
Differences in Free-Living Patterns of Sedentary Behaviour between Office Employees with Diabetes and Office Employees without Diabetes: A Principal Component Analysis for Clinical Practice

 , , ,
, , , 
Abstract
1. Background
2. Methods
2.1. Study Design
2.2. Setting
2.3. Variables and Data Measurement
2.4. Sample Size
2.5. Statistical Methods
3. Results
3.1. Description of the Participants in Patterns of Physical Activity and SB: Differences between T2D and NGM
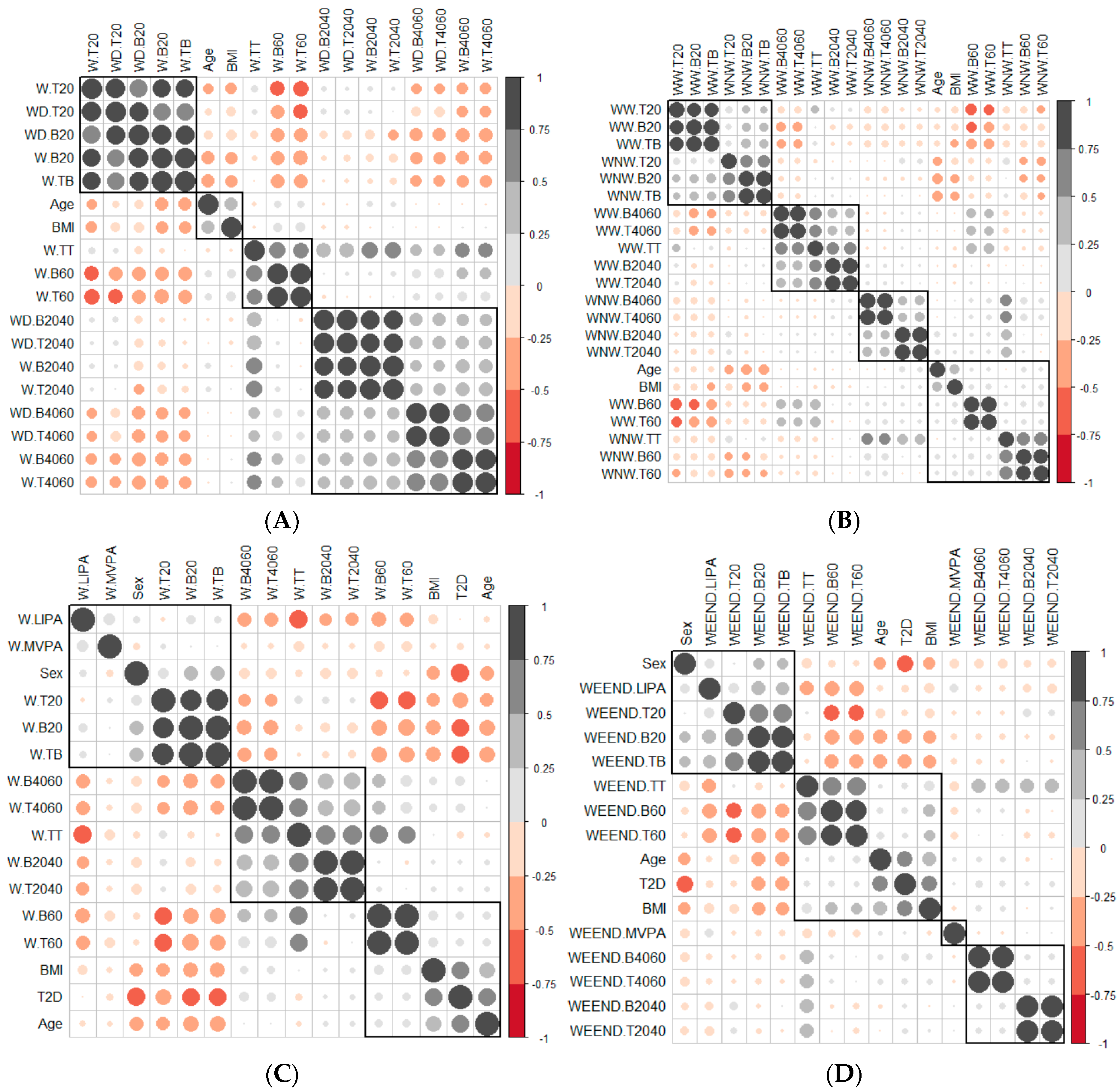
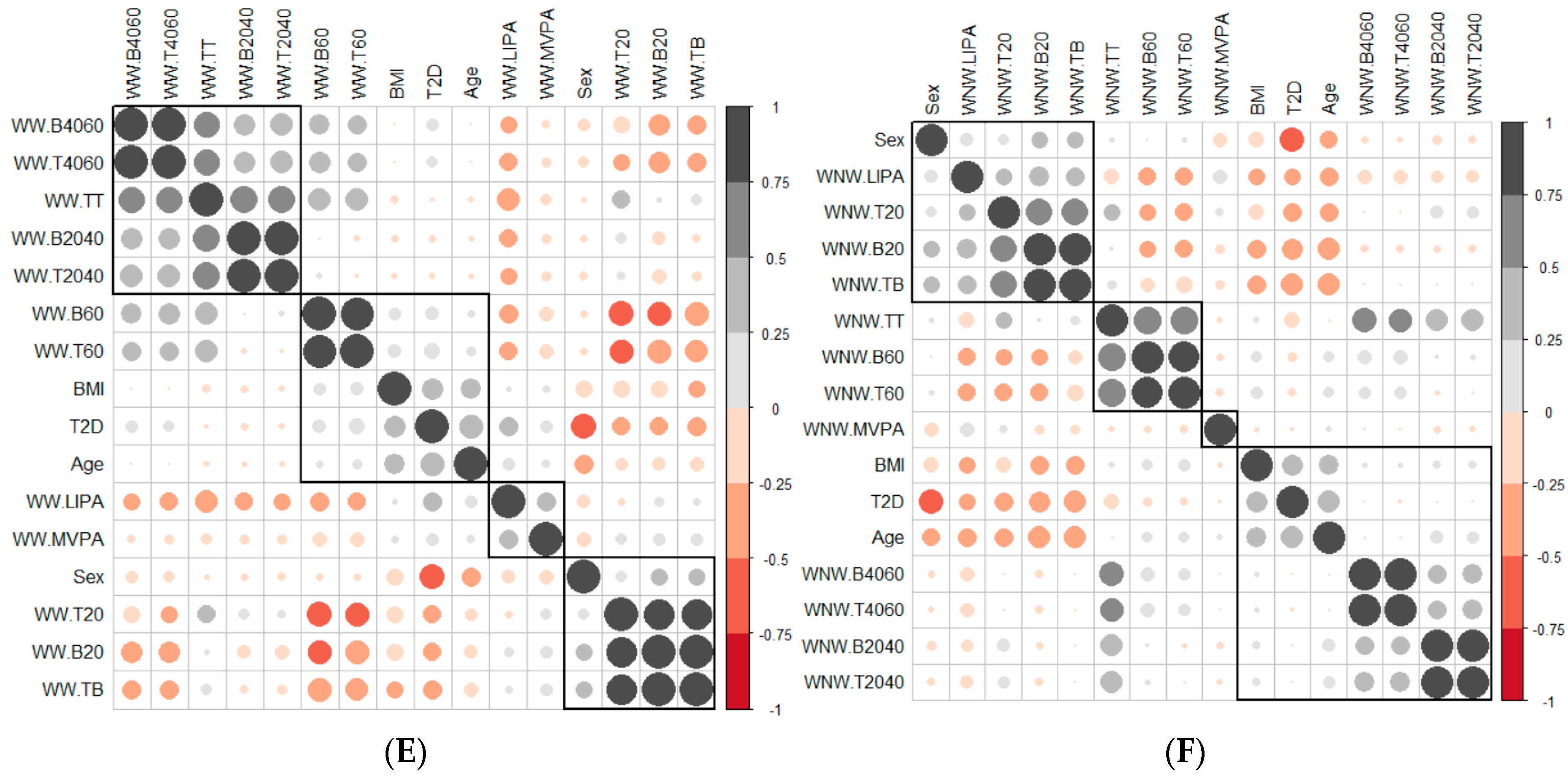
3.2. Correlation between Variables
3.2.1. Correlation between Age, BMI and SB Pattern Variables
3.2.2. Correlation between the Variables That Measured the SB Pattern on Weekdays and at Weekends
3.2.3. Correlation between the Variables That Measured the SB Pattern in Weekday Working Time and Weekday Non-Working Time
