Unmet Healthcare Needs of Children in Vulnerable Families in South Korea: Finding from the Community Child Center Child Panel Survey

Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
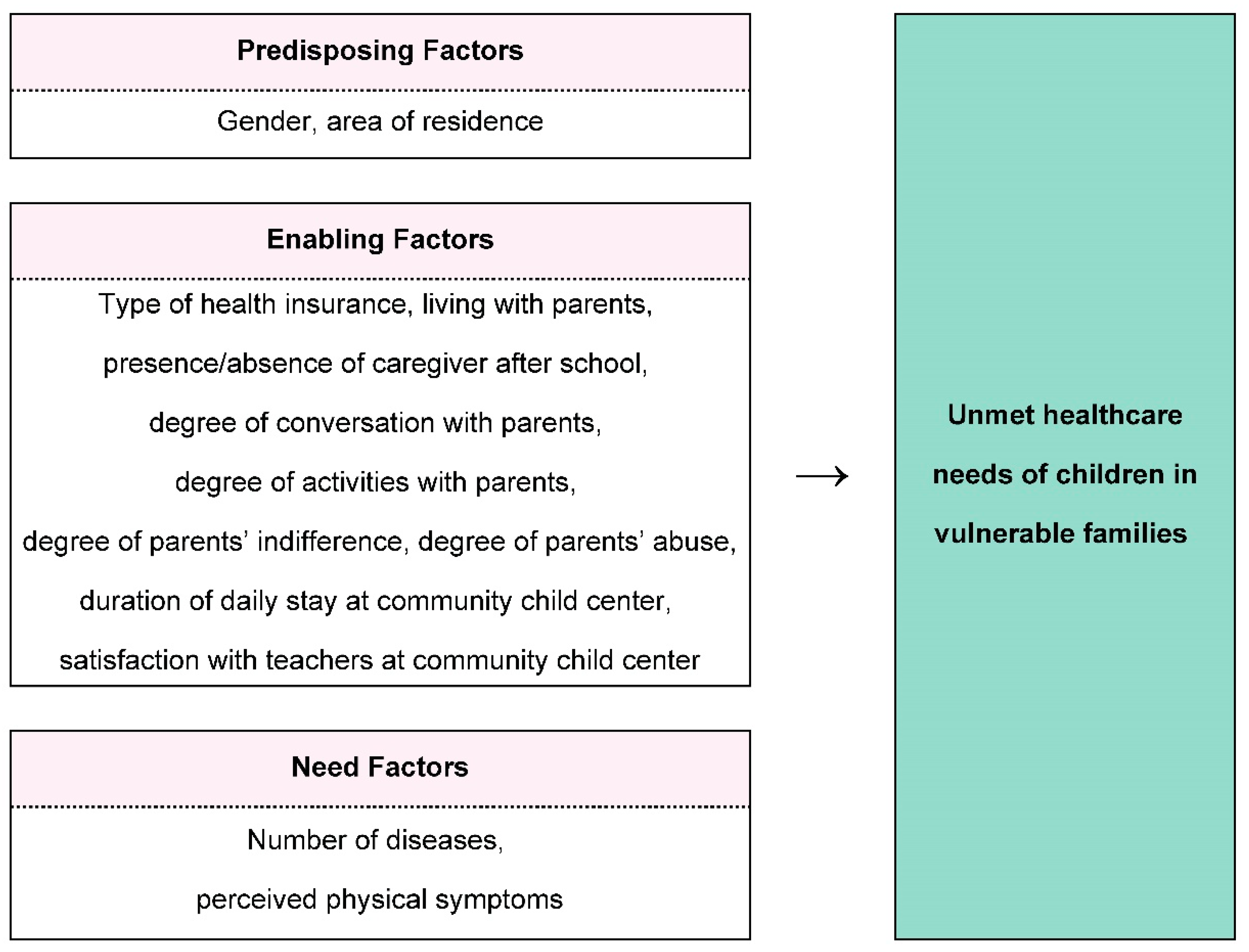
2.2. Conceptual Framework
2.2.1. Andersen Model Factors
2.2.2. Unmet Healthcare Needs
2.3. Data Source and Participants
2.4. Ethical Consideration
2.5. Selection and Definition of Study Variables
2.5.1. Unmet Healthcare Needs
2.5.2. Predisposing Factors
2.5.3. Enabling Factors
2.5.4. Need Factors
2.6. Data Analysis
3. Results
3.1. Participants’ Characteristics and Unmet Healthcare Needs
3.2. Unmet Healthcare Needs by Characteristics of Children in Vulnerable Families
3.3. Factors Affecting Unmet Healthcare Needs of Children in Vulnerable Families
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Ministry of Health and Welfare. National Health Plan 2020; Ministry of Health and Welfare: Seoul, Korea, 2011.
