
Environmental Barriers and Functional Outcomes in Patients with Schizophrenia in Taiwan: The Capacity-Performance Discrepancy


 ,
,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. The Reconstruction of the Health and Social Welfare System in Certification of Disability and Care Needs in Taiwan
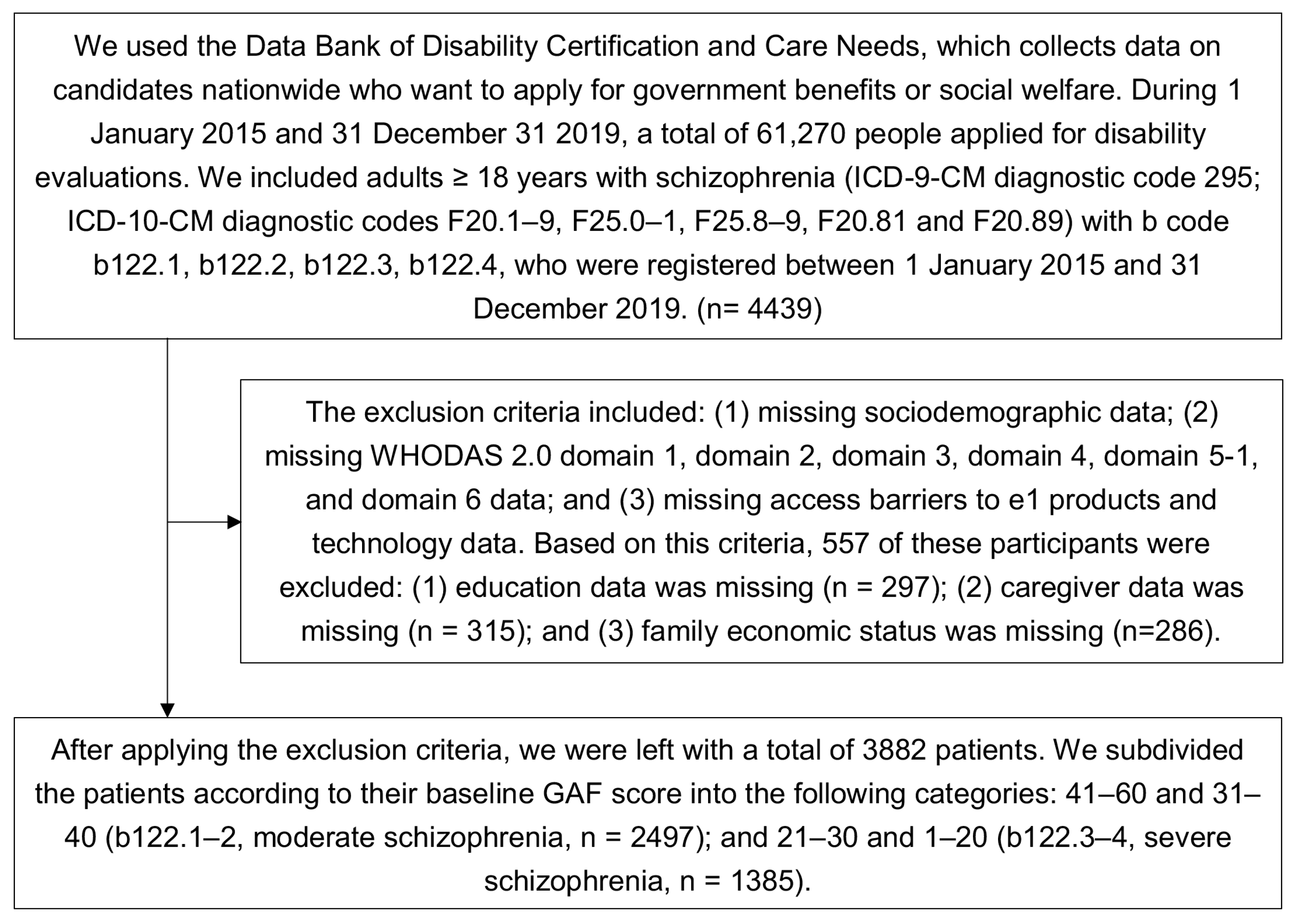
2.2. Study Participants and the Data including in the Data Bank of Certification of Disability and Care Needs
2.3. The Measurements of Summary Index (SI) of the WHODAS 2.0 Domain and the Capacity-Performance Discrepancy
2.4. Statistical Analysis
3. Results
4. Discussion
Study Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Horner-Johnson, W.; Dobbertin, K.; Lee, J.C.; Andresen, E.M. Disparities in chronic conditions and health status by type of disability. Disabil. Health J. 2013, 6, 280–286. [Google Scholar] [CrossRef]
- Ministry of Health and Welfare RoCT. The Disabled Population by Cause and Classification Taipei. 2021. Available online: https://dep.mohw.gov.tw/DOS/cp-2976-61124-113.html (accessed on 24 September 2021).
