
Factors Associated with Medication Non-Adherence among Patients with Multimorbidity and Polypharmacy Admitted to an Intermediate Care Center

 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
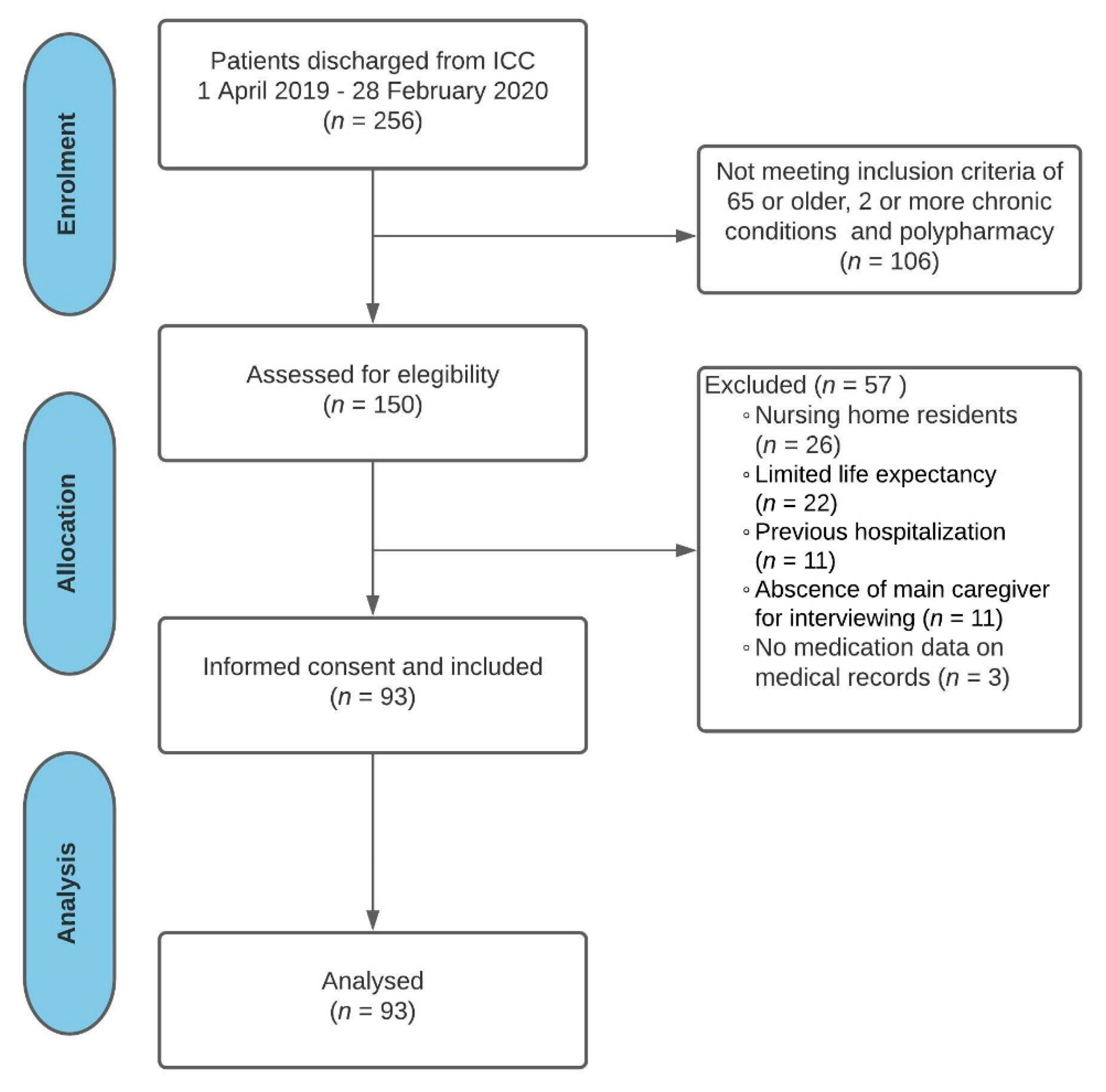
2.1. Study Site and Participants
2.2. Data Collection
2.2.1. Demographic and Clinical Data
2.2.2. Medication-Related Data
- Long-term medications: Estimated as the sum of every regularly scheduled medication intended to be administered for a period ≥ 3 months.
