Abstract
Homebirth is legal and has been regulated by law in Hungary since 2012. Despite the obvious advantages of homebirth, it has not yet been broadly accepted, due to various opinions related to safety and risks associated with giving birth outside of a hospital. Our study aimed at exploring both real maternal and feto-neonatal characteristics associated with Hungarian homebirths. A total of 2997 cases were considered in support of our retrospective cohort study. In the examined period, there was a significant, continual rise in the number of homebirths by a rate of 0.22% on average per year. Aggregated maternal complications (primary uterine inertia, prolonged second stage labour, and third stage haemorrhage) were prevalent among homebirth cases (1.29% vs. 0.72%, p < 0.05) and were associated with an average of 11.77% rate of transfer to a health care institution. On the other hand, the rate of operative (vaginal or caesarean) delivery was 26.31% among institutionalized births. A slightly better Apgar score and relatively high rate (20%) of caesarean deliveries were correlated with institutionalized births (p < 0.05). However, the overall intervention rate was lower among homebirths (0.11% vs. 42.57%) than institutional birth cases (p < 0.001). Overall, homebirth is a reliable option for childbirth for healthy and low-risk mothers with uncomplicated pregnancies, which is reflected in the increasing number of deliveries at home in Hungary. Furthermore, utilizing the experiences of countries where homebirth is a long-established method may further improve the outcome of homebirths in Hungary.
1. Introduction
Homebirth for cases with normal pregnancy and managed by a licenced midwife is a safe option for healthy, low-risk women [1,2]. The safest place for a woman to give birth to her baby is believed to be at a functional health facility, with a professionally trained birth attendant. However, during the recent global crisis or due to other reasons, many women may end up giving birth at home [3]. Homebirth is an act of a woman giving birth to a child in ones’ own home [4]. During the recent pandemic, many women felt detached from sexual and reproductive health services, due to quarantine protocols. Pregnant women were unwilling to come to their local health facilities, due to disruptions in transportation associated with nationwide lockdown measures while others shunned the hospital or clinic due to increased fear of the spread of infections [5]. Others worried about giving birth surgically [6], and some reported health care providers’ reluctance to support birthing women’s needs that conflict with their moral beliefs [7]. Hence, there can be a trend for women who prefer to deliver their newborns at home [8].
It is not possible to predict the outcome of a pregnancy accurately. Problems during pregnancy may include physical and mental conditions that can range from mild and annoying discomforts to severe, sometimes life-threatening, illnesses that affect the life of a mother and her newborn. For instance, birthweight that reflects intra-uterine growth is an important determinant factor for perinatal morbidity and mortality [9,10] and, in recent years, has been shown to be a marker of postnatal health risks [9]. Although much is known regarding the clinical management of labour and childbirth, less attention is given to what clinical interventions make women feel safe, comfortable, and positive regarding the experience in the birth of their babies [9]. At the same time, the high ratio of operative deliveries is a real problem in many countries. Women need to receive health care before and during pregnancy to decrease the risk of pregnancy complications [10]. The prenatal care performed by county midwives and obstetricians is well organized in Hungary. Thus, the selection of patients eligible for homebirth is determined easily. However, while some problems can be caused by or can be made worse while being pregnant, many problems are mild and do not progress, but they can harm the mother and her newborn when they do. To cite a specific instance, birthweight, which reflects intra-uterine growth retardation, is an important determinant factor regarding perinatal morbidity and mortality [11,12] and, in recent years, is a marker in identifying postnatal health risks [13].
In Hungary, homebirth was neither legal nor illegal until 2012. In October 2010, police detained a Hungarian gynaecologist named Agnes Geréb. She was given a two-year prison sentence in February 2012 by the Budapest appeals court for two home birth instances. One entailed being there at the delivery of twins, one of whom died. In the second instance, she helped deliver a baby who eventually died six months later after suffering from serious problems. Later, Geréb and her lawyer asked for a new trial, citing fresh expert submissions. At that time, Dr. János Áder, the president of Hungary, granted Dr. Agnes Geréb’s request for mercy and overturned her jail term. She is a well-regarded independent obstetrician and gynaecologist whose life’s work was the freedom of birthing. More significantly, her efforts led to legislation that made homebirth legalized in Hungary [14,15]. Since then, strict regulations determine the conditions of homebirth for both pregnant women and participants of medical services. Healthy women, aged between 18 and 40 years, with normal, uncomplicated, single pregnancy, who are able to reach a hospital in 20 min in case a complication happens, are eligible for homebirth [16,17]. During the perinatal period, the pregnant mother enters into a contract with two persons (obstetrician or midwife and also their substitutes) who are licensed and corresponded to obstetrical specifications and are also skilful with adult resuscitation and the management of the neonate [18].
