
A Participatory Intervention to Improve the Psychosocial Work Environment and Mental Health in Human Service Organisations. A Mixed Methods Evaluation Study

 , , ,
, , ,
Abstract
1. Introduction
1.1. Primary Interventions to Reduce Work-Related Mental Illness
1.2. Aim and Research Questions
- Can improvements over time be observed in the psychosocial work environment and health outcomes for the intervention group compared to the control group?
- Was the intervention implemented as intended (fidelity)?
- What were the participants’ (a) reactions to the intervention activities, (b) experiences of learning, and (c) changes in behaviours and work routines, related to the intervention (mediators)?
2. Materials and Methods
2.1. Study Design
2.2. Study Setting and Participants
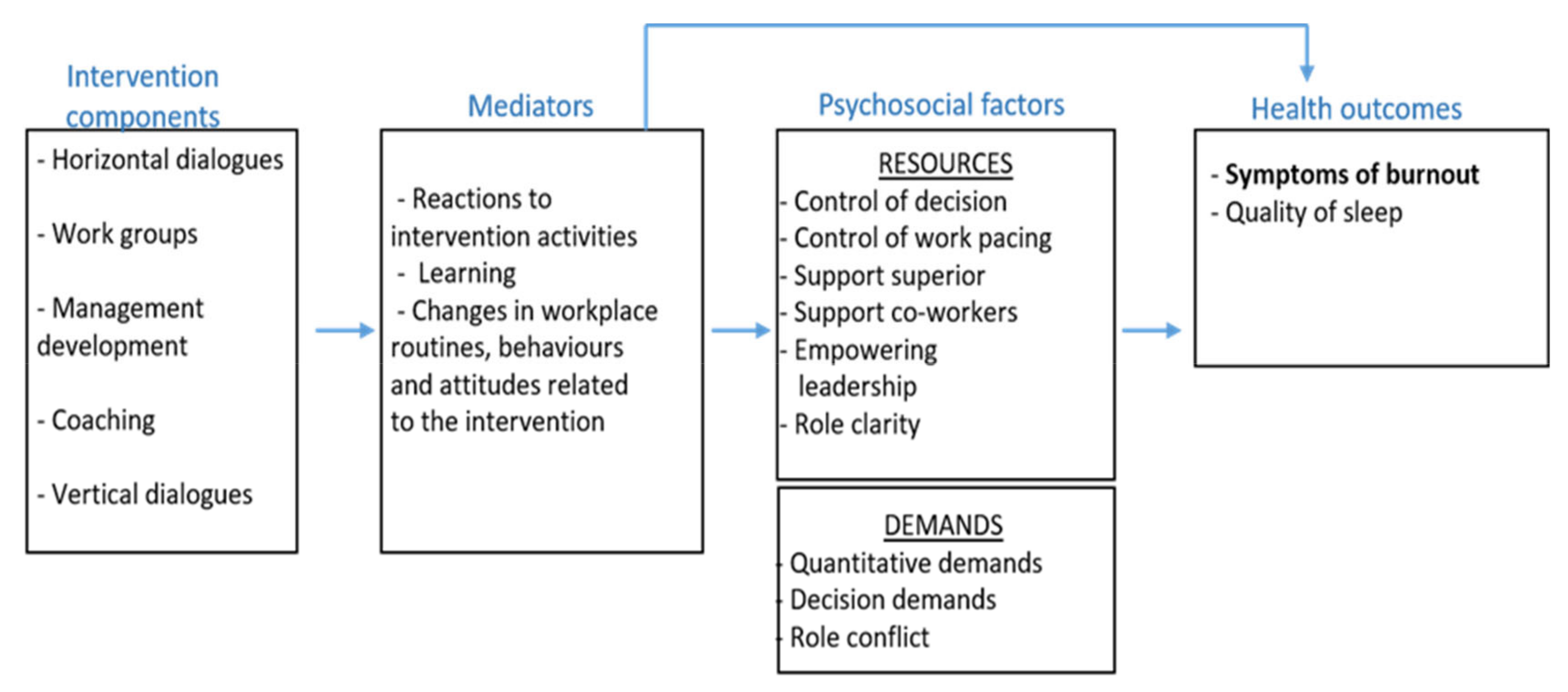
2.3. The Intervention
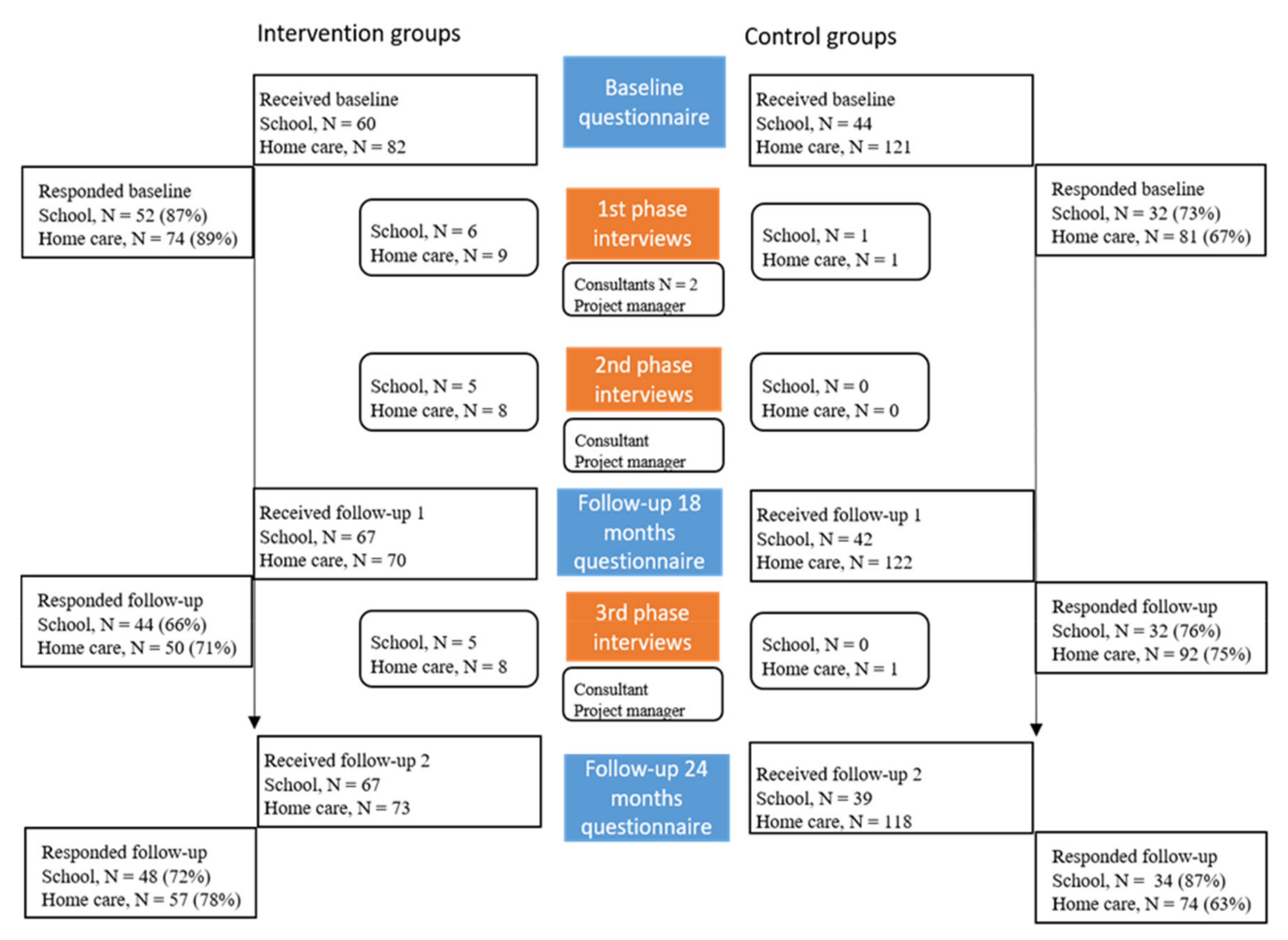
2.4. Data Collection
2.5. Outcome Measures
2.5.1. Primary Outcome
2.5.2. Secondary Outcomes and Covariates
2.6. Analysis
3. Results
3.1. Baseline Participant Characteristics and Outcome Measures
3.2. Did the Intervention Improve the Psychosocial Working Conditions, Quality of Sleep and Decrease Symptoms of Burnout?
3.3. Fidelity
3.4. Reactions, Learning, Changes in Behaviours and Work Routines
4. Discussion
4.1. Was There a Methodological Failure?
4.2. Was There a Program Theory Failure?
4.3. Was There an Implementation Failure?
4.4. Deteriorating Trend
4.5. Strengths and Limitations of the Study
4.6. Implications
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Försäkringskassan (Swedish Social Insurance Agency). Sjukfrånvaro i Psykiska Diagnoser: En Registerstudie av Sveriges Arbetande Befolkning i Åldern 20–69 år. Socialförsäkringsrapport 2020:8 (Sick Leave Due to Mental Disorders: A Register Based Study of the Working Population 20–69 Years in Sweden. Social Insurance Report 2020:8). Available online: https://www.forsakringskassan.se/wps/wcm/connect/e12b777c-e98a-488d-998f-501e621f4714/sjukfranvaro-i-psykiatriska-diagnoser-socialforsakringsrapport-2020-8.pdf (accessed on 28 March 2021).
- Akerstedt, T. Psychosocial stress and impaired sleep. Scand J. Work Environ. Health 2006, 32, 493–501. [Google Scholar] [CrossRef]
- Maslach, C.; Schaufeli, W.B.; Leiter, M.P. Job burnout. Annu Rev. Psychol. 2001, 52, 397–422. [Google Scholar] [CrossRef]