- Hyperpolypharmacy: Also known as excessive polypharmacy, defined as the use of 10 or more regularly scheduled long-term medications [24].
- Medication regimen complexity: Assessed as a continuous variable for all long-term medications (defined as regularly scheduled long-term medications plus when required (prn) medications) on admission using the Spanish-version Medication Regimen Complexity Index (MRCI) [25]. Furthermore, regimen complexity was also categorized as low (equivalent to MRCI < 20), medium–high (MRCI 20–39.5) or excessive (MRCI ≥ 40).
- Potentially inappropriate prescribing (PIP). Every patient’s treatment plan was analyzed by a geriatrician and a clinical pharmacist through the 4-stage patient-centered prescription (PCP) model, which centers therapeutic decisions on the patient’s global assessment. Such an approach represents an advanced medication review framework [28], which has been associated with reducing inappropriate prescribing and medication burden in patients with multimorbidity [29,30,31]. The PCP model was developed by the Central Catalonia Chronicity Research Group (C3RG) and its implementation in clinical practice is recommended by the Department of Health, Government of Catalonia (Spain) for elderly and frail patients with multimorbidity [32]. PIP was considered on admission in any of the following circumstances: absence of evidence-based indication, dosing unnecessarily high considering the patient’s specific therapeutic objectives, unacceptable ADEs, contraindicated drug–drug interaction, unnecessary therapeutic duplication, inappropriate dosing or pharmaceutical dosage form or any prescription characterized as potentially inappropriate by the American Geriatrics Society 2019 Updated Beers criteria® [33]. PIP was assessed as a continuous variable and categorized as moderate (≥2) and high (≥3) PIP burden.
- Self-reported adherence. A self-report measure of medication adherence was performed by using the Spanish-version Adherence to Refills and Medications Scale (ARMS-e) [34]. This scale consists of 12 items that assess patients’ ability to take and refill medications. Response options are on a Likert scale with responses of “none”, “some”, “most” or “all” of the time, which are given values from 1 to 4. Items were written so that a lower score is indicative of better medication adherence. The ARMS-e total score ranges from 12 to 48. Therefore, a patient that does not have any non-adherence issue will score 12, with higher scores indicating worst adherence. Written permission for conducting adherence assessments was obtained from the original developer of the English-version ARMS [35]. ARMS-e total score, based on an ordinal scale, was dichotomized through the median score using a cutoff value of 12 (optimal self-reported adherence = 12 and suboptimal self-reported adherence > 12).
- Medication management at home: Patients were grouped on three levels (independent, partially or totally assisted) with regard to their autonomy for medication administration and medication refills before hospital admission.
- Multiple discretized PDC: Medication adherence was assessed during a 6-month period before admission using the multiple discretized PDC, which was considered the main dependent variable. PDC for all regularly scheduled long-term medications was estimated as the sum of the days supplied for each medication according to electronic linked pharmacy claims data. At least two prescription refill dates during a period ≥ 90 days were required for each medication to calculate this ratio. The PDC rate was converted to a percentage based on the percentage of days covered by dispensed medication. Patients were considered adherent if PDC for each medication was ≥80% (excluding last refill) [15].
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Vetrano, D.L.; Palmer, K.; Marengoni, A.; Marzetti, E.; Lattanzio, F.; Roller-Wirnsberger, R.; Lopez Samaniego, L.; Rodríguez-Mañas, L.; Bernabei, R.; Onder, G. Frailty and Multimorbidity: A Systematic Review and Meta-analysis. J. Gerontol. Ser. A 2019, 74, 659–666. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, Q.D.; Wu, C.; Odden, M.C.; Kim, D.H. Multimorbidity patterns, frailty, and survival in community-dwelling older adults. J. Gerontol.-Ser. A Biol. Sci. Med. Sci. 2019, 74, 1265–1270. [Google Scholar] [CrossRef]
- Hughes, L.D.; McMurdo, M.E.T.; Guthrie, B. Guidelines for people not for diseases: The challenges of applying UK clinical guidelines to people with multimorbidity. Age Ageing 2013, 42, 62–69. [Google Scholar] [CrossRef]
- Fried, L.P.; Ferrucci, L.; Darer, J.; Williamson, J.D.; Anderson, G. Untangling the Concepts of Disability, Frailty, and Comorbidity: Implications for Improved Targeting and Care. J. Gerontol.-Ser. A Biol. Sci. Med. Sci. 2004, 59, 255–263. [Google Scholar] [CrossRef]
- Marengoni, A.; Onder, G. Guidelines, polypharmacy, and drug-drug interactions in patients with multimorbidity: A cascade of failure. BMJ 2015, 350, 10–11. [Google Scholar] [CrossRef] [PubMed]
- Vrijens, B.; De Geest, S.; Hughes, D.A.; Przemyslaw, K.; Demonceau, J.; Ruppar, T.; Dobbels, F.; Fargher, E.; Morrison, V.; Lewek, P.; et al. A new taxonomy for describing and defining adherence to medications. Br. J. Clin. Pharmacol. 2012, 73, 691–705. [Google Scholar] [CrossRef]
- World Health Organization. Adherence to Long-Term Therapies: Evidence for Action; World Health Organization: Geneva, Switzerland, 2003; Available online: http://apps.who.int/iris/bitstream/handle/10665/42682/9241545992.pdf?sequence=1 (accessed on 14 August 2021).
