
The Impact of Epidemics and Pandemics on the Mental Health of Healthcare Workers: A Systematic Review




Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources and Search Strategy
2.2. Eligibility Criteria
- Studies reporting the impact of a pandemic/epidemic on mental health outcomes of health care workers.
- Cross-sectional, case–control, and cohort studies. Intervention studies were considered for inclusion only when they had sufficient details about the baseline mental health outcomes.
- Studies were selected if data was from an original study
- Studies had to be published in a peer reviewed journal.
- Only English language studies were included.
- No restrictions were placed on the publication date.
- There was no limit on the geographical location of studies.
2.3. Data Extraction and Quality Appraisal
2.4. Data Analysis and Synthesis
3. Results
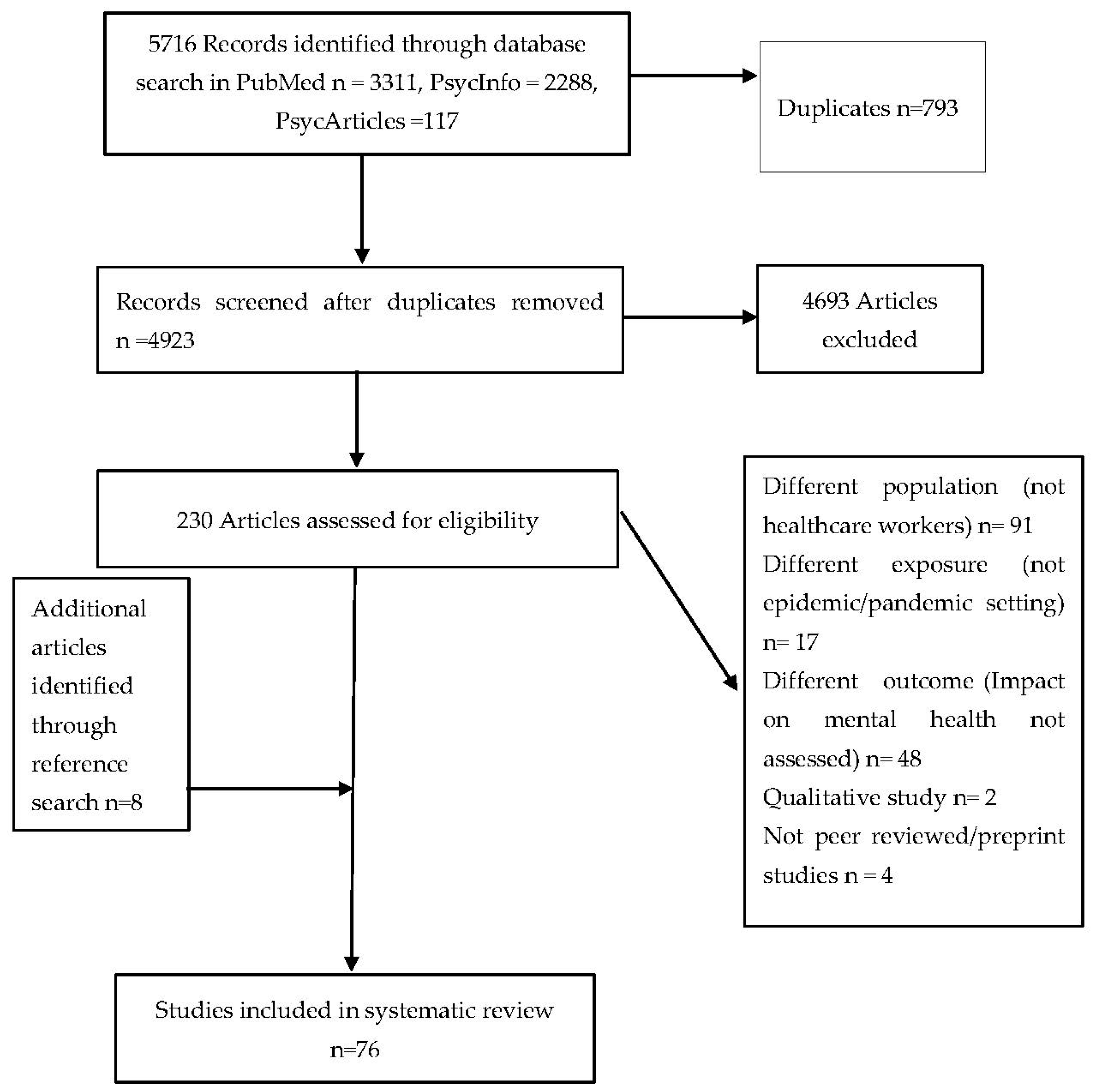
3.1. Study Selection Process
3.2. Characteristics of Selected Studies
3.3. Quality Appraisal
3.4. Commonly Used Mental Health Instruments in This Analysis
3.5. Mental Health Findings
3.5.1. Stress
3.5.2. Anxiety and Fear
3.5.3. Depression
3.5.4. Insomnia and Sleep Quality
3.5.5. Burnout (Emotional Exhaustion)
3.5.6. Stigma
4. Discussion
4.1. Protective Factors
4.2. Strengths and Limitations of This Review
4.3. Recommendations for Future Research and Mental Health Practice
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. Search Strategy

{kind=link}
| Search | Query | Items Found |
|---|---|---|
| #1 | (“health personnel” OR “ healthcare provider*” OR “healthcare worker*” OR “healthcare personnel” OR “ healthcare professional*” OR “healthcare staff” OR doctor OR physician OR “physician assistant*” OR nurse OR “healthcare assistant*” OR “allied health*” OR clinician OR “hospital worker*” OR “hospital staff” OR “hospital employee*”) | 1,923,975 |
| #2 | (epidemic* OR pandemic* OR SARS OR “severe acute respiratory syndrome” OR coronavirus OR MERS OR “middle east respiratory syndrome” OR MERS-CoV OR Ebola OR EVD OR H1N1 OR “influenza type A virus” OR H7N9 OR covid-19 OR 2019-nCoV OR SARS-COV-2 OR “2019 novel coronavirus”) | 220,091 |
| #3 | mental* OR psychiatric* OR psychological* OR resilience OR depression OR emotio* OR anxiety* OR nervous* OR stress* OR PTSD OR “post-traumatic stress disorder” OR insomnia OR “sleep disorder” OR DIMS OR “ disorder of initiating and maintaining sleep” OR burnout OR exhaustion OR fear OR panic OR stigma* OR discrimination OR “mental health” | 3,376,683 |
| #4 | #1 AND #2 AND #3 | 3311 |
| Search | Query | Items Found |
|---|---|---|
| #1 | (“health personnel” OR “ healthcare provider*” OR “healthcare worker*” OR “healthcare personnel” OR “ healthcare professional*” OR “healthcare staff” OR doctor OR physician OR “physician assistant*” OR nurse OR “healthcare assistant*” OR “allied health*” OR clinician OR “hospital worker*” OR “hospital staff” OR “hospital employee*”) | 17,759 |
| #2 | (epidemic* OR pandemic* OR SARS OR “severe acute respiratory syndrome” OR coronavirus OR MERS OR “middle east respiratory syndrome” OR MERS-CoV OR Ebola OR EVD OR H1N1 OR “influenza type A virus” OR H7N9 OR covid-19 OR 2019-nCoV OR SARS-COV-2 OR “2019 novel coronavirus”) | 932 |
| #3 | mental* OR psychiatric* OR psychological* OR resilience OR depression OR emotio* OR anxiety* OR nervous* OR stress* OR PTSD OR “post-traumatic stress disorder” OR insomnia OR “sleep disorder” OR DIMS OR “ disorder of initiating and maintaining sleep” OR burnout OR exhaustion OR fear OR panic OR stigma* OR discrimination OR “mental health” | 158,189 |
| #4 | #1 AND #2 AND #3 | 117 |
| #1 | (“health personnel” OR “ healthcare provider*” OR “healthcare worker*” OR “healthcare personnel” OR “ healthcare professional*” OR “healthcare staff” OR doctor OR physician OR “physician assistant*” OR nurse OR “healthcare assistant*” OR “allied health*” OR clinician OR “hospital worker*” OR “hospital staff” OR “hospital employee*”) | 344,711 |
| #2 | epidemic* OR pandemic* OR SARS OR “severe acute respiratory syndrome” OR coronavirus OR MERS OR “middle east respiratory syndrome” OR MERS-CoV OR Ebola OR EVD OR H1N1 OR “influenza type A virus” OR H7N9 OR covid-19 OR 2019-nCoV OR SARS-COV-2 OR “2019 novel coronavirus” | 41,531 |
| #3 | mental* OR psychiatric* OR psychological* OR resilience OR depression OR emotio* OR anxiety* OR nervous* OR stress* OR PTSD OR “post-traumatic stress disorder” OR insomnia OR “sleep disorder” OR DIMS OR “ disorder of initiating and maintaining sleep” OR burnout OR exhaustion OR fear OR panic OR stigma* OR discrimination OR “mental health” | 2,335,979 |
| #4 | #1 AND #2 AND #3 | 2288 |
Appendix B. Abbreviations in Table of Results
References
- Sim, F.; McKee, M.; Sim, F. Issues in Public Health; McGraw-Hill Education: Maidenhead, UK, 2011; ISBN 978-0-335-24422-5. [Google Scholar]
- WHO. Disease Outbreaks. Available online: http://www.who.int/emergencies/diseases/en/ (accessed on 13 July 2020).
- Levin, P.J.; Gebbie, E.N.; Qureshi, K. Can the health-care system meet the challenge of pandemic flu? Planning, ethical, and workforce considerations. Public Health Rep. 2007, 122, 573–578. [Google Scholar] [CrossRef]
- Lee, S.M.; Kang, W.S.; Cho, A.R.; Kim, T.; Park, J.K. Psychological impact of the 2015 MERS outbreak on hospital workers and quarantined hemodialysis patients. Compr. Psychiatry 2018, 87, 123–127. [Google Scholar] [CrossRef]
- Robert, R.; Kentish-Barnes, N.; Boyer, A.; Laurent, A.; Azoulay, E.; Reignier, J. Ethical dilemmas due to the Covid-19 pandemic. Ann. Intensive Care 2020, 10, 84. [Google Scholar] [CrossRef] [PubMed]
- Rimmer, A. How can I break bad news remotely? BMJ 2020, 369. [Google Scholar] [CrossRef]
- Shortage of Personal Protective Equipment Endangering Health Workers Worldwide. Available online: https://www.who.int/news-room/detail/03-03-2020-shortage-of-personal-protective-equipment-endangering-health-workers-worldwide (accessed on 14 July 2020).
- HSE Library. Bereavement Supports for Frontline Healthcare Staff Following the Death of a Colleague Due to COVID-19? Available online: https://hselibrary.ie/bereavement-supports-for-frontline-healthcare-staff-following-the-death-of-a-colleague-due-to-covid-19/ (accessed on 14 July 2020).
