An Update on Physical Activity Research among Children in Hong Kong: A Scoping Review

 , ,
, ,  ,
,  and
and
Abstract
1. Introduction
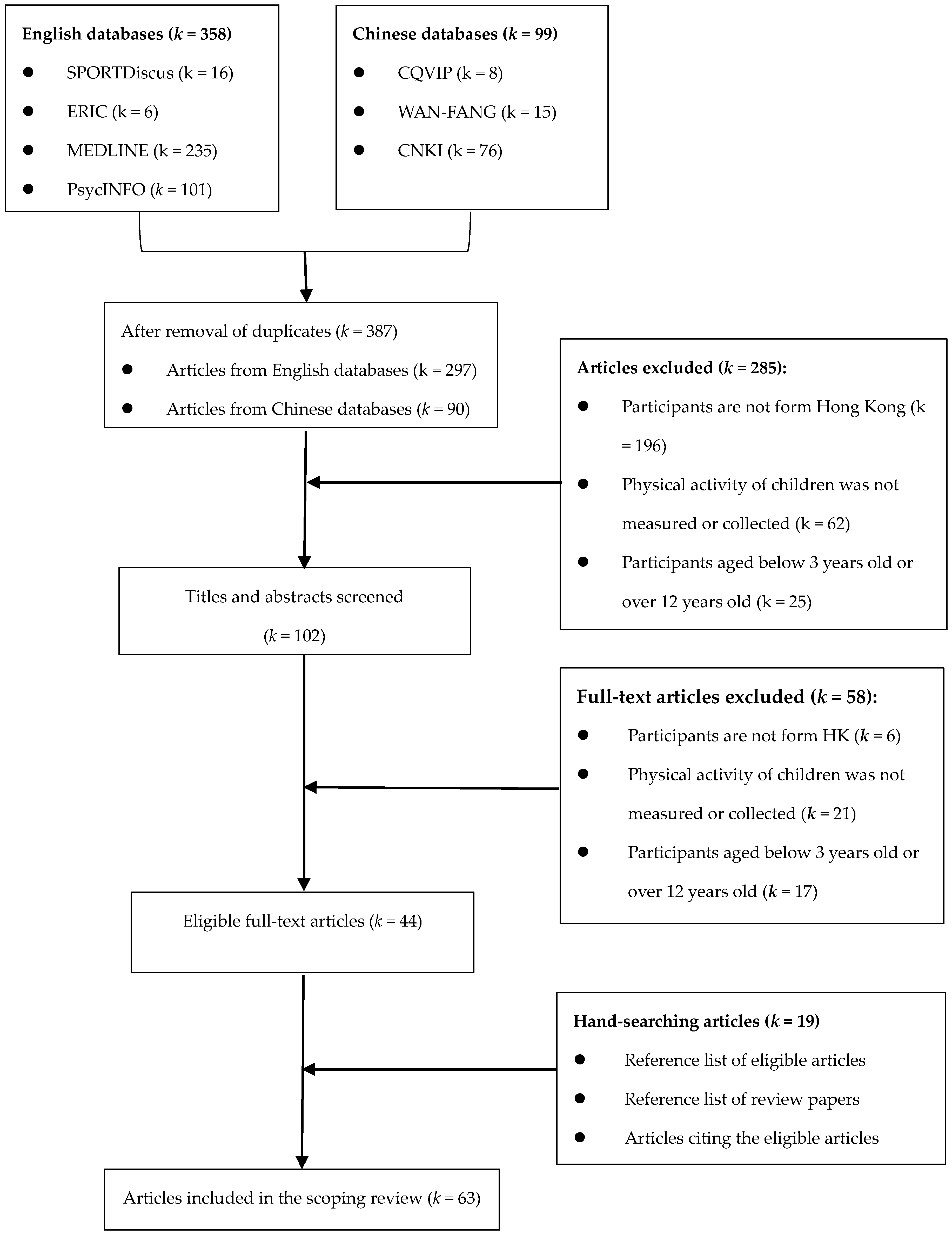
2. Methods
3. Results
3.1. Study Characteristics
3.2. Main Findings
3.2.1. Health Benefits of PA
3.2.2. Patterns of PA
3.2.3. Measures of PA and Related Constructs
3.2.4. Correlates of PA
3.2.5. Interventions for Promoting PA
4. Discussion
Limitations and Future Directions
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Aubert, S.; Barnes, J.D.; Abdeta, C.; Abi Nader, P.; Adeniyi, A.F.; Aguilar-Farias, N.; Tenesaca, D.S.A.; Bhawra, J.; Brazo-Sayavera, J.; Cardon, G.; et al. Global Matrix 3.0 Physical Activity Report Card Grades for Children and Youth: Results and Analysis From 49 Countries. J. Phys. Act. Health 2018, 15, 251–273. [Google Scholar] [CrossRef] [PubMed]
- Guthold, R.; Cowan, M.J.; Autenrieth, C.S.; Kann, L.; Riley, L.M. Physical Activity and Sedentary Behavior among Schoolchildren: A 34-Country Comparison. J. Pediatr. 2010, 157, 43–49.e1. [Google Scholar] [CrossRef] [PubMed]
- Tremblay, M.S.; Barnes, J.D.; González, S.A.; Katzmarzyk, P.T.; Onywera, V.O.; Reilly, J.J.; Tomkinson, G.R. Global Matrix 2.0: Report Card Grades on the Physical Activity of Children and Youth Comparing 38 Countries. J. Phys. Act. Health 2016, 13, S343–S366. [Google Scholar] [CrossRef] [PubMed]
- Huang, W.Y.; Wong, S.H.; Sit, C.H.; Wong, M.C.; Sum, R.K.; Wong, S.W.; Yu, J.J. Results from the Hong Kong’s 2018 report card on physical activity for children and youth. J. Exerc. Sci. Fit. 2019, 17, 14–19. [Google Scholar] [CrossRef]
- Sit, C.H.-P.; Yu, J.J.; Huang, W.Y.; Wong, M.C.-S.; Sum, R.K.-W.; Tremblay, M.S.; Wong, S.H.-S. Results from Hong Kong’s 2019 report card on physical activity for children and youth with special educational needs. J. Exerc. Sci. Fit. 2020, 18, 177–182. [Google Scholar] [CrossRef]
- Biddle, S.J.H.; Gorely, T.; Stensel, D.J. Health-enhancing physical activity and sedentary behaviour in children and adolescents. J. Sports Sci. 2004, 22, 679–701. [Google Scholar] [CrossRef]
- Janssen, I.; Leblanc, A.G. Systematic review of the health benefits of physical activity and fitness in school-aged children and youth. Int. J. Behav. Nutr. Phys. Act. 2010, 7, 40. [Google Scholar] [CrossRef]
- Sothern, M.S.; Loftin, M.; Suskind, R.M.; Udall, J.N.; Blecker, U. The health benefits of physical activity in children and adolescents: Implications for chronic disease prevention. Eur. J. Nucl. Med. Mol. Imaging 1999, 158, 271–274. [Google Scholar] [CrossRef]
- Sallis, J.F.; Prochaska, J.J.; Taylor, W.C. A review of correlates of physical activity of children and adolescents. Med. Sci. Sports Exerc. 2000, 32, 963–975. [Google Scholar] [CrossRef]
- Pate, R.R.; Trilk, J.L.; Byun, W.; Wang, J. Policies to Increase Physical Activity in Children and Youth. J. Exerc. Sci. Fit. 2011, 9, 1–14. [Google Scholar] [CrossRef][Green Version]
- Pate, R.R.; Flynn, J.I.; Dowda, M. Policies for promotion of physical activity and prevention of obesity in adolescence. J. Exerc. Sci. Fit. 2016, 14, 47–53. [Google Scholar] [CrossRef] [PubMed]
- Daugbjerg, S.B.; Kahlmeier, S.; Racioppi, F.; Martin-Diener, E.; Martin, B.; Oja, P.; Bull, F. Promotion of physical activity in the European region: Content analysis of 27 national policy documents. J. Phys. Act. Health 2009, 6, 805–817. [Google Scholar] [CrossRef] [PubMed]
- Department of Health, Hong Kong Special Administration Region of China. Action Plan to Promote Healthy Diet and Physical Activity Participation in Hong Kong. Available online: https://www.change4health.gov.hk/filemanager/common/image/strategic_framework/action_plan/action_plan_e.pdf (accessed on 16 May 2020).