- González-Bueno, J.; Calvo-Cidoncha, E.; Sevilla-Sánchez, D.; Molist-Brunet, N.; Espaulella-Panicot, J.; Codina-Jané, C. Patient-centered prescription model to improve therapeutic adherence in patients with multimorbidity. Farm. Hosp. 2018, 42, 128–134. [Google Scholar]
- Pagès-Puigdemont, N.; Tuneu, L.; Masip, M.; Valls, P.; Puig, T.; Mangues, M.A. Determinants of medication adherence among chronic patients from an urban area: A cross-sectional study. Eur. J. Public Health 2019, 29, 419–424. [Google Scholar] [CrossRef] [PubMed]
- Pednekar, P.P.; Ágh, T.; Malmenäs, M.; Raval, A.D.; Bennett, B.M.; Borah, B.J.; Hutchins, D.S.; Manias, E.; Williams, A.F.; Hiligsmann, M.; et al. Methods for Measuring Multiple Medication Adherence: A Systematic Review–Report of the ISPOR Medication Adherence and Persistence Special Interest Group. Value Health 2019, 22, 139–156. [Google Scholar] [CrossRef]
- Giardini, A.; Martin, M.T.; Cahir, C.; Lehane, E.; Menditto, E.; Strano, M.; Pecorelli, S.; Monaco, A.; Marengoni, A. Toward appropriate criteria in medication adherence assessment in older persons: Position Paper. Aging Clin. Exp. Res. 2016, 28, 371–381. [Google Scholar] [CrossRef]
- Stirratt, M.J.; Dunbar-Jacob, J.; Crane, H.M.; Simoni, J.M.; Czajkowski, S.; Hilliard, M.E.; Aikens, J.E.; Hunter, C.M.; Velligan, D.I.; Huntley, K.; et al. Self-report measures of medication adherence behavior: Recommendations on optimal use. Transl. Behav. Med. 2015, 5, 470–482. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, T.M.U.; Caze, A.L.; Cottrell, N. What are validated self-report adherence scales really measuring? A systematic review. Br. J. Clin. Pharmacol. 2014, 77, 427–445. [Google Scholar] [CrossRef]
- Torres-Robles, A.; Wiecek, E.; Cutler, R.; Drake, B.; Benrimoj, S.I.; Fernandez-Llimos, F.; Garcia-Cardenas, V. Using Dispensing Data to Evaluate Adherence Implementation Rates in Community Pharmacy. Front. Pharmacol. 2019, 10, 130. [Google Scholar] [CrossRef]
- Pednekar, P.; Malmenas, M.M.; Ágh, T.; Bennett, B.; Peterson, A. Measuring multiple medication adherence—Which measure when? Value Outcomes Spotligh 2017, 17–20. Available online: https://www.ispor.org/docs/default-source/publications/newsletter/measuring_multiple_medication_adherence_which_measure_when.pdf?sfvrsn=f9946e55_0 (accessed on 14 August 2021).
