Abstract
As the incidence and prevalence of diabetes increases, intervention through dietary education is becoming more important for diabetes control. This systematic review examines the evidence for the efficacy of dietary education interventions on diabetes control. The study subjects were patients with type 2 diabetes, and the main outcome variable was glycosylated hemoglobin level (HbA1c). The target studies were randomized controlled trials. Thirty-six studies were included in the analysis, of which 33 were included in the meta-analysis. The effect size between dietary education and general interventions was −0.42 (n = 5639, MD = −0.42; 95% CI −0.53 to −0.31) and was significantly different (Z = 7.73, p < 0.001). When subgroup analyses were performed following the application periods, intervention methods, and intervention contents, the mean differences in 4–6-month application, individual education, and diet-exercise-psychosocial intervention were −0.51, (n = 2742, 95% CI −0.71 to −0.32), −0.63 (n = 627, 95% CI −1.00 to −0.26), and −0.51 (n = 3244, 95% CI −0.71 to −0.32), respectively. Dietary education interventions provided for at least 3 months were highly effective in controlling HbA1c levels. Regarding the education method, individualized education was more effective, and contact or non-contact education may be applied for this. Combining diet, exercise, and psychosocial intervention is more effective than diet education alone.
1. Introduction
The incidence of diabetes mellitus is increasing worldwide. According to the International Diabetes Association, diabetes patients worldwide account for 8.3% of the total population, and it is expected that this number will reach 592 million by 2035 [1]. Diabetes is a chronic metabolic disease that causes complications such as cardiovascular disease, arteriosclerosis, hypertension, neuropathy, nephropathy, and diabetic retinopathy [2]. Type 2 diabetes usually occurs after the age of 40 and accounts for about 90% of all diabetes patients. Unlike type 1 diabetes, there are often no clear clinical symptoms in the early stages. The onset of type 2 diabetes is preceded by a decrease in insulin secretion, followed by a metabolic disorder due to an increase in insulin resistance [3]. In many cases, type 2 diabetes mellitus can be improved if weight is reduced through diet and exercise at an early stage [3].
Thus, the most basic goal of treatment is to maintain a normal blood glucose level [2]. Treatment options include insulin therapy, exercise, dietary intervention, and psychological intervention [2]. Although drug and insulin therapy are necessary, patient-centered dietary and exercises education interventions to prevent complications have also gained importance. Dietary education is essential and requires education, counseling, and diet management [4]. Previous studies have reported that dietary education interventions can cause a significant reduction in not only body mass index (BMI), glycated hemoglobin (HbA1c), and fasting blood sugar levels, but also the risk of microvascular complications and cardiovascular disease [5,6].
To the authors’ knowledge, a total of five systematic reviews of the effectiveness of dietary education interventions for patients with type 2 diabetes have been published previously. In these reviews, the intervention methods included remote therapy intervention, web education intervention, dietary carbohydrate restriction, and nutrition therapy [7,8,9,10,11]. However, dietary education is provided in various forms such as individualized, group, self-help group, and web-based education, and different content focusing on general or specific diet information is provided. Moreover, the duration of education varies with each study; thus, it is necessary to assess the effects of each of these aspects. Outcome variables to assess the effects of dietary education on blood glucose control were body weight, BMI, blood pressure, postprandial blood glucose, glycosylated hemoglobin level (HbA1c), and cholesterol; the most important outcome variable was HbA1c. HbA1c, an important indicator of glycemic control, is closely correlated with average blood sugar levels in diabetes patients, and it is also an indicator for the reduced risk of complications [12,13]. Thus, HbA1C is a suitable indicator to assess the clinical effects of dietary education.
This study aimed to systematically review randomized controlled trials (RCTs) that assessed HbA1c levels after providing dietary education interventions in various ways and with different content. Then, a meta-analysis was performed to estimate the effects of dietary education interventions in patients with type 2 diabetes.
2. Materials and Methods
2.1. Data Sources and Searches
In this study, we systematically reviewed RCTs that provided qualitative and quantitative data to assess the clinical effects of dietary education interventions in patients with type 2 diabetes. Literature searches were conducted up to March 2020 using international databases such as PubMed, EMBASE, CINAHL, and Cochrane Central Register of Controlled Trials. The domestic databases used to search for published journals and theses were DBpia, Korean Studies Information Service System, Research Information Service System, NDSL, and Korea Med. To increase the sensitivity of the literature search, gray literature such as theses, news, and presentations were searched for manually in addition to searching in electronic databases. MeSH terms and text words using AND/OR and truncation were used for the literature search. MeSH terms were used to search for articles in international databases. Studies that used the term “diabetes mellitus” as the intervention method were selected, and main variables such as “diet” and “education” terms were used for extraction. Filtering was used according to the characteristics of each database, and methods to increase the specificity and sensitivity of the search were used. The search terms used in the international databases were “Diabetes mellitus” and “Education” and “Diet” and “HbA1c.” The MeSH search function was not available in the domestic databases. Thus, concept words for “type 2 diabetes,” “metabolic syndrome,” “blood sugar control,” and “diet” were used as keywords to search for articles (Table 1). Research reports and theses were excluded from the study. This study was exempt from needing approval from the institutional review board as it is a systematic review (EUIRB2020-08).

Table 1.
Summary of randomized controlled trials on the effects of diet education for patients with type 2 diabetes mellitus.