- Aronsson, V.; Toivanen, S.; Leineweber, C.; Nyberg, A. Can a poor psychosocial work environment and insufficient organizational resources explain the higher risk of ill-health and sickness absence in human service occupations? Evidence from a Swedish national cohort. Scand. J. Public Health 2019, 47, 310–317. [Google Scholar] [CrossRef]
- Gray, C.; Wilcox, G.; Nordstokke, D. Teacher Mental Health, School Climate, Inclusive Education and Student Learning: A Review. Can. Psychol. 2017, 58, 203–210. [Google Scholar] [CrossRef]
- Arvidsson, I.; Håkansson, C.; Karlson, B.; Björk, J.; Persson, R. Burnout among Swedish school teachers–a cross-sectional analysis. BMC Public Health 2016, 16, 823. [Google Scholar] [CrossRef]
- Nieuwenhuijsen, K.; Bruinvels, D.; Frings-Dresen, M. Psychosocial work environment and stress-related disorders, a systematic review. Occup. Med. 2010, 60, 277–286. [Google Scholar] [CrossRef]
- Seidler, A.; Thinschmidt, M.; Deckert, S.; Then, F.; Hegewald, J.; Nieuwenhuijsen, K.; Riedel-Heller, S.G. The role of psychosocial working conditions on burnout and its core component emotional exhaustion—A systematic review. J. Occup. Med. Toxicol. 2014, 9, 10. [Google Scholar] [CrossRef]
- Harvey, S.B.; Modini, M.; Joyce, S.; Milligan-Saville, J.S.; Tan, L.; Mykletun, A.; Bryant, R.A.; Christensen, H.; Mitchell, P.B. Can work make you mentally ill? A systematic meta-review of work-related risk factors for common mental health problems. Occup. Environ. Med. 2017, 74, 301–310. [Google Scholar] [CrossRef]
- Cerdas, S.; Härenstam, A.; Johansson, G.; Nyberg, A. Development of job demands, decision authority and social support in industries with different gender composition–Sweden, 1991–2013. BMC Public Health 2019, 19, 758. [Google Scholar] [CrossRef] [PubMed]
- Kjellström, J.; Almquist, B.; Modin, B. Lärares arbetsvillkor och hälsa efter 1990-talets skolreformer [Teachers’ working conditions and health after the school reforms of the 1990s]. Arbetsmarknad Arbetsliv 2016, 22, 52–69. [Google Scholar]
- Szebehely, M.; Stranz, A.; Strandell, R. Vem ska arbeta i framtidens äldreomsorg? Arbetsrapport 2017:1 (Who will work in the future elderly care? Working Paper 2017:1). Available online: https://www.socarb.su.se/polopoly_fs/1.320035.1486983623!/menu/standard/file/Slutversion%20rapport%20feb13.pdf (accessed on 28 March 2021).