- McMullen, C.K.; Safford, M.M.; Bosworth, H.B.; Phansalkar, S.; Leong, A.; Fagan, M.B.; Trontell, A.; Rumptz, M.; Vandermeer, M.L.; Brinkman, W.B.; et al. Patient-centered priorities for improving medication management and adherence. Patient Educ. Couns. 2015, 98, 102–110. [Google Scholar] [CrossRef][Green Version]
- Salisbury, C.; Johnson, L.; Purdy, S.; Valderas, J.M.; Montgomery, A.A. Epidemiology and impact of multimorbidity in primary care: A retrospective cohort study. Br. J. Gen. Pract. 2011, 61, e12–e21. [Google Scholar] [CrossRef]
- Gómez-Batiste, X.; Martínez-Muñoz, M.; Blay, C.; Amblàs, J.; Vila, L.; Costa, X.; Espaulella, J.; Villanueva, A.; Oller, R.; Martori, J.C.; et al. Utility of the NECPAL CCOMS-ICO© tool and the Surprise Question as screening tools for early palliative care and to predict mortality in patients with advanced chronic conditions: A cohort study. Palliat. Med. 2017, 31, 754–763. [Google Scholar] [CrossRef] [PubMed]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. PLoS Med. 2007, 4, 1623–1627. [Google Scholar] [CrossRef]
- De Geest, S.; Zullig, L.L.; Dunbar-Jacob, J.; Helmy, R.; Hughes, D.A.; Wilson, I.B.; Vrijens, B. ESPACOMP medication adherence reporting guideline (EMERGE). Ann. Intern. Med. 2018, 169, 30–35. [Google Scholar] [CrossRef]
- Amblàs-Novellas, J.; Martori, J.C.; Espaulella, J.; Oller, R.; Molist-Brunet, N.; Inzitari, M.; Romero-Ortuno, R. Frail-VIG index: A concise frailty evaluation tool for rapid geriatric assessment. BMC Geriatr. 2018, 18, 1–12. [Google Scholar] [CrossRef]
- Palmer, K.; Marengoni, A.; Forjaz, M.J.; Jureviciene, E.; Laatikainen, T.; Mammarella, F.; Muth, C.; Navickas, R.; Prados-Torres, A.; Rijken, M.; et al. Multimorbidity care model: Recommendations from the consensus meeting of the Joint Action on Chronic Diseases and Promoting Healthy Ageing across the Life Cycle (JA-CHRODIS). Health Policy 2018, 122, 4–11. [Google Scholar] [CrossRef] [PubMed]
- Crum, R.M.; Anthony, J.C.; Bassett, S.S.; Folstein, M.F. Population-Based Norms for the Mini-Mental State Examination by Age and Educational Level. JAMA 1993, 269, 2386–2391. [Google Scholar] [CrossRef]
- Gutiérrez-Valencia, M.; Izquierdo, M.; Cesari, M.; Casas-Herrero, Á.; Inzitari, M.; Martínez-Velilla, N. The relationship between frailty and polypharmacy in older people: A systematic review. Br. J. Clin. Pharmacol. 2018, 84, 1432–1444. [Google Scholar] [CrossRef] [PubMed]
- Saez de la Fuente, J.; Such Diaz, A.; Cañamares-Orbis, I.; Ramila, E.; Izquierdo-Garcia, E.; Esteban, C.; Escobar-Rodríguez, I. Cross-cultural Adaptation and Validation of the Medication Regimen Complexity Index Adapted to Spanish. Ann. Pharmacother. 2016, 50, 918–925. [Google Scholar] [CrossRef]
- Hilmer, S.N.; Mager, D.E.; Simonsick, E.M.; Cao, Y.; Ling, S.M.; Windham, B.G.; Harris, T.B.; Hanlon, J.T.; Rubin, S.M.; Shorr, R.I.; et al. A drug burden index to define the functional burden of medications in older people. Arch. Intern. Med. 2007, 167, 781–787. [Google Scholar] [CrossRef]
- Byrne, C.J.; Walsh, C.; Cahir, C.; Ryan, C.; Williams, D.J.; Bennett, K. Anticholinergic and sedative drug burden in community-dwelling older people: A national database study. BMJ Open 2018, 8, e022500. [Google Scholar] [CrossRef]