3.2.4. Correlation between the Number of Breaks and the Time Spent in Sedentary Bouts
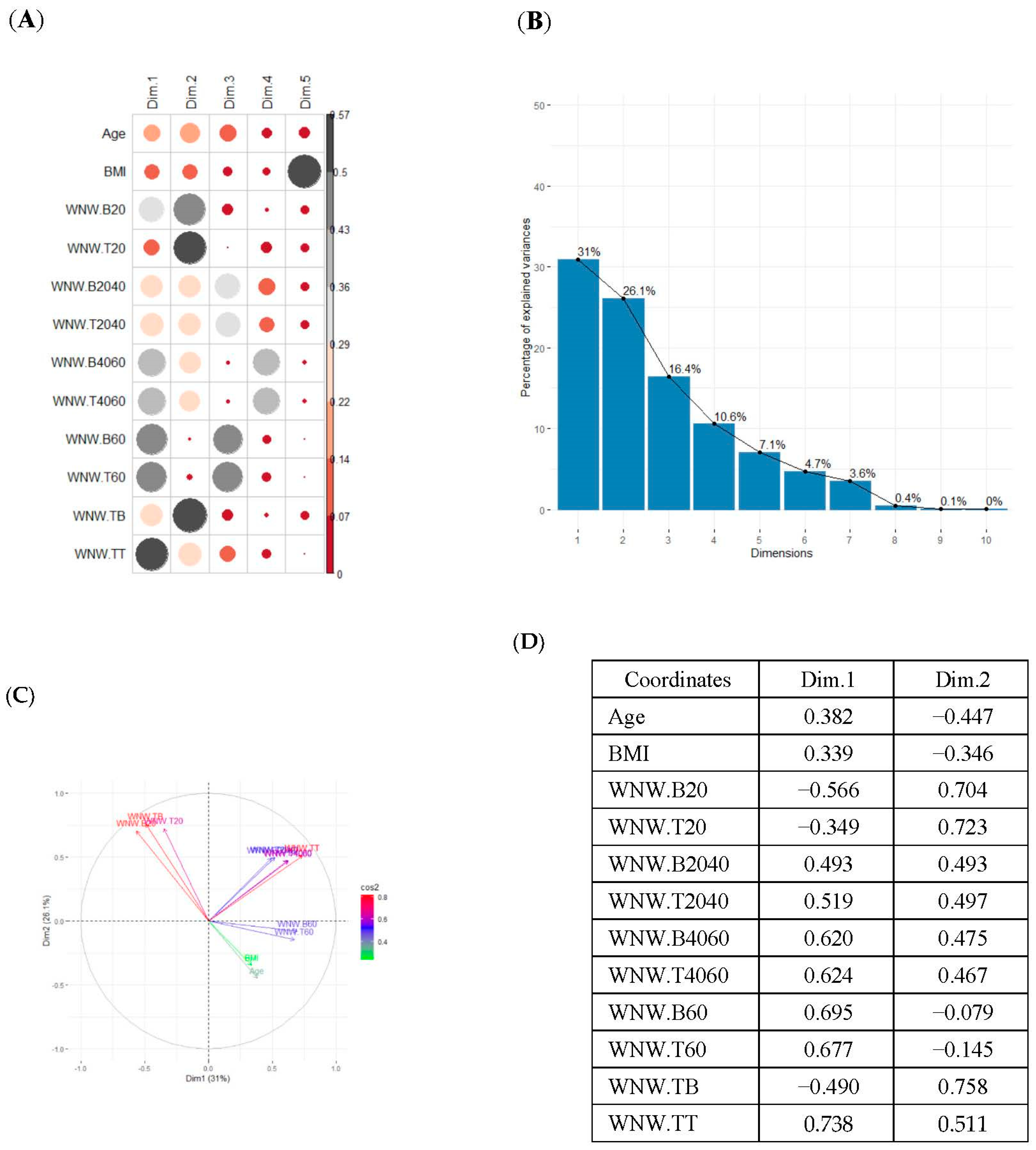
3.3. Principal Component Analysis
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- International Diabetes Federation. IDF Diabetes Atlas, 10th ed.; International Diabetes Federation: Brussels, Belgium, 2021; Available online: http://www.diabetesatlas.org/ (accessed on 25 February 2022).