2.2. Study Selection
Two investigators (the first and second authors) independently evaluated the articles for eligibility. Studies on the effects of dietary education interventions in type 2 diabetes patients, especially RCTs, were selected. Academic papers were chosen when there was an overlap between academic papers and a thesis. Participants, intervention, comparison, and outcome (PICO), which are the specific questions for systematic literature reviews, are as follows. The patient population of this study included adults with type 2 diabetes. Experimental interventions considered for this study were web-based, individualized or grouped, or self-help group dietary education interventions or diet-related educational interventions. The comparative intervention in this study was the general education intervention provided to diabetes patients. In this study, the control group was the group that received usual care provided to diabetic subjects. The outcome after the intervention in type 2 diabetes patients was blood glucose level. In this study, HbA1c, which is representative of the blood glucose level for the last 3 months, was assessed.
2.3. Inclusion and Exclusion Criteria
This systematic review considered for inclusion any RCT that assesses a Dietary Education intervention in type 2 diabetes mellitus population. The primary outcomes were HbA1c at different follow-up periods to measure the glycemic control of type 2 diabetes mellitus. Exclusion criteria were: (1) study designs other than RCTs; (2) type 1 diabetes mellitus population, prediabetes, gestational diabetes mellitus; (3) educational interventions that do not include dietary interventions; (4) Studies not published in Korean or English; (5) unpublished theses; and (6) experiments on animals or studies on children, preclinical studies.
2.4. Data Synthesis and Analysis
Cochrane Review Manager (RevMan, London, UK) software 5.3 was used for the analysis of selected studies that measured outcome variables and systematic intervention methods. Meta-analysis can be performed when multiple scientific studies address the same question, with each study reporting measurements that are expected to have some degree of error. The Cochrane Quality Assessment tool in Cochrane software evaluates the risk of selection bias, performance bias, detection bias, attrition bias, and reporting bias as low, high, or uncertain. Results were then entered into RevMan and evaluation results for the assessed risk were presented according to the evaluation criteria.
3. Results
3.1. Characteristics of Studies Selected for the Systematic Literature Review
Published journals were searched in domestic and international databases until March 2020, and gray journals were searched manually. A total of 36 studies were selected and included in the analysis (Table 1). The meta-analysis was performed on the 33 selected papers, wherein the outcome variables and intervention methods were the same. Of the 33 pieces of literature available for meta-analysis, 5 studies provided only dietary education interventions, the other 9 studies provided dietary education interventions and exercise therapy, and the remaining 19 studies provided dietary education interventions, exercise therapy, and psychosocial therapy. The results and number of experimental and control groups are presented in Table 1 and Figure 1.
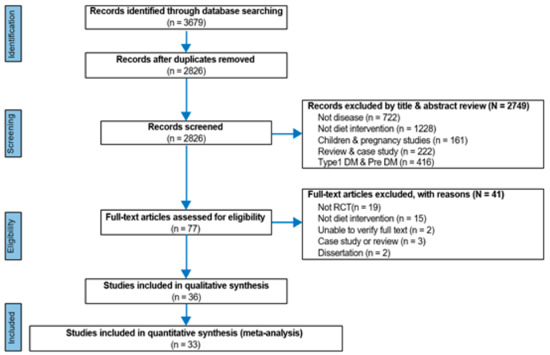
Figure 1.
Flowchart of the study selection process. DM = Diabetes mellitus, RCT = Randomized controlled trial.
3.2. Literature Quality Assessment
As a result of the quality evaluation of the study, there were several cases with unclear performance and detection bias; the attrition bias was due to the high attrition rate of the study participants. The results are shown in Figure 2.
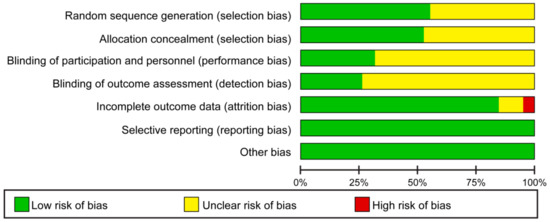
Figure 2.
Risk of bias graph.
3.3. Effects of Dietary Education Interventions on HbA1cin Type 2 Diabetes Patients
Among the selected 36 papers, the effect size on the dietary education of type 2 diabetes patients was meta-analyzed for 33 of which the effect size analysis was possible. In addition, subgroup analysis was performed according to education period, education method, and education content.
3.3.1. Comparison of the HbA1C Effect Size According to the Duration of Dietary Education Interventions in Type 2 Diabetes Patients
The effect size of HbA1C in type 2 diabetes patients was analyzed by dividing it into the type of educational intervention and follow-up time points.
HbA1C Effect Size at the Endpoints of Dietary Education Interventions
The effect size in the dietary education experimental group decreased by 0.28 (n = 385, MD = −0.28; 95% CI −0.65 to 0.09) compared with the control group; however, the difference was not significant (Z = 1.51, p < 0.13) (Figure 3).
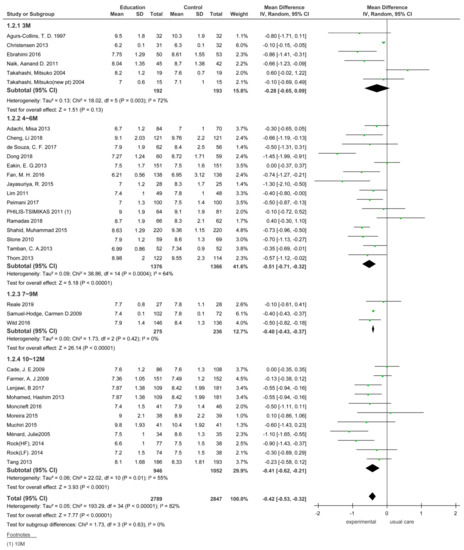
Figure 3.
Immediate effect of dietary education intervention on patients with type 2 diabetes. SD, standard deviation; CI, confidence interval; IV, inverse variance.
