Abstract
Objective: This study intended to examine the effects of Pilates exercise on pain, cardiorespiratory fitness, functional ability, and quality of life in children with polyarticular juvenile idiopathic arthritis. Methods: Forty children with polyarticular JIA aged 10–14 years old were randomly allocated into two groups: the control group (n = 20) received conventional physical therapy (CPT), and the experimental group (n = 20) received clinical Pilates exercises combined with CPT. Patients in both groups received their program three times/week for 3 months. Pain, cardiorespiratory fitness, functional ability, and quality of life were assessed through the visual analogue scale, cardiopulmonary exercise test, 6 min walk test, and PedsQL scale, respectively, just before and after treatment. Results: Pain (p = 0.001), cardiorespiratory markers (all p < 0.05), functional ability (p = 0.002), and overall quality of life (p = 0.007) improved significantly in the experimental groups compared to the control group. Conclusion: Incorporating Pilates exercises into CPT is likely more effective for decreasing pain intensity, improving cardiorespiratory fitness, augmenting functional ability, and promoting quality of life in children with JIA than CPT alone.
1. Introduction
Juvenile idiopathic arthritis (JIA) is one of the most common chronic childhood inflammatory diseases and is characterized by permanent joint inflammation attributable to immune system disturbance [1]. The inflammation starts before the patient reaches the age of 16, and the symptoms remain for at least 6 weeks [2]. JIA affects about 1 in every 1000 children of both sexes, with a greater incidence among girls. JIA comprises a heterogeneous group of disorders (specifically, oligoarticular, polyarticular, and systemic JIA), all of which show signs of joint inflammation, but their clinical presentation, illness progression, and prognosis are different [3]. Children with polyarticular JIA (i.e., have arthritis in more than five joints) have an extended refractory course of active disease and a greater risk of joint damage in comparison to children with other JIA subtypes [4].
Children with JIA often present with pain, morning stiffness, and swelling in the involved joints. They also experience muscle weakness and atrophy around the inflamed joints and activity limitations [5]. Moreover, patients with JIA have been shown to have a low aerobic fitness level, which results from a combination of factors related to the disease pathology and the usage of steroids [6]. Other possible causative factors of diminished aerobic capacity are reduced physical activity levels and physical deconditioning arising from pain, muscular weakness, joint stiffness, and decreased cardiac output [7].
Impaired aerobic fitness and lower levels of physical function during the active stage of the disease lead to functional declines among children with JIA [8]. Further, even during the inactive phase, fear of exercises and the belief that they are detrimental to the joints as well as a lack of understanding about their benefits results in functional limitations. Furthermore, social isolation, which is frequent in chronic diseases, may contribute to inactivity and decreased functional ability in JIA patients [9]. The chronicity of the disease, physical activity difficulties, and pain are all known to reduce health-related quality of life (HRQOL) among children with JIA and their caregivers [10]. According to Haverman et al. (2012), children with JIA showed a decline across the core quality of life domains—the physical, psychological, and social domains [11].
Therapeutic exercises play an essential role as a non-pharmacologic treatment for children with JIA. They have been effectively used to reduce pain, improve muscular function, increase physical activity, and promote quality of life in children with chronic musculoskeletal disorders [12]. Pilates is a type of exercise that focuses on developing stability, muscle control, muscle strength, flexibility, respiration, and posture by combining body–mind–spirit interaction [13]. Clinical Pilates exercise is usually perceived as an enjoyable activity by children with JIA; thereby, it can help them be more active for extended periods without causing discomfort while also allowing them to control their breathing and avoid becoming fatigued [14].
Although evidence is mounting for the beneficial effects of Pilates exercises on the cardiorespiratory fitness and physical activity level in healthy people and different patients (such as COPD, obesity, ankylosing spondylitis, and cystic fibrosis patients) [15,16,17], studies that have examined its effects in children with JIA are very limited. As such, the purpose of this study was to compare the effect of Pilates exercises plus conventional physical therapy versus conventional physical therapy alone on pain, cardiorespiratory fitness, functional status, and quality of life in children with polyarticular JIA. We hypothesized that the combined intervention would result in more favorable changes in all outcome measures compared to conventional physical therapy alone.