Outside of Hungary, several countries are considering the reintroduction of homebirths. This is based on claims of equal safety at lower intervention rates, compared to institutional births in which overtreatment may be present [19]. Furthermore, psycho-social advantages associated with homebirth for the mother are also beneficial [20] and the introduction of effective interprofessional collaboration should be driven for a safe home birth [21]. When the care for a patient is cohesive, the patient certainly benefits, as the health care team has worked together as a team to best address the pregnant women’s needs, wants, and values [22,23,24].
Homebirth is not yet widely accepted in Hungary [25], and the criminal stories covered by the media before 2012 most likely had an impact on the overall opinions of homebirth in Hungary [1,26]. Thus, our study attempts to explore the real maternal and feto-neonatal conditions and outcome characteristics regarding Hungarian homebirths.
2. Materials and Methods
2.1. Design and Sample Size
This is a comparative retrospective cohort study. We sourced data regarding homebirths (n = 1792 from 2012 through 2020) from the Hungarian obstetric database (also called the ‘Tauffer database”) [27]. The ‘Tauffer database’ is managed and made available to researchers through the efforts of the National Institute for Quality and Organizational Development in Health Care and Medicine (reference 76/2004, decree regarding the determination, collection, and analysis of health-related unidentifiable data; Ministry of Health, Social and Family Affairs, Hungary) [16]. Institutional birth data (n = 1205) obtained from the Obstetrics and Gynaecology Department of the University of Pécs were matched according to Hungarian criteria of homebirth. All mothers included in this study were older than 18 years of age yet younger than 40 years old if it is their first pregnancy. Additional prerequisites included soon-to-be mothers being within 37–41 weeks of gestation, it being single pregnancy, the foetuses being in the cephalic position, and there being no prior history of any form of complication(s) during pregnancy. Those who planned to give birth at home must have access to a health facility that is equipped with obstetrical and neonatal services within 20 min of travel. These were our criteria and are representative of the basic permissive standards regarding homebirth, as stated in Hungarian laws about homebirth [16].
Data related to outcome conditions and complications during pregnancy were collected by International Classifications of Diseases, 10th revision (ICD-10 codes) [28].
2.2. Variables
Maternal-related variables included were maternal age, parity (primi- and multi-parous), gestational age, previous abortion (one or more), mode of conception (spontaneous or artificial), types of rupture of membrane (preterm, term, or artificial) and mode of birth (spontaneous or instrumental).
Feto-neonatal variables included were the gender of the newborn, stillbirth, Apgar score measured five minutes following birth, early neonatal death at <168 h, birth weight, and birth weight percentiles. They were the independent variables, alongside which we have a dichotomous dependent variable (birthplaces, i.e., homebirth and institutional birth). Intervention was a health care variable.
2.3. Outcome Measures
Two primary outcomes were identified. First, “intervention” during birth, which is operationalized as undergoing intrapartum operative vaginal birth, or caesarean section and intrapartum artificial rupture of the membrane (AROM) is represented as ‘INTER2’. Secondly, perinatal mortality, in which it becomes operational, is a combination of stillbirths, intrapartum deaths, and early neonatal mortality until 168 h following delivery. The pooled outcome measures (Intervention * perinatal mortality) were used to estimate the risk ratio. The other secondary outcomes include maternal complications and outcome conditions.
2.4. Case-Mix Adjustment
Studies addressing the benefits and drawbacks of homebirth can be challenged due to their observational study design without case-mix adjustment regarding interventions and outcomes and the exclusion of women from the analysis, who, according to standardized birth guidelines, should have been referred to before birth.
The case-mix was represented by the prevalence of the “Big4” conditions representative of an important risk mediator. These four conditions are known to precede 85% of perinatal mortality. These four-neonatal conditions are congenital abnormalities, intra-uterine growth restriction (small for gestational age), preterm, and low Apgar score (<7, measured 5 min following delivery). In a system highlighted with optimal risk, at least two big conditions (“Big2”), i.e., small for gestational age and low Apgar score are still present [20].
When comparing mortality rates, the “Big2” case-mix adjustment is used. However, when comparing intervention rates, the intervention precedes the outcome regarding a low Apgar score. Therefore, a low Apgar score should be excluded, and an analysis is compiled. Then pooled analyses (Intervention * mortality case-mix advanced model) were used to determine the risk ratio among groups.
2.5. Data Analysis
The data were analysed using IBM SPSS statistics version 26. The excel datasets were cleaned and de-identified before exporting to SPSS. Descriptive statistics were generated using frequencies, percentages, means, and standard deviations. Data of continuous parametric variables were presented as a mean ± standard deviation. The results of the chi-square were presented in APA format [29].
