
Effective COVID-19 Control: A Comparative Analysis of the Stringency and Timeliness of Government Responses in Asia

 ,
,  , , , and
, , , and
Abstract
:1. Introduction
2. Methods
2.1. Country/Subregion Selection
2.2. Data
2.3. Indicators and Dimensions to Assess COVID-19 Responses
2.4. Development of the MSI and the IRI
2.5. Data Analysis
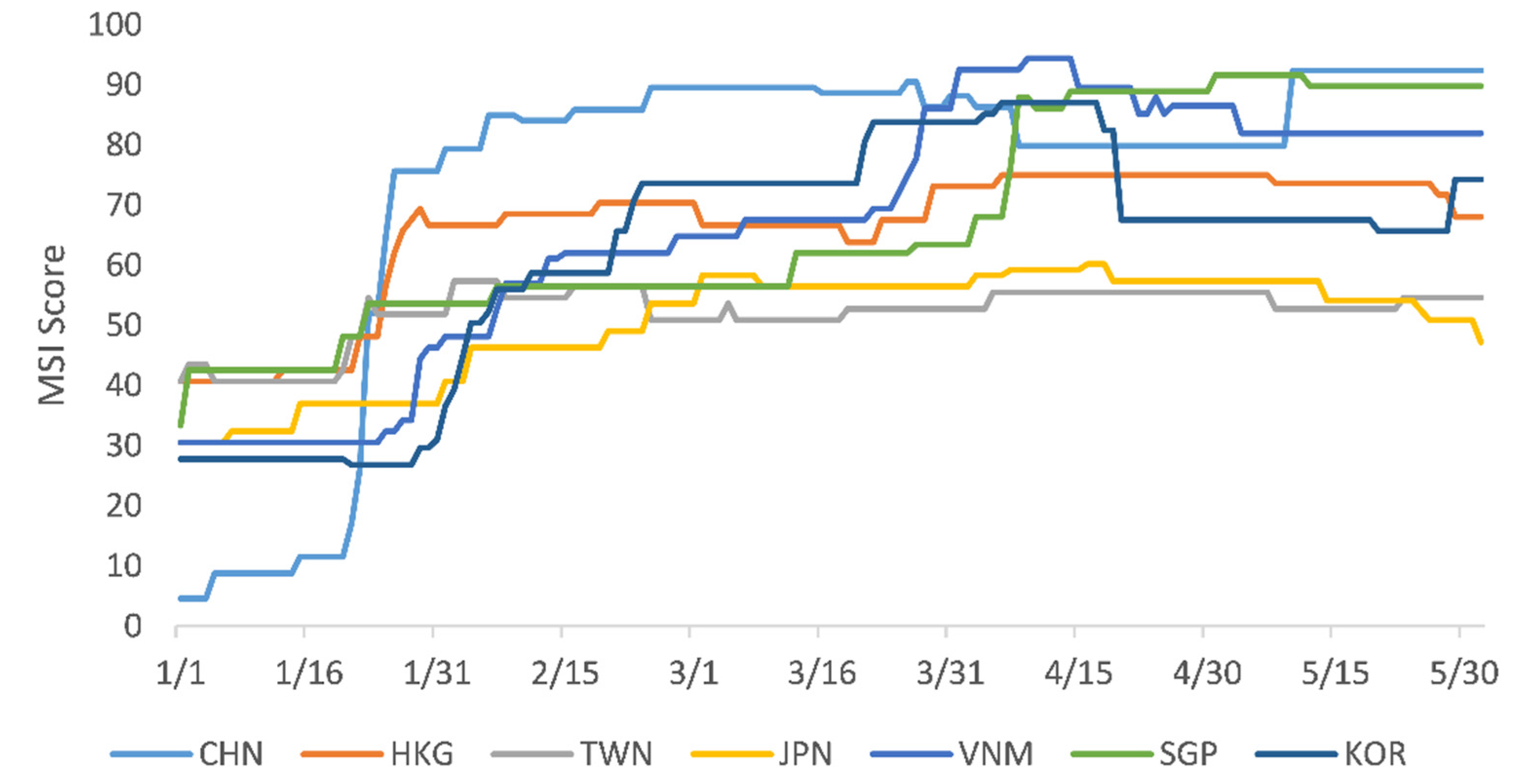
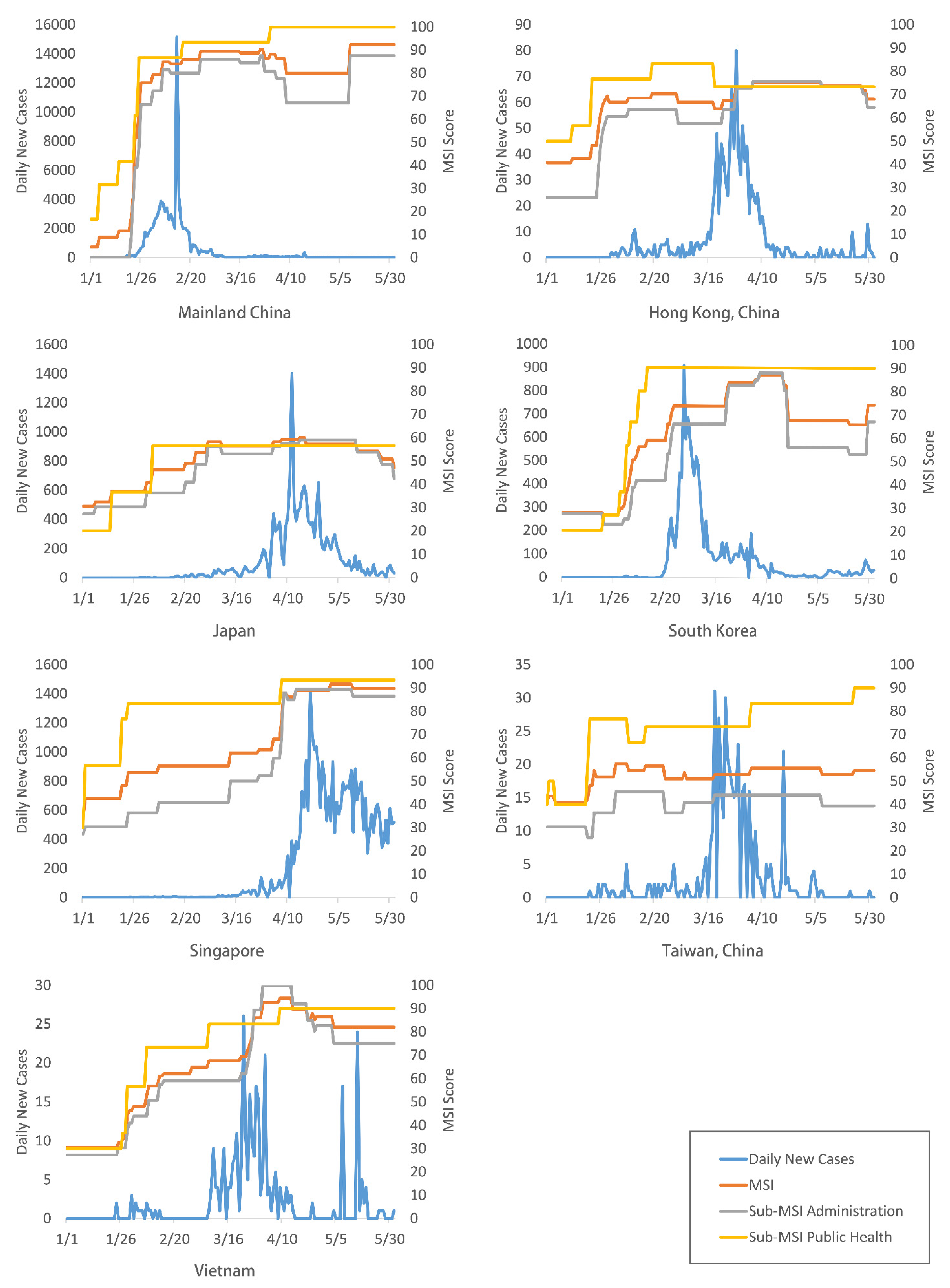
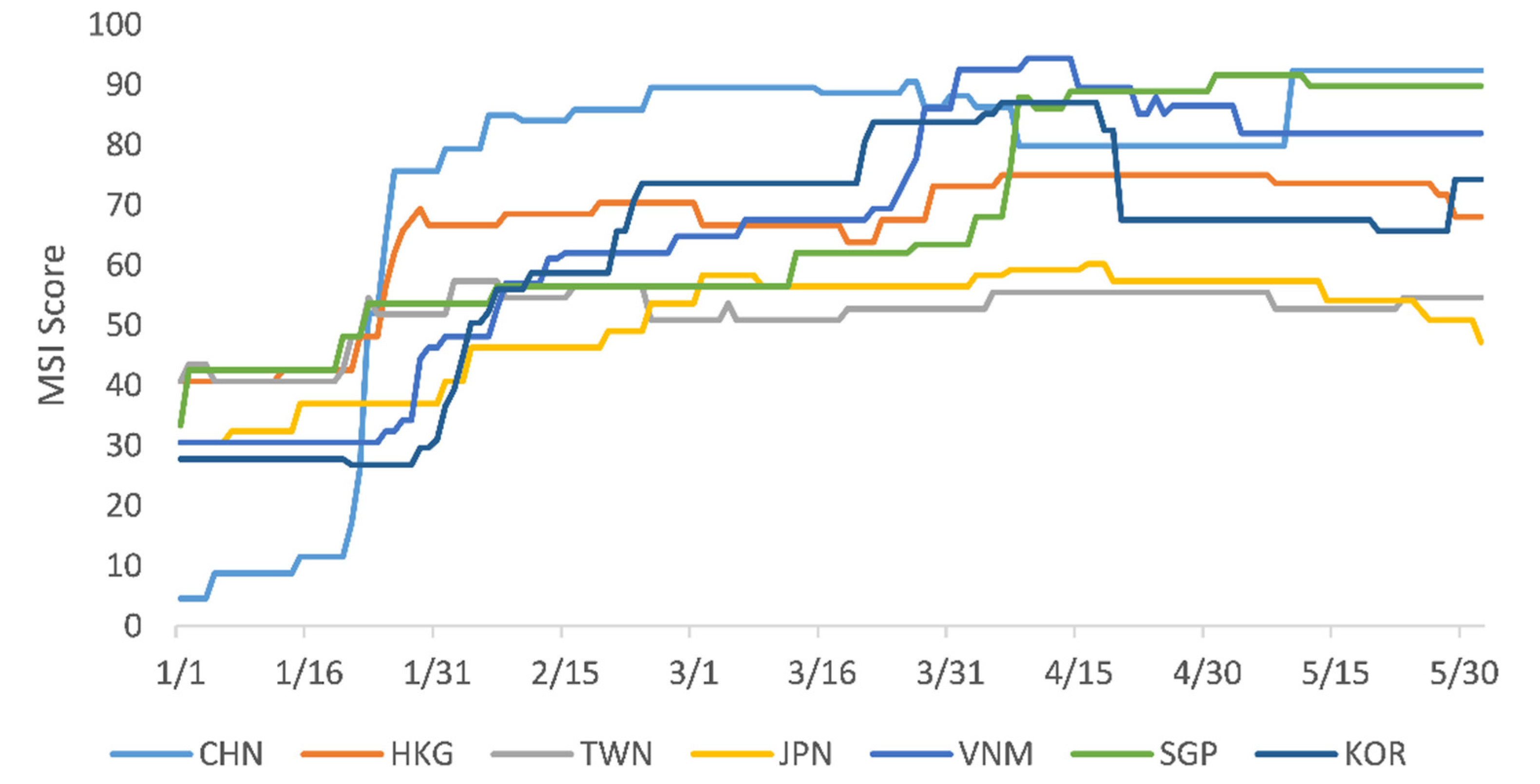
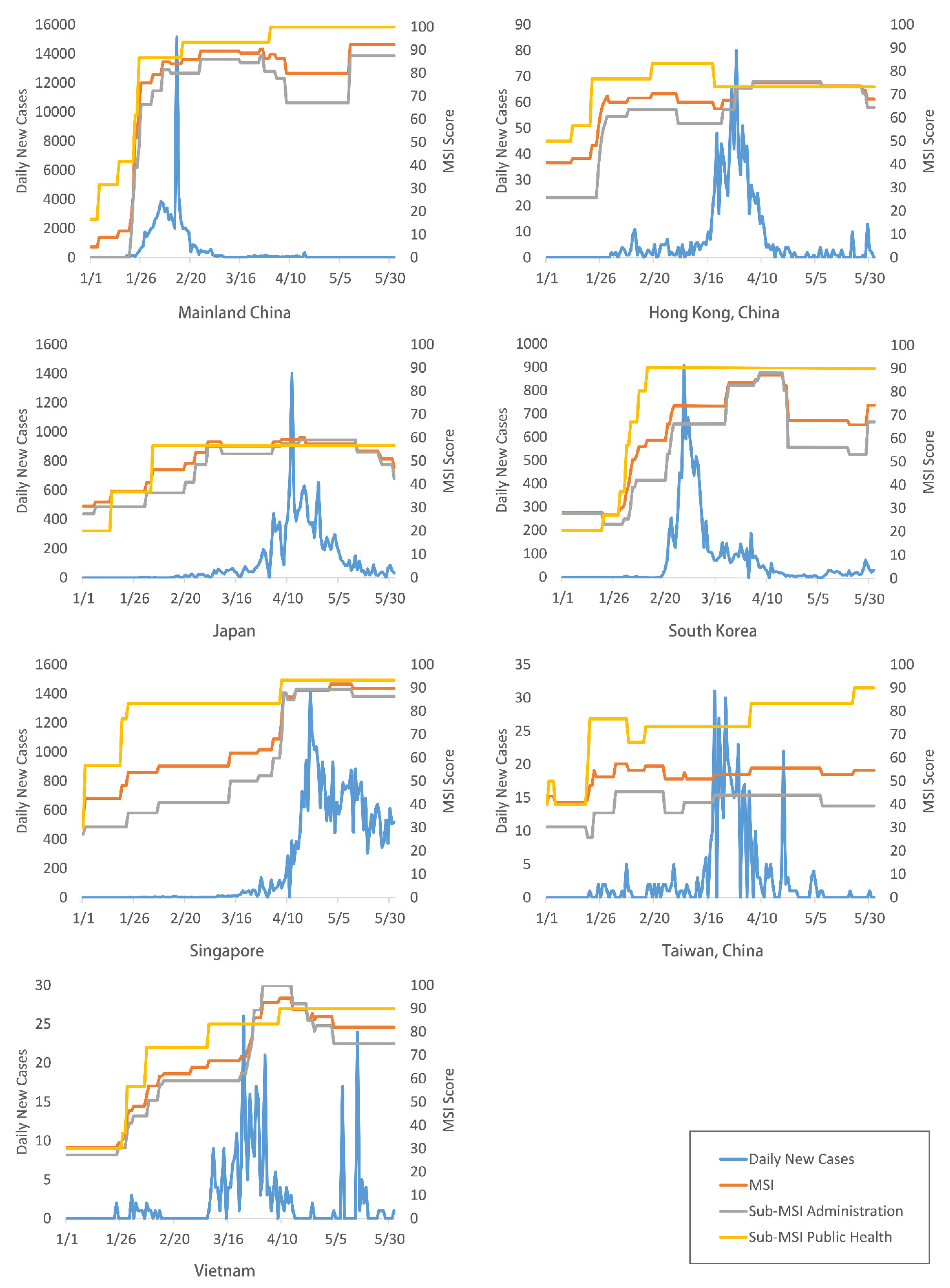
3. Results
Summary of the Government Response among the Study Sites
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| ID | Indicators Name | Meaurment | Coding Instructions |
|---|---|---|---|
| A1 | Coordinated governance | Ordinal | 0—No measures 1—Health sector coordination 2—Established multi-sector coordinated leading/governance team Blank—No data |
| A2 | Legislation and regulations | Binary | 0—No measures 1—Amended existing or developed new legisltions or regulations for COVID-19 Blank—No data |
| A3 | Border control | Ordinal | 0—No measures 1—Open to all countries with travelers * screening 2—Border closure with targeted countries 3—Border closure with all countries Blank—No data |
| A4 | Canceling public events | Ordinal scale + binary for geographic scope | 0—No measures 1—Recommended cancellation 2—Required cancellation Blank—No data 0—Targeted 1—General Blank—No data |
| A5 | Restrictions on gatherings | Ordinal scale + binary for geographic scope | 0—No restrictions 1—Restrictions on very large gatherings (the limit is above 1000 people) 2—Restrictions on gatherings between 101 and 1000 people 3—Restrictions on gatherings between 11 and 100 people 4—Restrictions on gatherings of 10 people or less Blank—No data 0—Targeted 1—General Blank—No data |
