
Hard to Reach or Just Not Enough? A Narrative Review of Inpatient Tobacco Cessation Programs in Pediatrics

Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Inclusion Criteria
2.3. Procedure
2.4. Ethics
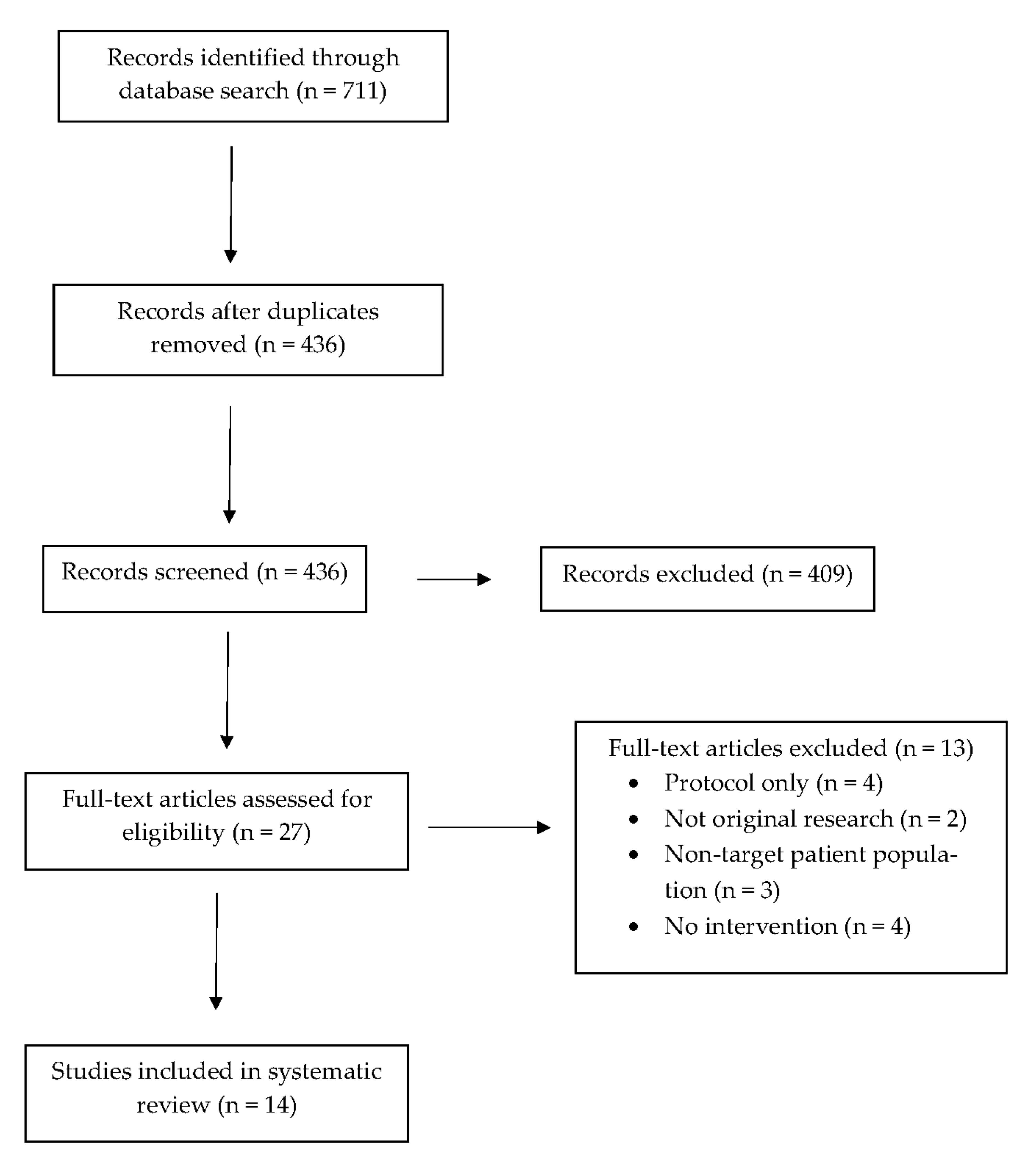
3. Results
3.1. Sociodemographic Characteristics of Participants
3.2. Research Teams
3.3. Study Designs
3.4. Settings for Recruitment
3.5. Sample Sizes
3.6. Inclusion and Exclusion Criteria
3.7. Theoretical Frameworks
3.8. Screening
3.9. Counseling
3.10. Sign-Out
3.11. Provision of Resources
3.11.1. NRT Products
3.11.2. Referral to Quitline
3.11.3. Miscellaneous Materials
3.12. Subjective Measures
3.13. Objective Measures
3.14. Follow-Up
3.15. Outcome Measures
3.15.1. Quit Attempt
3.15.2. Quitting
3.15.3. Secondary Outcome Measures
3.16. Data Analyses
3.17. Assessment of Outcomes
4. Discussion
4.1. Deliverers of Cessation Interventions across Diverse Inpatient Settings
4.2. Electronic-Based Cessation Strategy
4.3. Quitline Follow-Up
4.4. Loss to Follow-Up
4.5. Screening for Tobacco Use
4.6. Discrepancies in Defining Quit Attempts and Cessation
4.7. Environmental and Behavioral Changes
4.8. Provision of NRT Products
4.9. Attitudes of Clinicians towards the Provision of NRT to Caregivers
4.10. Target Population Considerations
4.11. Vaping Cessation Considerations
4.12. Subjective and Objective Measures
4.13. Future Directions of Research
4.14. Program-Building Recommendations
5. Limitations of This Narrative Review
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Bek, K.; Tomac, N.; Delibas, A.; Tuna, F.; Tezic, H.T.; Sungur, M. The effect of passive smoking on pulmonary function during childhood. Postgrad. Med. 1999, 75, 339–341. [Google Scholar] [CrossRef]