- Jablensky, A.; Sartorius, N.; Ernberg, G.; Anker, M.; Korten, A.; Cooper, J.E.; Day, R.; Bertelsen, A. Schizophrenia: Manifestations, incidence and course in different cultures. A World Health Organization ten-country study. Psychol. Med. Monogr. Suppl. 1992, 20, 1–97. [Google Scholar] [CrossRef]
- Liu, T.; Song, X.; Chen, G.; Paradis, A.D.; Zheng, X. Prevalence of schizophrenia disability and associated mortality among Chinese men and women. Psychiatry Res. 2014, 220, 181–187. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. The Global Burden of Disease: 2004 Update; World Health Organization: Geneva, Switzerland, 2008. [Google Scholar]
- Lêng, C.H.; Chou, M.H.; Lin, S.-H.; Yang, Y.K.; Wang, J.-D. Estimation of life expectancy, loss-of-life expectancy, and lifetime healthcare expenditures for schizophrenia in Taiwan. Schizophr. Res. 2016, 171, 97–102. [Google Scholar] [CrossRef] [PubMed]
- Świtaj, P.; Anczewska, M.; Chrostek, A.; Sabariego, C.; Cieza, A.; Bickenbach, J.; Chatterji, S. Disability and schizophrenia: A systematic review of experienced psychosocial difficulties. BMC Psychiatry 2012, 12, 193. [Google Scholar] [CrossRef]
- Gorostiaga, A.; Balluerka, N.; Guilera, G.; Aliri, J.; Barrios, M. Functioning in patients with schizophrenia: A systematic review of the literature using the International Classification of Functioning, Disability and Health (ICF) as a reference. Qual. Life Res. 2017, 26, 531–543. [Google Scholar] [CrossRef]
- Jones, S.H.; Thornicroft, G.; Coffey, M.; Dunn, G. A brief mental health outcome scale-reliability and validity of the Global Assessment of Functioning (GAF). Br. J. Psychiatry 1995, 166, 654–659. [Google Scholar] [CrossRef]
- Guilera, G.; Gómez-Benito, J.; Pino, O.; Rojo, J.E.; Cuesta, M.J.; Martínez-Arán, A.; Safont, G.; Tabares-Seisdedos, R.; Vieta, E.; Bernardo, M. Utility of the World Health Organization Disability Assessment Schedule II in schizophrenia. Schizophr. Res. 2012, 138, 240–247. [Google Scholar] [CrossRef] [PubMed]
- Holsbeeke, L.; Ketelaar, M.; Schoemaker, M.M.; Gorter, J.W. Capacity, capability, and performance: Different constructs or three of a kind? Arch. Phys. Med. Rehabil. 2009, 90, 849–855. [Google Scholar] [CrossRef]
- Menendez-Miranda, I.; Garcia-Portilla, M.P.; Garcia-Alvarez, L.; Arrojo, M.; Sanchez, P.; Sarramea, F.; Gomar, J.; Bobes-Bascaran, M.T.; Sierra, P.; Saiz, P.A.; et al. Predictive factors of functional capacity and real-world functioning in patients with schizophrenia. Eur. Psychiatry 2015, 30, 622–627. [Google Scholar] [CrossRef]
- Kurichi, J.E.; Kwong, P.L.; Xie, D.; Bogner, H.R. Predictive Indices for Functional Improvement and Deterioration, Institutionalization, and Death Among Elderly Medicare Beneficiaries. PM&R 2017, 9, 1065–1076. [Google Scholar] [CrossRef][Green Version]
- Norin, L.; Slaug, B.; Haak, M.; Jörgensen, S.; Lexell, J.; Iwarsson, S. Housing accessibility and its associations with participation among older adults living with long-standing spinal cord injury. J. Spinal Cord. Med. 2017, 40, 230–240. [Google Scholar] [CrossRef]
- Uchino, T.; Nemoto, T.; Yamaguchi, T.; Katagiri, N.; Tsujino, N.; Murakami, Y.; Tanaka, K.; Mizuno, M. Associations of personality traits with the capacity-performance discrepancy of functional outcome in patients with schizophrenia. Neuropsychiatr. Dis. Treat. 2019, 15, 2869–2877. [Google Scholar] [CrossRef]
