-Aguilera, M.C.; Alcaide-Ruggiero, L.; Arias-de la Rosa, I.; Román-Rodríguez, C.; Seguí, P.; Espinosa, M.; et al. Anti-dsDNA Antibodies Increase the Cardiovascular Risk in Systemic Lupus Erythematosus Promoting a Distinctive Immune and Vascular Activation. Arterioscler. Thromb. Vasc. Biol. 2021, 41, 2417–2430. [Google Scholar] [CrossRef] [PubMed]
- Weber, B.N.; Stevens, E.; Barrett, L.; Bay, C.; Sinnette, C.; Brown, J.M.; Divakaran, S.; Bibbo, C.; Hainer, J.; Dorbala, S.; et al. Coronary Microvascular Dysfunction in Systemic Lupus Erythematosus. J. Am. Heart Assoc. 2021, 10, e018555. [Google Scholar] [CrossRef]
- Campos-López, B.; Meza-Meza, M.R.; Parra-Rojas, I.; Ruiz-Ballesteros, A.I.; Vizmanos-Lamotte, B.; Muñoz-Valle, J.F.; Montoya-Buelna, M.; Cerpa-Cruz, S.; Bernal-Hernández, L.E.; De la Cruz-Mosso, U. Association of cardiometabolic risk status with clinical activity and damage in systemic lupus erythematosus patients: A cross-sectional study. Clin. Immunol. 2021, 222, 108637. [Google Scholar] [CrossRef] [PubMed]
- Croca, S.C.; Griffin, M.; Farinha, F.; Isenberg, D.A.; Nicolaides, A.; Rahman, A. Total plaque area and plaque echogenicity are novel measures of subclinical atherosclerosis in patients with systemic lupus erythematosus. Rheumatology 2021, 60, 4185–4198. [Google Scholar] [CrossRef]
- Correa-Rodríguez, M.; Pocovi-Gerardino, G.; Callejas-Rubio, J.-L.; Ríos-Fernández, R.; Martín-Amada, M.; Cruz-Caparrós, M.-G.; DelOlmo-Romero, S.; Ortego-Centeno, N.; Rueda-Medina, B. Vitamin D Levels are Associated with Disease Activity and Damage Accrual in Systemic Lupus Erythematosus Patients. Biol. Res. Nurs. 2021, 23, 455–463. [Google Scholar] [CrossRef] [PubMed]
- Fox, H.; Jung, O.; Bartel, C.; Hauser, I.A.; Ehrlich, J.R. Profile of cardiovascular risk factors in patients with systemic Lupus erythematosus: The CArdiovascular Risk Assessment STudy in Lupus erythematosus (CASTLE SLE) study. J. Fur Kardiol. 2018, 25, 128–134. [Google Scholar]
- Chandrashekara, S.; Dhote, S.V.; Anupama, K.R. The Differential Influence of Immunological Process of Autoimmune Disease on Lipid Metabolism: A Study on RA and SLE. Indian J. Clin. Biochem. 2019, 34, 52–59. [Google Scholar] [CrossRef]
- Rashad, N.M.; Allam, R.M.; Said, D.; Ali, A.E.; Mohy, N.M.; Abomandour, H.G. Influence of +299G>A and +62GEfA resistin gene promoter variants on cardiovascular risk in Egyptian women with systemic lupus erythematosus. Egypt. Rheumatol. 2019, 41, 215–220. [Google Scholar] [CrossRef]
- Quevedo-Abeledo, J.C.; Sánchez-Pérez, H.; Tejera-Segura, B.; Armas-Rillo, L.; Armas-González, E.; Machado, J.D.; González-Gay, M.A.; Díaz-González, F.; Ferraz-Amaro, I. Differences in Capacity of High-Density Lipoprotein Cholesterol Efflux between Patients with Systemic Lupus Erythematosus and Rheumatoid Arthritis. Arthritis Care Res. 2021, 73, 1590–1596. [Google Scholar] [CrossRef]
- Pocovi-Gerardino, G.; Correa-Rodríguez, M.; Callejas-Rubio, J.-L.; Ríos-Fernández, R.; Martín-Amada, M.; Cruz-Caparros, M.-G.; Rueda-Medina, B.; Ortego-Centeno, N. Beneficial effect of Mediterranean diet on disease activity and cardiovascular risk in systemic lupus erythematosus patients: A cross-sectional study. Rheumatology 2021, 60, 160–169. [Google Scholar] [CrossRef] [PubMed]