2. Materials and Methods
2.1. Study Design
This randomized, controlled clinical trial was conducted between August 2020 and July 2021 in the physical therapy outpatient clinic at the College of Applied Medical Sciences, Prince Sattam bin Abdulaziz University (PSAU), Saudi Arabia. PSAU’s Physical Therapy Research Ethics Committee (No: RHPT/0020/0035) provided ethical approval. Study measures were performed in agreement with the Declaration of Helsinki 1975 ethical standards for medical research. Before enrollment, all procedures were fully demonstrated to all patients and their caregivers. They were then requested to sign a consent form. A researcher who was not aware of treatment assignment evaluated pain severity, cardiorespiratory fitness, physical activity level, and quality of life before and after the intervention. This trial was registered at ClinicalTrials.gov (ID: NCT05231057).
2.2. Subjects
Patients were enrolled from the Maternity and Children’s Hospital and King Khalid Hospital (Pediatric Rheumatology Department) in Al-Kharj, Saudi Arabia. Inclusion criteria were as follows: polyarticular JIA according to the classification of International League of Associations for Rheumatology [18], age range from 10 to14 years old, and stable medical treatment. Subjects were excluded if they had contractures or congenital anomalies, history of surgery or systemic disease, or cardiorespiratory co-morbidities and participated in regular exercises or sports activity.
2.3. Assignment Procedure
Forty patients met the criteria. Following the baseline examination, they were divided into two equal-sized groups at random. Conventional physical therapy (CPT) was administered to the control group (n = 20), while Pilates exercises plus the conventional physical therapy program were administered to the experimental group (n = 20). An independent researcher used a simple randomization approach in which sealed non-transparent envelopes included a code for one of the two experimental sets (control or experimental). These were drawn to determine intervention assignment for each participant.
2.4. Outcome Measures
Pain, cardiorespiratory fitness, functional ability, and quality of life were evaluated just before and directly after the treatment by a pediatric physical therapy researcher who was blinded to the treatment procedures of both groups.
2.5. Primary Outcome Measures
2.5.1. Pain Assessment
Pain severity was measured using a 10 cm visual analog scale (VAS), with 0 demonstrating no pain or discomfort and 10 indicating the strongest pain experience. Participants were instructed to cut the line at a point that represented how much pain they felt at rest and/or during activity [19].
2.5.2. Cardiorespiratory Fitness Assessment
A graded cardiopulmonary exercise test was used to assess cardiopulmonary fitness. An electromagnetic cycle ergometer with electronic braking (ER900; Ergoline, Bitz, Germany) was used to assess the peak oxygen uptake (peak VO2), maximum heart rate (HRmax), and breath-by-breath minute ventilation (VE) according to the McMaster incremental cycle protocol [20]. Before starting the test, a simple demonstration was provided to each patient to familiarize them with the test measures. They were advised to avoid heavy meals or drinking caffeine three hours before testing and to wear light, comfortable clothing and shoes during test procedures. The test consisted of a conventional cycling rate of 50–70 rpm, beginning with a 25-watt load and increasing by 25 or 50 watts at 120 s breaks according to the tallness and sex of the participant. A 3 min active rest period at a training intensity of 25 watts was allowed at the end of the test, followed by a passive rest period of 3 min.
2.6. Secondary Outcome Measures
2.6.1. Functional Ability Assessment
Functional ability status was assessed using the Childhood Health Assessment Questionnaire (CHAQ-38). It assesses nine domains: dressing, grooming, getting out of bed, eating, ambulation, self-hygiene, grip reach, activities, and extra-curricular events. The results were transformed to a CHAQ disability score ranging from 0 to 3 (a higher mark indicates a higher level of disability) [21].
2.6.2. Quality of Life
The self-reported Pediatric Quality of Life Inventory was used to assess quality of life (PedsQL). PedsQL is a 23-item multidimensional measure of health-related quality of life (HRQL) in children and adolescents and is divided into 4 areas (physical: 8 items, emotional: 5 items, social: 5 items, and school functions: 3 items). This questionnaire has been approved for usage with kids and adolescents aged 2 to 18 years old [22]. On a 5-point scale, each item was rated (0 means never, and 4 means almost always). Items were converted to a 0–100 scale on a linear scale (0 = 100, 1 = 75, 2 = 50, 3 = 25, and 4 = 0). In this study, the physical health summary score was calculated by summing physical function item scores and dividing the total score by the number of rated items. Psychosocial health summary score was calculated by summing item scores of emotional, social, and school functions then dividing the total score by the number of rated items. The total summary score was calculated by summing all item scores in all domains (physical and psychosocial) and dividing the total score by the number of rated items). Greater scores equated to a higher quality of life.