- Bagcchi, S. Stigma during the COVID-19 Pandemic. Lancet Infect. Dis. 2020, 20, 782. [Google Scholar] [CrossRef]
- Ellis-Petersen, H.; Azizur Rahman, S. Indian doctors being evicted from homes over coronavirus fears. The Guardian, 30 March 2020. [Google Scholar]
- Brooks, S.K.; Dunn, R.; Amlôt, R.; Rubin, G.J.; Greenberg, N. A systematic, thematic review of social and occupational factors associated with psychological outcomes in healthcare employees during an infectious disease outbreak. J. Occup. Environ. Med. 2018, 60, 248–257. [Google Scholar] [CrossRef] [Green Version]
- Kisely, S.; Warren, N.; McMahon, L.; Dalais, C.; Henry, I.; Siskind, D. Occurrence, prevention, and management of the psychological effects of emerging virus outbreaks on healthcare workers: Rapid review and meta-analysis. BMJ 2020, 369. [Google Scholar] [CrossRef]
- Vizheh, M.; Qorbani, M.; Arzaghi, S.M.; Muhidin, S.; Javanmard, Z.; Esmaeili, M. The mental health of healthcare workers in the COVID-19 pandemic: A systematic review. J. Diabetes Metab. Disord. 2020, 1–12. [Google Scholar] [CrossRef]
- Muller, A.E.; Hafstad, E.V.; Himmels, J.P.W.; Smedslund, G.; Flottorp, S.; Stensland, S.Ø.; Stroobants, S.; Van de Velde, S.; Vist, G.E. The mental health impact of the Covid-19 pandemic on healthcare workers, and interventions to help them: A rapid systematic review. Psychiatry Res. 2020, 293, 113441. [Google Scholar] [CrossRef]
- Allan, S.M.; Bealey, R.; Birch, J.; Cushing, T.; Parke, S.; Sergi, G.; Bloomfield, M.; Meiser-Stedman, R. The prevalence of common and stress-related mental health disorders in healthcare workers based in pandemic-affected hospitals: A rapid systematic review and meta-analysis. Eur. J. Psychotraumatol. 2020, 11. [Google Scholar] [CrossRef]
- Sanghera, J.; Pattani, N.; Hashmi, Y.; Varley, K.F.; Cheruvu, M.S.; Bradley, A.; Burke, J.R. The impact of SARS-CoV-2 on the mental health of healthcare workers in a hospital setting—A systematic review. J. Occup. Health 2020, 62. [Google Scholar] [CrossRef]
- Shamseer, L.; Moher, D.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: Elaboration and explanation. BMJ 2015, 349. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- The Impact of Epidemics and Pandemics on the Mental Health of Healthcare Workers: A Systematic Review and Narrative Synthesis. Available online: https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=186331 (accessed on 16 August 2020).
- WHO. Definitions: Emergencies. Available online: https://www.who.int/hac/about/definitions/en/ (accessed on 14 September 2020).
- WHO. What Is a Pandemic? Available online: http://www.who.int/csr/disease/swineflu/frequently_asked_questions/pandemic/en/ (accessed on 14 September 2020).
- Martin, J. Critical Appraisal Checklist for Analytical Cross Sectional Studies; Joanna Briggs Institute: Brisbane, Australia, 2017; Volume 7, Available online: https://jbi.global/sites/default/files/2019-05/JBI_Critical_Appraisal-Checklist_for_Analytical_Cross_Sectional_Studies2017_0.pdf (accessed on 16 August 2020).
- Martin, J. Critical Appraisal Checklist for Cohort Studies; Joanna Briggs Institute: Brisbane, Australia, 2017; Volume 7, Available online: https://jbi.global/sites/default/files/2019-05/JBI_Critical_Appraisal-Checklist_for_Cohort_Studies2017_0.pdf (accessed on 16 August 2020).
- Amerio, A.; Bianchi, D.; Santi, F.; Costantini, L.; Odone, A.; Signorelli, C.; Costanza, A.; Serafini, G.; Amore, M.; Aguglia, A. Covid-19 pandemic impact on mental health: A web-based cross-sectional survey on a sample of Italian general practitioners. Acta Bio. Med. Atenei. Parm. 2020, 91, 83–88. [Google Scholar] [CrossRef]
- Cai, H.; Tu, B.; Ma, J.; Chen, L.; Fu, L.; Jiang, Y.; Zhuang, Q. Psychological impact and coping strategies of frontline medical staff in hunan between January and March 2020 during the outbreak of coronavirus disease 2019 (COVID-19) in Hubei, China. Med. Sci. Monit. 2020, 26, e924171-1–e924171-16. [Google Scholar] [CrossRef] [Green Version]
- Chew, N.W.S.; Lee, G.K.H.; Tan, B.Y.Q.; Jing, M.; Goh, Y.; Ngiam, N.J.H.; Yeo, L.L.L.; Ahmad, A.; Ahmed Khan, F.; Napolean Shanmugam, G.; et al. A Multinational, multicentre study on the psychological outcomes and associated physical symptoms amongst healthcare workers during COVID-19 outbreak. Brain Behav. Immun. 2020, 88, 559–565. [Google Scholar] [CrossRef]
- Du, J.; Dong, L.; Wang, T.; Yuan, C.; Fu, R.; Zhang, L.; Liu, B.; Zhang, M.; Yin, Y.; Qin, J.; et al. Psychological symptoms among frontline healthcare workers during COVID-19 outbreak in Wuhan. Gen. Hosp. Psychiatry 2020. [Google Scholar] [CrossRef]
- Hacimusalar, Y.; Kahve, A.C.; Yasar, A.B.; Aydin, M.S. Anxiety and hopelessness levels in COVID-19 pandemic: A comparative study of healthcare professionals and other community sample in Turkey. J. Psychiatr. Res. 2020, 129, 181–188. [Google Scholar] [CrossRef] [PubMed]
- Hu, D.; Kong, Y.; Li, W.; Han, Q.; Zhang, X.; Zhu, L.X.; Wan, S.W.; Liu, Z.; Shen, Q.; Yang, J.; et al. Frontline nurses’ burnout, anxiety, depression, and fear statuses and their associated factors during the COVID-19 outbreak in Wuhan, China: A large-scale cross-sectional study. EClinical Med. 2020, 24, 100424. [Google Scholar] [CrossRef] [PubMed]
- Kang, L.; Ma, S.; Chen, M.; Yang, J.; Wang, Y.; Li, R.; Yao, L.; Bai, H.; Cai, Z.; Xiang Yang, B.; et al. Impact on mental health and perceptions of psychological care among medical and nursing staff in Wuhan during the 2019 novel coronavirus disease outbreak: A cross-sectional study. Brain Behav. Immun. 2020, 87, 11–17. [Google Scholar] [CrossRef] [PubMed]
- Lai, J.; Ma, S.; Wang, Y.; Cai, Z.; Hu, J.; Wei, N.; Wu, J.; Du, H.; Chen, T.; Li, R.; et al. Factors associated with mental health outcomes among health care workers exposed to coronavirus disease 2019. JAMA Netw. Open 2020, 3, e203976. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Ge, J.; Yang, M.; Feng, J.; Qiao, M.; Jiang, R.; Bi, J.; Zhan, G.; Xu, X.; Wang, L.; et al. Vicarious traumatization in the general public, members, and non-members of medical teams aiding in COVID-19 control. Brain Behav. Immun. 2020, 88, 916–919. [Google Scholar] [CrossRef] [PubMed]
- Liang, Y.; Chen, M.; Zheng, X.; Liu, J. Screening for Chinese medical staff mental health by SDS and SAS during the outbreak of COVID-19. J. Psychosom. Res. 2020, 133, 110102. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.-Y.; Yang, Y.; Zhang, X.-M.; Xu, X.; Dou, Q.-L.; Zhang, W.-W.; Cheng, A.S.K. The prevalence and influencing factors in anxiety in medical workers fighting COVID-19 in China: A cross-sectional survey. Epidemiol. Infect. 2020, 148, e98. [Google Scholar] [CrossRef] [PubMed]
- Lu, W.; Wang, H.; Lin, Y.; Li, L. Psychological status of medical workforce during the COVID-19 pandemic: A cross-sectional study. Psychiatry Res. 2020, 288, 112936. [Google Scholar] [CrossRef]
- Mo, Y.; Deng, L.; Zhang, L.; Lang, Q.; Liao, C.; Wang, N.; Qin, M.; Huang, H. Work stress among Chinese Nurses to support wuhan in fighting against COVID-19 epidemic. J. Nurs. Manag. 2020, 28, 1002–1009. [Google Scholar] [CrossRef] [Green Version]
- Qi, J.; Xu, J.; Li, B.-Z.; Huang, J.-S.; Yang, Y.; Zhang, Z.-T.; Yao, D.-A.; Liu, Q.-H.; Jia, M.; Gong, D.-K.; et al. The Evaluation of sleep disturbances for Chinese frontline medical workers under the outbreak of COVID-19. Sleep Med. 2020, 72, 1–4. [Google Scholar] [CrossRef]
- Que, J.; Shi, L.; Deng, J.; Liu, J.; Zhang, L.; Wu, S.; Gong, Y.; Huang, W.; Yuan, K.; Yan, W.; et al. Psychological impact of the COVID-19 pandemic on healthcare workers: A cross-sectional study in China. Gen. Psychiatr 2020, 33. [Google Scholar] [CrossRef] [PubMed]
- Shechter, A.; Diaz, F.; Moise, N.; Anstey, D.E.; Ye, S.; Agarwal, S.; Birk, J.L.; Brodie, D.; Cannone, D.E.; Chang, B.; et al. Psychological distress, coping behaviors, and preferences for support among New York healthcare workers during the COVID-19 pandemic. Gen. Hosp. Psychiatry 2020, 66, 1–8. [Google Scholar] [CrossRef]
- Sun, D.; Yang, D.; Li, Y.; Zhou, J.; Wang, W.; Wang, Q.; Lin, N.; Cao, A.; Wang, H.; Zhang, Q. Psychological impact of 2019 novel coronavirus (2019-NCoV) outbreak in health workers in China. Epidemiol. Infect. 2020, 148, e96. [Google Scholar] [CrossRef] [PubMed]
- Tan, B.Y.Q.; Chew, N.W.S.; Lee, G.K.H.; Jing, M.; Goh, Y.; Yeo, L.L.L.; Zhang, K.; Chin, H.-K.; Ahmad, A.; Khan, F.A.; et al. Psychological impact of the COVID-19 pandemic on health care workers in Singapore. Ann. Intern. Med. 2020. [Google Scholar] [CrossRef] [Green Version]
- Temsah, M.-H.; Al-Sohime, F.; Alamro, N.; Al-Eyadhy, A.; Al-Hasan, K.; Jamal, A.; Al-Maglouth, I.; Aljamaan, F.; Al Amri, M.; Barry, M.; et al. The psychological impact of COVID-19 pandemic on health care workers in a MERS-CoV endemic country. J. Infect. Public Health 2020, 13, 877–882. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Xie, L.; Xu, Y.; Yu, S.; Yao, B.; Xiang, D. Sleep disturbances among medical workers during the outbreak of COVID-2019. Occup. Med. 2020, 70, 364–369. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.; Wang, J.; Luo, C.; Hu, S.; Lin, X.; Anderson, A.E.; Bruera, E.; Yang, X.; Wei, S.; Qian, Y. A Comparison of burnout frequency among oncology physicians and nurses working on the frontline and usual wards during the COVID-19 epidemic in Wuhan, China. J. Pain Symptom Manag. 2020, 60, e60–e65. [Google Scholar] [CrossRef]