- Zheng, Y.; Ley, S.H.; Hu, F.B. Global aetiology and epidemiology of type 2 diabetes mellitus and its complications. Nat. Rev. Endocrinol. 2018, 14, 88–98. [Google Scholar] [CrossRef]
- Tremblay, M.S.; Aubert, S.; Barnes, J.D.; Saunders, T.J.; Carson, V.; Latimer-Cheung, A.E.; Chastin, S.F.; Altenburg, T.M.; Chinapaw, M.J. Sedentary Behavior Research Network (SBRN)—Terminology Consensus Project process and outcome. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 75. [Google Scholar] [CrossRef] [PubMed]
- Van Der Berg, J.D.; Stehouwer, C.D.A.; Bosma, H.; Van Der Velde, J.H.P.M.; Willems, P.J.B.; Savelberg, H.H.C.M.; Schram, M.; Sep, S.J.S.; Van Der Kallen, C.J.H.; Henry, R.M.A.; et al. Associations of total amount and patterns of sedentary behaviour with type 2 diabetes and the metabolic syndrome: The Maastricht Study. Diabetologia 2016, 59, 709–718. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association. 5. Facilitating Behavior Change and Well-being to Improve Health Outcomes: Standards of Medical Care in Diabetes-2020. Diabetes Care 2020, 43 (Suppl. 1), S48–S65. [Google Scholar] [CrossRef] [PubMed]
- Bull, F.C.; Al-Ansari, S.S.; Biddle, S.; Borodulin, K.; Buman, M.P.; Cardon, G.; Carty, C.; Chaput, J.-P.; Chastin, S.; Chou, R.; et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br. J. Sports Med. 2020, 54, 1451–1462. [Google Scholar] [CrossRef] [PubMed]
- Cooper, A.R.; Sebire, S.; Montgomery, A.A.; Peters, T.J.; Sharp, D.J.; Jackson, N.; Fitzsimons, K.; Dayan, C.M.; Andrews, R.C. Sedentary time, breaks in sedentary time and metabolic variables in people with newly diagnosed type 2 diabetes. Diabetologia 2012, 55, 589–599. [Google Scholar] [CrossRef]
- Hamilton, M.T.; Hamilton, D.G.; Zderic, T.W. Sedentary behavior as a mediator of type 2 diabetes. Med. Sport. Sci. 2014, 60, 11–26. [Google Scholar] [CrossRef] [PubMed]
- Boerema, S.T.; van Velsen, L.; Vollenbroek, M.M.; Hermens, H.J. Pattern measures of sedentary behaviour in adults: A literature review. Digit. Health 2020, 6, 2055207620905418. [Google Scholar] [CrossRef]
- Edwardson, C.L.; Winkler, E.A.H.; Bodicoat, D.H.; Yates, T.; Davies, M.J.; Dunstan, D.W.; Healy, G.N. Considerations when using the activPAL monitor in field-based research with adult populations. J. Sport Health Sci. 2017, 6, 162–178. [Google Scholar] [CrossRef]
- Grant, R.W.; McCarthy, E.P.; Singer, D.E.; Meigs, J.B. Frequent outpatient contact and decreasing medication affordability in patients with diabetes from 1997 to 2004. Diabetes Care 2006, 29, 1386–1388. [Google Scholar] [CrossRef]
- American Diabetes Association. Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes. Diabetes Care 2020, 43 (Suppl. 1), S14–S31. [Google Scholar] [CrossRef] [PubMed]
- Chau, J.Y.; Van Der Ploeg, H.P.; Dunn, S.; Kurko, J.; Bauman, A.E. Validity of the occupational sitting and physical activity questionnaire. Med. Sci. Sports Exerc. 2012, 44, 118–125. [Google Scholar] [CrossRef] [PubMed]
- Bort-Roig, J.; Chirveches-Pérez, E.; Giné-Garriga, M.; Navarro-Blasco, L.; Bausà-Peris, R.; Iturrioz-Rosell, P.; González-Suárez, A.M.; Martínez-Lemos, I.; Puigoriol-Juvanteny, E.; Dowd, K.; et al. An mHealth Workplace-Based “Sit Less, Move More” Program: Impact on Employees’ Sedentary and Physical Activity Patterns at Work and Away from Work. Int. J. Environ. Res. Public Health 2020, 17, 8844. [Google Scholar] [CrossRef] [PubMed]