2.6.3. Conventional Physical Therapy Program (CPT)
All children in the two groups underwent the conventional PT program (40 min per session, 3 sessions each week over 3 months), which was delivered by a pediatric physical therapist. The key priorities were reliving pain, increasing flexibility and mobility, improving muscle strength, and promoting proprioceptive awareness as well as increasing aerobic fitness. In general, the program consists of pain reliving modalities, stretching exercises, active range of motion activities, weight bearing activities, aerobic exercises on a treadmill or a bicycle, and isometric exercises [23,24,25].
2.6.4. Pilates Exercises
Pilates exercises (25 min each session, 3 sessions each week over 3 months) were administered to patients in the experimental group by a pediatric physical therapist. Mats, Pilates bands or elastic bands, and Pilates ball are some of the several types of equipment used in Pilates exercises to attain various goals [26,27]. Detailed description of Pilates exercises is shown in Table 1.

Table 1.
Pilates exercises.
2.6.5. Sample Size Calculation
The analysis was conducted using G*Power program version 3.0.10 (Neu-Isenburg, Germany). A group sample size of 16 (totaling 32 for both groups) was needed to achieve 81.23% power to reject the null hypothesis of zero effect size on pain intensity when the population effect size is too small (Cohen’s d = 1.04; as calculated in a pilot study of eight children who received similar interventions). The significance level was 0.05 using a two-sided independent t-test. To account for a potential dropout rate of 20%, the sample size was increased to 40 (that is, 20 in each group).
2.6.6. Data Analysis
Data analyses were conducted with SPSS version 21 (SPSS Inc., Chicago, IL, USA). The Kolmogorov–Smirnov test was used to determine data normality. An independent t-test (for continuous data) and a Chi-square test (for categorical data) were used to assess baseline differences between the IMT and control groups. The analysis of covariance (ANCOVA) test was used to calculate the post-treatment