| A6 | In-person school closures | Ordinal scale + binary for geographic scope | 0—No measures 1—Recommended closing 2—Required closing at some levels 3—Required closing at all levels Blank—No data 0—Targeted 1—General Blank—No data |
| A7 | In-person workplace closures | Ordinal scale + binary for geographic scope | 0—No measures 1—Recommended closing (or recommend work from home) 2—Required closing (or work from home) for some sectors or categories of workers 3—Required closing (or work from home) for all-but-essential workplaces (e.g., grocery stores, doctors) Blank—No data 0—Targeted 1—General Blank—No data |
| A8 | Stay-at-home requirements | Ordinal scale + binary for geographic scope | 0—No measures 1—Recommended not leaving the house 2—Required not leaving the house with exceptions for daily exercise, grocery shopping, and “essential” trips 3—Required not leaving the house with minimal exceptions (e.g., allowed to leave once a week, or only one person can leave at a time, etc.) Blank- No data 0—Targeted 1—General Blank—No data |
| A9 | Closing public transportation | Ordinal scale + binary for geographic scope | 0—No measures 1—Recommended closing (or significantly reduced volume/route/means of transport available) 2—Required closing (or prohibited most citizens from using it) Blank—No data 0—Targeted 1—General Blank—No data |
| A10 | Restrictions on internal movement | Ordinal | 0—no measures 1—Recommended not to travel between regions/cities 2—Internal movement restrictions in place Blank—Bo data 0—Targeted 1—General Blank—No data |
| A11 | Transparent communications | Ordinal | 0—No measures 1—Establishing a transparent communications mechanism by the government though with pauses 2—Establishing nonstop transparent communications by the government on COVID-19 Blank—No data |
| P1 | Contact tracing | Ordinal | 0—No contact tracing 1—Limited contact tracing; not done for all cases 2—Comprehensive contact tracing; done for all identified cases Blank—No data |
