
The Effectiveness of Free Face Mask Distribution on Use of Face Masks. A Cluster Randomised Trial in Stovner District of Oslo, Norway

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Trial Registration
2.2. Setting
2.3. Intervention
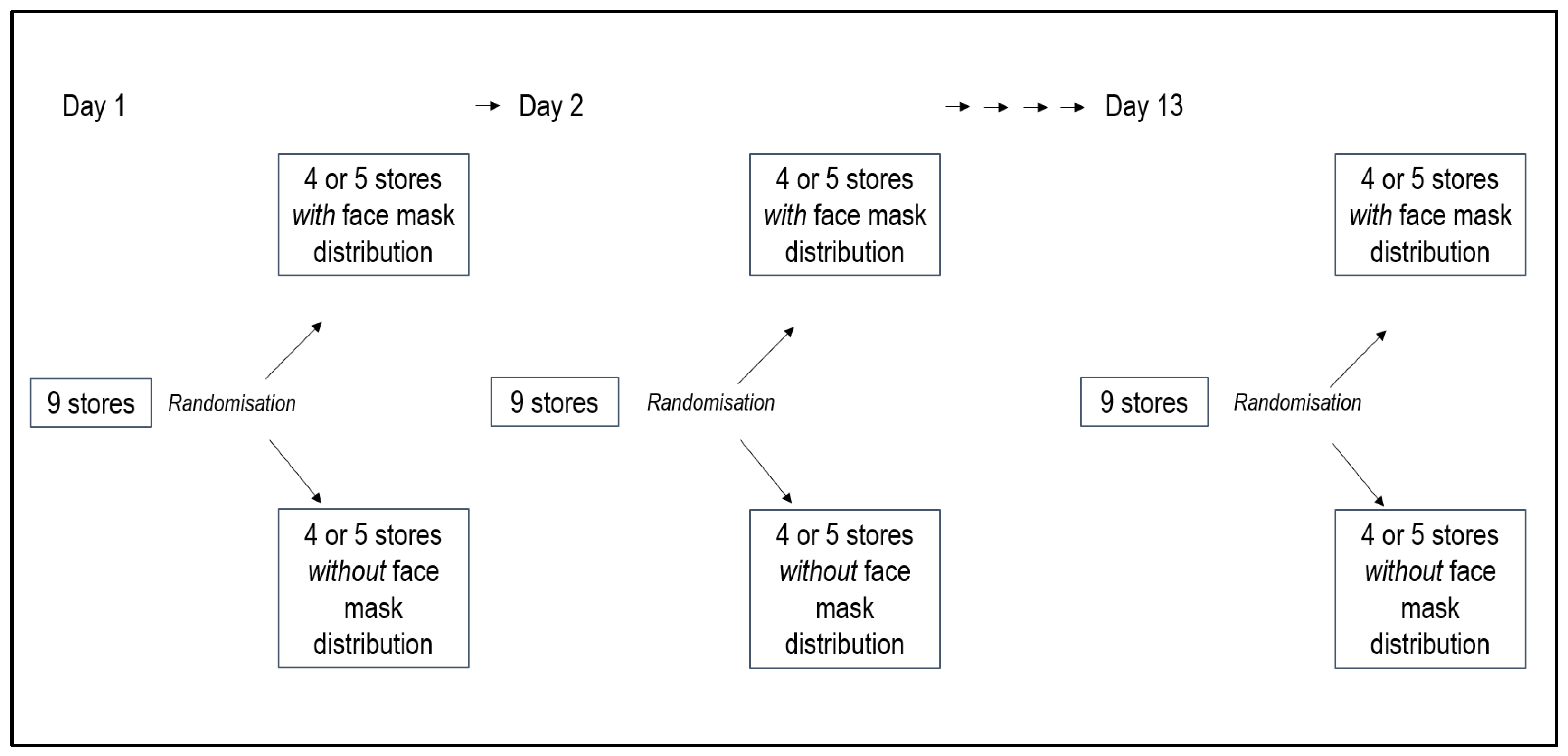
2.4. Randomisation Procedure
2.5. Analysis
2.6. Outcome Measurement
2.7. Sample Size Estimation
2.8. Ethics and Privacy Issues
3. Results
3.1. Descriptive Statistics
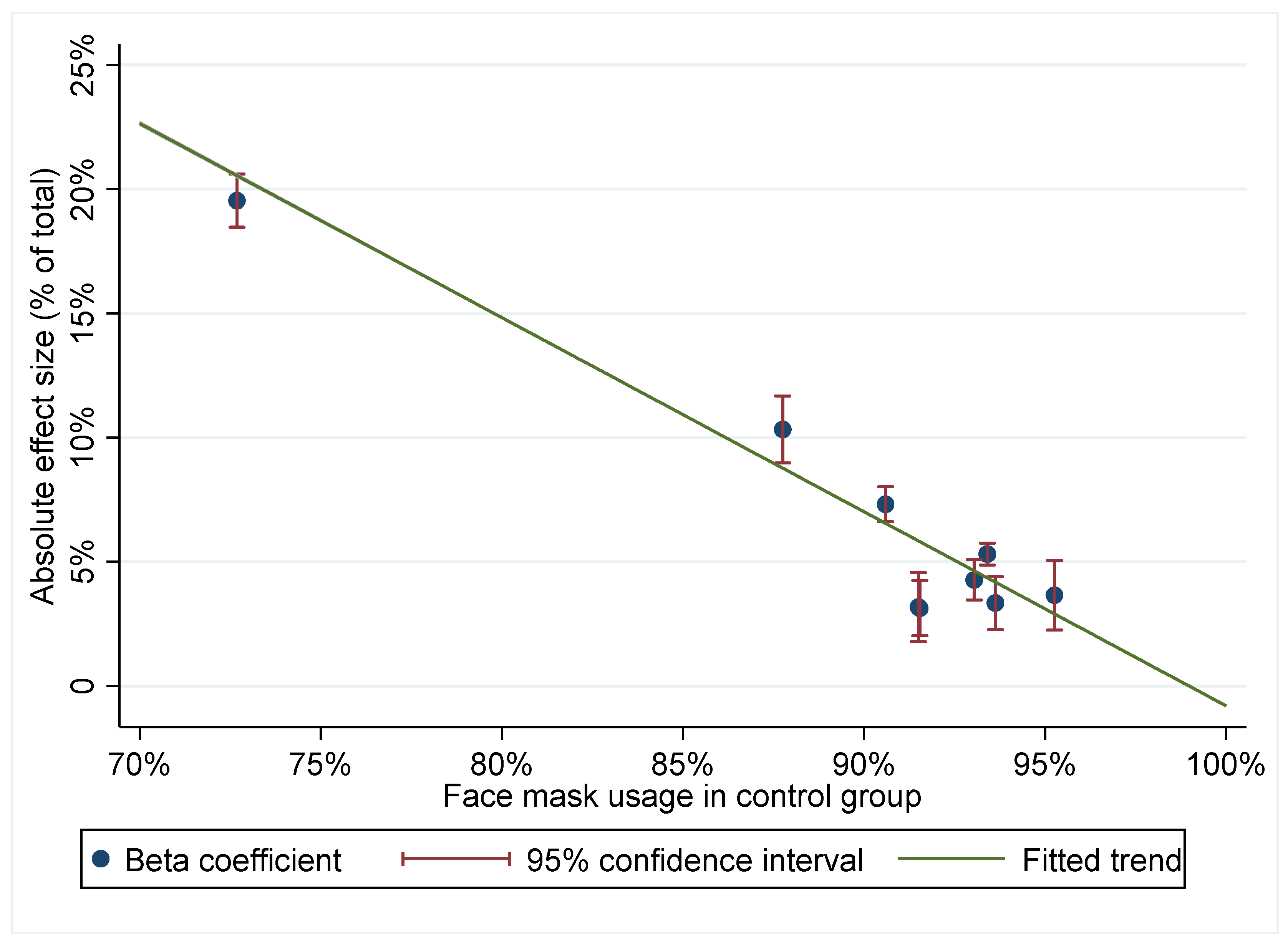
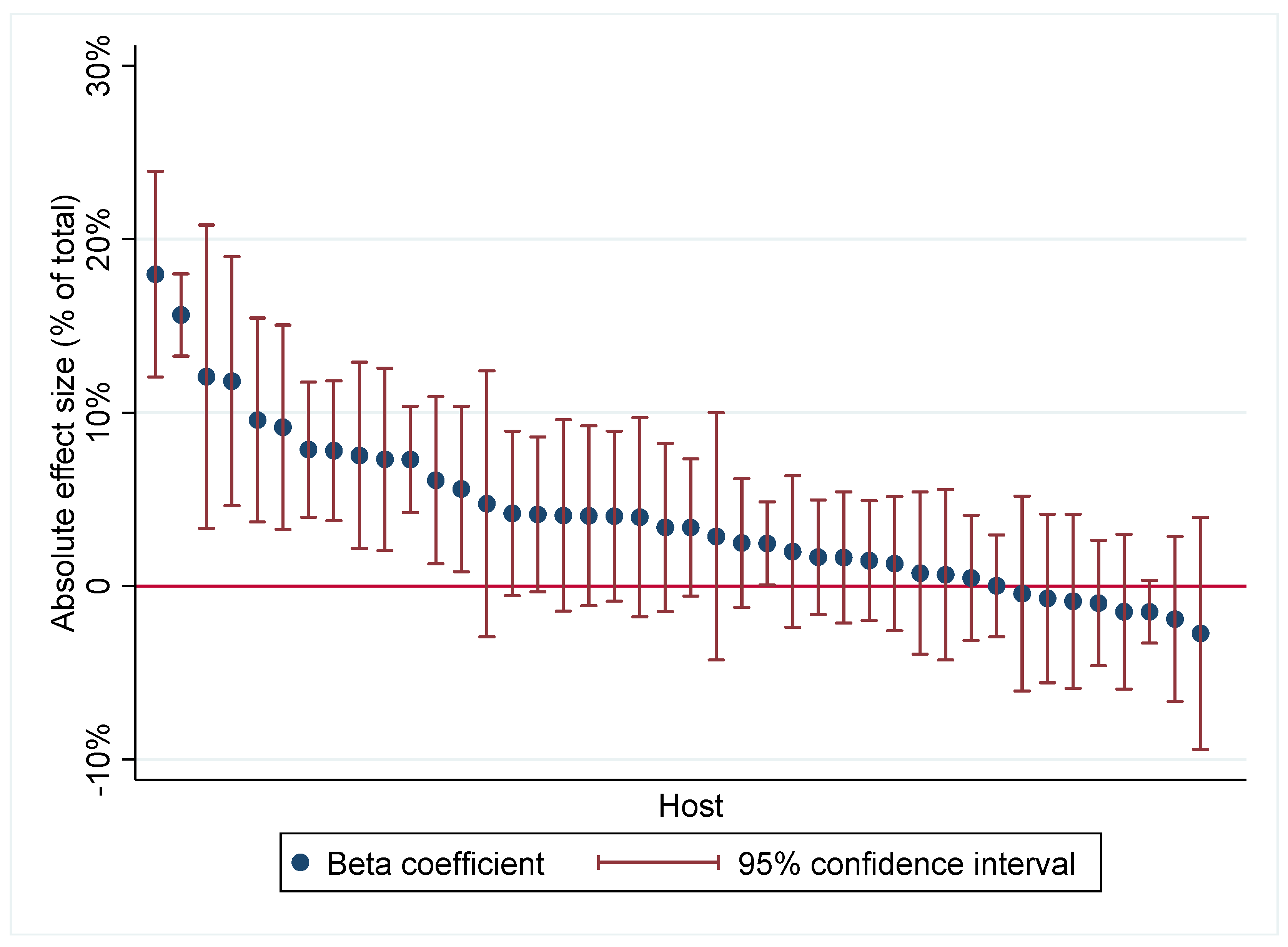