differences between the two groups (for primary and secondary outcome variables). To compare the two groups, the pre-treatment values of the dependent outcome variables were employed as covariates. The partial eta-squared equation was used to calculate the effect size (ES) for the significant ANCOVA. For all statistical tests, the level of significance was set at p < 0.05.
3. Results
Recruitment and Retention of Participants
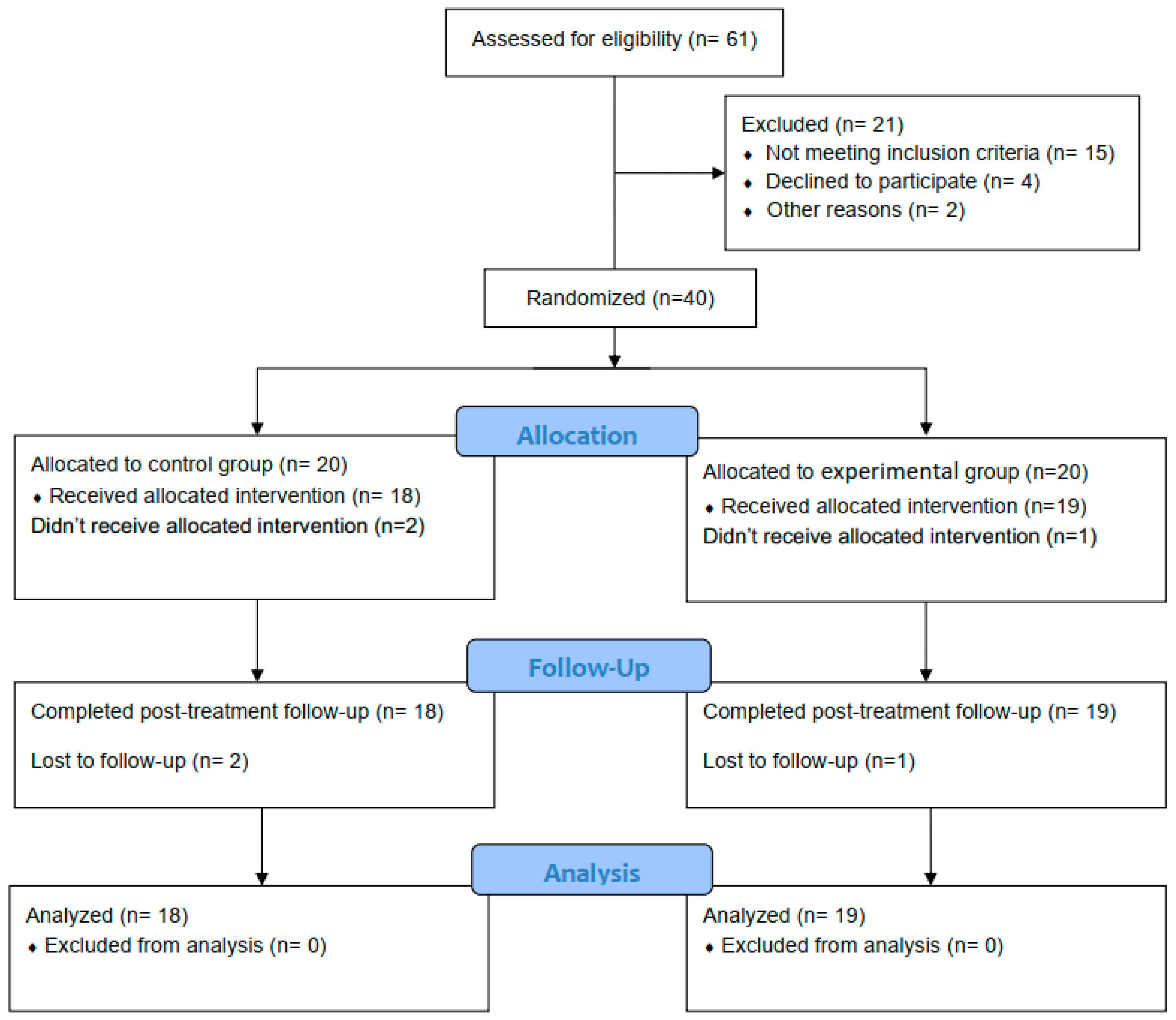
The children involved in the current study were screened for eligibility. Out of 61 possibly eligible children, 40 participants met the criteria for inclusion and were randomly assigned to either the control or the experimental group. Three children did not complete the study (one from the experimental group and two from the control group). The CONSORT flow chart is explained in Figure 1. The baseline demographic and clinical characteristics for each group are presented in Table 2. Additionally, the primary/secondary outcome measures in both groups at the pre-treatment point are shown in Table 3.
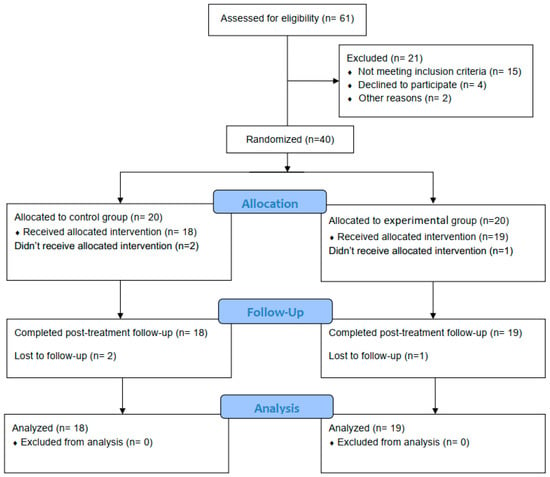
Figure 1.
Participants’ CONSORT flowchart.
Table 2.
Demographic and clinical characteristics of children in the IMT and control groups.
Table 3.
Primary/secondary outcome measures in the experimental and control group at the pre-treatment point.
Table 4 shows the post-treatment differences in the outcome variables between the experimental and control groups, which were controlled for pre-treatment values. In terms of pain intensity, there was a large significant difference between both groups in regard to the VAS scores (F (1, 34) = 12.23, p = 0.001, ES = 0.92), which were in favor of the experimental group. In addition, there were large significant differences in the cardiopulmonary fitness between the two groups, as measured by the peak VO2 (F (1, 34) = 8.45, p = 0.008, ES = 0.81), VE (F (1, 34) = 11.16, p = 0.002, ES = 0.90), and HRmax (F (1, 34) = 6.39, p = 0.004, ES = 0.84), where the experimental group showed better cardiopulmonary fitness than the control group.