- Pocovi-Gerardino, G.; Correa-Rodríguez, M.; Rubio, J.-L.C.; Fernández, R.R.; Amada, M.M.; Caparros, M.-G.C.; Rueda-Medina, B.; Ortego-Centeno, N. The Relationships of High-Sensitivity C-Reactive Protein and Homocysteine Levels with Disease Activity, Damage Accrual, and Cardiovascular Risk in Systemic Lupus Erythematosus. Biol. Res. Nurs. 2020, 22, 169–177. [Google Scholar] [CrossRef]
- Sánchez-Pérez, H.; Quevedo-Abeledo, J.C.; de Armas-Rillo, L.; Rua--Figueroa, Í.; Tejera-Segura, B.; Armas-González, E.; Machado, J.D.; García-Dopico, J.A.; Jimenez-Sosa, A.; Rodríguez--Lozano, C.; et al. Impaired HDL cholesterol efflux capacity in systemic lupus erythematosus patients is related to subclinical carotid atherosclerosis. Rheumatology 2020, 59, 2847–2856. [Google Scholar] [CrossRef] [PubMed]
- Ajeganova, S.; Gustafsson, T.; Lindberg, L.; Hafstrom, I.; Frostegard, J. Similar progression of carotid intima-media thickness in 7-year surveillance of patients with mild SLE and controls, but this progression is still promoted by dyslipidaemia, lower HDL levels, hypertension, history of lupus nephritis and a higher prednisolone usage in patients. Lupus Sci. Med. 2020, 7, e000362. [Google Scholar] [PubMed]
- Jordan-Gonzalez, P.; Shum, L.M.; Gonzalez-Sepulveda, L.; Vila, L.M. Clinical correlates and outcomes in a group of Puerto Ricans with systemic lupus erythematosus hospitalized due to severe infections. SAGE Open Med. 2018, 6, 2050312118778385. [Google Scholar] [CrossRef]
- Chanloung, W.; Kasitanon, N.; Wichainun, R.; Louthrenoo, W. Thrombotic risk assessment in patients with systemic lupus erythematosus: Validation of the adjusted-Global Antiphospholipid Syndrome Score (aGAPSS) in Thai patients. Int. J. Rheum. Dis. 2021, 24, 1510–1519. [Google Scholar] [CrossRef]
- Jiang, M.Y.; Hwang, J.C.; Feng, I.J. Impact of Diabetes Mellitus on the Risk of End-Stage Renal Disease in Patients with Systemic Lupus Erythematosus. Sci. Rep. 2018, 8, 6008. [Google Scholar] [CrossRef]
- Gergianaki, I.; Garantziotis, P.; Adamichou, C.; Saridakis, I.; Spyrou, G.; Sidiropoulos, P.; Bertsias, G. High Comorbidity Burden in Patients with SLE: Data from the Community-Based Lupus Registry of Crete. J. Clin. Med. 2021, 10, 998. [Google Scholar] [CrossRef]
- Falasinnu, T.; Chaichian, Y.; Simard, J.F. Impact of Sex on Systemic Lupus Erythematosus-Related Causes of Premature Mortality in the United States. J. Women’s Health 2017, 26, 1214–1221. [Google Scholar] [CrossRef]
- Gamal, S.M.; Mohamed, S.S.; Tantawy, M.; Siam, I.; Soliman, A.; Niazy, M.H. Lupus-related vasculitis in a cohort of systemic lupus erythematosus patients. Arch. Rheumatol. 2021, 36, 595–692. [Google Scholar] [CrossRef]
- Alian, S.; Khalil, S.; Zaghlol, R. Charlson Comorbidity Index in patients with systemic lupus erythematosus in Egypt and its relation with disease characteristics. Indian J. Rheumatol. 2019, 14, 277–282. [Google Scholar] [CrossRef]
- Behiry, M.E.; Salem, M.R.; Alnaggar, A.R. Assessment of nutritional status and disease activity level in Systemic Lupus Erythematosus patients at a tertiary care hospital. Rev. Colomb. De Reumatol. 2019, 26, 97–104. [Google Scholar]
- Dias-Santos, A.; Ferreira, J.T.; Pinheiro, S.; Cunha, J.P.; Alves, M.; Papoila, A.L.; Moraes-Fontes, M.F.; Proença, R. Neurodegeneration in systemic lupus erythematosus: Layer by layer retinal study using optical coherence tomography. Int. J. Retin. Vitr. 2020, 6, 15. [Google Scholar] [CrossRef] [PubMed]