- Department of Health, Hong Kong Special Administration Region of China. Towards 2025: Strategy and Action Plan to Prevent and Control Non-Communicable Diseases in Hong Kong. 2018. Available online: https://www.chp.gov.hk/files/pdf/saptowards2025_fullreport_en.pdf (accessed on 16 May 2020).
- Timperio, A.; Salmon, J.; Ball, K. Evidence-based strategies to promote physical activity among children, adolescents and young adults: Review and update. J. Sci. Med. Sport 2004, 7, 20–29. [Google Scholar] [CrossRef]
- He, G.; Huang, W.Y.; Wong, S.H. Physical activity research in Hong Kong from 1987 to 2012: Evidence on children and adolescents. Asia Pac. J. Public Health 2014, 26, 560–574. [Google Scholar] [CrossRef] [PubMed]
- Whitt-Glover, M.C.; Taylor, W.C.; Floyd, M.F.; Yore, M.M.; Yancey, A.K.; E Matthews, C. Disparities in Physical Activity and Sedentary Behaviors Among US Children and Adolescents: Prevalence, Correlates, and Intervention Implications. J. Public Health Policy 2009, 30, S309–S334. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef]
- Tsang, W.W.; Guo, X.; Fong, S.S.M.; Mak, K.-K.; Pang, M.Y.C. Activity participation intensity is associated with skeletal development in pre-pubertal children with developmental coordination disorder. Res. Dev. Disabil. 2012, 33, 1898–1904. [Google Scholar] [CrossRef]
- Kong, A.P.; Choi, K.C.; Li, A.M.; Hui, S.S.-C.; Chan, M.H.M.; Wing, Y.-K.; Ma, R.C.W.; Lam, C.W.; Lau, J.T.-F.; So, W.Y.; et al. Association between Physical Activity and Cardiovascular Risk in Chinese Youth Independent of Age and Pubertal Stage. BMC Public Health 2010, 10, 303. [Google Scholar] [CrossRef]
- Kwok, S.-Y.; So, H.-K.; Choi, K.-C.; Lo, A.F.C.; Li, A.M.; Sung, R.Y.T.; Nelson, E.A.S. Resting heart rate in children and adolescents: Association with blood pressure, exercise and obesity. Arch. Dis. Child. 2013, 98, 287–291. [Google Scholar] [CrossRef]
- Yu, C.C.; Sung, R.Y.; So, R.C.; Lui, K.C.; Lau, W.; Lam, P.K.; Lau, E.M. Effects of strength training on body composition and bone mineral content in children who are obese. J. Strength Cond. Res. 2005, 19, 667–672. [Google Scholar]
- Rowlands, A.V.; Eston, R.; Louie, L.H.T.; Ingledew, D.K.; Tong, K.K.; Fu, F.H. Physical Activity Levels of Hong Kong Chinese Children: Relationship with Body Fat. Pediatr. Exerc. Sci. 2002, 14, 286–296. [Google Scholar] [CrossRef]
- Wang, J.-J.; Gao, Y.; Lau, P.W.C. Prevalence of overweight in Hong Kong Chinese children: Its associations with family, early-life development and behaviors-related factors. J. Exerc. Sci. Fit. 2017, 15, 89–95. [Google Scholar] [CrossRef]
- Cheung, S.; Mak, J.Y. Physical activity participation and perceived physical competence of children in Hong Kong. J. Bio-Edu. 2004, 2, 21–24. [Google Scholar] [CrossRef]
- Ho, K.; Li, W.H.C.; Lam, K.K.W.; Wei, X.; Chiu, S.; Chan, G.C.-F.; Chung, O.K. Relationships among fatigue, physical activity, depressive symptoms, and quality of life in Chinese children and adolescents surviving cancer. Eur. J. Oncol. Nurs. 2019, 38, 21–27. [Google Scholar] [CrossRef] [PubMed]
- Lam, K.K.; Li, W.H.; Chiu, S.; Chan, G.C. The impact of cancer and its treatment on physical activity levels and quality of life among young Hong Kong Chinese cancer patients. Eur. J. Oncol. Nurs. 2016, 21, 83–89. [Google Scholar] [CrossRef] [PubMed]
- Tse, C.Y.A.; Lee, H.P.; Chan, K.S.K.; Edgar, V.B.; Wilkinson-Smith, A.; Lai, W.H.E. Examining the impact of physical activity on sleep quality and executive functions in children with autism spectrum disorder: A randomized controlled trial. Autism 2019, 23, 1699–1710. [Google Scholar] [CrossRef]
- Lindner, K.J. Sport Participation and Perceived Academic Performance of School Children and Youth. Pediatr. Exerc. Sci. 1999, 11, 129–143. [Google Scholar] [CrossRef]
- Yu, C.C.W.; Chan, S.; Cheng, F.; Sung, R.Y.T.; Hau, K. Are physical activity and academic performance compatible? Academic achievement, conduct, physical activity and self-esteem of Hong Kong Chinese primary school children. Educ. Stud. 2006, 32, 331–341. [Google Scholar] [CrossRef]
- Johns, D.P.; Ha, A.S. Home and recess physical activity of Hong Kong children. Res. Q. Exerc. Sport 1999, 70, 319–323. [Google Scholar] [CrossRef]
- Huang, W.Y.; Wong, S.H.-S. Time use clusters in children and their associations with sociodemographic factors. J. Public Health 2015, 38, e106–e113. [Google Scholar] [CrossRef][Green Version]
- Yu, C.W.; Sung, R.Y.T.; So, R.; Lam, K.; Nelson, E.A.S.; Li, A.M.C.; Yuan, Y.; Lam, P.K.W. Energy expenditure and physical activity of obese children: Cross-sectional study. Hong Kong Med. J. 2002, 8, 313–317. [Google Scholar] [PubMed]
- Lam, J.W.; Sit, C.H.; Cerin, E. Physical activity and sedentary behaviours in Hong Kong primary school children: Prevalence and gender differences. Prev. Med. 2010, 51, 96–97. [Google Scholar] [CrossRef] [PubMed]
- Cheung, P. Children’s after-school physical activity participation in Hong Kong: Does family socioeconomic status matter? Health Educ. J. 2016, 76, 221–230. [Google Scholar] [CrossRef]
- Cheung, P. Teachers as role models for physical activity: Are preschool children more active when their teachers are active? Eur. Phys. Educ. Rev. 2019, 26, 101–110. [Google Scholar] [CrossRef]
- Cheung, P.P. Association of after-school physical activity levels and organized physical activity participation in Hong Kong children. Eur. Phys. Educ. Rev. 2012, 18, 182–190. [Google Scholar] [CrossRef]
- Sit, C.; Lam, J.; McKenzie, T. Direct observation of children’s preferences and activity levels during interactive and on-line electronic games. J. Sci. Med. Sport 2010, 12, e135. [Google Scholar] [CrossRef][Green Version]
- Sit, C.H.P.; Lam, J.W.K.; McKenzie, T.L. Children’s Use of Electronic Games: Choices of Game Mode and Challenge Levels. Int. J. Pediatr. 2010, 2010, 1–6. [Google Scholar] [CrossRef][Green Version]
- Wang, J.; Gao, Y.; Kwok, H.H.; Huang, W.Y.; Li, S.; Li, L. Children with Intellectual Disability Are Vulnerable to Overweight and Obesity: A Cross-Sectional Study among Chinese Children. Child. Obes. 2018, 14, 316–326. [Google Scholar] [CrossRef]