Table 4.
Post-treatment differences in primary/secondary outcome measures between the experimental and control group: controlled for pre-treatment values.
Further, there was a large significant difference between the two groups concerning their functional status (F (1, 34) = 10.75, p = 0.002, ES = 0.89), as the mean CHAQ score was lower in the experimental group in comparison to the control group. Still, there were significant differences in the quality-of-life domains between both groups: the physical dimension (F (1, 34) = 7.21, p = 0.011, ES = 0.74), psychosocial dimension (F (1, 34) = 5.17, p = 0.029, ES = 0.59), and total scores (F (1, 34) = 8.20, p = 0.007, ES = 0.79) were all in favor of the experimental group.
4. Discussion
The current study was designed to evaluate the influence of Pilates exercises besides conventional physical therapy on pain, cardiorespiratory fitness, physical activity level, and quality of life in children with polyarticular JIA. Our results revealed that combining Pilates exercises with a conventional physical therapy program yielded favorable outcomes regarding the reduction in pain perception, the improvement of cardiorespiratory fitness, increasing the physical activity level, and the enhancement of quality of life.
The role of Pilates exercises in relieving pain may be attributed to the breathing exercises, which are a main component of Pilates, as breathing exercises improve lung capacity, blood oxygenation, and circulation. Pilates also encourages the brain to release normal endorphins and opiates, which reduces pain and stress [28]. Increased body flexibility may be a causative factor of decreasing pain as reported by Segal et al. [29], who reported that Pilates exercises increase flexibility, reduce muscle tension during exercise, reduce muscle aches, improve physical performance, and reduce the energy cost of joint movements. Our results are consistent with review research by Wells et al. [13], which concluded that Pilates exercises decrease pain intensity and increase functional ability in patients with low back pain more than traditional physical therapy programs. The results of this study are in agreement with research conducted by Unal et al. to examine the consequence of clinical Pilates exercises on JIA children, concluding that there was a positive impact of Pilates exercises on decreasing pain intensity and improving function and overall health status [14].
One possible explanation for the constructive effect of our results is the weekly exposure to the exercises, as the two interventions (Pilates + CPT) were delivered to improve cardiorespiratory fitness. The strengthening of the lumbopelvic region and core muscles that occurred during the exercises may have led to a better movement pattern in the limbs and better strength in the expiratory muscles [30]. Another cause may be due to the increased mobility of the rib cage and intercostal muscles during breathing exercises, which can lead to a more efficient breathing pattern, improved ventilation efficiency, greater flow of oxygenated blood into muscle, and improved pulmonary functions [31].
The results of our study are also in line with the study conducted by Souza et al. to investigate the effect of cardiorespiratory adaptation to Pilates training. They concluded that 15 successive weeks of Pilates training has a positive impact on cardiorespiratory factors such as VO2 max and ventilatory thresholds in sedentary women with decreased respiratory capacity levels [32]. Our results are also in agreement with Niehues, who concluded that Pilates exercises increase the strength of the abdominal muscles, which could be the cause of improvements in diaphragmatic function, enhancements in respiratory function, and improvements in cardiorespiratory fitness [33].
Our results also showed that 3 months of clinical Pilates exercises in adolescents with JIA improved their functional status. This improvement may be associated with reduced pain intensity and improved aerobic capacity. We verified this claim through a finding of a study by Limenis et al., who studied the association between physical activity levels and functional status with pain in JIA children and concluded that there was an inverse relationship between pain severity and functional activity level [34]. A study by Lelieveld et al. studied the functional activity in adolescents with JIA, and the results of this study show that a higher level of functional activity is related to a low pain level and a high level of well-being. PA is also associated with fitness level, as a decreased fitness level might be the cause for deconditioning and lower function [6].
The results of our current study revealed that there was enhancement in the HRQOL in children with JIA, and these results are consistent with the results of Calik et al., who stated that clinical Pilates exercises increase mobility in children and adolescents with JIA, making them more active in daily activities. This has enables them to improve their overall quality of life [27]. Our results are also in agreement with Mendonça et al., who concluded that the physical and psychosocial aspects of the HRQOL were positively improved in groups treated with Pilates exercises when compared to groups treated with a conventional physical therapy program [35].
