Patterns of Service Provision in Older People’s Mental Health Care in Australia

 , ,
, ,  ,
,
Abstract
1. Introduction
2. Materials and Methods
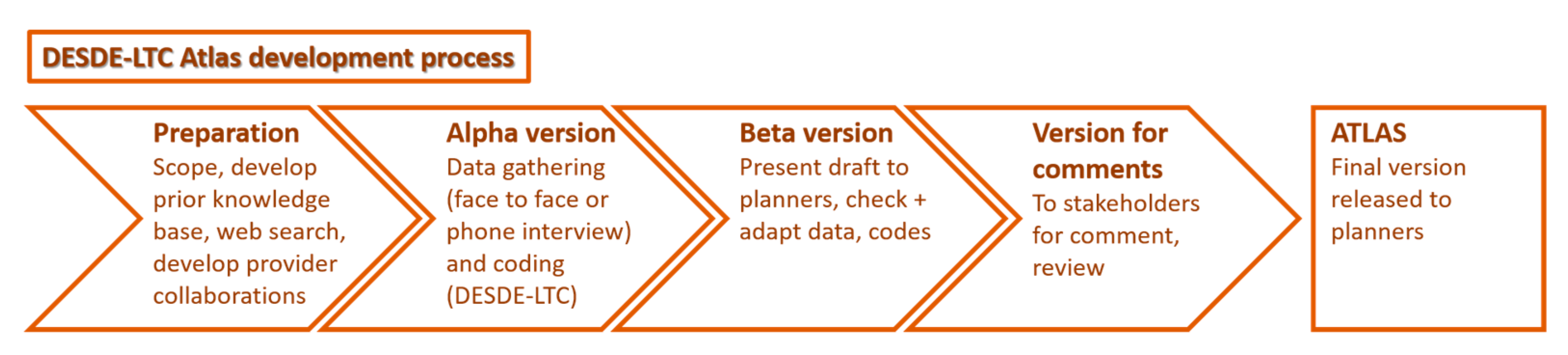
2.1. Study Desing and Procedure
2.2. Study Areas
2.3. Services
- (1)
- Residential care (ranging from acute wards to nursing homes and supported housing): includes services that provide beds overnight for acute or non-acute care. Acute care is care for crises due to deterioration in physical, mental, behavioural or social functioning related to the user’s health condition. Any other care is considered non-acute care. Hospitals, crisis houses, crisis hostels and emergency beds in community-based primary care setting (including those provided by non-health organisations) or mental health centres are examples of residential care.
- (2)
- Day care (ranging from day hospitals to social clubs): provides combinations of different interventions (e.g., structured activity, or social contact and/or support) to a group of users for a period longer than a visit during the course of a day. Acute day care is care for crises due to deterioration in physical, mental, behavioural or social functioning related to their health condition. Any other care is described as non-acute care.
- (3)
- Outpatient care (ranging from outpatient care in hospitals to community mental health centres and home-visit): provides acute and non-acute care at a point of time (care visit). Point of time interventions include face-to-face and on-line treatment for health issues and/or support for social difficulties. Services can be provided at the centre where the care team is based (non-mobile) or by outreach, including another centre or the users’ home (mobile).
- (4)
- Accessibility of care (ranging from transportation to managed care): Facilitates access to care by identifying providers and facilitating re-engagement, facilitating communication (e.g., sign language or translation), facilitating physical mobility of users (e.g., transportation), and navigating, access, management and cohesion of treatment, care and support.
- (5)
- Information for care (ranging from health information services to diagnostic and evaluation services): provides information and/or an assessment to users. Information provision can be interactive (such as face to face) or non-interactive such as pamphlets and webs. Assessment is not limited to health-related assessment and items such as work, education, and social and cultural support are also included. The assessment team does not provide direct care provision.
- (6)
- Self-help and voluntary care: includes any types of care provision by unpaid peers or graduate professionals. Self-help and voluntarily services, informal care associations and teams are also included in this category.
2.4. Inclusion and Exclusion Criteria
- (1)
- Providing specialised mental health services to people aged 65 years and over. Generic services for the general population, which were not specifically for, but could treat older people (e.g., general practitioners), were not included.
- (2)
- Having temporal and organisational stability. Services with administrative support, dedicated space, finance and documentation to track activity, and stable funding were included. Those with less than three years funding were identified with an extension code “v” (variable). Care programmes that were clearly intended for a short period (less than three years) and for a specific reason were excluded.
- (3)
- Being universally accessible, with no substantial out-of-pocket expenses.
- (4)
- Providing care within the boundaries of the defined PHNs.