An analysis of 14 studies that assessed HbA1c 4–6 months after the completion of dietary education showed that the effect size in the dietary education experimental group decreased by 0.51 (n = 2742, MD = −0.51; 95% CI −0.71 to −0.32) compared with the control group. The difference in the effect size between the two groups was significant (Z = 5.18, p < 0.001).
An analysis of three studies that assessed HbA1c 7–9 months after dietary education completion showed that the effect size in the dietary education experimental group decreased by 0.40 (n = 511, MD = −0.40; 95% CI −0.43 to −0.37) compared with that seen in the control group. The difference in the effect size between the two groups was significant (Z = 26.14, p < 0.001).
An analysis of 11 studies that assessed HbA1c 10–12 months after the completion of dietary education showed that the effect size in the dietary education experimental group decreased by 0.41 (n = 1998, MD = −0.41; 95% CI −0.62 to −0.21) compared with that in the control group. The difference in the effect size between the two groups was significant (Z = 3.93, p < 0.001).
HbA1c Effect Size in Dietary Education Interventions Assessed at Different Follow-up Time-Points
After completion of the dietary education intervention in type 2 diabetes patients, the effects were analyzed at different HbA1c measurement durations (Figure 4). An analysis of nine studies showed that the effect size of HbA1c during dietary education intervention for 3 months was not homogeneous (Education G. vs. Control group G.: I2 = 83%). Therefore, a random-effects model was used to analyze the results between the experimental and control groups; the effect size decreased by 0.32 (n = 672, MD = −0.32; 95% CI −0.59 to −0.05) in the experimental group compared with the control group, which was not significant (Z = 2.31, p = 0.02).
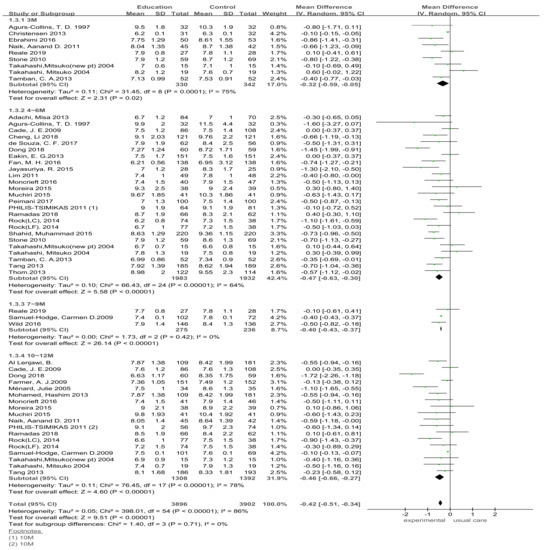
Figure 4.
Follow-up effect of dietary education intervention on patients with type 2 diabetes. SD, standard deviation; CI, confidence interval; IV, inverse variance.
An analysis of 25 studies that assessed HbA1C during dietary education for 4–6 months showed that the effect size of HbA1C in the experimental group decreased by 0.47 (n = 3915, MD = −0.47, 95% CI −0.63 to −0.30) compared with that in the comparison group; the difference was significant (Z = 5.58, p < 0.001).
An analysis of three studies that assessed HbA1C during dietary education for 7–9 months showed that the effect size of HbA1C in the experimental group decreased by 0.40 (n = 511, MD = −0.40; 95% CI −0.43 to −0.37) compared with the control group; the difference was significant (Z = 26.16, p < 0.001).
An analysis of HbA1C during dietary education for 10–12 months showed that the effect size of HbA1C in the experimental group decreased by 0.46 (n = 2600, MD = −0.46; 95% CI −0.66 to −0.27) compared with the control group; the difference was significant (Z = 4.60, p < 0.001).
3.3.2. Comparison of the Effect Size of HbA1C According to Dietary Education Intervention Methods
The HbA1C effect size was analyzed according to different methods of dietary education in patients with type 2 diabetes (Figure 5). The intervention methods were divided into non-face-to-face and face-to-face education. Ten studies used web- and mobile-phone-based non-face-to-face education and face-to-face education was classified into individualized and grouped education interventions. There were four and 19 studies on individualized and grouped education interventions, respectively.
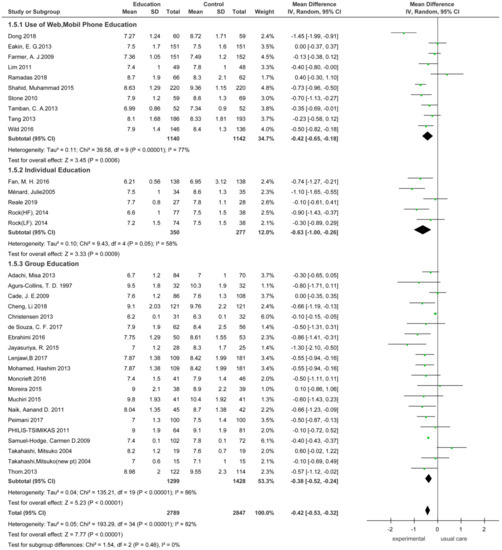
Figure 5.
Forest plot of the effect of the intervention method. SD, standard deviation; CI, confidence interval; IV, inverse variance.
An analysis of 10 studies on the web- and mobile phone-based non-face-to-face dietary education interventions showed that the effect size of HbA1C in the experimental group decreased by 0.42 (n = 2282, MD = −0.42 95% CI −0.65 to −0.18) compared with the control group, and the difference was significant (Z = 3.45, p = 0.006).
The effect size in the experimental group that received individual dietary education interventions decreased by 0.63 (n = 627, MD = −0.63; 95% CI: −1.00.to −0.26) compared with the control group, and the difference was significant (Z = 3.33, p < 0.009). The effect size in the experimental group that received grouped dietary education interventions decreased by 0.38 (n = 2727, MD = −0.38; 95% CI −0.52 to −0.24) compared with the control group, and the difference was significant (Z = 5.23, p < 0.001).