- Alòs, F.; Colomer, M.À.; Martin-Cantera, C.; Solís-Muñoz, M.; Bort-Roig, J.; Saigi, I.; Chirveches-Pérez, E.; Solà-Gonfaus, M.; Molina-Aragonés, J.M.; Puig-Ribera, A. Effectiveness of a healthcare-based mobile intervention on sedentary patterns, physical activity, mental well-being and clinical and productivity outcomes in office employees with type 2 diabetes: Study protocol for a randomized controlled trial. BMC Public Health 2022, 22, 1269. [Google Scholar] [CrossRef]
- Dowd, K.P.; Harrington, D.M.; Bourke, A.K.; Nelson, J.; Donnelly, A.E. The measurement of sedentary patterns and behaviors using the activPAL™ Professional physical activity monitor. Physiol. Meas. 2012, 33, 1887–1899. [Google Scholar] [CrossRef] [PubMed]
- Faul, F.; Erdfelder, E.; Lang, A.G.; Buchner, A.G. Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- Gorsuch, R.L. Factor Analysis, 2nd ed.; Hillsdale, N.J., Ed.; Lawrence Erlbaum Associates: Mahwah, NJ, USA, 1983. [Google Scholar]
- Hatcher, L. A Step-by-Step Approach to Using the SAS System for Factor Analysis and Structural Equation Modeling; SAS Institute, Inc.: Cary, NC, USA, 1994. [Google Scholar]
- Jolliffe, I.T. Principal Component Analysis for Special Types of Data. In Principal Component Analysis; Springer Series in Statistics; Springer: New York, NY, USA, 2002. [Google Scholar] [CrossRef]
- Burton, N.W.; Haynes, M.; van Uffelen, J.G.; Brown, W.J.; Turrell, G. Mid-aged adults’ sitting time in three contexts. Am. J. Prev. Med. 2012, 42, 363–373. [Google Scholar] [CrossRef] [PubMed]
- Chastin, S.F.; Egerton, T.; Leask, C.; Stamatakis, E. Meta-analysis of the relationship between breaks in sedentary behavior and cardiometabolic health. Obesity 2015, 23, 1800–1810. [Google Scholar] [CrossRef]
- Dempsey, P.C.; Larsen, R.N.; Winkler, E.A.H.; Owen, N.; Kingwell, B.A.; Dunstan, D.W. Prolonged uninterrupted sitting elevates postprandial hyperglycaemia proportional to degree of insulin resistance. Diabetes Obes. Metab. 2018, 20, 1526–1530. [Google Scholar] [CrossRef]
- Colberg, S.R.; Sigal, R.J.; Yardley, J.E.; Riddell, M.C.; Dunstan, D.W.; Dempsey, P.C.; Horton, E.S.; Castorino, K.; Tate, D.F. Physical activity/exercise and diabetes: A position statement of the American Diabetes Association. Diabetes Care 2016, 39, 2065–2079. [Google Scholar] [CrossRef]
- Vandelanotte, C.; Duncan, M.J.; Short, C.; Rockloff, M.; Ronan, K.; Happell, B.; Di Milia, L. Associations between occupational indicators and total, work-based and leisure-time sitting: A cross-sectional study. BMC Public Health 2013, 13, 1110. [Google Scholar] [CrossRef] [PubMed]
- Chau, J.Y.; van der Ploeg, H.P.; Merom, D.; Chey, T.; Bauman, A.E. Cross-sectional associations between occupational and leisure-time sitting, physical activity and obesity in working adults. Prev. Med. 2012, 54, 195–200. [Google Scholar] [CrossRef] [PubMed]
- Tigbe, W.W.; Lean, M.E.; Granat, M.H. A physically active occupation does not result in compensatory inactivity during out-of-work hours. Prev. Med. 2011, 53, 48–52. [Google Scholar] [CrossRef] [PubMed]
