
Exploration of Mental Readiness for Enhancing Dentistry in an Inter-Professional Climate



Abstract
:1. Introduction
1.1. Performance Competencies
1.2. Shared Inter-Professional Practices
1.3. Mental Readiness for Dentistry
1.4. Aim
- (a)
- defining challenging situations in dentistry;
- (b)
- isolating and evaluating the importance of physical ability, technical knowledge and mental skills in dentistry; and
- (c)
- determining and articulating if mental readiness skills are used in daily practices among seasoned dentists.
- (d)
- identify the practical implications (“the fit”) and confirm the capacity for a more comprehensive study of operational readiness with “exceptional” dentists.
2. Methods
Controlling Investigator and Information Bias
- All questions were treated in a standard way and in a particular order. Given the retrospective nature of the questions, the timeframe for subjects’ recall was kept to a minimum (within the last few months). Questions divided events into segments so details could be easily recalled.
- The investigator was experienced in answering queries and rephrasing questions when necessary to ensure participants understood before responding. Detailed interviewing was considered superior to a survey for collecting comprehensive information in a new area. General dentistry was captured through representation of both genders, a range of client- and facilities-types, and broad international experiences.
- Efforts were made to encourage honest, candid responses. The fact that the investigator was not a dentist, created an obvious non-judgmental atmosphere for participants to speak freely. All participants were given time to review a manuscript of their responses to ensure that it authentically captured the experience related to each question.
- Thematic analysis was performed on the data by an independent reviewer. A cross-checking procedure was used to independently assess the data with methodological rigour.
- Concurrent with previous studies [20,21,23], it was concluded that manipulating the responses of high-level achievers would be extremely difficult, since these performers tend to be self-directed and act according to their own principles. They are also very keen to articulate and to pass along relevant, realistic experiences to others in the field.
3. Results and Discussion
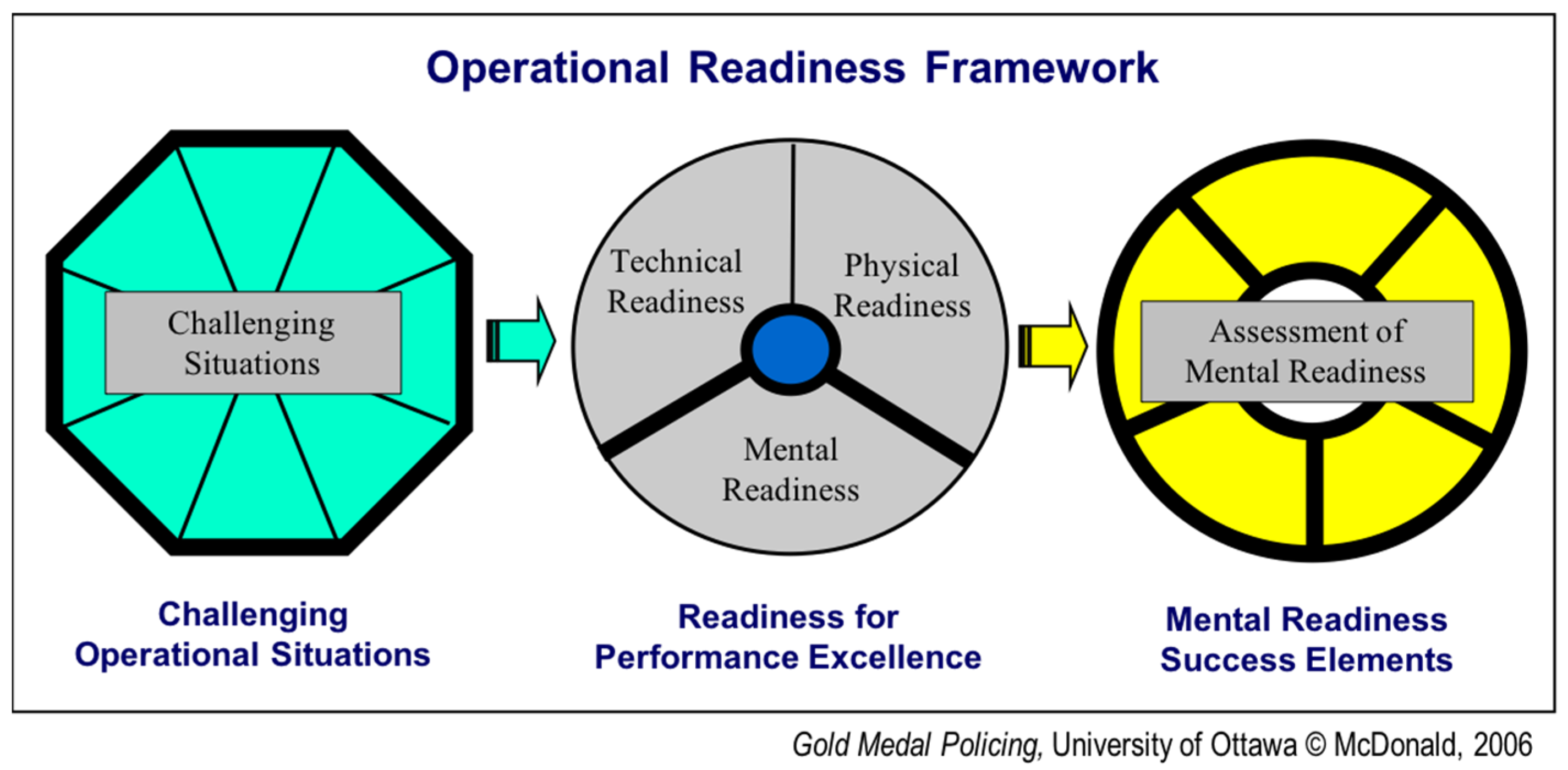
3.1. Challenging Operational Situations in Dentistry
- Particular patient behaviour—child crying and kicking (not necessarily in pain) ∙ patient’s unbelievably picky husband ∙ those really afraid of the needle ∙ patients experiencing homelessness (a love-hate relationship) ∙ cancer patient on medication with low white blood cell count.