- Cunningham, J.; O’Connor, G.T.; Dockery, D.W.; Speizer, F.E. Environmental tobacco smoke, wheezing, and asthma in children in 24 communities. Am. J. Respir. Crit. Care Med. 1996, 153, 218–224. [Google Scholar] [CrossRef]
- DiFranza, J.R.; Lew, R.A. Morbidity and mortality in children associated with the use of tobacco products by other people. Pediatrics 1996, 97, 560–568. [Google Scholar] [CrossRef]
- Howrylak, J.A.; Spanier, A.J.; Huang, B.; Peake, R.W.; Kellogg, M.D.; Sauers, H.; Kahn, R.S. Cotinine in children admitted for asthma and readmission. Pediatrics 2014, 133, e355–e362. [Google Scholar] [CrossRef]
- Millett, C.; Lee, J.T.; Laverty, A.A.; Glantz, S.A.; Majeed, A. Hospital admissions for childhood asthma after smoke-free legislation in England. Pediatrics 2013, 131, e495–e501. [Google Scholar] [CrossRef]
- Rosen, L.J.; Noach, M.B.; Winickoff, J.P.; Hovell, M.F. Parental smoking cessation to protect young children: A systematic review and meta-analysis. Pediatrics 2012, 129, 141–152. [Google Scholar] [CrossRef]
- Sweeney, L.; Taylor, L.; Peurifoy, J.; Kauffman, K.; Napolitano, N. Success of a tobacco cessation program for parents at a children’s hospital. Respir. Care 2020, 65, 407–412. [Google Scholar] [CrossRef]
- The U.S. Department of Health and Human Services. The Health Consequences of Involuntary Exposure to Tobacco Smoke: A Report of the Surgeon General; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2006.
- USDHHS. Health Consequences of Involuntary Exposure to Tobacco Smoke: A Report of the Surgeon General; U.S. Government Printing Office: Washington, DC, USA, 2006. Available online: http://www.gaspforair.org/gasp/gedc/pdf/Surgeon%20GeneralSummary06.pdf (accessed on 22 August 2021).
