
Unravelling the Perspectives of Day and Night Traders in Selected Markets within a Sub-Saharan African City with a Malaria Knowledge, Attitude and Practice Survey

 , , , , , , , ,
, , , , , , , , 
 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design, Area, and Population
2.2. Sample Size
2.3. Preparation of Questionnaire, Administration and Data Collection
2.4. Data Analysis
2.5. Ethical Considerations
3. Results
3.1. Demographic Characteristics of Study Respondents
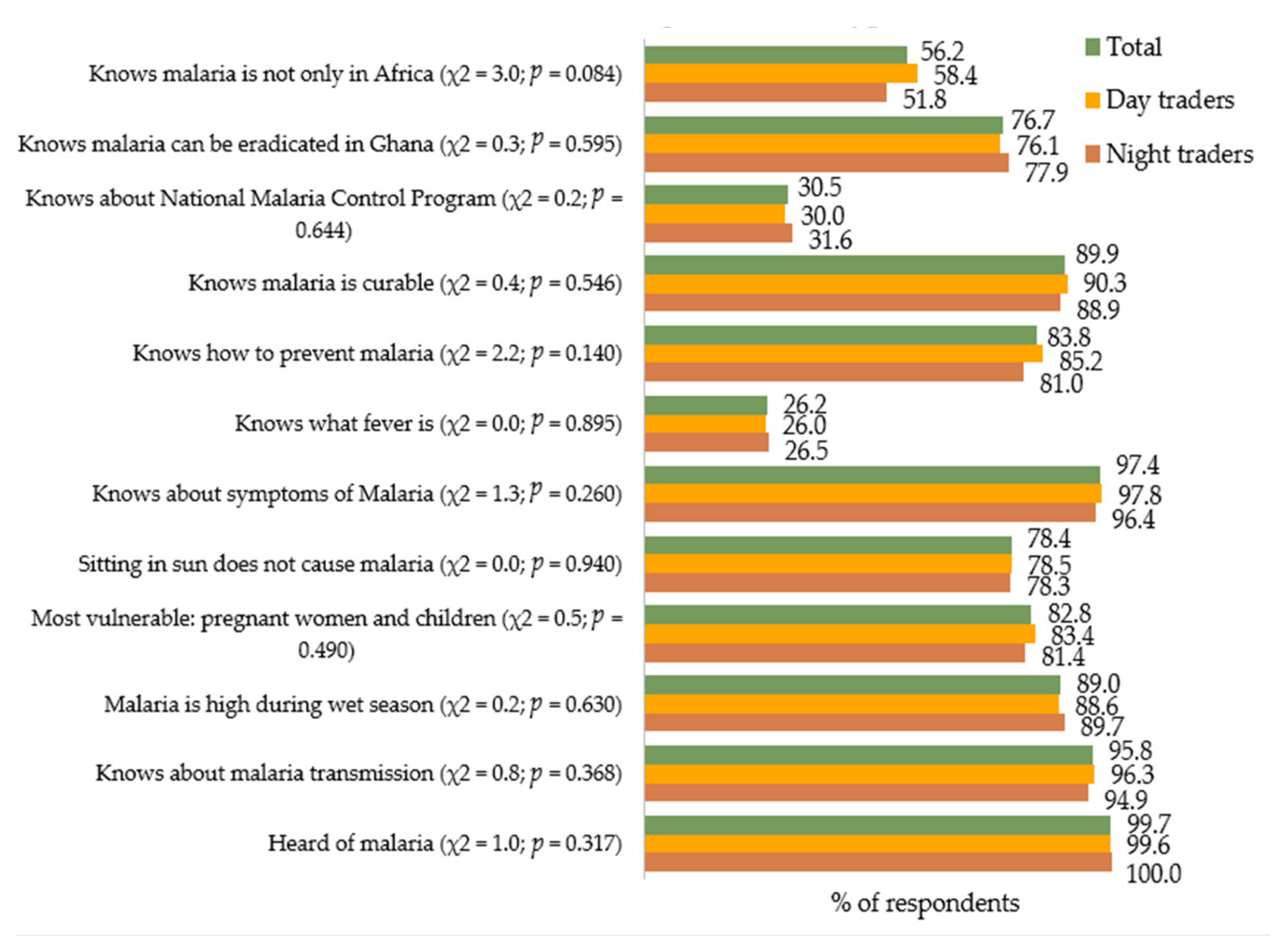
3.2. Knowledge on Malaria as Exhibited by the Respondents
3.3. Associations Between Respondents’ Demographic Characteristics and Knowledge Levels
3.4. Attitudes of Respondents toward Malaria
3.5. Associations between Attitudes and Knowledge Levels of Respondents
3.6. Malaria-Related Practices, Including Treatment and Control Choices, among the Respondents
3.7. Associations between Malaria-Related Practices and the Level of Knowledge
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Awine, T.; Malm, K.; Bart-Plange, C.; Silal, S.P. Towards malaria control and elimination in Ghana: Challenges and decision making tools to guide planning. Glob Health Action 2017, 10, 1381471. [Google Scholar] [CrossRef]
- World Health Organization. World Malaria Report 2017; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- World Health Organization. World Malaria Report 2015; World Health Organization: Geneva, Switzerland, 2016. [Google Scholar]
- World Health Organization. World Malaria Report 2019; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Deku, J.G.; Lokpo, S.Y.; Kye-Amoah, K.K.; Orish, V.N.; Ussher, F.A.; Esson, J.; Aduko, R.A.; Dakorah, M.P.; Osei-Yeboah, J. Malaria Burden and Trend among Clients Seeking Healthcare in the Western Region: A 4-Year Retrospective Study at the Sefwi-Wiawso Municipal Hospital, Ghana. Open Microbiol. J. 2018, 12, 404–411. [Google Scholar] [CrossRef]
- Ukoli, F. Prevention and Control of Parasitic Diseases in Tropical Africa: The Main Issues; University Press PLC: Ibadan, Nigeria, 1992. [Google Scholar]
- Godwin, J.T.; Mbaawuaga, M.E.; Akaa, P.D.; Alao, O.O.; Peters, E.J.; Utsalo, S.J.; Okwori, E.E.; Akosu, T.J.; Etukumana, E.A. Sociocultural factors influencing the control of malaria in an endemic city in north central Nigeria. Int. J. Biol. Med. Res. 2010, 1, 277–282. [Google Scholar]
- Jegede, A.S.; Amzat, J.; Salami, K.K.; Adejumo, P.O.; Oyetunde, M.O. Perceived causes of malaria among market women in Ibadan, Nigeria. Afr. J. Psychol. Study Soc. Issues 2005, 8, 335–347. [Google Scholar]
- Sachs, J.; Malaney, P. The economic and social burden of malaria. Nature 2002, 415, 680–685. [Google Scholar] [CrossRef]
- Sabin, L.L.; Rizal, A.; Brooks, M.I.; Singh, M.P.; Tuchman, J.; Wylie, B.J.; Joyce, K.M.; Yeboah-Antwi, K.; Singh, N.; Hamer, D.H. Attitudes, knowledge, and practices regarding malaria prevention and treatment among pregnant women in Eastern India. Am. J. Trop. Med. Hyg. 2010, 82, 1010–1016. [Google Scholar] [CrossRef]