- Procedural difficulty/risk—extraction of third molars ∙ bone grafts ∙ implants ∙ torn tongue ∙ being tired at end of the day ∙ lawsuits—the number one fear of dentists ∙ complications ∙ anything where you might permanently lose the tooth ∙ matching the colour and angulations on two front teeth
- Degree of complexity—minor things are not hard but complex things like opening flaps or surgical extraction of teeth ∙ mouth full of blood (is patient in pain?) ∙ sustaining proper sterilization practices ∙ equipping clinic with up-to-date first aid ∙ hazardous waste disposal ∙ lack of pharmacological knowledge
- Teaching/managing responsibilities—staff issues (e.g., lateness, illness, computers, staff-client problems) ∙ business part (versus just the technique part) is huge! ∙ asking for money if client is unhappy ∙ dealing with insurance telling you what to do ∙ having balance in my life
- Special relationship pressures—relatives or a family member (‘relativeoma’) of the patient or friends (‘privatitis’) ∙ multiple relationships to manage (dentist and staff/client/patient) ∙ the private-space thing for some dentists ∙ you start to hurt the patient from not having the person frozen when doing a procedure
3.2. Readiness for Performance Excellence
- No complications at 6-month follow-up;
- No immediate or 24-h post-pain;
- Patient was comfortable in the clinic;
- When everything goes well;
- When complications were dealt with successfully;
- A positive final result.
- A first-time procedural error;
- Final result achieved without profit;
- Something out-of-your-control;
- Something simple was missed like taking an X-ray or a tooth wiggling;
- A complication in the last half-hour of the day;
- Failure to educate the patient;
- A patient’s non-compliance.
- Physically—healthy and fit; has good ergonomics positioning (no stress-related injuries; e.g., back, neck, shoulders, arms, carpal tunnel); has good vision; manages fatigue; performs necessary hand-skill coordination, tactile sensitivity and manual dexterity; is artistic; carves nicely; uses mirror.
- Technically—has knowledge and application of dental techniques; knows and follows directives/laws; coordinates patient treatment plan and referrals; has good business practices (policies, billing, receivables); has modern equipment and instruments; effective at verbal and written communication.
- Mentally—confident; committed and compassionate; able to build relationships; clear-headed; adaptable to change; sets a goal and a plan; has a positive attitude and deals well with unplanned situations; able to concentrate and refocus; evaluates decisions with effective coping skills.
3.3. Physical and Technical Readiness
- Prerequisites for competences;
- Patient Examination Assessment and Diagnosis;
- Communication and Patient Education;
- Ethics and Jurisprudence;
- Treatment;
- Medical Emergencies;
- Practice Management.