2.5. Data Collection
2.6. Data Analysis and Mapping
2.7. Ethics Approvals
3. Results
3.1. Description of the Study Areas
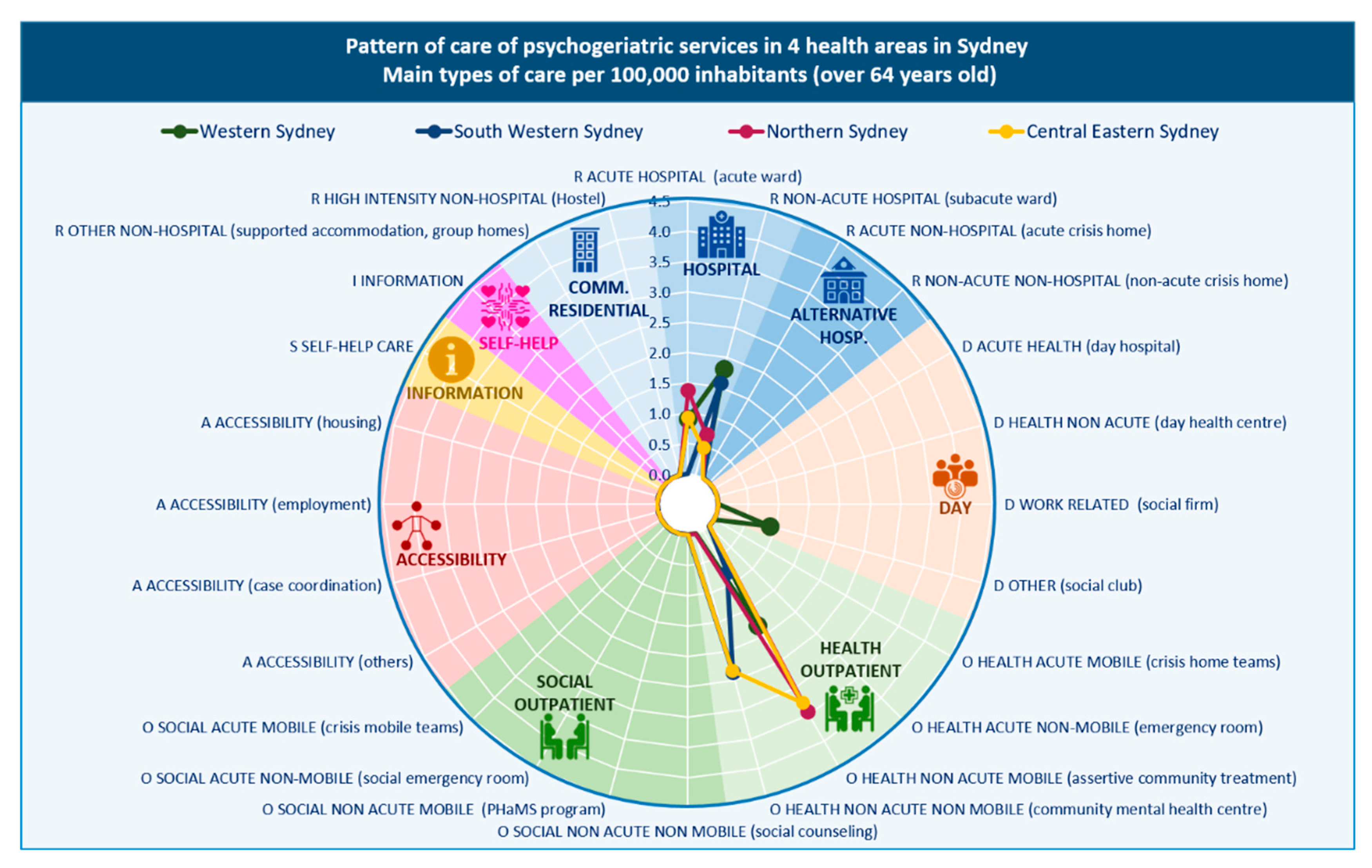
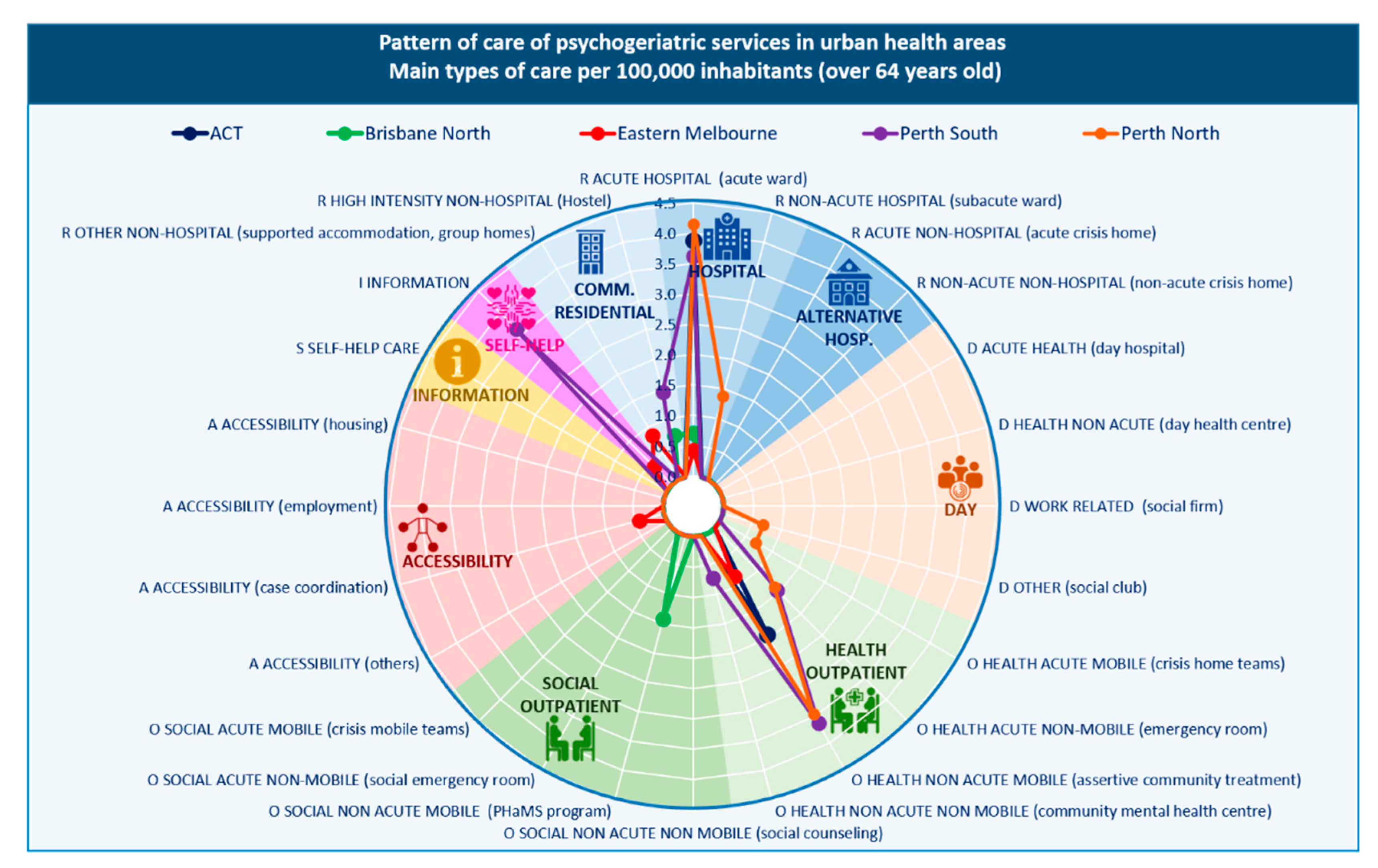
3.2. Overview of Services in Urban Areas
3.2.1. Availability of Care
3.2.2. Placement Capacity
3.2.3. Balance of Care
3.2.4. Diversity of Care
3.3. Overview of Services in Rural Areas
3.3.1. Availability of Care
3.3.2. Placement Capacity
3.3.3. Balance of Care
3.3.4. Diversity of Care
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Broad Category | Description | Other Common Terms | Main Type of Care (MTC) |
|---|---|---|---|
| Residential | Facilities which provide beds overnight for users for a purpose related to the clinical and social management of their health condition | Accommodation, Hospital, Residential | R |
| Hospital | ACUTE. Users are admitted to hospital typically within 24 h because of their crisis condition. Surveillance level and length of stay varies depending on the code | High Dependency Inpatient; Acute Care Unit; Intensive Care Unit; Psychiatric Assessment and Planning Unit; Specialised Acute Mental Health Units for Older People or Specialised Hospitals for Older People | R1–R3 |
| Hospital | NON-ACUTE. Facilities which do not satisfy acute conditions. It can be time limited or indefinite depending on the code. | Sub-acute; Community Care Units; Extended Care Mental Health Rehabilitation Unit; Extended Treatment | R4, R6 |
| Alternative to hospital | ACUTE. Facilities providing acute residential care outside the location of a registered hospital | Crisis homes | R0, R3.1 |
| Alternative to hospital | NON-ACUTE. Facilities with 24 h medical support on site. It can be time limited or indefinite depending on the code | Therapeutic Communities | R5, R7 |
| Community | HIGH INTENSITY. Facilities with 24 h (non-medical) support. Length of stay (4weeks to indefinite) varies depending on the code. | Step up-Step Down (SUSD); Prevention and Recovery Care (PARC); Rehabilitation residences; Supported accommodation; Specialised Residential Aged Care | R8, R11 |
| Community | MEDIUM AND LOW INTENSITY. Facilities with a range of support that varies from daily to fewer to 5 days a week depending on the code. Length of stay (4 weeks to indefinite) varies depending on the code. | Psychiatric Hostel; Group Houses; Supported Accommodation | R9, R10, R12, R13 |
| Day services | Facilities available to several users at a time that provide some combination of planned treatment for users’ needs, with regular opening hours during which they are normally available, and expect users to stay at the facilities beyond the periods during which they have face-to-face contact with staff. | Day services | D |