- Winickoff, J.P.; Hibberd, P.L.; Case, B.; Sinha, P.; Rigotti, N.A. Child hospitalization: An opportunity for parental smoking intervention. Am. J. Prev. Med. 2001, 21, 218–220. [Google Scholar] [CrossRef]
- Bailey, S.L.; Ennett, S.T.; Ringwalt, C.L. Potential mediators, moderators, or independent effects in the relationship between parents’ former and current cigarette use and their children’s cigarette use. Addict. Behav. 1993, 18, 601–621. [Google Scholar] [CrossRef]
- Farkas, A.J.; Distefan, J.M.; Choi, W.S.; Gilpin, E.A.; Pierce, J.P. Does parental smoking cessation discourage adolescent smoking? Prev. Med. 1999, 28, 213–218. [Google Scholar] [CrossRef]
- Kuo, D.Z.; Houtrow, A.J.; Arango, P.; Kuhlthau, K.A.; Simmons, J.M.; Neff, J.M. Family-centered care: Current applications and future directions in pediatric healthcare. Matern. Child Health 2012, 16, 297–305. [Google Scholar] [CrossRef]
- Abdullah, A.S.; Guangmin, N.; Kaiyong, H.; Jing, L.; Yang, L.; Zhang, Z.; Winickoff, J.P. Implementing tobacco control assistance in pediatric departments of Chinese Hospitals: A Feasibility Study. Pediatrics 2018, 141, S51–S62. [Google Scholar] [CrossRef] [PubMed]
- Boykan, R.; Messina, C.R. A comparison of parents of healthy versus sick neonates: Is there a difference in readiness and/or success in quitting smoking? Hosp. Pediatr. 2015, 5, 619–623. [Google Scholar] [CrossRef] [PubMed]
- Huang, K.; Yang, L.; Winickoff, J.P.; Liao, J.; Nong, G.; Zhang, Z.; Liang, X.; Liang, G.; Abdullah, A.S. The effect of a pilot pediatric in-patient department-based smoking cessation intervention on parental smoking and children’s secondhand smoke (SHS) exposure in Guangxi, China. Int. J. Environ. Res. Public Health 2016, 13, 1109. [Google Scholar] [CrossRef]
- Jenssen, B.P.; Shelov, E.D.; Bonafide, C.P.; Bernstein, S.L.; Fiks, A.G.; Bryant-Stephens, T. Clinical decision support tool for parental tobacco treatment in hospitalized children. Appl. Clin. Inform. 2016, 7, 399–411. [Google Scholar] [PubMed]
- Ling, S.; Wooderson, S.; Rees, K.; Neild, R.; Wright, I.R. A smoking cessation program in the neonatal intensive care unit. J. Smok. Cessat. 2008, 3, 73–76. [Google Scholar] [CrossRef][Green Version]
- Northrup, T.F.; Suchting, R.; Klawans, M.R.; Khan, A.M.; Villarreal, Y.R.; Green, C.; Stotts, A.L. Proactive delivery of nicotine replacement therapy to families of hospitalized infants in a NICU: A randomized controlled pilot trial. J. Neonatal Nurs. 2020, 26, 201–206. [Google Scholar] [CrossRef]
- Ralston, S.; Grohman, C.; Word, D.; Williams, S.J. A randomized trial of a brief intervention to promote smoking cessation for parents during child hospitalization. Pediatr. Pulmonol. 2013, 48, 608–613. [Google Scholar] [CrossRef]
- Ralston, S.; Roohi, M. A randomized, controlled trial of smoking cessation counseling provided during child hospitalization for respiratory illness. Pediatr. Pulmonol. 2008, 43, 561–566. [Google Scholar] [CrossRef]
- Walley, S.C.; Chime, C.; Powell, J.; Walker, K.; Bunczyk-Brown, J.; Funkhouser, E. A brief inpatient intervention using a short video to promote reduction of child tobacco smoke exposure. Hosp. Pediatr. 2015, 5, 534–541. [Google Scholar] [CrossRef]
- Winickoff, J.P.; Healey, E.A.; Regan, S.; Park, E.R.; Cole, C.; Friebely, J.; Rigotti, N.A. Using the postpartum hospital stay to address mothers’ and fathers’ smoking: The NEWS study. Pediatrics 2010, 125, 518–525. [Google Scholar] [CrossRef] [PubMed]
- Winickoff, J.P.; Hillis, V.J.; Palfrey, J.S.; Perrin, J.M.; Rigotti, N.A. A smoking cessation intervention for parents of children who are hospitalized for respiratory illness: The stop tobacco outreach program. Pediatrics 2003, 111, 140–145. [Google Scholar] [CrossRef] [PubMed]
- Walley, S.C.; Mussman, G.M.; Lossius, M.; Shadman, K.A.; Destino, L.; Garber, M.; Ralston, S.L. Implementing parental tobacco dependence treatment within bronchiolitis qi collaboratives. Pediatrics 2018, 141, e20173072. [Google Scholar] [CrossRef] [PubMed]
- Wilson, K.M.; Moss, A.; Lowary, M.; Holstein, J.; Gambino, J.; Juarez-Colunga, E.; Kerby, G.S.; Klein, J.D.; Hovell, M.; Winickoff, J.P. Intervening with Smoking Parents of Inpatients to Reduce Exposure: The INSPIRE Randomized Controlled Trial. Acad. Pediatr. 2021, in press. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| First Author, Year, Reference. Location | Trial Design | Guiding Framework | Participant Characteristics (Sample Size, % Male, Age) I: Intervention C: Control | Intervention Components | Dosing | Deliverer of Intervention | Measure of Smoking Cessation | Provider Training: Content and Duration | Findings |