Although the results of this study are mostly positive, there are some limitations that affect the generalizability of the results. First, the lack of long-term follow-up means further research is required to study the effects of Pilates exercises after 6–12 months. Second, a small sample size and relatively low power mean further studies are required to examine the influence of Pilates exercises on a large sample, thus resulting in more solid conclusions. Special consideration should be given when generalizing these findings, as this study was conducted on patients with only one specific type of polyarticular JIA and in one specific age group. As such, more research is desirable to explore the impact of Pilates exercises combined with a conventional physical therapy program on other types of JIA and on different age groups of children with JIA.
5. Conclusions
Notwithstanding the relatively limited sample, this work suggests that the incorporation of Pilates exercises into physical therapy programs is likely an effective strategy for decreasing pain intensity, improving cardiorespiratory fitness, augmenting the physical activity level, and promoting HRQOL in children with JIA. However, large randomized controlled trials could provide more definitive evidence.
Author Contributions
Conceptualization, A.R.A., F.H.K., M.A.B. and R.K.E.; methodology, A.R.A. and R.K.E.; formal analysis, R.K.E. and F.H.K.; investigation, F.H.K., M.A.B., S.M.H. and N.F.E.; resources, M.A.B., S.M.A. and G.S.A.; data curation, F.H.K., S.M.A., G.S.A., S.M.H. and N.F.E.; writing—original draft preparation, M.A.B., S.M.A., G.S.A. and R.K.E.; writing—review and editing, A.R.A., F.H.K., S.M.H. and N.F.E.; supervision, A.R.A., M.A.B. and R.K.E.; project administration, A.R.A., M.A.B. and R.K.E. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
All study procedures were approved by the physical therapy research ethics committee of the physiotherapy department at Prince Sattam bin Abdulaziz University (No: RHPT/0020/0035).
Informed Consent Statement
Parents signed a written consent form once they approved their children’s participation in the study.
Data Availability Statement
The authors declare that all relevant data supporting the findings of the study are available within the manuscript.
Acknowledgments
The authors would like to gratefully acknowledge all of the parents who supported their children in participating in the study program.
Conflicts of Interest
The authors declare that they have no conflict of interest.
References
- Lin, Y.T.; Wang, C.T.; Gershwin, M.E.; Chiang, B.L. The pathogenesis of oligoarticular/polyarticular vs. systemic juvenile idiopathic arthritis. Autoimmun. Rev. 2011, 10, 482–489. [Google Scholar] [CrossRef] [PubMed]
- Merino, R.; De Inocencio, J.; García-Consuegra, J. Evaluation of revised International League of Associations for Rheumatology classification criteria for juvenile idiopathic arthritis in Spanish children (Edmonton 2001). J. Rheumatol. 2005, 32, 559–561. [Google Scholar] [PubMed]
- Ravelli, A.; Martini, A. Juvenile idiopathic arthritis. Lancet 2007, 369, 767–778. [Google Scholar] [CrossRef] [Green Version]
- Ringold, S.; Seidel, K.D.; Koepsell, T.D.; Wallace, C.A. Inactive disease in polyarticular juvenile idiopathic arthritis: Current patterns and associations. Rheumatology 2009, 48, 972–977. [Google Scholar] [CrossRef] [Green Version]
- Oen, K.; Duffy, C.M.; Tse, S.M.; Ramsey, S.; Ellsworth, J.; Chédeville, G.; Chetaille, A.L.; Saint-Cyr, C.; Cabral, D.A.; Spiegel, L.R.; et al. Early outcomes and improvement of patients with juvenile idiopathic arthritis enrolled in a Canadian multicenter inception cohort. Arthritis Care Res. 2010, 62, 527–536. [Google Scholar] [CrossRef]