Ability, injury—The physical part is your hand skills, tactile sensitivity and manual dexterity combined with your health or sore back or whatever. The big injuries and pain from physical stress to avoid are in the back, neck, shoulders, lower-arms, knees, headaches, carpal tunnel and repetitive stress.
Artistry—The dentist has to be artistic in order to contour the tooth. I’ve seen a lot of colleagues who, when they first got into dental school, would have never thought that. Some people just don’t have the ability to draw nicely or carve nicely. So obviously, the outcome is not as good as they wished. However, there is no way around it.
How much?—The business aspect of dentistry was not given enough in dental school. You cannot invest too much or you’ll have to charge too much. Not all patients can afford it and you might lose business. The business part (versus just technical) is HUGE! You have to win your customers not only by your profession—your excellence in dentistry—but also by having a good one-on-one relationship with them. You have to be positive and you have to be convincing.
3.4. Mental Readiness Success Elements
3.4.1. Commitment
- Having compassion to reduce pain;
- setting high standards (e.g., prepared to include “green” and cultural accountability)
- feeling overall enjoyment;
- persisting through complexity;
- feeling responsible for your patients;
- remaining sincere to avoid complaints and lawsuits;
- creating a strong work–life balance.
Integrity redefined—Dentistry is more fragile now. More dentists choose group practices over sole ownership for greater protection to cope with customers. Integrity needs to include cultural preparedness, environmental accountability, patient comfort and ethics around payment requests. Being too conservative for dentist safety (or defensive medicine) is a bad practice. A dentist must preserve all aspects of what can be done to help the patient.
Daily balance—It is an ongoing challenge to keep your life in balance because unless YOU are right [laugh], nothin’ else is right. I work on a work-play-love-worship model. You need a balance of these things. You can’t work 24 h a day… I try on a daily basis to dedicate myself to each section… If you are aware of that from the start then you’re not likely to get into too much in one area. If you do, at least have the realization why you’re out of balance, and what needs to be done to rectify it. That is HUGE.
3.4.2. Confidence
- Acquire self-confidence through practice;
- Assess and accept patients who are like-minded;
- Know your patient;
- Promote team pride;
- Evoke the Peter Principle and refer to specialists;
- Join study-group clubs;
- Seek mentor support;
- Pursue continuous education (near and abroad).
Three-way pride—‘If you can’t brag on ‘em, fire ‘em!’ It’s a two-way street. If your staff can’t brag about you, they should leave. And the same with a patient: If a patient can’t brag about you as their dentist, then [spit sound]… they should leave too.
3.4.3. Positive Imagery
- Visualize the final result;
- Draw pictures of the tooth;
- Rehearse using visual aids;
- Prepare to treat with an optimistic mental attitude;
- Develop a positive patient-relationship.
Visualize first—You always try to see the final result in your head. It’s like a golf shot. You want to visualize where the shot’s going to ideally end up, and then you execute it… I’m doing it as I’m talking to them, if I can, because so many things come in to play.
3.4.4. Mental Preparation
- Pre-plan the logistics;
- Allow ample time for the appointment;
- Anticipate complications and options;
- Have daily preparation rituals;
- Put pictures up to explain the plan or present alternatives to waiting patients;
- Prepare for the unexpected.
Rituals, calm—I believe that if you are psychologically calm and relaxed, you can perform better… It is whatever keeps your psyche down—like drinking tea, reading sports results, doing mindfulness or yoga, praying… even taking one deep breath.
Retrench—Take a deep breath. Start with that. Retrench. Sometimes I’ll leave the room if the patient isn’t in any danger. Go back and retrench. Think about it for a couple of minutes. You’ve got that luxury.
3.4.5. Focus
- Have total concentration;
- Communicate non-verbally;
- Control your own emotions by staying calm and relaxed;
- Have a patient-centred mindset (e.g., sharing the steps aloud);
- Be nice;
- Be comfortable feeling the rhythm and flow of the procedure (the economy of movement);
- Create effortlessness in your practice.
Simply be nice—Dentists are probably one of the few professionals that people will allow to work in very close proximity for about an hour—really close in their mouth, face with your face, bodies very close to each other. Patients have to be really, really trusting of the dentist. It’s not only doing a good job from a technical aspect, you are also being allowed to be close to them. Patients we see every day are mostly in pain and not in a good mood… You have to be nice.
