The Correlation between Leader–Member Exchange and Organisational Commitment among Spanish Registered Nurses: The Moderating Role of Sex and Hospital Size

 , ,
, ,
Abstract
1. Introduction
1.1. LMX Theory
1.2. LMX (m) and Organisational Commitment
1.3. The Moderating Role of Empowerment in the Relationship between LMX (m) and Organisational Commitment
1.4. The Moderating Role of Perceived Organisational Support (POS) in the Relationship between LMX (m) and Organisational Commitment
1.5. The Moderating Role of Leader–Leader Exchange (LLX) in the Relationship between LMX (m) and Commitment
1.6. Aims
- (a)
- To verify the supposition that the quality of the supervisor–nurse interpersonal relationship correlates with organisational commitment;
- (b)
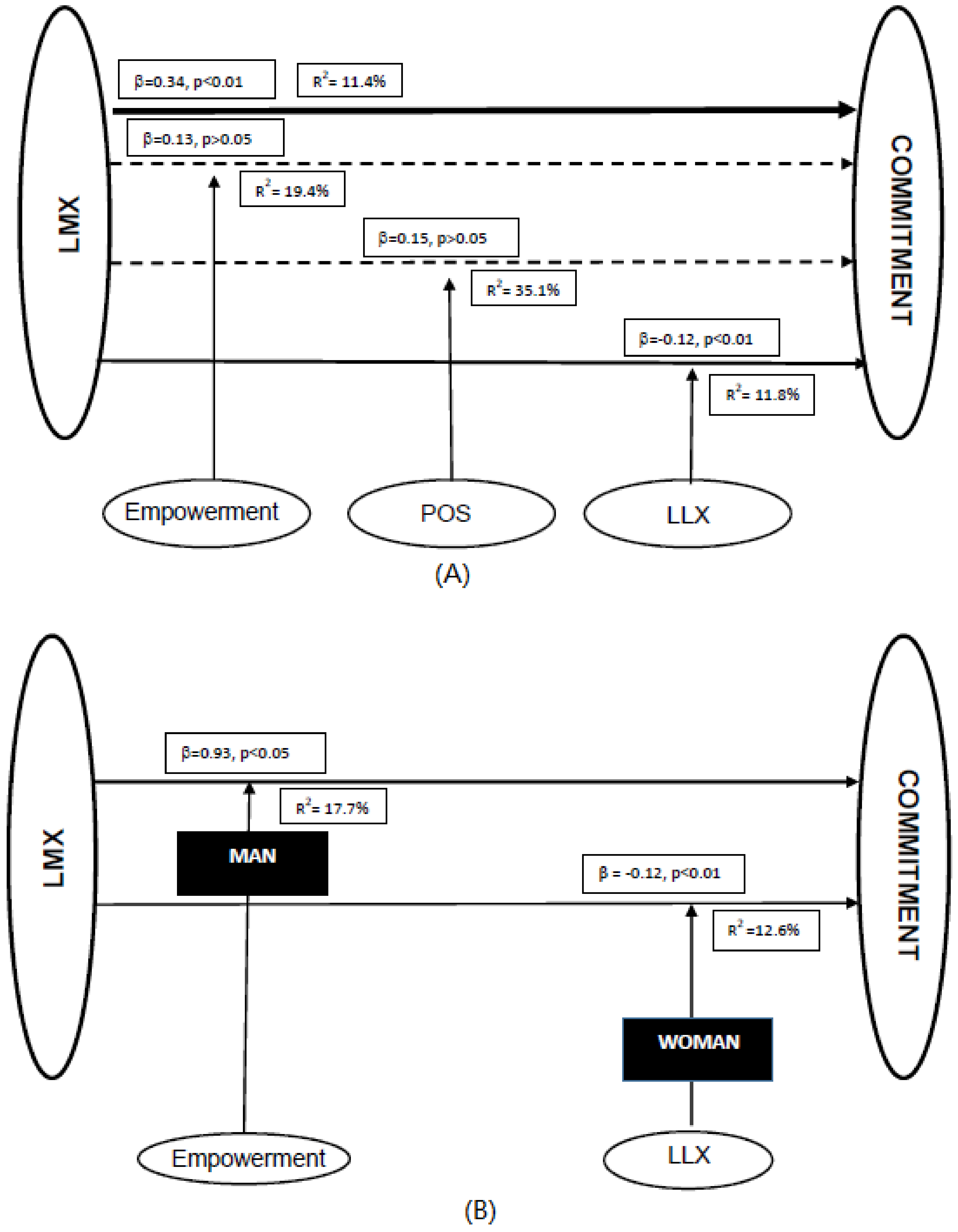
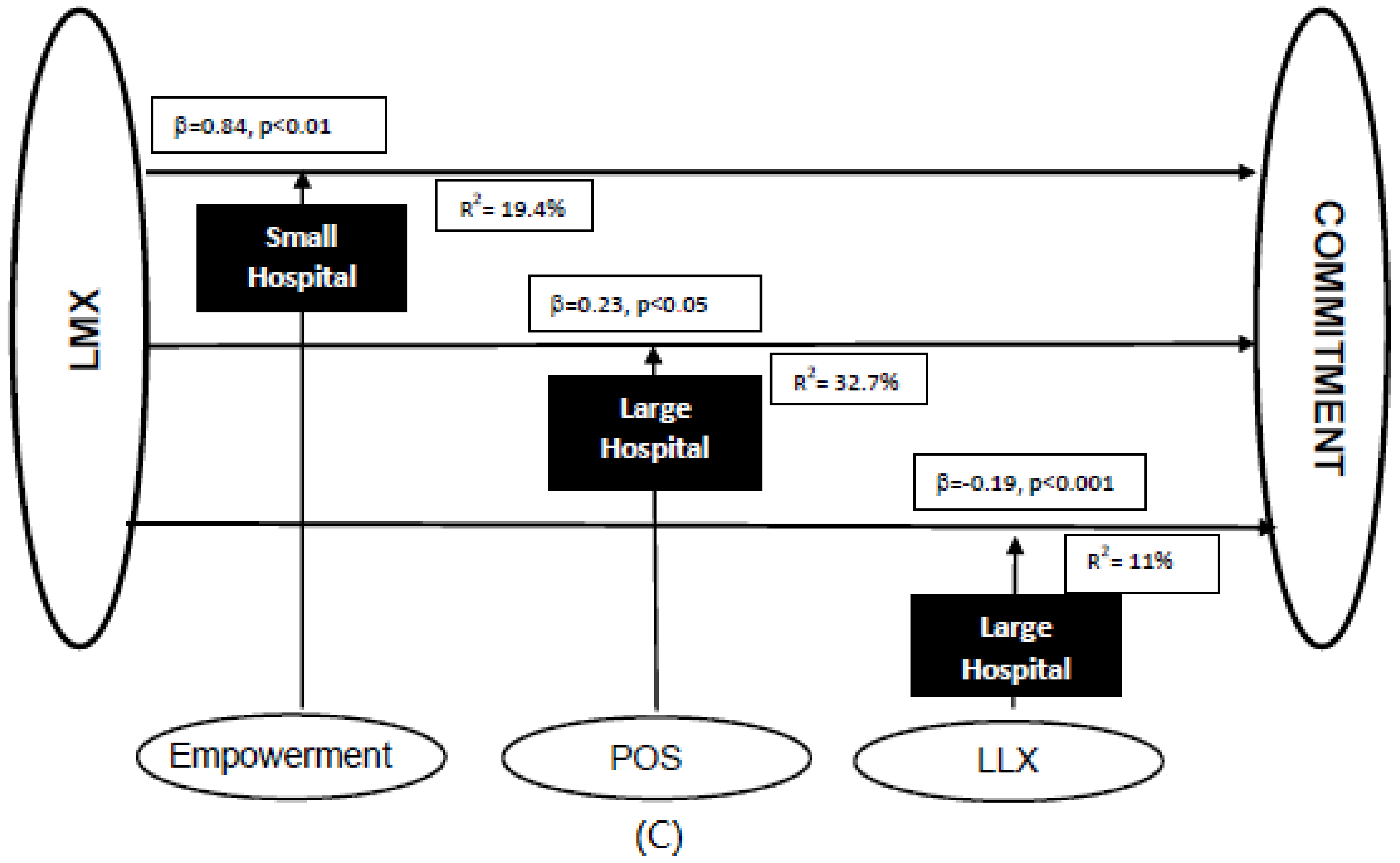
- To establish if the variables empowerment, perceived organisational support, and leader–leader exchange act as moderators in this relationship (Figure 1);
- (c)
- To determine if the moderating effect of these variables is influenced by the size of the hospital and the sex of the nurse.
