
Usability Study of a Multicomponent Exergame Training for Older Adults with Mobility Limitations

 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
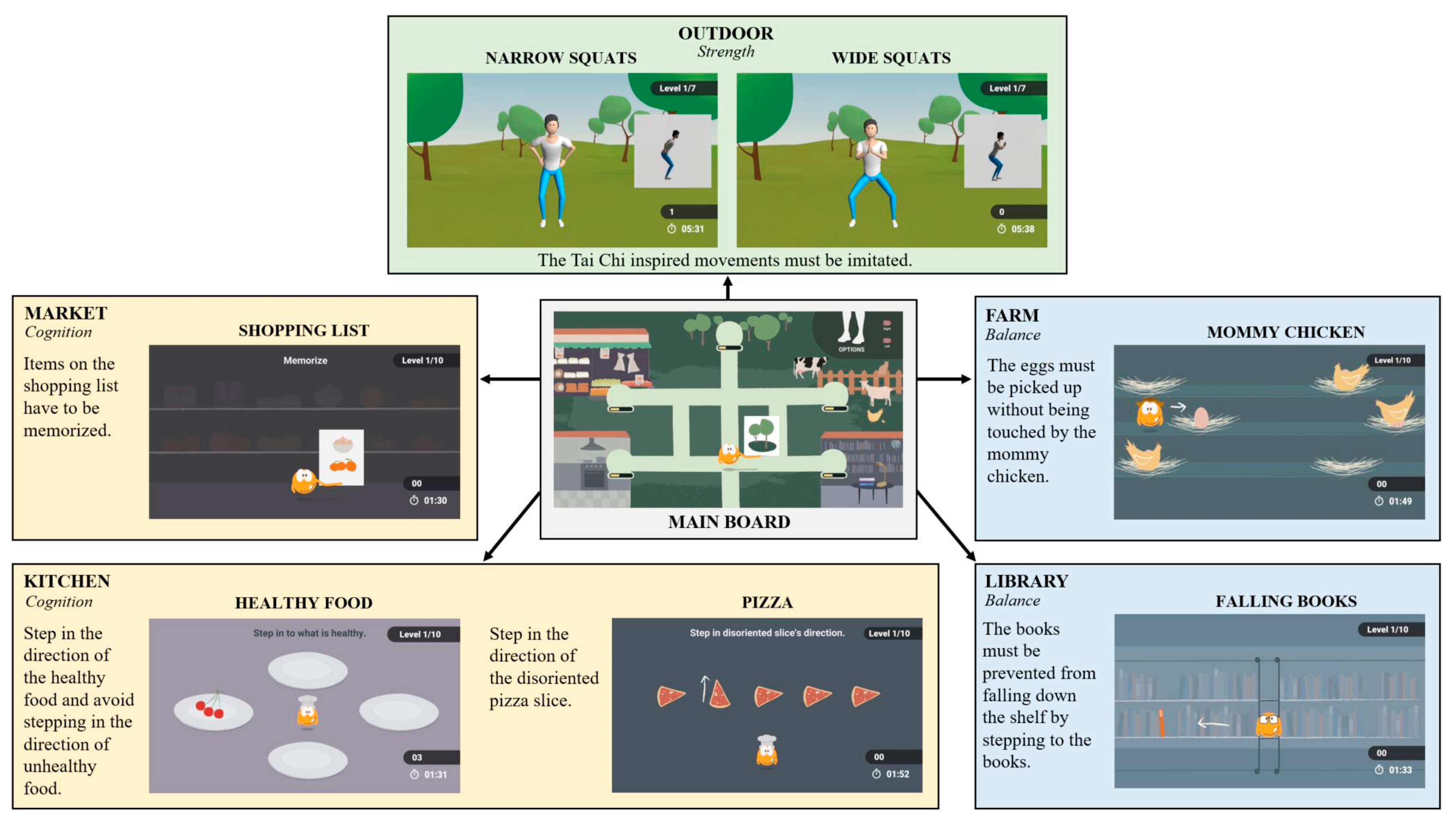
2.2. Exergame Intervention
2.3. Primary Outcomes
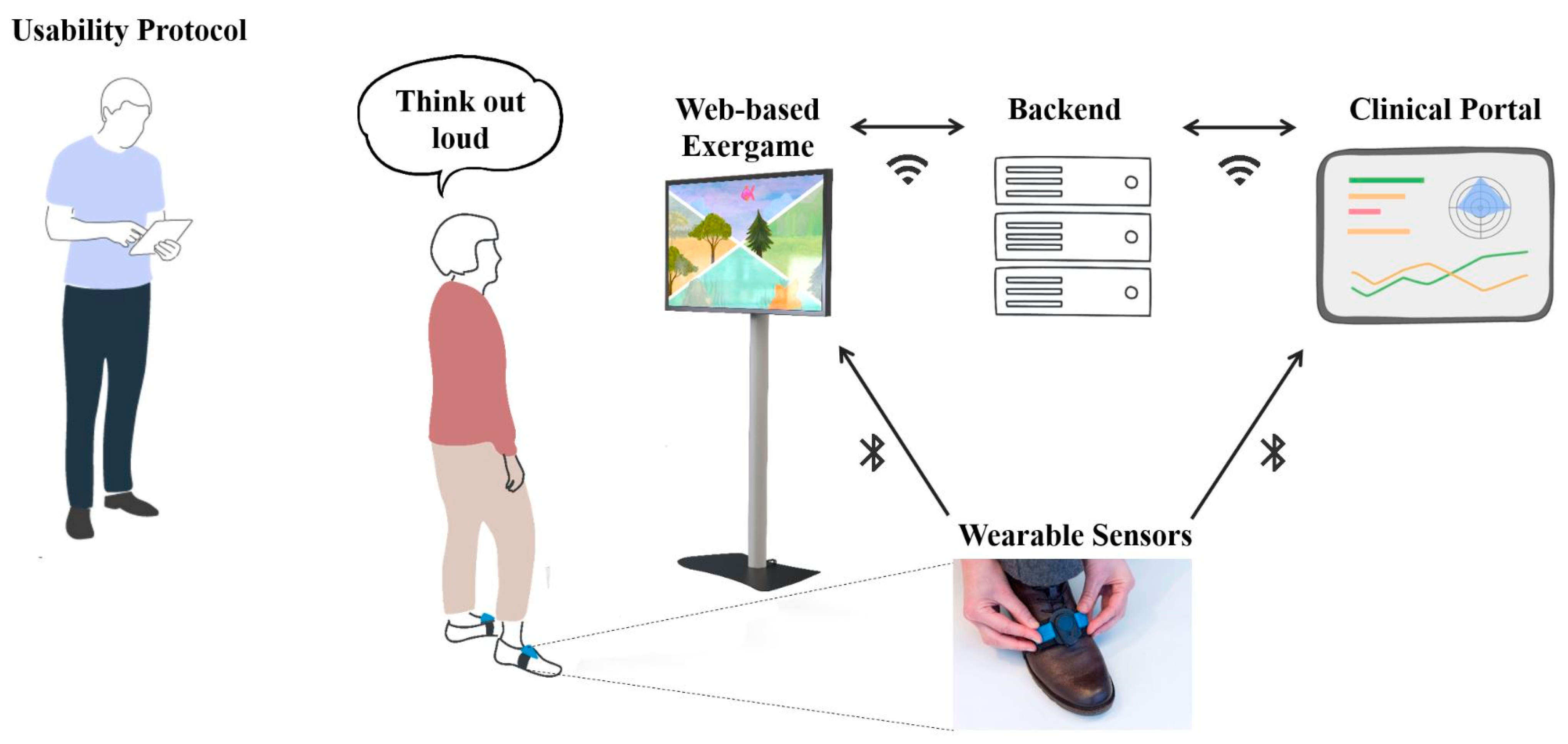
2.3.1. Qualitative Observation (Usability Protocol)
2.3.2. System Usability Scale
2.3.3. Qualitative Interview (Semi-Structured Interview)
2.4. Other Outcomes: Intensity Rating
2.5. Data Analysis
3. Results
3.1. Primary Outcome: Usability
3.1.1. Usability Protocol
3.1.2. System Usability Scale
3.1.3. Qualitative Interview Analysis
Game
P09: The diet, with healthy food. Because healthy eating is important to me.
P10: Mommy Chicken. Because you could go up or left/right or down. Is there enough time or not? Will the chicken catch me or not? …
P13: The bookcase because it is very familiar to me from home.
P06: The other minigames were very nice.P10: … The game environment was good and interesting. You knew where you had to go. The picture is good for the game.
P13: The pictures were not so clear. I didn’t necessarily see a vegetable there…. Is that a vegetable or not? Maybe it shouldn’t be drawn so modern, but in a way that you can see more of what it actually is.
P08: I didn’t notice any music, but I’m not that musical either.
P10: … Acoustics were good, the rhythm helps.
P04: I would like to know if I was any better or not, to know the progression.
P06: The feedback was perfect. I have always seen the success very well. I have not missed anything.
P06: Yes, the minigames were structured in an understandable way. I didn’t have to think much…
VITAAL Exergame Interaction
P02: It took me a long time to understand what I had to do. It was difficult at the beginning, but not afterwards.
P06: … It needs someone to do an introduction on the screen, but afterwards it goes very well.
P08: … Explanations would have been good. One could not know what was coming.
P12: Yes. I liked that the game controls were direct and not very complex.
P03: Steps forward and backward were recognized less well compared to left and right. A step to the left was detected better than a step to the right.
P06: The step backwards into the middle was sometimes refused. This bothered me a little and made me feel insecure. I did not know if I was causing this.