- Asante, K.P.; Abokyi, L.; Zandoh, C.; Owusu, R.; Awini, E.; Sulemana, A.; Amenga-Etego, S.; Adda, R.; Boahen, O.; Segbaya, S.; et al. Community perceptions of malaria and malaria treatment behaviour in a rural district of Ghana: Implications for artemisinin combination therapy. BMC Public Health 2010, 10, 409. [Google Scholar] [CrossRef]
- Assan, A.; Takian, A.; Hanafi-Bojd, A.A.; Rahimiforoushani, A.; Nematolahi, S. Knowledge, attitude, and practice about malaria: Socio-demographic implications for malaria control in rural Ghana. J. Public Health Policy 2017, 38, 445–463. [Google Scholar] [CrossRef]
- Attu, H.; Adjei, J.K. Local knowledge and practices towards malaria in an irrigated farming community in Ghana. Malar. J. 2018, 17, 150. [Google Scholar] [CrossRef]
- Brenyah, R.C.; Osakunor, D.N.M.; Ephraim, R.K.D. Factors influencing urban malaria: A comparative study of two communities in the Accra Metropolis. Afr. Health Sci. 2013, 13, 992–998. [Google Scholar] [CrossRef]
- Hoffman, S.J.; Guindon, G.E.; Lavis, J.N.; Ndossi, G.D.; Osei, E.J.; Sidibe, M.F.; Boupha, B. Assessing healthcare providers’ knowledge and practices relating to insecticide-treated nets and the prevention of malaria in Ghana, Laos, Senegal and Tanzania. Malar. J. 2011, 10, 363. [Google Scholar] [CrossRef]
- Nyavor, K.D.; Kweku, M.; Agbemafle, I.; Takramah, W.; Norman, I.; Tarkang, E.; Binka, F. Assessing the ownership, usage and knowledge of insecticide treated nets (ITNs) in malaria prevention in the hohoe municipality, Ghana. Pan Afr. Med. J. 2017, 28. [Google Scholar] [CrossRef] [PubMed]
- Mbohou Nchetnkou, C.; Foko, L.P.K.; Lehman, L.G. Knowledge, Attitude, and Practices towards Malaria among Employees from Enterprises in the Town of Douala, Cameroon. BioMed Res. Int. 2020, 2020, 8652084. [Google Scholar] [CrossRef]
- Okwa, O.O.; Soremekun, B.M.; Adeseko, O.; Raheem, A.M. Artisans and traders’ knowledge, attitude and practices of malaria in selected areas of Lagos, Nigeria. Mechanics 2012, 14, 16. [Google Scholar]
- Adusei, K.A.; Owusu-Ofori, A. Prevalence of Plasmodium parasitaemia in blood donors and a survey of the knowledge, attitude and practices of transfusion malaria among health workers in a hospital in Kumasi, Ghana. PLoS ONE 2018, 13, e0206303. [Google Scholar]
- Buabeng, K.O.; Matowe, L.K.; Smith, F.; Duwiejua, M.; Enlund, H. Knowledge of medicine outlets’ staff and their practices for prevention and management of malaria in Ghana. Pharm. World Sci. 2010, 32, 424–431. [Google Scholar] [CrossRef] [PubMed]
- Owusu-Ofori, A.; Gadzo, D.; Bates, I. Transfusion-transmitted malaria: Donor prevalence of parasitaemia and a survey of healthcare workers knowledge and practices in a district hospital in Ghana. Malar. J. 2016, 15, 234. [Google Scholar] [CrossRef] [PubMed]
- Prah, J.K.; Yeboah-Sarpong, A.; Pinkrah, R.; Ewudzi-Acquah, E. Assessment of the knowledge, attitude and practices of prescribers regarding malaria diagnosis: A cross sectional study among Ghanaian prescribers. Pan Afr. Med. J. 2019, 34, 207. [Google Scholar] [CrossRef]
- Owusu, E.D.; Cremers, A.L.; Brown, C.A.; Mens, P.F.; Grobusch, M.P. Knowledge, attitudes and practices regarding malaria in people living with HIV in rural and urban Ghana. Acta Trop. 2018, 181, 16–20. [Google Scholar] [CrossRef]