- Harvey, P.D.; Strassnig, M. Predicting the severity of everyday functional disability in people with schizophrenia: Cognitive deficits, functional capacity, symptoms, and health status. World Psychiatry Off. J. World Psychiatr. Assoc. (WPA) 2012, 11, 73–79. [Google Scholar] [CrossRef] [PubMed]
- Chang, K.-H.; Lin, Y.-N.; Liao, H.-F.; Yen, C.-F.; Escorpizo, R.; Yen, T.-H.; Liou, T.-H. Environmental effects on WHODAS 2.0 among patients with stroke with a focus on ICF category e120. Qual. Life Res. 2014, 23, 1823–1831. [Google Scholar] [CrossRef]
- Lien, W.-C.; Guo, N.-W.; Chang, J.-H.; Lin, Y.-C.; Kuan, T.-S. Relationship of perceived environmental barriers and disability in community-dwelling elderly in Taiwan—A population-based study. BMC Geriatr. 2014, 14, 59. [Google Scholar] [CrossRef]
- World Health Organization. International Classification of Functioning, Disability and Health: ICF; World Health Organization: Geneva, Switzerland, 2001. [Google Scholar]
- Hoyle, M.; Gustafsson, L.; Meredith, P.; Ownsworth, T. Participation after stroke: Do we understand all the components and relationships as categorised in the ICF? Brain Impair. 2012, 13, 4–15. [Google Scholar] [CrossRef]
- Corring, D. Exploring schizophrenia within the framework of the International Classification of Functioning, Disability and Health (ICF); Research Insights of the Regional Mental Health Care: London, UK, 2005; Volume 3, pp. 1–43. [Google Scholar]
- Samuel, R.; Thomas, E.; Jacob, K. Instrumental activities of daily living dysfunction among people with schizophrenia. Indian J. Psychol. Med. 2018, 40, 134–138. [Google Scholar] [CrossRef] [PubMed]
- Lin, J.-D.; Yen, C.-F.; Loh, C.-H. Difficulties and suggestions for disability evaluation enforcement based on WHO-ICF in Taiwan: Exploratory findings. J. Dis. Res. 2009, 7, 1–18. (In Chinese) [Google Scholar] [CrossRef]
- WHO. WHO Disability Assessment Schedule 2.0; WHO: Geneva, Switzerland, 2011. [Google Scholar]
- WHO. ICF Browser; WHO: Geneva, Switzerland, 2013; Available online: https://apps.who.int/classifications/icfbrowser/ (accessed on 15 July 2021).
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders; American Psychiatric Association: Washington, DC, USA, 1980. [Google Scholar]
- Liu, C.Y.; Hung, Y.T.; Chuang, Y.L.; Chen, Y.J.; Weng, W.S.; Liu, J.S.; Liang, K.Y. Incorporating development stratification of Taiwan townships into sampling design of large scale health interview survey. J. Health Manag. 2006, 4, 1–22. (In Chinese) [Google Scholar]
- Metz, C.E. Quantification of failure to demonstrate statistical significance: The usefulness of confidence intervals. Investig. Radiol. 1993, 28, 59–63. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Lang, A.-G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- Kushel, M.B.; Gupta, R.; Gee, L.; Haas, J.S. Housing instability and food insecurity as barriers to health care among low-income Americans. J. Gen. Int. Med. 2006, 21, 71–77. [Google Scholar] [CrossRef]
- Judd, F.; Jackson, H.; Komiti, A.; Murray, G.; Fraser, C.; Grieve, A.; Gomez, R. Help-seeking by rural residents for mental health problems: The importance of agrarian values. Aust. N. Z. J. Psychiatry 2006, 40, 769–776. [Google Scholar] [CrossRef]