2. Materials and Methods
2.1. Design
2.2. Sample/Participants
2.3. Data Collection
2.4. Measures
2.4.1. Leader–Member Exchange
2.4.2. Organisational Commitment
2.4.3. Empowerment
2.4.4. Perceived Organisational Support
2.4.5. Leader–Leader Exchange
2.5. Demographic Variables
2.6. Ethical Considerations
2.7. Data Analysis
- The descriptive statistics were calculated.
- An exploratory factor analysis was carried out for each variable to analyse the construct validity of the scales. The Kaiser–Meyer–Olkin test was utilised to check the suitability of the sampling for the factor analysis (values close to 1). The Bartlett sphericity was implemented to check that the extraction of factors was adequate and that the factorial analysis was significant for all cases. The Main Components method for the extraction of factors was also used and an orthogonal rotation was undertaken with the Varimax method. In order to verify the consistency of the instruments used to measure the variables the Cronbach alpha test was employed with each scale. The reliability values were very high, indicating good levels of consistency.
- A correlation matrix gave further variable crossings and a regression model forecast the LMX (m) based on the commitment of the nurse. The regression model followed the Stepwise methodology which allows for controlling inter-correlations among independent variables.
- A multiple linear regression model was used to check the intervention of moderating variables. The equation included the dependent variable (Y), the independent variable (X), the moderating variable (Z), and the product of the independent moderator (X × Z). The significance of the latter term indicates whether the variable in question is a moderating variable.
- The estimations were repeated by sub-samples of sex (men/women) and hospital size (large/small) in order to verify the weighting of these variables in the study.
3. Results
3.1. Descriptive Statistics
3.2. Hypotheses
3.2.1. Hypothesis 1
- Commitment = 2.92 + 0.45 x LMX (m) + e
- The percentage of explained variance (R2) is 11.4%.
3.2.2. Hypothesis 2
3.2.3. Hypothesis 3
3.2.4. Hypothesis 4
3.2.5. Hypothesis 5
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Bateman, T.S.; Strasser, S. A Longitudinal Analysis of the Antecedents of Organizational Commitment. Acad. Manag. J. 1984, 27, 95–112. [Google Scholar]
- Petty, M.; McGee, G.; Cavender, J. A meta-analysis of the relationships between individual job satisfaction and individual performance. Acad. Manag. Rev. 1998, 9, 712–721. [Google Scholar] [CrossRef]
- Eby, L.; Adam, D.; Russell, J.; Gaby, S. Perceptions of organisational readiness for change: Factors related to employees’ reactions to implementation of team based selling. Hum. Relat. 2000, 53, 419–442. [Google Scholar] [CrossRef]
- Griffeth, R.W.; Hom, P.W.; Gaertner, S. A meta-analysis of antecedents and correlates of employee turnover: Update, moderator tests and research implications for the next millennium. J. Manag. 2000, 26, 463–488. [Google Scholar] [CrossRef]
- Pitt, L.; Foreman, S.K.; Bromfield, D. Organizational commitment and service delivery: Evidence from an industrial setting in the UK. Int. J. Hum. Resour. Manag. 1995, 6, 369–389. [Google Scholar] [CrossRef]
- Lee, K.; Carswell, J.; Allen, N. A meta-analytic review of occupational commitment: Relations with person and work variables. J. Appl. Psychol. 2000, 85, 799–811. [Google Scholar] [CrossRef]
- Blanchard, K. Liderazgo de Máximo Nivel. La Clave de Una Organización de Alto Rendimiento; Granica: Barcelona, Spain, 2007. [Google Scholar]
- Kramer, M.; Schmalenberg, C.; Maguire, P. Aspectos esenciales del trabajo enfermero en los hospitales magnéticos. Parte III. Nursing 2005, 23, 14–17. [Google Scholar] [CrossRef]