- Lelieveld, O.T.; Armbrust, W.; Van Leeuwen, M.A.; Duppen, N.; Geertzen, J.H.; Sauer, P.J.; Van Weert, E. Physical activity in adolescents with juvenile idiopathic arthritis. Arthritis Care Res. 2008, 59, 1379–1384. [Google Scholar] [CrossRef]
- Takken, T.; Hemel, A.; van der Net, J.; Helders, P.J. Aerobic fitness in children with juvenile idiopathic arthritis: A systematic review. J. Rheumatol. 2002, 29, 2643–2647. [Google Scholar]
- Henderson, C.J.; Lovell, D.J.; Specker, B.L.; Campaigne, B.N. Physical activity in children with juvenile rheumatoid arthritis: Quantification and evaluation. Arthritis Care Res. 1995, 8, 114–119. [Google Scholar] [CrossRef]
- Malleson, P.; Bennett, S.M.; MacKinnon, M.; Jespersen, D.K.; Coutts, K.D.; Turner, S.P.; McKenzie, D.C. Physical fitness and its relationship to other indices of health status in children with chronic arthritis. J. Rheumatol. 1996, 23, 1059–1065. [Google Scholar]
- Gutierrez-Suarez, R.; Pistorio, A.; Cespedes Cruz, A.; Norambuena, X.; Flato, B.; Rumba, I.; Harjacek, M.; Nielsen, S.; Susic, G.; Mihaylova, D.; et al. Health-related quality of life of patients with juvenile idiopathic arthritis coming from 3 different geographic areas. The PRINTO multinational quality of life cohort study. Rheumatology 2007, 46, 314–320. [Google Scholar]
- Haverman, L.; Grootenhuis, M.A.; van den Berg, J.M.; van Veenendaal, M.; Dolman, K.M.; Swart, J.F.; Kuijpers, T.W.; van Rossum, M.A. Predictors of health-related quality of life in children and adolescents with juvenile idiopathic arthritis: Results from a web-based survey. Arthritis Care Res. 2012, 64, 694–703. [Google Scholar] [CrossRef] [PubMed]
- Singh-Grewal, D.; Wright, V.; Bar-Or, O.; Feldman, B.M. Pilot study of fitness training and exercise testing in polyarticular childhood arthritis. Arthritis Care Res. 2006, 55, 364–372. [Google Scholar] [CrossRef] [PubMed]
- Wells, C.; Kolt, G.S.; Bialocerkowski, A. Defining Pilates exercise: A systematic review. Complemen. Ther. Med. 2012, 20, 253–262. [Google Scholar] [CrossRef] [PubMed]
- Unal, E.; Dizmek, P.; Bilginer, Y.; Tayfur, A.C.; Besbas, N.; Ozen, S. The role of clinical pilates exercises in children wıth juvenile idiopathic arthritis: A pilot study. Pediatr. Rheumatol. 2011, 9, 117. [Google Scholar] [CrossRef] [Green Version]
- Cancelliero-Gaiad, K.M.; Ike, D.; Pantoni, C.B.; Borghi-Silva, A.; Costa, D. Respiratory pattern of diaphragmatic breathing and pilates breathing in COPD subjects. Braz. J. Phys. Ther. 2014, 18, 291–299. [Google Scholar] [CrossRef] [Green Version]
- Martínez-Pubil, J.A.; Acebal-González, A.; Álvarez, R.F.; Vega-Álvarez, J.A. Pilates en pacientes con espondilitis anquilosante: Repercusión en la función pulmonar. Fisioterapia 2017, 39, 250–256. [Google Scholar] [CrossRef]
- Franco, C.B.; Ribeiro, A.F.; Morcillo, A.M.; Zambon, M.P.; Almeida, M.B.; Rozov, T. Effects of Pilates mat exercises on muscle strength and on pulmonary function in patients with cystic fibrosis. J. Bras. Pneumol. 2014, 40, 521–527. [Google Scholar] [CrossRef] [Green Version]
- Hofer, M. Classification of childhood arthritis. Best Pract. Res. Clin. Rheumatol. 2002, 16, 379–396. [Google Scholar] [CrossRef]
- Burckhardt, C.S.; Jones, K.D. Adult Measures of Pain: The McGill Pain Questionnaire (MPQ). Arthritis Rheum. Arthritis Care Res. 2003, 49, S96–S104. [Google Scholar] [CrossRef]
- Bar-Or, O.; Rowland, T.W. Pediatric Exercise Medicine: From Physiologic Principles to Health Care Application; Human Kinetics: Champaign, IL, USA, 2004. [Google Scholar]