- Liu, T.; Zhang, L.; Pang, L.; Li, N.; Chen, G.; Zheng, X. Schizophrenia-related disability in China: Prevalence, gender, and geographic location. Psychiatr. Serv. 2015, 66, 249–257. [Google Scholar] [CrossRef]
- Kotwani, P.; Balzer, L.; Kwarisiima, D.; Clark, T.D.; Kabami, J.; Byonanebye, D.; Bainomujuni, B.; Black, D.; Chamie, G.; Jain, V.; et al. Evaluating linkage to care for hypertension after community-based screening in rural Uganda. Trop. Med. Int. Health 2014, 19, 459–468. [Google Scholar] [CrossRef]
- Chiu, W.-T.; Yen, C.-F.; Teng, S.-W.; Liao, H.-F.; Chang, K.-H.; Chi, W.C.; Wang, Y.-H.; Liou, T.-H. Implementing disability evaluation and welfare services based on the framework of the International Classification of Functioning, Disability and Health: Experiences in Taiwan. BMC Health Serv. Res. 2013, 13, 416. [Google Scholar] [CrossRef]
- Li, J.; Deng, Q.; Zhang, Y.; Wu, D.; Li, G.; Liu, J.; Zhang, L.; Wang, H.-M.D. Three novel dietary phenolic compounds from pickled Raphanus Sativus L. inhibit lipid accumulation in obese mice by modulating the gut microbiota composition. Mol. Nutr. Food Res. 2021, 65, 2000780. [Google Scholar] [CrossRef] [PubMed]
- Teng, Y.-N.; Chang, H.-C.; Chao, Y.-Y.; Cheng, H.-L.; Lien, W.-C.; Wang, C.-Y. Etoposide triggers cellular senescence by inducing multiple centrosomes and primary cilia in adrenocortical tumor cells. Cells 2021, 10, 1466. [Google Scholar] [CrossRef]
- Beal, G.; Veldhorst, G.; McGrath, J.-L.; Guruge, S.; Grewal, P.; DiNunzio, R.; Trimnell, J. Constituting community: Creating a place for oneself. Psychiatry 2005, 68, 199–211. [Google Scholar] [CrossRef]
- Lee, E.E.; Martin, A.S.; Kaufmann, C.N.; Liu, J.; Kangas, J.; Daly, R.E.; Tu, X.M.; Depp, C.A.; Jeste, D.V. Comparison of schizophrenia outpatients in residential care facilities with those living with someone: Study of mental and physical health, cognitive functioning, and biomarkers of aging. Psychiatry Res. 2019, 275, 162–168. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Element | Evidence |
|---|---|
| Population | Schizophrenic patients |
| Exposure | Environmental barriers |
| Comparison | No environmental barriers |
| Outcome | More capacity-performance discrepancy |
| Moderate Schizophrenia (n = 2497) | Severe Schizophrenia (n = 1385) | p | Statistics (Statistical Tests) | Degrees of Freedom (df) | |
|---|---|---|---|---|---|
| Female (n, %) | 1179 (47.2) | 637 (46.0) | 0.464 | 0.536 (chi-squared test) | 1 |
| Age (years old, mean (SD)) | 48.3 (14.4) | 55.9 (13.5) | <0.001 | 16.490 (t-test) | 3001.4 |
| Education | <0.001 | 72.658 (chi-squared test) | 1 | ||
| >Primary | 1678 (67.2) | 739 (53.4) | |||
| ≤Primary | 819 (32.8) | 646 (46.6) | |||
| Residence | <0.001 | 321.747 (chi-squared test) | 1 | ||
| Community | 1066 (42.7) | 201 (14.5) | |||
| Institution | 1431 (57.3) | 1184 (85.5) | |||
| Primary caregiver | <0.001 | 94.701 (chi-squared test) | 1 | ||
| Yes | 801 (32.1) | 244 (17.6) | |||
| No | 1696 (67.9) | 1141 (82.4) | |||
| Urbanization level | 0.037 | 6.621 (chi-squared test) | 2 | ||
| Rural | 560 (22.4) | 361 (26.1) | |||
| Suburban | 707 (28.3) | 380 (27.4) | |||
| Urban | 1230 (49.3) | 644 (46.5) | |||
| Work status | <0.001 | 75.311 (chi-squared test) | 1 | ||
| Employment | 156 (6.3) | 6 (0.4) | |||