In consideration of statistical analysis, we used logistic regression models. Model 1, a binary logistic regression analysis, was presented as a crude odds ratio (COR), and Model 2, the multivariable logistic regression, was presented as an adjusted odds ratio (AOR) after adjusting for the confounders. In our study, a two-sided p value < 0.05 was considered statistically significant at a 95% confidence interval. All the explanatory variables with a threshold of p < 0.20 on a binary logistic regression model were fitted to a multivariable regression model and adjusted for confounders. Statistical significance was also cross-checked using backwards and forward stepwise regression analysis and demonstrated the same statistical significance.
Third, we compared the perinatal mortality rates after the “Big4” adjustment using an intention-to-treat-like approach. The intention-to-treat analysis is primarily used in RCTs [30]. However, we used the ‘intention-to-treat-like’ analysis approach, implying that all women having a home or institutional birth outcome were included, independent from later referral during labour. In consideration of this analysis, a nested multiple stepwise regression model (stepwise analysis; inclusion p < 0.20; exclusion p > 0.20) was used (model 1). Additionally, a pseudo-multicollinearity test was performed before running a multivariate logistic regression analysis and none were multicollinear.
3. Results
3.1. Baseline Characteristics of Participants
A total of 2997 women were included in our study. During the considered period, 1792 mothers who experienced homebirths were compared with 1205 mothers who experienced an institutionalized birth. Our data have shown that the homebirths slowly increased over time by a rate of 0.22% per year on average (see Figure 1).
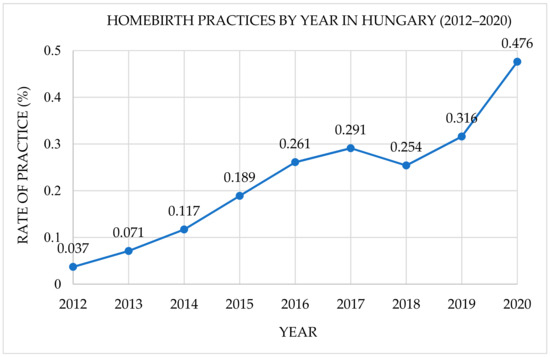
Figure 1.
Trends of homebirth practices by year in Hungary (2012–2020).
In terms of homebirths, the mean maternal age at first delivery was 33.16 ± 4.71, they were multiparous (66.50%), and the majority experienced a spontaneous mode of childbirth (94.01%); whereas, for institutional childbirths, 29.69 ± 5.44 was the mean maternal age at first delivery, 55.90% were primiparous, and 888 (73.69%) experienced spontaneous vaginal deliveries. The chi-square test of independence showed advanced-age mothers (≥35 years) were more likely to deliver at home, compared with younger-aged women (<35), Χ2(1, n = 2997) = 85.58, p < 0.001. Notably, mothers who had no prior history of previous spontaneous abortion were more likely to experience homebirths (p < 0.001), whereas nearly 332 (18.50%) women who had homebirths, and 11 (0.90%) who had institutional births used artificial means to conceive, Χ2(2, n = 2997) = 220.56, p < 0.001 (see Table 1).

Table 1.
Baseline characteristics of women who experienced home births and institutional births in Hungary from 2012–2020.
3.2. Feto-Neonatal Birth Characteristics and Outcome
Of the total 2997 newborns, 1537 (51.30%) were male, 1460 (48.70%) were female, (99.89%) were born alive, and 3 (0.11%) were reported as fatal cases (stillborn) during childbirth. The mean Apgar score at 5 min was 9.87 (±0.61) at home and 9.92 (±0.31) at institutions, respectively. Newborns from mothers who experienced homebirths had a slightly lower Apgar score at 5 min than when compared with institutional births Χ2(2, n = 2997) = 15.78, p < 0.001 (see Table 2).
Table 2.
Characteristics and outcomes of the newborns from mothers who experienced home birth and institutional births in Hungary, 2012–2020.
The mean birth weight was slightly higher in-homebirths (3556.87 ± 439.29), compared to institutional births (3433.16 ± 426.74), Χ2(2, n = 2997) = 22.34, p < 0.001, of which, the majority were appropriate and large for gestational age (59.01%, 39.50%), while few were small for gestational age (1.50%), and they were below 10th birth weight percentiles (see Figure 2).
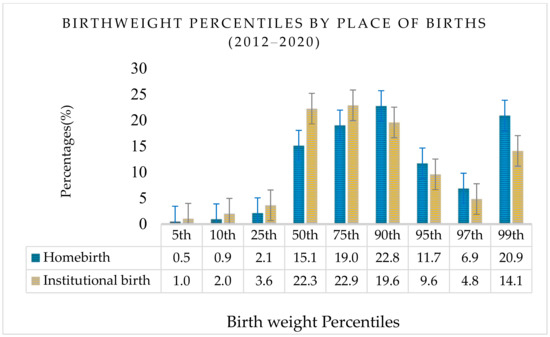
Figure 2.
Birth weight percentiles by place of birth in Hungary (2012–2020).