- Irastorza, X.; Milczarek, M.; Cockburn, W. Second European Survey of Enterprises on New and Emerging Risks (ESENER-2): Overview Report: Managing Safety and Health at Work; Publications Office of the European Union: Luxembourg, 2016. [Google Scholar]
- Nielsen, K.; Miraglia, M. What works for whom in which circumstances? On the need to move beyond the ‘what works?’ question in organizational intervention research. Hum. Relat. 2016, 70, 40–62. [Google Scholar] [CrossRef]
- Joyce, S.; Modini, M.; Christensen, H.; Mykletun, A.; Bryant, R.; Mitchell, P.B.; Harvey, S.B. Workplace interventions for common mental disorders: A systematic meta-review. Psychol. Med. 2016, 46, 683–697. [Google Scholar] [CrossRef]
- Richardson, K.M.; Rothstein, H.R. Effects of occupational stress management intervention programs: A meta-analysis. J. Occup. Health Psychol. 2008, 13, 69. [Google Scholar] [CrossRef]
- Ruotsalainen, J.H.; Verbeek, J.H.; Mariné, A.; Serra, C. Preventing occupational stress in healthcare workers. Cochrane Database Syst. Rev. 2014, 8, 12. [Google Scholar]
- Naghieh, A.; Montgomery, P.; Bonell, C.P.; Thompson, M.; Aber, J.L. Organisational interventions for improving wellbeing and reducing work-related stress in teachers. Cochrane Database Syst. Rev. 2015. [Google Scholar] [CrossRef]
- Montano, D.; Hoven, H.; Siegrist, J. Effects of organisational-level interventions at work on employees’ health: A systematic review. BMC Public Health 2014, 14, 135. [Google Scholar] [CrossRef]
- Craig, P.; Dieppe, P.; Macintyre, S.; Michie, S.; Nazareth, I.; Petticrew, M. Developing and evaluating complex interventions: The new Medical Research Council guidance. BMJ 2008, 337. [Google Scholar] [CrossRef]
- Moore, G.F.; Evans, R.E. What theory, for whom and in which context? Reflections on the application of theory in the development and evaluation of complex population health interventions. SSM Popul. Health 2017, 3, 132–135. [Google Scholar] [CrossRef]
- Kristensen, T.S. Intervention studies in occupational epidemiology. J. Occup. Environ. Med. 2005, 62, 205–210. [Google Scholar] [CrossRef]
- Abildgaard, J.S.; Hasson, H.; von Thiele Schwarz, U.; Løvseth, L.T.; Ala-Laurinaho, A.; Nielsen, K. Forms of participation: The development and application of a conceptual model of participation in work environment interventions. Econ. Ind. Democr. 2018. [Google Scholar] [CrossRef]
- LaMontagne, A.D.; Keegel, T.; Louie, A.M.; Ostry, A.; Landsbergis, P.A. A systematic review of the job-stress intervention evaluation literature, 1990–2005. Int J. Occup. Med. Environ. Health 2007, 13, 268–280. [Google Scholar] [CrossRef]
- Nielsen, K.; Antino, M.; Rodríguez-Muñoz, A.; Sanz-Vergel, A. Is it me or us? The impact of individual and collective participation on work engagement and burnout in a cluster-randomized organisational intervention. Work Stress 2021, 1–24. [Google Scholar] [CrossRef]
- Nielsen, K.; Abildgaard, J.S. Organizational interventions: A research-based framework for the evaluation of both process and effects. Work Stress 2013, 27, 278–297. [Google Scholar] [CrossRef]
- Nielsen, K.; Randall, R. Opening the black box: Presenting a model for evaluating organizational-level interventions. Eur. J. Work Organ. Psychol. 2013, 22, 601–617. [Google Scholar] [CrossRef]
- Moore, G.F.; Audrey, S.; Barker, M.; Bond, L.; Bonell, C.; Hardeman, W.; Moore, L.; O’Cathain, A.; Tinati, T.; Wight, D.; et al. Process evaluation of complex interventions: Medical Research Council guidance. BMJ 2015, 350, h1258. [Google Scholar] [CrossRef]
- Lundmark, R.; Hasson, H.; von Thiele Schwarz, U.; Hasson, D.; Tafvelin, S. Leading for change: Line managers’ influence on the outcomes of an occupational health intervention. Work Stress 2017, 31, 276–296. [Google Scholar] [CrossRef]
- Schelvis, R.M.C.; Wiezer, N.M.; van der Beek, A.J.; Twisk, J.W.R.; Bohlmeijer, E.T.; Oude Hengel, K.M. The effect of an organizational level participatory intervention in secondary vocational education on work-related health outcomes: Results of a controlled trial. BMC Public Health 2017, 17. [Google Scholar] [CrossRef]
- Doyle, L.; Brady, A.-M.; Byrne, G. An overview of mixed methods research. J. Res. Nurs. 2009, 14, 175–185. [Google Scholar] [CrossRef]
- Schelvis, R.M.; Oude Hengel, K.M.; Burdorf, A.; Blatter, B.M.; Strijk, J.E.; van der Beek, A.J. Evaluation of occupational health interventions using a randomized controlled trial: Challenges and alternative research designs. Scand J. Work Environ. Health 2015, 41, 491–503. [Google Scholar] [CrossRef]