Get it right—It’s not just doing the technical. Getting the right relationship with the patient makes things easier. People don’t like the damn needle. If people like you, you can hurt them a bit. Okay, it hurts but if they don’t like you, it hurts a lot more for them [laugh].
3.4.6. Distraction Control
- Use creative personal means to immediately control the excitement;
- Be honest with the patient;
- Be willing to apologize;
- Be willing to be flexible;
- Redo or correct;
- Put the distraction on hold;
- Take charge and push through;
- Avoid mental fatigue by taking a walk, drinking tea or switching tasks.
Control doubts—Now we don’t use amalgams anymore because of the mercury. It’s always in the back of your mind—‘half of what I’m doin’ is wrong.’ However, you do what you can. You have to have goals. You have to be honest and sincere. Mistakes happen but you did what you could and it’s out of your control.
Get back on track—I am reasonably fit and well rested when I go in there so I don’t feel that physical fatigue. It is mostly mental if I start to lose my edge in being sharp. Dentists have to be able to calm down in a way that nobody else notices like using humour, lowering your voice, speaking very slowly or taking time to choose the right words. Slowing down and talking in a calm way actually calms the patient as well.
3.4.7. Evaluation and Coping
- Be reflective;
- Have a realistic goal;
- Discuss at study group;
- Invest in continuing education;
- Recognize and assess technological changes;
- Seek patient feedback;
- Do your best;
- Adjust after an error;
- Recognize unexpected setbacks;
- Practice work–life balance.
Perfection—You can never do it right. Generally, you’re very self-critical of most things you do. You see what could have been better, even though the patient’s not in any particular danger—little tiny things and sometimes bigger stuff—then maybe you start over because you’re not happy with it.
Amicable—Absorb their ignorance. You say, ‘Well, I cannot do this because of this and this. Even though I’m telling you this, you might want to get a second opinion.’ You can throw it back. It’s a good release for you. ‘You know what? If you’re going to challenge my judgment, I’d rather not see you’—but you say it in a really nice way.
Painful pressures—There’s a lot of pressures financially and ethically. It’s extremely stressful after five years—it is difficult to expand, make everyone happy or everything else you don’t think about. Some dentists are uncomfortable with the private-space thing—and that’s not good. It can all lead to a lot of psychological problems (like depression and drugs) in looking for an out because it’s so painful.
Exercise restraint—Banks come calling offering the world for some immediate gratification which can be appealing after almost a decade of schooling. Hold off on big purchases until the practice is paid off—most often after 10-years. Joining a group practice or associate can still mean overwhelming debt. Debt affects motivation and satisfaction with a ripple-effect on safe and competent delivery of treatment. It’s a lousy way to start what should be a rewarding career-chapter.
3.5. Comparisons across Professions
3.5.1. Surgeons
Building confidence—Surgeons have great belief in the significance of their interventions. The most successful moments in my life are those when I removed a tumor. That experience over the years has led to building-up my confidence.—Oncology surgeon
Team visualization—I meet with the surgery team and together we visualize the operation scenarios and discuss the details. This is the most important preparatory step and it really does not matter who eventually performs the surgery.—Cardiothoracic surgeon
Patient preparations—Beforehand, you communicate with your patient so they understand what you are going to do and what complications could happen. You see the patient has confidence in you.—Cardiac surgeon
3.5.2. Social Workers
4. Conclusions
- Significance of mental readiness: Compared to dentists, top performers in other high-risk professions demonstrate excellent technical and physical skills but where dentists stand out is their proficiency in mental readiness [17,18,19,20,21] (McDonald et al., 2016, 2015, 1995; McDonald, 2006; Zhang et al., 2000). Similarly, these case studies indicated that well-honed mental readiness was a major contributor (49%) to best performances in demanding and routine dental procedures. If confirmed, this would allow insight for training, evaluating and benchmarking excellence specific to dentistry. By extension, improving mental readiness could increase productivity and morale in the delivery of quality patient care.
- Job-specific operational readiness is critically important for preparedness. For these dentists, the weighted importance for readiness was: physical 23%, technical 28% and mental 49%. Trainees need to comprehend and progress through these readiness competencies to be fully functioning dentists. Training allocations in dentistry have not changed in 40 years. The curriculum in 1980 was the same as today—10% surgery, 10% orthodontics, 10% periodontics, 10% prosthetics and many small topics at 5% each (e.g., paedodontics, oral mucosa, community dentistry and prevention, endodontics, rehabilitation).
