
Diurnal Temperature Ranges in Relation to Lower Limb Amputation Rate of Diabetic Foot in South Korea: A Population Based Nationwide Study

 , , ,
, , ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Diurnal Temperature Range (DTR) of Each Region
2.3. Definition of Diabetic Foot Amputation/Ulcer
2.4. Study Area
2.5. Statistical Analyses
3. Results
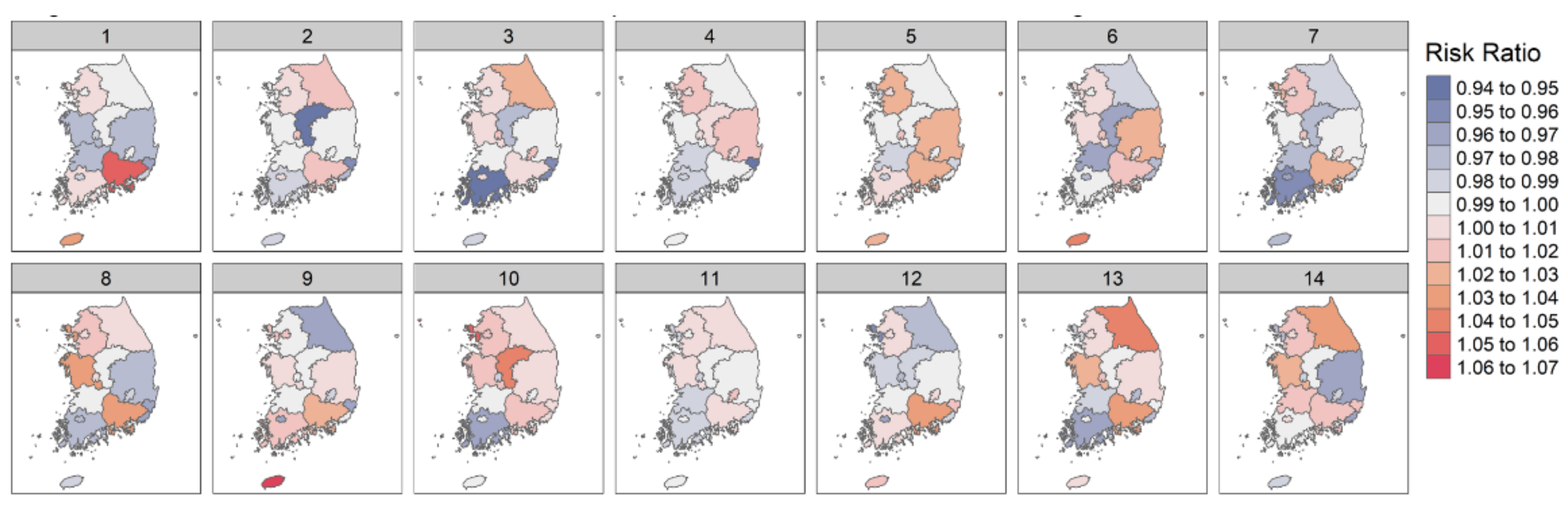
3.1. Association between DTR and Amputation of Diabetic Foot in Each Region
3.2. Association between DTR and Amputation of Diabetic Foot in Sub-Region According to Latitude
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Keatinge, W.R.; Coleshaw, S.R.; Cotter, F.; Mattock, M.; Murphy, M.; Chelliah, R. Increases in platelet and red cell counts, blood viscosity, and arterial pressure during mild surface cooling: Factors in mortality from coronary and cerebral thrombosis in winter. BMJ 1984, 289, 1405–1408. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chun, D.-I.; Kim, S.; Kim, J.; Yang, H.-J.; Kim, J.H.; Cho, J.-H.; Yi, Y.; Kim, W.J.; Won, S.H. Epidemiology and Burden of Diabetic Foot Ulcer and Peripheral Arterial Disease in Korea. J. Clin. Med. 2019, 8, 748. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yavuz, M.; Ersen, A.; Hartos, J.; Lavery, L.A.; Wukich, D.K.; Hirschman, G.B.; Armstrong, D.G.; Quiben, M.U.; Adams, L.S. Temperature as a Causative Factor in Diabetic Foot Ulcers: A Call to Revisit Ulceration Pathomechanics. J. Am. Podiatr. Med. Assoc. 2019, 109, 345–350. [Google Scholar] [CrossRef] [PubMed]
- Lavery, L.A.; Higgins, K.R.; Lanctot, D.R.; Constantinides, G.P.; Zamorano, R.G.; Athanasiou, K.A.; Armstrong, D.G.; Agrawal, C.M. Preventing Diabetic Foot Ulcer Recurrence in High-Risk Patients: Use of temperature monitoring as a self-assessment tool. Diabetes Care 2007, 30, 14–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Won, S.H.; Chun, D.-I.; Cho, J.; Park, I.K.; Yi, Y. Relationship between the Diurnal Temperature Range and Wound Healing of Diabetic Foot: Animal Study. J. Korean Foot Ankle Soc. 2020, 24, 142–147. [Google Scholar] [CrossRef]
- Liang, W.-M.; Liu, W.-P.; Kuo, H.-W. Diurnal temperature range and emergency room admissions for chronic obstructive pulmonary disease in Taiwan. Int. J. Biometeorol. 2009, 53, 17–23. [Google Scholar] [CrossRef] [PubMed]
- Ying, B.W.; Song, X.B.; Fan, H.; Wang, L.L.; Li, Y.S.; Cheng, Z.; Cheng, H.; Wen, F.Q. Plasma Ghrelin Levels and Weight Loss in Chinese Uygur Patients with Chronic Obstructive Pulmonary Disease. J. Int. Med. Res. 2008, 36, 1371–1377. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, G.; Zhang, Y.; Song, G.; Jiang, L.; Zhao, N.; Chen, B.; Kan, H. Is diurnal temperature range a risk factor for acute stroke death? Int. J. Cardiol. 2007, 116, 408–409. [Google Scholar] [CrossRef] [PubMed]