P10: Sometimes I was a bit too impatient until the signal from the sensor reached the screen. The screen did not follow.
P10: The arrow is hard to see if you have black shoes. You have to make sure that the arrow is facing forwards.
P06: Yes. The introduction on the screen was not very clear, I needed help… But otherwise, it is actually very simple.
P08: I did not find them easy to handle. I have never put on such sensors.
P14: No, there were no technical problems. Once, the sensors did not react properly.
P12: Yes, it was fun. I haven’t done anything like that in a long time.
P15: I really liked the handling and experience of the VITAAL exergame, I would do it more often.
Body and Mind
P10: Yes, I felt immersed in the game. That has to do with concentration as well. You are immediately focused.
P10: Yes, I noticed how good or bad I was in the game. Especially with the cakes I was wrong for a while, there you had to concentrate a lot. I also saw the points and knew immediately whether I was good or bad.
P08: Did I receive points? I did not notice.
P06: I focused more on the cognitive, 100%.
P12: I focused on solving the task as determinedly as possible and not letting myself get distracted. I focused more on the game.
P15: Back and forth, front and back … I focused more on the steps and the body than on the game.
P14: I focused on both, physical and mental. You have to coordinate both.
P07: Yes, the movements felt natural to me.
P03: I felt good while playing. It was fun, varying, and enjoyable.
P06: … I am enthusiastic about Exergame, I think it is very good. … after 6–7 min you are part of the game.
P12: … There were fluctuations at the beginning, a bit of uncertainty about what it’s all about, what I have to do. After that, it became a bit more relaxed.
Motivation
P10: It was interesting, especially that it had different minigames.
P15: Yes, it really motivated me. I had to move a lot.
P09: The game is fun when you can learn something and improve your reaction.
P10: Yes, I could imagine that the game is still fun after playing it several times and that you become ambitious over time.
P14: It’s certainly good for the body when you do something like this.
P13: I can’t do anything with this subject matter and these drawings. It could be that it becomes boring. For it not to be boring, the subjects and drawings would have to be more realistic, like photographs, not sketches.