- Seguro, L.P.C.; Paupitz, J.A.; Caparbo, V.F.; Bonfa, E.; Pereira, R.M.R. Increased visceral adipose tissue and altered adiposity distribution in premenopausal lupus patients: Correlation with cardiovascular risk factors. Lupus 2018, 27, 1001–1006. [Google Scholar] [CrossRef] [PubMed]
- Tsyhanyk, L.; Abrahamovych, U.; Abrahamovych, O.; Chemes, V.; Guta, S. Bone Mineral Density and the Prevalence of Its Disorders in Patients with Systemic Lupus Erythematosus and Syntropic Comorbid Lesions. Georgian Med. News 2021, 103–108. [Google Scholar]
- Pedrosa, T.D.N.; Kupa, L.D.V.K.; Pasoto, S.G.; Aikawa, N.E.; Duarte, N.; Borba, E.F.; Bonfá, E.; Silva, C.A.A. The influence of obesity on hydroxychloroquine blood levels in lupus nephritis patients. Lupus 2021, 30, 554–559. [Google Scholar] [CrossRef]
- Apostolopoulos, D.; Vincent, F.; Hoi, A.; Morand, E. Associations of metabolic syndrome in SLE. Lupus Sci. Med. 2020, 7, e000436. [Google Scholar] [CrossRef]
- Gomez, A.; Butrus, F.H.; Johansson, P.; Åkerström, E.; Soukka, S.; Emamikia, S.; Enman, Y.; Pettersson, S.; Parodis, I. Impact of overweight and obesity on patient-reported health-related quality of life in systemic lupus erythematosus. Rheumatology 2021, 60, 1260–1272. [Google Scholar] [CrossRef]
- Kang, J.-H.; Xu, H.; Choi, S.-E.; Park, D.-J.; Lee, J.-K.; Kwok, S.-K.; Kim, S.-K.; Choe, J.-Y.; Kim, H.-A.; Sung, Y.-K.; et al. Obesity increases the incidence of new-onset lupus nephritis and organ damage during follow-up in patients with systemic lupus erythematosus. Lupus 2020, 29, 578–586. [Google Scholar] [CrossRef]
- Meza-Meza, M.R.; Vizmanos-Lamotte, B.; Muñoz-Valle, J.F.; Parra-Rojas, I.; Garaulet, M.; Campos-López, B.; Montoya-Buelna, M.; Cerpa-Cruz, S.; Martínez-López, E.; Oregon-Romero, E.; et al. Relationship of Excess Weight with Clinical Activity and Dietary Intake Deficiencies in Systemic Lupus Erythematosus Patients. Nutrients 2019, 11, 2683. [Google Scholar] [CrossRef]
- Hammam, N.; Rashad, S.M.; Mohamed, A.A.A. Metabolic syndrome in systemic lupus erythematosus patients: Relationship to disease activity and neuropsychiatric lupus. Z. Rheumatol. 2018, 77, 938–945. [Google Scholar] [CrossRef] [PubMed]
- Mak, A.; Kow, N.Y.; Schwarz, H.; Gong, L.; Tay, S.H.; Ling, L.H. Endothelial dysfunction in systemic lupus erythematosus—A case-control study and an updated meta-analysis and meta-regression. Sci. Rep. 2017, 7, 7320. [Google Scholar] [CrossRef] [PubMed]
- Tektonidou, M.G.; Kravvariti, E.; Konstantonis, G.; Tentolouris, N.; Sfikakis, P.P.; Protogerou, A. Subclinical atherosclerosis in Systemic Lupus Erythematosus: Comparable risk with Diabetes Mellitus and Rheumatoid Arthritis. Autoimmun. Rev. 2017, 16, 308–312. [Google Scholar] [CrossRef] [PubMed]
- Tsang, A.S.M.W.; Bultink, I.E.; Heslinga, M.; Voskuyl, A.E. Both prolonged remission and Lupus Low Disease Activity State are associated with reduced damage accrual in systemic lupus erythematosus. Rheumatology 2017, 56, 121–128. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Search | Query | Record Retrieved |
|---|---|---|
| #1 | ((“lupus erythematosus, systemic”[MeSH Terms] OR “lupus erythematosus systemic”[Title/Abstract]) AND (“Obesity”[MeSH Terms] OR “Obesity”[Title/Abstract])) AND ((humans[Filter]) AND (2017/1/1:2022/4/30[pdat]) AND (english[Filter] OR spanish[Filter]) AND (alladult[Filter])) | 43 |