3.3.3. Comparison of the Effect Size of HbA1C According to Dietary Education Contents
There were five studies on dietary-centered education interventions. Interventions in the group included a low-carbonate group, low-fat group, low glycemic index (GI) diet group, and low-fruit group vs. high-fruit group. There were nine dietary and exercise education interventions and 19 studies on dietary, exercise, and psychosocial education interventions (Figure 6).
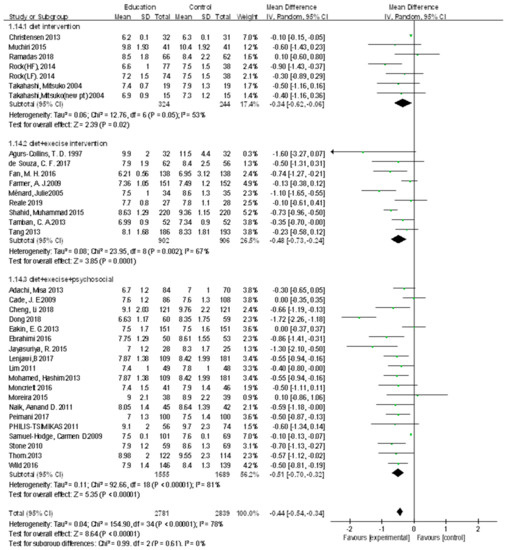
Figure 6.
Forest plot of the effect of diet education. SD, standard deviation; CI, confidence interval; IV, inverse variance.
A comparison between the experimental and control groups that underwent dietary-centered education interventions and general interventions, respectively, showed that the effect size decreased by 0.15 (n = 568, MD = −0.15; 95% CI −0.46 to 0.17) in the experimental group compared with the control group, which was not significant (Z = 0.92, p = 0.36).
Comparison between the experimental and control groups that underwent dietary and exercise education intervention and general intervention, respectively, showed that the effect size decreased by 0.48 (n = 1808, MD = −0.48; 95% CI −0.73 to −0.24) in the experimental group compared with the comparison group, which was significant (Z = 3.85, p < 0.001).
A comparison between the experimental and control groups that underwent dietary exercise and a psychosocial education intervention and a general intervention, respectively, showed that the effect size decreased by 0.48 (n = 3260, MD = −0.48; 95% CI −0.61 to −0.35 in the experimental group compared with the comparison group, and the difference was significant (Z = 7.21, p < 0.001).
3.4. Publication Bias
The 33 studies analyzed in the meta-analysis are scattered around the effect estimate, whereas the large-scale studies are distributed at the top of the graph. Small-scale studies are distributed at the bottom of the graph and the graph is shaped like a funnel; it indicates that there is no publication bias (Figure 7).
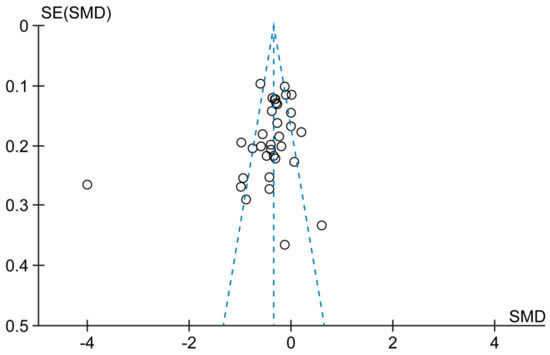
Figure 7.
Funnel plot of comparison. SE: Standard Error, SD: standard deviation.
4. Discussion
This systematic literature review was performed to assess the effects of dietary education interventions in type 2 diabetes patients. The interventions included web-based, self-help, and individualized or grouped dietary or educational interventions that included diet. Comparison groups consisted of type 2 diabetes patients who were provided with general education interventions. HbA1c was selected as the outcome variable.
We found that HbA1c levels were lower in the experimental group after dietary education interventions compared with those in the control group. Diet and exercise interventions are emphasized as important in diabetes guidelines [35] and nutritional interventions are effective in controlling blood sugar levels [11]. Therefore, dietary education interventions for diabetes patients are thought to be effective interventions for controlling blood sugar levels. Subgroup analysis was performed to analyze HbA1c levels according to the duration of dietary education. HbA1c levels assessed after 4–6, 7–9, and 10–12 months of dietary education interventions were lower in the experimental group than in the control group. In contrast, HbA1c assessed after 3 months of an education intervention did not show a significant difference between the two groups. In addition, HbA1C levels according to the duration of dietary education intervention, including the follow-up period, were lower in the experimental group at 4–6, 7–9, and 10–12 months. Studies have shown that a repetitive and long-term dietary education intervention that offers follow-up management was more effective than a short-term education intervention [35]. Moreover, considering that HbA1c reflects the blood sugar level at 3 months, it is thought that dietary education interventions for 4 months or longer are necessary. In particular, there is a need for continuous control of blood glucose levels in diabetes to prevent complications. Maintaining HbA1c levels < 6.5% for 6 years is known to help prevent complications, including microvascular complications [50]. Therefore, continuous follow-up interventions would be necessary in addition to dietary education interventions for 4 months or longer.
Analysis of face-to-face and web- and mobile phone-based non-face-to-face education interventions showed that both face-to-face (individualized and group education) and non-face-to-face interventions were effective. In particular, individual education interventions showed low heterogeneity between studies and large effect sizes. Experimental studies reported that HbA1c decreased by 1.0%–2.0% in type 1 and type 2 diabetes patients after individual nutritional education [51,52]. Furthermore, systematic reviews have shown that web-based education interventions led to decreased HbA1C [8,9]. Considering these findings, individual education seems to be effective and should be given to diabetes patients.