- Fuge, T.G.; Ayanto, S.Y.; Gurmamo, F.L. Assessment of knowledge, attitude and practice about malaria and ITNs utilization among pregnant women in Shashogo District, Southern Ethiopia. Malar. J. 2015, 14, 235. [Google Scholar] [CrossRef]
- Anene-okeke, C.G.; Isah, A.; Aluh, D.O.; Ezeme, A.L. Knowledge and practice of malaria prevention and management among non-medical students of university of Nigeria, Nsukka. Int. J. Community Med. Public Health 2018, 5, 461–465. [Google Scholar] [CrossRef]
- Usman, S.O.; Ipinmoye, T.O.; Adu, A.S.; Fadero, T.; Edet-Utan, O.; Isola, I.N.; Ibrahim, A.; Oluberu, O.A.; Ojediran, T.E.; Akintayo-Usman, N.O. Knowledge and practice of malaria prevention among nonmedical students of higher institutions in Ondo State, Nigeria. Int. J. 2015, 1, 15. [Google Scholar]
- Sumari, D.; Dillip, A.; Ndume, V.; Mugasa, J.P.; Gwakisa, P.S. Knowledge, attitudes and practices on malaria in relation to its transmission among primary school children in Bagamoyo district, Tanzania. Malar. World J. 2016, 7, 1–6. [Google Scholar]
- Habtai, H.; Ghebremeskel, T.; Mihreteab, S.; Mufunda, J.; Ghebremichael, A. Knowledge, attitudes and practices (KAP) about malaria among people visiting referral hospitals of Eritrea. J. Eritrean Med. Assoc. 2008, 4, 42–46. [Google Scholar]
- Singh, R.; Musa, J.; Singh, S.; Ebere, U.V. Knowledge, attitude and practices on malaria among the rural communities in Aliero, Northern Nigeria. J. Family Med. Prim. Care 2014, 3, 39. [Google Scholar] [CrossRef]
- Khairy, S.; Al-Surimi, K.; Ali, A.; Shubily, H.M.; Al Walaan, N.; Househ, M.; El-Metwally, A. Knowledge, attitude and practice about malaria in south-western Saudi Arabia: A household-based cross-sectional survey. J. Infect. Public Health 2017, 10, 499–506. [Google Scholar] [CrossRef]
- Tamirat, A.; Geremew, M.; Abamecha, F.; Wollancho, W. Knowledge, Attitude and Practice about malaria in Maji District, Bench Maji Zone, Southwest Ethiopia. J. Trop. Dis. Public Health 2016, 4, 3. [Google Scholar] [CrossRef]
- Forero, D.A.; Chaparro, P.E.; Vallejo, A.F.; Benavides, Y.; Gutiérrez, J.B.; Arévalo-Herrera, M.; Herrera, S. Knowledge, attitudes and practices of malaria in Colombia. Malar. J. 2014, 13, 165. [Google Scholar] [CrossRef]
- Hlongwana, K.W.; Mabaso, M.L.; Kunene, S.; Govender, D.; Maharaj, R. Community knowledge, attitudes and practices (KAP) on malaria in Swaziland: A country earmarked for malaria elimination. Malar. J. 2009, 8, 29. [Google Scholar] [CrossRef]
- Dlamini, S.V.; Liao, C.W.; Dlamini, Z.H.; Siphepho, J.S.; Cheng, P.C.; Chuang, T.W.; Fan, C.K. Knowledge of human social and behavioral factors essential for the success of community malaria control intervention programs: The case of Lomahasha in Swaziland. J. Microbiol. Immunol. Infect 2017, 50, 245–253. [Google Scholar] [CrossRef]
- Ghana Statistical Service-GSS. Ghana Malaria Indicator Survey 2019; GSS: Accra, Ghana; ICF: Rockville, MD, USA, 2020; Available online: https://dhsprogram.com/publications/publication-MIS35-MIS-Final-Reports.cfm (accessed on 18 December 2020).