- Wu, K.; Wei, X. Analysis of psychological and sleep status and exercise rehabilitation of front-line clinical staff in the fight against COVID-19 in China. Med. Sci. Monit. Basic Res. 2020, 26, e924085. [Google Scholar] [CrossRef] [PubMed]
- Xiao, X.; Zhu, X.; Fu, S.; Hu, Y.; Li, X.; Xiao, J. Psychological impact of healthcare workers in China during COVID-19 pneumonia epidemic: A multi-center cross-sectional survey investigation. J. Affect. Disord. 2020, 274, 405–410. [Google Scholar] [CrossRef] [PubMed]
- Xiaoming, X.; Ming, A.; Su, H.; Wo, W.; Jianmei, C.; Qi, Z.; Hua, H.; Xuemei, L.; Lixia, W.; Jun, C.; et al. The psychological status of 8817 hospital workers during COVID-19 epidemic: A cross-sectional study in Chongqing. J. Affect. Disord. 2020, 276, 555–561. [Google Scholar] [CrossRef]
- Xing, J.; Sun, N.; Xu, J.; Geng, S.; Li, Y. Study of the mental health status of medical personnel dealing with new coronavirus pneumonia. PLoS ONE 2020, 15. [Google Scholar] [CrossRef] [PubMed]
- Zhang, C.; Yang, L.; Liu, S.; Ma, S.; Wang, Y.; Cai, Z.; Du, H.; Li, R.; Kang, L.; Su, M.; et al. Survey of insomnia and related social psychological factors among medical staff involved in the 2019 novel coronavirus disease outbreak. Front. Psychiatry 2020, 11. [Google Scholar] [CrossRef]
- Zhang, S.X.; Liu, J.; Afshar Jahanshahi, A.; Nawaser, K.; Yousefi, A.; Li, J.; Sun, S. At the height of the storm: Healthcare staff’s health conditions and job satisfaction and their associated predictors during the epidemic peak of COVID-19. Brain Behav. Immun. 2020, 87, 144–146. [Google Scholar] [CrossRef]
- Zhu, J.; Sun, L.; Zhang, L.; Wang, H.; Fan, A.; Yang, B.; Li, W.; Xiao, S. Prevalence and influencing factors of anxiety and depression symptoms in the first-line medical staff fighting against COVID-19 in Gansu. Front. Psychiatry 2020, 11. [Google Scholar] [CrossRef] [PubMed]
- Alsubaie, S.; Temsah, M.H.; Al-Eyadhy, A.A.; Gossady, I.; Hasan, G.M.; Al-rabiaah, A.; Jamal, A.A.; Alhaboob, A.A.; Alsohime, F.; Somily, A.M. Middle East respiratory syndrome coronavirus epidemic impact on healthcare workers’ risk perceptions, work and personal lives. J. Infect. Dev. Ctries. 2019, 13, 920–926. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, J.-S.; Lee, E.-H.; Park, N.-R.; Choi, Y.H. Mental health of nurses working at a government-designated hospital during a MERS-CoV outbreak: A cross-sectional study. Arch. Psychiatr. Nurs. 2018, 32, 2–6. [Google Scholar] [CrossRef] [Green Version]
- Oh, N.; Hong, N.; Ryu, D.H.; Bae, S.G.; Kam, S.; Kim, K.-Y. Exploring nursing intention, stress, and professionalism in response to infectious disease emergencies: The experience of local public hospital nurses during the 2015 MERS outbreak in South Korea. Asian Nurs Res. 2017, 11, 230–236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tang, L.; Pan, L.; Yuan, L.; Zha, L. Prevalence and related factors of post-traumatic stress disorder among medical staff members exposed to H7N9 patients. Int. J. Nurs. Sci. 2017, 4, 63–67. [Google Scholar] [CrossRef]
- Ji, D.; Ji, Y.-J.; Duan, X.-Z.; Li, W.-G.; Sun, Z.-Q.; Song, X.-A.; Meng, Y.-H.; Tang, H.-M.; Chu, F.; Niu, X.-X.; et al. Prevalence of psychological symptoms among ebola survivors and healthcare workers during the 2014-2015 ebola outbreak in Sierra Leone: A cross-sectional study. Oncotarget 2017, 8, 12784–12791. [Google Scholar] [CrossRef] [Green Version]
- Bukhari, E.E.; Temsah, M.H.; Aleyadhy, A.A.; Alrabiaa, A.A.; Alhboob, A.A.; Jamal, A.A.; Binsaeed, A.A. Middle east respiratory syndrome coronavirus (MERS-CoV) outbreak perceptions of risk and stress evaluation in nurses. J. Infect. Dev. Ctries 2016, 10, 845–850. [Google Scholar] [CrossRef] [Green Version]
- Khalid, I.; Khalid, T.J.; Qabajah, M.R.; Barnard, A.G.; Qushmaq, I.A. Healthcare workers emotions, perceived stressors and coping strategies during a MERS-CoV outbreak. Clin. Med. Res. 2016, 14, 7–14. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.S.; Choi, J.S. Factors influencing emergency nurses’ burnout during an outbreak of Middle East respiratory syndrome coronavirus in Korea. Asian Nurs Res. 2016, 10, 295–299. [Google Scholar] [CrossRef] [Green Version]
- Lehmann, M.; Bruenahl, C.A.; Addo, M.M.; Becker, S.; Schmiedel, S.; Lohse, A.W.; Schramm, C.; Löwe, B. Acute ebola virus disease patient treatment and health-related quality of life in health care professionals: A controlled study. J. Psychosom. Res. 2016, 83, 69–74. [Google Scholar] [CrossRef]
- Li, L.; Wan, C.; Ding, R.; Liu, Y.; Chen, J.; Wu, Z.; Liang, C.; He, Z.; Li, C. Mental distress among liberian medical staff working at the China ebola treatment unit: A cross sectional study. Health Qual. Life Outcomes 2015, 13, 156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mohammed, A.; Sheikh, T.L.; Gidado, S.; Poggensee, G.; Nguku, P.; Olayinka, A.; Ohuabunwo, C.; Waziri, N.; Shuaib, F.; Adeyemi, J.; et al. An evaluation of psychological distress and social support of survivors and contacts of Ebola virus disease infection and their relatives in Lagos, Nigeria: A cross sectional study—2014. BMC Public Health 2015, 15. [Google Scholar] [CrossRef] [Green Version]
- Liu, X.; Kakade, M.; Fuller, C.J.; Fan, B.; Fang, Y.; Kong, J.; Guan, Z.; Wu, P. Depression after exposure to stressful events: Lessons learned from the severe acute respiratory syndrome epidemic. Compr. Psychiatry 2012, 53, 15–23. [Google Scholar] [CrossRef]
- Matsuishi, K.; Kawazoe, A.; Imai, H.; Ito, A.; Mouri, K.; Kitamura, N.; Miyake, K.; Mino, K.; Isobe, M.; Takamiya, S.; et al. Psychological impact of the pandemic (H1N1) 2009 on general hospital workers in Kobe. Psychiatry Clin. Neurosci. 2012, 66, 353–360. [Google Scholar] [CrossRef]
- Goulia, P.; Mantas, C.; Dimitroula, D.; Mantis, D.; Hyphantis, T. General hospital staff worries, perceived sufficiency of information and associated psychological distress during the A/H1N1 influenza pandemic. BMC Infect. Dis 2010, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, P.; Fang, Y.; Guan, Z.; Fan, B.; Kong, J.; Yao, Z.; Liu, X.; Fuller, C.J.; Susser, E.; Lu, J.; et al. The psychological impact of the SARS epidemic on hospital employees in China: Exposure, risk perception, and altruistic acceptance of risk. Can. J. Psychiatry 2009, 54, 302–311. [Google Scholar] [CrossRef] [PubMed]
- Styra, R.; Hawryluck, L.; Robinson, S.; Kasapinovic, S.; Fones, C.; Gold, W.L. Impact on health care workers employed in high-risk areas during the Toronto SARS outbreak. J. Psychosom. Res. 2008, 64, 177–183. [Google Scholar] [CrossRef] [PubMed]
- Wu, P.; Liu, X.; Fang, Y.; Fan, B.; Fuller, C.J.; Guan, Z.; Yao, Z.; Kong, J.; Lu, J.; Litvak, I.J. Alcohol abuse/dependence symptoms among hospital employees exposed to a SARS outbreak. Alcohol. Alcohol. 2008, 43, 706–712. [Google Scholar] [CrossRef]
- Chen, N.-H.; Wang, P.-C.; Hsieh, M.-J.; Huang, C.-C.; Kao, K.-C.; Chen, Y.-H.; Tsai, Y.-H. Impact of severe acute respiratory syndrome care on the general health status of healthcare workers in Taiwan. Infect. Control. Hosp. Epidemiol. 2007, 28, 75–79. [Google Scholar] [CrossRef]
- Lin, C.; Peng, Y.; Wu, Y.; Chang, J.; Chan, C.; Yang, D. The psychological effect of severe acute respiratory syndrome on emergency department staff. Emerg. Med. J. 2007, 24, 12–17. [Google Scholar] [CrossRef]
- Marjanovic, Z.; Greenglass, E.R.; Coffey, S. The relevance of psychosocial variables and working conditions in predicting nurses’ coping strategies during the SARS crisis: An online questionnaire survey. Int. J. Nurs. Stud. 2007, 44, 991–998. [Google Scholar] [CrossRef]
- Chen, R.; Chou, K.-R.; Huang, Y.-J.; Wang, T.-S.; Liu, S.-Y.; Ho, L.-Y. Effects of a SARS prevention programme in Taiwan on nursing staff’s anxiety, depression and sleep quality: A longitudinal survey. Int. J. Nurs. Stud. 2006, 43, 215–225. [Google Scholar] [CrossRef]
- Fiksenbaum, L.; Marjanovic, Z.; Greenglass, E.R.; Coffey, S. Emotional exhaustion and state anger in nurses who worked during the SARS outbreak: The role of perceived threat and organizational support. Can. J. Community Ment. Health 2006, 25, 89–103. [Google Scholar] [CrossRef]
- Maunder, R.G.; Lancee, W.J.; Balderson, K.E.; Bennett, J.P.; Borgundvaag, B.; Evans, S.; Fernandes, C.M.B.; Goldbloom, D.S.; Gupta, M.; Hunter, J.J.; et al. Long-term psychological and occupational effects of providing hospital healthcare during SARS outbreak. Emerg. Infect. Dis 2006, 12, 1924–1932. [Google Scholar] [CrossRef]
- Chan, S.S.C.; Leung, G.M.; Tiwari, A.F.Y.; Salili, F.; Leung, S.S.K.; Wong, D.C.N.; Wong, A.S.F.; Lai, A.S.F.; Lam, T.H.; Chan, S.S.C.; et al. The Impact of Work-Related Risk on Nurses during the SARS Outbreak in Hong Kong. Fam. Community Health 2005, 28, 274–287. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.-S.; Wu, H.-Y.; Yang, P.; Yen, C.-F. Psychological distress of nurses in Taiwan who worked during the outbreak of SARS. Psychiatr. Serv. 2005, 56, 76–79. [Google Scholar] [CrossRef]
- Grace, S.L.; Hershenfield, K.; Robertson, E.; Stewart, D.E. The occupational and psychosocial impact of SARS on academic physicians in three affected hospitals. Psychosomatics 2005, 46, 385–391. [Google Scholar] [CrossRef] [PubMed]