| Day | ACUTE HEALTH. Users are admitted to the service to because of their crisis condition. Admittance varies typically from 72 h to 4 weeks, depending on the code | Day Hospital services (non-existent in Australia) | D0–D1 |
| Day | NON-ACUTE HEALTH. Typically, at least 20% of staff are qualified health professionals with at least a four year university degree. Depending on the code it can be high (equivalent to 4 half days) or low intensity | Recovery Services; Rehabilitation Services, Therapeutic Day services, Outpatient ECT services, | D4.1, D8.1 |
| Day | WORK-RELATED. Facilities which provide users with the opportunity to work. The salary varies depending on the code: normal wage; 50% of typical wage; not paid or symbolic pay. | Disability Enterprises; Social firms; Workers Coop; Occupational centres; Integration workplace; sheltered work | D2–D3, D6–D7 |
| Day | OTHER. Facilities providing education, social or other non-health-related care. Depending on the code it can be high (equivalent to 4 half days) or low intensity. Structured (activities available more than 25% o opening hours) or non-structured. | Social Clubs; Club Houses; Vocational training; psychiatric drop-in centre, Day centres | D4.2–D4.4, D8.2–D8.4, D5, D9, D10 |
| Outpatient | Facilities providing contact between staff and users for some purpose related to management of their condition that are not provided as a part of delivery of residential or day and structured activity care teams, as defined below. | Community or ambulatory care; psychosocial support | O |
| Health | ACUTE MOBILE. The service provides assessment and initial treatment in response to a health-related crisis, typically same day response during working hours or at least within 72 h after the care demand. At least 50% of contacts take place outside the service (e.g., user’s home). Depending on the code it can be 24 h or limited hours. | Crisis and Assessment Teams; Assertive Community Treatment | O1.1, O2.1 |
| Health | ACUTE NON-MOBILE. The service provides assessment and initial treatment in response to a health-related crisis, the purpose is to treat the user in the service, in no case mobile attention exceeds 50% of overall activity. Depending on the code it can be 24 h or limited hours. | Emergency Units or Depts, Psychiatric Emergency; Psychiatric Liaison | O3.1, O4.1 |
| Health | NON-ACUTE MOBILE. The service does not fulfil criteria for acute care. At least 50% of contacts take place outside the service (e.g., user’s home). Depending on the code it can be high intensity (3 times/week), medium intensity (once a fortnight), low intensity (once a month or less) | Mobile Support and Treatment Team; Community Outreach, Specialised Community Mental Health Teams for Older People | O5.1, O6.1, O7.1 |