- Griese-Mammen, N.; Hersberger, K.E.; Messerli, M.; Leikola, S.; Horvat, N.; van Mil, J.W.F.; Kos, M. PCNE definition of medication review: Reaching agreement. Int. J. Clin. Pharm. 2018, 40, 1199–1208. [Google Scholar] [CrossRef]
- Molist Brunet, N.; Sevilla-Sánchez, D.; Amblàs Novellas, J.; Codina Jané, C.; Gómez-Batiste, X.; McIntosh, J.; Espaulella Panicot, J. Optimizing drug therapy in patients with advanced dementia: A patient-centered approach. Eur. Geriatr. Med. 2014, 5, 66–71. [Google Scholar] [CrossRef]
- Molist-Brunet, N.; Sevilla-Sánchez, D.; Puigoriol-Juvanteny, E.; González-Bueno, J.; Solà- Bonada, N.; Cruz-Grullón, M.; Espaulella-Panicot, J. Optimizing drug therapy in frail patients with type 2 diabetes mellitus. Aging Clin. Exp. Res. 2020, 32, 1551–1559. [Google Scholar] [CrossRef] [PubMed]
- Molist-Brunet, N.; Sevilla-Sánchez, D.; González-Bueno, J.; Garcia-Sánchez, V.; Segura-Martín, L.A.; Codina-Jané, C.; Espaulella-Panicot, J. Therapeutic optimization through goal-oriented prescription in nursing homes. Int. J. Clin. Pharm. 2021, 43, 990–997. [Google Scholar] [CrossRef]
- Departament de Salut. Generalitat de Catalunya. Bases Conceptuals i Model d’atenció per a les Persones fràgils, amb Cronicitat Complexa o Avançada; Departament de Salut: Barcelona, Spain, 2020; Available online: https://salutweb.gencat.cat/web/.content/_ambits-actuacio/Linies-dactuacio/Estrategies-de-salut/Cronicitat/Documentacio-cronicitat/arxius/Model-de-Bases-de-Cronicitat.pdf (accessed on 14 August 2021).
- Fick, D.M.; Semla, T.P.; Steinman, M.; Beizer, J.; Brandt, N.; Dombrowski, R.; DuBeau, C.E.; Pezzullo, L.; Epplin, J.J.; Flanagan, N.; et al. American Geriatrics Society 2019 Updated AGS Beers Criteria® for Potentially Inappropriate Medication Use in Older Adults. J. Am. Geriatr. Soc. 2019, 67, 674–694. [Google Scholar]
- González-Bueno, J.; Calvo-Cidoncha, E.; Sevilla-Sánchez, D.; Espaulella-Panicot, J.; Codina-Jané, C.; Santos-Ramos, B. Spanish translation and cross-cultural adaptation of the ARMS-scale for measuring medication adherence in polypathological patients. Aten. Primaria 2017, 49, 459–464. [Google Scholar] [CrossRef] [PubMed]
- Kripalani, S.; Risser, J.; Gatti, M.E.; Jacobson, T.A. Development and Evaluation of the Adherence to Refills and Medications Scale (ARMS) among Low-Literacy Patients with Chronic Disease. Value Health 2009, 12, 118–123. [Google Scholar] [CrossRef]
- Kuntz, J.L.; Safford, M.M.; Singh, J.A.; Phansalkar, S.; Slight, S.P.; Her, Q.L.; Lapointe, N.A.; Mathews, R.; O’Brien, E.; Brinkman, W.B.; et al. Patient-centered interventions to improve medication management and adherence: A qualitative review of research findings. Patient Educ. Couns. 2014, 97, 310–326. [Google Scholar] [CrossRef] [PubMed]
- Wimmer, B.C.; Cross, A.J.; Jokanovic, N.; Wiese, M.D.; George, J.; Johnell, K.; Diug, B.; Bell, J.S. Clinical Outcomes Associated with Medication Regimen Complexity in Older People: A Systematic Review. J. Am. Geriatr. Soc. 2017, 65, 747–753. [Google Scholar] [CrossRef]