- Ho, S.M.Y.; Kwong-Lo, R.S.Y.; Mak, C.W.Y.; Wong, J.S. Fear of severe acute respiratory syndrome (SARS) among health care workers. J. Consult. Clin. Psychol 2005, 73, 344–349. [Google Scholar] [CrossRef]
- Koh, D.; Lim, M.K.; Chia, S.E.; Ko, S.M.; Qian, F.; Ng, V.; Tan, B.H.; Wong, K.S.; Chew, W.M.; Tang, H.K.; et al. Risk perception and impact of severe acute respiratory syndrome (SARS) on work and personal lives of healthcare workers in Singapore: What can we learn? Med. Care 2005, 43, 676–682. [Google Scholar] [CrossRef]
- Lee, S.-H.; Juang, Y.-Y.; Su, Y.-J.; Lee, H.-L.; Lin, Y.-H.; Chao, C.-C. Facing SARS: Psychological impacts on SARS team nurses and psychiatric services in a Taiwan general hospital. Gen. Hosp. Psychiatry 2005, 27, 352–358. [Google Scholar] [CrossRef]
- Phua, D.H.; Tang, H.K.; Tham, K.Y. Coping responses of emergency physicians and nurses to the 2003 severe acute respiratory syndrome outbreak. Acad. Emerg. Med. 2005, 12, 322–328. [Google Scholar] [CrossRef]
- Tham, K.; Tan, Y.; Loh, O.; Tan, W.; Ong, M.; Tang, H. Psychological morbidity among emergency department doctors and nurses after the SARS outbreak. Hong Kong J. Emerg. Med. 2005, 12, 215–223. [Google Scholar] [CrossRef]
- Wong, T.W.; Yau, J.K.Y.; Chan, C.L.W.; Kwong, R.S.Y.; Ho, S.M.Y.; Lau, C.C.; Lau, F.L.; Lit, C.H. The psychological impact of severe acute respiratory syndrome outbreak on healthcare workers in emergency departments and how they cope. Eur. J. Emerg. Med. 2005, 12, 13–18. [Google Scholar] [CrossRef] [PubMed]
- Bai, Y.; Lin, C.-C.; Lin, C.-Y.; Chen, J.-Y.; Chue, C.-M.; Chou, P. Survey of stress reactions among health care workers involved with the SARS outbreak. Psychiatr. Serv. 2004, 55, 1055–1057. [Google Scholar] [CrossRef]
- Chan, A.O.M.; Huak, C.Y. Psychological impact of the 2003 severe acute respiratory syndrome outbreak on health care workers in a medium size regional general hospital in Singapore. Occup Med. 2004, 54, 190–196. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chong, M.-Y.; Wang, W.-C.; Hsieh, W.-C.; Lee, C.-Y.; Chiu, N.-M.; Yeh, W.-C.; Huang, O.-L.; Wen, J.-K.; Chen, C.-L. psychological impact of severe acute respiratory syndrome on health workers in a tertiary hospital. Br. J. Psychiatry 2004, 185, 127–133. [Google Scholar] [CrossRef] [Green Version]
- Chua, S.E.; Cheung, V.; Cheung, C.; McAlonan, G.M.; Wong, J.W.S.; Cheung, E.P.T.; Chan, M.T.Y.; Wong, M.M.C.; Tang, S.W.; Choy, K.M.; et al. Psychological effects of the SARS outbreak in Hong Kong on high-risk health care workers. Can. J. Psychiatry 2004, 49, 391–393. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nickell, L.A.; Crighton, E.J.; Tracy, C.S.; Al-Enazy, H.; Bolaji, Y.; Hanjrah, S.; Hussain, A.; Makhlouf, S.; Upshur, R.E.G. Psychosocial effects of SARS on hospital staff: Survey of a large tertiary care institution. CMAJ 2004, 170, 793–798. [Google Scholar] [CrossRef] [Green Version]
- Poon, E.; Liu, K.; Cheong, D.; Lee, C.; Yam, L.; Tang, W. Impact of severe acute respiratory syndrome on anxiety levels of frontline health care workers. Hong Kong Med. J. 2004, 10, 325–330. [Google Scholar]
- Sim, K.; Chong, P.N.; Chan, Y.H.; Soon, W.S.W. Severe acute respiratory syndrome-related psychiatric and posttraumatic morbidities and coping responses in medical staff within a primary health care setting in Singapore. J. Clin. Psychiatry 2004, 65, 1120–1127. [Google Scholar] [CrossRef]
- Sin, S.S.; Huak, C.Y. Psychological impact of the SARS outbreak on a Singaporean rehabilitation department including commentary by Leong, I., Thompson DR. Int. J. Ther. Rehabil. 2004, 11, 417–424. [Google Scholar] [CrossRef]
- Tam, C.W.C.; Pang, E.P.F.; Lam, L.C.W.; Chiu, H.F.K. Severe acute respiratory syndrome (SARS) in Hong Kong in 2003: Stress and psychological impact among frontline healthcare workers. Psychol. Med. 2004, 34, 1197–1204. [Google Scholar] [CrossRef]
- Verma, S.; Mythily, S.; Chan, Y.H.; Deslypere, J.P.; Teo, E.K.; Chong, S.A. Post-SARS psychological morbidity and stigma among general practitioners and traditional Chinese medicine practitioners in Singapore. Ann. Acad. Med. Singap. 2004, 33, 743–748. [Google Scholar]
- Wong, W.C.W.; Lee, A.; Tsang, K.K.; Wong, S.Y.S. How did general practitioners protect themselves, their family, and staff during the SARS epidemic in Hong Kong? J. Epidemiol. Community Health 2004, 58, 180–185. [Google Scholar] [CrossRef] [Green Version]
- Lung, F.-W.; Lu, Y.-C.; Chang, Y.-Y.; Shu, B.-C. Mental symptoms in different health professionals during the SARS attack: A follow-up study. Psychiatr. Q. 2009, 80, 107–116. [Google Scholar] [CrossRef]
- Lancee, W.J.; Maunder, R.G.; Goldbloom, D.S. Prevalence of psychiatric disorders among Toronto hospital workers one to two years after the SARS outbreak. Psychiatr. Serv. 2008, 59, 91–95. [Google Scholar] [CrossRef]
- McAlonan, G.M.; Lee, A.M.; Cheung, V.; Cheung, C.; Tsang, K.W.T.; Sham, P.C.; Chua, S.E.; Wong, J.G.W.S. Immediate and sustained psychological impact of an emerging infectious disease outbreak on health care workers. Can. J. Psychiatry 2007, 52, 241–247. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Su, T.-P.; Lien, T.-C.; Yang, C.-Y.; Su, Y.L.; Wang, J.-H.; Tsai, S.-L.; Yin, J.-C. Prevalence of psychiatric morbidity and psychological adaptation of the nurses in a structured SARS caring unit during outbreak: A prospective and periodic assessment study in Taiwan. J. Psychiatr. Res. 2007, 41, 119–130. [Google Scholar] [CrossRef]
- Bardhan, R.; Heaton, K.; Davis, M.; Chen, P.; Dickinson, D.A.; Lungu, C.T. A Cross sectional study evaluating psychosocial job stress and health risk in emergency department nurses. Int. J. Environ. Res. Public Health 2019, 16, 3243. [Google Scholar] [CrossRef] [Green Version]
- Sok, S.; Sim, H.; Han, B.; Park, S.J. Burnout and related factors of nurses caring for DNR patients in intensive care units, South Korea. Int. J. Environ. Res. Public Health 2020, 17, 8899. [Google Scholar] [CrossRef] [PubMed]
- González-Cabrera, J.M.; Fernández-Prada, M.; Iribar, C.; Molina-Ruano, R.; Salinero-Bachiller, M.; Peinado, J.M. Acute stress and anxiety in medical residents on the emergency department duty. Int. J. Environ. Res. Public Health 2018, 15, 506. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wright, K.B. Researching internet-based populations: Advantages and disadvantages of online survey research, online questionnaire authoring software packages, and web survey services. J. Comput. Mediat. Commun. 2005, 10. [Google Scholar] [CrossRef]
| Study (Year)/Country | Disease Outbreak | Participants (Setting) | Mental Health Outcome Measures (Instrument) | Main Findings |
|---|---|---|---|---|
| Amerio et al. (2020) [23] Italy | COVID-19 Epidemic | N = 131 General Practitioners (General Practice) | Depression (PHQ-9) Anxiety (GAD-7) Insomnia (ISI) Health Related Quality of Life HrQoL (SF-12) | 22 9%: PHQ-9 ≥ 10 moderate to severe depression and 77.1%: PHQ-9 ≤ 10 Mild to moderate depression Physicians with moderate to severe depression had higher severity for anxiety and insomnia and poorer HrQoL. Physicians with moderate to severe depression perceived less adequate PPE |
| Cai et al. (2020) [24] China | COVID-19 Pandemic | N = 534 HCWs (Hospital) | Emotions, factors that increase stress, factors that reduce stress, coping strategies (self-designed questionnaire) | Medical staff were anxious regarding their safety and the safety of their families and reported adverse psychological effects from reports of mortality from COVID-19 infection. |
| Chew et al. (2020) [25] Singapore and India | COVID-19 Pandemic | N = 906 HCWs. 480 from Singapore and 426 from India (Hospital) | Depression, anxiety, and stress (DASS-21) Psychological distress and PTSD (IES) | 15.7% participants had anxiety. 10.6% had depression. 5.2% had stress. There was no difference in psychological outcomes between study participants from the two countries. The presence of physical symptoms was associated with higher mean scores in the IES-R, DASS-21 scales |
| Du et al. (2020) [26] China | COVID-19 Pandemic | N = 134 HCWs 60 Wuhan vs. 74 Outreach (Hospital) | Depression (BDI-II) Anxiety (BAI) Stress (PSS) | 12.4% Depressive symptoms (BDI-II scores ≥ 14) 20.1% Anxiety symptoms (BAI scores ≥ 8) 59.0% moderate to severe stress (PSS scores ≥14) Depression and anxiety higher in Wuhan vs. outreach workers Depression and anxiety higher in females and those having poor family support. |
| Hacimusalar et al. (2020) [27] Turkey | COVID-19 Pandemic | N = 2156 1121 HCWs vs. 1035 non-HCWs (society/social media) | State Trait Anxiety Scale (STAI) Hopelessness (BHS) | The hopelessness and state anxiety levels of HCWs were higher than non-HCWs. Nurses’ anxiety and hopelessness levels were higher than doctors and other HCWs. Anxiety and hopelessness levels were higher in females, those living with a high-risk individual at home, those with difficulty in caring for their children, those with increased working hours and those whose income decreased |
| Hu et al. (2020) [28] China | COVID-19 Pandemic | N = 2014 nurses (Hospital) | Burnout (MBI) Anxiety (SAS) Depression (SDS) Fear (FS-HPs) | Burnout: High burnout during work Anxiety: 27.1% Mild, 11.0% Moderate, 3.3% Severe Depression: 32.8% Mild, 9.6% Moderate, 1.1% Severe Fear:28% Moderate, 36.2% High HCWs who had low self-efficacy and did not have family and social support had worse mental health outcomes |