- Inter-professional preparedness: Similarities and differences were evident between health professions such as dental, surgical and social services. COVID-19 has shown us that it is possible to shape new activities and reset traditional ways in a changing environment. For example, training in the role of gloves to reduce facial self-touching is a shared strategy across health professions. At a recent US-Europe Congress [31] (Roundtable Discussion, 2021), it was identified that virtual mobility now supports presenting complex and rare cases at international, inter-professional Grand Rounds. All parties would need some common knowledge about each other’s profession (i.e., able to properly convey information in medical doctor’s language and vice versa). Everyone would need to know their role and learn how to communicate well together. Additionally, linking electronic medical records to dental records (i.e., oral cavity and dental database) would be useful and symbolic. Similarly, mental readiness practices may be ideal to share across disciplines such as daily rituals, visualization, de-escalation and patient empowerment.
- Critical mental practices: Certain mental practices may hold more importance in some dental procedures. For example, projecting confidence and focusing under pressure may apply best in particular surgeries. Successful mental practices can therefore be isolated, emphasized and evaluated to improve specific clinical competencies.
- Adaptedtraining tools: Three practical tools found to have beneficial effects in social services and policing [30,32] (McDonald & Hale, 2020; Ontario Police College, 2008, respectively), have been tailored and drafted for dentistry. The adaptation was based on the study findings and review by a subject matter expert in dentistry.
4.1. Personal Profile of Challenging Situations in Dentistry
4.2. Operational Readiness Performance Indicators for Dentistry
4.3. Clinical Training Assessment for Dentistry Trainees
5. Recommendations
- Conduct a comprehensive operational readiness dentistry study: These results provide impetus to conduct interviews with wider and different environments, ages and range of dental specialties. Building on this research, a comprehensive, operational readiness study with highly respected dentists would distinguish dental specializations (vertical training) and augment inter-professional teamwork (horizontal training).
- Update dental curriculum: A new method is needed to reassess the weight of different aspects to reduce over-crowding of the fundamentals. While the overhaul of dental schools described in La Cascada Declaration [12] (Cohen et al., 2013) may be too extreme, these detailed, case-study results may lead to changes. As preliminary results, they give cause to re-examine the current dental-school curriculum, the number of dentists trained and the inter-professional possibilities linked to population health needs.
- Seek inter-professional training opportunities: “Traditional” approaches are shifting in dentistry as: graduates choose group versus sole practices; preventive health measures are imposed during pandemics; and frequent travel restrictions occur between borders. Life-work balance, dentist-patient relationships, ‘team’ work and international mentoring opportunities may all require new strategies to succeed. Finding common grounds for inter-professional preparedness may be valuable for dentistry.
- Enhance recruitment, training and follow-up: The recruitment and selection process could also be further refined to prefer candidates who demonstrate critical mental skills needed to face and cope with the complexities in dentistry. Mental readiness can be integrated into existing dentistry learning objectives. As students acquire new physical abilities and technical know-how, mental skills can be integrated into the curriculum and final assessment. A five-year follow-up by dental schools may help to remind new graduates of the full complement of skills needed and to support them in their practice.
- Test operational tools: The goal of clinical training is to develop a competent, independently functioning dentist who will provide dental services in a safe, courteous and effective manner. To achieve this goal, a trainee must demonstrate competence in performance indicators. A clinical trial with current dental students would create a preliminary step to assess pre- and post-exposure to the Operational Readiness Framework through the three draft tools. Student and instructor feedback would give further insight into effective applications of mental readiness to dentistry.
6. Measures of Potential Impact
- adaptable preparedness strategies for the ever-changing, post-pandemic conditions
- early reflection and practice of “survival” skills in mental readiness
- more holistic integration of “soft skills” and operational procedures into dental education
- early inter-professional collaboration to advance learning, leadership and public-health involvement.