3.2. Main Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mask Use in the Context of COVID-19. Interim Guidance; World Health Organization: Geneva, Switzerland, 2020.
- Felter, C.B.N. Which Countries are Requiring Face Masks? Available online: https://www.cfr.org/in-brief/which-countries-are-requiring-face-masks (accessed on 16 April 2021).
- Vestrheim, D.F.; Iversen, B.G.; Flottorp, S.; Denison, E.; Oxman, A.D. COVID-19: Should Individuals in the Community without Respiratory Symptoms Wear Facemasks to Reduce the Spread of COVID-19?—Update 1; Norwegian Institute of Public Health: Oslo, Norway, 2020.
- Bundgaard, H.; Bundgaard, J.S.; Raaschou-Pedersen, D.E.T.; von Buchwald, C.; Todsen, T.; Norsk, J.B.; Pries-Heje, M.M.; Vissing, C.R.; Nielsen, P.B.; Winslow, U.C.; et al. Effectiveness of Adding a Mask Recommendation to Other Public Health Measures to Prevent SARS-CoV-2 Infection in Danish Mask Wearers: A Randomized Controlled Trial. Ann. Intern. Med. 2021, 174, 335–343. [Google Scholar] [CrossRef] [PubMed]
- Advice and Rules in the City of Oslo. Available online: https://www.oslo.kommune.no/english/coronavirus/advice-and-rules-in-the-city-of-oslo/ (accessed on 21 May 2021).