- Portoghese, I.; Galletta, M.; Battistelli, A.; Saiani, L.; Penna, M.P.; Allegrini, E. Change-related expectations and commitment to change of nurses: The role of leadership and communication. J. Nurs. Manag. 2012, 20, 582–591. [Google Scholar] [CrossRef]
- Gerstner, C.R.; Day, D.V. Meta-analytic review of leader-member exchange theory: Correlates and construct issues. J. Appl. Psychol. 1997, 82, 827–844. [Google Scholar] [CrossRef]
- Cohen, D. The aging nursing workforce: How to retain experienced nurses. J. Healthc. Manag. 2006, 51, 233–245. [Google Scholar] [CrossRef]
- Thompson, D.N.; Hoffman, L.A.; Sereika, S.M.; Lorenz, H.L.; Wolf, G.A.; Burns, H.K.; Minnier, T.E.; Ramanujam, R. A relational leadership perspective on unit-level safety climate. J. Nurs. Adm. 2011, 41, 479–487. [Google Scholar] [CrossRef] [PubMed]
- Mansueti, N.; Grandi, M.G.; Grazio, A. The Leader Member Exchange (Lmx) in Organizational Health Context. Observational Study at the Department of Rehabilitation. Int. J. Med. Pharm. 2016, 4, 1–38. [Google Scholar] [CrossRef]
- Schriesheim, C.A.; Castro, S.L.; Cogliser, C.C. Leader-member exchange (LMX) research: A comprehensive review of theory, measurement, and data-analytic practices. Leadersh. Q. 1999, 10, 63–113. [Google Scholar] [CrossRef]
- Liden, R.C.; Erdogan, B.; Wayne, S.J.; Sparrowe, R.T. Leader–member exchange, differentiation, and task interdependence: Implications for individual and group performance. J. Organ. Behav. 2006, 2, 723–746. [Google Scholar] [CrossRef]
- Liden, R.C.; Graen, G. Generalizability of the vertical dyad linkage model of leadership. Acad. Manag. J. 1980, 23, 451–465. [Google Scholar] [CrossRef]
- Liden, R.C.; Maslyn, J.M. Multidimensionality of leader-member exchange: An empirical assessment through scale development. J. Manag. 1998, 24, 43–72. [Google Scholar] [CrossRef]
- Erdogan, B.; Bauer, T. Leader–Member Exchange Theory. Int. Encycl. Soc. Behav. Sci. 2015, 13, 641–647. [Google Scholar] [CrossRef]
- Labrague, L.J.; McEnroe–Petitte, D.M.; Tsaras, K.; Cruz, J.P.; Colet, P.C.; Gloef, D.S. Organizational commitment and turnover intention among rural nurses in the Philippines: Implications for nursing management International. J. Nurs. Sci. 2018, 5, 403–408. [Google Scholar] [CrossRef]
- Sepahvand, F.; Atashzadeh-Shoorideh, F.; Parvizy, S.; Tafreshi, M.Z. The relationship between some demographic characteristics and organizational commitment of nurses working in the Social Security Hospital of Khorramabad. Electron. Physician 2017, 9, 4503–4509. [Google Scholar] [CrossRef]
- Dulebohn, J.H.; Bommer, W.H.; Liden, R.C.; Brouer, R.L.; Ferris, G.R. A Meta-Analysis of Antecedents and Consequences of Leader-Member Exchange Integrating the Past with an Eye toward the Future. J. Manag. 2012, 38, 1715–1759. [Google Scholar] [CrossRef]
- Sparrowe, R.T.; Liden, R.C. Two routes to influence: Integrating leader–member exchange and social network perspectives. Adm. Sci. Q. 2005, 50, 505–535. [Google Scholar] [CrossRef]
- Dienesch, R.M.; Liden, R.C. Leader-member exchange model of leadership: A critique and further development. Acad. Manag. 1986, 11, 618–634. [Google Scholar] [CrossRef]
- Brouer, R.; Harris, K. Dispositional and situational moderators of the relationship between leader-member exchange and work tension. J. Appl. Soc. Psychol. 2007, 37, 1418–1441. [Google Scholar] [CrossRef]
- Duchon, D.; Green, S.; Taber, T. Vertical dyad linkage: A longitudinal assessment of antecedents, measures and consequences. J. Appl. Psychol. 1986, 71, 56–60. [Google Scholar] [CrossRef]