|---|---|---|---|---|---|---|---|---|---|
| Abdullah, 2018 [14] China | RCT, quasi-experimental | Transtheoretical Model (Stages of Change), Clinical practice guidelines of Tobacco Use and Dependence, Chronic Care Model | 969 I: 28.6% C: 24.8% I: 18–24 yrs (11.4%) 25–44 yrs (78.0%) 45 yrs+ (10.6%) C: 18–24 yrs (11.0%) 25–44 yrs (77.4%) 45 yrs+ (11.6%) | Intervention group: counseling, self-help smoking cessation guide, NRT prescription | 2 in-person or over-the-phone individual counseling sessions (each between 20–30 min) provided by pediatric resident fellows at initial contact and 1-month follow-up | Pediatric resident fellows at the smoking cessation counseling clinic in the hospital | Chart reviews | Clinical practice guidelines of Tobacco Use and Dependence-2As and R, 5As | Intervention was feasible and acceptable in the delivery of tobacco control assistance. There were no significant differences in smoking cessation between the intervention and control hospital caregivers for at least a day (p = 0.684) or quitting smoking completely (p = 0.510), increase in initiating smokefree homes post-intervention after 3 months as 55% of caregivers reported not smoking at home compared to 32% of caregivers who had at baseline, smokefree vehicles increased as 76% of caregivers reported that no one had smoked inside their vehicles at the 3-month follow-up timepoint in comparison to 54% of caregivers who had at baseline, 70% of caregivers had enacted smokefree rules in their vehicles at 3-month follow-up compared to 52% of them at baseline |
| Northrup, 2020 [19] United States | RCT, group comparison | Motivational interviewing | 32 I: 6.2% C: 0% Mean Age: I: 30.6 yrs (SD 9.7) C: 29.9 yrs (SD 4.3) | Intervention group: motivational advice and NRT prescription; Control group: Quitline referral | Intervention group: baseline assessment visit, two in-hospital motivational advice sessions by a research associate, 2-weeks of 14 mg or 21 mg transdermal patches for every smoker in the home, 2 follow-up assessment visits at the hospital or by phone at 2-weeks and 1-month post hospitalization; Control group: baseline assessment visit, smoking fact sheet about the harms of tobacco smoke exposure, Quitline referral, 2 follow-up assessment visits at the hospital or by phone at 2-weeks and 1-month post hospitalization | Research associate | Self-report | Research associate adopted session content from a previous tobacco smoke exposure protocol | Intervention was feasible and acceptable. Most caregivers in both intervention and control groups made at least one quit attempt. Reported smoking declined in the intervention group of caregivers receiving motivational advice and NRT at the first and second follow-up timepoints, self-reported home bans on indoor smoking and car-smoking bans were relatively high at baseline and rose further by the final study visit |
| Ralston, 2013 [13] United States | RCT, group comparison | Clinical practice guidelines of Tobacco Use and Dependence, Transtheoretical Model (Stages of Change) | 62 I: 20% C:34% Mean Age: I: 29.9 yrs C: 28.3 yrs | Intervention group: counseling, Quitline referral, cessation brochure; Control group: brochure already available to all hospitalized patients and their families | Intervention group: received brief intervention involving counseling < 10 min long, tobacco cessation recommendations from a pediatric hospitalist, contact information for the state Quitline, and a comprehensive smoking cessation brochure created by the American Cancer Society; 2-month follow-up phone call post-hospitalization; Control group: received only an injury prevention brochure that is already given to families of pediatric patients who are hospitalized; 2-month follow-up phone call post-hospitalization | Pediatric hospitalist | Self-report | Assessed caregiver’s degree of nicotine dependence with the Fagerstrom measure in combination with the clinical practice guidelines of Tobacco Use and Dependence as the basis to provide the cessation intervention | 18% of caregivers reported quitting at the 2-month follow-up timepoint. 45% of caregivers reported at least one quit attempt at the 2-month follow-up timepoint; 19 caregivers who were lost to follow-up were analyzed as continuing smokers |