Different dietary education intervention contents were also analyzed. Subgroup analysis of a dietary-centered education intervention, dietary and athletic education intervention, and dietary exercise and psychosocial intervention showed that the effect size of HbA1c was significantly reduced in the two intervention groups, except for the dietary-centered education intervention. This finding is consistent with the results of a 20-year follow-up study, which showed significantly decreased HbA1C after a dietary and athletic education interventions [53]. Similar findings were reported by another study where HbA1c significantly decreased after a dietary education and moderate exercise strategy that included a decrease of 500–750 kcal and 175 min of moderate-intensity exercise per week. Therefore, combining diet, exercise, and psychosocial intervention is considered more effective than diet education alone.
The limitations of this study are as follows. First, the contents and methods of interventions were diverse between studies, and it was difficult to divide them into different groups. Second, the literature search was limited to articles published in academic journals. Thus, research reports and theses were excluded. Moreover, a tendency to publish only statistically significant results was noted. Therefore, there may be a possibility of publication bias or overestimation of the results. Another limitation is that the results of the sub-analysis on dietary education interventions could not be derived as intervention methods and detailed contents were not provided in studies. The studies included in this meta-analysis have included complex dietary education interventions, so there may be high heterogeneity. Therefore, it is necessary to carefully interpret the research results.
5. Conclusions
Dietary education interventions are very effective in controlling blood sugar, and a duration of at least 3 months is required. Individual education is more effective than face-to-face or web and mobile phone education. Further, interventions are thought to be more effective when dietary, exercise, and psychosocial education interventions are provided together rather than when dietary education is provided alone. Studies with long-term as opposed to short-term interventions are needed; web- and mobile-based individual dietary education interventions would be more effective than group interventions. Further research is necessary to present a wide range of generalized results, including the specific variables in the study.
Author Contributions
Conceptualization, J.K. and M.-H.H.; Methodology, J.K. and M.-H.H.; Software, J.K.; Validation, J.K. and M.-H.H.; Formal Analysis, J.K. and M.-H.H.; Investigation, J.K. and M.-H.H.; Resources, J.K. and M.-H.H.; Data Curation, J.K. and M.-H.H.; Writing—Original Draft Preparation, J.K. and M.-H.H.; Writing J.K. and M.-H.H. Review & Editing, J.K. and M.-H.H.; Visualization, J.K.; Supervision, M.-H.H.; Project Administration, J.K. and M.-H.H.; Funding Acquisition, M.-H.H. Both authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the National Research Foundation of Korea (NRF) grant by the Korean Government, grant number NRF-2020R1F1A1076225.
Institutional Review Board Statement
This study was approved for exemption from the institutional review board before the study due to it being a systematic review (EUIRB2020-08).
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
References
- Atlas, D. International Diabetes Federation, IDF Diabetes Atlas, 7th ed.; International Diabetes Federation: Brussels, Belgium, 2015. [Google Scholar]
- Kim, M.K.; Ko, S.H.; Kim, B.Y.; Kang, E.S.; Noh, J.; Kim, S.K.; Park, S.O.; Hur, K.Y.; Chon, S.; Moon, M.K.; et al. 2019 Clinical Practice Guidelines for Type 2 Diabetes Mellitus in Korea. Diabetes Metab. J. 2019, 43, 398–406. [Google Scholar] [CrossRef]
- DeFronzo, R.A.; Ferrannini, E.; Groop, L.; Henry, R.R.; Herman, W.H.; Holst, J.J.; Hu, F.B.; Kahn, C.R.; Raz, I.; Shulman, G.; et al. Type 2 diabetes mellitus. Nat. Rev. Dis. Prim. 2015, 1, 15019. [Google Scholar] [CrossRef]
- Silva, F.M.; Kramer, C.K.; De Almeida, J.C.; Steemburgo, T.; Gross, J.L.; Azevedo, M.J. Fiber intake and glycemic control in patients with type 2 diabetes mellitus: A systematic review with meta-analysis of randomized controlled trials. Nutr. Rev. 2013, 71, 790–801. [Google Scholar] [CrossRef]
- Yang, S.H.; Chung, H.-K.; Lee, S.-M. Effects of Activity-Based Personalized Nutrition Education on Dietary Behaviors and Blood Parameters in Middle-Aged and Older Type 2 Diabetes Korean Outpatients. Clin. Nutr. Res. 2016, 5, 237–248. [Google Scholar] [CrossRef]