| Kang et al. (2020) [29] China | COVID-19 Pandemic | N = 994 183 Doctors and 811 Nurses (hospital) | Depression (PHQ-9) Anxiety (GAD-7) Insomnia (ISI) Distress (IES) | 36% had subthreshold mental health disturbances (mean PHQ9: 2.4, GAD-7: 1.5, ISI: 2.8, IES-R: 6.1), 34.4% had mild disturbances (mean PHQ-9: 5.4, GAD-7: 4.6, ISI: 6.0, IES-R: 22.9), 22.4% had moderate disturbances (mean PHQ-9: 9.0, GAD-7: 8.2, ISI: 10.4, IES-R: 39.9) 6.2% had severe disturbances (mean PHQ-9: 15.1, GAD-7: 15.1, ISI: 15.6, IES-R: 60.0) Women had more psychological burden than men |
| Lai et al. (2020) [30] China | COVID-19 Pandemic | N = 1257 764 Nurses 493 Doctors (Hospital) | Depression (PHQ-9) Anxiety (GADS-7) Insomnia (ISI-7) Distress (IES) | 50.4% Depression, 44.6% Anxiety, 34.0% Insomnia, 71.5% Distress Nurses had more severe degrees of mental health symptoms than other HCWs Females had worse mental health symptoms compared to men. Frontline HCWS had higher levels of mental health symptoms compared to second line workers. HCWS in Wuhan had more distress compared to HCWs outside Wuhan and outside Hubei province |
| Li et al. (2020) [31] China | COVID-19 Pandemic | N = 526 nurses and 214 general public 234 frontline nurses 292 non frontline nurses (Hospital) | Vicarious traumatization (Self-developed questionnaire) | Vicarious traumatization scores for non-front-line nurses were significantly higher than those of front-line nurses. Vicarious traumatization scores of the general public were significantly higher than those of the front-line nurses. No significant difference was noted in vicarious traumatization scores between the general public and non-front-line nurse |
| Liang et al. (2020) [32] China | COVID-19 Pandemic | N = 56 HCWs (Hospital) | Anxiety (SAS) Depression (SDS) | Several staff were experiencing clinically significant depressive and anxiety symptoms. |
| Liu et al. (2020) [33] China | COVID-19 Pandemic | N = 512 HCWs (Hospital) | Anxiety (SAS) | 12.5% Anxiety prevalence Anxiety score was significantly higher among the medical staff treating confirmed cases vs. those who had not. Staff from Hubei province had higher anxiety compared to staff from other parts of China |
| Lu et al. (2020) [34] China | COVID-19 Pandemic | N = 2299 HCWs (hospital) | Fear (NRS) Anxiety (HAMA) Depression (HAMD) | Medical staff experienced more fear, anxiety, and depression compared to administrative staff. Front line medical staff in direct contact with COVID-19 patients in the respiratory, emergency, infectious disease, and ICU departments had higher scores of fear, anxiety, and depression compared to those who did not have contact with infected patients. Lack of PPE, loneliness from being isolated from family and loved ones worsened anxiety and depression |
| Mo et al. (2020) [35] China COVID-19 Pandemic | COVID-19 Pandemic | 180 nurses (Hospital) | Stress (SOS) Anxiety (SAS) | Nurses’ anxiety scores were significantly higher than the national standard scores (32.19 vs. 29.78) Anxiety scores were positively correlated to total stress load. Being an only child in their family and more working hours a week predicted higher levels of anxiety and stress. |
| Qi et al. (2020) [36] China | COVID-19 Pandemic | N = 1306 medical workers 801 FMW vs. 505 non-FMW (hospital) | Sleep quality (PSQI) Insomnia (AIS) Anxiety (VAS) Depression (VAS) | FMW had a higher prevalence of sleep disturbances PSQI > 6 compared to non FMW (78.4% vs. 61.0%) FMW had a higher prevalence of sleep disturbances AIS > 6 compared to non FMW (51.7% vs. 31.6%) FMW had higher depression and anxiety scores compared to non FMW |
| Que et al. (2020) [37] China | COVID-19 Pandemic | N = 2285 HCWs (Hospital) | Anxiety (GAD-7) Depression (PHQ-9) Insomnia (ISI) | 56.59% Overall psychological problems 46.04% Anxiety 44.37% Depression 28.75% Insomnia Frontline HCWs had a higher risk of anxiety, insomnia and overall psychological problems compared to non-frontline HCWs. Highest prevalence of anxiety and insomnia was observed in nurses |
| Shechter et al. (2020) [38] USA | COVID-19 Pandemic | N = 657 HCWs (Hospital) | PTSD (PC-PTSD) Psychological (PHQ-2) Depression (GAD-2) Insomnia (ISI) Sleep quality (PSQI) | 57% PTSD symptoms 48% depressive symptoms 33% anxiety symptoms 26% reported severe or very severe sleep problems. Nurses were more likely than attending physicians to screen positive for stress, depression, anxiety, and sleep problems. Lack of national guidelines and lack of adequate PPE were major stressors. 59% Physical exercise was the most common coping behavior. 33% accessed a therapist with online self-guided counselling. Women reported more severe symptoms compared to men |
| Sun et al. (2020) [39] China | COVID-19 Pandemic | N = 442 HCWs (hospital) | Distress (IES) Distress (2019-nCov impact questionnaire) | Quarantined HCWs experienced the most distress. Females had more distress compared to males. Older HCWs ≥ 56 years old experienced more distress compared to younger HCWs ≤ 25 years old |
| Tan et al. (2020) [40] Singapore | COVID-19 Pandemic | N = 470 296 Medical vs. 174 non-medical HCWs (Hospital) | Depression, Anxiety and Stress (DASS-21) Distress (IES-R) | 14.5% anxiety, 8.9% depression 6.6% stress 7.7% PTSD symptoms Anxiety and distress were significantly higher among nonmedical HCWs that the medical personnel |
| Temsah et al. (2020) [41] Saudi Arabia | COVID-19 Pandemic | N= 582 HCW (hospital) | Anxiety (GAD-7) Worry (1–5 worry rating scale) | 68.25% mild anxiety, 20.8% moderate anxiety, 2.9% very high anxiety 41.1% were more stressed about COVID than MERS-CoV. The most frequent concern was transmitting the infection to family and friends than to themselves. |
| Wang et al. (2020) [42] China | COVID-19 Pandemic | N = 123 48 Doctors 75 Nurses (Children’s hospital) | Sleep quality (PSQI) Anxiety (SAS) Depression (SDS) | 38% Sleep disturbance 7% Anxiety 25% Depression Sleep disturbance associated factors: Being an only child Exposure to COVID-19 patients Depression |
| Wu et al. (2020) [43] China | COVID-19 Pandemic | N = 190 HCWs 96 FL (frontline) 94 UW (usual ward) | Burnout (MBI) | The group working on the FLs had a significantly lower frequency of burnout (13% vs. 39%) and were less worried about being infected compared with the UW group. The possible explanation for this unexpected trend was FL HCWs had received timely and accurate information hence they had a high sense of control of their situation |
| Wu and Wei (2020) [44] China | COVID-19 Pandemic | N = 120 60 cases (COVID designated hospitals) 60 controls (non-COVID designated hospital | Sleep quality (PSQI) Anxiety (SAS) Depression (SDS) General symptoms (SCL-90) PTSD (PCL-C) | Poor sleep quality, anxiety, depression, and general health symptoms were higher among cases (frontline workers in COVID designated hospitals) compared to the controls. Cases had higher levels of anxiety, depression, and insomnia compared to the controls. |
| Xiao et al. (2020) [45] China | COVID-19 Pandemic | N = 958 HCWs (Hospital) | Anxiety And depression (HAD) Stress (PSS) | 55.1% psychological stress 54.2% anxiety 58% depression Stress, Anxiety and Depression levels related to: Female gender Exposure to confirmed cases |
| Xiaoming et al. (2020) [46] China | COVID-19 Pandemic | N = 8817 HCWs (Hospital) | Depression (PHQ-9) Anxiety (GAD-7) Suicidal and self-harm ideation (SSI) | 30.2% Depression, 20.7% Anxiety, 46.2% Somatic symptoms Risk factors of psychological impact: female, single, Tujia minority, low educational background, county hospital, need for psychological assistance, no confidence, ignorance about the epidemic, willingness to attend parties, and poor self-rated health condition |
| Xing et al. (2020) [47] China | COVID-19 Pandemic | N = 548 HCWs (Hospital) | Mental health status (SCL-90) | The overall mean SCL90 score of somatization, obsessive-compulsive, anxiety, phobic anxiety, and psychoticism was much higher in the HCWS compared to the national general population (norm group) |
| Zhang et al. (2020) [48] China | COVID-19 Pandemic | N = 1563 HCWs (hospital) | Insomnia (ISI) Anxiety (GAD) Depression (PHQ-9) Psychological response (IES) | 36.1% insomnia symptoms Insomnia symptoms associated with: Lower education, Being a doctor, Female sex Currently working in an isolation unit Worried about being infected. Perceived lack of helpfulness Very strong uncertainty regarding Effective disease control |
| Zhang et al. (2020) Iran [49] | COVID-19 Pandemic | N = 304 HCWs (hospital) | Distress (K6) (SF-12) Depression (PHQ-12) | 28.0% Anxiety, 30.6% Depression, 20.1% Distress Older workers better mental but not physical health Females had more distress and depression. HCWs at private institutions had better mental health than those at public institutions. PPE access predicted better physical, mental health, and less distress |
| Zhu et al. (2020) [50] China | COVID-19 Pandemic | N = 165 HCWs (hospital) | Anxiety (SAS) Depression (SDS) Coping (SCSQ) | Nurses had more Anxiety symptoms compared to doctors (27.9% vs. 11.4%) Risk factors Anxiety—History of depression or anxiety Depression—Female |