- Pasina, L.; Brucato, A.L.; Falcone, C.; Cucchi, E.; Bresciani, A.; Sottocorno, M.; Taddei, G.C.; Casati, M.; Franchi, C.; Djade, C.D.; et al. Medication non-adherence among elderly patients newly discharged and receiving polypharmacy. Drugs Aging 2014, 31, 283–289. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Jover, V.; Mira, J.; Carratala-Munuera, C.; Gil-Guillen, V.; Basora, J.; López-Pineda, A.; Orozco-Beltrán, D. Inappropriate Use of Medication by Elderly, Polymedicated, or Multipathological Patients with Chronic Diseases. Int. J. Environ. Res. Public Health 2018, 15, 310. [Google Scholar] [CrossRef]
- Bonini, G.; Pasina, L.; Cortesi, L.; Cesari, M.; Bergamaschini, L. Inappropriate prescribing in intermediate care facilities. Aging Clin. Exp. Res. 2021, 33, 1085–1088. [Google Scholar] [CrossRef] [PubMed]
- Moriarty, F.; Cahir, C.; Bennett, K.; Hughes, C.M.; Kenny, R.A.; Fahey, T. Potentially inappropriate prescribing and its association with health outcomes in middle-Aged people: A prospective cohort study in Ireland. BMJ Open 2017, 7, e016562. [Google Scholar] [CrossRef]
- Wallace, E.; McDowell, R.; Bennett, K.; Fahey, T.; Smith, S.M. Impact of Potentially Inappropriate Prescribing on Adverse Drug Events, Health Related Quality of Life and Emergency Hospital Attendance in Older People Attending General Practice: A Prospective Cohort Study. J. Gerontol. A Biol. Sci. Med. Sci. 2017, 72, 271–277. [Google Scholar] [CrossRef]
- Tommelein, E.; Mehuys, E.; Petrovic, M.; Somers, A.; Colin, P.; Boussery, K. Potentially inappropriate prescribing in community-dwelling older people across Europe: A systematic literature review. Eur. J. Clin. Pharmacol. 2015, 71, 1415–1427. [Google Scholar] [CrossRef] [PubMed]
- Sevilla-Sanchez, D.; Molist-Brunet, N.; Amblàs-Novellas, J.; Roura-Poch, P.; Espaulella-Panicot, J.; Codina-Jané, C. Adverse drug events in patients with advanced chronic conditions who have a prognosis of limited life expectancy at hospital admission. Eur. J. Clin. Pharmacol. 2017, 73, 79–89. [Google Scholar] [CrossRef]
- Kvarnström, K.; Westerholm, A.; Airaksinen, M.; Liira, H. Factors Contributing to Medication Adherence in Patients with a Chronic Condition: A Scoping Review of Qualitative Research. Pharmaceutics 2021, 13, 1100. [Google Scholar] [CrossRef] [PubMed]
- Bosworth, H.B.; Fortmann, S.P.; Kuntz, J.; Zullig, L.L.; Mendys, P.; Safford, M.; Phansalkar, S.; Wang, T.; Rumptz, M.H. Recommendations for Providers on Person-Centered Approaches to Assess and Improve Medication Adherence. J. Gen. Intern. Med. 2017, 32, 93–100. [Google Scholar] [CrossRef]
- Kim, S.; Bennett, K.; Wallace, E.; Fahey, T.; Cahir, C. Measuring medication adherence in older community-dwelling patients with multimorbidity. Eur. J. Clin. Pharmacol. 2018, 74, 357–364. [Google Scholar] [CrossRef] [PubMed]
- Weir, D.L.; Lee, T.C.; McDonald, E.G.; Motulsky, A.; Abrahamowicz, M.; Morgan, S.; Buckeridge, D.; Tamblyn, R. Both New and Chronic Potentially Inappropriate Medications Continued at Hospital Discharge Are Associated with Increased Risk of Adverse Events. J. Am. Geriatr. Soc. 2020, 68, 1184–1192. [Google Scholar] [CrossRef]
- Moriarty, F.; Bennett, K.; Kenny, R.A.; Fahey, T.; Cahir, C. Comparing Potentially Inappropriate Prescribing Tools and Their Association with Patient Outcomes. J. Am. Geriatr. Soc. 2020, 68, 526–534. [Google Scholar] [CrossRef]