| #2 | ((“lupus erythematosus, systemic”[MeSH Terms] OR “lupus erythematosus systemic”[Title/Abstract]) AND (“Diabetes Mellitus”[MeSH Terms] OR “Diabetes Mellitus”[Title/Abstract])) AND ((humans[Filter]) AND (2017/1/1:2022/4/30[pdat]) AND (english[Filter] OR spanish[Filter]) AND (alladult[Filter])) | 73 |
| #3 | ((“lupus erythematosus, systemic”[MeSH Terms] OR “lupus erythematosus systemic”[Title/Abstract]) AND “Cardiovascular Risk”[Title/Abstract]) AND ((humans[Filter]) AND (2017/1/1:2022/4/30[pdat]) AND (english[Filter] OR spanish[Filter]) AND (alladult[Filter])) | 103 |
| Study Characteristics | No of Studies | Study Characteristics | No of Studies |
|---|---|---|---|
| Year of Publication | Number of Participants | ||
| 2017 | 9 | <50 | 10 |
| 2018 | 13 | 50–100 | 22 |
| 2019 | 14 | 101–150 | 16 |
| 2020 | 16 | >150 | 25 |
| 2021 | 19 | ||
| 2022 * | 2 | ||
| Geographic region | Type of study reported by the authors | ||
| Europa | 37 | Cross-sectional | 37 |
| North America | 11 | Cohort | 10 |
| South America | 9 | Prospective cohort | 7 |
| Africa | 7 | Retrospective cohort | 3 |
| Asia | 7 | Case-control | 2 |
| Oceania | 1 | Clinical trial | 2 |
| Multi-site ** | 1 | Retrospective study | 2 |
| Setting | Prospective study | 1 | |
| Specialized hospital clinic | 67 | Not stated | 9 |
| Hospitalized patients | 1 | ||
| Population-based registries | 3 | ||
| Both clinical- and community-based sources | 2 | Time frame | |
| Percentage of women | <1 year | 8 | |
| <90 | 18 | 1–5 years | 28 |
| 90–100 | 54 | >5 years | 13 |
| Not stated | 1 | Not stated | 24 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hernández-Negrín, H.; Ricci, M.; Mancebo-Sevilla, J.J.; Sanz-Cánovas, J.; López-Sampalo, A.; Cobos-Palacios, L.; Romero-Gómez, C.; Pérez de Pedro, I.; Ayala-Gutiérrez, M.d.M.; Gómez-Huelgas, R.; et al. Obesity, Diabetes, and Cardiovascular Risk Burden in Systemic Lupus Erythematosus: Current Approaches and Knowledge Gaps—A Rapid Scoping Review. Int. J. Environ. Res. Public Health 2022, 19, 14768. https://doi.org/10.3390/ijerph192214768
Hernández-Negrín H, Ricci M, Mancebo-Sevilla JJ, Sanz-Cánovas J, López-Sampalo A, Cobos-Palacios L, Romero-Gómez C, Pérez de Pedro I, Ayala-Gutiérrez MdM, Gómez-Huelgas R, et al. Obesity, Diabetes, and Cardiovascular Risk Burden in Systemic Lupus Erythematosus: Current Approaches and Knowledge Gaps—A Rapid Scoping Review. International Journal of Environmental Research and Public Health. 2022; 19(22):14768. https://doi.org/10.3390/ijerph192214768
Chicago/Turabian StyleHernández-Negrín, Halbert, Michele Ricci, Juan José Mancebo-Sevilla, Jaime Sanz-Cánovas, Almudena López-Sampalo, Lidia Cobos-Palacios, Carlos Romero-Gómez, Iván Pérez de Pedro, María del Mar Ayala-Gutiérrez, Ricardo Gómez-Huelgas, and et al. 2022. "Obesity, Diabetes, and Cardiovascular Risk Burden in Systemic Lupus Erythematosus: Current Approaches and Knowledge Gaps—A Rapid Scoping Review" International Journal of Environmental Research and Public Health 19, no. 22: 14768. https://doi.org/10.3390/ijerph192214768
APA StyleHernández-Negrín, H., Ricci, M., Mancebo-Sevilla, J. J., Sanz-Cánovas, J., López-Sampalo, A., Cobos-Palacios, L., Romero-Gómez, C., Pérez de Pedro, I., Ayala-Gutiérrez, M. d. M., Gómez-Huelgas, R., & Bernal-López, M. R. (2022). Obesity, Diabetes, and Cardiovascular Risk Burden in Systemic Lupus Erythematosus: Current Approaches and Knowledge Gaps—A Rapid Scoping Review. International Journal of Environmental Research and Public Health, 19(22), 14768. https://doi.org/10.3390/ijerph192214768