| Alsubaie et al. (2019) [51] Saudi Arabia | MERS-CoV Epidemic | N =516 HCWs (hospital) | Knowledge, anxiety (self-developed questionnaire) | The mean anxiety score was the same for physicians, nurses, and technicians. Non-physicians expressed higher levels of anxiety toward the risk of transmitting MERS-CoV to their families |
| Park et al. (2018) [52] Korea | MERS-CoV Epidemic | N = 187 Nurses | Overall health status (SF-36) Stigma (self) Stress (PSS-10) | Greater stigma was directly associated with worse mental health. Hardiness was inversely related to mental health via stress |
| Oh, et al. (2017) [53] South Korea | MERS-CoV Epidemic | N = 313 nurses (hospital) | Stress (stress questionnaire) | The group exposed to MERS confirmed or suspected cases experienced more stress as compared to those who had not exposed to it. Prior outbreak nursing experience had a protective effect |
| Tang et al. (2017) [54] China | H7N9 Epidemic | N = 102 26 Doctors, 62 Nurses and 14 Interns (Hospital) | PTSD (PCL-C) | 20.59% PTSD symptoms Higher scores: Nurses Female Low professional title Frequent contact with patients Aged between 20 years and 30 years. Less than three years of work experience No outbreak training or related experience |
| Ji et al. (2017) [55] Sierra Leone (SL) | Ebola Epidemic | N =143 59 SL medical staff 21 SL logistic staff, 22 SL medical students, 41 Chinese medical staff, 18 EVD survivors. (hospital) | Psychological Symptoms (SCL-90-R) | The order of psychological symptoms from high to low was EVD survivors, SL medical staff, SL logistic staff, SL medical students, and Chinese medical staff. Psychological symptoms were the highest in EVD survivors and the lowest in Chinese medical staff. Mental state of Chinese medical staff was the same at arrival and before leaving. |
| Bukhari et al. (2016) [56] Saudi Arabia | MERS-CoV Epidemic | N = 386 HCWs (hospital) | Perception of exposure, perceived risk of infection and distress (IES) | Worry about contracting MERS-CoV: 7.8% extremely worried, 20.5% very worried. Worry about transmitting MERS-CoV to family members: 12.2% extremely worried, 21.0% very worried. Females were more worried than males |
| Khalid et al. (2016) [57] Saudi Arabia | MERS-CoV Epidemic | N = 117 (Hospital) | Stress and coping strategies (Self-developed questionnaire) | 96% were stressed by seeing colleagues contracting the infection, being intubated for respiratory failure, and caring for these sick colleagues. 94% were worried about transmitting MERS-CoV to family and friends. 96% were nervous and scared. Following strict personal protective measures was the most common coping strategy |
| Kim and Choi (2016) [58] Korea | MERS-CoV Epidemic | N= 215 nurses (Hospital) | Burnout (OLBI) Stress (Parker and DeCotiis) Fear (self-developed scale) | Burnout was higher in those who had nursed MERS-CoV infected or suspected patients than those who did not. Job stress was the biggest influencing factor of burnout. Poor hospital resources for treatment of MERS-CoV and poor support from family and friends increased burnout |
| Lehmann et al. (2016) [59] Germany | Ebola Epidemic | N = 86 HCWs group1: internal medicine ward group2: ebola treatment ward group3: laboratory (hospital) | Health-related quality of life (SF-12) Anxiety (GAD-7) Depression (PHQ-9) | No significant differences in HrQoL, subjective risk of infection, and most other psychosocial variables. Ebola patient treatment group had higher levels of social isolation than both other groups. The best predictors of poor physical and mental HrQoL were perceived lack of knowledge about the Ebola virus disease and fatigue |
| Li et al. (2015) [60] Liberia | Ebola Epidemic | N = 52 16 nurses and 13 cleaners (hospital) | Psychological status (SCL90-R) (PST) Distress (PSDI) | Mental distress among participants was not very serious. Cleaners had higher levels of obsessive compulsive, anxiety, positive symptom total and phobic anxiety vs. Treatment staff. Males had more interpersonal sensitivity and paranoid ideation than females |
| Mohammed et al. (2015) [61] Nigeria | Ebola Virus Disease (EVD) Epidemic | N = 117 (45 HCWs) (community) | Psychological distress (GHQ) Social Support (OSSS) | Non HCWs had higher levels of distress compared to HCWs. Losing a relation to the EVD outbreak was associated with high levels of distress. |
| Liu et al. (2012) China [62] | SARS Epidemic | N = 549 HCWs (Hospital) | Depression (CES-D) Stress (IES) Trauma exposure (self-developed questionnaire) | Depression: 7.2% Mild, 14.0% Moderate, 8.8%High Being single, females, history of quarantine, history of other traumatic events before SARS, and perceived SARS-related risk level during the outbreak increased the odds of having a high level of depressive symptoms 3 years later. High stress during and after the outbreak was associated with high current depressive symptoms. Altruistic acceptance of risk reduced depressive symptoms |
| Matsuishi et al. (2012) [63] Japan | H1N1 Pandemic | N = 1625 HCWs (hospital) | Stress (IES) | Workers in high-risk work environments had higher stress and exhaustion than did workers in low-risk work environments. Total stress score of nurses was higher than that of doctors. HCWs in their 50s felt more exhaustion as compared with workers in their 20s |
| Goulia et al. (2010) [64] Greece | A/H1N1 Pandemic | N = 436 (Hospital) | Anxiety (Self-developed questionnaire) Distress (GHQ-28) | 20.7% mild to moderate psychological distress (GHQ-28 > 5) 6.8% severe psychological distress (GHQ-28 > 11) 56.7% moderately high anxiety The most frequent concern was infection of family and friends and the health consequences of the disease. Nurses had highest distress compared to other HCWs |
| Wu et al. (2009) [65] China | SARS Epidemic | N = 549 (hospital) | Psychological distress (IES) Work exposure, exposure to traumatic events, Fear | 10% had post-traumatic symptoms. Altruistic acceptance of risk was negatively related to PTS. High PTS symptoms associated with: History of quarantine, age under 50 years, high levels of exposure to SARS patients, high perceived SARS related risk levels, higher levels of current fear of SARS |
| Styra et al. (2008) [66] Canada | SARS Epidemic | N = 248 HCWs 88 Low Risk vs. 160 High Risk (hospital) | Self-developed questionnaire | High risk HCWs experienced greater distress Factors that cause distress (a) perception of risk to themselves, (b) impact of SARS crisis on their work life (c) depressive affect (d) working in a high-risk unit (e) HCWs who cared for only one SARS patient experienced more post-traumatic stress symptoms compared to those caring for multiple SARS patients |
| Wu et al. (2008) [67] China | SARS Epidemic | N = 549 HCWs (hospital) | Depression (CES-D) Alcohol abuse/dependence (NHSDA) Distress (IES-R) | 19% of the hospital employees had at least one alcohol use-related symptom, while <5% had two or more symptoms. Alcohol use related symptoms higher in: Male Age between 36 and 50, Low educational levels Upper-middle level family income levels Units with high levels of exposure to SARS Quarantined during the SARS outbreak. |
| Chen et al. (2007) [68] Taiwan | SARS Epidemic | N = 90 HCWs 82 control subjects (hospital) | General health status (MOS SF-36) | SARS HCWs had low scores vs. control group, for vitality, social functioning, and mental health. The HCWs social functioning, role emotional, and role physical subscales significantly improved after self-quarantine and off-duty shifts. |
| Lin et al. (2007) [69] Taiwan | SARS Epidemic | N = 92 HCWs (emergency department vs. psychiatry ward) (Hospital) | Psychological status (DTS-C) (CHQ-12) | 19.3% had symptoms of PTSD (DTS-C scores >40) 47.78% had minor psychiatric morbidity (CHQ-12 scores >3) Emergency department staff had higher psychiatric morbidity, and experienced PTSD symptoms more often and more severely than psychiatry ward staff. |
| Marjanovic et al. (2007) [70] Canada | SARS Epidemic | N = 333 nurses (hospital) | Burnout (MBI) Anger (STAXI) Organizational support (SPOS) Trust in equipment/infection control, avoidance, and vigor (self-developed) | Higher levels of vigor, organizational support, and trust in equipment/infection control initiative decreased avoidance behavior, burnout, and state anger. Lower levels of contact with SARS patients, and lesser time spent in quarantine decreased avoidance behavior, burnout, and state anger. |
| Cheng et al. (2006) Taiwan [71] | SARS Epidemic | N = 116 nurses (hospital) | Anxiety (SAS) Depression (SDS) Sleep quality (PSQI) | Moderate anxiety, Moderate depression, Moderate poor sleep quality |
| Fiksenbaum et al. (2006) [72] Canada | SARS Epidemic | 333 nurses (hospital) | Perceived SARS threat (self-developed questionnaire) Emotional exhaustion (MBI-GS) State anger (STAXI) | Nurses who had contact with SARS patients. - higher levels of perceived SARS threat, - higher levels of emotional exhaustion - Higher levels of state anger Higher levels of organizational support predicted lower perceived SARS threat, emotional exhaustion, and state anger. |
| Maunder et al. (2006) [73] Canada SARS Epidemic | SARS Epidemic | N = 769 73.5% nurses, 8.3% clerical, 2.9% physicians, 2.3% respiratory therapists, 12.9% others HCWs (hospital) | Stress (IES) Distress (K10) Burnout (MBI) Increase in smoking, drinking alcohol, Stigma, job stress, (WCQ), Toronto HCWs vs. Hamilton HCWs | Toronto hospitals treated SARS patients. Hamilton hospitals did not treat SARS patients. Toronto HCWs reported significantly higher levels of burnout, psychological distress and post-traumatic stress compared to Hamilton HCWs. Toronto HCWs had an increase in smoking and drinking alcohol and other behaviors that can interfere with work and relationship |