- Capraro, V.; Barcelo, H. Telling people to “rely on their reasoning” increases intentions to wear a face covering to slow down COVID-19 transmission. Appl. Cogn. Psychol. 2021, 35, 693–699. [Google Scholar] [CrossRef] [PubMed]
- Betsch, C.; Korn, L.; Sprengholz, P.; Felgendreff, L.; Eitze, S.; Schmid, P.; Bohm, R. Social and behavioral consequences of mask policies during the COVID-19 pandemic. Proc. Natl. Acad. Sci. USA 2020, 117, 21851–21853. [Google Scholar] [CrossRef] [PubMed]
- Abaluck, J.; Kwong, L.H.; Styczynski, A.; Haque, A.; Kabir, M.A.; Bates-Jefferys, E.; Crawford, E.; Benjamin-Chung, J.; Benhachmi, S.; Raihan, S.; et al. Normalizing Community Mask-Wearing: A Cluster Randomized Trial in Bangladesh; National Bureau of Economic Research: Cambridge, MA, USA, 2021. [Google Scholar]
- Helsinki Distributes Free Masks to People in Need. Available online: https://www.hel.fi/uutiset/en/kaupunginkanslia/helsinki-distributes-free-masks (accessed on 3 August 2021).
- Gita-Carlos, R.A. PRRD Orders LGUs to Distribute Free Face Masks. Available online: https://www.pna.gov.ph/articles/1131812 (accessed on 3 August 2021).
- Durkee, A. Biden Administration to Distribute More Than 25 Million Face Masks to Disadvantaged Groups. Available online: https://www.forbes.com/sites/alisondurkee/2021/02/24/report-biden-administration-to-send-face-masks-to-key-disadvantaged-populations (accessed on 3 August 2021).
- Madhavan, D. Traffic Inspector Distributes Free Face Masks to Commuters. Available online: https://www.thehindu.com/news/cities/chennai/traffic-inspector-distributes-free-face-masks-to-commuters/article34288757.ece (accessed on 3 August 2021).
- Jones, S. Austria Makes Masks Compulsory As Protection Debate Shifts. Available online: https://www.ft.com/content/f68f3063-5024-4654-9389-bcc7ee1efd8e (accessed on 3 August 2021).
- Wang, T.; Lurie, M.; Govindasamy, D.; Mathews, C. The Effects of School-Based Condom Availability Programs (CAPs) on Condom Acquisition, Use and Sexual Behavior: A Systematic Review. AIDS Behav. 2018, 22, 308–320. [Google Scholar] [CrossRef] [Green Version]
- Statusrapport COVID-19 Tirsdag 27. April 2021 [Status Report COVID-19 Tuesday 27. April 2021]; Oslo kommune: Oslo, Norway, 2021.
- Koronatall for Oslo [Corona numbers for Oslo]. Available online: https://www.oslo.kommune.no/koronavirus/koronatall-for-oslo/ (accessed on 22 May 2021).