- Nathan, D.M.; Barrett-Connor, E.; Crandall, J.; Edelstein, S.L.; Goldberg, R.; Horton, E.S.; Knowler, W.; Mather, K.J.; Orchard, T.; Pi-Sunyer, X.; et al. Long-term effects of lifestyle intervention or metformin on diabetes development and microvascular complications over 15-year follow-up: The Diabetes Prevention Program Outcomes Study. Lancet Diabetes Endocrinol. 2015, 3, 866–875. [Google Scholar] [CrossRef]
- Huang, J.; Qin, S.; Huang, L.; Tang, Y.; Ren, H.; Hu, H. Efficacy and safety of Rhizoma curcumea longae with respect to improving the glucose metabolism of patients at risk for cardiovascular disease: A meta-analysis of randomised controlled trials. J. Hum. Nutr. Diet. 2019, 32, 591–606. [Google Scholar] [CrossRef]
- Hou, C.; Carter, B.; Hewitt, J.; Francisa, T.; Mayor, S. Do Mobile Phone Applications Improve Glycemic Control (HbA1c) in the Self-management of Diabetes? A Systematic Review, Meta-analysis, and GRADE of 14 Randomized Trials. Diabetes Care 2016, 39, 2089–2095. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.E.; Kim, E.; Kim, G. The effects of diabetes management programs using mobile app: A systematic review and a me-ta-analysis. J. Korea Contents Assoc. 2015, 15, 300–307. [Google Scholar] [CrossRef]
- Snorgaard, O.; Poulsen, G.M.; Andersen, H.K.; Astrup, A. Systematic review and meta-analysis of dietary carbohydrate restriction in patients with type 2 diabetes. BMJ Open Diabetes Res. Care 2017, 5, e000354. [Google Scholar] [CrossRef]
- Razaz, J.M.; Rahmani, J.; Varkaneh, H.K.; Thompson, J.; Clark, C.; Abdulazeem, H. The health effects of medical nutrition therapy by dietitians in patients with diabetes: A systematic review and meta-analysis. Prim. Care Diabetes 2019, 13, 399–408. [Google Scholar] [CrossRef]
- Wei, N.; Zheng, H.; Nathan, D.M. Empirically Establishing Blood Glucose Targets to Achieve HbA 1c Goals. Diabetes Care 2014, 37, 1048–1051. [Google Scholar] [CrossRef]
- Clarke, P.M.; Gray, A.M.; Briggs, A.; Farmer, A.J.; Fenn, P.; Stevens, R.J.; Matthews, D.R.; Stratton, I.; Holman, R.R.; on behalf of the UK Prospective Diabetes Study (UKPDS) Group. A model to estimate the lifetime health outcomes of patients with Type 2 diabetes: The United Kingdom Prospective Diabetes Study (UKPDS) Outcomes Model (UKPDS no. 68). Diabetologia 2004, 47, 1747–1759. [Google Scholar] [CrossRef] [PubMed]
- Adachi, M.; Yamaoka, K.; Watanabe, M.; Nishikawa, M.; Kobayashi, I.; Hida, E.; Tango, T. Effects of lifestyle education program for type 2 diabetes patients in clinics: A cluster randomized controlled trial. BMC Public Health 2013, 13, 467. [Google Scholar] [CrossRef]
- Agurs-Collins, T.D.; Kumanyika, S.K.; Have, T.R.T.; Adams-Campbell, L.L. A Randomized Controlled Trial of Weight Reduction and Exercise for Diabetes Management in Older African-American Subjects. Diabetes Care 1997, 20, 1503–1511. [Google Scholar] [CrossRef]
- Cade, J.E.; Kirk, S.; Nelson, P.; Hollins, L.; Deakin, T.; Greenwood, D.C.; Harvey, E.L. Can peer educators influence healthy eating in people with diabetes? Results of a randomized controlled trial. Diabet. Med. 2009, 26, 1048–1054. [Google Scholar] [CrossRef] [PubMed]
- Cheng, L.; Sit, J.W.; Choi, K.-C.; Chair, S.-Y.; Li, X.; Wu, Y.; Long, J.; Tao, M. Effectiveness of a patient-centred, empowerment-based intervention programme among patients with poorly controlled type 2 diabetes: A randomised controlled trial. Int. J. Nurs. Stud. 2018, 79, 43–51. [Google Scholar] [CrossRef]
- Christensen, A.S.; Viggers, L.; Hasselström, K.; Gregersen, S. Effect of fruit restriction on glycemic control in patients with type 2 diabetes—A randomized trial. Nutr. J. 2013, 12, 29. [Google Scholar] [CrossRef]
- Dong, Y.; Wang, P.; Dai, Z.; Liu, K.; Jin, Y.; Li, A.; Wang, S.; Zheng, J. Increased self-care activities and glycemic control rate in relation to health education via Wechat among diabetes patients: A randomized clinical trial. Medicine 2018, 97, e13632. [Google Scholar] [CrossRef] [PubMed]
- Eakin, E.G.; Reeves, M.M.; Winkler, E.; Healy, G.; Dunstan, D.; Owen, N.; Marshal, A.M.; Wilkie, K.C. Six-Month Outcomes from Living Well with Diabetes: A Randomized Trial of a Telephone-Delivered Weight Loss and Physical Activity Intervention to Improve Glycemic Control. Ann. Behav. Med. 2013, 46, 193–203. [Google Scholar] [CrossRef]
- Ebrahimi, H.; Sadeghi, M.; Amanpour, F.; Vahedi, H. Evaluation of empowerment model on indicators of metabolic control in patients with type 2 diabetes, a randomized clinical trial study. Prim. Care Diabetes 2016, 10, 129–135. [Google Scholar] [CrossRef] [PubMed]
- Amendezo, E.; Timothy, D.W.; Karamuka, V.; Robinson, B.; Kavabushi, P.; Ntirenganya, C.; Uwiragiye, J.; Mukantagwabira, D.; Bisimwa, J.; Marie, H.U.; et al. Effects of a lifestyle education program on glycemic control among patients with diabetes at Kigali University Hospital, Rwanda: A randomized controlled trial. Diabetes Res. Clin. Pr. 2017, 126, 129–137. [Google Scholar] [CrossRef] [PubMed]