Newborns with relatively high birth weight were more likely to be born at home when compared with institutionalized deliveries, Χ2(2, n = 2997) = 22.34, p < 0.001 (see Table 2).
Of the five early neonatal deaths (<168 h afterbirth), three (0.20%) were from home and two (0.17%) were among institutional births, and the reported stillbirths (0.17%) and intrapartum death at the institution (0.17%) were among transferred cases.
3.3. Maternal and Feto-Neonatal Birth Outcome Conditions and Complications
Of the total 2997 singleton births, 1183 (66.02%) homebirths and 884 (73.36%) institutional births were reported to have no obstetric complications. A relatively higher number of mothers who experienced institutional births had prolonged first-stage labour (3.32%), perineal laceration during birth (6.72%), or obstetric laceration of the cervix (2.91%) and 35 (2.91%) were anaemic (p < 0.05). Third-stage haemorrhage and delayed and secondary postpartum haemorrhage (1.40%, 0.84%) were prevalent maternal conditions reported from home births, respectively (see Table 3). A relatively higher number of foetal conditions, including foetal heart rate anomaly and meconium-stained amniotic fluid, at 22 (1.23%) were reported from homebirth cases (see Table 3). Overall, the women who had homebirths were 1.28% times the risk of complications, compared to women who had institutionalized births.
Table 3.
Comparisons of maternal and feto-neonatal homebirth and institutional birth-related conditions and complications in Hungary, 2012–2020.
Regarding other determinants, the operative birth rate at the institution was 0.26 (26.31%) and about 0.05 (5.39%) were vacuum deliveries, while the institutional caesarean section rate was 0.21 (20.90%) (see Table 4). Only 24 (1.34%) women who experienced homebirths had an intention to operative birth. On average, the institutional transfer rate was 11.77%.
Table 4.
Summary statistics of women and feto-neonatal home and institutional birth characteristics and outcomes: Pooled risk measures (Intervention (C/s and AROM) * Perinatal mortality); using intention-to-treat-like approach and case-mix adjustment.
The intervention rate was lower among homebirth cases (0.11%) compared with institutionalized births (42.57%) (p < 0.001). The crude intervention risk was significantly lower for women who experienced homebirths (COR 0.02, [95%CI 0.01–0.06, p < 0.001]) compared with women who experienced institutional births (Table 4, model 1). All maternal and neonatal risk factors (except the presence of a history of abortion, mode of birth and ROM) showed a significant difference. The adjusted intervention risk ratio demonstrates the birthplace indeed has a significant effect on the likelihood of intervention (AOR 0.02, [95%CI 0.01–0.05, p < 0.001]) (Table 4, model 2). Perinatal mortality was 11 (0.61%) among homebirths and 6 (0.49%) among institutionalized births, however, has not demonstrated any significant association with birthplace (see Table 4).
4. Discussion
According to our study, home births have been a more common occurrence in Hungary over the past ten years. As a result, the average homebirth rate in Hungary is 0.22%, which is considerably low when compared with the Netherlands (17%), New Zealand (3.5%), Australia (0.3%), or the United Kingdom (2.4%) [20,31,32,33]. Studies have indicated homebirth choice is controversial and enshrouded in debate. Generally, of issues related to risk and safety in a well-integrated health care system, homebirth is also deemed safe for healthy, low-risk women [1,2].
In Hungary, very little research has been published regarding homebirths for a multitude of reasons, specifically, the lack of funding and institutional support. However, beyond Hungary, studies indicate women, who planned homebirths, have experienced a very low risk of instrumental vaginal birth and caesarean section, therefore, a higher probability of spontaneous vaginal delivery [19,34,35,36,37]. Our study has also shown that the majority of low-risk women who gave birth at home have experienced a spontaneous mode of delivery (p < 0.001). A study originating from four Nordic countries has shown the majority of low-risk multiparous women who experienced spontaneous birth in their previous pregnancies were more likely to give birth at home [34]. Moreover, low-risk pregnancies attended by qualified midwives bring in positive results among both maternal and newborn health levels, including low rates of obstetric intervention [35,36,37].
Additionally, our study demonstrates how advanced age mothers (aged ≥ 35years) were more likely to experience homebirths than when compared with younger age mothers (p < 0.001), and our finding is consistent with the other studies, which aptly substantiated a general indication of the increased number of late childbearing age women aged 35 and above [38,39,40]. Today, it is becoming common for women in developed countries to delay their childbearing age. This phenomenon is due to multiple factors, yet effective birth control methods significantly contribute to postponing motherhood [41].
In our study, obstetrical complications related to mothers were prevalent among homebirths, while, relatively speaking, neonatal-related pathologic conditions and complications were more frequent among homebirth cases (p < 0.05). Other studies have shown that complications were more likely among planned homebirths [37,42].