- Sit, C.H.; Lindner, K.J.; Sherrill, C. Sport Participation of Hong Kong Chinese Children with Disabilities in Special Schools. Adapt. Phys. Act. Q. 2002, 19, 453–471. [Google Scholar] [CrossRef]
- Sit, C.H.-P.; Huang, W.Y.; Yu, J.J.; McKenzie, T.L. Accelerometer-Assessed Physical Activity and Sedentary Time at School for Children with Disabilities: Seasonal Variation. Int. J. Environ. Res. Public Health 2019, 16, 3163. [Google Scholar] [CrossRef]
- Leung, K.-M.; Chung, P.-K.; Ransdell, L.B.; Gao, Y. Evaluation of the Psychometric Properties of the Parents’ proxy MPAQ-C in Chinese Population. Meas. Phys. Educ. Exerc. Sci. 2016, 20, 1–9. [Google Scholar] [CrossRef]
- Wang, J.-J.; Baranowski, T.; Lau, W.P.; Chen, T.-A.; Pitkethly, A.J. Validation of the Physical Activity Questionnaire for Older Children (PAQ-C) among Chinese Children. Biomed. Environ. Sci. 2016, 29, 177–186. [Google Scholar] [PubMed]
- Huang, Y.; Wong, S.H.; Salmon, J. Reliability and Validity of the Modified Chinese Version of the Children’s Leisure Activities Study Survey (CLASS) Questionnaire in Assessing Physical Activity among Hong Kong Children. Pediatr. Exerc. Sci. 2009, 21, 339–353. [Google Scholar] [CrossRef]
- Louie, L.H.T.; Chan, L. The Use of Pedometry to Evaluate the Physical Activity Levels among Preschool Children in Hong Kong. Early Child Dev. Care 2003, 173, 97–107. [Google Scholar] [CrossRef]
- Sit, C.H.; Capio, C.M.; Cerin, E.; Mckenzie, T.L. Assessment of measures of physical activity of children with cerebral palsy at home and school: A pilot study. J. Child Adolesc. Behav. 2013, 1, 1–4. [Google Scholar] [CrossRef]
- Suen, Y.N.; Cerin, E.; Mellecker, R. Development and reliability of a scale of physical-activity related informal social control for parents of Chinese pre-schoolers. Int. J. Behav. Nutr. Phys. Act. 2014, 11, 87. [Google Scholar] [CrossRef]
- Cerin, E.; Suen, Y.N.; Barnett, A.; Huang, W.Y.; Mellecker, R. Validity of a scale of neighbourhood informal social control relevant to pre-schoolers’ physical activity: A cross-sectional study. SSM Popul. Health 2016, 3, 57–65. [Google Scholar] [CrossRef]
- Suen, Y.N.; Cerin, E.; Huang, W.Y.; Mellecker, R.R. Measures of Environmental Correlates of Physical Activity for Urban Chinese Preschool-Aged Children: Development and Reliability. SAGE Open 2015, 5. [Google Scholar] [CrossRef]
- Liang, Y.; Lau, P.W.; Huang, W.Y.; Maddison, R.; Baranowski, T. Validity and reliability of questionnaires measuring physical activity self-efficacy, enjoyment, social support among Hong Kong Chinese children. Prev. Med. Rep. 2014, 1, 48–52. [Google Scholar] [CrossRef]
- Wong, M.C.S.; Chen, T.-A.; Baranowski, T.; Lau, P.W.C. Item response modeling: A psychometric assessment of the children’s fruit, vegetable, water, and physical activity self-efficacy scales among Chinese children. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 126. [Google Scholar] [CrossRef]
- Huang, W.Y.; Wong, S.H.-S.; Salmon, J.; Hui, S.S.-C. Reliability and validity of psychosocial and environmental correlates measures of physical activity and screen-based behaviors among Chinese children in Hong Kong. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 16. [Google Scholar] [CrossRef] [PubMed]
- Bauman, A.; Reis, R.S.; Sallis, J.F.; Wells, J.C.; Loos, R.J.F.; Martin, B.W. Lancet Physical Activity Series Working Group. Correlates of physical activity: Why are some people physically active and others not? Lancet 2012, 380, 258–271. [Google Scholar] [CrossRef]
- Sallis, J.F.; Cervero, R.; Ascher, W.L.; Henderson, K.A.; Kraft, M.K.; Kerr, J. An ecological approach to creating active living communities. Annu. Rev. Public Health 2006, 27, 297–322. [Google Scholar] [CrossRef] [PubMed]
- He, G.; Huang, Y.J.; Wong, H.S.; Fung, Y.-P. Neighborhood Built Environment and Physical Activity among Hong Kong Children: A Pilot Study Using GIS. Chin. J. Sports Med. 2015, 34, 431–436. (In Chinese) [Google Scholar]
- He, G.; Cerin, E.; Huang, W.Y.; Wong, S.H. Understanding Neighborhood Environment Related to Hong Kong Children’s Physical Activity: A Qualitative Study Using Nominal Group Technique. PLoS ONE 2014, 9, e106578. [Google Scholar] [CrossRef]
- Chow, B.C.; McKenzie, T.L.; Louie, L.H.T. Children’s Physical Activity and Environmental Influences during Elementary School Physical Education. J. Teach. Phys. Educ. 2008, 27, 38–50. [Google Scholar] [CrossRef]
- Chow, B.C.; McKenzie, T.L.; Louie, L. Children’s Physical Activity and Associated Variables during Preschool Physical Education. Adv. Phys. Educ. 2015, 5, 39–49. [Google Scholar] [CrossRef][Green Version]
- Huang, W.Y.; Wong, S.H.; He, G. Is a Change to Active Travel to School an Important Source of Physical Activity for Chinese Children? Pediatr. Exerc. Sci. 2017, 29, 161–168. [Google Scholar] [CrossRef]
- Cheung, P.P.; Chow, B.C. Parental mediatory role in children’s physical activity participation. Health Educ. 2010, 110, 351–366. [Google Scholar] [CrossRef]
- Leung, K.-M.; Chung, P.-K.; Kim, S. Parental support of children’s physical activity in Hong Kong. Eur. Phys. Educ. Rev. 2016, 23, 141–156. [Google Scholar] [CrossRef]
- Suen, Y.N.; Cerin, E.; Wu, S.L. Parental Practices Encouraging and Discouraging Physical Activity in Hong Kong Chinese Preschoolers. J. Phys. Act. Health 2015, 12, 361–369. [Google Scholar] [CrossRef] [PubMed]
- Chan, C.H.S.; Ha, A.S.; Ng, J.Y.Y.; Lubans, D.R. Associations between fundamental movement skill competence, physical activity and psycho-social determinants in Hong Kong Chinese children. J. Sports Sci. 2018, 37, 229–236. [Google Scholar] [CrossRef] [PubMed]
- Fong, S.S.; Lee, V.Y.; Chan, N.N.; Chan, R.S.; Chak, W.-K.; Pang, M.Y.C. Motor ability and weight status are determinants of out-of-school activity participation for children with developmental coordination disorder. Res. Dev. Disabil. 2011, 32, 2614–2623. [Google Scholar] [CrossRef] [PubMed]