- Fan, M.-H.; Huang, B.-T.; Tang, Y.-C.; Han, X.-H.; Dong, W.-W.; Wang, L.-X. Effect of individualized diabetes education for type 2 diabetes mellitus: A single-center randomized clinical trial. Afr. Health Sci. 2017, 16, 1157–1162. [Google Scholar] [CrossRef]
- Farmer, A.J.; Wade, A.N.; French, D.; Simon, J.; Yudkin, P.; Gray, A.; Craven, A.; Goyder, L.; Holman, R.R.; Mant, D.; et al. Blood glucose self-monitoring in type 2 diabetes: A randomised controlled trial. Health Technol. Assess. 2009, 13, 1–50. [Google Scholar] [CrossRef]
- Jayasuriya, R.; Pinidiyapathirage, M.; Jayawardena, R.; Kasturiratne, A.; De Zoysa, P.; Godamunne, P.; Gamage, S.; Wickremasinghe, A. Translational research for Diabetes Self-Management in Sri Lanka: A randomized controlled trial. Prim. Care Diabetes 2015, 9, 338–345. [Google Scholar] [CrossRef]
- Lim, S.; Kang, S.M.; Shin, H.; Lee, H.J.; Yoon, J.W.; Yu, S.H.; Kim, S.-Y.; Yoo, S.Y.; Jung, H.S.; Park, K.S.; et al. Improved Glycemic Control without Hypoglycemia in Elderly Diabetic Patients Using the Ubiquitous Healthcare Service, a New Medical Information System. Diabetes Care 2011, 34, 308–313. [Google Scholar] [CrossRef] [PubMed]
- Al Lenjawi, B.; Mohamed, H.; Amuna, P.; Zotor, F.; Ziki, M.D.A. Nurse-led theory-based educational intervention improves glycemic and metabolic parameters in South Asian patients with type II diabetes: A randomized controlled trial. Diabetol. Int. 2016, 8, 95–103. [Google Scholar] [CrossRef]
- Ménard, J.; Payette, H.; Baillargeon, J.-P.; Maheux, P.; Lepage, S.; Tessier, D.; Ardilouze, J.-L. Efficacy of intensive multitherapy for patients with type 2 diabetes mellitus: A randomized controlled trial. Can. Med. Assoc. J. 2005, 173, 1457–1466. [Google Scholar] [CrossRef][Green Version]
- Mohamed, H.; Al-Lenjawi, B.; Amuna, P.; Zotor, F.; Elmahdi, H. Culturally sensitive patient-centred educational programme for self-management of type 2 diabetes: A randomized controlled trial. Prim. Care Diabetes 2013, 7, 199–206. [Google Scholar] [CrossRef]
- Muchiri, J.W.; Gericke, G.J.; Rheeder, P. Effect of a nutrition education programme on clinical status and dietary behaviours of adults with type 2 diabetes in a resource-limited setting in South Africa: A randomised controlled trial. Public Health Nutr. 2015, 19, 142–155. [Google Scholar] [CrossRef] [PubMed]
- Moreira, R.C.; Mantovani, M.D.F.; Soriano, J.V. Nursing Case Management and Glycemic Control among Brazilians with Type 2 Diabetes: Pragmatic Clinical Trial. Nurs. Res. 2015, 64, 272–281. [Google Scholar] [CrossRef]
- Moncrieft, A.E.; Llabre, M.M.; McCalla, J.R.; Gutt, M.; Mendez, A.J.; Gellman, M.D.; Goldberg, R.B.; Schneiderman, N. Effects of a Multicomponent Life-Style Intervention on Weight, Glycemic Control, Depressive Symptoms, and Renal Function in Low-Income, Minority Patients with Type 2 Diabetes: Results of the Community Approach to Lifestyle Modification for Diabetes Randomized Controlled Trial. Psychosom. Med. 2016, 78, 851–860. [Google Scholar] [CrossRef] [PubMed]
- Naik, A.D.; Palmer, N.; Petersen, N.J.; Street, R.L.; Rao, R.; Suarez-Almazor, M.; Haidet, P. Comparative Effectiveness of Goal Setting in Diabetes Mellitus Group Clinics: Randomized clinical trial. Arch. Intern. Med. 2011, 171, 453–459. [Google Scholar] [CrossRef] [PubMed]
- Peimani, M.; Monjazebi, F.; Ghodssi-Ghassemabadi, R.; Nasli-Esfahani, E. A peer support intervention in improving glycemic control in patients with type 2 diabetes. Patient Educ. Couns. 2018, 101, 460–466. [Google Scholar] [CrossRef]
- Philis-Tsimikas, A.; Fortmann, A.; Lleva-Ocana, L.; Walker, C.; Gallo, L.C. Peer-Led Diabetes Education Programs in High-Risk Mexican Americans Improve Glycemic Control Compared with Standard Approaches: A Project Dulce promotora randomized trial. Diabetes Care 2011, 34, 1926–1931. [Google Scholar] [CrossRef] [PubMed]
- Ramadas, A.; Chan, C.K.Y.; Oldenburg, B.; Hussein, Z.; Quek, K.F. Randomised-controlled trial of a web-based dietary intervention for patients with type 2 diabetes: Changes in health cognitions and glycemic control. BMC Public Health 2018, 18, 1–13. [Google Scholar] [CrossRef]
- Rock, C.L.; Flatt, S.W.; Pakiz, B.; Taylor, K.S.; Leone, A.F.; Brelje, K.; Heath, D.D.; Quintana, E.L.; Sherwood, N.E. Weight Loss, Glycemic Control, and Cardiovascular Disease Risk Factors in Response to Differential Diet Composition in a Weight Loss Program in Type 2 Diabetes: A Randomized Controlled Trial. Diabetes Care 2014, 37, 1573–1580. [Google Scholar] [CrossRef]