- Onwuegbuzie, A.J.; Collins, K.M. A Typology of Mixed Methods Sampling Designs in Social Science Research. Qual. Rep. 2007, 12, 281–316. [Google Scholar]
- Demerouti, E.; Bakker, A.B.; Nachreiner, F.; Schaufeli, W.B. The job demands-resources model of burnout. J. Appl Psychol. 2001, 86, 499. [Google Scholar] [CrossRef] [PubMed]
- Siegrist, J. Adverse health effects of high-effort/low-reward conditions. J. Occup. Health Psychol. 1996, 1, 27–41. [Google Scholar] [CrossRef]
- Mellor, N.; Smith, P.; Mackay, C.; Palferman, D. The “Management Standards” for stress in large organizations. Int. J. Workplace Health Manag. 2013, 6, 4–17. [Google Scholar] [CrossRef]
- Shirom, A.; Melamed, S. A Comparison of the Construct Validity of Two Burnout Measures in Two Groups of Professionals. Int. J. Stress Manag. 2006, 13, 176–200. [Google Scholar] [CrossRef]
- Dallner, M.; Elo, A.-L.; Gamberale, F.; Gamberale, F.; Hottinen, V.; Knardahl, S.; Lindström, K.; Skogstad, A.; Lindström-Espeling, K. Validation of the General Nordic Questionnaire (QPS Nordic) for Psychological and Social Factors at Work; Nordic Council of Ministers [Nordiska ministerrådet]: Copenhagen, Denmark, 2000.
- Nordin, M.; Åkerstedt, T.; Nordin, S. Psychometric evaluation and normative data for the Karolinska Sleep Questionnaire. Sleep Biol. Rhythm. 2013, 11, 216–226. [Google Scholar] [CrossRef]
- Lundgren-Nilsson, Å.; Jonsdottir, I.H.; Pallant, J.; Ahlborg, G., Jr. Internal construct validity of the Shirom-Melamed Burnout Questionnaire (SMBQ). BMC Public Health 2012, 12, 1. [Google Scholar] [CrossRef] [PubMed]
- Arapovic-Johansson, B.; Wåhlin, C.; Hagberg, J.; Kwak, L.; Björklund, C.; Jensen, I. Participatory work place intervention for stress prevention in primary health care. A randomized controlled trial. Eur. J. Work. Organ. Psychol. 2018, 27, 219–234. [Google Scholar] [CrossRef]
- Björklund, C.; Grahn, A.; Jensen, I.; Bergström, G. Does survey feedback enhance the psychosocial work environment and decrease sick leave? Eur. J. Work Organ. Psychol. 2007, 16, 76–93. [Google Scholar] [CrossRef]
- Costantini, G.; Saraulli, D.; Perugini, M. Uncovering the Motivational Core of Traits: The Case of Conscientiousness. Eur. J. Pers. 2020, 34, 1073–1094. [Google Scholar] [CrossRef]
- Derrick, B.; Toher, D.; White, P. How to compare the means of two samples that include paired observations and independent observations: A companion to Derrick, Russ, Toher and White (2017). Quant. Methods Psychol. 2017, 13. [Google Scholar] [CrossRef]
- Derrick, B.; Russ, B.; Toher, D.; White, P. Test statistics for the comparison of means for two samples that include both paired and independent observations. J. Mod. Appl. Stat. Methods 2017, 16, 9. [Google Scholar] [CrossRef]
- Shaffer, J.P. Multiple hypothesis testing. Annu. Rev. Psychol. 1995, 46, 561–584. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef]
- Kirkpatrick, D. Great ideas revisited. Train. Dev. 1996, 50, 54–60. [Google Scholar]
- Semmer, N.K. Job stress interventions and organization of work. Scand. J. Work Environ. Health 2006, 32, 515–527. [Google Scholar] [CrossRef] [PubMed]
- Aust, B.; Rugulies, R.; Finken, A.; Jensen, C. When workplace interventions lead to negative effects: Learning from failures. Scand. J. Public Health 2010, 38, 106–119. [Google Scholar] [CrossRef] [PubMed]
- Gupta, N.; Wahlin-Jacobsen, C.D.; Abildgaard, J.S.; Henriksen, L.N.; Nielsen, K.; Holtermann, A. Effectiveness of a participatory physical and psychosocial intervention to balance the demands and resources of industrial workers: A cluster-randomized controlled trial. Scand. J. Work Environ. Health 2017, 44, 58–68. [Google Scholar] [CrossRef]
- Barnett, A.G.; Van Der Pols, J.C.; Dobson, A. Regression to the mean: What it is and how to deal with it. Int. J. Epidemiol 2005, 34, 215–220. [Google Scholar] [CrossRef]
- Centrum för arbets- och miljömedicin [Center of Occupational and Environmental Medicine]. Arbetshälsorapport Stockholm Region [Occupational Health Report Stockholm Region]; EO Grafiska: Stockholm, Sweden, 2016. [Google Scholar]
- Mellor, N.; Mackay, C.; Packham, C.; Jones, R.; Palferman, D.; Webster, S.; Kelly, P. ‘Management standards’ and work-related stress in Great Britain: Progress on their implementation. Saf. Sci. 2011, 49, 1040–1046. [Google Scholar] [CrossRef]
- Hewitt, C.E.; Kumaravel, B.; Dumville, J.C.; Torgerson, D.J. Assessing the impact of attrition in randomized controlled trials. J. Clin. Epidemiol. 2010, 63, 1264–1270. [Google Scholar] [CrossRef]