- Lichtman, J.H.; Leifheit-Limson, E.C.; Jones, S.B.; Wang, Y.; Goldstein, L.B. Average Temperature, Diurnal Temperature Variation, and Stroke Hospitalizations. J. Stroke Cerebrovasc. Dis. 2016, 25, 1489–1494. [Google Scholar] [CrossRef] [PubMed]
- Lim, Y.-H.; Hong, Y.-C.; Kim, H. Effects of diurnal temperature range on cardiovascular and respiratory hospital admissions in Korea. Sci. Total Environ. 2012, 417–418, 55–60. [Google Scholar] [CrossRef] [PubMed]
- Tian, Y.; Liu, H.; Si, Y.; Cao, Y.; Song, J.; Li, M.; Wu, Y.; Wang, X.; Xiang, X.; Juan, J.; et al. Association between temperature variability and daily hospital admissions for cause-specific cardiovascular disease in urban China: A national time-series study. PLoS Med. 2019, 16, e1002738. [Google Scholar] [CrossRef] [PubMed]
- Ge, W.Z.; Xu, F.; Zhao, Z.H.; Zhao, J.Z.; Kan, H.D. Association between diurnal temperature range and respiratory tract infections. Biomed. Environ. Sci. 2013, 26, 222–225. [Google Scholar] [CrossRef] [PubMed]
- Park, J.E.; Son, W.S.; Ryu, Y.; Choi, S.B.; Kwon, O.; Ahn, I. Effects of temperature, humidity, and diurnal temperature range on influenza incidence in a temperate region. Influenza Other Respir. Viruses 2020, 14, 11–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zheng, S.; Zhu, W.; Wang, M.; Shi, Q.; Luo, Y.; Miao, Q.; Nie, Y.; Kang, F.; Mi, X.; Bai, Y. The effect of diurnal temperature range on blood pressure among 46,609 people in Northwestern China. Sci. Total Environ. 2020, 730, 138987. [Google Scholar] [CrossRef] [PubMed]
- Guo, S.; DiPietro, L.A. Factors Affecting Wound Healing. J. Dent. Res. 2010, 89, 219–229. [Google Scholar] [CrossRef]
- Lee, W.-H.; Lim, Y.-H.; Dang, T.N.; Seposo, X.; Honda, Y.; Guo, Y.-L.L.; Jang, H.-M.; Kim, H. An Investigation on Attributes of Ambient Temperature and Diurnal Temperature Range on Mortality in Five East-Asian Countries. Sci. Rep. 2017, 7, 10207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Whitaker, H.J.; Steer, C.D.; Farrington, C.P. Self-controlled case series studies: Just how rare does a rare non-recurrent outcome need to be? Biom. J. 2018, 60, 1110–1120. [Google Scholar] [CrossRef] [Green Version]
- Farrington, P.; Whitaker, H.; Weldeselassie, Y.G. Self-Controlled Case Series Studies: A Modelling Guide with R.; CRC Press: Boca Raton, FL, USA, 2018. [Google Scholar]
- Tennekes, M. tmap: Thematic Maps in R. J. Stat. Softw. 2018, 84, 1–39. [Google Scholar] [CrossRef] [Green Version]