| P2T | Testing policy | Ordinal | 0—No testing policy 1—Only those who both (a) have symptoms AND (b) meet specific criteria (e.g., key workers, admitted to hospital, came into contact with a known case, returned from overseas) 2—Testing of anyone showing COVID-19 symptoms 3—Open public testing (e.g., “drive through” testing available to asymptomatic people) Blank—No data |
| P3 | Quarantine | Ordinal | 0—No quarantine policy 1—Only targeted to international travelers 2—Quarantining all persons with infection risks, including travelers, close contacts, suspected cases and recovered patients Blank—No data |
| P4 | Public information campaigns | Ordinal | 0—No COVID-19 public information campaign 1—Public officials urging caution about COVID-19 2—Coordinated public information campaigns (e.g., across traditional and social media) Blank—No data |
| P5 | Mask-wearing | Ordinal | 0—No measures 1—Recommended mask-wearing in public places 2—Compulsory mask-wearing in public places Blank—No data |
| H1 | Increasing the supply of PPE | Ordinal | 0—No measures 1—Some action to increase the supply of PPE 2—Used all-societal resources to the increase supply of PPE Blank—No data |
| H2 | Building/strengthening health facilities | Ordinal | 0—No measures 1—Renovated health facilities or strengthen infection control in health facilities 2—Built new health facilities for COVID-19 patients only Blank—No data |
References
- Roser, M.; Ritchie, H.; Ortiz-Ospina, E.; Hasell, J. Coronavirus Pandemic (COVID-19). Our World Data. Published Online 4 March 2020. Available online: https://ourworldindata.org/coronavirus (accessed on 2 August 2021).
- COVID-19 Situation Update Worldwide, As of Week 50 2020. European Centre for Disease Prevention and Control. Available online: https://www.ecdc.europa.eu/en/geographical-distribution-2019-ncov-cases (accessed on 18 December 2020).