| Health | NON-ACUTE NON-MOBILE. The service does not fulfil criteria for acute care. The purpose is to treat the user in the service, in no case mobile attention exceeds 50% of overall activity. Depending on the code it can be high intensity (3 times/week), medium intensity (once a fortnight), low intensity (once a month or less) | Outpatients; Specialised Outpatient Clinics for Older People; Clinic services, Dual Diagnosis; Community Care/Continuing Care, | O8.1, O9.1, O10.1 |
| Social | NON-ACUTE NON-MOBILE. As in non-acute non mobile health but providing other type of care different than health (social, work) | Daily Living, Living Skills Development or Support eg: Art therapy classes, financial or budgeting support (centre based) | O8.2, O9.2, O10.2 |
| Social | NON-ACUTE MOBILE. As in non-acute mobile health but providing other type of care different than health (social, work) | Personal Helpers and Mentors; Psychosocial outreach support | O5.2, O6.2, O7.2 |
| Social | ACUTE NON-MOBILE. As in acute non mobile health but providing other type of care different than health (social, work) | Family and sexual violence crisis services | O3.2, O4.2 |
| Social | ACUTE MOBILE NON-HEALTH. As in acute mobile health but providing other type of care different than health (social, work) | O1.2, O2.2 | |
| Accessibility | Facilities which main aim is to facilitate accessibility to care for users with a specific condition | A | |
| Services that facilitates the access to information; Services that facilitates physical mobility; services that facilitates personal accompaniment; Services that facilitates case coordination; Services that facilitates access to employment or housing. | Partners In Recovery (now ceased), Tenancy Support | A1–A5 | |
| Information | Facilities that provide users from the defined target group with information and/or an assessment of their needs. Does not entail subsequent monitoring/follow-up or direct care provision | I | |
| Guidance and assessment. Information | Telephone triage; Intake & Assessment; Support helplines; Lifeline; Hotline, Information services; Leaflets; Websites | I1–I2 |
References
- Kirchberger, I.; Meisinger, C.; Heier, M.; Zimmermann, A.K.; Thorand, B.; Autenrieth, C.S.; Peters, A.; Ladwig, K.H.; Döring, A. Patterns of multimorbidity in the aged population. results from the KORA-Age study. PLoS ONE 2012, 7. [Google Scholar] [CrossRef] [PubMed]
- Wister, A.; Kendig, H.; Mitchell, B.; Fyffe, I.; Loh, V. Multimorbidity, health and aging in Canada and Australia: A tale of two countries. BMC Geriatr. 2016, 16. [Google Scholar] [CrossRef] [PubMed]
- Yaffe, K.; Middleton, L.E.; Lui, L.Y.; Spira, A.P.; Stone, K.; Racine, C.; Ensrud, K.E.; Kramer, J.H. Mild cognitive impairment, dementia, and their subtypes in oldest old women. Arch. Neurol. 2011, 68, 631–636. [Google Scholar] [CrossRef] [PubMed]
- Institute for Health Metrics and Evaluation Global Burden of Disease Study. 2017. Available online: http://ghdx.healthdata.org/gbd-2017 (accessed on 17 September 2020).