| Ralston, 2008 [21] United States | RCT, group comparison | Clinical practice guidelines of Tobacco Use and Dependence, Transtheoretical Model (Stages of Change) | 42 I: 48% C:34% I: Caregivers- ≥25 yrs (76%) C: Caregivers- ≥25 yrs (71%) | Intervention group: counseling; NRT prescription; Control group: brief counseling and Quitline referral | Intervention group: received extensive smoking cessation counseling from a pediatric hospitalist that involved problem-solving emphasis and lasted > 10 min; caregivers prescribed an 8-week tapering course of nicotine patches beginning with 4 weeks at 21 mg, 2 weeks at 14 mg, and 2 weeks at 7 mg if they smoked > 15 cigarettes/day; for caregivers who smoked < 15 cigarettes/day but still scored at least a 3 on the Fagerstrom, a regimen of 4 weeks of the 14 mg patches followed by 4 weeks of the 7 mg patches were prescribed; 3 and 6-month follow-up phone calls post-hospitalization; Control group: received brief smoking cessation counseling and referral to the state Quitline; 3 and 6-month follow-up phone calls post-hospitalization | Pediatric hospitalist | Self-report | Assessed caregiver’s degree of nicotine dependence with the Fagerstrom measure in combination with the clinical practice guidelines of Tobacco Use and Dependence as the basis to provide the cessation intervention | 19% of caregivers in the intervention group and 4.8% of caregivers in the control group were self-reported quitters at the 3-month follow-up timepoint. Final quit rate was 14% in the intervention group at the 6-month follow-up timepoint. 33% of caregivers were lost to follow-up by 6 months and thus analyzed as continuing smokers |
| Wilston et al., 2021 [26] United States | Single-blind RCT | Clinical practice guidelines of Tobacco Use and Dependence-5A model | 252 I: 30.33% (n = 37) C: 31.54% (n = 41) Mean Age: I: 31.8 yrs (SD: 7.3) C: 32.2 yrs (SD: 7.6) | Intervention group: motivational interviewing, education on how to protect children from tobacco exposure, cessation strategies, Quitline referral, NRT provision, follow-up surveys over 1 year; control group: cessation coaches gave brief advice about the importance of quitting smoking and/or reducing their child’s exposure, Quitline referral | Intervention group: cessation coaches offered daily brief (15–30 min) motivational interviewing sessions by phone post-discharge, caregivers received information about protecting children from smoking in the home that included from other smokers or visitors, focused on resolving barriers, identifying triggers, promoting alternatives, and setting a quit date, referral to the state Quitline, 14 days of free dual NRT with patches, lozenges or gum dosed according to number of cigarettes smoked per day, provided standard guidance on NRT use from the package insert, 6-month and 12-month follow-up surveys completed either by phone, online, or in-person; control group: received Ask, Assess, and Advise components of the 5A model, Quitline referral | Diverse cohort of personnel trained to become cessation coaches that included respiratory therapists and research staff | Self-report, cotinine-verified tobacco abstinence | Educational sessions to providers and staff centered on the benefits of reducing tobacco exposure and quitting smoking for the health of their children, 3–4 h online or in-person workshop on motivational interviewing, 1-h tobacco specific motivational interviewing training, ongoing practice sessions addressing different scenarios and assessing skills as well as periodic in-person observation by study leadership | Intervention was feasible and acceptable. 15% quit rate among caregivers in the intervention group and 8% quit rate among caregivers in the control group |