- SARS-CoV-2 Variants. World Health Organization. Available online: http://www.who.int/csr/don/31-december-2020-sars-cov2-variants/en/ (accessed on 25 January 2021).
- World Health Organization. Tracking SARS-CoV-2 Variants. Available online: https://www.who.int/en/activities/tracking-SARS-CoV-2-variants/ (accessed on 4 August 2021).
- Lopez Bernal, J.; Andrews, N.; Gower, C.; Gallagher, E.; Simmons, R.; Thelwall, S.; Stowe, J.; Tessier, E.; Groves, N.; Dabrera, G.; et al. Effectiveness of Covid-19 Vaccines against the B.1.617.2 (Delta) Variant. N. Engl. J. Med. 2021. [Google Scholar] [CrossRef]
- Prem, K.; Liu, Y.; Russell, T.W.; Kucharski, A.J.; Eggo, R.M.; Davies, N. The effect of control strategies to reduce social mixing on outcomes of the COVID-19 epidemic in Wuhan, China: A modelling study. Lancet Public Health 2020, 5, e261–e270. [Google Scholar] [CrossRef] [Green Version]
- Leung, K.; Wu, J.T.; Liu, D.; Leung, G.M. First-wave COVID-19 transmissibility and severity in China outside Hubei after control measures, and second-wave scenario planning: A modelling impact assessment. Lancet 2020, 395, 1382–1393. [Google Scholar] [CrossRef]
- Wong, J.E.L.; Leo, Y.S.; Tan, C.C. COVID-19 in Singapore—Current Experience: Critical Global Issues That Require Attention and Action. JAMA 2020, 323, 1243. [Google Scholar] [CrossRef] [PubMed]
- Pan, A.; Liu, L.; Wang, C.; Guo, H.; Hao, X.; Wang, Q.; Huang, J.; He, N.; Yu, H.; Lin, X.; et al. Association of Public Health Interventions With the Epidemiology of the COVID-19 Outbreak in Wuhan, China. JAMA 2020, 323, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thomas, H.; Webster, S.; Petherick, A.; Phillips, T.; Kira, B. Oxford COVID-19 Government Response Tracker. Blavatnik School of Government. Available online: https://www.bsg.ox.ac.uk/research/research-projects/coronavirus-government-response-tracker (accessed on 20 December 2020).
- OxCGRT/Covid-Policy-Tracker. GitHub. Available online: https://github.com/OxCGRT/covid-policy-tracker (accessed on 20 December 2020).
- Hartfield, M.; Alizon, S. Introducing the outbreak threshold in epidemiology. PLOS Pathog. 2013, 9, e1003277. [Google Scholar] [CrossRef] [Green Version]
- The Party Central Committee Sets Up a Leading Group for Epidemic Response. The Paper. Available online: https://www.thepaper.cn/newsDetail_forward_5639081 (accessed on 1 July 2020).
- Prevention and Control of COVID-19 in Taiwan. Available online: https://www.cdc.gov.tw/En/Category/Page/0vq8rsAob_9HCi5GQ5jH1Q (accessed on 1 July 2020).
- Low, J. COVID-19 Crisis Management: An Early Look. Ethos. Available online: https://www.csc.gov.sg/articles/covid-19-crisis-management-an-early-look (accessed on 3 June 2020).
- Law to Cope with Coronavirus Impact Clears Legislative Floor—Focus Taiwan. Available online: https://focustaiwan.tw/politics/202002250010 (accessed on 1 July 2020).
- Shanghai, Tianjin, Chongqing, and ANHUI Launch a First-Level Response Mechanism for Major Public Health Emergencies. Chinese Government Website. Available online: http://www.gov.cn/xinwen/2020-01/24/content_5472050.htm (accessed on 1 July 2020).
- Protection from Online Falsehoods and Manipulation Act. POFMA Office. Available online: https://www.pofmaoffice.gov.sg/regulations/protection-from-online-falsehoods-and-manipulation-act/ (accessed on 1 July 2020).
- Umeda, S. South Korea: Parliament Responded Quickly to COVID-19 by Amending Three Acts. Global Legal Monitor. Published 4 June 2020. Available online: http://www.loc.gov/law/foreign-news/article/south-korea-parliament-responded-quickly-to-covid-19-by-amending-three-acts/ (accessed on 1 July 2020).
- Q68: How Did the Chinese Government Address Misinformation Amid the COVID-19 Outbreak? Center for International Knowledge on Development, China (CIKD). Available online: http://www.cikd.org/english/detail?leafId=213&docId=1420 (accessed on 1 July 2020).
- Department of Health—Press Release. Available online: https://www.dh.gov.hk/textonly/english/press/2020/press_2020.html (accessed on 1 July 2020).
- Lessons from Taiwan’s Experience with COVID-19. Atlantic Council. Published 7 April 2020. Available online: https://www.atlanticcouncil.org/blogs/new-atlanticist/lessons-from-taiwans-experience-with-covid-19/ (accessed on 1 July 2020).
- Legal News. SingaporeLegalAdvice.com. Available online: https://singaporelegaladvice.com/legal-news/ (accessed on 1 July 2020).
- How South Korea Flattened the Curve. ProQuest. Available online: http://search.proquest.com/docview/2381936994/C3AECB690C424A35PQ/1?accountid=10598 (accessed on 1 July 2020).
- Information on the Novel Coronavirus Diseases (COVID-19). Ministry of Foreign Affairs of Japan. Available online: https://www.mofa.go.jp/p_pd/pds/page22e_000910.html (accessed on 1 July 2020).
- China ends 76-Day Lockdown of Wuhan City, Where the Virus Outbreak Started. CNBC. Published 8 April 2020. Available online: https://www.cnbc.com/2020/04/08/coronavirus-china-ends-lockdown-of-wuhan-city-where-outbreak-started.html (accessed on 1 July 2020).
- Singapore to Close Schools, Most Workplaces with Rising Virus Cases. Bloomberg.com. Published 3 April 2020. Available online: https://www.bloomberg.com/news/articles/2020-04-03/singapore-pm-says-more-steps-coming-on-virus-lee-speaks-at-4pm (accessed on 1 July 2020).
- All Schools in Japan Told to Close Until April over Virus Outbreak. The Japan Times. Available online: https://www.japantimes.co.jp/news/2020/02/27/national/hokkaido-coronavirus-school/ (accessed on 1 July 2020).
- MOE Postpones Start of 2020 Spring Semester. Ministry of Education of the People’s Republic of China. Available online: https://en.moe.gov.cn/news/press_releases/202001/t20200130_417069.html (accessed on 1 July 2020).
- CE Announces Activation of Emergency Response Level in Relation to Novel Coronavirus Infection. Available online: https://www.info.gov.hk/gia/general/202001/26/P2020012600087.htm (accessed on 1 July 2020).
- CHP Closely Monitors Cluster of Pneumonia Cases on Mainland. Available online: https://www.info.gov.hk/gia/general/201912/31/P2019123100667.htm (accessed on 1 July 2020).