Stakeholder Reactions
Undergraduates—Since COVID, we are requested to be ready in a new way for dental practice. Each of the seven dimensions for mental readiness must now be assessed with a COVID lens. Evaluation and coping are of particular importance in adapting to our new, rapidly evolving rules. Our new dressing sequence has itself become a preparation ritual. Despite these difficulties, maintaining a positive management style for finding solutions remains critical. Commitment now means working with a new satellite team and operators. We need to redefine our focus and distraction control since human touch now has barriers which circumvent what was once possible. Finally, we must find a way to remain confident while adhering to strictly imposed rules.—Forum with 10 Dental Undergraduates, Europe 2021
Hygienist—There is a significant investment that goes into preparing for this profession and many who come out sadly find out that they hate it. Given the intimacy, brevity and sheer responsibility (fiscal, employment, medico-legal, technical), if you don’t like it, it’s going to be a big slog. Early reflection on readiness may help post-grads achieve clearer direction, in addition to happiness, satisfaction and pride in their work. Building confidence, rituals and coping strategies are early survival practices much needed for work–life balance in dentistry.—Seasoned Dental Hygienist, North America, 2021
Seasoned Dentist—‘Manual dexterity’ is one performance indicator that contributors to the overall physical-technical-mental readiness needed for a fully functioning dentist. Knowing the appropriate ratio and offering autonomous mentoring quotes can help schools recognize and promote mind–body-spirit balance at the undergraduate level. Schools encourage a life outside of dentistry albeit through music, cooking, etc. Future research is needed to reflect operational readiness and balance not only in general dentistry but also the demands in the specialties (orthodontics, oral surgery, periodontics, paedodontics).—Experienced Dentist, North America, 2019
Dean—An administrator’s job is to watch for trends and appropriately adapt programs. This research reinforces the need for: early integrating of inter-professional teams, re-examining ‘integrity’ and emphasizing mental readiness. Dentistry today is less about developing a team but rather working in teams. Treating a cleft palate or sleep apnea involves the evolution and collaboration across professional teams of speech therapists, neurologists and surgeons. Integrating first-year dental students with advanced nursing students would be an evidence-based approach to promote learning, leadership and a higher involvement in public health.—Dean of Dentistry, Europe, 2019
7. Limitations of the Study
- The sampling size of seasoned dentists was small and not intended to make inferences to all dentists. Overall transferability of the Operational Readiness Framework for dentistry was considered more important than generalizability. Case studies permit exploration and description to enhance (in this case) the understanding of mental readiness in dentistry, expand the knowledge base and generate hypotheses for future study [33] (Richardson, 1994).
- Selection and method bias: Dentists’ free time for research is limited and difficult to access. While referral sampling was required to allow for this preliminary study, it made it impossible to determine the sampling error. At this time, an in-depth, face-to-face meeting was the best method available to explore this under-researched area for this medical specialty.
8. Strengths of the Study
- The qualitative nature of this research elicited candid conversation to collect comprehensive information and unexpected viewpoints in a new subject matter for dentistry.
- The study design also incorporated measures to quantify the relative importance of physical, technical and mental readiness for a dentist’s overall preparedness.
- The track-record across other high-risk professions of this empirical approach may offer innovative, evidence-based direction for change in the dentistry curriculum.
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Yip, H.K.; Smales, R. Review of competency-based education in dentistry. Br. Dent. J. 2000, 189, 324–326. [Google Scholar] [CrossRef]
- Thammasitboon, K.; Sukotjo, C.; Howell, H.; Karimbux, N. Problem-Based Learning at the Harvard School of Dental Medicine: Self-Assessment of Performance in Postdoctoral Training. J. Dent. Educ. 2007, 71, 1080–1089. [Google Scholar] [CrossRef] [PubMed]