| Unemployment | 2341 (93.8) | 1379 (99.6) | |||
| Family economic status | <0.001 | 54.731 (chi-squared test) | 1 | ||
| General | 1464 (58.6) | 641 (46.3) | |||
| Middle low-low | 1033 (41.4) | 744 (53.7) | |||
| WHODAS 2.0 (mean (SD)) | |||||
| Cognition (domain 1) | |||||
| Capacity | 38.2 (25.3) | 60.6 (28.4) | <0.001 | 24.449 (t-test) | 2515.8 |
| Performance | 36.1 (24.4) | 58.1 (28.4) | <0.001 | 24.271 (t-test) | 2591 |
| Mobility (domain 2) | |||||
| Capacity | 20.4 (28.5) | 40.4 (37.0) | <0.001 | 17.504 (t-test) | 2254.8 |
| Performance | 17.7 (25.0) | 35.3 (33.5) | <0.001 | 17.102 (t-test) | 2305.2 |
| Self-care (domain 3) | |||||
| Capacity | 18.9 (25.6) | 41.9 (34.6) | <0.001 | 21.738 (t-test) | 2096 |
| Performance | 14.5 (20.8) | 31.7 (30.7) | <0.001 | 18.616 (t-test) | 2236.5 |
| Getting along (domain 4) | |||||
| Capacity | 39.8 (25.5) | 56.2 (28.8) | <0.001 | 17.633 (t-test) | 2551.1 |
| Performance | 39.0 (25.2) | 54.8 (28.8) | <0.001 | 17.127 (t-test) | 2577.5 |
| Life activities (domain 5-1) | |||||
| Capacity | 44.3 (32.8) | 66.3 (36.9) | <0.001 | 18.457 (t-test) | 2486.2 |
| Performance | 40.8 (32.4) | 61.3 (38.2) | <0.001 | 16.741 (t-test) | 2588 |
| Social participation (domain 6) | |||||
| Capacity | 36.4 (23.2) | 48.8 (26.7) | <0.001 | 14.526 (t-test) | 2500.1 |
| Performance | 34.4 (22.1) | 45.5 (25.9) | <0.001 | 13.422 (t-test) | 2536.8 |
| Overall summary index (SI) | |||||
| Capacity | 33.4 (21.6) | 52.0 (25.4) | <0.001 | 23.101 (t-test) | 2427.7 |
| Performance | 31.0 (19.9) | 47.9 (24.2) | <0.001 | 22.151 (t-test) | 2495.7 |
| Chapter e1 | 737 (29.5) | 523 (37.8) | <0.001 | 27.634 (chi-squared test) | 1 |
| Category e110 | 174 (7.0) | 170 (12.3) | <0.001 | 31.056 (chi-squared test) | 1 |
| Category e115 | 215 (8.6) | 203 (14.7) | <0.001 | 33.901 (chi-squared test) | 1 |
| Category e120 | 319 (12.8) | 285 (20.6) | <0.001 | 41.278 (chi-squared test) | 1 |
| Category e125 | 163 (6.5) | 177 (12.8) | <0.001 | 43.574 (chi-squared test) | 1 |
| Category e130 | 227 (9.1) | 177 (12.8) | <0.001 | 13.002 (chi-squared test) | 1 |
| Category e165 | 537 (21.5) | 391 (28.2) | <0.001 | 21.150 (chi-squared test) | 1 |
| Parameters | e110 without Accessibility Barrier | e110 with Accessibility Barrier | p | e115 without Accessibility Barrier | e115 with Accessibility Barrier | p | e120 without Accessibility Barrier | e120 with Accessibility Barrier | p |
|---|---|---|---|---|---|---|---|---|---|
| Total | 3538 (91.1) | 344 (8.9) | 3464 (89.2) | 418 (10.8) | 3278 (84.4) | 604 (15.6) | |||
| Age groups | <0.001 | 0.005 | <0.001 | ||||||
| 18–64 years | 2935 (83.0) | 259 (75.3) | 2871 (82.9) | 323 (77.3) | 2729 (83.3) | 465 (77.0) | |||
| ≥65 years | 603 (17.0) | 85 (24.7) | 593 (17.1) | 95 (22.7) | 549 (16.8) | 139 (23.0) | |||
| Impairment | <0.001 | <0.001 | <0.001 | ||||||
| Moderate | 2323 (65.7) | 174 (50.6) | 2282 (65.9) | 215 (51.4) | 2178 (66.4) | 319 (52.8) | |||
| Severe | 1215 (34.3) | 170 (49.4) | 1182 (34.1) | 203 (48.6) | 1100 (33.6) | 285 (47.2) | |||
| Sex | 0.069 | 0.380 | 0.122 | ||||||
| Male | 1899 (53.7) | 167 (48.5) | 1852 (53.5) | 214 (51.2) | 1762 (53.8) | 304 (50.3) | |||
| Female | 1639 (46.3) | 177 (51.5) | 1612 (46.5) | 204 (48.8) | 1516 (46.3) | 300 (49.7) | |||
| Primary caregiver | 0.063 | 0.681 | 0.460 | ||||||