- Hvinden, B.; Bang, K.; Fjørtoft, K.; Holand, I.; Johnsen, R.; Kolstad, I.; Monsen, T.; Nevøy, A.; Sandmo, E.; Skilbrei, M.-L.; et al. Guidelines for Research Ethics in the Social Sciences, Humanities, Law and Theology; The National Committee for Research Ethics in the Social Sciences and the Humanities (NESH): Oslo, Norway, 2019. [Google Scholar]
- Michie, S.; van Stralen, M.M.; West, R. The behaviour change wheel: A new method for characterising and designing behaviour change interventions. Implement. Sci. 2011, 6, 42. [Google Scholar] [CrossRef] [Green Version]
- Kellerer, J.D.; Rohringer, M.; Deufert, D. Behavior in the use of face masks in the context of COVID-19. Public Health Nurs. 2021. [Google Scholar] [CrossRef]
- Rahimi, Z.; Shirali, G.A.; Araban, M.; Mohammadi, M.J.; Cheraghian, B. Mask use among pedestrians during the COVID-19 pandemic in Southwest Iran: An observational study on 10,440 people. BMC Public Health 2021, 21, 133. [Google Scholar] [CrossRef] [PubMed]
- Tam, V.C.W.; Tam, S.Y.; Khaw, M.L.; Law, H.K.W.; Chan, C.P.L.; Lee, S.W.Y. Behavioural insights and attitudes on community masking during the initial spread of COVID-19 in Hong Kong. Hong Kong Med. J. 2021, 27, 106–112. [Google Scholar] [CrossRef] [PubMed]
- Semenza, J.C.; Adlhoch, C.; Baka, A.; Broberg, E.; Cenciarelli, O.; De Angelis, S.; Einoder-Moreno, M.; Dalmau, I.J.Q.; Kinross, P.; Kinsman, J.; et al. COVID-19 research priorities for non-pharmaceutical public health and social measures. Epidemiol. Infect. 2021, 149, e87. [Google Scholar] [CrossRef]
- McCartney, M. We need better evidence on non-drug interventions for COVID-19. BMJ 2020, 370, m3473. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total | Mask Distribution | No Mask Distribution | |
|---|---|---|---|
| Individual level | |||
| Mean (SD) mask usage, percentage | 94.4 (23.1) | 97.1 (16.6) | 91.7 (27.5) |
| Mean (SD) correct usage, percentage | 91.6 (27.8) | 95.0 (21.9) | 88.4 (32.0) |
| No. of observations | 21,524 | 11,126 | 10,398 |
| Cluster level, weighted | |||
| Mean (SD) mask usage, percentage | 94.4 (5.3) | 97.1 (2.1) | 91.7 (6.0) |
| Mean (SD) correct usage, percentage | 91.6 (6.7) | 95.0 (3.1) | 88.4 (7.5) |
| Mean (SD) No. of obs. | 252 (114) | 221 (99) | 281 (120) |
| No. of clusters | 117 | 61 | 56 |
| With Face Mask Distribution n/N (%) | Without Face Mask Distribution n/N (%) | Intra-Cluster Correlation Coefficient | Absolute Difference (95% Confidence Interval a) | Relative Difference (95% Confidence Interval a) | p-Value a | |
|---|---|---|---|---|---|---|
| Face mask use (correct and incorrect) | 10,102/10,398 (97.2%) | 10,207/11,126 (91.7%) | 0.048 | 0.060 (0.035–0.085) | 1.062 (1.036–1.088) | 0.001 |
| Correct use of face mask | 9873/10,398 (95.0%) | 9840/11,126 (88.4%) | 0.054 | 0.072 (0.046–0.099) | 1.075 (1.047–1.104) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fretheim, A.; Elgersma, I.H.; Kristiansen, F.A.; Varmbo, C.R.; Olsbø, M.K.S.; Glover, I.H.S.; Flatø, M. The Effectiveness of Free Face Mask Distribution on Use of Face Masks. A Cluster Randomised Trial in Stovner District of Oslo, Norway. Int. J. Environ. Res. Public Health 2021, 18, 8971. https://doi.org/10.3390/ijerph18178971
Fretheim A, Elgersma IH, Kristiansen FA, Varmbo CR, Olsbø MKS, Glover IHS, Flatø M. The Effectiveness of Free Face Mask Distribution on Use of Face Masks. A Cluster Randomised Trial in Stovner District of Oslo, Norway. International Journal of Environmental Research and Public Health. 2021; 18(17):8971. https://doi.org/10.3390/ijerph18178971
Chicago/Turabian StyleFretheim, Atle, Ingeborg Hess Elgersma, Fredrik Aaeng Kristiansen, Caroline Rømming Varmbo, Miriam Kristine Salame Olsbø, Iselin Havstein Strand Glover, and Martin Flatø. 2021. "The Effectiveness of Free Face Mask Distribution on Use of Face Masks. A Cluster Randomised Trial in Stovner District of Oslo, Norway" International Journal of Environmental Research and Public Health 18, no. 17: 8971. https://doi.org/10.3390/ijerph18178971
APA StyleFretheim, A., Elgersma, I. H., Kristiansen, F. A., Varmbo, C. R., Olsbø, M. K. S., Glover, I. H. S., & Flatø, M. (2021). The Effectiveness of Free Face Mask Distribution on Use of Face Masks. A Cluster Randomised Trial in Stovner District of Oslo, Norway. International Journal of Environmental Research and Public Health, 18(17), 8971. https://doi.org/10.3390/ijerph18178971