We found that 1.5% of newborns from mothers who experienced homebirths had a relatively low Apgar score. Studies have shown that a newborn with a low Apgar score reflects a greater risk for obstetric and pregnancy-related complications [19,35,39,43]. Additionally, our findings are consistent with a study by Chandra et al. [44] regarding differences in maternal characteristics and pregnancy outcomes, which has shown a significant association between a low Apgar score of 5 min or poor pregnancy outcomes.
Studies from countries with long-term experiences with homebirth confirm that deliveries at home with low-risk mothers with no previous history of obstetric complications show similar outcomes to institutional childbirths [19,45].
In our study, the hospital transfer rate was 11.77%. A systematic review of a large number of studies has shown that homebirth with such a transfer rate is considered reasonable, and an indication for the system is well integrated and able to support a pregnant mother’s choice regarding the place of birth [46]. Women who planned homebirth were considerably low risk throughout labour, and less likely to be transferred to an institution for advanced obstetric care, which typically results in a prolonged duration in second-stage labour [35]. This condition again is associated with the use of episiotomy, which may also be associated with perineal lacerations and intrapartum haemorrhage [37,39]. Similarly, our study also showed primary uterine inertia, prolonged second-stage labour, and third-stage haemorrhage, which were reported in women who experienced homebirths. The shorter duration of second-stage labour regarding institutional births may be due to higher intervention rates (episiotomy and option for operative delivery). Additionally, our study showed that “Big2” pregnancies at home exhibit a mortality disadvantage, suggesting comparatively lower intervention rates. The occurrence of overtreatment in the institution cannot be excluded. However, the benefit of fewer interventions among the homebirth group seems to be counterbalanced by substantially increased rates of complications. Our findings were partially inconsistent with a study from the Netherlands, in which increased larger sample sizes (n = 146,752) demonstrated that planned home births, attended by registered community midwives, confirm the lower risk of medical intervention, resulting in equal rates of complications [20]. In the Netherlands, the current homebirth rate is historically low, and it has never been this low before, with people’s experiences largely contributing to reaching this phenomenon. Other possible explanations were due to the increased chances for women who planned homebirth to switch their birthplace to an institution following a medical condition they recently experienced just before or during labour. Nonetheless, the safety and risks related to homebirth are not well expounded upon, and are very much a topic of debate, and published literature also substantiates regional variability [19,34,35,36,38,39,47].
4.1. Strength
As far as we are aware, this is the first study of its sort to describe homebirth characteristics in Hungary.
Notably, case-mix adjustment and intention-to-treat approach resulted in the most important aspect and strengthened our study. Without adjusting for this, one risks confounding the issue by indication bias.
4.2. Limitations
- Tauffer database is a compulsory database, however, some outcome variables were missed (like estimated volume of blood loss and birth outcomes of transferred cases) and less likely to be compared.
- The NICU admission, maternal weight (BMI), reason(s) used to transfer cases, and one-minute Apgar scores were not recorded in the compulsory database regarding homebirth cases.
- Lack of detailed information regarding maternal dropout and transfer for obstetric care, midwifery experiences, training, and their practices implemented in monitoring and evaluating feto–maternal conditions before and during birth.
- Despite baseline matching the potential confounders and restriction to low-risk women in our study, the possibility of residual confounding cannot be excluded given an observational study.
5. Conclusions
In careful consideration of our findings, both maternal and foetal–neonatal outcome conditions were relatively better among institutional cases when considering a comparatively lower perinatal mortality rate and fewer maternal complications. However, these slightly better results were associated with a high intervention rate. However, further research may be needed if this difference is being observed due to less detection of risk groups.
Midwives should be regularly trained regarding strict clinical guidelines to precisely identify danger signs of imminent complications and upon those conditions pursue immediate hospital transfer to successfully avoid avoidable complications. More detailed statistical evidence will probably promote an exploration of the way to further improve the homebirth conditions in Hungary. Moreover, considering the experiences of countries with long-lasting practices of homebirth would support one in reaching the highest level of this significant human event at home.
Author Contributions
Conceptualization, G.A.W., V.P., G.M.C. and P.T.; methodology, G.A.W., V.P. and P.T.; software, validation, formal analysis, data curation, writing—original draft preparation, G.A.W., V.V. and P.T.; writing—review and editing, G.A.W., V.P., V.V. and P.T.; visualization, supervision, V.P.; K.K.; G.M.C. and P.T. All authors have read and agreed to the published version of the manuscript.
Funding
This research was supported by The National Laboratory on Human Reproduction and by the RRF 2.3.1-21-2022-00012 Fund.