- Forlani, C.; Morri, M.; Ferrari, B.; Dalmonte, E.; Menchetti, M.; De Ronchi, D.; Atti, A.R. Prevalence and gender differences in late-life depression: A population-based study. Am. J. Geriatr. Psychiatry 2014, 22, 370–380. [Google Scholar] [CrossRef] [PubMed]
- Erlangsen, A.; Banks, E.; Joshy, G.; Calear, A.L.; Welsh, J.; Batterham, P.J.; Salvador-Carulla, L. Measures of mental, physical, and social wellbeing and their association with death by suicide and self-harm in a cohort of 266,324 persons aged 45 years and over. Soc. Psychiatry Psychiatr. Epidemiol. 2020. [Google Scholar] [CrossRef]
- Jané-Llopis, E.; Gabilondo, A. Consensus Paper: Mental Health in Older People; European Communities: Luxembourg, 2008. [Google Scholar]
- Social Protection Committee and the European Union. Adequate Social Protection for Long-Term Care Needs in an Ageing Society; Publications Office of the European Union: Luxembourg, 2014. [Google Scholar]
- Stansfield, J.; South, J.; Mapplethorpe, T. What are the elements of a whole system approach to community-centred public health? A qualitative study with public health leaders in England’s local authority areas. BMJ Open 2020, 10. [Google Scholar] [CrossRef]
- Roxby, A.C.; Greninger, A.L.; Hatfield, K.M.; Lynch, J.B.; Dellit, T.H.; James, A.; Taylor, J.; Page, L.C.; Kimball, A.; Arons, M.; et al. Detection of SARS-CoV-2 Among Residents and Staff Members of an Independent and Assisted Living Community for Older Adults—Seattle, Washington, 2020. MMWR. Morb. Mortal. Wkly. Rep. 2020, 69, 416–418. [Google Scholar] [CrossRef]
- Salvador-Carulla, L.; Rosenberg, S.; Mendoza, J.; Tabatabaei-Jafari, H. Rapid response to crisis: Health system lessons from the active period of COVID-19. Heal. Policy Technol. 2020. [Google Scholar] [CrossRef]
- Productivity Commission. An Ageing Australia: Preparing for the Future; Productivity Commission: Canberra, Australia, 2013; ISBN 978-1-74037-462-0. [Google Scholar]
- O’Connor, D.W.; Jackson, K.; Lie, D.; McGowan, H.; McKay, R. Survey of aged psychiatry services’ support of older Australians with very severe, persistent behavioural symptoms of dementia. Aust. J. Ageing 2018, 37, E133–E138. [Google Scholar] [CrossRef]
- Furst, M.A.; Bagheri, N.; Salvador-Carulla, L. An ecosystems approach to mental health services research. BJ Psych. Int. 2020, 1–3. [Google Scholar] [CrossRef]
- Romero-López-Alberca, C.; Gutiérrez-Colosía, M.R.; Salinas-Pérez, J.A.; Almeda, N.; Furst, M.A.; Johnson, S.; Salvador-Carulla, L. Standardised description of health and social care: A systematic review of use of the ESMS/DESDE (European Service Mapping Schedule/Description and Evaluation of Services and DirectoriEs). Eur. Psychiatry 2019, 61, 97–110. [Google Scholar] [CrossRef] [PubMed]
- Johri, M.; Beland, F.; Bergman, H. International experiments in integrated care for the elderly: A synthesis of the evidence. Int. J. Geriatr. Psychiatry 2003, 18, 222–235. [Google Scholar] [CrossRef] [PubMed]
- OECD; Eurostat; WHO. A System of Health Accounts 2011; OECD Publishing: Brussels, Belgium, 2011; ISBN 978-92-64-11600-9. [Google Scholar]
- García-Alonso, C.R.; Almeda, N.; Salinas-Pérez, J.A.; Gutiérrez-Colosía, M.R.; Uriarte-Uriarte, J.J.; Salvador-Carulla, L. A decision support system for assessing management interventions in a mental health ecosystem: The case of Bizkaia (Basque Country, Spain). PLoS ONE 2019, 14, e0212179. [Google Scholar] [CrossRef] [PubMed]
- Castelpietra, G.; Simon, J.; Gutiérrez-Colosía, M.R.; Rosenberg, S.; Salvador-Carulla, L. Disambiguation of psychotherapy: A search for meaning. Br. J. Psychiatry 2020, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Van Spijker, B.A.; Salinas-Perez, J.A.; Mendoza, J.; Bell, T.; Bagheri, N.; Furst, M.A.; Reynolds, J.; Rock, D.; Harvey, A.; Rosen, A.; et al. Service availability and capacity in rural mental health in Australia: Analysing gaps using an Integrated Mental Health Atlas. Aust. N. Z. J. Psychiatry 2019, 53, 1–13. [Google Scholar] [CrossRef]
- Salinas-Perez, J.A.; Gutierrez-Colosia, M.R.; Furst, M.A.; Suontausta, P.; Bertrand, J.; Almeda, N.; Mendoza, J.; Rock, D.; Sadeniemi, M.; Cardoso, G.; et al. Patterns of Mental Health Care in Remote Areas: Kimberley (Australia), Nunavik (Canada), and Lapland (Finland). Can. J. Psychiatry 2020, 1–10. [Google Scholar] [CrossRef]
- Salinas-Perez, J.A.; Salvador-Carulla, L.; Saldivia, S.; Grandon, P.; Minoletti, A.; Romero Lopez-Alberca, C. Integrated mapping of local mental health systems in Central Chile. Pan Am. J. Public Heal. 2018, 42, e144. [Google Scholar] [CrossRef]
- Salinas-Perez, J.A.; Gutierrez-Colosia, M.R.; Romero Lopez-Alberca, C.; Poole, M.; Rodero-Cosano, M.L.; Garcia-Alonso, C.R.; Salvador-Carulla, L. Todo está en el mapa: Atlas Integrales de Salud Mental para la planificación de servicios. Informe SESPAS 2020. Gac. Sanit. 2020. [Google Scholar] [CrossRef]
- Gutiérrez-Colosía, M.R.; Salvador-Carulla, L.; Salinas-Pérez, J.A.; García-Alonso, C.R.; Cid, J.; Salazzari, D.; Montagni, I.; Tedeschi, F.; Cetrano, G.; Chevreul, K.; et al. Standard comparison of local mental health care systems in eight European countries. Epidemiol. Psychiatr. Sci. 2017, 1–14. [Google Scholar] [CrossRef]
- Sadeniemi, M.; Almeda, N.; Salinas-Pérez, J.A.; Gutiérrez-Colosía, M.R.; García-Alonso, C.; Ala-Nikkola, T.; Joffe, G.; Pirkola, S.; Wahlbeck, K.; Cid, J.; et al. A Comparison of Mental Health Care Systems in Northern and Southern Europe: A Service Mapping Study. Int. J. Environ. Res. Public Heal. 2018, 15, 1133. [Google Scholar] [CrossRef]
- Fernandez, A.; Salinas-Perez, J.A.; Gutierrez-Colosia, M.R.; Prat-Pubill, B.; Serrano-Blanco, A.; Molina, C.; Jorda, E.; Garcia-Alonso, C.R.; Salvador-Carulla, L. Use of an integrated Atlas of Mental Health Care for evidence informed policy in Catalonia (Spain). Epidemiol. Psychiatr. Sci. 2015, 24, 512–524. [Google Scholar] [CrossRef] [PubMed]
- Fernandez, A.; Gillespie, J.A.; Smith-Merry, J.; Feng, X.; Astell-Burt, T.; Maas, C.; Salvador-Carulla, L. Integrated mental health atlas of the Western Sydney Local Health District: Gaps and recommendations. Aust. Heal. Rev. 2017, 41, 38–44. [Google Scholar] [CrossRef] [PubMed]
- Public Health Information Development Unit (PHIDU) Social Health Atlases of Australia. Available online: http://phidu.torrens.edu.au/social-health-atlases (accessed on 17 September 2020).