P10: Yes, I could imagine it, if you could download it. For the brain, coordination, agility… it has a little bit of everything in it.
Training
P03: Yes, it was challenging. Especially mentally.
P12: To really step on the ground with the tip of your foot was challenging.
P14: In the back was the effort, there was fatigue.
P15: … especially the squats at the end. That’s when I needed a rest.
In contrast, some subjects wished for a more physically demanding training program (n = 5).
P09: … More physically demanding would also be good.
P15: You had to really concentrate, and make sure you took the right steps.
P12: It should not be much more at a time, that half hour was good.
P14: That was good. In the beginning, the training should not be longer.
P09: No, I have never been afraid to fall.
Comparison to Conventional Therapy/Exercises
P15: In my head, I had to do more compared to the other therapies.
P04: It is easier compared to therapy.
P02: About the same effort compared to therapy/everyday life.
Suggestions
P01: It just doesn’t have enough body intensity in it. The body is not used enough in this game.
P15: Yes, I would have more ideas, minigames with animals from the mountains such as chamois or ibex.
3.1.4. Other Outcome Results
4. Discussion
4.1. Limitations
4.2. Implications for the VITAAL Exergame
- Another movement for the “exit function” should be considered, as calf raises seem to be difficult for older adults with mobility limitations.
- Design aspects such as contrast and size are important when it comes to the usability of exergames for older adults. Therefore, the size or contrast of the arrow on the sensors should be adjusted to ensure easier handling. Furthermore, the design of the food in the “Healthy Food” minigame should be revised and presented in a more realistic design.
- Especially for older adults, explanations on how the exergame is installed (sensor connection), how the game control works, and what the game tasks includes are required.
- Even though the step detection algorithm works quite well, minor changes should be made to react faster to participant movements.
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Decade of Healthy Ageing: Baseline Report; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Isaacs, B. An Introduction to Geriatrics; Baillière, Tindall & Cassell: London, UK, 1965. [Google Scholar]
- Davis, J.C.; Best, J.R.; Bryan, S.; Li, L.C.; Hsu, C.L.; Gomez, C.; Vertes, K.; Liu-Ambrose, T. Mobility Is a Key Predictor of Change in Well-Being Among Older Adults Who Experience Falls: Evidence From the Vancouver Falls Prevention Clinic Cohort. Arch. Phys. Med. Rehabil. 2015, 96, 1634–1640. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patla, A.E.; Shumway-Cook, A. Dimensions of mobility: Defining the complexity and difficulty associated with community mobility. J. Aging Phys. Act. 1999, 7, 7–19. [Google Scholar] [CrossRef]
- Hoffman, J.M.; Shumway-Cook, A.; Yorkston, K.M.; Ciol, M.A.; Dudgeon, B.J.; Chan, L. Association of Mobility Limitations With Health Care Satisfaction and Use of Preventive Care: A Survey of Medicare Beneficiaries. Arch. Phys. Med. Rehabil. 2007, 88, 583–588. [Google Scholar] [CrossRef] [PubMed]
- Courtney-Long, E.A.; Carroll, D.D.; Zhang, Q.C.; Stevens, A.C.; Griffin-Blake, S.; Armour, B.S.; Campbell, V.A. Prevalence of disability and disability type among adults—United States, 2013. MMWR—Morb. Mortal. Wkly. Rep. 2015, 64, 777. [Google Scholar] [CrossRef] [PubMed]
- He, W.; Larsen, L. Older Americans with a Disability: 2008–2012; American Community Survey Reports; U. S. Government Printing Office: Washington, DC, USA, 2014.
- Jefferis, B.J.; Merom, D.; Sartini, C.; Wannamethee, S.G.; Ash, S.; Lennon, L.T.; Iliffe, S.; Kendrick, D.; Whincup, P.H. Physical Activity and Falls in Older Men: The Critical Role of Mobility Limitations. Med. Sci. Sports Exerc. 2015, 47, 2119–2128. [Google Scholar] [CrossRef] [Green Version]
- Shumway-Cook, A.; Ciol, M.A.; Hoffman, J.; Dudgeon, B.J.; Yorkston, K.; Chan, L. Falls in the Medicare Population: Incidence, Associated Factors, and Impact on Health Care. Phys. Ther. 2009, 89, 324–332. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mänty, M.; Heinonen, A.; Viljanen, A.; Pajala, S.; Koskenvuo, M.; Kaprio, J.; Rantanen, T. Self-reported preclinical mobility limitation and fall history as predictors of future falls in older women: Prospective cohort study. Osteoporos. Int. 2010, 21, 689–693. [Google Scholar] [CrossRef] [PubMed]