- Yu, J.; Sit, C.H.P.; Capio, C.M.; Burnett, A.; Ha, A.S.C.; Huang, W.Y.J. Fundamental movement skills proficiency in children with developmental coordination disorder: Does physical self-concept matter? Disabil. Rehabil. 2015, 38, 45–51. [Google Scholar] [CrossRef] [PubMed]
- Capio, C.M.; Sit, C.H.; Abernethy, B.; Masters, R.S. Fundamental movement skills and physical activity among children with and without cerebral palsy. Res. Dev. Disabil. 2012, 33, 1235–1241. [Google Scholar] [CrossRef]
- Wang, J.-J.; Baranowski, T.; Lau, P.W.C.; Chen, T.-A.; Zhang, S.-G. Psychological Correlates of Self-Reported and Objectively Measured Physical Activity among Chinese Children—Psychological Correlates of PA. Int. J. Environ. Res. Public Health 2016, 13, 1006. [Google Scholar] [CrossRef]
- Lau, P.W.C.; Lee, A.; Ransdell, L. Parenting Style and Cultural Influences on Overweight Children’s Attraction to Physical Activity. Obesity 2007, 15, 2293–2302. [Google Scholar] [CrossRef]
- Wong, S.H.; Huang, W.Y.; Cerin, E.; Gao, Y.; Lai, P.C.; Burnett, A. Home and neighbourhood environment: Association with children’s physical activity and obesity-related dietary behaviour. Hong Kong Med. J. 2016, 22, 43–47. [Google Scholar]
- Suen, Y.N.; Cerin, E.; Barnett, A.; Huang, W.Y.; Mellecker, R.R. Associations of Socio-demographic, Family, and Neighborhood Factors with Physical Activity-Related Parenting Practices Among Hong Kong Preschoolers’ Parents. Matern. Child Health J. 2019, 23, 678–691. [Google Scholar] [CrossRef]
- Huang, W.Y.; Wong, S.H.; Salmon, J. Correlates of physical activity and screen-based behaviors in Chinese children. J. Sci. Med. Sport 2013, 16, 509–514. [Google Scholar] [CrossRef]
- Lam, K.K.W.; Li, W.H.C.; Ho, K.; Chung, O.K.J.; Chan, C.F.G. Factors contributing to the low physical activity level for Hong Kong Chinese children hospitalised with cancer: An exploratory study. J. Clin. Nurs. 2016, 26, 190–201. [Google Scholar] [CrossRef] [PubMed]
- Sobko, T.; Jia, Z.; Kaplan, M.; Lee, A.; Tseng, C.-H. Promoting healthy eating and active playtime by connecting to nature families with preschool children: Evaluation of pilot study “Play&Grow”. Pediatr. Res. 2016, 81, 572–581. [Google Scholar] [PubMed]
- Wang, J.-J.; Baranowski, T.; Lau, P.W.C.; Buday, R.; Gao, Y. Story Immersion May Be Effective in Promoting Diet and Physical Activity in Chinese Children. J. Nutr. Educ. Behav. 2017, 49, 321–329.e1. [Google Scholar] [CrossRef] [PubMed]
- Wong, E.M.Y.; Cheng, M.M.H. Effects of motivational interviewing to promote weight loss in obese children. J. Clin. Nurs. 2013, 22, 2519–2530. [Google Scholar] [CrossRef]
- McManus, A.M.; Masters, R.S.; Laukkanen, R.M.; Yu, C.C.; Sit, C.H.; Ling, F. Using heart-rate feedback to increase physical activity in children. Prev. Med. 2008, 47, 402–408. [Google Scholar] [CrossRef]
- Capio, C.M.; Sit, C.H.; Eguia, K.F.; Abernethy, B.; Masters, R.S. Fundamental movement skills training to promote physical activity in children with and without disability: A pilot study. J. Sport Health Sci. 2015, 4, 235–243. [Google Scholar] [CrossRef]
- Sit, C.H.-P.; Yu, J.J.; Wong, S.H.-S.; Capio, C.M.; Masters, R. A school-based physical activity intervention for children with developmental coordination disorder: A randomized controlled trial. Res. Dev. Disabil. 2019, 89, 1–9. [Google Scholar] [CrossRef]
- Yu, J.; Sit, C.H.; Burnett, A.; Capio, C.M.; Ha, A.S.; Huang, W.Y. Effects of Fundamental Movement Skills Training on Children with Developmental Coordination Disorder. Adapt. Phys. Act. Q. 2016, 33, 134–155. [Google Scholar] [CrossRef]
- Li, W.H.C.; Chung, J.O.K.; Ho, K.; Chiu, S.Y.; Lopez, V. Effectiveness of an integrated adventure-based training and health education program in promoting regular physical activity among childhood cancer survivors. Psycho-Oncology 2013, 22, 2601–2610. [Google Scholar] [CrossRef]
- Li, W.; Ho, K.Y.; Lam, K.K.W.; Lam, H.; Chiu, S.; Chan, G.C.-F.; Cheung, A.; Ho, L.; Chung, J.O.K. Adventure-based training to promote physical activity and reduce fatigue among childhood cancer survivors: A randomized controlled trial. Int. J. Nurs. Stud. 2018, 83, 65–74. [Google Scholar] [CrossRef]
- Lam, K.K.W.; Li, W.H.C.; Chung, O.K.; Ho, K.; Chiu, S.; Lam, H.; Chan, G.C.-F. An integrated experiential training programme with coaching to promote physical activity, and reduce fatigue among children with cancer: A randomised controlled trial. Patient Educ. Couns. 2018, 101, 1947–1956. [Google Scholar] [CrossRef] [PubMed]
- Goldfield, G.S.; Harvey, A.; Grattan, K.P.; Adamo, K.B. Physical Activity Promotion in the Preschool Years: A Critical Period to Intervene. Int. J. Environ. Res. Public Health 2012, 9, 1326–1342. [Google Scholar] [CrossRef] [PubMed]
- Troiano, R.P.; McClain, J.J.; Brychta, R.J.; Chen, K.Y. Evolution of accelerometer methods for physical activity research. Br. J. Sports Med. 2014, 48, 1019–1023. [Google Scholar] [CrossRef] [PubMed]
- Maxwell, S.E.; Cole, D.A. Bias in cross-sectional analyses of longitudinal mediation. Psychol. Meth 2007, 12, 23–44. [Google Scholar] [CrossRef] [PubMed]
- Taylor, W.; Baranowski, T. Physical Activity, Cardiovascular Fitness, and Adiposity in Children. Res. Q. Exerc. Sport 1991, 62, 157–163. [Google Scholar] [CrossRef] [PubMed]
- Rowlands, A.V.; Eston, R.; Ingledew, D.K. Measurement of Physical Activity in Children with Particular Reference to the Use of Heart Rate and Pedometry. Sports Med. 1997, 24, 258–272. [Google Scholar] [CrossRef]
- Andersen, L.B.; Riddoch, C.; Kriemler, S.; Hills, A.P. Physical activity and cardiovascular risk factors in children. Br. J. Sports Med. 2011, 45, 871–876. [Google Scholar] [CrossRef]
- Pesonen, A.-K.; Sjöstén, N.M.; Matthews, K.A.; Heinonen, K.; Martikainen, S.; Kajantie, E.; Tammelin, T.; Eriksson, J.G.; Strandberg, T.; Räikkönen, K. Temporal Associations between Daytime Physical Activity and Sleep in Children. PLoS ONE 2011, 6, e22958. [Google Scholar] [CrossRef]