- Yeo, E. Current condition and policy issues of child poverty in Korea. Health Welf. Policy Forum 2018, 259, 25–39. [Google Scholar]
- Ministry of Gender Equality and Family. Survey of Single Parent Family; Ministry of Gender Equality and Family: Seoul, Korea, 2018.
- Hernandez, V.R.; Montana, S.; Clarke, K. Child health inequality: Framing a social work response. Health Soc. Work 2010, 35, 291–301. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.S. Health disparity and health welfare among children from low-income families. Child Health Nurs. Res. 2013, 19, 247–251. [Google Scholar] [CrossRef]
- Lim, M.S. A Study of improvements in the treatment of local children’s center workers. Korean J. Educ. Res. 2016, 37, 15–32. [Google Scholar]
- Kim, K. Korean child’s right to live: The actual conditions and change of poverty, family, environment, safety and health. J. Child Rights 2010, 14, 1–39. [Google Scholar]
- Kim, E.; Kim, K.; Yoo, D. Comparison of health care utilization and morbidity of children with and without disabilities in Korea. J. Korea 2017, 17, 696–706. [Google Scholar] [CrossRef]
- Carr, W.; Wolfe, S. Unmet needs as sociomedical indicators. Int. J. Health Serv. 1976, 6, 417–430. [Google Scholar] [CrossRef] [PubMed]
- Diamant, A.L.; Hays, R.D.; Morales, L.S.; Ford, W.; Calmes, D.; Asch, S.; Duan, N.; Fielder, E.; Kim, S.; Fielding, J.; et al. Delays and unmet need for health care among adult primary care patients in a restructured urban public health system. Am. J. Public Health 2004, 94, 783–789. [Google Scholar] [CrossRef] [PubMed]
- Andersen, R.M. Revisiting the behavioral model and access to medical care: Does it matter? J. Health Soc. Behav. 1995, 36, 1–10. [Google Scholar] [CrossRef]
- Andersen, R.; Newman, J.F. Societal and individual determinants of medical care utilization in the United States. The Milbank Memorial Fund Quarterly. Health Soc. 1973, 83, 95–124. [Google Scholar]
- Kim, J. Factors affecting the choice of medical care use by the poor. Korean J. Soc. Welfare Stud. 2008, 37, 5–33. [Google Scholar] [CrossRef]
- Kim, S.; Lee, C. Analysis of factors affecting unmet healthcare needs of married immigrant women. J. Korean Acad. Nurs. 2013, 43, 770–780. [Google Scholar] [CrossRef] [PubMed]
- Song, K.S.; Lee, J.H.; Rhim, K.H. Factors associated with unmet needs for health care. Korean Public Health Res. 2011, 37, 131–140. [Google Scholar]
- Naavaal, S.; Barker, L.K.; Griffin, S.O. The effect of health and dental insurance on US children’s dental care utilization for urgent and non-urgent dental problems—2008. J. Public Health Dent. 2017, 77, 54–62. [Google Scholar] [CrossRef]
- Graham, A.; Hasking, P.; Brooker, J.; Clarke, D.; Meadows, G. Mental health service use among those with depression: An exploration using Andersen’s behavioral model of health service use. J. Affect Disord. 2017, 208, 170–176. [Google Scholar] [CrossRef]
- Vingilis, E.; Wade, T.; Seeley, J. Predictors of adolescent health care utilization. J. Adoles. 2007, 30, 773–800. [Google Scholar] [CrossRef]
- Ministry of Health and Welfare. The National Community Child Care Center Statistical Survey Report 2018; Ministry of Health and Welfare: Seoul, Korea, 2019. Available online: https://www.icareinfo.go.kr/ (accessed on 16 October 2020).
- Ministry of Health and Welfare. Report for Community Child Center Support Project; Ministry of Health and Welfare: Seoul, Korea, 2019.