- Crowne, D.P.; Marlowe, D. The Approval Motive: Studies in Evaluative Dependence; Wiley: New York, NY, USA, 1964. [Google Scholar]
- Cedstrand, E.; Nyberg, A.; Bodin, T.; Augustsson, H.; Johansson, G. Study protocol of a co-created primary organizational-level intervention with the aim to improve organizational and social working conditions and decrease stress within the construction industry–a controlled trial. BMC Public Health 2020, 20, 1–8. [Google Scholar] [CrossRef]
- Peters, S.E.; Nielsen, K.M.; Nagler, E.M.; Revette, A.C.; Madden, J.; Sorensen, G. Ensuring organization-intervention fit for a participatory organizational intervention to improve food service workers’ health and wellbeing: Workplace organizational health study. J. Occup. Environ. Med. 2020, 62, e33–e45. [Google Scholar] [CrossRef]
- Von Thiele Schwarz, U.; Lundmark, R.; Hasson, H. The dynamic integrated evaluation model (DIEM): Achieving sustainability in organizational intervention through a participatory evaluation approach. Stress Health 2016, 32, 285–293. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Intervention Component | Target Groups | Aim/Content |
|---|---|---|
| Kick-off | All employees and politicians | Inform about the project, anchoring. |
| Joint education | Managers, management teams and politicians | Education on organizational and social work environment. |
| Feedback and discussion | Municipality management team | Anchoring of the project to enhance support from management. |
| Feedback and discussion | Political board and the committees representing the two administrations met within each group together with the HR-representative and the external consultant. | Anchoring of the project to enhance support from the politicians. Discussions on the progress of the project and occupational health related issues. |
| Leadership coaching | All team managers (n = 5), unit managers (n = 3), department managers (n = 2) and the two administrative managers. | The overall theme was “leading for health”. However, everyone enrolled in the coaching program formulated his or her own goal for the coaching. |
| Horizontal dialogue meetings | All frontline employees and first-line managers | Make team-specific risk assessments and action plans. |
| Management development | Management teams at 3 levels within the two administrations and the top management team within the municipality. | Clarify goals and create a clear mission for each team. All teams were offered support by the external consultant regarding the topic “leading for health”. A prioritized general focus for these meetings was the clarification of goals and roles, in order to create a clear mission for each team. |
| Vertical dialogues | Chairman of the political committee, managers from all management levels and employee representatives. | Resolve prioritized obstacles within the work environment. Questions discussed for example: parking permissions, subsidized clothes. |
| Work groups (This component was developed during the project. It was not in the original plan) | Representatives from the home care unit. | The work groups involved a couple of frontline workers from the different teams and were led by one team leader together with the external consultant or an HR representative. 5 work groups were organised on the topics: (1) staffing, planning, travel time for the unit (2) our meetings (3) employeeship (4) staffing, planning, travel time for a certain team (5) This is us. |
| Individual stress management (This component was developed during the project. It was not in the original plan) | All employees at the school. | Individual stress management |
| School | ||||||
| Baseline | 18 Months | 24 Months | ||||
| Background variables | Intervention N = 52 | Control N = 32 | Intervention N = 44 | Control N = 32 | Intervention N = 48 | Control N = 34 |
| Age | N (%) | N (%) | N (%) | N (%) | N (%) | N (%) |
| <35 | 10 (21) | 7 (22) | 11 (25) | 9 (28) | 9 (19) | 10 (29) |
| 36–45 | 13 (28) | 10 (31) | 13 (29.5) | 12 (38) | 17 (35) | 12 (35) |
| >46 | 24 (51) | 15 (47) | 20 (45.5) | 11 (34) | 22 (46) | 12 (36) |
| Education | ||||||
| Elementary school (9 years) | 8 (16) | 4 (13.3) | 1 (2) | 5 (17) | 3 (6) | 4 (12) |
| Upper elementary school (>9 years) | 5 (10) | 2 (6.7) | 8 (19) | 3 (10) | 8 (17) | 1 (3) |
| University/college | 38 (74) | 24 (80) | 34 (79) | 22 (73) | 37 (77) | 29 (85) |
| Females | 36 (70.6) | 28 (87.5) | 24 (54.5) | 26 (87) | 32 (67) | 28 (82) |
| Occupation | ||||||
| Teacher | 26 (59) | 18 (56.3) | 24 (60) | 21 (68) | 28 (65) | 17 (68) |