| Winickoff, 2010 [23] United States | RCT, group comparison | Motivational interviewing; Social Learning Theory; Transtheoretical Model (Stages of Change); Health Belief Model; Chronic Care Model; Clinical practice guidelines of Tobacco Use and Dependence-5A model; behavior and systems framework | 101 I: 33% C: 34% Mean Age: I: 28 yrs C: 30 yrs | Intervention group: motivational interview, counseling, contact information for the Quitline, pamphlet on smoke exposure; Control group: pamphlet with Quitline information | Intervention group: 15-min motivational interview to help caregivers move toward accepting cessation support by enrolling in evidence-based tobacco treatment such as the state Quitline with follow-up feedback from the patient’s pediatrician; 1 individual counseling session; pamphlet about smoke exposure and contact information for the Quitline; 3-month follow-up phone call; Control group: contact information pamphlet for the Quitline; 3-month follow-up phone call | Nurse practitioners and trained research assistants | Follow-up from Quitline, self-report, 7-day point prevalence of cotinine-verified tobacco abstinence at 3 months postpartum | Adapted materials and messages specifically tailored for parental smokers (www.ceasetobacco.org accessed on 22 August 2021); cognitive behavioral and stage-based techniques; Clinical practice guidelines of Tobacco Use and Dependence-5As | Intervention was feasible and acceptable. There was no statistically significant difference in self-reported cessation, cotinine-confirmed cessation, or relapse prevention between the intervention and control groups |
| Boykan, 2015 [15] United States | Prospective, group comparison | Not reported | 224 Newborn Nursery: 25% (n = 46) NICU: 23% (n = 11) Mean Age: Newborn Nursery: 28.6 yrs (SD = 5.7) NICU: 28.6 yrs (SD = 7.5) | Quitline referral | Templates were built within the existing electronic health record to facilitate referral to the New York State Quitline for caregiver smokers of NICU and newborn nursery patients through direct data transfer from the EHR to the Quitline; caregivers were contacted by the Quitline within 3 days after referral and offered a range of quitline services that included telephone coaching and NRT; follow-up with Quitline 7 months post-referral; follow-up phone calls 6–9 months post-referral | Healthcare providers (primarily nurses) | Follow-up from Quitline, self-report | Opt-to-Quit program overview that establishes a systematic policy in which all smokers are offered referral to the New York State Quitline before discharge from a healthcare facility | Intervention was feasible and acceptable. Among the 35 caregivers with available quit status data after 7 and 8 months, there was not a statistically significant difference in quit rates or cutting back. 39% of caregivers in the newborn nursery quit compared with 0% in the NICU. 39% of caregivers in the newborn nursery cut back compared with 71% of caregivers in the NICU. 80% of mothers quit or cut back. 46% of fathers quit or cut back |
| Huang, 2016 [16] China | Prospective, cross-sectional | Clinical practice guidelines of Tobacco Use and Dependence-5A model | 107 62% Caregivers:18–30 yrs: (42%) 31–44 yrs: (39%) 45+ yrs: (19%) | Counseling and education, pamphlet, poster, sign, and sticker | Focused on the following aspects: (1) health risks of smoking and secondhand smoke exposure; (2) enforcing a strict no-smoking policy at home and in the car; (3) introducing methods and medications for smoking cessation; (4) offering cessation brochures describing the health risks of smoking and children’s secondhand smoke exposure; and (5) providing posters, no-smoking signs, and stickers; 3-month follow-up phone calls | Pediatricians trained as smoking cessation counselors | Self-report | Training consisted of lectures, demonstrations, case reviews, in-class discussions, and role plays. Primary content of the training included epidemiology of smoking and secondhand smoke exposure in China, health hazards of smoking, strategies for smoking cessation including the use of cessation medications and ethical aspects of human research | Intervention was feasible and acceptable. 7% of smokers had quit smoking (defined as had not smoked any cigarettes during the previous 7 days of the follow-up phone call), smokefree homes increased post-intervention at time of 3-month follow-up as 49% of caregivers reported smoking at home compared to 69% of caregivers who did at baseline, there was a nearly 20% increase in smokefree vehicles noted at the 3-month follow-up timepoint as 22% of caregivers reported not smoking inside their vehicles compared to 43% of caregivers who had at baseline |