- Reale, R.; Tumminia, A.; Romeo, L.; La Spina, N.; Baratta, R.; Padova, G.; Tomaselli, L.; Frittitta, L. Short-term efficacy of high intensity group and individual education in patients with type 2 diabetes: A randomized single-center trial. J. Endocrinol. Investig. 2018, 42, 403–409. [Google Scholar] [CrossRef] [PubMed]
- Samuel-Hodge, C.D.; Keyserling, T.C.; Park, S.; Johnston, L.F.; Gizlice, Z.; Bangdiwala, S.I. A Randomized Trial of a Church-Based Diabetes Self-management Program for African Americans with Type 2 Diabetes. Diabetes Educ. 2009, 35, 439–454. [Google Scholar] [CrossRef]
- Shahid, M.; Mahar, S.A.; Shaikh, S.; Shaikh, Z.U. Mobile phone intervention to improve diabetes care in rural areas of Pakistan: A randomized controlled trial. J. Coll. Physicians Surg. Pak. 2015, 25, 166–171. [Google Scholar]
- De Souza, C.F.; Dalzochio, M.B.; Zucatti, A.T.N.; De Nale, R.; De Almeida, M.T.; Gross, J.L.; Leitao, C. Efficacy of an education course delivered to community health workers in diabetes control: A randomized clinical trial. Endocrine 2017, 57, 280–286. [Google Scholar] [CrossRef]
- Spencer, M.S.; Rosland, A.-M.; Kieffer, E.C.; Sinco, B.R.; Valerio, M.; Palmisano, G.; Anderson, M.; Guzman, J.R.; Heisler, M. Effectiveness of a Community Health Worker Intervention among African American and Latino Adults with Type 2 Diabetes: A Randomized Controlled Trial. Am. J. Public Health 2011, 101, 2253–2260. [Google Scholar] [CrossRef] [PubMed]
- Stone, R.A.; Rao, R.H.; Sevick, M.A.; Cheng, C.; Hough, L.J.; MacPherson, D.S.; Franko, C.M.; Anglin, R.A.; Obrosky, D.S.; Derubertis, F.R. Active Care Management Supported by Home Telemonitoring in Veterans with Type 2 Diabetes: The DiaTel randomized controlled trial. Diabetes Care 2009, 33, 478–484. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, M.; Araki, A.; Ito, H. Development of a new method for simple dietary education is elderly individuals with diabetes mellitus. Nippon. Ronen Igakkai Zasshi. Jpn. J. Geriatr. 2002, 39, 527–532. [Google Scholar] [CrossRef]
- Tamban, C.; Isip-Tan, I.T.; Jimeno, C. Use of Short Message Services (SMS) for the Management of Type 2 Diabetes Mellitus: A Randomized Controlled Trial. J. ASEAN Fed. Endocr. Soc. 2013, 28, 143–149. [Google Scholar] [CrossRef]
- Tang, P.C.; Overhage, J.; Chan, A.S.; Brown, N.L.; Aghighi, B.; Entwistle, M.P.; Hui, S.L.; Hyde, S.M.; Klieman, L.H.; Mitchell, C.J.; et al. Online disease management of diabetes: Engaging and Motivating Patients Online with Enhanced Resources-Diabetes (EMPOWER-D), a randomized controlled trial. J. Am. Med Inform. Assoc. 2013, 20, 526–534. [Google Scholar] [CrossRef]
- Thom, D.H.; Ghorob, A.; Hessler, D.; De Vore, D.; Chen, E.; Bodenheimer, T.A. Impact of Peer Health Coaching on Glycemic Control in Low-Income Patients with Diabetes: A Randomized Controlled Trial. Ann. Fam. Med. 2013, 11, 137–144. [Google Scholar] [CrossRef] [PubMed]
- Varney, J.E.; Weiland, T.; Inder, W.; Jelinek, G.A. Effect of hospital-based telephone coaching on glycaemic control and adherence to management guidelines in type 2 diabetes, a randomised controlled trial. Intern. Med. J. 2014, 44, 890–897. [Google Scholar] [CrossRef]
- Wild, S.H.; Hanley, J.; Lewis, S.C.; McKnight, J.A.; McCloughan, L.B.; Padfield, P.L.; Parker, R.A.; Paterson, M.; Pinnock, H.; Sheikh, A.; et al. Supported Telemonitoring and Glycemic Control in People with Type 2 Diabetes: The Telescot Diabetes Pragmatic Multicenter Randomized Controlled Trial. PLoS Med. 2016, 13, e1002098. [Google Scholar] [CrossRef]
- Ohkubo, Y.; Kishikawa, H.; Araki, E.; Miyata, T.; Isami, S.; Motoyoshi, S.; Kojima, Y.; Furuyoshi, N.; Shichiri, M. Intensive insulin therapy prevents the progression of diabetic microvascular complications in Japanese patients with non-insulin-dependent diabetes mellitus: A randomized prospective 6-year study. Diabetes Res. Clin. Pr. 1995, 28, 103–117. [Google Scholar] [CrossRef]
- Franz, M.J.; Powers, M.A.; Leontos, C.; Holzmeister, L.A.; Kulkarni, K.; Monk, A.; Wedel, N.; Gradwell, E. The Evidence for Medical Nutrition Therapy for Type 1 and Type 2 Diabetes in Adults. J. Am. Diet. Assoc. 2010, 110, 1852–1889. [Google Scholar] [CrossRef] [PubMed]
- Evert, A.B.; Boucher, J.L.; Cypress, M.; Dunbar, S.A.; Franz, M.J.; Mayer-Davis, E.J.; Neumiller, J.J.; Nwankwo, R.; Verdi, C.L.; Urbanski, P.; et al. Nutrition Therapy Recommendations for the Management of Adults with Diabetes. Diabetes Care 2013, 37, S120–S143. [Google Scholar] [CrossRef] [PubMed]
- Li, G.; Zhang, P.; Wang, J.; Gregg, E.; Yang, W.; Gong, Q.; Li, H.; Li, H.; Jiang, Y.; An, Y.; et al. The long-term effect of lifestyle interventions to prevent diabetes in the China Da Qing Diabetes Prevention Study: A 20-year follow-up study. Lancet 2008, 371, 1783–1789. [Google Scholar] [CrossRef]







Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).