- Leung, H.B.; Ho, Y.C.; Wong, W.C.; Guerin, J. Seasonal variations in non-traumatic major lower limb amputation in Hong Kong Chinese diabetic patients. Hong Kong Med. J. 2007, 13, 379. [Google Scholar]
- Jehan, S. Seasonal Variations and Hospitalization Due to Diabetic Foot Complications. J. Rawalpindi Med. Coll. 2013, 17, 201–203. [Google Scholar]



{kind=link}
{kind=link}
{kind=link}
| Region | Risk Ratio (95% Confidence Interval) along Lag Day (Range: 1–14) (1) | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | |
| Seoul | 0.997 (0.983–1.011) | 1.000 (0.986–1.014) | 0.993 (0.979–1.007) | 1.001 (0.987–1.015) | 1.002 (0.988–1.016) | 1.000 (0.986–1.014) | 1.007 (0.993–1.021) | 1.008 (0.994–1.022) | 1.013 (0.999–1.027) | 1.015 (1.001–1.029) * | 0.996 (0.982–1.01) | 1.001 (0.987–1.015) | 1.005 (0.991–1.019) | 1.010 (0.995–1.023) |
| Incheon | 1.003 (0.959–1.049) | 0.999 (0.955–1.045) | 1.000 (0.956–1.046) | 1.003 (0.959–1.049) | 0.988 (0.945–1.034) | 1.010 (0.966–1.057) | 1.024 (0.978–1.07) | 1.034 (0.989–1.082) | 1.017 (0.972–1.064) | 1.052 (1.006–1.101) * | 0.982 (0.939–1.027) | 0.959 (0.917–1.003) | 0.990 (0.946–1.036) | 0.977 (0.933–1.021) |
| Gyeong-gi | 1.006 (0.99–1.022) | 1.007 (0.991–1.023) | 1.007 (0.991–1.023) | 1.017 (1.001–1.033) * | 1.021 (1.004–1.036) ** | 1.010 (0.994–1.026) | 1.017 (1.001–1.033) * | 1.012 (0.996–1.028) | 0.999 (0.983–1.015) | 1.018 (1.002–1.034) * | 1.004 (0.988–1.02) | 1.003 (0.987–1.019) | 1.003 (0.987–1.019) | 1.017 (1.001–1.033) * |
| Busan | 0.988 (0.961–1.016) | 0.980 (0.954–1.007) | 0.954 (0.928–0.981) *** | 0.994 (0.967–1.022) | 0.999 (0.972–1.027) | 0.979 (0.953–1.006) | 0.985 (0.96–1.011) | 0.970 (0.943–0.996) * | 0.994 (0.967–1.022) | 1.005 (0.978–1.033) | 0.990 (0.963–1.018) | 0.985 (0.958–1.013) | 0.971 (0.944–0.997) * | 0.969 (0.944–0.994) * |
| Daegu | 0.998 (0.975–1.022) | 0.998 (0.975–1.022) | 1.013 (0.99–1.037) | 1.006 (0.983–1.03) | 0.998 (0.975–1.022) | 1.005 (0.982–1.029) | 1.005 (0.982–1.029) | 0.988 (0.965–1.012) | 0.982 (0.959–1.006) | 0.998 (0.975–1.022) | 1.012 (0.989–1.036) | 1.007 (0.984–1.031) | 0.978 (0.955–1.001) | 0.987 (0.964–1.011) |
| Daejeon | 0.986 (0.955–1.016) | 1.016 (0.985–1.048) | 1.016 (0.985–1.048) | 1.007 (0.976–1.039) | 1.013 (0.982–1.045) | 1.018 (0.987–1.051) | 1.020 (0.988–1.052) | 1.007 (0.976–1.039) | 0.998 (0.967–1.03) | 0.989 (0.959–1.021) | 0.981 (0.95–1.011) | 0.979 (0.949–1.01) | 1.015 (0.983–1.046) | 0.986 (0.956–1.018) |
| Gwangju | 0.986 (0.954–1.02) | 1.005 (0.974–1.037) | 1.001 (0.97–1.033) | 0.985 (0.954–1.015) | 0.990 (0.959–1.022) | 0.973 (0.941–1.006) | 0.962 (0.93–0.994) * | 0.98 (0.948–1.013) | 0.962 (0.93–0.994) * | 0.997 (0.966–1.029) | 0.993 (0.962–1.025) | 0.965 (0.934–0.998) * | 0.998 (0.967–1.03) | 1.009 (0.978–1.041) |