- Gu, X.; Chang, M.; Solmon, M.A. Physical Activity, Physical Fitness, and Health-Related Quality of Life in School-Aged Children. J. Teach. Phys. Educ. 2016, 35, 117–126. [Google Scholar] [CrossRef]
- Carroll, B.; Loumidis, J. Children’s perceived competence and enjoyment in physical education and physical activity outside school. Eur. Phys. Educ. Rev. 2001, 7, 24–43. [Google Scholar] [CrossRef]
- Dwyer, T.; Sallis, J.F.; Blizzard, L.; Lazarus, R.; Dean, K. Relation of Academic Performance to Physical Activity and Fitness in Children. Pediatr. Exerc. Sci. 2001, 13, 225–237. [Google Scholar] [CrossRef]
- Metallinos-Katsaras, E.S.; Freedson, P.S.; Fulton, J.E.; Sherry, B. The Association between an Objective Measure of Physical Activity and Weight Status in Preschoolers. Obesity 2007, 15, 686–694. [Google Scholar] [CrossRef] [PubMed]
- Hoelscher, D.M.; Kirk, S.; Ritchie, L.; Cunningham-Sabo, L. Position of the Academy of Nutrition and Dietetics: Interventions for the Prevention and Treatment of Pediatric Overweight and Obesity. J. Acad. Nutr. Diet. 2013, 113, 1375–1394. [Google Scholar] [CrossRef] [PubMed]
- Biddle, S.J.H.; Ciaccioni, S.; Thomas, G.; Vergeer, I. Physical activity and mental health in children and adolescents: An updated review of reviews and an analysis of causality. Psychol. Sport Exerc. 2019, 42, 146–155. [Google Scholar] [CrossRef]
- Ploughman, M. Exercise is brain food: The effects of physical activity on cognitive function. Dev. Neurorehabilit. 2008, 11, 236–240. [Google Scholar] [CrossRef] [PubMed]
- Donnelly, J.E.; Hillman, C.H.; Castelli, D.; Etnier, J.L.; Lee, S.; Tomporowski, P.; Lambourne, K.; Szabo-Reed, A.N. Physical Activity, Fitness, Cognitive Function, and Academic Achievement in Children: A Systematic Review. Med. Sci. Sports Exerc. 2016, 48, 1197–1222. [Google Scholar] [CrossRef]
- Camacho-Miñano, M.J.; LaVoi, N.M.; Barr-Anderson, D.J. Interventions to promote physical activity among young and adolescent girls: A systematic review. Health Educ. Res. 2011, 26, 1025–1049. [Google Scholar] [CrossRef]
- Murphy, N.A.; Carbone, P.S.; American Academy of Pediatrics Council on Children With Disabilities. Promoting the Participation of Children with Disabilities in Sports, Recreation, and Physical Activities. Pediatrics 2008, 121, 1057–1061. [Google Scholar] [CrossRef]
- Shields, N.; Synnot, A.J.; Barr, M. Perceived barriers and facilitators to physical activity for children with disability: A systematic review. Br. J. Sports Med. 2012, 46, 989–997. [Google Scholar] [CrossRef]
- Grant, S.J.; Beauchamp, M.R.; Blanchard, C.M.; Carson, V.; Gardner, B.; Warburton, D.E.R.; Rhodes, R.E. Parents and children active together: A randomized trial protocol examining motivational, regulatory, and habitual intervention approaches. BMC Public Health 2020, 20, 1–14. [Google Scholar] [CrossRef]
- Rhodes, R.E.; Guerrero, M.D.; Vanderloo, L.M.; Barbeau, K.; Birken, C.S.; Chaput, J.-P.; Faulkner, G.; Janssen, I.; Madigan, S.; Mâsse, L.C.; et al. Development of a consensus statement on the role of the family in the physical activity, sedentary, and sleep behaviours of children and youth. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 1–31. [Google Scholar] [CrossRef] [PubMed]
- Lubans, D.R.; Foster, C.; Biddle, S.J.H. A review of mediators of behavior in interventions to promote physical activity among children and adolescents. Prev. Med. 2008, 47, 463–470. [Google Scholar] [CrossRef] [PubMed]
- Martin, J.R.; Chater, A.; Lorencatto, F. Effective behaviour change techniques in the prevention and management of childhood obesity. Int. J. Obes. 2013, 37, 1287–1294. [Google Scholar] [CrossRef] [PubMed]
- Clark, A.M. What are the components of complex interventions in healthcare? Theorizing approaches to parts, powers and the whole intervention. Soc. Sci. Med. 2013, 93, 185–193. [Google Scholar] [CrossRef] [PubMed]
- Craig, P.; Dieppe, P.; MacIntyre, S.; Michie, S.; Nazareth, I.; Petticrew, M. Developing and evaluating complex interventions: The new Medical Research Council guidance. BMJ 2008, 337, a1655. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics | Number of Studies | Percentages | |
|---|---|---|---|
| Year of publication | |||
| 2016–2020 | 25 | 39.7% | |
| 2011–2015 | 20 | 31.7% | |
| 2006–2010 | 11 | 17.5% | |
| 1999–2005 | 7 | 11.1% | |
| Age range of participants | |||
| Preschool children (3–5 years old) | 9 | 14.3% | |
| School-aged children (6–12 years old) | 51 | 81.0% | |
| Preschool and school-aged children (3–12 years old) | 3 | 4.8% | |
| Range of sample size a | |||
| 100 and below | 22 | 36.1% | |
| 101–500 | 24 | 39.3% | |
| 501–1000 | 8 | 13.1% | |
| 1000 and above | 7 | 11.5% | |
| Population | |||
| Healthy children | 44 | 69.8% | |
| Children with special educational needs | 13 | 20.6% | |
| Children with disease b | 6 | 9.6% | |
| Types of special educational needs | |||
| Coordination disorder | 5 | 38.5% | |
| Cerebral palsy | 4 | 30.8% | |
| Multiple disabilities c | 2 | 15.4% | |
| Autism spectrum | 1 | 7.7% | |
| Intellectual disorder | 1 | 7.7% | |
| Study design | |||
| Cross-sectional | 40 | 63.5% | |
| Randomized controlled trial | 10 | 15.9% | |
| Longitudinal | 8 | 12.7% | |
| Qualitative | 3 | 4.7% | |
| Non-randomized controlled trial | 2 | 3.2% | |
| Types of PA measures | |||
| Single type: Self-report | 44 | 69.8% | |
| Single type: Device measured | 11 | 17.5% | |
| Combined type: Self-report & devices | 6 | 9.5% | |
| Single type: Objective observation | 2 | 3.2% | |
| Reference | Characteristics | Design | Health Benefits | Main Findings | ||
|---|---|---|---|---|---|---|
| N | Age | |||||
| [19] | Tsang et al. (2012) | 63 | 6–10 | CS | Skeletal development | Limited PA was related to delayed skeletal development among pre-pubertal children with developmental coordination disorder (r = 0.339, p < 0.05). |
| [20] | Kong et al. (2010) | 2119 | 6–20 | CS | Reduced cardiovascular risk factors | PA was negatively related to Chinese youth’s cardiovascular risk factors (r = −0.455, p = 0.006) after adjusting for sex and pubertal stage. |