| Early childhood educator | 4 (9) | 4 (12.5) | 5 (12.5) | 1 (3) | 3 (7) | 1 (4) |
| Recreation leader | 5 (11) | 5 (15.6) | 2 (5) | 3 (10) | 1 (2) | 3 (12) |
| Others | 9 (20) | 5 (15.6) | 9 (28.5) | 6 (19) | 11 (26) | 4 (16) |
| Work time | ||||||
| Full time | 37 (74) | 29 (90.6) | 39 (91) | 28 (88) | 42 (89) | 29 (85) |
| Part time (chosen) | 12 (24) | 3 (9.4) | 3 (7) | 3 (9) | 4 (9) | 5 (15) |
| Part time (not chosen) | 1 (2) | 0 | 1 (2) | 1 (3) | 1 (2) | 0 |
| Job tenure | ||||||
| <1 | 16 (31.4) | 6 (18.7) | 7 (16) | 6 (19) | 10 (20.8) | 4 (12) |
| 1–2 | 11 (21.6) | 4 (12.5) | 16 (36) | 7 (22) | 7 (14.6) | 8 (23) |
| 3–5 | 6 (11.7) | 5 (15.6) | 3 (7) | 3 (9) | 10 (20.8) | 7 (21) |
| >5 | 18 (35.3) | 17 (53.2) | 18 (41) | 16 (50) | 21 (43.8) | 15 (44) |
| Answered before (at 24 months) | N (%) | N (%) | ||||
| Yes, both times | 24 (50) | 16 (47.1) | ||||
| Answered one of them | 8 (17) | 11 (32.4) | ||||
| No, none of them | 11 (23) | 6 (17.6) | ||||
| Do not remember | 4 (8) | 1 (2.9) | ||||
| Missing | 1 (2) | 0 | ||||
| Elderly Care | ||||||
| Baseline | 18 Months | 24 Months | ||||
| Background variables | Intervention N = 74 | Control N = 81 | Intervention N = 50 | Control N = 92 | Intervention N = 57 | Control N = 74 |
| Age | N (%) | N (%) | N (%) | N (%) | N (%) | N (%) |
| <35 | 16 (25) | 12 (21) | 11 (22) | 11 (12) | 15 (26) | 7 (10) |
| 36–45 | 13 (20) | 5 (8) | 11 (22) | 19 (21) | 13 (23) | 15 (20) |
| >46 | 36 (55) | 41 (71) | 27 (56) | 70 (67) | 29 (51) | 51 (70) |
| Education | ||||||
| Elementary school | 9 (12.7) | 10 (14) | 6 (12) | 18 (20) | 6 (10.5) | 14 (19) |
| Upper elementary school | 51 (71.8) | 53 (75) | 33 (69) | 61 (68) | 39 (68.5) | 49 (66) |
| University/college | 11 (15.5) | 8 (11) | 9 (19) | 11 (12) | 12 (21) | 11 (15) |
| Females | 66 (90) | 73 (94.8) | 42 (89) | 80(89) | 49 (86) | 62 (84) |
| Occupation | ||||||
| Care assistant | 23 (34.8) | 16 (22) | 11 (33) | 12 (16.5) | 19 (41) | 11 (19) |
| Assistant nurse | 43 (65.2) | 56 (78) | 21 (64) | 60 (82) | 27 (59) | 48 (81) |
| Nurse | 0 | 0 | 1 (3) | 0 | 0 | 0 |
| Cleaner | 0 | 0 | 0 | 1 (1.5) | 0 | 0 |
| Work time | ||||||
| Full time | 42 (58) | 39 (53.5) | 22 (46) | 49 (56.5) | 28 (51) | 37 (53) |
| Part time (chosen) | 28 (39) | 31 (42.5) | 26 (54) | 35 (40) | 27 (49) | 32 (45.5) |
| Part time (not chosen) | 2 (3) | 3 (4) | 0 | 3 (3.5) | 0 | 1 (1.5) |
| Job tenure | ||||||
| <1 | 10 (13.7) | 10 (13) | 4 (8) | 7 (8) | 4 (7) | 5 (7) |
| 1–2 | 9 (12.3) | 13 (17) | 3 (6) | 14 (15) | 3 (5) | 12 (16) |
| 3–5 | 15 (20.5) | 8 (10) | 8 (16.5) | 12 (13) | 16 (28) | 11 (15) |
| >5 | 39 (53.5) | 46 (60) | 34 (69.5) | 58 (64) | 34 (60) | 46 (62) |
| Answered before (at 24 months) | N (%) | N (%) | ||||
| Yes, both | 34 (60) | 31 (42) | ||||
| Answered one of them | 4 (7) | 16 (22) | ||||
| No, none of them | 4 (7) | 7 (10) | ||||
| Do not remember | 10 (17.5) | 16 (22) | ||||
| Missing | 5 (8.5) | 4 (4) | ||||
| School | ||||||
| Baseline | 18 Months | 24 Months | ||||
| Intervention N = 52 | Control N = 32 | Intervention N = 44 | Control N = 32 | Intervention N = 48 | Control N = 34 | |
| M (Sd) | M (Sd) | M (Sd) | M (Sd) | M (Sd) | M (Sd) | |
| Primary outcome | ||||||
| Burnout (1–7) | 2.5 (1.2) | 2.1 (1.1) | 2.5 (1.2) | 2.3 (1.1) | 2.7 (1.2) | 2.1 (1.0) |
| Secondary outcomes | ||||||
| Role conflict (1–5) | 2.5 (0.8) | 2.5 (0.7) | 2.7 (0.8) | 2.3 (0.8) | 3.0 (0.8) | 2.6 (0.6) |
| Role clarity (1–5) | 4.4 (0.6) | 4.5 (0.5) | 4.2 (0.9) | 4.7 (0.5) | 4.1 (0.8) | 4.6 (0.5) |
| Social support manager (1–5) | 4.4 * (0.6) | 4.0 (0.7) | 3.7 (1.0) | 4.2 (0.9) | 3.4 (1.0) | 4.1 (0.6) |
| Empowering leadership (1–5) | 3.6 (1.1) | 3.3 (0.7) | 3.0 (1.0) | 3.5 (0.9) | 2.9 (1.1) | 3.4 (0.7) |
| Social support colleagues (1–5) | 4.5 (0.6) | 4.3 (0.7) | 4.2 (0.6) | 4.3 (0.7) | 4.0 (0.7) | 4.5 (0.6) |
| Control of decision (1–5) | 2.9 (0.6) | 2.9 (0.6) | 2.9 (0.5) | 2.8 (0.6) | 2.7 (0.6) | 2.8 (0.6) |
| Control of work pacing (1–5) | 2.3 * (0.8) | 1.8 (0.5) | 2.4 (0.9) | 1.8 (0.6) | 2.2 (0.9) | 2.0 (0.7) |
| Quantitative job demands (1–5) | 2.9 (1.0) | 3.0 (0.9) | 3.0 (0.8) | 3.0 (0.8) | 3.3 (1.0) | 3.1 (0.7) |
| Decision demands (1–5) | 3.9 (0.7) | 4.0 (0.6) | 3.9 (0.6) | 4.0 (0.6) | 4.0 (0.6) | 4.0 (0.5) |
| Quality of sleep (1–6) 1 | 2.8 (0.8) | 2.6 (1.1) | 2.8 (1.0) | 2.8 (0.8) | 2.9 (0.9) | 2.7 (0.8) |
| Elderly Care | ||||||
| Baseline | 18 Months | 24 Months | ||||
| Intervention N = 74 | Control N = 81 | Intervention N = 50 | Control N = 92 | Intervention N = 57 | Control N = 74 | |