- Rubenstein, L.Z. Falls in older people: Epidemiology, risk factors and strategies for prevention. Age Ageing 2006, 35 (Suppl. 2), ii37–ii41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heiland, E.G.; Welmer, A.K.; Wang, R.; Santoni, G.; Angleman, S.; Fratiglioni, L.; Qiu, C. Association of mobility limitations with incident disability among older adults: A population-based study. Age Ageing 2016, 45, 812–819. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Melzer, D.; Lan, T.-Y.; Guralnik, J.M. The predictive validity for mortality of the index of mobility-related limitation—Results from the EPESE study. Age Ageing 2003, 32, 619–625. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hennessy, S.; Kurichi, J.E.; Pan, Q.; Streim, J.E.; Bogner, H.R.; Xie, D.; Stineman, M.G. Disability Stage is an Independent Risk Factor for Mortality in Medicare Beneficiaries Aged 65 Years and Older. PM R 2015, 7, 1215–1225. [Google Scholar] [CrossRef] [Green Version]
- Rosso, A.L.; Taylor, J.A.; Tabb, L.P.; Michael, Y.L. Mobility, Disability, and Social Engagement in Older Adults. J. Aging Health 2013, 25, 617–637. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, C.-T.; Yeh, C.-J.; Lee, M.-C.; Lin, H.-S.; Chen, V.C.-H.; Hsieh, M.-H.; Yen, C.-H.; Lai, T.-J. Social support and mobility limitation as modifiable predictors of improvement in depressive symptoms in the elderly: Results of a national longitudinal study. Arch. Gerontol. Geriatr. 2012, 55, 530–538. [Google Scholar] [CrossRef] [PubMed]
- Schulz, R.; Beach, S.R.; Czaja, S.J.; Martire, L.M.; Monin, J.K. Family Caregiving for Older Adults. Annu. Rev. Psychol. 2020, 71, 635–659. [Google Scholar] [CrossRef]
- Musich, S.; Wang, S.S.; Ruiz, J.; Hawkins, K.; Wicker, E. The impact of mobility limitations on health outcomes among older adults. Geriatr. Nurs. 2018, 39, 162–169. [Google Scholar] [CrossRef] [PubMed]
- Bahureksa, L.; Najafi, B.; Saleh, A.; Sabbagh, M.; Coon, D.; Mohler, M.J.; Schwenk, M. The Impact of Mild Cognitive Impairment on Gait and Balance: A Systematic Review and Meta-Analysis of Studies Using Instrumented Assessment. Gerontology 2017, 63, 67–83. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brown, C.J.; Flood, K.L. Mobility Limitation in the Older Patient: A Clinical Review. JAMA 2013, 310, 1168–1177. [Google Scholar] [CrossRef] [PubMed]
- Groessl, E.J.; Kaplan, R.M.; Rejeski, W.J.; Katula, J.A.; King, A.C.; Frierson, G.; Glynn, N.W.; Hsu, F.C.; Walkup, M.; Pahor, M. Health-related quality of life in older adults at risk for disability. Am. J. Prev. Med. 2007, 33, 214–218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pirker, W.; Katzenschlager, R. Gait disorders in adults and the elderly: A clinical guide. Wien. Klin. Wochenschr. 2017, 129, 81–95. [Google Scholar] [CrossRef] [Green Version]
- Lee, Y.-J.; Hung, W.-L. The relationship between exercise participation and well-being of the retired elderly. Aging Ment. Health 2011, 15, 873–881. [Google Scholar] [CrossRef] [PubMed]
- Schoene, D.; Valenzuela, T.; Lord, S.R.; de Bruin, E.D. The effect of interactive cognitive-motor training in reducing fall risk in older people: A systematic review. BMC Geriatr. 2014, 14, 1. [Google Scholar] [CrossRef] [Green Version]
- Sherrington, C.; Whitney, J.C.; Lord, S.R.; Herbert, R.D.; Cumming, R.G.; Close, J.C.T. Effective Exercise for the Prevention of Falls: A Systematic Review and Meta-Analysis. J. Am. Geriatr. Soc. 2008, 56, 2234–2243. [Google Scholar] [CrossRef]
- Skelton, D.A.; Dinan, S.M. Exercise for falls management: Rationale for an exercise programme aimed at reducing postural instability. Physiother. Theory Pract. 1999, 15, 105–120. [Google Scholar] [CrossRef]
- de Bruin, E.; Schmidt, A. Walking behaviour of healthy elderly: Attention should be paid. Behav. Brain Funct. 2010, 6, 59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Segev-Jacubovski, O.; Herman, T.; Yogev-Seligmann, G.; Mirelman, A.; Giladi, N.; Hausdorff, J.M. The interplay between gait, falls and cognition: Can cognitive therapy reduce fall risk? Expert Rev. Neurother. 2011, 11, 1057–1075. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yogev-Seligmann, G.; Hausdorff, J.M.; Giladi, N. The role of executive function and attention in gait. Mov. Disord. 2008, 23, 329–342. [Google Scholar] [CrossRef] [Green Version]
- Holtzer, R.; Verghese, J.; Xue, X.; Lipton, R.B. Cognitive processes related to gait velocity: Results from the Einstein Aging Study. Neuropsychology 2006, 20, 215. [Google Scholar] [CrossRef] [PubMed]
- Mirelman, A.; Herman, T.; Brozgol, M.; Dorfman, M.; Sprecher, E.; Schweiger, A.; Giladi, N.; Hausdorff, J.M. Executive function and falls in older adults: New findings from a five-year prospective study link fall risk to cognition. PLoS ONE 2012, 7, e40297. [Google Scholar] [CrossRef] [PubMed]
- Buchman, A.S.; Boyle, P.A.; Leurgans, S.E.; Barnes, L.L.; Bennett, D.A. Cognitive function is associated with the development of mobility impairments in community-dwelling elders. Am. J. Geriatr. Psychiatry J. Am. Assoc. Geriatr. Psychiatry 2011, 19, 571–580. [Google Scholar] [CrossRef] [Green Version]