- Amusan, V.O.; Umar, Y.A.; Vantsawa, P.A. Knowledge, attitudes and practices on malaria prevention and control among private security guards within Kaduna Metropolis, Kaduna State-Nigeria. Sci. J. Public Health 2017, 5, 240–245. [Google Scholar] [CrossRef]
- Munisi, D.Z.; Nyundo, A.A.; Mpondo, B.C. Knowledge, attitude and practice towards malaria among symptomatic patients attending Tumbi Referral Hospital: A cross-sectional study. PLoS ONE 2019, 14, e0220501. [Google Scholar] [CrossRef]
- Ismail, N.E.; Jimam, N.S.; Dapar, M.L. Assessment of primary health care workers’ knowledge, attitudes and practices on uncomplicated malaria management in Plateau state, Nigeria. Int. J. Pharm. Sci. Res. 2019, 10, 286–293. [Google Scholar]
- Adegun Joel, A.; Adegboyega, J.A.; Awosusi Ajoke, O. Knowledge and the preventive strategies of malaria among migrant farmers in Ado-Ekiti Local Government Area of Ekiti State, Nigeria. Am. J. Sci. Ind. Res. 2011, 2, 883–889. [Google Scholar] [CrossRef]
- Jimam, N.S.; Ismail, N.E. Predictors of patients’ knowledge, attitudes and practices (KAP) regarding uncomplicated malaria in the primary healthcare facilities of Plateau state, Nigeria. J. Health Res. 2020, 34, 330–344. [Google Scholar] [CrossRef]
- Adedotun, A.; Morenikeji, O.; Odaibo, A. Knowledge, attitudes and practices about malaria in an urban community in south-western Nigeria. J. Vector Borne Dis. 2010, 47, 155. [Google Scholar]
- World Health Organization. Guidelines for the Treatment of Malaria; World Health Organization: Geneva, Switzerland, 2015. [Google Scholar]



{kind=link}
{kind=link}
| Characteristics | Night Traders | Day Traders | Total | χ2 | p-Value |
|---|---|---|---|---|---|
| n (%) | n (%) | n (%) | |||
| Age Group | 8.72 | 0.121 | |||
| 15–20 years | 36 (14.23) | 49 (9.66) | 85 (11.18) | ||
| 21–25 years | 53 (20.95) | 115 (22.68) | 168 (22.11) | ||
| 26–30 years | 62 (24.51) | 154 (30.37) | 216 (28.42) | ||
| 31–35 years | 55 (21.74) | 121 (23.87) | 176 (23.16) | ||
| 36–40 years | 16 (6.32) | 23 (4.54) | 39 (5.13) | ||
| >40 years | 31 (12.25) | 45 (8.88) | 76 (10.00) | ||
| Gender | 0.33 | 0.564 | |||
| Male | 83 (32.81) | 177 (34.91) | 260 (34.21) | ||
| Female | 170 (67.19) | 330 (65.09) | 500 (65.79) | ||
| Marital Status | 2.60 | 0.273 | |||
| Married | 100 (39.53) | 200 (39.45) | 300 (39.47) | ||
| Never married/single | 139 (54.94) | 291 (57.40) | 430 (56.58) | ||
| Widowed/divorced/separated | 14 (5.53) | 16 (3.16) | 30 (3.95) | ||
| Market | 181.22 | <0.001 *** | |||
| Agbogbloshie | 0 (0.00) | 56 (11.05) | 56 (7.37) | ||
| Tema Community 1 | 0 (0.00) | 164 (32.35) | 164 (21.58) | ||
| Dodowa | 0 (0.00) | 8 (1.58) | 8 (1.05) | ||
| Kaneshie | 5 (1.98) | 30 (5.92) | 35 (4.61) | ||
| Korle-Bu | 30 (11.86) | 30 (5.92) | 60 (7.89) | ||
| Kwashieman | 27 (10.67) | 27 (5.33) | 54 (7.11) | ||
| Madina | 104 (41.11) | 104 (20.51) | 208 (27.37) | ||
| Makola | 35 (13.83) | 35 (6.90) | 70 (9.21) | ||
| Roadside market | 13 (5.14) | 13 (2.56) | 26 (3.42) | ||
| Tema Station | 39 (15.42) | 40 (7.89) | 79 (10.39) | ||
| Products Sold | 3.97 | 0.553 | |||
| Prepared food | 53 (20.95) | 97 (19.13) | 150 (19.74) | ||
| Fruits and vegetables | 44 (17.39) | 103 (20.32) | 147 (19.34) | ||
| Clothes | 20 (7.91) | 56 (11.05) | 76 (10.00) | ||
| Drinks | 40 (15.81) | 72 (14.20) | 112 (14.74) | ||
| Electricals and electronics | 21 (8.30) | 47 (9.27) | 68 (8.95) | ||
| Other | 75 (29.64) | 132 (26.04) | 207 (27.24) | ||
| Frequency with which Traders went to the Market to Trade Each Week | 12.43 | 0.014 * | |||
| <4 times | 17 (6.72) | 51 (10.06) | 68 (8.95) | ||
| 4 times | 16 (6.32) | 39 (7.69) | 55 (7.24) | ||