- Lam, C.; Young, N.; Marwaha, J.; McLimont, M.; Feldman, B.M. Revised versions of the Childhood Health Assessment Questionnaire (CHAQ) are more sensitive and suffer less from a ceiling effect. Arthritis Rheumatol. 2004, 51, 881–889. [Google Scholar] [CrossRef]
- Varni, J.W.; Seid, M.; Kurtin, P.S. PedsQL™ 4.0: Reliability and validity of the Pediatric Quality of Life Inventory™ Version 4.0 Generic Core Scales in healthy and patient populations. Med. Care 2001, 39, 800–812. [Google Scholar] [CrossRef]
- Elnaggar, R.K.; Mahmoud, W.S.; Moawd, S.A.; Azab, A.R. Impact of core stability exercises on bone mineralization and functional capacity in children with polyarticular juvenile idiopathic arthritis: A randomized clinical trial. Clin. Rheumatol. 2021, 40, 245–253. [Google Scholar] [CrossRef]
- Azab, A.R.; Hamed, A.S. Effect of Kinesio taping on balance in children with juvenile idiopathic arthritis. Life Sci. J. 2018, 15, 104–110. [Google Scholar]
- Azab, A.R.; Ibrahim, A.R.; Radwan, N.L. Effect of extracorporeal shockwave therapy on selected gait parameters in children with juvenile idiopathic arthritis. Int. J. Ther. Rehabil. Res. 2016, 5, 180. [Google Scholar] [CrossRef]
- Azab, A.R.; Abdelbasset, W.K.; Basha, M.A.; Mahmoud, W.S.; Elsayed, A.E.; Saleh, A.K.; Elnaggar, R.K. Incorporation of Pilates-based core strengthening exercises into the rehabilitation protocol for adolescents with patellofemoral pain syndrome: A randomized clinical trial. Eur. Rev. Med. Pharmacol. Sci. 2022, 26, 1091–1100. [Google Scholar]
- Calık, B.B.; Kabul, E.G.; Korkmaz, C.; Tekin, Z.E.; Yener, G.O.; Yuksel, S. The efficacy of clinical Pilates exercises in children and adolescents with juvenile idiopathic arthritis: A pilot study. Rev. Colomb. Reum. 2020, 27, 269–277. [Google Scholar]
- Jadhav, M.; Rao, K. Effect of Pilates on osteoarthritis of Knee. Int. J. Multidisc. Res. Dev. 2019, 3, 198–203. [Google Scholar]
- Segal, N.A.; Hein, J.; Basford, J.R. The effects of Pilates training on flexibility and body composition: An observational study. Arch. Phys. Med. Rehabil. 2004, 85, 1977–1981. [Google Scholar] [CrossRef]
- Finatto, P.; Silva, E.S.; Okamura, A.B.; Almada, B.P.; Oliveira, H.B.; Peyre-Tartaruga, L.A. Pilates training improves 5-km run performance by changing metabolic cost and muscle activity in trained runners. PLoS ONE 2018, 13, e0194057. [Google Scholar]
- Tinoco-Fernández, M.; Jiménez-Martín, M.; Sánchez-Caravaca, M.A.; Fernández-Pérez, A.M.; Ramírez-Rodrigo, J.; Villaverde-Gutiérrez, C. The Pilates method and cardiorespiratory adaptation to training. Res. Sports Med. 2016, 24, 266–271. [Google Scholar] [CrossRef]
- Souza, C.; Krüger, R.L.; Schmit, E.F.; Wagner Neto, E.S.; Reischak-Oliveira, Á.; de Sá, C.K.; Loss, J.F. Cardiorespiratory Adaptation to Pilates Training. Res. Q. Exerc. Sport 2021, 92, 453–459. [Google Scholar] [CrossRef]
- Niehues, J.R. Pilates method for lung function and functional capacity in obese adults. Altern. Ther. Health Med. 2015, 21, 73. [Google Scholar]
- Limenis, E.; Grosbein, H.A.; Feldman, B.M. The relationship between physical activity levels and pain in children with juvenile idiopathic arthritis. J. Rheumatol. 2014, 41, 345–351. [Google Scholar] [CrossRef]
- Mendonça, T.M.; Terreri, M.T.; Silva, C.H.; Neto, M.B.; Pinto, R.M.; Natour, J.; Len, C.A. Effects of Pilates exercises on health-related quality of life in individuals with juvenile idiopathic arthritis. Arch. Phys. Med. Rehabil. 2013, 94, 2093–2102. [Google Scholar] [CrossRef]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).