| Jenssen, 2016 [17] nited States | Single arm prospective and mixed-methods | Clinical practice guidelines of Tobacco Use and Dependence-5A model; health information technology | 52 Not Reported Not Reported | Counseling, Quitline referral, NRT prescription, behavioral counseling resources | Brief smoking cessation counseling, NRT prescription for either of the following: (1) 2 mg or 4 mg nicotine gum based on whether caregiver smoked first cigarette >30 min after waking up (2 mg) or ≥30 min after waking up (4 mg); or (2) 14 mg or 21 mg nicotine patch based on whether caregiver smoked <10 cigarettes/day (14 mg) or > 10 cigarettes/day (21 mg); Quitline referral placed in discharge instructions; contact information for additional treatment options involving behavioral health resources | First-year pediatric residents | Chart review | Approximately 15–30 min in length and included brief smoking cessation counseling through the 5A model, prescribing NRT including relative contraindications to use and utilization of the parental tobacco clinical decision support tool | Intervention was feasible and acceptable. Limited to process measures of referral and treatment as the outcomes of the study |
| Ling, 2008 [18] Australia | Prospective, longitudinal | Motivational interviewing | 42 Not Reported Not Reported | Counseling, NRT prescription, smoking cessation information, QUIT program registration | Brief motivational counseling largely provided by a social worker, neonatal clinical nurse consultant who were supported by information, advice, and clinical supervision by the Drug and Alcohol staff within the hospital; 14–21 mg nicotine patches for 2 weeks prescribed by a neonatologist with support from a pharmacist to caregiver based on smoking history; supply of written smoking cessation information (QUIT kits, New South Wales Department of Health, Australia), QUIT program registration (NSW Department of Health, Australia), 3–9 month follow-ups via phone calls or at routine neonatal outpatient clinic visits | Social worker and neonatal clinical nurse consultant | Self-report | Training on behavioral treatments | At a median time of 6.5 months after transdermal nicotine patch use (range 3–9 months), 33% (n = 14) caregivers were not smoking. 64% of caregivers who quit long-term purchased follow-up nicotine patches after initial supply finished compared to 25% of caregivers who continued to smoke. Purchase of follow-up patches was a significant predictor of success in quitting. Relapse rate was 52%—29 respondents quit initially but 15 of these relapsed. Median time to relapse was 3 weeks with a range of 0.5–12 weeks after beginning program |
| Sweeney 2020 [7] United States | Prospective, cross-sectional | Cognitive behavioral techniques; coping skills | 138 44% (33) Age Mean: 31 years | Counseling, NRT prescription, referrals to Quitline and additional community resources | Counseling focused on stressors and triggers, finding alternative ways to manage cravings (stress balls, exercise, meditation, yoga, journaling, adult coloring); provision of NRT that included a combination of over-the-counter NRT (nicotine patches, gum and lozenges) in various doses; referred to outpatient and community programs through the American Lung Association Quitline or state or county department of health; 1-week follow-up phone call post-discharge | Respiratory therapists | Self-report | Training to become certified as tobacco treatment specialists | The intervention was feasible and acceptable; no cessation outcomes reported |
| Walley, 2015 [22] United States | Prospective, cross-sectional | Health Belief Model | 167 30% 31.5 ± 10.6 yrs | Motivational video, educational materials, Quitline referral | Caregivers viewed a 7-min long motivational video, “Smoking and Kids Don’t Mix” created by an internal hospital team that reviewed adverse health effects of childhood tobacco smoke exposure and recommended behaviors to reduce exposure that included home and vehicle smoking bans and smoking cessation; received written smoking cessation materials; Quitline referral; 1 and 3-month follow-up phone calls to assess knowledge, behavioral changes that included quit attempts, smoking reduction or cessation, and methods used to quit or reduce smoking | Internal hospital team consisting of pediatricians, nurses, and media experts | Self-report | Materials obtained from the Children’s of Alabama Patient Health and Information Center and the American Academy of Pediatrics Julius B. Richmond Center for Excellence | Among the 71 caregivers who were smokers at baseline, 13 of them reported smoking cessation at the 3-month follow-up timepoint. Intervention resulted in behavior changes that ultimately decreased secondhand and thirdhand smoke exposure (e.g., washing hands, changing clothes, initiation of home and vehicle smoking bans) |