- Australian Bureau of Statistics 2016 Census. Available online: https://www.abs.gov.au/websitedbs/censushome.nsf/home/2016 (accessed on 17 September 2020).
- Australian Bureau of Statistics Socio-Economic Indexes for Areas (SEIFA). Available online: https://www.abs.gov.au/websitedbs/censushome.nsf/home/seifa (accessed on 17 September 2020).
- McGrail, M.R.; Humphreys, J.S. The index of rural access: An innovative integrated approach for measuring primary care access. BMC Health Serv. Res. 2009, 9, 124. [Google Scholar] [CrossRef] [PubMed]
- Research School of Population Health Atlas of Mental Health Care. Available online: https://rsph.anu.edu.au/research/projects/atlas-mental-health-care (accessed on 17 September 2020).
- Salvador-Carulla, L.; Álvarez-Gálvez, J.; Romero, C.; Gutiérrez-Colosía, M.R.; Weber, G.; McDaid, D.; Dimitrov, H.; Sprah, L.; Kalseth, B.; Tibaldi, G.; et al. Evaluation of an integrated system for classification, assessment and comparison of services for long-term care in Europe: The eDESDE-LTC study. BMC Health Serv. Res. 2013, 13, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Salvador-Carulla, L.; Romero, C.; Martinez, A.; Haro, J.M.; Bustillo, G.; Ferreira, A.; Gaite, L.; Johnson, S. Assessment instruments: Standardization of the European Service Mapping Schedule (ESMS) in Spain. Acta Psychiatr. Scand. 2000, 405, 24–32. [Google Scholar] [CrossRef]
- Salvador-Carulla, L.; Poole, M.; Gonzalez-Caballero, J.L.; Romero, C.; Salinas, J.A.; Lagares-Franco, C.M.; González-Caballero, J.L.; Romero, C.; Salinas, J.A.; Lagares-Franco, C.M.; et al. Development and usefulness of an instrument for the standard description and comparison of services for disabilities (DESDE). Acta Psychiatr. Scand. 2006, 114, 19–28. [Google Scholar] [CrossRef] [PubMed]
- Montagni, I.; Salvador-Carulla, L.; Mcdaid, D.; Straßmayr, C.; Endel, F.; Näätänen, P.; Kalseth, J.; Kalseth, B.; Matosevic, T.; Donisi, V.; et al. The REFINEMENT Glossary of Terms: An International Terminology for Mental Health Systems Assessment. Adm. Policy Ment. Heal. Ment. Heal. Serv. Res. 2018, 45, 342–351. [Google Scholar] [CrossRef]
- Salvador-Carulla, L.; Amaddeo, F.; Gutiérrez-Colosía, M.R.; Salazzari, D.; Gonzalez-Caballero, J.L.; Montagni, I.; Tedeschi, F.; Cetrano, G.; Chevreul, K.; Kalseth, J.; et al. Developing a tool for mapping adult mental health care provision in Europe: The REMAST research protocol and its contribution to better integrated care. Int. J. Integr. Care 2015, 15, e042. [Google Scholar] [CrossRef]
- Marewski, J.N.; Gigerenzer, G. Heuristic decision making in medicine. Dialogues Clin. Neurosci. 2012, 14, 77–89. [Google Scholar]
- Davies, N.; Mathew, R.; Wilcock, J.; Manthorpe, J.; Sampson, E.L.; Lamahewa, K.; Iliffe, S. A co-design process developing heuristics for practitioners providing end of life care for people with dementia. BMC Palliat. Care 2016, 15, 68. [Google Scholar] [CrossRef]
- Parliament of Australia Population. Available online: https://www.aph.gov.au/About_Parliament/Parliamentary_Departments/Parliamentary_Library/pubs/BriefingBook46p/Population (accessed on 17 September 2020).