- Ha, B.T.T.; Ngoc Quang, L.; Mirzoev, T.; Tai, N.T.; Thai, P.Q.; Dinh, P.C. Combating the COVID-19 epidemic: Experiences from Vietnam. Int. J. Environ. Res. Public Health 2020, 17, 3125. [Google Scholar] [CrossRef] [PubMed]
- Legislative Council of the Hong Kong Special Administrative Region. Panel on Health Services (Papers). Available online: https://www.legco.gov.hk/yr19-20/english/panels/hs/papers/hs_n6.htm (accessed on 1 July 2020).
- Coronavirus Disease 19(COVID-19). Ministry of Health and Welfare. Available online: http://ncov.mohw.go.kr/en/ (accessed on 1 July 2020).
- Guangdong Province Decides to Initiate a Primary Response to Major Public Health Emergencies. Highlights. Available online: http://www.sz.gov.cn/szzt2010/yqfk2020/ywjj/content/post_6685320.html (accessed on 1 July 2020).
- Hubei Launches Level I Response to Major Public Health Emergencies. The Paper. Available online: https://www.thepaper.cn/newsDetail_forward_5621889 (accessed on 1 July 2020).
- Singapore Pledges $2.7 Billion More, Virus Measures Extended. Bloomberg.com. Published 21 April 2020. Available online: https://www.bloomberg.com/news/articles/2020-04-21/singapore-extends-partial-lockdown-measures-until-june-1 (accessed on 1 July 2020).
- Ministry of Health & Welfare: News & Welfare Services. Available online: https://www.mohw.go.kr/eng/nw/nw0101vw.jsp?PAR_MENU_ID=1007&MENU_ID=100701&page=1&CONT_SEQ=353953 (accessed on 1 July 2020).
- COVID-19 (Temporary Measures) (Control Order) Regulations 2020. Singapore Statutes Online. Available online: https://sso.agc.gov.sg/SL/COVID19TMA2020-S254-2020?DocDate=20200407 (accessed on 1 July 2020).
- Tokyo Governor Urges People to Stay Indoors over Weekend as Virus Cases Spike. The Japan Times. Available online: https://www.japantimes.co.jp/news/2020/03/25/national/science-health/tokyo-logs-40-coronavirus-cases/ (accessed on 1 July 2020).
- COVID-19 Emergency Strength Disease Page. Health Ministry. Available online: https://ncov.moh.gov.vn/ (accessed on 1 July 2020).
- Help Speed up Contact Tracing with TraceTogether. Available online: http://www.gov.sg/article/help-speed-up-contact-tracing-with-tracetogether (accessed on 1 July 2020).
- South Korea Keeps Covid-19 at bay without a Total Lockdown. The Economist. Available online: http://www.economist.com/asia/2020/03/30/south-korea-keeps-covid-19-at-bay-without-a-total-lockdown (accessed on 1 July 2020).
- COVID-19 Strategy: The Japan Model. Available online: https://thediplomat.com/2020/04/covid-19-strategy-the-japan-model/ (accessed on 1 July 2020).
- Bingqin, L.; Xiao, C. Proactive and coordinated response to COVID-19: Comparing the experience of China, South Korea and Singapore during the first 100 days. Available online: http://cikd.org/english/detail?leafId=213&docId=1540 (accessed on 1 July 2020).
- Wuhan City: Epidemiological Investigation and Testing of Five Types of Personnel. Hubei Provincial Health Commission. Available online: http://wjw.hubei.gov.cn/bmdt/mtjj/mtgz/202004/t20200421_2236177.shtml (accessed on 1 July 2020).
- National Screening, Wuhan Fights again. Hubei Provincial Health Commission. Available online: http://wjw.hubei.gov.cn/bmdt/mtjj/mtgz/202005/t20200521_2283084.shtml (accessed on 1 July 2020).
- Wong, S.Y.S.; Kwok, K.O.; Chan, F.K.L. What can countries learn from Hong Kong’s response to the COVID-19 pandemic? Can. Med. Assoc. J. 2020, 192, E511–E515. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, C.J.; Ng, C.Y.; Brook, R.H. Response to COVID-19 in Taiwan: Big data analytics, new technology, and proactive testing. JAMA 2020, 323, 1341–1342. [Google Scholar] [CrossRef] [PubMed]
- Ng, Y. Evaluation of the effectiveness of surveillance and containment measures for the first 100 patients with COVID-19 in Singapore: 2 January–29 February 2020. MMWR Morb Mortal Wkly Rep. 2020, 69, 307. [Google Scholar] [CrossRef]
- Viet Nam Has Conducted 275,000 COVID-19 Tests, Health Official Says—Viet Nam Has Conducted 275,000 COVID-19 Tests, Health Official Says. VGP News. Available online: http://news.chinhphu.vn/Home/Viet-Nam-has-conducted-275000-COVID19-tests-health-official-says/20205/40083.vgp (accessed on 1 July 2020).
- Siripala, T. Japan’s Surge in COVID-19 Infections Threatens to Derail Healthcare System. Available online: https://thediplomat.com/2020/04/japans-surge-in-covid-19-infections-threatens-to-derail-healthcare-system/ (accessed on 1 July 2020).
- KCDC. Available online: http://www.cdc.go.kr (accessed on 1 July 2020).
- Q32: Why do COVID-19 Patients Need Collective or Home Quarantine for 14 Days after Being Discharged from Hospitals? Center for International Knowledge on Development, China (CIKD). Available online: http://www.cikd.org/english/detail?leafId=213&docId=1321 (accessed on 1 July 2020).
- [Q&A] All Overseas Arrivals Required to Spend 2 Weeks in Quarantine as of 1 April. Available online: http://english.hani.co.kr/arti/english_edition/e_national/935085.html (accessed on 1 July 2020).
- China (Taiwan) M of FA Republic of. FAQ: Taiwan’s 14-Day Quarantine Requirements. Taiwan Today. 18 March 2020. Available online: https://taiwantoday.tw/news.php?unit=2&post=173589 (accessed on 1 July 2020).
- Everything You Need to Know about Quarantine Orders. Available online: http://www.gov.sg/article/everything-you-need-to-know-about-quarantine-orders (accessed on 1 July 2020).
- New Covid-19 Tourism Policies in Vietnam. Vietnam Tourism. Available online: http://vietnam.travel/things-to-do/covid-19-travel-policies-vietnam (accessed on 1 July 2020).
- Welle, D. How Vietnam Is Winning Its “War” on Coronavirus. DW.COM. Available online: https://www.dw.com/en/how-vietnam-is-winning-its-war-on-coronavirus/a-52929967 (accessed on 1 July 2020).
- Coronavirus Travel Restrictions and Bans Globally: Updating List. The New York Times. Available online: https://www.nytimes.com/article/coronavirus-travel-restrictions.html (accessed on 1 July 2020).