| Chan SSC et al. (2005) [74] Hong Kong | SARS Epidemic | N = 1470 nurses (hospital) | General health status, anxiety, and stress (SARS NSQ) | 52.6–63.5% considered their general health to be good. 68.3–80.1% nurses always/often perceived stress from the SARS epidemic. 85.9–95.6% nurses perceived their stress came from work. |
| Cheng et al. (2005) Taiwan [75] | SARS Epidemic | N = 184 nurses 85 high risk group 30 conscripted from low to high-risk group 69 control group (hospital) | Stress (IES) Psychiatric morbidity (SCL-90-R) | 11% had stress reaction syndrome. Of these, 17% high-risk group 10% conscripted group 2% control group High risk group had higher stress and psychiatric morbidity than to the control group. Conscripted group had higher stress and psychiatric morbidity than to the control group and high-risk group. |
| Grace et al. (2005) [76] Canada | SARS Epidemic | N = 193 physicians (Hospital) | Psychological distress and stigma (Self-designed questionnaire) | Psychological distress: Physicians providing direct care to SARS patients (45.7%) Physicians not providing direct care to SARS patients (17.7%) Stigma 36% |
| Ho et al. (2005) [77] Hong Kong | SARS Epidemic | N = 179 Sample 1: (N= 82) during peak of epidemic. Sample 2: (N = 97) HCWs who recovered from SARS (hospital) | Fear (SFS) Self-Efficacy (SES) PTSD (IES) | Fear Sample 1: fear related to infection. Sample 2: fear about death, discrimination, quarantine, and side effects of SARS treatment. Self-efficacy Sample 1: low self-efficacy related to more fear. Sample 2: low self-efficacy related to insecurity and instability. PTSD Sample 2: SARS-related fears strongly related to PTSD |
| Koh et al. (2005) [78] Singapore | SARS Epidemic | N = 10,511 (Hospital) | Stress (IES) Perception of risk and stigma (self-developed questionnaire) | 76% perceived a great personal risk of falling ill with SARS. 56% of clinical staff in contact with SARS patients had increased work stress. 53% experienced increase in workload 49% experienced social stigmatization 31% experienced ostracism by family members |
| Lee et al. (2005) [79] Taiwan | SARS Epidemic | N = 26 nurses (Hospital) | Stress and coping strategies (self-developed SARS team questionnaire) | 92% stressed about being negligent and endangering co-workers, 92% stressed about frequent modification of infection control procedures. 92% stressed about the uncertainty of when the epidemic will be under control. 89% stressed about inflicting SARS on family members. Taking protective measures and actively acquiring more information were the most common coping strategies. Adequate PPE and reasonable staffing/shift were motivating factors to work during the outbreaks |
| Phua et al. (2005) [80] Singapore | SARS Epidemic | N = 96 HCWS (hospital) | Coping (COPE) Psychiatric morbidity (GHQ) Stress (IES) | 17.7% psychiatric morbidity (IES ≥26) 18.8% psychiatric morbidity (GHQ ≥ 5) Nurses reported higher psychiatric morbidity compared to physicians. |
| Tham et al. (2005) [81] China | SARS Epidemic | N = 99 41 doctors 58 nurses (Hospital) | Post event morbidity (IES) Psychiatric morbidity (GHQ) | 17.7% Post-traumatic stress morbidity (IES ≥ 26) 18.8% Psychiatric morbidity (GHQ 28 ≥ 5) Nurses had higher IES and psychiatric morbidity than the doctors. Females had higher IES and psychiatric morbidity than the males |
| Wong et al. (2005) [82] Hong Kong | SARS Epidemic | N = 466 HCWs (Hospital) | Distress (Self-designed questionnaire) Coping strategies (COPE) | Distress level was highest for nurses, followed by doctors and HCA. The overall distress level was related to: Vulnerability/loss of control, Health of self Health of family and others, Changes in work, being isolated. Frequently adopted coping strategies were acceptance, active coping, and positive framing |
| Bai et al. (2004) [83] Taiwan | SARS Epidemic | N = 338 218 HCWs and 79 administrative personnel (hospital) | Stress (SARS-related stress reactions questionnaire) | 5% acute stress disorder 20% felt stigmatized and rejected in their neighborhood. 9% HCWs reported reluctance to work or had considered resignation. Quarantine increased stress. HCWs reported more insomnia, exhaustion, and uncertainty about the frequent modifications to infection control procedures compared to administrative staff |
| Chan and Huak (2004) [84] Singapore | SARS Epidemic | N = 661 Doctors and nurses (hospital) | Psychiatric caseness (GHQ-28) PTSD (IES) | 27% had GHQ-28 score ≥ 5, indicating presence of psychiatric symptoms. 20% had IES scores ≥ 30, indicating the presence of post-traumatic stress disorder (PTSD). Doctors were 1.6 times more likely to experience psychiatric symptoms compared with the nurses. Marital status: Single HCWs were 1.4 times more likely to experience psychiatric symptoms compared with married HCWs. |
| Chong et al. (2004) [85] Taiwan | SARS Epidemic | N = 1257 (Hospital) | Psychiatric morbidity (CHQ) | Psychiatric morbidity 75.3% Those who were responsible for the care of SARS patients manifested higher rates of psychiatric morbidity. Females had greater psychiatric morbidity than men |
| Chua et al. (2004) [86] Hong Kong | SARS Epidemic | N = 271 HCWs and N = 342 healthy control subjects | Stress (PSS-10) | Stress levels were raised in both groups (PSS-10 ≥ 18), but there were no group differences. PSS-10 HCWs: 18.6; PSS-10 Controls: 18.3 HCWs had more protective psychological effects vs. controls |
| Nickell et al. (2004) [87] Canada | SARS Epidemic | N = 2001 HCWs N = 510 GHQ | Stress (GHQ-12) | 29% had emotional distress. More nurses experienced emotional distress compared to other professionals. Emotional distress was significantly increased in those HCWs who had part-time employment status. Higher levels of concern for self and family were associated with a higher perception of risk of death from SARS |
| Poon et al. (2004) [88] Hong Kong | SARS Epidemic | N = 1926 1903 HCWs and 230 administrative staff (controls) | Anxiety (STAI) Burnout (MBI) | Anxiety was significantly higher among those who had contact with SARS patients that those who did not have this contact. Frontline HCWs had significantly higher anxiety and burnout compared to the administrative staff controls. Female nurses experienced more anxiety. |
| Sim et al. (2004) [89] Singapore | SARS Epidemic | N = 277 21 doctors and 186 nurses (Hospital) | Psychiatric morbidity and post-traumatic stress (Self-designed questionnaire) | 20.6% Psychiatric morbidity 9.4% Posttraumatic morbidity Psychiatric morbidity and posttraumatic morbidity were associated with higher scores of coping efforts including self-distraction, behavioral disengagement, social support, venting, planning, and self-blame |
| Sin SS and Huak CY (2004) [90] Singapore | SARS Epidemic | N = 47 therapists.(Hospital) | Psychiatric distress (GHQ) Stress (IES) Self- developed Questionnaire on ways of coping | 23.4% Psychiatric symptoms 12.8% Post-traumatic stress symptoms Support from colleagues, taking precautionary measures, getting clear directives and disease information, support from family and friends were the most common helpful coping strategies. Availability of adequate PPE gave HCWs a sense of control and reduced their stress |
| Tam et al. (2004) [91] Hong Kong | SARS Epidemic | N = 652 HCWs (Hospital) | Psychiatric morbidity (GHQ) | 68% high level of stress. 57% psychological distress. 56.7% psychiatric morbidity High stress risk factors younger age, being a nurse, female, direct care of SARS patients and poorer self-rated physical health condition, inadequate social support. |
| Verma et al. (2004) [92] Singapore | SARS Epidemic | N = 1050 721 GPs N = 329 TCM (traditional Chinese medicine) (General practice) | Psychological distress (GHQ-28) PTSD (IES-R) Stigma (HIV stigma scale) | More GPs were directly involved in the care of patients with SARS. 14.1% GPs, 6% TCMs had psychological distress (GHQ-28 > 7) More GPs had psychological distress compared to TCM practitioners. The mean score of the GHQ somatic, anxiety, and social dysfunction subscales were higher in GPs as compared to practitioners. GPs experienced more stigma. |
| Wong et al. (2004) [93] Hong Kong | SARS Epidemic | N = 137 GPs (General Practice) | Anxiety (Self-designed questionnaire) | Significant anxiety was found in family doctors. 75% requested more investigations. 25% over-prescribed antibiotics Young doctors found their quality of life more affected than their older colleagues |
| Study (Year)/Country | Disease Outbreak | Participants (Setting), Period of Assessment | Mental Health Outcome Measures (Instrument) | Main Findings |
|---|---|---|---|---|
| Lee et al. (2018) [4] Korea | MERS-CoV Epidemic | N= 359 HCWs (Hospital) 6 Weeks | Distress (IES-R) | First survey: 64.1% PTSD-like symptoms, 51.5% PTSD Second survey (N = 77 from the high-risk group): 54.5% PTSD-like symptoms, 40.3% PTSD PTSD symptoms were higher in HCWs who performed MERS related tasks. |