- Eggenberger, P.; Theill, N.; Holenstein, S.; Schumacher, V.; de Bruin, E.D. Multicomponent physical exercise with simultaneous cognitive training to enhance dual-task walking of older adults: A secondary analysis of a 6-month randomized controlled trial with 1-year follow-up. Clin. Interv. Aging 2015, 10, 1711–1732. [Google Scholar] [CrossRef] [Green Version]
- Pichierri, G.; Wolf, P.; Murer, K.; de Bruin, E.D. Cognitive and cognitive-motor interventions affecting physical functioning: A systematic review. BMC Geriatr. 2011, 11, 29. [Google Scholar] [CrossRef] [Green Version]
- Bamidis, P.; Vivas, A.; Styliadis, C.; Frantzidis, C.; Klados, M.; Schlee, W.; Siountas, A.; Papageorgiou, S. A review of physical and cognitive interventions in aging. Neurosci. Biobehav. Rev. 2014, 44, 206–220. [Google Scholar] [CrossRef]
- Izquierdo, M.; Merchant, R.A.; Morley, J.E.; Anker, S.D.; Aprahamian, I.; Arai, H.; Aubertin-Leheudre, M.; Bernabei, R.; Cadore, E.L.; Cesari, M.; et al. International Exercise Recommendations in Older Adults (ICFSR): Expert Consensus Guidelines. J. Nutr. Health Aging 2021, 25, 824–853. [Google Scholar] [CrossRef]
- Bangsbo, J.; Blackwell, J.; Boraxbekk, C.J.; Caserotti, P.; Dela, F.; Evans, A.B.; Jespersen, A.P.; Gliemann, L.; Kramer, A.F.; Lundbye-Jensen, J.; et al. Copenhagen Consensus statement 2019: Physical activity and ageing. Br. J. Sports Med. 2019, 53, 856–858. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tomás, M.T.; Galán-Mercant, A.; Carnero, E.A.; Fernandes, B. Functional Capacity and Levels of Physical Activity in Aging: A 3-Year Follow-up. Front. Med. 2018, 4, 244. [Google Scholar] [CrossRef]
- Dias, J.F.; Oliveira, V.C.; Borges, P.R.T.; Dutra, F.; Mancini, M.C.; Kirkwood, R.N.; Resende, R.A.; Sampaio, R.F. Effectiveness of exercises by telerehabilitation on pain, physical function and quality of life in people with physical disabilities: A systematic review of randomised controlled trials with GRADE recommendations. Br. J. Sports Med. 2021, 55, 155–162. [Google Scholar] [CrossRef] [PubMed]
- de Bruin, E.; Schoene, D.; Pichierri, G.; Smith, S.T. Use of virtual reality technique for the training of motor control in the elderly Some theoretical considerations. Z. Gerontol. Geriatr. 2010, 43, 229–234. [Google Scholar] [CrossRef]
- Oh, Y.; Yang, S. Defining exergames & exergaming. In Proceedings of the Meaningful Play 2010, East Lansing, MI, USA, 21–23 October 2010; pp. 1–17. [Google Scholar]
- Rizzo, A.; Kim, G.J. A SWOT analysis of the field of virtual reality rehabilitation and therapy. Presence—Teleoper. Virtual Environ. 2005, 14, 119–146. [Google Scholar] [CrossRef]
- Bamidis, P.D. Building neuroscientific evidence and creating best practices for Active and Healthy Aging through ubiquitous exergaming and Living Labs. In Proceedings of the 2015 37th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Milan, Italy, 25–29 August 2015; IEEE: Piscataway, NJ, USA, 2015. [Google Scholar]
- Konstantinidis, E.I.; Billis, A.S.; Mouzakidis, C.A.; Zilidou, V.I.; Antoniou, P.E.; Bamidis, P.D. Design, implementation, and wide pilot deployment of fitForAll: An easy to use exergaming platform improving physical fitness and life quality of senior citizens. IEEE J. Biomed. Health Inform. 2016, 20, 189–200. [Google Scholar] [CrossRef]
- Smith, S.T.; Schoene, D. The use of exercise-based videogames for training and rehabilitation of physical function in older adults: Current practice and guidelines for future research. Aging Health 2012, 8, 243–252. [Google Scholar] [CrossRef]
- Stanmore, E.; Stubbs, B.; Vancampfort, D.; de Bruin, E.D.; Firth, J. The effect of active video games on cognitive functioning in clinical and non-clinical populations: A meta-analysis of randomized controlled trials. Neurosci. Biobehav. Rev. 2017, 78, 34–43. [Google Scholar] [CrossRef]
- Mura, G.; Carta, M.G.; Sancassiani, F.; Machado, S.; Prosperini, L. Active exergames to improve cognitive functioning in neurological disabilities: A systematic review and meta-analysis. Eur. J. Phys. Rehabil. Med. 2018, 54, 450–462. [Google Scholar] [CrossRef] [PubMed]
- Pirovano, M.; Surer, E.; Mainetti, R.; Lanzi, P.L.; Borghese, N.A. Exergaming and rehabilitation: A methodology for the design of effective and safe therapeutic exergames. Entertain. Comput. 2016, 14, 55–65. [Google Scholar] [CrossRef]
- Nawaz, A.; Skjaeret, N.; Helbostad, J.L.; Vereijken, B.; Boulton, E.; Svanaes, D. Usability and acceptability of balance exergames in older adults: A scoping review. Health Inform. J. 2016, 22, 911–931. [Google Scholar] [CrossRef]
- Hoffmann, K.; Sportwiss, D.; Hardy, S.; Wiemeyer, J.; Gobel, S. Personalized Adaptive Control of Training Load in Cardio-Exergames—A Feasibility Study. Games Health J. 2015, 4, 470–479. [Google Scholar] [CrossRef] [PubMed]
- Uzor, S.; Baillie, L. Investigating the long-term use of exergames in the home with elderly fallers. Proceedings of the SIGCHI Conference on Human Factors in Computing Systems, Toronto, ON, Canada, 26 April–1 May 2014; ACM: New York, NY, USA, 2014. [Google Scholar]