- Kurita, S.; Shibata, A.; Ishii, K.; Koohsari, M.J.; Owen, N.; Oka, K. Patterns of objectively assessed sedentary time and physical activity among Japanese workers: A cross-sectional observational study. BMJ Open. 2019, 9, e021690. [Google Scholar] [CrossRef]
- Homer, A.R.; Taylor, F.C.; Dempsey, P.C.; Wheeler, M.J.; Sethi, P.; Townsend, M.K.; Grace, M.S.; Green, D.J.; Cohen, N.D.; Larsen, R.N.; et al. Frequency of Interruptions to Sitting Time: Benefits for Postprandial Metabolism in Type 2 Diabetes. Diabetes Care 2021, 44, 1254–1263. [Google Scholar] [CrossRef]
- Healy, G.N.; Clark, B.K.; Winkler, E.A.; Gardiner, P.A.; Brown, W.J.; Matthews, C.E. Measurement of adults’ sedentary time in population-based studies. Am. J. Prev. Med. 2011, 41, 216–227. [Google Scholar] [CrossRef]
- Aunger, J.; Wagnild, J. Objective and subjective measurement of sedentary behavior in human adults: A toolkit. Am. J. Hum. Biol. 2022, 34, e23546. [Google Scholar] [CrossRef]
- Soriguer, F.; Goday, A.; Bosch-Comas, A.; Bordiú, E.; Calle-Pascual, A.; Carmena, R.; Casamitjana, R.; Castaño, L.; Castell, C.; Catalá, M.; et al. Prevalence of diabetes mellitus and impaired glucose regulation in Spain: The Di@betes Study. Diabetologia 2012, 55, 88–93. [Google Scholar] [CrossRef]
- Ausubel, J.H.; Grubler, A. Working less and living longer: Long-term trends in working time and time budgets. Technol. Forecast. Soc. Change 1995, 50, 195–213. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| TYPE 2 DIABETES | NORMAL GLUCOSE METABOLISM | Between Groups T2D vs. NGM | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | n | Mean | SD | n | 95% CI | p-Value | ||
| Age (years) | 55.8 | 6.3 | 77 | 45.2 | 8.9 | 128 | −12.68 | −8.52* | <0.001 |
| BMI (kg/m2) | 31.4 | 5.5 | 77 | 24.9 | 4.9 | 132 | −7.98 | −5.02* | <0.001 |
| WEEKDAY—TOTAL TIME | |||||||||
| Light-intensity physical activity (minutes/day) | 75.4 | 34.1 | 80 | 75.2 | 21.1 | 132 | −8.45 | 8.05 | 0.9624 |
| Moderate to vigorous physical activity (minutes/day) | 43.7 | 27.2 | 79 | 47.7 | 21.3 | 132 | −2.98 | 10.98 | 0.2656 |
| Sedentary time (minutes/day) | 572 | 144.8 | 75 | 599.3 | 101.8 | 132 | −9.60 | 64.20 | 0.1518 |
| Standing time (minutes/day) | 273.4 | 106 | 80 | 302.4 | 80.6 | 132 | 2.14 | 55.86 * | 0.0371 |
| Total sedentary breaks (number/day) | 50.3 | 17.2 | 75 | 82 | 28.4 | 132 | 25.49 | 37.85 * | <0.001 |
| Sedentary breaks <20 min (number/day) | 43.2 | 17 | 75 | 74.3 | 29.5 | 132 | 24.79 | 37.41 * | <0.001 |
| Sedentary breaks of 20–40 min (number/day) | 5 | 2.1 | 75 | 4.8 | 1.8 | 132 | −0.74 | 0.38 | 0.5290 |
| Sedentary breaks of 40–60 min (number/day) | 1.7 | 1 | 75 | 1.5 | 0.8 | 132 | −0.55 | −0.33 * | 0.0313 |
| Sedentary breaks >60 min (number/day) | 1.6 | 1.2 | 75 | 1.4 | 0.9 | 132 | −0.56 | 0.05 | 0.1034 |
| Time spent in sedentary bouts <20 min (minutes/day) | 198.7 | 70.1 | 75 | 270.3 | 67.8 | 132 | 52.06 | 91.14 * | <0.001 |
| Time spent in sedentary bouts 20–40 min (minutes/day) | 138.9 | 56.3 | 75 | 133.6 | 49.4 | 132 | −20.53 | 9.87 | 0.4954 |
| Time spent in sedentary bouts 40–60 min (minutes/day) | 84 | 47.3 | 75 | 71.1 | 38.6 | 132 | −25.34 | −0.34 * | 0.0472 |
| Time spent in sedentary bouts >60 min (minutes/day) | 150.5 | 111.3 | 75 | 124.3 | 85.7 | 132 | −55.14 | 2.80 | 0.0806 |
| WEEKDAY—WORKING TIME | |||||||||