- Hess, L.M.; Raebel, M.A.; Conner, D.A.; Malone, D.C. Measurement of adherence in pharmacy administrative databases: A proposal for standard definitions and preferred measures. Ann. Pharmacother. 2006, 40, 1280–1288. [Google Scholar] [CrossRef]


{kind=link}
| Characteristic | Total N = 93 | Non-Adherent 1 N = 74 (79.6%) | Adherent 1 N = 19 (20.4%) | p Value 2 |
|---|---|---|---|---|
| Demographic and Clinical Factors | ||||
| Age in years (mean (SD)) | 83.0 (6.1) | 83.0 (6.2) | 83.1 (5.6) | 0.926 |
| Sex (n (%)) | ||||
| Male | 32 (34.4%) | 27 (84.4%) | 5 (15.6%) | 0.405 |
| Female | 61 (65.6%) | 47 (77.0%) | 14 (23.0%) | |
| Chronic conditions (mean (SD)) | 7.40 (1.8) | 7.57 (1.9) | 6.74 (1.7) | 0.079 |
| Frailty (Frail-VIG) (mean (SD)) | 0.28 (0.11) | 0.29 (0.11) | 0.27 (0.11) | 0.633 |
| Activities of daily living (Barthel index) (mean (SD)) | 80.4 (19.7) | 80.3 (20.0) | 80.8 (19.2) | 0.919 |
| Cognitive impairment | ||||
| Absence (MMSE > 24) (n (%)) | 53 (57.0%) | 43 (81.1%) | 10 (18.9%) | |
| Mild (MMSE 21–24) (n (%)) | 23 (24.7%) | 16 (69.6%) | 7 (30.4%) | 0.832 |
| Moderate (MMSE 10–20) (n (%)) | 17 (18.3%) | 15 (88.2%) | 2 (11.8%) | |
| Medication Factors | ||||
| Long-term medications (mean (SD)) | 8.81 (2.8) | 9.26 (2.8) | 7.05 (2.2) | 0.002 |
| Hyperpolypharmacy (≥10 medications) | 58 (62.4%) | 42 (72.4%) | 16 (27.6%) | |
| No (n (%)) | 35 (37.6%) | 32 (91.4%) | 3 (8.6%) | 0.028 |
| Yes (n (%)) | ||||
| Medication regimen complexity score (MRCI) (mean (SD)) | 24.8 (10.7) | 26.1 (10.7) | 19.7 (9.7) | 0.020 |
| Medication regimen complexity (categorized) | 0.022 | |||
| Low (MRCI < 20) (n (%)) | 36 (38.7%) | 23 (63.9%) | 13 (36.1%) | |
| Moderate-high (MRCI 20–39.5) (n (%)) | 46 (49.5%) | 42 (91.3%) | 4 (8.7%) | |
| Excessive (MRCI ≥ 40) (n (%)) | 11 (11.8%) | 9 (81.8%) | 2 (18.2%) | |
| Anticholinergic and sedative risk score (DBI) (mean (SD)) | 0.99 (0.81) | 1.03 (0.83) | 0.82 (0.72) | 0.311 |
| Number of potentially inappropriate prescriptions (mean (SD)) | 2.55 (1.5) | 2.69 (1.4) | 2.00 (1.7) | 0.074 |
| Moderate (≥2) PIP burden | ||||
| No (n (%)) | 25 (26.9%) | 17 (68.0%) | 8 (32.0%) | 0.093 |
| Yes (n (%)) | 68 (73.1%) | 57 (83.8%) | 11 (16.2%) | |
| High (≥3) PIP burden | ||||
| No (n (%)) | 56 (60.2%) | 40 (71.4%) | 16 (28.6%) | 0.017 |
| Yes (n (%)) | 37 (39.8%) | 34 (91.9%) | 3 (8.1%) | |
| Self-reported adherence (ARMS-e total score) (mean (SD)) | 16.8 (4.1) | 17.6 (4.1) | 13.9 (2.9) | 0.001 |
| Self-reported adherence (categorized) | <0.001 | |||
| Optimal (ARMS-e = 12) (n (%)) | 23 (24.7%) | 11 (47.8%) | 12 (52.2%) | |
| Suboptimal (ARMS-e > 12) (n (%)) | 70 (75.3%) | 63 (90.0%) | 7 (10.0%) | |
| Patient autonomy for medication administration at home | ||||
| Independent (n (%)) | 46 (49.5%) | 36 (78.3%) | 10 (21.7%) | 0.564 |
| Partially assisted (n (%)) | 32 (34.4%) | 25 (78.1%) | 7 (21.9%) | |
| Totally assisted (n (%)) | 15 (16.1%) | 13 (86.7%) | 2 (13.3%) | |
| Patient autonomy for medication refill at home | ||||
| Independent (n (%)) | 35 (37.6%) | 26 (74.3%) | 9 (25.7%) | 0.093 |
| Partially assisted (n (%)) | 13 (14.0%) | 8 (61.5%) | 5 (38.5%) | |
| Totally assisted (n (%)) | 45 (48.4%) | 40 (88.9%) | 5 (11.1%) | |