- Gerling, K.M.; Schulte, F.P.; Smeddinck, J.; Masuch, M. Game Design for Older Adults: Effects of Age-Related Changes on Structural Elements of Digital Games; Springer: Berlin/Heidelberg, Germany, 2012. [Google Scholar]
- Ijsselsteijn, W.; Nap, H.H.; de Kort, Y.; Poels, K. Digital game design for elderly users. Proceedings of the 2007 conference on Future Play, Toronto, ON, Canada, 14–17 November 2007; ACM: New York, NY, USA, 2007. [Google Scholar]
- Gerling, K.M.; Schild, J.; Masuch, M. Exergame design for elderly users: The case study of SilverBalance. Proceedings of the 7th International Conference on Advances in Computer Entertainment Technology, Taipei, Taiwan, 17–19 November 2010; ACM: New York, NY, USA, 2010. [Google Scholar]
- Eckert, J.K.; Morgan, L.A.; Swamy, N. Preferences for receipt of care among community-dwelling adults. J. Aging Soc. Policy 2004, 16, 49–65. [Google Scholar] [CrossRef]
- Silveira, P.; van het Reve, E.; Daniel, F.; Casati, F.; de Bruin, E.D. Motivating and assisting physical exercise in independently living older adults: A pilot study. Int. J. Med. Inform. 2013, 82, 325–334. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kushniruk, A.W.; Patel, V.L. Cognitive and usability engineering methods for the evaluation of clinical information systems. J. Biomed. Inform. 2004, 37, 56–76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stookey, A.D.; Katzel, L.I.; Steinbrenner, G.; Shaughnessy, M.; Ivey, F.M. The short physical performance battery as a predictor of functional capacity after stroke. J. Stroke Cereb. Dis. 2014, 23, 130–135. [Google Scholar] [CrossRef] [Green Version]
- Vasunilashorn, S.; Coppin, A.K.; Patel, K.V.; Lauretani, F.; Ferrucci, L.; Bandinelli, S.; Guralnik, J.M. Use of the Short Physical Performance Battery Score to predict loss of ability to walk 400 meters: Analysis from the InCHIANTI study. J. Gerontol. A Biol. Sci. Med. Sci. 2009, 64, 223–229. [Google Scholar] [CrossRef]
- Vazzana, R.; Bandinelli, S.; Lauretani, F.; Volpato, S.; Lauretani, F.; Di Iorio, A.; Abate, M.; Corsi, A.M.; Milaneschi, Y.; Guralnik, J.M.; et al. Trail Making Test predicts physical impairment and mortality in older persons. J. Am. Geriatr. Soc. 2010, 58, 719–723. [Google Scholar] [CrossRef] [Green Version]
- Thomann, A.E.; Goettel, N.; Monsch, R.J.; Berres, M.; Jahn, T.; Steiner, L.A.; Monsch, A.U. The Montreal Cognitive Assessment: Normative Data from a German-Speaking Cohort and Comparison with International Normative Samples. Available online: http://www.mocatest.ch/test/ (accessed on 24 May 2021).
- Hwang, W.; Salvendy, G. Number of people required for usability evaluation: The 10 ± 2 rule. Commun. ACM 2010, 53, 130–133. [Google Scholar] [CrossRef]
- Lan, C.; Lai, J.S.; Chen, S.Y.; Wong, M.K. Tai Chi Chuan to improve muscular strength and endurance in elderly individuals: A pilot study. Arch. Phys. Med. Rehabil. 2000, 81, 604–607. [Google Scholar] [CrossRef]
- Lan, C.; Wolf, S.L.; Tsang, W.W. Tai chi exercise in medicine and health promotion. Evid. Based Complement. Altern. Med. 2013, 2013, 298768. [Google Scholar] [CrossRef] [PubMed]
- Okubo, Y.; Schoene, D.; Lord, S.R. Step training improves reaction time, gait and balance and reduces falls in older people: A systematic review and meta-analysis. Br. J. Sports Med. 2017, 51, 586–893. [Google Scholar] [CrossRef]
- Kattenstroth, J.-C.; Kalisch, T.; Holt, S.; Tegenthoff, M.; Dinse, H.R. Six months of dance intervention enhances postural, sensorimotor, and cognitive performance in elderly without affecting cardio-respiratory functions. Front. Aging Neurosci. 2013, 5, 5. [Google Scholar] [CrossRef] [Green Version]
- Merom, D.; Cumming, R.; Mathieu, E.; Anstey, K.J.; Rissel, C.; Simpson, J.M.; Morton, R.L.; Cerin, E.; Sherrington, C.; Lord, S.R. Can social dancing prevent falls in older adults? A protocol of the Dance, Aging, Cognition, Economics (DAnCE) fall prevention randomised controlled trial. BMC Public Health 2013, 13, 477. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gajewski, P.D.; Falkenstein, M. Physical activity and neurocognitive functioning in aging—A condensed updated review. Eur. Rev. Aging Phys. Act. 2016, 13, 1. [Google Scholar] [CrossRef] [Green Version]
- Guimaraes, V.; Sousa, I.; Correia, M.V. Orientation-Invariant Spatio-Temporal Gait Analysis Using Foot-Worn Inertial Sensors. Sensors 2021, 21, 3940. [Google Scholar] [CrossRef]
- Eccles, D.W.; Arsal, G. The think aloud method: What is it and how do I use it? Qual. Res. Sport Exerc. Health 2017, 9, 514–531. [Google Scholar] [CrossRef]
- Lewis, C.; Rieman, J. Task-Centered User Interface Design. A Practical Introduction; University of Colorado, Boulder, Department of Computer Science: Boulder, CO, USA, 1993. [Google Scholar]
- Brooke, J. SUS-A quick and dirty usability scale. Usability Eval. Ind. 1996, 189, 4–7. [Google Scholar]