- Japan Imposes 14-Day Self-Quarantine for Travelers from United States. Stars and Stripes. Available online: https://www.stripes.com/news/pacific/japan-imposes-14-day-self-quarantine-for-travelers-from-united-states-1.623498 (accessed on 1 July 2020).
- Chen, L.; Xiao, C. China’s Strategies and Actions Against COVID-19 and Key Insights. Available online: http://www.cikd.org/english/detail?leafId=213&docId=1541 (accessed on 1 July 2020).
- Huynh, T.L.D. The COVID-19 containment in Vietnam: What are we doing? J. Glob. Health 2020, 10, 010338. [Google Scholar] [CrossRef] [PubMed]
- How to Redeem the New Reusable Mask. Available online: https://www.gov.sg/article/when-should-i-wear-a-mask (accessed on 1 July 2020).
- Maintain Social Distancing, Wear Masks and Take Public Transportation to Prevent Wuhan Pneumonia. Taiwan English News. Available online: https://www.taiwannews.com.tw/ch/news/3910606 (accessed on 1 July 2020).
- Cheng, V.C.; Wong, S.; Chuang, V.W.; So, S.Y.; Chen, J.H.; Sridhar, S.; To, K.K.; Chan, J.F.; Hung, I.F.; Ho, P.; et al. The role of community-wide wearing of face mask for control of coronavirus disease 2019 (COVID-19) epidemic due to SARS-CoV-2. J. Infect. 2020, 81, 107–114. [Google Scholar] [CrossRef] [PubMed]
- Face Masks in a Pandemic: From “Useless” to “Indispensable”. The Japan Times. Available online: https://www.japantimes.co.jp/news/2020/05/01/world/science-health-world/face-masks-pandemic/ (accessed on 1 July 2020).
- Environmental Cleaning Guidelines. National Environmental Agency of Singapore. Available online: https://www.nea.gov.sg/our-services/public-cleanliness/environmental-cleaning-guidelines (accessed on 1 July 2020).
- Lin, C.; Braund, W.E.; Auerbach, J.; Chou, J.H.; Teng, J.H.; Tu, P.; Mullen, J. Policy decisions and use of information technology to fight COVID-19, Taiwan. Emerg. Infect. Dis. J. 2020, 26, 1506. [Google Scholar] [CrossRef] [PubMed]
- What Can Data on Testing Tell Us about the Pandemic? Our World in Data. Available online: https://ourworldindata.org/what-can-data-on-testing-tell-us-about-the-pandemic (accessed on 1 July 2020).
- Nguyen, D. Vietnam Successfully Designs Test Kit for New Coronavirus. Vietnam Insider. Published 4 March 2020. Available online: https://vietnaminsider.vn/vietnam-successfully-designs-test-kit-for-new-coronavirus/ (accessed on 1 July 2020).
- Utzerath, F.B.D.L.-J.; Bird, R.; Cheng, G. Contact Tracing Apps in China, Hong Kong, Singapore and South Korea | Lexology. Available online: https://www.lexology.com/library/detail.aspx?g=99dca469-455d-4f7a-b025-00bf1d10ff6b (accessed on 30 June 2020).
- Q41: Health Code: What and How? Center for International Knowledge on Development, China (CIKD). Available online: http://www.cikd.org/english/detail?leafId=213&docId=1342 (accessed on 20 December 2020).
- Fighting Covid-19: East Asian Responses to the Pandemic. Institut Montaigne. Available online: https://www.institutmontaigne.org/en/publications/fighting-covid-19-east-asian-responses-pandemic (accessed on 30 June 2020).
- Saiidi, U. Hong Kong Is Putting Electronic Wristbands on Arriving Passengers to Enforce Coronavirus Quarantine. CNBC. Published 18 March 2020. Available online: https://www.cnbc.com/2020/03/18/hong-kong-uses-electronic-wristbands-to-enforce-coronavirus-quarantine.html (accessed on 30 June 2020).
- Zou, H.; Shu, Y.; Feng, T. How Shenzhen, China avoided widespread community transmission: A potential model for successful prevention and control of COVID-19. Infect. Dis. Poverty 2020, 9, 1–4. [Google Scholar] [CrossRef]
- Park, O.; Park, Y.J.; Park, S.Y.; Kim, Y.M.; Kim, J.; Lee, J.; Park, E.; Kim, D.; Jeon, B.H.; Ryu, B.; et al. Contact transmission of COVID-19 in South Korea: Novel investigation techniques for tracing contacts. Osong Public Health Res. Perspect. 2020, 11, 60–63. [Google Scholar] [CrossRef] [Green Version]
- Vietnam’s Exemplary Response to COVID-19. The ASEAN Post. Available online: https://theaseanpost.com/article/vietnams-exemplary-response-covid-19 (accessed on 30 June 2020).
- Robots and Drones are Now Used to Fight COVID-19. Available online: https://www.forbes.com/sites/bernardmarr/2020/03/18/how-robots-and-drones-are-helping-to-fight-coronavirus/#580cc37b2a12 (accessed on 30 June 2020).
- Remote Platform, Bluezone App Launched in Support of Medical Treatment, Including COVID-19. VGP News. Available online: http://news.chinhphu.vn/Home/Remote-platform-Bluezone-app-launched-in-support-of-medical-treatment-including-COVI19/20204/39790.vgp (accessed on 30 June 2020).
- Japanese Ministry, METI, Launches Free Remote Health Consultation Service to Address COVID-19 Related Concerns. Healthcare IT News. 24 March 2020. Available online: https://www.healthcareitnews.com/news/asia-pacific/japanese-ministry-meti-launches-free-remote-health-consultation-service-address (accessed on 30 June 2020).
- Lee, D.; Lee, J. Testing on the move: South Korea’s rapid response to the COVID-19 pandemic. Transp. Res. Interdiscip. Perspect. 2020, 5, 100111. [Google Scholar] [CrossRef]
- 3 Ways China Is Using Drones to Fight Coronavirus. World Economic Forum. Available online: https://www.weforum.org/agenda/2020/03/three-ways-china-is-using-drones-to-fight-coronavirus/ (accessed on 30 June 2020).
- Sealed in: Chinese Trapped at Home by Coronavirus Feel the Strain. Reuters. Published 22 February 2020. Available online: https://www.reuters.com/article/us-china-health-quarantine-idUSKCN20G0AY (accessed on 30 June 2020).
- Hermesauto. Coronavirus: Stay Home for Singapore Portal Launched to Help People Make Purposeful Use of Time during Circuit Breaker. The Straits Times. 11 April 2020. Available online: https://www.straitstimes.com/singapore/coronavirus-stay-home-for-singapore-portal-launched-to-help-people-make-purposeful-use-of (accessed on 30 June 2020).