| 5 times | 91 (35.97) | 225 (44.38) | 316 (41.58) | ||
| 6 times | 99 (39.13) | 144 (28.40) | 243 (31.97) | ||
| 7 times | 30 (11.86) | 48 (9.47) | 78 (10.26) |
| Level of Knowledge on Malaria | ||||||
|---|---|---|---|---|---|---|
| Characteristics | Total | Poor | Moderate | High | χ2 | p-Value |
| n | n (%) | n (%) | n (%) | |||
| Age Group | 20.97 | 0.021 * | ||||
| 15–20 years | 85 | 2 (2.35) | 56 (65.88) | 27 (31.76) | ||
| 21–25 years | 168 | 13 (7.74) | 93 (55.36) | 62 (36.90) | ||
| 26–30 years | 216 | 3 (1.39) | 111 (51.39) | 102 (47.22) | ||
| 31–35 years | 176 | 11 (6.25) | 95 (53.98) | 70 (39.77) | ||
| 36–40 years | 39 | 0 (0.00) | 20 (51.28) | 19 (48.72) | ||
| >40 years | 76 | 5 (6.58) | 42 (55.26) | 29 (38.16) | ||
| Gender | 1.74 | 0.420 | ||||
| Male | 260 | 10 (3.85) | 151 (58.08) | 99 (38.08) | ||
| Female | 500 | 24 (4.80) | 266 (53.20) | 210 (42.00) | ||
| Marital Status | 3.57 | 0.467 | ||||
| Married | 300 | 10 (3.33) | 166 (55.33) | 124 (41.33) | ||
| Never married/single | 430 | 24 (5.58) | 234 (54.42) | 172 (40.00) | ||
| Widowed/divorced/separated | 30 | 0 (0.00) | 17 (56.67) | 13 (43.33) | ||
| Market | 51.27 | <0.001 *** | ||||
| Agbogbloshie | 56 | 1 (1.79) | 31 (55.36) | 24 (42.86) | ||
| Tema Community 1 | 164 | 7 (4.27) | 81 (49.39) | 76 (46.34) | ||
| Dodowa | 8 | 0 (0.00) | 2 (25.00) | 6 (75.00) | ||
| Kaneshie | 35 | 0 (0.00) | 26 (74.29) | 9 (25.71) | ||
| Korle-Bu | 60 | 0 (0.00) | 34 (56.67) | 26 (43.33) | ||
| Kwashieman | 54 | 4 (7.41) | 26 (48.15) | 24 (44.44) | ||
| Madina | 208 | 16 (7.69) | 124 (59.62) | 68 (32.69) | ||
| Makola | 70 | 0 (0.00) | 34 (48.57) | 36 (51.43) | ||
| Roadside market | 26 | 0 (0.00) | 24 (92.31) | 2 (7.69) | ||
| Tema Station | 79 | 6 (7.59) | 35 (44.30) | 38 (48.10) | ||
| Products Sold by the Traders | 14.67 | 0.145 | ||||
| Prepared food | 150 | 4 (2.67) | 76 (50.67) | 70 (46.67) | ||
| Fruits and vegetables | 147 | 8 (5.44) | 83 (56.46) | 56 (38.10) | ||
| Clothes | 76 | 1 (1.32) | 44 (57.89) | 31 (40.79) | ||
| Drinks | 112 | 2 (1.79) | 64 (57.14) | 46 (41.07) | ||
| Electricals and electronics | 68 | 6 (8.82) | 42 (61.76) | 20 (29.41) | ||
| Other | 207 | 13 (6.28) | 108 (52.17) | 86 (41.55) | ||
| Number of Times Respondents Went to the Market to Trade | 13.53 | 0.095 | ||||
| <4 times | 68 | 0 (0.00) | 38 (55.88) | 30 (44.12) | ||
| 4 times | 55 | 2 (3.64) | 34 (61.82) | 19 (34.55) | ||
| 5 times | 316 | 21 (6.65) | 174 (55.06) | 121 (38.29) | ||
| 6 times | 243 | 11 (4.53) | 124 (51.03) | 108 (44.44) | ||
| 7 times | 78 | 0 (0.00) | 47 (60.26) | 31 (39.74) | ||
| Characteristics | Night Traders | Day Traders | Total | χ2 | p-Value |
|---|---|---|---|---|---|
| n (%) | n (%) | n (%) | |||
| Respondents’ Affirmation of Malaria History | 0.03 | 0.853 | |||
| Yes | 229 (90.51) | 461 (90.93) | 690 (90.79) | ||
| No | 24 (9.49) | 46 (9.07) | 70 (9.21) | ||
| Number of Times Respondents had had Malaria | 0.56 | 0.906 | |||
| 1–3 times | 102 (40.32) | 212 (41.81) | 314 (41.32) | ||
| 4–6 times | 95 (37.55) | 178 (35.11) | 273 (35.92) | ||
| 7–10 times | 30 (11.86) | 66 (13.02) | 96 (12.63) | ||
| More than 10 times | 26 (10.28) | 51 (10.06) | 77 (10.13) | ||
| Symptoms that Informed Respondents’ Malaria Suspicion | 3.85 | 0.698 | |||
| Fever | 96 (37.94) | 165 (32.54) | 261 (34.34) | ||
| Vomiting | 17 (6.72) | 44 (8.68) | 61 (8.03) | ||
| Weakness | 60 (23.72) | 134 (26.43) | 194 (25.53) | ||
| Loss of appetite | 57 (22.53) | 122 (24.06) | 179 (23.55) | ||
| Anemia | 14 (5.53) | 23 (4.54) | 37 (4.87) | ||
| No idea | 7 (2.77) | 12 (2.37) | 19 (2.50) | ||
| Others | 2 (0.79) | 7 (1.38) | 9 (1.18) | ||