Institutional Review Board Statement
This study received ethical approval and was assigned an approval number, KK/608-1/2021, from the University of Pecs, Ethics Committee. It was conducted in full accordance with the Helsinki Declaration, and it adhered to the mandates of the general authorization to process personal data for scientific research purposes by the Hungarian Data Protection Authority. The need for informed consent, according to national legislation, was waived by the IRB, since this was a retrospective cohort study.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data that support the findings of this study (Tauffer database) are available; however, certain restrictions apply regarding the availability of these data, which were used under license for the current study, and are, therefore, not publicly available.
Acknowledgments
We acknowledge Sára Jeges for her valuable contributions and technical assistance during data processing and analysis. We also wish to extend our appreciation to Abraham Sahlemichael for his statistical advice and general contribution in support of our study.
Conflicts of Interest
The authors declare no conflict of interest. The funding sources did not have a role in the study design, collection, analysis, and interpretation of data, or in writing and submitting this manuscript.
References
- Catling-Paull, C.; Foureur, M.J.; Homer, C.S.E. Publicly-Funded Homebirth Models in Australia. Women Birth 2012, 25, 152–158. [Google Scholar] [CrossRef] [PubMed]
- Sassine, H.; Burns, E.; Ormsby, S.; Dahlen, H.G. Why Do Women Choose Homebirth in Australia? A National Survey. Women Birth 2021, 34, 396–404. [Google Scholar] [CrossRef] [PubMed]
- United Nations. Children Fund Maternal and Newborn Health and COVID-19—UNICEF DATA 2020; United Nations: New York, NY, USA, 2020. [Google Scholar]
- Definition of Homebirth. Available online: https://www.dictionary.com/browse/homebirth (accessed on 11 August 2022).
- Médecins Sans Frontières(MSF). Women Face Greater Danger during Coronavirus COVID-19 Pandemic. Available online: https://www.msf.org/women-and-girls-face-greater-dangers-during-covid-19-pandemic (accessed on 11 January 2022).
- Rajbanshi, S.; Norhayati, M.N.; Hussain, N.; Hazlina, N. A Qualitative Study to Explore the Barriers for Nonadherence to Referral to Hospital Births by Women with High-Risk Pregnancies in Nepal. Int. J. Environ. Res. Public Health Artic. J Env. Res Public Health 2021, 18, 5801. [Google Scholar] [CrossRef] [PubMed]
- Opdam, F.; van Dillen, J.; de Vries, M.; Hollander, M. How to Make the Hospital an Option Again: Midwives’ and Obstetricians’ Experiences with a Designated Clinic for Women Who Request Different Care than Recommended in the Guidelines. Int. J. Environ. Res. Public. Health 2021, 18, 1627. [Google Scholar] [CrossRef]
- De Freytas-Tamira, K. Pregnant and Scared of ‘Covid Hospitals,’ They’re Giving Birth at Home. The New York Times. 21 April 2020. Available online: https://www.nytimes.com/2020/04/21/nyregion/coronavirus-home-births.html (accessed on 11 January 2022).
- World Health Organization. Intrapartum Care for a Positive Childbirth Experience; World Health Organizaton: Geneva, Switzerland, 2018; ISBN 9789241550215.
- Center for Disease Control and Prevention. Pregnancy Complications. Maternal and Infant Health. Reproductive Health. 2018. Available online: https://www.cdc.gov/reproductivehealth/maternalinfanthealth/pregnancy-complications.html (accessed on 3 July 2022).
- Ilori, I.U.; Ituen, A.M.; Eyo, C.S. Factors Associated with Mortality in Neonatal Surgical Emergencies in a Developing Tertiary Hospital in Nigeria. Open J. Pediatr. 2013, 3, 231–235. [Google Scholar] [CrossRef]
- Katz, J.; Lee, A.C.C.; Kozuki, N.; Lawn, J.E.; Cousens, S.; Blencowe, H.; Ezzati, M.; Bhutta, Z.A.; Marchant, T.; Willey, B.A.; et al. Mortality Risk in Preterm and Small-for-Gestational-Age Infants in Low-Income and Middle-Income Countries: A Pooled Country Analysis. Lancet 2013, 382, 417–425. [Google Scholar] [CrossRef]
- Hanson, M.A.; Gluckman, P.D. Early Developmental Conditioning of Later Health and Disease: Physiology or Pathophysiology? Physiol. Rev. 2014, 94, 1027–1076. [Google Scholar] [CrossRef]
- Symon, A. Clemency for Hungarian Homebirth Midwife Ágnes Geréb. Br. J. Midwifery 2018, 26, 618–619. [Google Scholar] [CrossRef]
- Szigeti, T. Amid Controversy, Home-Birth Midwife and Activist Ágnes Geréb Sentenced to Two Years in Prison. Hungary Today, 11 January 2018. [Google Scholar]
- WHO. Essential Values and Fundamental Principles, Fundamental Law of Hungary. Law Fundam. Xx Artic. Cliv Act Care Health. 2015. Available online: https://tasz.hu/files/tasz/imce/alternative_translation_of_the_draft_constituion.pdf (accessed on 3 July 2022).