- Bi, Q.; Wu, Y.; Mei, S.; Ye, C.; Zou, X.; Zhang, Z.; Liu, X.; Wei, L.; Truelove, S.A.; Zhang, T.; et al. Epidemiology and transmission of COVID-19 in 391 cases and 1286 of their close contacts inShenzhen, China: A retrospective cohort study. Lancet Infect. Dis. 2020, 20, 911–919. [Google Scholar] [CrossRef]
- Chang, M.-C.; Kahn, R.; Li, Y.-A.; Lee, C.-S.; Buckee, C.O.; Chang, H.-H. Modeling the impact of human mobility and travel restrictions on the potential spread of SARS-CoV-2 in Taiwan. medRxiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Koo, J.R.; Cook, A.R.; Park, M.; Sun, Y.; Sun, H.; Tao, J.; Clarence, L.; Borame, T.; Dickens, L. Interventions to mitigate early spread of SARS-CoV-2 in Singapore: A modelling study. Lancet Infect. Dis. 2020, 20, 678–688. [Google Scholar] [CrossRef] [Green Version]
- Yoo, K.J.; Kwon, S.; Choi, Y.; Bishai, D. Systematic Assessment of South Korea’s Capabilities to Control COVID-19. Health Policy J. 2021, 125, 568–576. [Google Scholar] [CrossRef]
- Variation in Government Responses to COVID-19. Available online: https://www.bsg.ox.ac.uk/research/publications/variation-government-responses-covid-19 (accessed on 21 December 2020).
- Koh, W.C.; Naing, L.; Wong, J. Estimating the impact of physical distancing measures in containing COVID-19: An empirical analysis. Int. J. Infect. Dis. 2020, 100, 42–49. [Google Scholar] [CrossRef]
- Dergiades, T.; Milas, C.; Panagiotidis, T. How Effectively Have Governments Responded to COVID-19 so Far? British Politics and Policy at LSE. Published 1 June 2020. Available online: https://blogs.lse.ac.uk/politicsandpolicy/ (accessed on 21 December 2020).
- Liu, Y.; Morgenstern, C.; Kelly, J.; Lowe, R.; CMMID COVID-19 Working Group; Jit, M. The Impact of Non-Pharmaceutical Interventions on SARS-CoV-2 Transmission across 130 Countries and Territories. Health Policy 2020, 19, 1–12. [Google Scholar] [CrossRef]
- Nkengasong, J. China’s response to a novel coronavirus stands in stark contrast to the 2002 SARS outbreak response. Nat. Med. 2020, 26, 310–311. [Google Scholar] [CrossRef]
- Choi, S.M.Y.; Lam, P.Y. Enhancing legal preparedness for the prevention and control of infectious diseases: Experience from severe acute respiratory syndrome in Hong Kong. Public Health 2009, 123, 242–246. [Google Scholar] [CrossRef] [PubMed]
- NHCC. Available online: https://www.cdc.gov.tw/En/Category/MPage/gL7-bARtHyNdrDq882pJ9Q (accessed on 1 July 2020).
- Okabe, N. Epidemiological situation on pandemic influenza H1N1 2009 in the world and in Japan. JMAJ 2011, 54, 277–283. [Google Scholar]
- 2015 MERS outbreak in Republic of Korea. Available online: https://www.who.int/westernpacific/emergencies/2015-mers-outbreak (accessed on 23 December 2020).
- Category of Communicable Disease Control. Taiwan Centers for Disease Control. Available online: https://www.cdc.gov.tw/En/Category/ListPage/HrXtdwzKFsLSdd6z2a1x5A (accessed on 1 July 2020).
- Communicable Disease Control Act. Laws & Regulations Database of the Republic of China. Available online: https://law.moj.gov.tw/ENG/LawClass/LawHistory.aspx?pcode=L0050001 (accessed on 1 July 2020).
- Normile, D. Coronavirus Cases Have Dropped Sharply in South Korea. What’s the Secret to its Success? Science|AAAS. Published 17 March 2020. Available online: https://www.sciencemag.org/news/2020/03/coronavirus-cases-have-dropped-sharply-south-korea-whats-secret-its-success (accessed on 1 July 2020).
- Oh, M.; Park, W.B.; Park, S.; Choe, P.G.; Bang, J.H.; Song, K.; Kim, E.S.; Kim, H.B.; Kim, N.J. Middle East respiratory syndrome: What we learned from the 2015 outbreak in the Republic of Korea. Korean J. Intern. Med. 2018, 33, 233–246. [Google Scholar] [CrossRef] [PubMed]
| Indicator ID | Included in OxCGRT | Indicator Name | Description |
|---|---|---|---|
| Administrative | |||
| A1 | No | Coordinated governance | Recorded establishing a national task force/committee consisting of leaders from different ministries/sectors |
| A2 | No | Legislation and regulations | Recorded developing or amending existing legislation and regulations for COVID-19 control |
| A3 | Yes | Border control | Recorded border control for COVID-19 control |
| A4 | Yes | Canceling public events | Recorded canceling public events |
| A5 | Yes | Restrictions on gatherings | Recorded the cut-off size for bans on private gatherings |
| A6 | Yes | School closures | Recorded school and university closures |
| A7 | Yes | Workplace closures | Recorded workplace closures |
| A8 | Yes | Stay-at-home requirements | Recorded “shelter-in-place” and otherwise confine to the home |
| A9 | Yes | Closing public transportation | Recorded public transportation closures |
| A10 | Yes | Restrictions on internal movement | Recorded restrictions on moving between regions/cities |
| A11 | No | Transparent communications | Recorded establishing transparent communications working mechanism |
| Public health | |||
| P1 | Yes | Contact tracing | Recorded government policy on contact tracing after a positive diagnosis |
| P2 | Yes | Testing policy | Recorded government policy on who has access to testing |
| P3 | No | Quarantine | Recorded government policy on quarantine |
| P4 | Yes | Public information campaigns | Recorded presence of public information campaigns on COVID-19 |
| P5 | No | Mask-wearing | Recorded mask-wearing policy for COVID-19 control |
| Health system | |||
| H1 | No | Increasing the supply of PPE | Recorded actions on increasing the supply of PPE for health professionals |
| H2 | No | Building/strengthening health facilities | Recorded actions to build or strengthen health facilities |
| Key Control Measures | Geographic Coverage | Common Practice | Variation in Implementation |
|---|---|---|---|
| Administrative | |||
| Establishing coordinated governance [13,14,15,30,31,32,33,34] | All but JP | Established at the very early stage of the outbreak, with high-level political leadership and commitment, and multi-sectoral or multi-ministerial coordination. | Governments differ in the timeliness of establishing this coordinated high-level leadership (e.g., HK, TW, SG, and VN did so even before there were ≤5 confirmed cases) |
| Amending/adding legislations or regulations [14,16,17,18,19,35,36] | CHN, TW, SG, SK and VN | Governments usually add new regulations or pass new acts related to COVID-19 control, and impose severe penalties to violators for enforcement. | New rules differ in legislative nature (Act, Regulations, etc.), regulated thematic areas and enforcement stringency (e.g., SG and SK have issued strict penalty rules for violation). |
| Transparently sharing epidemiological status [20,22,23,24,25,32] | All | Press conferences were held across the study sites and media tools were used to present timely updates to the public. | Governments differ in the timeliness of establishing these transparent sharing mechanisms. Variations also exist in format and frequency. |
| Implementing mobility restrictions interventions [26,27,28,29,37,38,39,40] | All | Governments have used their executive power to implement administrative interventions to restrict people’s mobility, including border control, lockdowns, and social distancing. Lockdowns and social distancing were achieved through interventions such as traffic control, non-essential business closures, shelter-in-place policies, in-person school closures, etc. | Study sites differ in the package of interventions implemented and the stringency of their implementation. |