| Respondents’ Reliance on Laboratory Tests for Confirmation of Malaria Suspicion | 0.08 | 0.779 | |||
| Yes | 62 (24.51) | 129 (25.44) | 191 (25.13) | ||
| No | 191 (75.49) | 378 (74.56) | 569 (74.87) | ||
| The First Thing Respondents Did Upon Experiencing Malaria-Like Symptoms | 1.37 | 0.712 | |||
| Visiting the hospital | 76 (31.93) | 157 (32.85) | 233 (32.54) | ||
| Visiting the drug store | 113 (47.48) | 222 (46.44) | 335 (46.79) | ||
| Self-medication at home | 35 (14.71) | 79 (16.53) | 114 (15.92) | ||
| Disregard symptoms | 14 (5.88) | 20 (4.18) | 34 (4.75) | ||
| Factors that Promoted Respondents’ Malaria Care Seeking | 0.73 | 0.865 | |||
| Gravity of symptoms | 187 (79.24) | 378 (80.08) | 565 (79.80) | ||
| Cost of hospital care | 6 (2.54) | 14 (2.97) | 20 (2.82) | ||
| Duration of symptoms | 29 (12.29) | 49 (10.38) | 78 (11.02) | ||
| Availability of time | 14 (5.93) | 31 (6.57) | 45 (6.36) | ||
| Respondents’ Responses Regarding Having Close Friends Who had had Malaria | 0.26 | 0.609 | |||
| Yes | 239 (95.60) | 468 (94.74) | 707 (95.03) | ||
| No | 11 (4.40) | 26 (5.26) | 37 (4.97) | ||
| Respondents’ Malaria Episodes Sometimes Coincided with their Friends’ Malaria Episodes | 0.16 | 0.691 | |||
| Yes | 10 (3.95) | 22 (4.58) | 32 (4.37) | ||
| No | 243 (96.05) | 458 (95.42) | 701 (95.63) |
| Level of Knowledge on Malaria | χ2 | p-Value | ||||
|---|---|---|---|---|---|---|
| Characteristics | Total | Poor | Moderate | High | ||
| N | n (%) | n (%) | n (%) | |||
| Sources of Information on Malaria | 147.21 | <0.001 * | ||||
| Home | 151 | 5 (3.31) | 98 (64.90) | 48 (31.79) | ||
| Family and neighbors | 12 | 7 (58.33) | 5 (41.67) | 0 (0.00) | ||
| Health workers | 160 | 7 (4.38) | 74 (46.25) | 79 (49.38) | ||
| Mass media (radio, TV, etc.) | 416 | 8 (1.92) | 227 (54.57) | 181 (43.51) | ||
| Other | 21 | 7 (33.33) | 13 (61.90) | 1 (4.76) | ||
| Respondents’ Affirmation of Malaria History | 1.38 | 0.501 | ||||
| Yes | 690 | 31 (4.49) | 374 (54.20) | 285 (41.30) | ||
| No | 70 | 3 (4.29) | 43 (61.43) | 24 (34.29) | ||
| Number of Times Respondents had had Malaria | 10.30 | 0.112 | ||||
| 1–3 times | 314 | 13 (4.14) | 155 (49.36) | 146 (46.50) | ||
| 4–6 times | 273 | 13 (4.76) | 164 (60.07) | 96 (35.16) | ||
| 7–10 times | 96 | 3 (3.13) | 52 (54.17) | 41 (42.71) | ||
| More than 10 times | 77 | 5 (6.49) | 46 (59.74) | 26 (33.77) | ||
| Symptoms that Informed Respondents’ Malaria Suspicion | 14.12 | 0.293 | ||||
| Fever | 261 | 12 (4.60) | 141 (54.02) | 108 (41.38) | ||
| Vomiting | 61 | 2 (3.28) | 41 (67.21) | 18 (29.51) | ||
| Weakness | 194 | 11 (5.67) | 100 (51.55) | 83 (42.78) | ||
| Loss of appetite | 179 | 6 (3.35) | 95 (53.07) | 78 (43.58) | ||
| Anemia | 37 | 3 (8.11) | 18 (48.65) | 16 (43.24) | ||
| No idea | 19 | 0 (0.00) | 15 (78.95) | 4 (21.05) | ||
| Others | 9 | 0 (0.00) | 7 (77.78) | 2 (22.22) | ||
| Respondents’ Reliance on Laboratory Tests for Confirmation of Malaria Suspicion | 11.66 | 0.003 * | ||||
| Yes | 191 | 13 (6.81) | 119 (62.30) | 59 (30.89) | ||
| No | 569 | 21 (3.69) | 298 (52.37) | 250 (43.94) | ||
| The First Thing Respondents Did Upon Experiencing Malaria-Like Symptoms | 5.97 | 0.427 | ||||
| Visiting the hospital | 233 | 11 (4.72) | 119 (51.07) | 103 (44.21) | ||
| Visiting the drug store | 335 | 15 (4.48) | 177 (52.84) | 143 (42.69) | ||
| Self-medication at home | 114 | 5 (4.39) | 71 (62.28) | 38 (33.33) | ||
| Disregard symptoms | 34 | 0 (0.00) | 20 (58.82) | 14 (41.18) | ||
| Factors that Promoted Respondents’ Malaria Care Seeking | 5.12 | 0.528 | ||||
| Gravity of symptoms | 565 | 28 (4.96) | 302 (53.45) | 235 (41.59) | ||
| Cost of hospital care | 20 | 0 (0.00) | 13 (65.00) | 7 (35.00) | ||