| Light-intensity physical activity (minutes/day) | 37.5 | 26.2 | 53 | 24.5 | 11.9 | 115 | −20.34 | −5.66 * | 0.0010 |
| Moderate to vigorous physical activity (minutes/day) | 20.7 | 14.6 | 25 | 18.4 | 11.4 | 98 | −8.42 | 3.82 | 0.4692 |
| Sedentary time (minutes/day) | 283.8 | 129.6 | 47 | 294.4 | 64.5 | 115 | −28.07 | 49.29 | 0.5950 |
| Standing time (minutes/day) | 2.3 | 1.2 | 53 | 1.9 | 0.9 | 115 | −0.76 | −0.04 * | 0.0336 |
| Total sedentary breaks (number/day) | 28.5 | 15.2 | 46 | 41.7 | 19.1 | 115 | 7.70 | 18.84 * | <0.001 |
| Sedentary breaks <20 min (number/day) | 24.8 | 14.7 | 46 | 37.9 | 20 | 115 | 7.53 | 18.71 * | <0.001 |
| Sedentary breaks of 20–40 min (number/day) | 2.7 | 1.6 | 46 | 2.8 | 1.3 | 115 | −0.4 | 0.63 | 0.6609 |
| Sedentary breaks of 40–60 min (number/day) | 0.8 | 0.7 | 46 | 0.7 | 0.6 | 115 | −0.39 | 0.06 | 0.1633 |
| Sedentary breaks >60 min (number/day) | 0.6 | 0.7 | 46 | 0.4 | 0.5 | 115 | −0.47 | 0.00 | 0.0513 |
| Time spent in sedentary bouts <20 min (minutes/day) | 116.4 | 65.7 | 46 | 153.7 | 53.6 | 115 | 16.10 | 58.61 * | 0.0010 |
| Time spent in sedentary bouts 20–40 min (minutes/day) | 73.5 | 44.5 | 46 | 75.6 | 35.6 | 115 | −12.23 | 16.45 | 0.7753 |
| Time spent in sedentary bouts 40–60 min (minutes/day) | 39.4 | 32.7 | 46 | 32.3 | 29.5 | 115 | −17.99 | 3.64 | 0.1999 |
| Time spent in sedentary bouts >60 min (minutes/day) | 60.6 | 81 | 46 | 32.9 | 45.3 | 115 | −52.47 | −3.05 * | 0.0327 |
| WEEKDAY—NON-WORKING TIME | |||||||||
| Light-intensity physical activity (minutes/day) | 45.3 | 25.9 | 68 | 49.6 | 15.9 | 115 | −2.47 | 11.07 | 0.2187 |
| Moderate to vigorous physical activity (minutes/day) | 29 | 19.9 | 68 | 30.4 | 17.2 | 115 | −4.29 | 7.01 | 0.6395 |
| Sedentary time (minutes/day) | 272.5 | 89.6 | 46 | 311.8 | 81.7 | 115 | 9.58 | 69.05 * | 0.0119 |
| Standing time (minutes/day) | 165.9 | 83 | 68 | 184.5 | 49.5 | 115 | −2.99 | 40.19 | 0.0963 |
| Total sedentary breaks (number/day) | 23.6 | 8.6 | 46 | 38.6 | 15.1 | 115 | 11.31 | 18.70 * | <0.001 |
| Sedentary breaks <20 min (number/day) | 19.6 | 8.5 | 46 | 34.6 | 15.4 | 115 | 11.24 | 18.66 * | <0.001 |
| Sedentary breaks of 20–40 min (number/day) | 2.2 | 0.8 | 46 | 2.2 | 1.0 | 115 | −0.35 | 0.25 | 0.7487 |
| Sedentary breaks of 40–60 min (number/day) | 0.9 | 0.5 | 46 | 0.9 | 0.5 | 115 | −0.18 | 0.17 | 0.9512 |
| Sedentary breaks >60 min (number/day) | 0.9 | 0.6 | 46 | 1.0 | 0.7 | 115 | −0.11 | 0.33 | 0.3441 |
| Time spent in sedentary bouts <20 min (minutes/day) | 85.4 | 35.5 | 46 | 116.3 | 36.8 | 115 | 18.72 | 43.15 * | <0.001 |
| Time spent in sedentary bouts 20–40 min (minutes/day) | 62.1 | 22.5 | 46 | 61.7 | 29.0 | 115 | −8.70 | 7.98 | 0.9334 |
| Time spent in sedentary bouts 40–60 min (minutes/day) | 41.3 | 24.3 | 46 | 41.7 | 26.2 | 115 | −8.00 | 8.92 | 0.9154 |
| Time spent in sedentary bouts >60 min (minutes/day) | 83.8 | 66.1 | 46 | 92.1 | 69.9 | 115 | −14.60 | 31.15 | 0.4825 |
| WEEKEND | |||||||||
| Light-intensity physical activity (minutes/day) | 67.3 | 36.2 | 77 | 80 | 30.4 | 132 | 3.14 | 22.26 * | 0.0106 |
| Moderate to vigorous physical activity (minutes/day) | 34.9 | 31.1 | 73 | 33.9 | 33.1 | 132 | −10.05 | 8.05 | 0.8297 |
| Sedentary time (minutes/day) | 548.3 | 135.1 | 73 | 518.2 | 117 | 132 | −66.77 | 6.58 | 0.1120 |