| [21] | Kwok et al. (2013) | 14,842 | 6–18 | CS | Resting heart rate | Higher levels of PA was associated with lower levels of resting heart rate (boys: β = −0.13, p < 0.001; girls: β = −0.10, p < 0.001). |
| [22] | Yu et al. (2005) | 82 | 9–12 | RCT | Lean body mass, Total bone mineral content | Obese children’s lean mass and total bone mineral content significantly increased after a six-week exercise program (strength training, aerobic exercise, and agility training). |
| [23] | Rowlands et al. (2002) | 50 | 8–11 | CS | Less body fatness | Objectively measured PA was significantly correlated with sum of skinfolds in boys (r = −0.50, p < 0.05) but not girls. |
| [24] | Wang et al. (2017) | 894 | 9–12 | CS | Prevalence of overweight | PA was not significantly related to prevalence of overweight in Chinese children (AOR = 0.95, 95%CI = 0.73, 1.23; p > 0.05). |
| [25] | Cheung & Mak (2014) | 1012 | 9–14 | CS | Perceived physical competence | PA was significantly related to perceived physical competence (r = 0.354, p < 0.001). |
| [26] | Ho et al. (2019) | 400 | 7–18 | CS | Less cancer fatigue | PA significantly related to fatigue among children surviving cancer (r = −0.56, p < 0.01). |
| [27] | Lam et al. (2016) | 76 | 9–18 | CS | Quality of life | PA predicted life quality among young cancer patients in Hong Kong (β = 0.72, p < 0.001). |
| [28] | Tse et al. (2019) | 40 | 8–12 | RCT | Sleep quality, Executive functions | After 12-week PA intervention of basketball skill learning, children with ASD’s sleep quality and inhibitory control significantly improved, but not working memory capacity. |
| [29] | Lindner (1999) | 4690 | 9–18 | CS | Academic performance | Sport participation significantly related to academic performance of children aged 11–12 (r = 0.12, p < 0.05). |
| [30] | Yu et al. (2006) | 333 | 8–12 | CS | Academic performance | PA was not significantly related to academic performance (r = −0.067, p > 0.05). |
| Reference | Characteristics | Design | PA Measures | Patterns of PA | ||
|---|---|---|---|---|---|---|
| N | Age | |||||
| [31] | Johns & Ha (1999) | 40 | 6–8 | LS | Children’s health evaluation system | Percentage of active time spent at home and school: Active = 18.14%; Very active = 3.04% |
| [32] | Huang & Wang (2015) | 1013 | 9–13 | CS | Children’s Leisure Activities Study Survey | Percentage of children reached recommended PA, and mean MVPA per day: Boys = 9.1%, 178 min, Girl = 11.9%, 165 min. |
| [33] | Yu et al. (2002) | 36 | 7–17 | CS | Diary | Obese children spent 30% less time in physical activity than non-obese children. |
| [34] | Lam et al. (2010) | 1147 | 9–13 | CS | China Health and Nutrition Survey | Outside-school MVPA per week: Boys = 229 min, Girls = 212 min; In-school MVAP per week: Boys = 160 min, Girls = 163 min; Total MVPA per week: Boys = 389 min, Girls = 375 min. |
| [35] | Cheung (2017) | 663 | 6–13 | CS | Three-day physical activity recall | Times of after-school 30-min sports-type activity: Boys = 1.1; Girls = 0.7; Mother’s education/income: High = 0.72/0.75; Medium = 1.04/0.83; Low = 1.23/0.99. Father’s education/income: High = 0.71/0.71; Medium = 1.04/0.74; Low = 1.17/1.00. |
| [36] | Cheng (2020) | 248 | 5–6 | CC | Step count pedometer | Step counts during 30 min PE lesson with active/less active teacher: Boys = 1795/1010 steps; Girls = 1608/889 steps. |
| [37] | Cheung (2012) | 456 | 10–12 | CS | Three-day physical activity recall | After-school 30-min PA participation with/without organized PA: Light intensity PA: 5.55/6.28 times; Moderate intensity PA: 1.24/1.18 times; Hard intensity PA: 0.79/0.42 times; Very hard intensity PA: 0.25/0.05 times. |
| [38] | Sit et al. (2010) JPAH | 70 | 9–12 | LS | System for Observing Fitness Instruction Time | Percentage and averaged MVPA during the 60-min games: Bowling game = 38.9%, 22.4 min; Running game = 52.7%; 29.1 min. |
| [39] | Sit et al. (2010) IJP | 60 | 9–12 | LS | System for Observing Fitness Instruction Time | MVPA during game modes per time: Interactive bowling = 78 min; Computer bowling = 3.7 min; Interactive running game = 98.4 min; Computer running game = 4.3 min. |
| [40] | Wang et al. (2018) | 524 | 8–16 | CS | Global Physical Activity Questionnaire | Disabilities = ID. 6.1% children engaged in MVPA 60 min per day, and 91.6% children engaged in MVPA below 60 min per day. |
| [41] | Sit et al. (2002) | 237 | 9–19 | CS | Sport participation questionnaire | Disabilities = PD, VI, HI, MD, maladjustment. Averaged PA: Frequency = 4–6 times per month, Duration = 10–30 min per time. |
| [42] | Sit et al. (2019) | 270 | 7–18 | LS | ActiGraph accelerometer | Disabilities = VI, HI, PD, ID, and SD. Percentage and averaged MVPA during school day: Winter = 4.5%, 18.6 min, Summer= 4%, 15.6 min. |
| Reference | Characteristics | Measures | Internal Consistency Reliability | Test-Retest Reliability | Criteria-Related Validity | ||
|---|---|---|---|---|---|---|---|
| N | Age | ||||||
| [43] | Leung et al. (2016) | 40 | 6–9 | Modified Physical Activity Questionnaire for Children (MPAQ-C) | α = 0.79 | ICC = 0.94; (n = 32) | Pedometers: r = 0.63 |
| [44] | Wang et al. (2016) | 742 | 8–13 | Physical Activity Questionnaire for Older Children (PAQ-C) | α = 0.79 | ICC = 0.82; (n = 94) | Accelerometer MVPA: r = 0.33 |
| [45] | Huang et al. (2009) | 220 | 9–12 | Modified Chinese version of the Children’s Leisure Activities Study Survey (CLASS) | - | ICC = 0.71; (n = 139) | Accelerometer MVPA: Boy: r = 0.27, Girl: r = 0.48 |
| [46] | Louie & Chan (2003) | 148 | 3.3–5.1 | Yamax Digiwalker DW-200 pedometers | - | - | Children Activity Rating’s Scale: r = 0.64 |
| [47] | Sit et al. (2013) | 5 | 7–13 | Behaviors of Eating and Activity for Children’s Health Evaluation System (BEACHES) | - | - | Children with CP: Accelerometer and active category (ICC = 0.85). |
| [48] | Suen et al. (2014) | 61 a | 3–5 | PA-related neighborhood informal social control scale for parents of preschoolers (PANISC-PP) b | T1: α = 0.74–0.90 T2: α = 0.78–0.90 | ICC = 0.61–0.75; | - |