| Walley, 2018 [25] United States | Retrospective | Clinical practice guidelines of Tobacco Use and Dependence-5A model and derived 2A and 1 R (ask, advise, and refer) model | BQIP: 21 Hospitals (1869 charts reviewed) SIB: 35 Hospitals (4389 charts reviewed) Not Reported Not Reported | Counseling, referrals to community resources | Research teams across both hospital sites received a tobacco change package of interventions that included suggested best practices to increase screening of children for tobacco smoke exposure and provision of tobacco-dependence treatment and referrals for caregivers; counseling; pharmacotherapy; personalized advice to quit smoking; referral to local resources and the Quitline; NRT prescription recommendation | Pediatric hospitalists | Chart review-intervention rate is defined as the rate of documentation of cessation counseling or referral for services in the chart for children with positive tobacco exposure screens | Each hospital site received coaching and feedback. In the BQIP collaborative, the tobacco-dependence treatment interventions recommended were based on the clinical practice guidelines 5A model; a derived 2A and 1 R version was also provided. | Change package interventions were feasible and acceptable. Cessation outcomes were not assessed across both collaboratives. |
| Winickoff, 2003 [24] United States | Prospective, cross-sectional | Transtheoretical Model (Stages of Change); Motivational interviewing | 71 24% (n = 17) 33 ± 9 yrs | Counseling, provision of educational materials, NRT prescription, sign-out to caregiver’s primary care provider, Quitline referral | Counseling that assessed caregiver’s stage of change and involved motivational interviewing; provision of educational materials on smoke exposure, cost of smoking, ingredients in cigarettes, and health benefits of quitting; 1-week supply of NRT products (nicotine gum or patches); 5-day and 10-day follow-up phone calls within 2 weeks of program enrollment; a note faxed to caregiver’s primary care provider about caregiver’s enrollment in the program and sign-out for follow-up by this provider; Quitline referral; 2-month follow-up phone call to assess caregiver’s quit attempts, smoking behaviors, and satisfaction with the program | Counselors | Self-report | The in-hospital counseling session included the techniques of motivational interviewing. Materials provided were from the STOP library that consists of 25 separate 1–2 page sheets of information designed to respond to the specific concerns raised by parents during the interview | Intervention was feasible and acceptable. 35 parents reported having made a quit attempt that lasted 24 h in the 2 months after program enrollment. 15 parents reported 7-day abstinence at 2-month follow-up, 60% of caregivers reported smoking inside their homes at baseline, significant decrease in smoking indoors at time of 2-month follow-up post hospitalization as only 15% of caregivers reported smoking inside their homes, 29% of caregivers had rules about no smoking at home at baseline and by time of 2-month follow-up, there was a substantial increase in enforcing smokefree rules at home as 71% of caregivers had implemented them |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jawed, A.; Jassal, M. Hard to Reach or Just Not Enough? A Narrative Review of Inpatient Tobacco Cessation Programs in Pediatrics. Int. J. Environ. Res. Public Health 2021, 18, 13423. https://doi.org/10.3390/ijerph182413423
Jawed A, Jassal M. Hard to Reach or Just Not Enough? A Narrative Review of Inpatient Tobacco Cessation Programs in Pediatrics. International Journal of Environmental Research and Public Health. 2021; 18(24):13423. https://doi.org/10.3390/ijerph182413423
Chicago/Turabian StyleJawed, Aysha, and Mandeep Jassal. 2021. "Hard to Reach or Just Not Enough? A Narrative Review of Inpatient Tobacco Cessation Programs in Pediatrics" International Journal of Environmental Research and Public Health 18, no. 24: 13423. https://doi.org/10.3390/ijerph182413423
APA StyleJawed, A., & Jassal, M. (2021). Hard to Reach or Just Not Enough? A Narrative Review of Inpatient Tobacco Cessation Programs in Pediatrics. International Journal of Environmental Research and Public Health, 18(24), 13423. https://doi.org/10.3390/ijerph182413423