- The Privacy Act Regulation and Protection Group of Hungary. Hungary: Essential Values and Fundamental Principles; The Privacy Act Regulation and Protection Group of Hungary: Budapest, Hungary, 2011. [Google Scholar]
- Eggermont, M. News & Views: The Choice of Child Delivery Is a European Human Right. Eur. J. Health Law 2012, 19, 257–269. [Google Scholar] [CrossRef]
- Galera-Barbero, T.M.; Aguilera-Manrique, G. Planned Home Birth in Low-Risk Pregnancies in Spain: A Descriptive Study. Int. J. Environ. Res. Public. Health 2021, 18, 3784. [Google Scholar] [CrossRef]
- Kooy, J.; Birnie, E.; Denktas, S.; Steegers, E.A.P.; Bonsel, G.J. Planned Home Compared with Planned Hospital Births: Mode of Delivery and Perinatal Mortality Rates, an Observational Study. BMC Pregnancy Childbirth 2017, 17, 177. [Google Scholar] [CrossRef]
- Saxell, L.; Harris, S.; Elarar, L. The Collaboration for Maternal and Newborn Health: Interprofessional Maternity Care Education for Medical, Midwifery, and Nursing Students. J. Midwifery Womens Health 2009, 54, 314–320. [Google Scholar] [CrossRef]
- Vedam, S.; Leeman, L.; Cheyney, M.; Fisher, T.J.; Myers, S.; Low, L.K.; Ruhl, C. Transfer from Planned Home Birth to Hospital: Improving Interprofessional Collaboration. J. Midwifery Womens Health 2014, 59, 624–634. [Google Scholar] [CrossRef]
- Reeves, S.; Xyrichis, A.; Zwarenstein, M. Teamwork, Collaboration, Coordination, and Networking: Why We Need to Distinguish between Different Types of Interprofessional Practice. J. Interprof. Care 2018, 32, 1–3. [Google Scholar] [CrossRef]
- Ohta, R.; Ryu, Y.; Yoshimura, M. Realist Evaluation of Interprofessional Education in Primary Care through Transprofessional Role Play: What Primary Care Professionals Learn Together. Educ. Prim. Care 2021, 32, 91–99. [Google Scholar] [CrossRef]
- The Guardian The Right to a Home Birth in Hungary. The Guardian. 9 November 2010. Available online: https://www.theguardian.com/world/2010/nov/09/home-birth-in-hungary (accessed on 23 January 2022).
- Rigg, E.C.; Schmied, V.; Peters, K.; Dahlen, H.G. A Survey of Women in Australia Who Choose the Care of Unregulated Birthworkers for a Birth at Home. Women Birth 2020, 33, 86–96. [Google Scholar] [CrossRef]
- Zsirai, L.; Csákány, G.M.; Vargha, P.; Fülöp, V.; Tabák, Á.G. Breech Presentation: Its Predictors and Consequences. An Analysis of the Hungarian Tauffer Obstetric Database (1996–2011). Acta Obstet. Gynecol. Scand. 2016, 95, 347–354. [Google Scholar] [CrossRef]
- International Statistical Classification of Diseases and Related Health Problems 10th Revision (ICD-10). 10th ICD-10-CM Codes for Pregnancy, Childbirth and the Puerperium. 2021. Available online: https://icd.who.int/browse10/2019/en#/XV (accessed on 3 July 2021).
- APA Guidelines: Part A: Reporting Results of Common Statistical Tests in APA Format. Statistics 2010, 5, 1–8.
- Abraha, I.; Cherubini, A.; Cozzolino, F.; De Florio, R.; Luchetta, M.L.; Rimland, J.M.; Folletti, I.; Marchesi, M.; Germani, A.; Orso, M.; et al. Deviation from Intention to Treat Analysis in Randomised Trials and Treatment Effect Estimates: Meta-Epidemiological Study. BMJ 2015, 350, h2445. [Google Scholar] [CrossRef]
- Ministry of Health NZ. Report on Maternity Web Tool. Available online: https://www.health.govt.nz/publication/report-maternity-web-tool (accessed on 18 January 2022).
- Australian Institute of Health and Welfare. Australia’s Mothers and Babies 2018—In Brief, Summary—Australian Institute of Health and Welfare. Available online: https://www.aihw.gov.au/reports/mothers-babies/australias-mothers-and-babies-2018-in-brief/summary (accessed on 18 January 2022).
- Office for National Statistics. Birth Characteristics in England and Wales. 2020. Available online: https://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/livebirths/bulletins/birthcharacteristicsinenglandandwales/2020 (accessed on 18 January 2022).