| [49] | Cerin et al. (2017) | 394 a | 3–5 | PA-related neighborhood informal social control scale for parents of preschoolers (PANISC-PP) b | α = 0.82–0.89 | - | - |
| [50] | Suen et al. (2015) | 61 | 3–5 | Measures of environmental correlates of physical activity for urban Chinese preschool-aged children c | T1: α = 0.67–0.90 T2: α = 0.76–0.91 | ICC = 0.45–0.93 | - |
| [51] | Liang et al. (2014) | 273 | 8–12 | PA Self-efficacy (PASE); Adapted PA Enjoyment Scale (PAES); PA social support: social support from family (SSFA); social support from friends (SSFR). | PASE: α = 0.78 PAES: α = 0.90 SSFA: α = 0.86 SSFR: α = 0.90 | PASE: ICC = 0.88 PAES: ICC = 0.82 SSFA: ICC = 0.86 SSFR: ICC = 0.91 | Self-reported PA: PASE: r = 0.40, PAES: r = 0.23, SSFA: r = 0.40, SSFR: r = 0.35 |
| [52] | Wang et al. (2017) | 763 | 8–13 | Self-efficacy for physical activity (PASE) d | α = 0.91 | - | - |
| [53] | Huang et al. (2011) | 303 | 9–14 | Psychosocial and environmental correlates measures of PA and screen-based behaviors d | α = 0.50–0.75 | ICC = 0.78–0.89 | MVPA: Self-efficacy (r = 0.25), home PA environment (r = 0.14) and peer support for PA (r = 0.25). |
| Reference | Characteristics | Design | Correlates | Main Findings | ||
|---|---|---|---|---|---|---|
| N | Age | |||||
| Community-level correlates | ||||||
| [56] | He et al. (2015) | 81 | 7–11 | LS | Neighborhood environment | Children in the close-to-recreational-facility neighborhood had a higher level of accelerometer-measured MVPA as compared to children in the far-to-recreational-facility neighborhood (p < 0.05). |
| [57] | He et al. (2014) | 34 | 10–11 | QS | Neighborhood environment | 16 environmental factors perceived as most important to children’s PA, including facilitators (e.g., sufficient lighting, bridge or tunnel, few cars on roads, and convenient transportation), and barriers (e.g., crimes nearby, too much noise, and too many people in recreation grounds). |
| Organizational correlates | ||||||
| [58] | Chow et al. (2008) | 105 a | 9–12 | LS | Environmental; Instructor-related characteristics | Lesson context (β = 0.29), lesson content (β = 0.23), temperature (β = 0.20), and active teacher behavior (β = 0.25) significantly predicted children’s MVPA percentage during PE lessons. |
| [59] | Chow et al. (2015) | 25 a | 3–6 | CS | Teachers’ behavior during structured PE lessons | Proportion of lesson time teachers spent instructing (r = −0.21) and managing (r = −0.26) negatively related to children’s PA. Proportion of time teachers spent observing students positively related to children’s PA (r = 0.29). |
| [60] | Huang et al. (2017) | 677 | 7–10 | LS | School travel modes | A change from passive to active travel to school was positively associated with changes in the percentage of time spent in MVPA (β = 1.76). |
| Interpersonal correlates | ||||||
| [61] | Cheung & Chow (2010) | 872 | 10–13 | CS | Parental influence | Parental influence imposed a total (β = 0.31) effect on children’s PA, which is divided as direct (β = 0.19) and indirect effect via children’s PA perception and physical self-perceptions (β = 0.12). |
| [62] | Leung et al. (2017) | 478 b | 6–9 | CS | Parental support; parents’ perceived competence & exercise benefits of children | Parents’ perceived children’s competence (β = 0.18) and exercise benefits (β = 0.29) predicted parental support, which in turn predicted children’s PA (β = 0.68). |
| [63] | Suen et al. (2015) | 45 | 3–5 | QS | Parental provision | Parental provision of instrumental, motivational, and conditional support can encourage child’s PA. Parental safety concerns, focusing on academic achievement, lack of time and resources, promotion of sedentary behaviors could discourage child’s PA. |
| Individual correlates | ||||||
| [64] | Chan et al. (2019) | 763 | 7–11 | CS | FMS; Locomotor skills | Locomotor skills significantly related to perceived movement skill competence (β = 0.11), and perceived movement skill competence significantly related to objective PA (β = 0.59). Locomotor skills related to self-reported PA via perceived physical competence and enjoyment (β = 0.08). |
| [65] | Fong et al. (2011) | 81 | 3–16 | CS | Motor ability | Motor ability was positively associated with PA among children with developmental coordination disorder in Hong Kong (r = 0.264). |
| [66] | Yu et al. (2016) | 130 | 7–10 | CS | FMS proficiency | FMS proficiency was positively related to PA in Hong Kong children with respect to locomotor skill (r = 0.21) and running (r = 0.26). |
| [67] | Capio et al. (2012) | 62 | 4–10 | CS | FMS proficiency | Weekdays PA was significantly and positively related to process-oriented (β = 0.406–0.717) and product-oriented (β = 0.333–0.556) FMS proficiency among children with cerebral palsy. Similar patterns revealed for weekend PA and FMS proficiency. |
| [68] | Wang et al. (2016) | 449 | 8–13 | CS | Self-efficacy; autonomous motivation | Self-efficacy (r = 0.63) and autonomous (r = 0.50) motivation were positively associated with PA. |
| Correlates from multiple levels | ||||||
| [69] | Lau et al. (2007) | 104 | 8–12 | CS | Parental influence; Child’s perceived competence | Father’s role modeling significantly predicted attraction to PA in overweight boys (β = 0.46) but not girls. Child’s perceived competence significantly predicted the attraction to PA by both boys (β = 0.63) and girls (β = 0.66). |
| [70] | Wong et al. (2016) | 1265 | 8–12 | CS | Home and neighborhood environments | Parental role modelling for physical activity (β = 0.046 and β = 0.146) and preference for outdoor play (β = −0.059 and β = −0.11) significantly related to objective and subjective MVPA. Attractive natural sights significantly related to objective MVPA (β = 0.101), social network significantly related to subjective MVPA (β = 0.095). |
| [71] | Suen et al. (2019) | 411 b | 3–5 | CS | Socio-demographic, family/home characteristics, neighborhood environments | Socio-demographic and family/home characteristics significantly related to parenting practices encouraging and discouraging PA. Parent-perceived neighborhood characteristics significantly related to parenting practices discouraging PA only. |