- Cogliser, C.C.; Schriesheim, C.A. Exploring work unit context and leader-member exchange: A multilevel perspective. J. Organ. Behav. 2000, 21, 487–511. [Google Scholar] [CrossRef]
- Gouldner, A.W. The norm of reciprocity: A preliminary statement. Am. Sociol. Rev. 1960, 25, 161–178. [Google Scholar] [CrossRef]
- Dansereau, F.; Graen, G.B.; Haga, W.J. A vertical dyad linkage approach to leadership within formal organizations: A longitudinal investigation of the role making process. Organ. Behav. Hum. Perform. 1975, 13, 46–78. [Google Scholar] [CrossRef]
- Ansari, M.A.; Hung, D.K.; Aafaqi, R. Leader-member exchange and attitudinal outcomes: Role of procedural justice climate. Leadersh. Organ. Dev. J. 2007, 28, 690–709. [Google Scholar] [CrossRef]
- Kirkman, B.L.; Rosen, B. Beyond self-management: Antecedents and consequences of team empowerment. Acad. Manag. J. 1999, 42, 58–74. [Google Scholar] [CrossRef]
- Liden, R.C.; Wayne, S.; Sparrowe, R. An examination of the mediating role of psychological empowerment on the relations between the job, interpersonal relationships and work outcomes. J. Appl. Psychol. 2000, 85, 407–416. [Google Scholar] [CrossRef]
- Spreitzer, G. Taking stock: A review of more than twenty years of research on empowerment at work. In The SAGE Handbook of Organizational Behaviour; Cooper, C., Barling, J., Eds.; SAGE: Thousand Oaks, CA, USA, 2007; Volume 1, pp. 54–72. [Google Scholar] [CrossRef]
- Spreitzer, G. Social Structural Characteristics of Psychological Empowerment. Acad. Manag. J. 1996, 39, 483–504. [Google Scholar] [CrossRef]
- Eisenberger, R.; Fasolo, P.; Davis-LaMastro, V. Perceived organizational support and employee diligence, commitment, and innovation. J. Appl. Psychol. 1990, 75, 51–59. [Google Scholar] [CrossRef]
- Laschinger, H.; Nosko, A.; Wilk, P.; Finegan, J. Effects of unit empowerment and perceived support for professional nursing practice on unit effectiveness and individual nurse well-being: A time-lagged study. Int. J. Nurs. Stud. 2014, 51, 1615–1623. [Google Scholar] [CrossRef] [PubMed]
- Eisenberger, R.; Huntington, R.; Hutchison, S.; Sowa, D. Perceived organizational support. J. Appl. Psychol. 1986, 71, 500–507. [Google Scholar] [CrossRef]
- Settoon, R.P.; Bennett, N.; Liden, R.C. Social exchange in organizations: Perceived organizational support, leader-member exchange, and employee reciprocity. J. Appl. Psychol. 1996, 81, 219–227. [Google Scholar] [CrossRef]
- Wayne, S.J.; Shore, L.M.; Bommer, W.H.; Tetrick, L.E. The role of fair treatment and rewards in perceptions of organizational support and leader-member exchange. J. Appl. Psychol. 2002, 87, 590–598. [Google Scholar] [CrossRef]
- Eisenberger, R.; Cummings, J.; Armeli, S.; Lynch, P. Perceived organizational support, discretionary treatment and job satisfaction. J. Appl. Psychol. 1997, 82, 812–820. [Google Scholar] [CrossRef]
- Blau, P. Exchange and Power in Social Life; Wiley: New York, NY, USA, 1964. [Google Scholar]
- Pérez, E.; Oteo, L.A. Función Directiva y Recursos Humanos en Sanidad; Díaz de Santos: Madrid, Spain, 2006. [Google Scholar]
- Tangirala, S.; Green, S.G.; Ramanujam, R. In the shadow of the boss’s boss: Effects of supervisors’ upward exchange relationships on employees. J. Appl. Psychol. 2007, 92, 309–320. [Google Scholar] [CrossRef]
- Tansky, J.W.; Cohen, D.J. The relationship between organizational support, employee development, and organizational commitment: An empirical study. Hum. Resour. Dev. Q. 2001, 12, 285–300. [Google Scholar] [CrossRef]
- Sparrowe, R.T.; Liden, R.C. Process and structure in leader-member exchange. Acad. Manag. Rev. 1997, 22, 522–552. [Google Scholar] [CrossRef]
- Sluss, D.; Klimchak, M.; Holmes, J.J. Perceived organizational support as a mediator between relational Exchange and organizational identification. J. Vocat. Behav. 2008, 73, 457–464. [Google Scholar] [CrossRef]