- Cornwell, E.Y.; Waite, L.J. Social disconnectedness, perceived isolation, and health among older adults. J. Health Soc. Behav. 2009, 50, 31–48. [Google Scholar] [CrossRef] [PubMed]
- Hawkley, L.C.; Capitanio, J.P. Perceived social isolation, evolutionary fitness and health outcomes: A lifespan approach. Philos. Trans. R. Soc. B Biol. Sci. 2015, 370. [Google Scholar] [CrossRef]
- Manthorpe, J.; Moriarty, J. Examining day centre provision for older people in the UK using the Equality Act 2010: Findings of a scoping review. Heal. Soc. Care Community 2014, 22, 352–360. [Google Scholar] [CrossRef]
- Phillipson, L.; Johnson, K.; Cridland, E.; Hall, D.; Neville, C.; Fielding, E.; Hasan, H. Knowledge, help-seeking and efficacy to find respite services: An exploratory study in help-seeking carers of people with dementia in the context of aged care reforms 11 Medical and Health Sciences 1117 Public Health and Health Services. BMC Geriatr. 2019, 19. [Google Scholar] [CrossRef]
- Zarit, S.H.; Kim, K.; Femia, E.E.; Almeida, D.M.; Savla, J.; Molenaar, P.C.M. Effects of adult day care on daily stress of caregivers: A within-person approach. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2011, 66, 538–546. [Google Scholar] [CrossRef]
- Garde, E.L.; Manning, V.; Lubman, D.I. Characteristics of clients currently accessing a national online alcohol and drug counselling service. Australas. Psychiatry 2017, 25, 250–253. [Google Scholar] [CrossRef]
- Community Affairs References Committee. Accessibility and Quality of Mental Health Services in Rural and Remote Australia; Commonwealth of Australia: Canberra, Australia, 2018. [Google Scholar]
- Perkins, D.; Farmer, J.; Salvador-Carulla, L.; Dalton, H.; Luscombe, G.; Salvador-Carulla, L.; Dalton, H.; Luscombe, G. The Orange Declaration on rural and remote mental health. Aust. J. Rural Health 2019, 27, 374–379. [Google Scholar] [CrossRef]
- Djulbegovic, B.; Elqayam, S.; Dale, W. Rational decision making in medicine: Implications for overuse and underuse. J. Eval. Clin. Pract. 2018, 24, 655–665. [Google Scholar] [CrossRef]
- Saunders, C.L.; Elliott, M.N.; Lyratzopoulos, G.; Abel, G.A. Beyond the ecological fallacy: Potential problems when studying healthcare organisations. J. R. Soc. Med. 2016, 109, 92–97. [Google Scholar] [CrossRef]
- Gibert, K.; García-Alonso, C.; Salvador-Carulla, L. Integrating clinicians, knowledge and data: Expert-based cooperative analysis in healthcare decision support. Heal. Res. Policy Syst. 2010, 8, 28. [Google Scholar] [CrossRef]
- Rock, D.; Cross, S.P. Regional planning for meaningful person-centred care in mental health: Context is the signal not the noise. Epidemiol. Psychiatr. Sci. 2020, 29, e104. [Google Scholar] [CrossRef] [PubMed]
- Iruin-Sanz, A.; Pereira-Rodriguez, C.; Nuno-Solinis, R. The role of geographic context on mental health: Lessons from the implementation of mental health atlases in the Basque Country (Spain). Epidemiol. Psychiatr. Sci. 2015, 24, 42–44. [Google Scholar] [CrossRef] [PubMed]
- Furst, M.A.; Salinas-Perez, J.A.; Hopman, K.; Bagheri, N.; Campos, W.; Gillespie, J.; Mendoza, J.; Salvador-Carulla, L. The Integrated Atlas of Psychosocial Care in the Western Sydney Primary Health Network Region; Centre for Mental Health Research, Australian National University: Canberra, Australia, 2019. [Google Scholar]




| Indicators | ACT | Central and Eastern Sydney | Western Sydney | South Western Sydney | Northern Sydney | Brisbane North | Eastern Melbourne | Perth North | Perth South | Country WA | WNSW | Australia |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Area (km2) | 2351 | 626 | 766 | 6186 | 890 | 3901 | 3,956 | 2975 | 5148 | 2,477,561 | 433,379 | 7,594,238 |
| Total population, 2016 | 411,667 | 1,599,658 | 975,083 | 989,536 | 928,456 | 1,003,843 | 1,531,395 | 1,062,621 | 981,218 | 531,613 | 307,905 | 24,592,907 |
| Population aged 65 years and over 2015-2016 (%) | 51,621 (12.54) | 214,452 (13.41) | 110,943 (11.38) | 127,273 (12.86) | 145,457 (15.67) | 140,576 (14.00) | 238,619 (15.58) | 144,949 (13.64) | 138,113 (14.08) | 76,913 (14.47) | 56,345 (18.30) | 3,790,791 (15.41) |
| Density ratio, 2016 | 175.10 | 2555.36 | 1272.95 | 159.96 | 1043.21 | 257.33 | 387.11 | 357.18 | 190.60 | 0.21 | 0.71 | 3.19 |
| Ageing index, 2016 (%) | 66.06 | 88.43 | 54.07 | 60.22 | 84.71 | 74.96 | 85.33 | 71.96 | 72.19 | 70.25 | 89.37 | 81.80 |