| Standing time (minutes/day) | 235.3 | 96.8 | 73 | 297.1 | 97.3 | 132 | 34.22 | 89.38 * | <0.001 |
| Total sedentary breaks (number/day) | 38.3 | 12 | 73 | 59.3 | 27.2 | 132 | 15.62 | 26.36 * | <0.001 |
| Sedentary breaks <20 min (number/day) | 31.9 | 12.3 | 73 | 52.5 | 27.8 | 132 | 15.14 | 26.12 * | <0.001 |
| Sedentary breaks of 20–40 min (number/day) | 3.8 | 1.7 | 73 | 3.6 | 1.7 | 132 | −0.74 | 0.21 | 0.2848 |
| Sedentary breaks of 40–60 min (number/day) | 1.6 | 1 | 73 | 1.4 | 1.0 | 132 | −0.54 | 0.02 | 0.0729 |
| Sedentary breaks >60 min (number/day) | 2.1 | 1.3 | 73 | 1.9 | 1.0 | 132 | −0.59 | 0.11 | 0.1840 |
| Time spent in sedentary bouts <20 min (minutes/day) | 151.2 | 61.6 | 73 | 166.8 | 64.7 | 132 | −2.28 | 33.39 | 0.0910 |
| Time spent in sedentary bouts 20–40 min (minutes/day) | 109.4 | 46.9 | 73 | 99.7 | 46.5 | 132 | −37.03 | 17.60 | 0.4981 |
| Time spent in sedentary bouts 40–60 min (minutes/day) | 79.1 | 49.5 | 73 | 67.1 | 46.9 | 132 | −25.89 | 1.75 | 0.0908 |
| Time spent in sedentary bouts >60 min (minutes/day) | 208.5 | 134.4 | 73 | 184.6 | 113.9 | 132 | −60.13 | 12.38 | 0.2015 |
| PCA Variables | Variability Explained by the First Two Components | Grouping of Patients Based on the 2 Dimensions Obtained with PCA |  |
|---|---|---|---|
| Weekday and weekend | 61.6% |  | |
| Weekday | 61% |  | |
| Weekday working time | 63.1% |  | |
| Weekday non-working time | 57.1 |  | |
| Weekend | 54.7 |  | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Colomer, F.A.; Cugat, M.À.C.; Bort-Roig, J.; Chirveches-Pérez, E.; Zaldúa, Y.C.; Martín-Cantera, C.; Franch-Nadal, J.; Puig-Ribera, A. Differences in Free-Living Patterns of Sedentary Behaviour between Office Employees with Diabetes and Office Employees without Diabetes: A Principal Component Analysis for Clinical Practice. Int. J. Environ. Res. Public Health 2022, 19, 12245. https://doi.org/10.3390/ijerph191912245
Colomer FA, Cugat MÀC, Bort-Roig J, Chirveches-Pérez E, Zaldúa YC, Martín-Cantera C, Franch-Nadal J, Puig-Ribera A. Differences in Free-Living Patterns of Sedentary Behaviour between Office Employees with Diabetes and Office Employees without Diabetes: A Principal Component Analysis for Clinical Practice. International Journal of Environmental Research and Public Health. 2022; 19(19):12245. https://doi.org/10.3390/ijerph191912245
Chicago/Turabian StyleColomer, Francesc Alòs, Mª Àngels Colomer Cugat, Judit Bort-Roig, Emilia Chirveches-Pérez, Yoseba Cánovas Zaldúa, Carlos Martín-Cantera, Josep Franch-Nadal, and Anna Puig-Ribera. 2022. "Differences in Free-Living Patterns of Sedentary Behaviour between Office Employees with Diabetes and Office Employees without Diabetes: A Principal Component Analysis for Clinical Practice" International Journal of Environmental Research and Public Health 19, no. 19: 12245. https://doi.org/10.3390/ijerph191912245
APA StyleColomer, F. A., Cugat, M. À. C., Bort-Roig, J., Chirveches-Pérez, E., Zaldúa, Y. C., Martín-Cantera, C., Franch-Nadal, J., & Puig-Ribera, A. (2022). Differences in Free-Living Patterns of Sedentary Behaviour between Office Employees with Diabetes and Office Employees without Diabetes: A Principal Component Analysis for Clinical Practice. International Journal of Environmental Research and Public Health, 19(19), 12245. https://doi.org/10.3390/ijerph191912245