- Greenwood, L.F.; Lewis, D.W.; Burgess, R.C. How competent do our graduates feel? J. Dent. Educ. 1998, 62, 307–313. [Google Scholar] [CrossRef] [PubMed]
- Yiu, C.K.; McGrath, C.; Bridges, S.M.; Corbet, E.F.; Botelho, M.; Dyson, J.; Chan, L. Graduates’ Perceived Preparedness for Dental Practice from PBL and Traditional Curricula. J. Dent. Educ. 2011, 75, 1270–1279. [Google Scholar] [CrossRef]
- Gregorczyk, S.; Bailet, H. Assessing the cultural competency of dental students and residents. J. Dent. Educ. 2008, 72, 1122–1127. [Google Scholar] [CrossRef] [PubMed]
- Hewlett, E.; Davidson, P.; Nakazono, T.; Baumeister, S.; Carreon, D.; Freed, J. Effect of school environment on dental students’ perceptions of cultural competency curricula and preparedness to care for diverse populations. J. Dent. Educ. 2007, 71, 810–818. [Google Scholar] [CrossRef] [PubMed]
- Schönwetter, D.J.; Law, D.; Mazurat, R.; Sileikyte, R.; Nazarko, O. Assessing graduating dental students’ competencies: The impact of classroom, clinic and externships learning experiences. Eur. J. Dent. Educ. 2011, 15, 142–152. [Google Scholar] [CrossRef]
- Collins, W. Trends in dental education. J. Am. Coll. Dent. 1975, 42, 44–50. [Google Scholar]
- Baelum, V.; Luan, W.M.; Chen, X.; Fejerskov, O. A 10-year study of the progression of destructive periodontal disease in adult and elderly Chinese. J. Periodontol. 1997, 68, 1033–1042. [Google Scholar] [CrossRef]
- Fejerskov, O.; Escobar, G.; Jøssing, M.; Baelum, V. A functional natural dentition for all—And for life? The oral healthcare system needs revision. J. Oral Rehabil. 2013, 40, 707–722. [Google Scholar] [CrossRef]
- Norderyd, O.; Koch, G.; Papias, A.; Köhler, A.A.; Helkimo, A.N.; Brahm, C.O.; Lindmark, U.; Lindfors, N.; Mattsson, A.; Rolander, B. Oral health of individuals aged 3–80 years in Jönköping, Sweden during 40 years (1973–2013). II. Review of clinical and radiographic findings. Swed. Dent. J. 2015, 39, 69–86. [Google Scholar]
- Cohen, L.K.; Dahlen, G.; Escobar, A.; Fejerskov, O.; Johnson, N.W.; Manji, F. Why a radical overhaul of dentistry is needed. Indian J. Dent. Res. 2017, 28, 471–474. [Google Scholar] [PubMed]
- FDI World Dental Federation. Optimal Oral Health through Inter-Professional Education and Collaborative Practice, Vision 2020; FDI World Dental Federation: Geneva, Switzerland, 2015; Version 5.1; pp. 1–53. [Google Scholar]
- Lamprecht, R.; Guse, J.; Schimmel, M.; Müller, F.; Heydecke, G.; Reissmann, D. Benefits of combined quantitative and qualitative evaluation of learning experience in a gerodotology course for dental students. BMC Med. Educ. 2020, 20, 281. [Google Scholar] [CrossRef] [PubMed]
- Leung, A.; Fine, P.; Blizard, R.; Tonni, I.; Louca, C. Teacher feedback and student learning: A quantitative study. Eur. J. Dent. Educ. 2020. [Google Scholar] [CrossRef] [PubMed]
- Tonni, I.; Gadbury-Amyot, C.C.; Govaerts, M.; Ten Cate, O.; Davis, J.; Garcia, L.T. Valachovic RW. ADEA-ADEE Shaping the Future of Dental Education III: Assessment in competency-based dental education: Ways forward. J. Dent. Educ. 2020, 84, 97–104. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.-X.; Luk, W.; Arthur, D.; Wong, T. Nursing competencies: Personal characteristics contributing to effective nursing performance. J. Adv. Nurs. 2001, 33, 467–474. [Google Scholar] [CrossRef] [PubMed]
- McDonald, J.; Gyorkos, T. Operational Readiness for conducting global health research abroad. Can. J. Public Health 2016, 107, 387–389. [Google Scholar] [CrossRef]
- McDonald, J.; Dahal, G.; Tyshenko, M.; Sloan, D.; Sharma, S. Operational readiness: Links to Sherpas’ peak performance in tourist mountain-guiding. In Sustainable Livelihood Systems in Nepal; International Union for Conservation of Nature, Nepal Country Office (IUCN Nepal): Kathmandu, Nepal, 2015; pp. 281–308. [Google Scholar]
- McDonald, J.; Orlick, T.; Letts, M. Mental readiness in surgeons and its links to performance excellence in surgery. J. Pediatr. Orthop. 1995, 15, 691–697. [Google Scholar] [CrossRef]
- McDonald, J. Gold Medal Policing: Mental Readiness and Performance Excellence; Sloan Associate Press: New York, NY, USA, 2006. [Google Scholar]
- Krewski, D.; Westphal, M.; Andersen, M.; Paoli, G.; Chiu, W.; Al-Zoughool, M.; Croteau, M.; Burgoon, L.; Cote, I. A framework for the next generation of risk science. Environ. Health Perspect. 2014, 122, 796–805. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Orlick, T.; Partington, J. Mental links to excellence. Sport Psychol. 1988, 2, 105–130. [Google Scholar] [CrossRef]
- Orlick, T. Wheel of Excellence. 2003. Available online: http://www.zoneofexcellence.com/Articles/wheel.htm. (accessed on 30 June 2021).