| Unemployment, 2016 (%) | 4.48 | 4.22 | 5.98 | 6.32 | 3.97 | 5.19 | 4.75 | 5.80 | 6.26 | 5.76 | 5.70 | 5.88 |
| Low income households (households in bottom 40% of income distribution), 2016 (%) | 40.41 | 31.90 | 38.12 | 46.62 | 24.52 | 34.65 | 36.63 | 39.06 | 44.34 | 47.66 | 49.26 | 40.54 |
| SEIFA Index of Relative Socio-economic Disadvantage (based on Australian score of 1000), 2016 | 1075 | 1036 | 1005 | 945 | 1093 | 1032 | 1048 | 1039 | 1013 | 976 | 954 | 1000 |
| People 65 years and over with a profound or severe disability and living in the community, 2016 | 13.67% | 16.15% | 17.98% | 22.04% | 11.36% | 13.48% | 13.74% | 12.55% | 13.34% | 11.56% | 12.65% | 14.34% |
| Residential aged care places per 1,000 population aged 65 years and over, 2016 | 47.91 | 58.03 | 45.83 | 52.71 | 61.36 | 50.56 | 55.55 | 45.11 | 49.37 | 41.13 | 61.02 | 52.61 |
| Study Areas | Urban Study Areas | Rural Study Areas | Australia | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Brisbane North | ACT | Eastern Melbourne | Central & Eastern Sydney | Northern Sydney | South Western Sydney | Western Sydney | Perth South | Perth North | Total | Country Western Australia | Western NSW | Total | Total Number/Estimation (95% CI) | |
| Mental health service provision (raw numbers) | ||||||||||||||
| Number of MTC | 4 | 3 | 7 | 15 | 8 | 6 | 6 | 20 | 17 | 86 | 22 | 2 | 24 | 110 |
| Diversity of MTC in older people (>64) | 3 | 2 | 6 | 5 | 3 | 3 | 5 | 6 | 7 | 19 | 6 | 2 | 7 | 19 |
| Diversity of MTC in the general adult population (>18) | 31 | 29 | 39 | 48 | 32 | 26 | 29 | 32 | 35 | 69 | 25 | 24 | 36 | 71 |
| Diversity of MTC in children, adolescent and young adults (<25) | 6 † | 12 | 20 | 7 ‡ | 8 | 4 | 7 | 15 | 8 | 33 †,‡ | 11 | 6 | 13 | 34 |
| Balance of care (percentage of total MTC) | ||||||||||||||
| Health care (%) | 25.0 | 100.0 | 42.9 | 100.0 | 100.0 | 100.0 | 83.3 | 65.0 | 94.1 | 81.4 | 100.0 | 100.0 | 100.0 | 85.5 (78.9–92.0) |
| Other care (%) | 75.0 | 0.0 | 57.1 | 0.0 | 0.0 | 0.0 | 16.7 | 35.0 | 5.9 | 18.6 | 0.0 | 0.0 | 0.0 | 14.5 (8.0–21.1) |
| Care classification (percentage of total MTC) | ||||||||||||||
| Hospital (%) | 25.0 | 66.7 | 14.3 | 20,0 | 37.5 | 33.3 | 50.0 | 25.0 | 47.1 | 32.6 | 0.0 | 50.0 | 4.2 | 26.4 (18.1–34.6) |
| Community residential (%) | 25.0 | 0.0 | 28.6 | 0.0 | 0.0 | 0.0 | 0.0 | 10.0 | 0.0 | 5.8 | 0.0 | 0.0 | 0.0 | 4.5 (0.7–8.4) |
| Day care (%) | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 16.7 | 0.0 | 5.9 | 2.3 | 0.0 | 0.0 | 0.0 | 1.8 (−0.7–4.3) |
| Health outpatient (%) | 0.0 | 33.3 | 28.6 | 80.0 | 62.5 | 66.7 | 33.3 | 40.0 | 47.1 | 48.8 | 100.0 | 33.3 | 95.8 | 59.1 (49.9–68.3) |
| Social outpatient (%) | 50.0 | 0.0 | 14.3 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 3.5 | 0.0 | 0.0 | 0.0 | 2.7 (−0.3–5.8) |
| Info. (%) | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 25.0 | 0.0 | 5.8 | 0.0 | 0.0 | 0.0 | 4.5 (0.7–8.4) |
| Access. (%) | 0.0 | 0.0 | 14.3 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 1.2 | 0.0 | 0.0 | 0.0 | 0.9 (−0.9–2.7) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tabatabaei-Jafari, H.; Salinas-Perez, J.A.; Furst, M.A.; Bagheri, N.; Mendoza, J.; Burke, D.; McGeorge, P.; Salvador-Carulla, L. Patterns of Service Provision in Older People’s Mental Health Care in Australia. Int. J. Environ. Res. Public Health 2020, 17, 8516. https://doi.org/10.3390/ijerph17228516
Tabatabaei-Jafari H, Salinas-Perez JA, Furst MA, Bagheri N, Mendoza J, Burke D, McGeorge P, Salvador-Carulla L. Patterns of Service Provision in Older People’s Mental Health Care in Australia. International Journal of Environmental Research and Public Health. 2020; 17(22):8516. https://doi.org/10.3390/ijerph17228516
Chicago/Turabian StyleTabatabaei-Jafari, Hossein, Jose A. Salinas-Perez, Mary Anne Furst, Nasser Bagheri, John Mendoza, David Burke, Peter McGeorge, and Luis Salvador-Carulla. 2020. "Patterns of Service Provision in Older People’s Mental Health Care in Australia" International Journal of Environmental Research and Public Health 17, no. 22: 8516. https://doi.org/10.3390/ijerph17228516
APA StyleTabatabaei-Jafari, H., Salinas-Perez, J. A., Furst, M. A., Bagheri, N., Mendoza, J., Burke, D., McGeorge, P., & Salvador-Carulla, L. (2020). Patterns of Service Provision in Older People’s Mental Health Care in Australia. International Journal of Environmental Research and Public Health, 17(22), 8516. https://doi.org/10.3390/ijerph17228516