| Ulsan | 0.967 (0.919–1.017) | 0.960 (0.913–1.011) | 0.953 (0.905–1.002) | 0.948 (0.900–0.997) * | 0.983 (0.936–1.033) | 0.978 (0.931–1.026) | 0.996 (0.948–1.046) | 0.967 (0.919–1.017) | 0.962 (0.914–1.012) | 1.009 (0.961–1.06) | 0.994 (0.945–1.046) | 1.016 (0.968–1.067) | 0.996 (0.948–1.046) | 1.018 (0.969–1.069) |
| Kyeonsannam-do | 1.056 (1.026–1.088) *** | 1.017 (0.988–1.047) | 1.007 (0.978–1.037) | 1.000 (0.969–1.032) | 1.024 (0.992–1.056) | 1.014 (0.982–1.045) | 1.025 (0.996–1.056) | 1.035 (1.005–1.065) * | 1.028 (0.998–1.058) | 1.015 (0.986–1.045) | 1.005 (0.974–1.037) | 1.035 (1.003–1.068) * | 1.035 (1.004–1.069) * | 1.020 (0.991–1.051) |
| Kyeonsanbuk-do | 0.976 (0.937–1.017) | 0.997 (0.957–1.039) | 0.993 (0.953–1.035) | 1.019 (0.978–1.062) | 1.026 (0.985–1.069) | 1.03 (0.989–1.074) | 0.999 (0.959–1.041) | 0.976 (0.937–1.017) | 1.002 (0.962–1.044) | 1.01 (0.969–1.052) | 0.992 (0.952–1.034) | 0.992 (0.952–1.034) | 1.008 (0.967–1.05) | 0.967 (0.928–1.007) |
| Jeollanam-do | 1.008 (0.958–1.061) | 0.989 (0.94–1.041) | 0.945 (0.896–0.996) | 0.984 (0.935–1.036) | 1.006 (0.956–1.059) | 1.000 (0.95–1.052) | 0.958 (0.91–1.008) | 0.98 (0.931–1.031) | 1.013 (0.965–1.064) | 0.965 (0.918–1.016) | 0.990 (0.941–1.042) | 1.003 (0.953–1.055) | 0.967 (0.919–1.017) | 0.991 (0.942–1.043) |
| Jeollabuk-do | 0.971 (0.939–1.003) | 0.994 (0.963–1.026) | 0.993 (0.962–1.025) | 0.985 (0.954–1.015) | 0.981 (0.949–1.014) | 0.962 (0.930–0.994) * | 0.971 (0.939–1.003) | 0.999 (0.966–1.033) | 0.994 (0.963–1.026) | 0.995 (0.964–1.027) | 0.987 (0.957–1.019) | 0.994 (0.963–1.026) | 0.988 (0.956–1.022) | 1.012 (0.981–1.044) |
| Chungcheongnam-do | 0.978 (0.935–1.023) | 0.995 (0.951–1.041) | 1.001 (0.957–1.047) | 0.994 (0.95–1.04) | 0.996 (0.952–1.042) | 1.004 (0.96–1.05) | 0.993 (0.949–1.039) | 1.034 (0.99–1.079) | 1.006 (0.964–1.05) | 1.014 (0.971–1.059) | 1.005 (0.961–1.051) | 0.99 (0.946–1.036) | 1.023 (0.978–1.07) | 1.021 (0.978–1.066) |
| Chungcheongbuk-do | 0.991 (0.953–1.031) | 0.945 (0.907–0.984) ** | 0.974 (0.936–1.012) | 1.004 (0.965–1.044) | 0.999 (0.959–1.041) | 0.962 (0.923–1.002) | 0.977 (0.94–1.016) | 0.995 (0.957–1.035) | 0.992 (0.954–1.032) | 1.042 (1.002–1.084) * | 0.993 (0.954–1.032) | 0.989 (0.949–1.031) | 0.992 (0.952–1.034) | 0.991 (0.953–1.031) |
| Gangwon-do | 0.991 (0.947–1.037) | 1.014 (0.969–1.061) | 1.024 (0.979–1.072) | 1.000 (0.956–1.046) | 0.996 (0.952–1.042) | 0.987 (0.944–1.033) | 0.987 (0.944–1.033) | 1.005 (0.961–1.051) | 0.965 (0.923–1.01) | 1.002 (0.958–1.048) | 1.008 (0.964–1.055) | 0.979 (0.935–1.023) | 1.042 (0.996–1.09) | 1.039 (0.995–1.085) |