- DentEd. Advisory Committee on the Training of Dental Practitioners: Competences Required for the Practice of Dentistry in the European Union; DentEd.: Cambridge, UK, 2010; Core knowledge, Section II; pp. 1–4. [Google Scholar]
- Quinn, B.; Field, J.; Gorter, R.; Akota, I.; Manzanares, M.C.; Paganelli, C.; Davies, J.; Dixon, J.; Gabor, G.; Mendes, R.; et al. COVID-19: The immediate response of European academic dental institutions and future implications for dental education. Eur. J. Dent. Educ. 2020, 24, 811–814. [Google Scholar] [CrossRef] [PubMed]
- Chang, T.-Y.; Hong, G.; Paganelli, C.; Phantumvanit, P.; Chang, W.-J.; Shieh, Y.-S.; Hsu, M.-l. Innovation of dental education during COVID-19 pandemic. J. Dent. Sci. 2021, 16, 15–20. [Google Scholar] [CrossRef] [PubMed]
- Duane, B.; Harford, S.; Ramasubbu, D.; Stancliffe, R.; Pasdeki-Clewer, E.; Lomax, R.; Steinbach, I. Environmentally sustainable dentistry: A brief introduction to sustainable concepts within the dental practice. Br. Dent. J. 2019, 226, 292–295. [Google Scholar] [CrossRef]
- Royal College of Dental Surgeons of Ontario. First 125 Years: 1868–1993; Royal College of Dental Surgeons of Ontario: Toronto, ON, Canada, 1993; pp. 1–32. Available online: https://az184419.vo.msecnd.net/rcdso/pdf/RCDSO%20History%20Booklet.pdf (accessed on 30 June 2021).
- McDonald, J.; Hale, K. Mental preparedness for frontline workers in homelessness services in Ottawa, Canada. Int. J. Homelessness 2021, in press. [Google Scholar]
- Roundtable Discussion. Inter-professional education and practice in US/EU point of view. In Proceedings of the 9th Virtual World Congress of Dental Students (Virtual), 5–7 May 2021. [Google Scholar]
- Ontario Police College. Police Trainee Field Training Manual; Queen’s Printer for Ontario: Toronto, ON, Canada, 2008; pp. 1–180. [Google Scholar]
- Richardson, V. Conducting Research on practice. Educ. Res. 1994, 23, 3–10. [Google Scholar] [CrossRef]

{kind=link}
| Readiness Factors | Mean % | Standard Deviation |
|---|---|---|
| Physical Readiness | 23 | 11.39 |
| Technical Readiness | 28 | 13.47 |
| Mental Readiness | 49 | 23.47 |
| Readiness Factors | Dentists | Surgeons | Health Researchers | Social Worker | Police | Olympians |
|---|---|---|---|---|---|---|
| Physical Readiness | 23% | 10% | 18% | 24% | 28% | 38% |
| Technical Readiness | 28% | 41% | 42% | 29% | 32% | 20% |
| Mental Readiness | 49% | 49% | 40% | 47% | 40% | 42% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
McDonald, J.M.; Paganelli, C. Exploration of Mental Readiness for Enhancing Dentistry in an Inter-Professional Climate. Int. J. Environ. Res. Public Health 2021, 18, 7038. https://doi.org/10.3390/ijerph18137038
McDonald JM, Paganelli C. Exploration of Mental Readiness for Enhancing Dentistry in an Inter-Professional Climate. International Journal of Environmental Research and Public Health. 2021; 18(13):7038. https://doi.org/10.3390/ijerph18137038
Chicago/Turabian StyleMcDonald, Judy M., and Corrado Paganelli. 2021. "Exploration of Mental Readiness for Enhancing Dentistry in an Inter-Professional Climate" International Journal of Environmental Research and Public Health 18, no. 13: 7038. https://doi.org/10.3390/ijerph18137038
APA StyleMcDonald, J. M., & Paganelli, C. (2021). Exploration of Mental Readiness for Enhancing Dentistry in an Inter-Professional Climate. International Journal of Environmental Research and Public Health, 18(13), 7038. https://doi.org/10.3390/ijerph18137038