- Zhou, L.; Wang, M.; Chen, G.; Shi, J. Supervisors’ upward exchange relationships and subordinate outcomes: Testing the multilevel mediation role of empowerment. J. Appl. Psychol. 2012, 97, 668–680. [Google Scholar] [CrossRef] [PubMed]
- Somech, A. Relationships of participative leadership with relational demography variables: A multi-level perspective. J. Organ. Behav. 2003, 24, 1003–1018. [Google Scholar] [CrossRef]
- Milner, K.; Katz, L.A.; Fisher, J.; Notrica, V. Gender and the quality of the leader-member exchange: Findings from a South African organization. S. Afr. J. Psychol. 2007, 3, 316–329. [Google Scholar] [CrossRef]
- Estiri, M.; Amiri, N.S.; Khajeheian, D.; Rayej, H. Leader-member exchange and organizational citizenship behavior in hospitality industry: A study on effect of gender. Eurasian Bus. Rev. 2018, 8, 267–284. [Google Scholar] [CrossRef]
- Green, S.G.; Anderson, S.E.; Shiversa, S.L. Demographic and Organizational Influences on Leader–Member Exchange and Related Work Attitudes. Organ. Behav. Hum. Decis. Process. 1996, 66, 203–214. [Google Scholar] [CrossRef]
- Liden, R.C.; Sparrowe, R.T.; Wayne, S.J. Leader–member exchange theory: The past and potential for the future. Res. Pers. Hum. Resour. Manag. 1997, 15, 47–119. [Google Scholar]
- Graen, G.B.; Uhl-Bien, M. Relationship-based approach to leadership: Development of leader-member exchange (LMX) theory of leadership over 25 years: Applying a multi-level, multi-domain perspective. Leadersh. Q. 1995, 6, 219–247. [Google Scholar] [CrossRef]
- De la Rosa, M.D.; Carmona, A. Cómo afecta la relación del empleado con el líder a su compromiso con la organización. Universia Bus. Rev. 2010, 26, 112–133. [Google Scholar]
- Mowday, R.T.; Steers, R.M.; Porter, L.W. The measurement of organizational commitment. J. Vocat. Behav. 1979, 14, 224–247. [Google Scholar] [CrossRef]
- Spreitzer, G.M. Psychological empowerment in the workplace: Dimensions, measurement, and validation. Acad. Manag. J. 1995, 38, 1442–1465. [Google Scholar] [CrossRef]
- Ortega, V. Adaptación al castellano de la versión abreviada de Survey of Perceived Organizational Support. Encuentros Psicol. Soc. 2003, 1, 3–6. [Google Scholar]
- Van Breukelen, W.; Konst, D.; Van Der Vlist, R. Effects of LMX and differential treatment on work unit commitment. Psychol. Rep. 2002, 91, 220–230. [Google Scholar] [CrossRef] [PubMed]
- Brunetto, Y.; Shriberg, A.; Farr-Wharton, R.; Shacklock, K.; Newman, S.; Dienger, J. The importance of supervisor-nurse relationships, teamwork, wellbeing, affective commitment and retention of North American nurses. J. Nurs. Manag. 2013, 21, 827–837. [Google Scholar] [CrossRef] [PubMed]
- Robson, A.; Robson, F. Investigation of nurses’ intention to leave: A study of a sample of UK nurses. J. Health. Organ. Manag. 2016, 30, 154–173. [Google Scholar] [CrossRef] [PubMed]
- Gholami, M.; Saki, M.; Pour, A.H. Nurses’ perception of empowerment and its relationship with organizational commitment and trust in teaching hospitals in Iran. J. Nurs. Manag. 2019, 27, 1020–1029. [Google Scholar] [CrossRef] [PubMed]
- Lee, E.K.; Ji, E.J. The Moderating Role of Leader–Member Exchange in the Relationships between Emotional Labor and Burnout in Clinical Nurses. Asian Nurs. Res. 2018, 12, 56–61. [Google Scholar] [CrossRef]
- Kuokkanen, L.; Suominen, T.; Rankinen, S.; Kukkurainen, M.L.; Savikko, N.; Doran, D. Organizational change and work-related empowerment. J. Nurs. Manag. 2007, 15, 500–507. [Google Scholar] [CrossRef]
- Brunetto, Y.; Shacklock, K.; Teo, S.; Farr-Wharton, R.; Nelson, S. Nurses’ supervisors, learning options and organisational commitment: Australia, Brazil and England. J. Nurs. Manag. 2015, 23, 1029–1038. [Google Scholar] [CrossRef]