| Characteristic | Non-Adherence 1 (Bivariate Analysis 2) | Non-Adherence 1 (Multivariate Analysis 2) | ||||
|---|---|---|---|---|---|---|
| OR | 95% CI | p Value | OR | 95% CI | p Value | |
| Chronic conditions | 1.30 | 0.97–1.74 | 0.083 | - | - | - |
| Long-term medications | 1.46 | 1.13–1.89 | 0.004 | - | - | - |
| Hyperpolypharmacy (≥10 medications) | ||||||
| No | 1.00 | Ref | Ref | - | - | - |
| Yes | 4.06 | 1.09–15.15 | 0.037 | |||
| Medication regimen complexity score (MRCI) | 1.07 | 1.01–1.14 | 0.025 | - | - | - |
| Medication regimen complexity (categorized) | ||||||
| Low (MRCI < 20) | 1.00 | Ref | Ref | |||
| Moderate-high (MRCI 20–39.5) | 5.94 | 1.73–20.32 | 0.005 | - | - | - |
| Excessive (MRCI ≥ 40) | 2.54 | 0.48–13.60 | 0.275 | |||
| Number of potentially inappropriate prescriptions | 1.47 | 0.96–2.24 | 0.079 | - | - | - |
| Moderate (≥2) PIP burden | ||||||
| No | 1.00 | Ref | Ref | - | - | - |
| Yes | 2.44 | 0.85–7.04 | 0.099 | |||
| High (≥3) PIP burden | ||||||
| No | 1.00 | Ref | Ref | 1.00 | Ref | Ref |
| Yes | 4.53 | 1.22–16.89 | 0.024 | 3.90 | 0.95–15.99 | 0.059 |
| Self-reported adherence (ARMS-e total score) | 1.38 | 1.13–1.67 | 0.001 | - | - | - |
| Self-reported adherence (categorized) | ||||||
| Optimal (ARMS-e = 12) | 1.00 | Ref | Ref | 1.00 | Ref | Ref |
| Suboptimal (ARMS-e > 12) | 9.82 | 3.17–30.42 | <0.001 | 8.99 | 2.80–28.84 | <0.001 |
| Patient autonomy for medication refill at home | ||||||
| Independent | 1.00 | Ref | Ref | |||
| Partially assisted | 2.77 | 0.83–9.19 | 0.096 | - | - | - |
| Totally assisted | 0.55 | 0.14–2.14 | 0.391 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
González-Bueno, J.; Sevilla-Sánchez, D.; Puigoriol-Juvanteny, E.; Molist-Brunet, N.; Codina-Jané, C.; Espaulella-Panicot, J. Factors Associated with Medication Non-Adherence among Patients with Multimorbidity and Polypharmacy Admitted to an Intermediate Care Center. Int. J. Environ. Res. Public Health 2021, 18, 9606. https://doi.org/10.3390/ijerph18189606
González-Bueno J, Sevilla-Sánchez D, Puigoriol-Juvanteny E, Molist-Brunet N, Codina-Jané C, Espaulella-Panicot J. Factors Associated with Medication Non-Adherence among Patients with Multimorbidity and Polypharmacy Admitted to an Intermediate Care Center. International Journal of Environmental Research and Public Health. 2021; 18(18):9606. https://doi.org/10.3390/ijerph18189606
Chicago/Turabian StyleGonzález-Bueno, Javier, Daniel Sevilla-Sánchez, Emma Puigoriol-Juvanteny, Núria Molist-Brunet, Carles Codina-Jané, and Joan Espaulella-Panicot. 2021. "Factors Associated with Medication Non-Adherence among Patients with Multimorbidity and Polypharmacy Admitted to an Intermediate Care Center" International Journal of Environmental Research and Public Health 18, no. 18: 9606. https://doi.org/10.3390/ijerph18189606
APA StyleGonzález-Bueno, J., Sevilla-Sánchez, D., Puigoriol-Juvanteny, E., Molist-Brunet, N., Codina-Jané, C., & Espaulella-Panicot, J. (2021). Factors Associated with Medication Non-Adherence among Patients with Multimorbidity and Polypharmacy Admitted to an Intermediate Care Center. International Journal of Environmental Research and Public Health, 18(18), 9606. https://doi.org/10.3390/ijerph18189606