| Primary outcome | ||||||
| Burnout (1–7) | 2.4 (1.1) | 2.2 (1.2) | 2.4 (1.0) | 1.9 (1.1) | 2.9 (1.2) | 1.9 (0.9) |
| Secondary outcomes | ||||||
| Role conflict (1–5) | 2.9 * (0.7) | 2.6 (0.9) | 3.0 (0.6) | 2.4 (0.9) | 3.0 (0.8) | 2.3 (0.9) |
| Role clarity (1–5) | 3.9 * (0.8) | 4.5 (0.5) | 4.0 (0.8) | 4.6 (0.5) | 4.1 (0.6) | 4.6 (0.6) |
| Social support manager (1–5) | 3.8 * (0.8) | 4.2 (0.9) | 3.5 (0.9) | 4.3 (0.7) | 3.4 (1.0) | 4.3 (0.8) |
| Empowering leadership (1–5) | 3.0 * (1.1) | 3.6 (1.0) | 2.5 (0.9) | 4.0 (1.0) | 2.6 (1.1) | 3.9 (1.0) |
| Social support colleagues (1–5) | 4.2 (0.8) | 4.3 (0.7) | 4.2 (0.8) | 4.3 (0.7) | 4.2 (0.7) | 4.2 (0.9) |
| Control of decision (1–5) | 2.3 * (0.5) | 2.7 (0.8) | 2.3 (0.6) | 2.9 (0.8) | 2.3 (0.7) | 2.9 (0.8) |
| Control of work pacing (1–5) | 2.1 * (0.6) | 2.5 (0.8) | 2.0 (0.8) | 3.0 (0.8) | 2.0 (0.8) | 2.9 (0.8) |
| Quantitative job demands (1–5) | 2.9 (0.7) | 2.7 (0.8) | 3.0 (0.7) | 2.5 (0.9) | 3.0 (0.7) | 2.5 (0.8) |
| Decision demands (1–5) | 3.6 (0.7) | 3.7 (0.8) | 3.5 (0.7) | 3.3 (0.8) | 3.6 (0.6) | 3.3 (0.7) |
| Quality of sleep (1–6) 1 | 2.7 (0.7) | 2.7 (1.1) | 2.7 (0.8) | 2.6 (1.0) | 3.1 (0.8) | 2.5 (1.0) |
| School | ||||||||
| Experiment vs. Control 18 Months | Experiment vs. Control 24 Months | |||||||
| Weighted for Background Variables | Weighted for Baseline Measure | Weighted for Background Variables | Weighted for Baseline Measure | |||||
| Primary outcome | Mean diff. | p-value 1 | Mean diff. | p-value 1 | Mean diff. | p-value 1 | Mean diff. | p-value 1 |
| Burnout | 0.39 | 1.0 | 0.12 | 1 | 0.95 | 0.13 | 0.31 | 1.0 |
| Secondary outcomes | ||||||||
| Role conflict | −0.53 | 0.13 * | −0.13 | 1.0 | −0.93 | 0.001 | −0.24 | 1.0 |
| Role clarity | −0.17 | 1.0 | −0.24 | 1.0 | −0.62 | 0.001 | −0.27 | 0.66 |
| Social support manager | −0.91 | 0.001 * | −0.25 | 1.0 | −1.18 | 0.001 | −0.28 | 1.0 |
| Empowering leadership | −0.85 | 0.001 | −0.35 | 1.0 | −0.92 | 0.001 | −0.06 | 1.0 |
| Social support colleagues | −0.24 | 1.0 | −0.12 | 1.0 | −0.59 | 0.001 | −0.25 | 1.0 |
| Control of decision | −0.31 | 0.66 | 0.06 | 1.0 | −0.33 | 1.0 * | −0.01 | 1.0 |
| Control of work pacing | 0.61 | 0.26 | 0.22 | 1.0 | −0.18 | 1.0 * | 0.02 | 1.0 |
| Quantitative job demands | 0.29 | 1.0 | 0.06 | 1.0 | 0.62 | 0.53 | 0.12 | 1.0 |
| Decision demands | 0.60 | 0.001 * | 0.04 | 1.0 | 0.14 | 1.0 * | 0.02 | 1.0 |
| Quality of sleep | 0.16 | 1.0 * | −0.04 | 1.0 | 0.51 | 1.0 | −0.06 | 1.0 |
| Elderly Care | ||||||||
| Experiment vs. Control 18 Months | Experiment vs. Control 24 Months | |||||||
| Weighted for Background Variables | Weighted for Baseline Measure | Weighted for Background Variables | Weighted for Baseline Measure | |||||
| Primary outcome | Mean diff. | p-value 1 | Mean diff. | p-value 1 | Mean diff. | p-value 1 | Mean diff. | p-value 1 |
| Burnout | 0.40 | 1.0 | 0.37 | 1.0 | 0.75 | 0.13 | 0.62 | 0.001 * |
| Secondary outcomes | ||||||||
| Role conflict | −0.67 | 0.001 | −0.24 | 1.0 * | −0.67 | 0.001 | −0.35 | 0.13 |
| Role clarity | −0.41 | 0.13 * | −0.38 | 0.001 * | −0.45 | 0.001 | −0.37 | 0.001 |
| Social support manager | −1.03 | 0.001 | −0.66 | 0.001 | −0.78 | 0.001 | −0.65 | 0.001 |
| Empowering leadership | −1.29 | 0.001 * | −1.03 | 0.001 | −1.08 | 0.001 | −0.80 | 0.001 |
| Social support colleagues | 0.26 | 1.0 | −0.02 | 1.0 | 0.29 | 1.0 * | −0.15 | 1.0 * |
| Control of decision | −0.30 | 0.40 | −0.26 | 0.66 | −0.35 | 0.13 | −0.30 | 0.13 |
| Control of work pacing | −0.67 | 0.001 | −0.51 | 0.001 | −0.79 | 0.001 | −0.50 | 0.001 |
| Quantitative job demands | 0.54 | 0.001 | 0.42 | 0.001 | 0.32 | 1.0 * | 0.36 | 0.001 |
| Decision demands | 0.65 | 0.001 | 0.12 | 1.0 | 0.12 | 1.0 | 0.22 | 1.0 |
| Quality of sleep | −0.02 | 1.0 | 0.04 | 1.0 | 0.29 | 1.0 | 0.31 | 1.0 |
| Type of Intervention Component | No. Planned/Delivered | Dose Received N/% |
| Kick-off (all employees and politicians) | 2 times × 2 h/2 times × 2 h | 149/not available |
| Joint education (managers, management teams and politicians) | 6 times, 2 parts. Each part was supposed to be delivered 3 times each/Part one was delivered twice and part two was delivered once. | Part one = 11/not available |
| Feedback and discussion (municipality management team) | 7 times × 1 h/2 times × 75 min | Not available |
| Feedback and discussion (political board) | 7 times × 1 h/2 times × 2 h | Not available |
| Leadership coaching | School 6 h per person/4.3 h per person Social services 6 h per person/5.4 h per person | Not available |