- Mol, M.; van Schaik, A.; Dozeman, E.; Ruwaard, J.; Vis, C.; Ebert, D.D.; Etzelmueller, A.; Mathiasen, K.; Moles, B.; Mora, T.; et al. Dimensionality of the system usability scale among professionals using internet-based interventions for depression: A confirmatory factor analysis. BMC Psychiatry 2020, 20, 218. [Google Scholar] [CrossRef]
- Tullis, T.; Albert, W.; Dumas, J.S.; Loring, B.A. Measuring the User Experience: Collecting Analyzing, and Presenting Usability Metrics: Second Edition; Morgan Kaufmann: Burlington, MA, USA, 2008. [Google Scholar]
- Adcock, M.; Sonder, F.; Schättin, A.; Gennaro, F.; de Bruin, E.D. A usability study of a multicomponent video game-based training for older adults. Eur. Rev. Aging Phys. Act. 2020, 17, 3. [Google Scholar] [CrossRef] [Green Version]
- Vaziri, D.D.; Aal, K.; Ogonowski, C.; Von Rekowski, T.; Kroll, M.; Marston, H.R.; Poveda, R.; Gschwind, Y.J.; Delbaere, K.; Wieching, R.; et al. Exploring user experience and technology acceptance for a fall prevention system: Results from a randomized clinical trial and a living lab. Eur. Rev. Aging Phys. Act. 2016, 13, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nawaz, A.; Skjæret, N.; Ystmark, K.; Helbostad, J.L.; Vereijken, B.; Svanæs, D. Assessing seniors’ user experience (UX) of exergames for balance training. In Proceedings of the 8th Nordic Conference on Human-Computer Interaction: Fun, Fast, Foundational, Helsinki, Finland, 26–30 October 2014; Association for Computing Machinery: New York, NY, USA, 2014; pp. 578–587. [Google Scholar]
- Jansen-Kosterink, S.; Veld, R.; Schönauer, C.; Kaufmann, H.; Hermens, H.; Vollenbroek-Hutten, M. A Serious Exergame for Patients Suffering from Chronic Musculoskeletal Back and Neck Pain: A Pilot Study. Games Health J. 2013, 2, 299–307. [Google Scholar] [CrossRef]
- Bangor, A.; Kortum, P.; Miller, J. Determining what individual SUS scores mean: Adding an adjective rating scale. J. Usability Stud. 2009, 4, 114–123. [Google Scholar]
- World Health Organization. Global Recommendations on Physical Activity for Health; World Health Organization: Geneva, Switzerland, 2010; p. 60. [Google Scholar]
- Mayring, P.; Fenzl, T. Qualitative Inhaltsanalyse. In Handbuch Methoden der Empirischen Sozialforschung; Baur, N., Blasius, J., Eds.; Springer Fachmedien Wiesbaden: Wiesbaden, Germany, 2019; pp. 633–648. [Google Scholar]
- Mayring, P. Qualitative Content Analysis: Theoretical Foundation, Basic Procedures and Software Solution; Social Science Open Access Repository (SSOAR): Klagenfurt, Austria, 2014. [Google Scholar]
- Fenzl, T.; Mayring, P. QCAmap: Eine Interaktive Webapplikation für Qualitative Inhaltsanalyse; Beltz Juventa: Weinheim, Germany, 2017. [Google Scholar]
- Mayring, P. QCAmap Step by Step—A Software Handbook; QCAmap: Klagenfurt, Austria, 2020. [Google Scholar]
- Downey, R.G.; King, C.V. Missing Data in Likert Ratings: A Comparison of Replacement Methods. J. Gen. Psychol. 1998, 125, 175–191. [Google Scholar] [CrossRef]
- Peretti, A.; Amenta, F.; Tayebati, S.K.; Nittari, G.; Mahdi, S.S. Telerehabilitation: Review of the State-of-the-Art and Areas of Application. JMIR Rehabil. Assist. Technol. 2017, 4, e7. [Google Scholar] [CrossRef] [PubMed]
- Seron, P.; Oliveros, M.J.; Gutierrez-Arias, R.; Fuentes-Aspe, R.; Torres-Castro, R.C.; Merino-Osorio, C.; Nahuelhual, P.; Inostroza, J.; Jalil, Y.; Solano, R.; et al. Effectiveness of Telerehabilitation in Physical Therapy: A Rapid Overview. Phys. Ther. 2021, 101, pzab053. [Google Scholar] [CrossRef]
- Brach, M.; Hauer, K.; Rotter, L.; Werres, C.; Korn, O.; Konrad, R.; Göbel, S. Modern principles of training in exergames for sedentary seniors: Requirements and approaches for sport and exercise sciences. Int. J. Comput. Sci. Sport 2012, 11, 86–99. [Google Scholar]
- Bleakley, C.M.; Charles, D.; Porter-Armstrong, A.; McNeill, M.D.; McDonough, S.M.; McCormack, B. Gaming for health: A systematic review of the physical and cognitive effects of interactive computer games in older adults. J. Appl. Gerontol. 2015, 34, Np166–Np189. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Shen, Z.; Liu, S.; Yuan, D.; Miao, C. Ping Pong: An Exergame for Cognitive Inhibition Training. Int. J. Hum.–Comput. Interact. 2021, 37, 1104–1115. [Google Scholar] [CrossRef]
- Bangor, A.; Kortum, P.T.; Miller, J.T. An Empirical Evaluation of the System Usability Scale. Int. J. Hum.–Comput. Interact. 2008, 24, 574–594. [Google Scholar] [CrossRef]
- Meekes, W.; Stanmore, E.K. Motivational Determinants of Exergame Participation for Older People in Assisted Living Facilities: Mixed-Methods Study. J. Med. Internet Res. 2017, 19, e238. [Google Scholar] [CrossRef]
- Beck, L.A. Csikszentmihalyi, Mihaly. (1990). Flow: The Psychology of Optimal Experience. J. Leis. Res. 1992, 24, 93–94. [Google Scholar] [CrossRef]