| Lung et al. (2009) [94] Taiwan | SARS Epidemic | N = 127 HCWs (hospital) 8 months | Psychiatric morbidity (CHQ), Personality (EPQ) at the first stage and the CHQ again a year later | Initial assessment (shortly after the SARS epidemic was under control): 17.3% had psychiatric symptoms (CHQ > 3) At follow up (after 1 year): 15.4% had psychiatric symptoms (CHQ > 3) Stress was from job, families, and daily life events. A higher percentage of physicians (35%), compared to nurses (25%), developed psychiatric symptoms |
| Lancee et al. (2008) [95] Canada | SARS Epidemic | N = 139 103 nurses 15 clerical staff (hospital) One year | Distress (IES) Distress (K-10) Burnout (MBI) (SCID) (CAPS) | 30% Lifetime prevalence of psychiatric diagnosis 4% New episode major depression Incidence 2% New-onset PTSD incidence 5% New onset psychiatric disorder incidence New episodes associated with history of psychiatric disorder before the outbreak and less years of healthcare experience. New episodes inversely related to perceived adequacy of training |
| McAlonan et al. (2007) [96] Hong Kong | SARS Epidemic | Doctors, nurses, and healthcare assistants First sample 106 High risk vs. 70 low risk Follow up. 71 High Risk 113 Low Risk (Hospital) One year | First sample Stress (PSS-10) Follow up sample Depression, Anxiety and Stress (DASS-21) Post-traumatic stress (IES) (PSS-10) | 2003 peak of SARS outbreak PSS -10 scores for both groups were elevated but not significantly different from each other. High Risk (17.0) Low risk (15.9) 2004 Follow up. High Risk group remained highly stressed. High risk (18.56) Low risk (14.81) High-Risk group also had higher levels of depression, anxiety, and post-traumatic stress. |
| Su et al. (2007) [97] Taiwan | SARS Epidemic | N = 102 Nurses 70 SARS 32 Non-SARS (hospital) 7 Weeks | Depression (BDI) Anxiety (STAI) Post-traumatic Stress (DTS-C) Insomnia (PSQI) | Depression symptom ratings decreased as the SARS epidemic decreased regardless of which group (SARS vs. non-SARS unit nurses) was assessed. Anxiety symptoms decreased as a function of time. Fifty percent decrease in PTSD symptom scores at the end of the study for each group. After 7 weeks: Depression, insomnia, and stress was higher in SARS unit nurses vs. non-SARS unit nurses. Depression (38.5% vs. 3.1%) Insomnia (37% vs. 9.7%) Post-traumatic stress symptoms (33% vs. 18.7%) No differences in anxiety |
| Study | Johanna Briggs Institute Score | Were the Criteria for Inclusion in the Sample Clearly Defined? | Were the Study Subjects and the Setting Described in Detail? | Exposure Measured in a Valid and Reliable Way? | Objective, Standard Criteria Used for Measurement of the Condition? | Confounding Factors Identified? | Strategies to Deal with Confounding Factors Stated? | Outcomes Measured in a Valid and Reliable Way? | Appropriate Statistical Analysis Used? |
|---|---|---|---|---|---|---|---|---|---|
| Amerio et al. (2020) | 8 | Y | Y | Y | Y | Y | Y | Y | Y |
| Cai et al. (2020) | 5 | Y | Y | Y | Y | N | N | N | Y |
| Chew et al. (2020) | 8 | Y | Y | Y | Y | Y | Y | Y | Y |
| Du et al. (2020) | 5 | N | Y | Y | Y | N | N | Y | Y |
| Hacimusalar et al. (2020) | 8 | Y | Y | Y | Y | Y | Y | Y | Y |
| Hu et al. (2020) | 6 | Y | Y | Y | Y | N | N | Y | Y |
| Kang et al. (2020) | 7 | N | Y | Y | Y | Y | Y | Y | Y |
| Lai et al. (2020) | 8 | Y | Y | Y | Y | Y | Y | Y | Y |
| Li et al. (2020) | 6 | Y | Y | Y | Y | N | N | Y | Y |
| Liang et al. (2020) | 5 | N | Y | Y | Y | N | N | Y | Y |
| Liu et al. (2020) | 8 | Y | Y | Y | Y | Y | Y | Y | Y |
| Lu et al. (2020) | 8 | Y | Y | Y | Y | Y | Y | Y | Y |
| Mo et al. (2020) | 5 | Y | Y | Y | Y | Y | Y | Y | Y |
| Qi et al. (2020) | 8 | Y | Y | Y | Y | Y | Y | Y | Y |
| Que et al. (2020) | 8 | Y | Y | Y | Y | Y | Y | Y | Y |
| Shechter et al. (2020) | 6 | Y | Y | Y | Y | N | N | Y | Y |
| Sun et al. (2020) | 8 | Y | Y | Y | Y | Y | Y | Y | Y |
| Tan et al. (2020) | 7 | N | Y | Y | Y | Y | Y | Y | Y |
| Temsah et al. (2020) | 8 | Y | Y | Y | Y | Y | Y | Y | Y |
| Wang et al. (2020) | 7 | N | Y | Y | Y | Y | Y | Y | Y |
| Wu et al. (2020) | 8 | Y | Y | Y | Y | Y | Y | Y | Y |
| Wu and Wei (2020) | 8 | Y | Y | Y | Y | Y | Y | Y | Y |
| Xiao et al. (2020) | 7 | N | Y | Y | Y | Y | Y | Y | Y |
| Xiaoming (2020) | 8 | Y | Y | Y | Y | Y | Y | Y | Y |
| Xing et al. (2020) | 8 | Y | Y | Y | Y | Y | Y | Y | Y |
| Zhang et al. (2020) | 8 | Y | Y | Y | Y | Y | Y | Y | Y |
| Zhang et al. (2020) | 5 | N | Y | Y | Y | N | N | Y | Y |
| Zhu et al. (2020) | 8 | Y | Y | Y | Y | Y | Y | Y | Y |
| Alsubaie et al. (2019) | 6 | N | Y | Y | N | Y | Y | Y | Y |
| Park et al. (2018) | 8 | Y | Y | Y | Y | Y | Y | Y | Y |
| Oh, et al. (2017) | 8 | Y | Y | Y | Y | Y | Y | Y | Y |
| Tang et al. (2017) | 6 | Y | Y | Y | Y | N | N | Y | Y |
| Ji et al. (2017) | 6 | N | Y | Y | Y | N | N | Y | Y |
| Bukhari et al. (2016) | 6 | N | Y | Y | Y | Y | N | Y | Y |
| Khalid et al. (2016) | 5 | Y | Y | Y | Y | N | N | Y | N |
| Kim et al. (2016) | 8 | Y | Y | Y | Y | Y | Y | Y | Y |
| Lehmann et al. (2016) | 8 | Y | Y | Y | Y | Y | Y | Y | Y |
| Li et al. (2015) | 8 | Y | Y | Y | Y | Y | Y | Y | Y |
| Mohammed (2015) | 8 | Y | Y | Y | Y | Y | Y | Y | Y |
| Liu et al. (2012) | 8 | Y | Y | Y | Y | Y | Y | Y | Y |
| Matsuishi et al. (2012) | 8 | Y | Y | Y | Y | Y | Y | Y | Y |
| Goulia et al. (2010) | 8 | Y | Y | Y | Y | Y | Y | Y | Y |
| Wu et al. (2009) | 8 | Y | Y | Y | Y | Y | Y | Y | Y |
| Styra et al. (2008) | 8 | Y | Y | Y | Y | Y | Y | Y | Y |
| Wu et al. (2008) | 8 | Y | Y | Y | Y | Y | Y | Y | Y |
| Chen (2007) | 8 | Y | Y | Y | Y | Y | Y | Y | Y |
| Lin et al. (2007) | 6 | Y | Y | Y | Y | N | N | Y | Y |
| Marjanovic et al. (2007) | 6 | Y | Y | Y | Y | N | N | Y | Y |
| Chen et al. (2006) | 8 | Y | Y | Y | Y | Y | Y | Y | Y |
| Fiksenbaum et al. (2006) | 8 | Y | Y | Y | Y | Y | Y | Y | Y |
| Maunder et al. (2006) | 8 | Y | Y | Y | Y | Y | Y | Y | Y |
| Chan et al. (2005) | 8 | Y | Y | Y | Y | Y | Y | Y | Y |
| Cheng et al. (2005) | 8 | Y | Y | Y | Y | Y | Y | Y | Y |
| Grace et al. (2005) | 5 | Y | Y | Y | N | N | N | Y | Y |
| Ho et al. (2005) | 8 | Y | Y | Y | Y | Y | Y | Y | Y |
| Koh et al. (2005) | 8 | Y | Y | Y | Y | Y | Y | Y | Y |
| Lee et al. (2005) | 5 | N | Y | Y | Y | N | N | Y | Y |
| Phua et al. (2005) | 6 | Y | Y | Y | Y | N | N | Y | Y |
| Tham et al. (2005) | 8 | Y | Y | Y | Y | Y | Y | Y | Y |
| Wong et al. (2005) | 6 | Y | Y | Y | Y | N | N | Y | Y |
| Bai et al. (2004) | 6 | N | Y | Y | Y | Y | Y | N | Y |
| Chan et al. (2004) | 8 | Y | Y | Y | Y | Y | Y | Y | Y |
| Chong et al. (2004) | 8 | Y | Y | Y | Y | Y | Y | Y | Y |
| Chua et al. (2004) | 6 | Y | Y | Y | Y | N | N | Y | Y |
| Nickell et al. (2004) | 8 | Y | Y | Y | Y | Y | Y | Y | Y |
| Poon et al. (2004) | 6 | Y | Y | Y | Y | N | N | Y | Y |
| Sim et al. (2004) | 7 | N | Y | Y | Y | Y | Y | Y | Y |
| Sin.S.S. and Huak C.Y (2004) | 6 | Y | Y | Y | Y | N | N | Y | Y |
| Tam et al. (2004) | 8 | Y | Y | Y | Y | Y | Y | Y | Y |
| Verma et al. (2004) | 8 | Y | Y | Y | Y | Y | Y | Y | Y |
| Wong et al. (2004) | 5 | Y | Y | Y | Y | N | N | N | Y |
| Study | Johanna Briggs Institute Score | Were the Criteria for Inclusion in the Sample Clearly Defined? | Were the Study Subjects and the Setting Described in Detail? | Exposure Measured in a Valid and Reliable Way? | Objective, Standard Criteria Used for Measurement of the Condition? | Confounding Factors Identified? | Strategies to Deal with Confounding Factors Stated? | Outcomes Measured in a Valid and Reliable Way? | Appropriate Statistical Analysis Used? | Was the Follow Up Time Reported and Sufficient to Be Long Enough for Outcomes to Occur? | Was Follow Up Complete, and If Not, Were the Reasons to Loss to Follow Up Described and Explored? | Were Strategies to Address Incomplete Follow-Up Utilized? |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Lee et al. (2018) | 7 | Y | Y | Y | Y | N | N | Y | Y | Y | N | N |
| Lung et al. (2009) | 8 | N | N | Y | Y | Y | Y | Y | Y | Y | Y | N/A |
| Lancee et al. (2008) | 9 | Y | Y | Y | Y | Y | Y | Y | Y | Y | N | N |
| McAlonan et al. (2007) | 9 | Y | Y | Y | Y | Y | Y | Y | Y | Y | N | N |
| Su T.P. (2007) | 10 | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | N/A |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chigwedere, O.C.; Sadath, A.; Kabir, Z.; Arensman, E. The Impact of Epidemics and Pandemics on the Mental Health of Healthcare Workers: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 6695. https://doi.org/10.3390/ijerph18136695
Chigwedere OC, Sadath A, Kabir Z, Arensman E. The Impact of Epidemics and Pandemics on the Mental Health of Healthcare Workers: A Systematic Review. International Journal of Environmental Research and Public Health. 2021; 18(13):6695. https://doi.org/10.3390/ijerph18136695
Chicago/Turabian StyleChigwedere, Ottilia Cassandra, Anvar Sadath, Zubair Kabir, and Ella Arensman. 2021. "The Impact of Epidemics and Pandemics on the Mental Health of Healthcare Workers: A Systematic Review" International Journal of Environmental Research and Public Health 18, no. 13: 6695. https://doi.org/10.3390/ijerph18136695
APA StyleChigwedere, O. C., Sadath, A., Kabir, Z., & Arensman, E. (2021). The Impact of Epidemics and Pandemics on the Mental Health of Healthcare Workers: A Systematic Review. International Journal of Environmental Research and Public Health, 18(13), 6695. https://doi.org/10.3390/ijerph18136695