| Jeju-do | 1.037 (0.958–1.125) | 0.987 (0.907–1.074) | 0.982 (0.903–1.069) | 0.997 (0.917–1.081) | 1.021 (0.942–1.107) | 1.044 (0.961–1.134) | 0.975 (0.895–1.063) | 0.986 (0.905–1.075) | 1.062 (0.982–1.148) | 0.998 (0.919–1.084) | 0.996 (0.917–1.081) | 1.011 (0.933–1.096) | 1.001 (0.92–1.089) | 0.984 (0.903–1.073) |
| Risk Ratio (95% Confidence Interval) Along Lag Day (Range: 1–14) (1) | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | |
| Region 1 (2) | 1.000 (0.990–1.010) | 1.003 (0.993–1.013) | 1.000 (0.990–1.010) | 1.008 (0.998–1.018) | 1.009 (0.999–1.019) | 1.004 (0.994–1.014) | 1.011 (1.001–1.021) | 1.011 (1.001–1.021) | 1.005 (0.995–1.015) | 1.017 (1.007–1.027) | 0.999 (0.989–1.009) | 0.999 (0.989–1.009) | 1.005 (0.995–1.015) | 1.012 (1.002–1.022) |
| Risk Ratio (95% Confidence Interval) Along Lag Day (Range: 1–14) (1) | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | |
| Region 2 (2) | 1.003 (0.987–1.019) | 0.991 (0.976–1.007) | 0.976 (0.961–0.992) | 0.988 (0.973–1.004) | 1.001 (0.985–1.017) | 0.988 (0.973–1.004) | 0.99 (0.975–1.006) | 0.993 (0.978–1.009) | 1.003 (0.987–1.019) | 1.002 (0.986–1.018) | 0.994 (0.979–1.01) | 1.005 (0.989–1.021) | 0.993 (0.978–1.009) | 0.997 (0.981–1.013) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Won, S.H.; Chung, H.-J.; Lee, J.; Jeon, Y.J.; Chun, D.-I.; Min, T.-H.; Cho, J.; Won, S.; Yi, Y. Diurnal Temperature Ranges in Relation to Lower Limb Amputation Rate of Diabetic Foot in South Korea: A Population Based Nationwide Study. Int. J. Environ. Res. Public Health 2021, 18, 9191. https://doi.org/10.3390/ijerph18179191
Won SH, Chung H-J, Lee J, Jeon YJ, Chun D-I, Min T-H, Cho J, Won S, Yi Y. Diurnal Temperature Ranges in Relation to Lower Limb Amputation Rate of Diabetic Foot in South Korea: A Population Based Nationwide Study. International Journal of Environmental Research and Public Health. 2021; 18(17):9191. https://doi.org/10.3390/ijerph18179191
Chicago/Turabian StyleWon, Sung Hun, Hyung-Jin Chung, Jinyoung Lee, Ye Jin Jeon, Dong-Il Chun, Tae-Hong Min, Jaeho Cho, Sungho Won, and Young Yi. 2021. "Diurnal Temperature Ranges in Relation to Lower Limb Amputation Rate of Diabetic Foot in South Korea: A Population Based Nationwide Study" International Journal of Environmental Research and Public Health 18, no. 17: 9191. https://doi.org/10.3390/ijerph18179191
APA StyleWon, S. H., Chung, H.-J., Lee, J., Jeon, Y. J., Chun, D.-I., Min, T.-H., Cho, J., Won, S., & Yi, Y. (2021). Diurnal Temperature Ranges in Relation to Lower Limb Amputation Rate of Diabetic Foot in South Korea: A Population Based Nationwide Study. International Journal of Environmental Research and Public Health, 18(17), 9191. https://doi.org/10.3390/ijerph18179191