| [72] | Huang et al. (2013) | 303 | 8–15 | CS | Neighborhood environment; school sports teams; family and peer support; self-efficacy | After adjusting age and other significant correlates, self-efficacy (B = 0.89), school sport teams (B = 1.77) significantly associated with MVPA for boys. School sport teams (B = 1.50), homework (B = 0.19), peer support for PA (B = 0.95), and home PA environment (B = 1.21) significantly associated with PA for girls. |
| [73] | Lam et al. (2016) | 25 | 9–18 | QS | Factors contributing to low PA levels for Chinese children with cancer | Qualitative findings revealed that physical condition, misunderstanding about physical activity, emotional disturbances, and social influences had negative impacts on PA among children hospitalized with cancer. |
| Reference | Characteristics | Design | Interventions | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| N | Age | IG and CG | Weeks | Treatment | PA Measures | Time of Measures | Main Findings | |||
| [74] | Sobko et al. (2017) | 240 | 2–4 | One group | IG: Modified “Play&Grow” program. | 12 | 45 min, once per week | IPAQ | Baseline and post-intervention. | No significant improvement on PA after intervention. |
| [75] | Wang et al. (2017) | 179 | 8–12 | QE-RCT | IG: Video game (Diab) CG: No intervention. | 8–10 | 40 min, once per week. | PAQ-C; ActiGraph GT3X. | Baseline, post-intervention, and 8–10 week post-intervention. | Self-reported PA significantly increased after intervention (mean difference = 1.9, p < 0.05), but not maintained after 8–10 weeks. |
| [76] | Wong & Cheng (2013) | 185 | 9–11 | QE-RCT | IG1: MI + ; a IG2: MI; a CG: No intervention | 14 | 30 min, six-section program | 7 consecutive days self-record exercise log. | Baseline and post-intervention. | Both MI+ and MI improved PA. MI+ had more calorie consumed from PA than MI (F = 5.24, p = 0.02) |
| [77] | McManus et al. (2008) | 210 | 9–11 | CT | IG-E: Education + HR feedback IG-NE: HR feedback CG: No intervention. | 4 | 2 weeks with heart rate feedback, and 2 weeks without. | HR; Children’s attraction to physical activity scale. | Baseline, during intervention, and 6 month post-intervention. | HR feedback increased total daily PA (24%, p < 0.001) and vigorous PA (0.6%, p < 0.05), but effects do not persist when feedback removed. |
| [78] | Capio et al. (2014) | 50 | 3–10 | RCT | TP & Disabilities: CP IG: FMS training CG: No intervention | 4 | 45 min, once per week | Uni-axial accelerometers | 7-day pre and post intervention. | Significant changes in weekday PA for both training groups. Weekend MVPA significantly increased for FMS training of children with CP. |
| [79] | Sit et al. (2019) | 131 | 6–10 | RCT | TP & Disabilities: DCD IG: FMS training CG: Conventional PE lessons | 8 | 40 min, once per week | ActiGraph active monitor (GT3X). | Baseline, post-intervention, 1 week, 3&12 months post intervention. | FMS training improved %MVPA on weekdays in all time of measurements, and weekends in 3-months after intervention. |
| [80] | Yu et al. (2016) | 84 | 7–10 | RCT | TP & Disabilities: DCD IG: FMS training CG: No intervention | 6 | 35 min, twice per week | ActiGraph active monitor (GT3X). | Baseline, post-intervention, & 6-weeks post intervention. | Significant interaction effects on PA volume (p = 0.043) and light PA (p = 0.026) but no significant main and interaction effects for MVPA. |
| [81] | Li et al. (2013) | 71 | 9–16 | RCT | Disease: Cancer IG: 4-day adventure-based training & health education. CG: Placebo. | 4 days | 40 min, per session in day 1–3; 90 min for day 4 session. | CUHK Physical Activity Rating for Children and Youth | Baseline, & 3, 6, 9 months after the beginning of intervention. | Experimental group showed significantly higher PA stages of change (p < 0.001) and PA (p < 0.001) than control group at all follow-ups. |
| [82] | Li et al. (2018) | 222 | 9–16 | RCT | Disease: Cancer IG: 4-day adventure-based training program CG: Placebo. | 4 days | From 09:00 to 16:45 per day | CUHK Physical Activity Rating for Children and Youth | Baseline, 6 and 12 months after the intervention began. | Experimental group improved PA levels than control group at the 6-month (p < 0.001) and 12-month (p < 0.001) follow-ups. |
| [83] | Lam et al. (2018) | 70 | 9–18 | RCT | Disease: Cancer IG: Integrated experiential training + home visit. CG: Placebo. | 24 | 60 min, once per week. | CUHK Physical Activity Rating for Children and Youth | Baseline, and 6 and 9 months after the beginning of intervention. | Experimental group improved PA levels than control group at the 6-month (p < 0.001) and 9-month (p < 0.001) after start of intervention. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, C.-Q.; Chung, P.-K.; Cheng, S.-S.; Yeung, V.W.-C.; Zhang, R.; Liu, S.; Rhodes, R.E. An Update on Physical Activity Research among Children in Hong Kong: A Scoping Review. Int. J. Environ. Res. Public Health 2020, 17, 8521. https://doi.org/10.3390/ijerph17228521
Zhang C-Q, Chung P-K, Cheng S-S, Yeung VW-C, Zhang R, Liu S, Rhodes RE. An Update on Physical Activity Research among Children in Hong Kong: A Scoping Review. International Journal of Environmental Research and Public Health. 2020; 17(22):8521. https://doi.org/10.3390/ijerph17228521
Chicago/Turabian StyleZhang, Chun-Qing, Pak-Kwong Chung, Shi-Shi Cheng, Vincent Wing-Chun Yeung, Ru Zhang, Sam Liu, and Ryan E. Rhodes. 2020. "An Update on Physical Activity Research among Children in Hong Kong: A Scoping Review" International Journal of Environmental Research and Public Health 17, no. 22: 8521. https://doi.org/10.3390/ijerph17228521
APA StyleZhang, C.-Q., Chung, P.-K., Cheng, S.-S., Yeung, V. W.-C., Zhang, R., Liu, S., & Rhodes, R. E. (2020). An Update on Physical Activity Research among Children in Hong Kong: A Scoping Review. International Journal of Environmental Research and Public Health, 17(22), 8521. https://doi.org/10.3390/ijerph17228521