- Connolly, M.; Jacobs, S.; Scott, K. Clinical leadership, structural empowerment and psychological empowerment of registered nurses working in an emergency department. J. Nurs. Manag. 2018, 26, 881–887. [Google Scholar] [CrossRef]
- Farr-Wharton, R.; Brunetto, Y.; Shacklock, K. The impact of intuition and supervisor-nurse relationships on empowerment and affective commitment by generation. J. Adv. Nurs. 2012, 68, 1391–1401. [Google Scholar] [CrossRef] [PubMed]
- Laschinger, H.; Finegan, J.; Wilk, P. Context matters: The impact of unit leadership and empowerment on nurses’ organizational commitment. J. Nurs. Adm. 2009, 39, 228–235. [Google Scholar] [CrossRef] [PubMed]
- Wayne, S.J.; Shore, L.M.; Liden, R.C. Perceived organizational support and leader-member exchange: A social exchange perspective. Acad. Manag. J. 1997, 40, 82–111. [Google Scholar] [CrossRef]
- El Akremi, A.; Colaianni, G.; Portoghese, I.; Galletta, M.; Battistelli, A. How organizational support impacts affective commitment and turnover among Italian nurses: A multilevel mediation model. Int. J. Hum. Resour. Manag. 2014, 25, 1185–1207. [Google Scholar] [CrossRef]
- Conger, J. Qualitative research as the cornerstone methodology for understanding leadership. Leadersh. Q. 1998, 9, 107–121. [Google Scholar] [CrossRef]
- Podsakoff, P.; MacKenzie, S.; Lee, C.; Podsakoff, N. Common method biases in behavioral research. J. Appl. Psychol. 2003, 88, 879–903. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Initial | LLX | POS | EMP | ||
|---|---|---|---|---|---|
| Sex | Men | 5.1 | 6.7 | 33.6 | 17.7 |
| Women | 12.1 | 12.6 | 35.4 | 19.7 | |
| Hospital size | Small | 13.4 | 14.5 | 34.9 | 19.4 |
| Large | 9.6 | 11.0 | 32.7 | 19.1 | |
| Global | 11.4 | 11.8 | 35.1 | 19.4 |
| Initial | LLX | POS | EMP | ||
|---|---|---|---|---|---|
| Sex | Men | 0.284 *** | −0.051 | 0.113 | 0.240 * |
| Women | 0.466 *** | −0.028 ** | 0.024 | 0.005 | |
| Hospital size | Small | 0.495 *** | 0.005 | −0.015 | 0.222 ** |
| Large | 0.403 *** | −0.047 *** | 0.051 * | −0.036 | |
| Global | 0.451 *** | −0.028 ** | 0.032 | 0.035 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
López-Ibort, N.; González-de la Cuesta, D.; Antoñanzas-Lombarte, T.; Gascón-Catalán, A. The Correlation between Leader–Member Exchange and Organisational Commitment among Spanish Registered Nurses: The Moderating Role of Sex and Hospital Size. Int. J. Environ. Res. Public Health 2020, 17, 721. https://doi.org/10.3390/ijerph17030721
López-Ibort N, González-de la Cuesta D, Antoñanzas-Lombarte T, Gascón-Catalán A. The Correlation between Leader–Member Exchange and Organisational Commitment among Spanish Registered Nurses: The Moderating Role of Sex and Hospital Size. International Journal of Environmental Research and Public Health. 2020; 17(3):721. https://doi.org/10.3390/ijerph17030721
Chicago/Turabian StyleLópez-Ibort, Nieves, Delia González-de la Cuesta, Teresa Antoñanzas-Lombarte, and Ana Gascón-Catalán. 2020. "The Correlation between Leader–Member Exchange and Organisational Commitment among Spanish Registered Nurses: The Moderating Role of Sex and Hospital Size" International Journal of Environmental Research and Public Health 17, no. 3: 721. https://doi.org/10.3390/ijerph17030721
APA StyleLópez-Ibort, N., González-de la Cuesta, D., Antoñanzas-Lombarte, T., & Gascón-Catalán, A. (2020). The Correlation between Leader–Member Exchange and Organisational Commitment among Spanish Registered Nurses: The Moderating Role of Sex and Hospital Size. International Journal of Environmental Research and Public Health, 17(3), 721. https://doi.org/10.3390/ijerph17030721