- Huang, H.-C.; Pham, T.T.L.; Wong, M.-K.; Chiu, H.-Y.; Yang, Y.-H.; Teng, C.-I. How to create flow experience in exergames? Perspective of flow theory. Telemat. Inform. 2018, 35, 1288–1296. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Participant Characteristics | n = 13 |
|---|---|
| Age in years | 80.5 ± 4.9 (71–89) |
| Weight in kg | 69.1 ± 13.6 (51–98) |
| Height in cm | 164.3 ± 4.8 (158–172) |
| Education in years | 11.9 ± 2.8 (9–19) |
| MoCA Score | 26.9 ± 1.9 (24–30) |
| SPPB Score | 8.5 ± 1.3 (6–10) |
| Sex [n, %] | |
| Female | 9 (69.2) |
| Male | 4 (30.8) |
| Self-evaluation of muscle strength [n, %] | |
| Very good | 1 (7.7) |
| Good | 2 (15.4) |
| Medium | 7 (53.8) |
| Bad | 3 (23.1) |
| I don’t know | 0 (0.0) |
| Problems with legs [n, %] | |
| No | 6 (46.2) |
| Sometimes | 5 (38.5) |
| Always | 2 (15.4) |
| I don’t know | 0 (0.0) |
| Fear of falling [n, %] | |
| Never | 7 (53.8) |
| Sometimes | 4 (30.8) |
| Often | 1 (7.7) |
| Always | 1 (7.7) |
| Number of falls during last 6 month * [n, %] | |
| Never | 8 (61.5) |
| Once | 2 (15.4) |
| More than once | 3 (23.1) |
| Walking aids [n, %] | |
| No | 10 (76.9) |
| Cane/Stick/Crutch | 3 (23.1) |
| Rollator | 0 (0.0) |
| Physical activity [n, %] | |
| >3 x/week | 8 (61.5) |
| 1–3 x/week | 5 (38.5) |
| 1 x/week | 0 (0.0) |
| No | 0 (0.0) |
| Use of video games in everyday life [n, %] | |
| Yes | 2 (15.4) |
| No | 11 (84.6) |
| Experience with exergames [n, %] | |
| Yes | 8 (61.5) |
| No | 5 (38.5) |
| Urinary incontinence * [n, %] | |
| Yes | 2 (15.4) |
| No | 10 (76.9) |
| Missing | 1 (7.7) |
| Cognitive impairment * [n, %] | |
| Yes | 2 (15.4) |
| No | 10 (76.9) |
| Missing | 1 (7.7) |
| VITAAL Exergame Interaction | Summary:Despite the explanations built into the game, additional guidance was needed on the technical equipment, the game controls, and the games. | |
| Positive aspects | Negative aspects | |
|
| |
| Game Design | Summary:The games were found to be beautifully and interestingly designed. Nevertheless, recognizing specific objects was not always easy. | |
| Positive aspects | Negative aspects | |
|
| |
| Emotions | Summary:The game is fun, makes you laugh, and motivates you to play. However, if the game is not successful, it can also lead to disappointment, frustration, and dissatisfaction. | |
| Positive aspects | Negative aspects | |
|
| |
| Exercises | Summary:The steps and the squats can be performed properly and correctly in most cases. Most of the games are not physically demanding, except for the squats. The games are mainly cognitively demanding and require concentration. | |
| Positive aspects | Negative aspects | |
|
| |
| Risks/ Limitations | Summary:The calf raises, which are needed as an exit function, are not possible for many or only possible with help. Knee pain can limit strength training. | |
| Positive aspects | Negative aspects | |
|
| |
| Physical (0–10 Scale) | Cognitive (0–10 Scale) | |
|---|---|---|
| Balance | ||
| Falling Books [n] | n = 12 | n = 9 |
| 5.7 ± 1.4 (4–8) | 4.9 ± 2.8 (1–9) | |
| Mommy Chicken [n] | n = 8 | n = 5 |
| 5.6 ± 1.7 (3–8) | 5.6 ± 3.0 (2–9) | |
| Cognition | ||
| Healthy Food [n] | n = 10 | n = 8 |
| 2.5 ± 1.7 (0–6) | 4.0 ± 2.2 (2–8) | |
| Pizza [n] | n = 10 | n = 9 |
| 5.2 ± 2.5 (2–9) | 5.9 ± 1.9 (3–8) | |
| Shopping List [n] | n = 3 | n = 3 |
| 3.3 ± 4.2 (0–8) | 5.7 ± 3.5 (2–9) | |
| Strength | ||
| Narrow Squats [n] | n = 7 | n = 7 |
| 6.6 ± 1.0 (5–8) | 2.4 ± 2.2 (0–7) | |
| Wide Squats [n] | n = 3 | n = 3 |
| 6.3 ± 2.1 (4–8) | 2.0 ± 2.0 (0–4) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Thalmann, M.; Ringli, L.; Adcock, M.; Swinnen, N.; de Jong, J.; Dumoulin, C.; Guimarães, V.; de Bruin, E.D. Usability Study of a Multicomponent Exergame Training for Older Adults with Mobility Limitations. Int. J. Environ. Res. Public Health 2021, 18, 13422. https://doi.org/10.3390/ijerph182413422
Thalmann M, Ringli L, Adcock M, Swinnen N, de Jong J, Dumoulin C, Guimarães V, de Bruin ED. Usability Study of a Multicomponent Exergame Training for Older Adults with Mobility Limitations. International Journal of Environmental Research and Public Health. 2021; 18(24):13422. https://doi.org/10.3390/ijerph182413422
Chicago/Turabian StyleThalmann, Melanie, Lisa Ringli, Manuela Adcock, Nathalie Swinnen, Jacqueline de Jong, Chantal Dumoulin, Vânia Guimarães, and Eling D. de Bruin. 2021. "Usability Study of a Multicomponent Exergame Training for Older Adults with Mobility Limitations" International Journal of Environmental Research and Public Health 18, no. 24: 13422. https://doi.org/10.3390/ijerph182413422
APA StyleThalmann, M., Ringli, L., Adcock, M., Swinnen, N., de Jong, J., Dumoulin, C., Guimarães, V., & de Bruin, E. D. (2021). Usability Study of a Multicomponent Exergame Training for Older Adults with Mobility Limitations. International Journal of Environmental Research and Public Health, 18(24), 13422. https://doi.org/10.3390/ijerph182413422