| Duration of symptoms | 78 | 3 (3.85) | 47 (60.26) | 28 (35.90) | ||
| Availability of time | 45 | 0 (0.00) | 26 (57.78) | 19 (42.22) | ||
| Respondents’ Responses Regarding Having Close Friends Who had had Malaria | 5.19 | 0.075 | ||||
| Yes | 707 | 29 (4.10) | 381 (53.89) | 297 (42.01) | ||
| No | 37 | 3 (8.11) | 25 (67.57) | 9 (24.32) | ||
| Respondents’ Malaria Episodes Sometimes Coincided with their Friends’ Malaria Episodes | 11.11 | 0.004 * | ||||
| Yes | 32 | 5 (15.63) | 17 (53.13) | 10 (31.25) | ||
| No | 701 | 26 (3.71) | 382 (54.49) | 293 (41.80) | ||
| Night Traders | Day Traders | Total | χ2 | p-Value | |
|---|---|---|---|---|---|
| Characteristics | n (%) | n (%) | n (%) | ||
| Respondents’ Choice of Drugs for Malaria Treatment | 6.13 | 0.189 | |||
| ACTs | 194 (76.68) | 381 (75.15) | 575 (75.66) | ||
| Chloroquine | 10 (3.95) | 23 (4.54) | 33 (4.34) | ||
| Paracetamol | 12 (4.74) | 20 (3.94) | 32 (4.21) | ||
| Herbal | 26 (10.28) | 39 (7.69) | 65 (8.55) | ||
| Other | 11 (4.35) | 44 (8.68) | 55 (7.24) | ||
| Respondents’ Preferred Type of Malaria Treatment | 0.16 | 0.686 | |||
| Orthodox | 212 (83.79) | 404 (82.62) | 616 (83.02) | ||
| Herbal | 41 (16.21) | 85 (17.38) | 126 (16.98) | ||
| Use of Insecticide-Treated Bed Nets | 2.24 | 0.134 | |||
| Yes | 107 (43.15) | 185 (37.45) | 292 (39.35) | ||
| No | 141 (56.85) | 309 (62.55) | 450 (60.65) | ||
| Rationale for Non-Use of Treated Bed Nets | 3.01 | 0.556 | |||
| Discomfort | 99 (66.89) | 200 (62.50) | 299 (63.89) | ||
| Allergy to content of the nets | 30 (20.27) | 59 (18.44) | 89 (19.02) | ||
| Perception of bed nets as sources of illness | 1 (0.68) | 3 (0.94) | 4 (0.85) | ||
| No particular reason | 15 (10.14) | 45 (14.06) | 60 (12.82) | ||
| Other | 3 (2.03) | 13 (4.06) | 16 (3.42) | ||
| Preferred Malaria Prevention Measures | 3.71 | 0.447 | |||
| Clearing of bushes and stagnant water | 19 (7.63) | 54 (10.82) | 73 (9.76) | ||
| Residual spraying | 10 (4.02) | 19 (3.81) | 29 (3.88) | ||
| Use of insecticide-treated bed nets | 85 (34.14) | 147 (29.46) | 232 (31.02) | ||
| Insecticide spray/coil | 134 (53.82) | 274 (54.91) | 408 (54.55) | ||
| Other | 1 (0.40) | 5 (1.00) | 6 (0.80) | ||
| Reason for Chosen Malaria Prevention Measure | 3.09 | 0.543 | |||
| Perceived lack of side effects | 11 (4.49) | 22 (4.49) | 33 (4.49) | ||
| Perceived superior efficiency | 132 (53.88) | 257 (52.45) | 389 (52.93) | ||
| Lower cost of choice | 19 (7.76) | 58 (11.84) | 77 (10.48) | ||
| Easy access to choice | 61 (24.90) | 110 (22.45) | 171 (23.27) | ||
| Owing to recommendations by others | 22 (8.98) | 43 (8.78) | 65 (8.84) | ||
| Willingness to Volunteer Information about Malaria to Others | 2.38 | 0.123 | |||
| Yes | 136 (54.62) | 302 (60.52) | 438 (58.56) | ||
| No | 113 (45.38) | 197 (39.48) | 310 (41.44) |
| Level of Knowledge about Malaria | ||||||
|---|---|---|---|---|---|---|
| Characteristics | Total | Poor | Moderate | High | χ2 | p-Value |
| n | n (%) | n (%) | n (%) | |||
| Respondents’ Choice of Drugs for Malaria Treatment | 26.49 | 0.001 * | ||||
| ACTs | 575 | 24 (4.17) | 291 (50.61) | 260 (45.22) | ||
| Chloroquine | 33 | 1 (3.03) | 25 (75.76) | 7 (21.21) | ||
| Paracetamol | 32 | 0 (0.00) | 20 (62.50) | 12 (37.50) | ||
| Herbal | 55 | 5 (9.09) | 36 (65.45) | 14 (25.45) | ||
| Other | 65 | 4 (6.15) | 45 (69.23) | 16 (24.62) | ||
| Respondents’ Preferred Type of Malaria Treatment | 10.74 | 0.005 * | ||||
| Orthodox | 616 | 25 (4.06) | 323 (52.44) | 268 (43.51) | ||
| Herbal | 126 | 7 (5.56) | 84 (66.67) | 35 (27.78) | ||
| Use of Insecticide-Treated Bed Nets | 9.80 | 0.007 * | ||||