| Yes | 967 (27.3) | 78 (22.7) | 936 (27.0) | 109 (26.4) | 875 (26.7) | 170 (28.2) | |||
| No | 2571 (72.7) | 266 (77.3) | 2528 (73.0) | 309 (73.9) | 2403 (73.3) | 434 (71.9) | |||
| Education | <0.001 | <0.001 | <0.001 | ||||||
| >Primary | 2234 (63.1) | 183 (53.2) | 2191 (63.3) | 226 (54.1) | 2087 (63.7) | 330 (54.6) | |||
| ≤Primary | 1304 (36.9) | 161 (46.8) | 1273 (36.8) | 192 (45.9) | 1191 (36.3) | 274 (45.4) | |||
| Residence | 0.002 | 0.042 | 0.106 | ||||||
| Community | 1180 (33.4) | 87 (25.3) | 1149 (33.2) | 118 (28.2) | 1087 (33.2) | 180 (29.8) | |||
| Institution | 2358 (66.7) | 257 (74.7) | 2315 (66.8) | 300 (71.8) | 2191 (66.8) | 424 (70.2) | |||
| Urbanization level | 0.002 | <0.001 | 0.061 | ||||||
| Rural | 830 (23.5) | 91 (26.5) | 804 (23.2) | 117 (28.0) | 764 (23.3) | 157 (26.0) | |||
| Suburban | 970 (27.4) | 117 (34.0) | 950 (27.4) | 137 (32.8) | 905 (27.6) | 182 (30.1) | |||
| Urban | 1738 (49.1) | 136 (39.5) | 1710 (49.4) | 164 (39.2) | 1609 (49.1) | 265 (43.9) | |||
| Work status | 0.003 | 0.003 | <0.001 | ||||||
| Employed | 158 (4.5) | 4 (1.2) | 156 (4.5) | 6 (1.4) | 155 (4.7) | 7 (1.2) | |||
| Unemployed | 3380 (95.5) | 340 (98.8) | 3308 (95.5) | 412 (98.6) | 3123 (95.3) | 597 (98.8) | |||
| Family economic status | 0.002 | 0.128 | 0.624 | ||||||
| General | 1946 (55.0) | 159 (46.2) | 1893 (54.7) | 212 (50.7) | 1783 (54.4) | 322 (53.3) | |||
| Middle low-Low | 1592 (45.0) | 185 (53.8) | 1571 (45.4) | 206 (49.3) | 1495 (45.6) | 282 (46.7) |
| Moderate Schizophrenia (n = 2497) | Severe Schizophrenia (n = 1385) | |
|---|---|---|
| Accessibility of e110 | ||
| with barrier | 0 ** (0–9.34) | 0.57 (0–9.65) |
| without barrier | 0 ** (0–4.36) | 0 (0–10.31) |
| Accessibility of e115 | ||
| with barrier | 0 ** (0–9.42) | 1.09 (0–9.60) |
| without barrier | 0 ** (0–4.45) | 0 (0–10.31) |
| Accessibility of e120 | ||
| with barrier | 0 ** (0–11.56) | 0 * (0–9.31) |
| without barrier | 0 ** (0–3.39) | 0 * (0–10.53) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lien, W.-C.; Wang, W.-M.; Wang, H.-M.D.; Lin, F.-H.; Yao, F.-Z. Environmental Barriers and Functional Outcomes in Patients with Schizophrenia in Taiwan: The Capacity-Performance Discrepancy. Int. J. Environ. Res. Public Health 2022, 19, 315. https://doi.org/10.3390/ijerph19010315
Lien W-C, Wang W-M, Wang H-MD, Lin F-H, Yao F-Z. Environmental Barriers and Functional Outcomes in Patients with Schizophrenia in Taiwan: The Capacity-Performance Discrepancy. International Journal of Environmental Research and Public Health. 2022; 19(1):315. https://doi.org/10.3390/ijerph19010315
Chicago/Turabian StyleLien, Wei-Chih, Wei-Ming Wang, Hui-Min David Wang, Feng-Huei Lin, and Fen-Zhi Yao. 2022. "Environmental Barriers and Functional Outcomes in Patients with Schizophrenia in Taiwan: The Capacity-Performance Discrepancy" International Journal of Environmental Research and Public Health 19, no. 1: 315. https://doi.org/10.3390/ijerph19010315
APA StyleLien, W.-C., Wang, W.-M., Wang, H.-M. D., Lin, F.-H., & Yao, F.-Z. (2022). Environmental Barriers and Functional Outcomes in Patients with Schizophrenia in Taiwan: The Capacity-Performance Discrepancy. International Journal of Environmental Research and Public Health, 19(1), 315. https://doi.org/10.3390/ijerph19010315