| Public Health | |||
| Aggressive contact tracing aided by digital tools [41,42,43,44] | All but JP | Contact tracing is done through massive and careful epidemiological investigations among close contacts of people who test positive. Given its labor-intensive nature, most countries mobilized human resources and adopted digital tools to assist with the process. | All are similar except for Japan, which uses a different cluster-based approach to trace contacts and did not implement aggressive measures, to protect personal privacy. |
| Extensive testing [45,46,47,48,49,50,51,52] | All but JP | Governments focused on conducting nucleic acid amplification tests to detect the virus in suspected cases and in close contacts of confirmed cases. | All are similar except for Japan, which had adopted a restrictive testing approach aiming to not overwhelm its healthcare system. |
| Strict quarantine [48,53,54,55,56,57,58,59,60,61] | All but JP | Quarantine has been implemented among people with infection risk, including close contacts, suspected cases, travelers, and recovered COVID-19 patients. | All are similar except for Japan, in which quarantine policies are comparatively loose and target only travelers. |
| Mask-wearing (compulsory and voluntary) [43,62,63,64,65,66,67] | All | Both healthy and infected people are encouraged to wear masks in public places. | Compulsory mask-wearing was observed in some study sites from the very beginning (e.g., CHN, VN), while voluntary mask-wearing was observed in others (HK, SK and JP). Some adjusted their policy to make mask-wearing compulsory for all, including for healthy people (SG and TW). |
| Disinfecting public places [68] | All | Regular and thorough disinfection of public places, especially those with large population mobility and density. | No variations |
| Widespread temperature screening | All | Wide thermal equipment was set up in public places such as subway entries and airports and manual temperature checks were given to people before entering a residential area or closed building | No variations |
| Health education/awareness campaigns [45] | All | Health education and awareness campaigns were usually implemented on TV, social media, and phones and in public places, etc. | No variations |
| Health system | |||
| Improving health service delivery [45,62,69,70,71] | All | Governments focused on increasing testing capacity, building new health facilities, increasing the supply of PPE, and improving the triage of patients to improve health service delivery. | Governments differ in the timeliness of initiating these actions, and in the resources utilized for implementation. |
| Mobilizing the health workforce [45] | CHN, SG, and SK | Human resources for health were mobilized from other regions to support the most heavily affected places. | Study sites differ in the scale of health workforce mobilization and the types of health workers mobilized. |
| Increasing health financing [24] | All | Effective financing strategies were implemented to cover the majority, if not all, of the testing and treatment costs through health insurance plus special subsidies. | Study sites differ in the costs and population coverage (eg. SK had everything covered). |
| Enhancing health information systems [45] | CHN | Careful monitoring, review, and timely publication of cases and a strong oversight and accountability mechanism | Data unavailable |
| Purpose | Data Collected | Intrusiveness | Examples |
|---|---|---|---|
| Regular documentation and analysis | Health, travel history, drug purchase behaviors, etc. | High | CHN, TW, HK—border control health declaration by scanning a QR code [72] CHN—“Health code” [73], drug purchase direct reporting system [34], health self-reporting system, online registration system for employees to contain risk, etc. TW [74]—big data system to integrate health insurance and customs and immigration database; a digital platform to operate a nationalized system of mask distribution, and the “NHI Express App” for users to check mask availability SK—big data system to collect people’s credit card transaction data, CCTV footage, and mobile phone locations etc. |
| Real-time tracking and alert system | Health, travel history, GPS location, CCTV footage, etc. | High | TW [14]—electronic security monitoring system and SMS notifications; social distancing alert app HK [75]—wristbands and mobile app SK [24]—cell phones vibrate with emergency alerts when cases are nearby |
| Contact tracing | Health, basic socio-economic status, travel history, credit card, CCTV footage, etc. | High | CHN [76], TW [14], SK [77], VN [78]—using big data to trace contacts SG [42]—TraceTogether (mobile app) VN [41]—Bluezone (mobile app) |
| Online health consultation and diagnosis | Health, travel history, and other relevant information per request | Medium | CHN [79]—remote consultation with doctors online; AI-assisted diagnosis JP [80], VN [81]—remote consultation SK [82]—self-diagnosis app |
| Non-human-contact delivery and management | N/A | Low | CHN [79,83]— Drones: delivery of goods and medical samples; disinfection; crowd management Robots: meals delivery and disinfection |
| Peer and community support | N/A | Low | CHN [84]—WeChat group to coordinate needs for living essential goods for collective order and delivery SG [85]—“Stay Home for Singapore” portal |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, S.; Guo, L.; Alghaith, T.; Dong, D.; Alluhidan, M.; Hamza, M.M.; Herbst, C.H.; Zhang, X.; Tagtag, G.C.A.; Zhang, Y.; et al. Effective COVID-19 Control: A Comparative Analysis of the Stringency and Timeliness of Government Responses in Asia. Int. J. Environ. Res. Public Health 2021, 18, 8686. https://doi.org/10.3390/ijerph18168686
Chen S, Guo L, Alghaith T, Dong D, Alluhidan M, Hamza MM, Herbst CH, Zhang X, Tagtag GCA, Zhang Y, et al. Effective COVID-19 Control: A Comparative Analysis of the Stringency and Timeliness of Government Responses in Asia. International Journal of Environmental Research and Public Health. 2021; 18(16):8686. https://doi.org/10.3390/ijerph18168686
Chicago/Turabian StyleChen, Shu, Lei Guo, Taghred Alghaith, Di Dong, Mohammed Alluhidan, Mariam M. Hamza, Christopher H. Herbst, Xinqi Zhang, Gabrielle Charis Alano Tagtag, Yi Zhang, and et al. 2021. "Effective COVID-19 Control: A Comparative Analysis of the Stringency and Timeliness of Government Responses in Asia" International Journal of Environmental Research and Public Health 18, no. 16: 8686. https://doi.org/10.3390/ijerph18168686
APA StyleChen, S., Guo, L., Alghaith, T., Dong, D., Alluhidan, M., Hamza, M. M., Herbst, C. H., Zhang, X., Tagtag, G. C. A., Zhang, Y., Alazemi, N., Saber, R., Alsukait, R., & Tang, S. (2021). Effective COVID-19 Control: A Comparative Analysis of the Stringency and Timeliness of Government Responses in Asia. International Journal of Environmental Research and Public Health, 18(16), 8686. https://doi.org/10.3390/ijerph18168686