| Horizontal dialogue meetings (workshops in the team or at the unit) | School 7 workshops per team/7 workshops per team Social services 7 workshops per team/6–8 among the four teams | Mandatory |
| Management development (management teams at 3 levels) | School Senior 12 h/2 times × 2 h Middle 12 h/3 times × 2 h First-line 12 h/15 times × 2 h Social services Senior 12 h/4 times × 2 h Middle 12 h/5 times × 3 h First-line 12 h/26 times × 2 h | Not available |
| Vertical dialogues (with politicians, managers and employee representatives) | School Not planned/7 times × 1 h Social services Not planned/5 times × 1 h | |
| Work groups | Not planned 5 groups, 28 times ×2 h (4–8 meetings per group). | |
| Individual stress management | Not planned/8 times × 90 min |
| Type of Intervention Component | Reactions | Learning | Changes in Behaviours and Routines |
|---|---|---|---|
| Leadership coaching | Themes: Rewarding (emotional relief) Appreciated, meaningful. They report getting support in resolving complicated situations with employees, co-workers or their closest manager. | Themes: Rewarding (skill development) Contributed to both personal and professional development. Improved skills in conflict management, how to organize meetings and how to coach employees are reported. | |
| Horizontal dialogue meetings (workshops in the team or at the unit) | Themes: Lack of change and disagreement on the format. Disappointment due to the lack of changes coming out from the project. Positive about the possibility to listen to each other and discuss work-related challenges (all). Frustration about how the meetings are organised. | Themes: Better understanding of work routines and colleagues. How decisions formally are taken and who is responsible for what (home care). | |
| Management development (management teams at 3 levels) | Themes: Mutual mental models (home care) Helped them clarify the goals and roles of the team, giving its members a mutual understanding of each other and of what they wish to achieve | Themes: Mutual mental models (home care) The four work groups operate more equal, applying the same work routines more often than before | |
| Vertical dialogues (with politicians, managers and employee representatives) | Themes: A sense of being listened to Appreciated the opportunity to communicate the needs of the organisation directly to the politicians. | Themes: Potentially moving towards change One example of an actual change in work routines due to the vertical dialogues is reported. It is within the home care where the suggestion of purchasing winter jackets for the workers has been approved. | |
| Work groups | Themes: Meaningful participation Experiences of being listened to and taken seriously (involved). | Themes: Meaningful participation Introduction of dedicated time to write and read reports from a day’s work. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cedstrand, E.; Nyberg, A.; Sanchez-Bengtsson, S.; Alderling, M.; Augustsson, H.; Bodin, T.; Mölsted Alvesson, H.; Johansson, G. A Participatory Intervention to Improve the Psychosocial Work Environment and Mental Health in Human Service Organisations. A Mixed Methods Evaluation Study. Int. J. Environ. Res. Public Health 2021, 18, 3546. https://doi.org/10.3390/ijerph18073546
Cedstrand E, Nyberg A, Sanchez-Bengtsson S, Alderling M, Augustsson H, Bodin T, Mölsted Alvesson H, Johansson G. A Participatory Intervention to Improve the Psychosocial Work Environment and Mental Health in Human Service Organisations. A Mixed Methods Evaluation Study. International Journal of Environmental Research and Public Health. 2021; 18(7):3546. https://doi.org/10.3390/ijerph18073546
Chicago/Turabian StyleCedstrand, Emma, Anna Nyberg, Sara Sanchez-Bengtsson, Magnus Alderling, Hanna Augustsson, Theo Bodin, Helle Mölsted Alvesson, and Gun Johansson. 2021. "A Participatory Intervention to Improve the Psychosocial Work Environment and Mental Health in Human Service Organisations. A Mixed Methods Evaluation Study" International Journal of Environmental Research and Public Health 18, no. 7: 3546. https://doi.org/10.3390/ijerph18073546
APA StyleCedstrand, E., Nyberg, A., Sanchez-Bengtsson, S., Alderling, M., Augustsson, H., Bodin, T., Mölsted Alvesson, H., & Johansson, G. (2021). A Participatory Intervention to Improve the Psychosocial Work Environment and Mental Health in Human Service Organisations. A Mixed Methods Evaluation Study. International Journal of Environmental Research and Public Health, 18(7), 3546. https://doi.org/10.3390/ijerph18073546