- Edqvist, M.; Blix, E.; Hegaard, H.K.; Ólafsdottir, O.Á.; Hildingsson, I.; Ingversen, K.; Mollberg, M.; Lindgren, H. Perineal Injuries and Birth Positions among 2992 Women with a Low Risk Pregnancy Who Opted for a Homebirth. BMC Pregnancy Childbirth 2016, 16, 196. [Google Scholar] [CrossRef]
- Bolten, N.; de Jonge, A.; Zwagerman, E.; Zwagerman, P.; Klomp, T.; Zwart, J.J.; Geerts, C.C. Effect of Planned Place of Birth on Obstetric Interventions and Maternal Outcomes among Low-Risk Women: A Cohort Study in the Netherlands. BMC Pregnancy Childbirth 2016, 16, 329. [Google Scholar] [CrossRef]
- De Jonge, A.; Mesman, J.A.J.M.; Manniën, J.; Zwart, J.J.; Van Dillen, J.; Van Roosmalen, J. Severe Adverse Maternal Outcomes among Low Risk Women with Planned Home versus Hospital Births in the Netherlands: Nationwide Cohort Study. BMJ Online 2013, 346, f3263. [Google Scholar] [CrossRef] [PubMed]
- Christensen, L.F.; Overgaard, C. Are Freestanding Midwifery Units a Safe Alternative to Obstetric Units for Low-Risk, Primiparous Childbirth? An Analysis of Effect Differences by Parity in a Matched Cohort Study. BMC Pregnancy Childbirth 2017, 17, 14. [Google Scholar] [CrossRef] [PubMed]
- Londero, A.P.; Rossetti, E.; Pittini, C.; Cagnacci, A.; Driul, L. Maternal Age and the Risk of Adverse Pregnancy Outcomes: A Retrospective Cohort Study. BMC Pregnancy Childbirth 2019, 19, 261. [Google Scholar] [CrossRef] [PubMed]
- Shan, D.; Qiu, P.Y.; Wu, Y.X.; Chen, Q.; Li, A.L.; Ramadoss, S.; Wang, R.R.; Hu, Y.Y. Pregnancy Outcomes in Women of Advanced Maternal Age: A Retrospective Cohort Study from China. Sci. Rep. 2018, 8, 12239. [Google Scholar] [CrossRef] [PubMed]
- McMahon, C.A.; Boivin, J.; Gibson, F.L.; Hammarberg, K.; Wynter, K.; Saunders, D.; Fisher, J. Age at First Birth, Mode of Conception and Psychological Wellbeing in Pregnancy: Findings from the Parental Age and Transition to Parenthood Australia (PATPA) Study. Hum. Reprod. 2011, 26, 1389–1398. [Google Scholar] [CrossRef] [PubMed]
- Beaujouan, É.; Sobotka, T. Late Childbearing Continues to Increase in Developed Countries. Popul. Soc. 2019, 562, 1–4. [Google Scholar]
- Bliddal, M.; Broe, A.; Pottegård, A.; Olsen, J.; Langhoff-Roos, J. The Danish Medical Birth Register. Eur. J. Epidemiol. 2018, 33, 27–36. [Google Scholar] [CrossRef]
- Salustiano, E.M.A.; Campos, J.A.D.; Ibidi, S.M.; Ruano, R.; Zugaib, M. Low Apgar Scores at 5 Minutes in a Low Risk Population: Maternal and Obstetrical Factors and Postnatal Outcome. Rev. Assoc. Méd. Bras. 2012, 58, 587–593. [Google Scholar] [CrossRef]
- Chandra, I.; Sun, L. Third Trimester Preterm and Term Premature Rupture of Membranes: Is There Any Difference in Maternal Characteristics and Pregnancy Outcomes? J. Chin. Med. Assoc. 2017, 80, 657–661. [Google Scholar] [CrossRef]
- Reitsma, A.; Simioni, J.; Brunton, G.; Kaufman, K.; Hutton, E.K. Maternal Outcomes and Birth Interventions among Women Who Begin Labour Intending to Give Birth at Home Compared to Women of Low Obstetrical Risk Who Intend to Give Birth in Hospital: A Systematic Review and Meta-Analyses. EClinicalMedicine 2020, 21, 100319. [Google Scholar] [CrossRef]
- Blix, E.; Kumle, M.; Kjærgaard, H.; Øian, P.; Lindgren, H.E. Transfer to Hospital in Planned Home Births: A Systematic Review. BMC Pregnancy Childbirth 2014, 14, 179. [Google Scholar] [CrossRef]
- Fisher, J.; Wynter, K.; Hammarberg, K.; McBain, J.; Gibson, F.; Boivin, J.; McMahon, C. Age, Mode of Conception, Health Service Use and Pregnancy Health: A Prospective Cohort Study of Australian Women. BMC Pregnancy Childbirth 2013, 13, 88. [Google Scholar] [CrossRef]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).