| Yes | 292 | 8 (2.74) | 145 (49.66) | 139 (47.60) | ||
| No | 450 | 25 (5.56) | 258 (57.33) | 167 (37.11) | ||
| Rationale for Non-Use of Treated Bed Nets | 4.65 | 0.794 | ||||
| Discomfort | 299 | 14 (4.68) | 165 (55.18) | 120 (40.13) | ||
| Allergy to content of the nets | 89 | 6 (6.74) | 52 (58.43) | 31 (34.83) | ||
| Perception of bed nets as sources of illness | 4 | 0 (0.00) | 2 (50.00) | 2 (50.00) | ||
| No particular reason | 60 | 2 (3.33) | 35 (58.33) | 23 (38.33) | ||
| Other | 16 | 1 (6.25) | 12 (75.00) | 3 (18.75) | ||
| Preferred Malaria Prevention Measures | 13.06 | 0.110 | ||||
| Clearing of bushes and stagnant water | 73 | 5 (6.85) | 40 (54.79) | 28 (38.36) | ||
| Residual spraying | 29 | 3 (10.34) | 17 (58.62) | 9 (31.03) | ||
| Use of insecticide-treated bed nets | 232 | 6 (2.59) | 114 (49.14) | 112 (48.28) | ||
| Insecticide spray/coil | 408 | 18 (4.41) | 231 (56.62) | 159 (38.97) | ||
| Other | 6 | 0 (0.00) | 5 (83.33) | 1 (16.67) | ||
| Reason for Chosen Malaria Prevention Measure | 28.65 | <0.001 * | ||||
| Perceived lack of side effects | 33 | 0 (0.00) | 17 (51.52) | 16 (48.48) | ||
| Perceived superior efficiency | 389 | 11 (2.83) | 204 (52.44) | 174 (44.73) | ||
| Lower cost of choice | 77 | 1 (1.30) | 52 (67.53) | 24 (31.17) | ||
| Easy access to choice | 171 | 17 (9.94) | 86 (50.29) | 68 (39.77) | ||
| Owing to recommendations by others | 65 | 1 (1.54) | 42 (64.62) | 22 (33.85) | ||
| Willingness to Volunteer Information about Malaria to Others | 3.26 | 0.196 | ||||
| Yes | 438 | 23 (5.25) | 230 (52.51) | 185 (42.24) | ||
| No | 310 | 9 (2.90) | 177 (57.10) | 124 (40.00) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tetteh-Quarcoo, P.B.; Dayie, N.T.K.D.; Adutwum-Ofosu, K.K.; Ahenkorah, J.; Afutu, E.; Amponsah, S.K.; Abdul-Rahman, M.; Kretchy, J.-P.; Ocloo, J.Y.; Nii-Trebi, N.I.; et al. Unravelling the Perspectives of Day and Night Traders in Selected Markets within a Sub-Saharan African City with a Malaria Knowledge, Attitude and Practice Survey. Int. J. Environ. Res. Public Health 2021, 18, 3468. https://doi.org/10.3390/ijerph18073468
Tetteh-Quarcoo PB, Dayie NTKD, Adutwum-Ofosu KK, Ahenkorah J, Afutu E, Amponsah SK, Abdul-Rahman M, Kretchy J-P, Ocloo JY, Nii-Trebi NI, et al. Unravelling the Perspectives of Day and Night Traders in Selected Markets within a Sub-Saharan African City with a Malaria Knowledge, Attitude and Practice Survey. International Journal of Environmental Research and Public Health. 2021; 18(7):3468. https://doi.org/10.3390/ijerph18073468
Chicago/Turabian StyleTetteh-Quarcoo, Patience B., Nicholas T. K. D. Dayie, Kevin Kofi Adutwum-Ofosu, John Ahenkorah, Emmanuel Afutu, Seth K. Amponsah, Mubarak Abdul-Rahman, James-Paul Kretchy, Janet Y. Ocloo, Nicholas I. Nii-Trebi, and et al. 2021. "Unravelling the Perspectives of Day and Night Traders in Selected Markets within a Sub-Saharan African City with a Malaria Knowledge, Attitude and Practice Survey" International Journal of Environmental Research and Public Health 18, no. 7: 3468. https://doi.org/10.3390/ijerph18073468
APA StyleTetteh-Quarcoo, P. B., Dayie, N. T. K. D., Adutwum-Ofosu, K. K., Ahenkorah, J., Afutu, E., Amponsah, S. K., Abdul-Rahman, M., Kretchy, J.-P., Ocloo, J. Y., Nii-Trebi, N. I., Yalley, A. K., Hagan, O. C. K., Niriwa, B. P., Aghasili, C. C., Kotey, F. C. N., Donkor, E. S., Ayeh-Kumi, P. F., & Udofia, E. A. (2021). Unravelling the Perspectives of Day and Night Traders in Selected Markets within a Sub-Saharan African City with a Malaria Knowledge, Attitude and Practice Survey. International Journal of Environmental Research and Public Health, 18(7), 3468. https://doi.org/10.3390/ijerph18073468