- Headquarters for Community Child Centers. Community Child Center Child Panel Survey; Headquarters for Community Child Centers: Seoul, Korea, 2018. [Google Scholar]
- Huh, S.I.; Kim, S.J. Unmet needs for health care among Korean adults: Differences across age groups. Korean J. Health Econ. Policy 2007, 13, 1–16. [Google Scholar]
- Pledger, M.J.; Cumming, J.; Burnette, M.; Daubé, J. Unmet need of GP services in Pacific people and other New Zealanders. N. Z. Med. J. 2011, 124, 35–45. [Google Scholar]
- Huh, M. The Study for the Development and Validation of “Parenting Behavior Inventory” Perceived by Adolescents. Doctoral Dissertation, Ewha Womans University, Seoul, Korea, 1999. [Google Scholar]
- Jo, B.; Im, G. Development and validation of Emotional or Behavioral Problems Scale. Korean J. Counsel. Psychother. 2003, 15, 729–746. [Google Scholar]
- McDonald, J.H. Handbook of Biological Statistics, 3rd ed.; Sparky House Publishing: Baltimore, MD, USA, 2014. [Google Scholar]
- Lee, J.Y.; Lee, E.Y. Health Medical Statistics; Gyechuk Munwhasa: Seoul, Korea, 2008. [Google Scholar]
- Hargreaves, D.S.; Elliott, M.N.; Viner, R.M.; Richmond, T.K.; Schuster, M.A. Unmet health care need in US adolescents and adult health outcomes. Pediatrics 2015, 136, 513–520. [Google Scholar] [CrossRef]
- Edelstein, B.L.; Chinn, C.H. Update on disparities in oral health and access to dental care for America’s children. Acad. Pediatr. 2009, 9, 415–419. [Google Scholar] [CrossRef]
- Flores, G.; Tomany-Korman, S.C. Racial and ethnic disparities in medical and dental health, access to care, and use of services in US children. Pediatrics 2008, 121, e286–e298. [Google Scholar] [CrossRef]
- Toomey, S.L.; Chien, A.T.; Elliott, M.N.; Ratner, J.; Schuster, M.A. Disparities in unmet need for care coordination: The national survey of children’s health. Pediatrics 2013, 131, 217–224. [Google Scholar] [CrossRef] [PubMed]
- Statistics Korea. Health Insurance Patient Care Expense Survey. 2018. Available online: http://kostat.go.kr/portal/korea/index.action (accessed on 19 October 2020).
- Kim, S.A.; SEO, Y.; Woo, K.S.; Shin, Y. A systematic review of studies on current status and influencing factors of unmet medical needs in Korea. J. Crit. Soc. Welf. 2019, 62, 53–92. [Google Scholar] [CrossRef]
- Korea Institute for Health and Social Affairs. Health Status of Marriage Immigrant Women and Children from Multicultural Families and Health Policy Recommendations; Korea Institute for Health and Social Affairs: Seoul, Korea, 2012. [Google Scholar]
- Kim, S.; Huh, S. Financial burden of health care expenditures and unmet needs by socioeconomic status. Korean J. Health Econ. Policy 2011, 17, 47–70. [Google Scholar]
- Pocock, B.; Clarke, J. Can’t Buy Me Love? Young Australian’s Views on Parental Work, Time, Guilt and Their Own Consumption (Discussion Paper No. 61); The Australia Institute: Canberra, Australia, 2004. [Google Scholar]
- Lee, J. Health inequality in children and adolescents: A review with implications for the sociology of education. Korean J. Sociol. Educ. 2016, 26, 69–95. [Google Scholar] [CrossRef]
- Brown, N.M.; Green, J.C.; Desai, M.M.; Weitzman, C.C.; Rosenthal, M.S. Need and unmet need for care coordination among children with mental health conditions. Pediatrics 2014, 133, e530–e537. [Google Scholar] [CrossRef]
- Williams, K.A.; Chapman, M.V. Unmet health and mental health need among adolescents: The roles of sexual minority status and child-parent connectedness. Am. J. Orthopsychiatry 2012, 82, 473–481. [Google Scholar] [CrossRef]
- De Panfilis, D.; Dubowitz, H. Family connections: A program for preventing child neglect. Child Maltreat. 2005, 10, 108–123. [Google Scholar] [CrossRef]
- Erickson, M.F.; Egeland, B. Child neglect. In The APSAC Handbook on Child Maltreatment; Myers, J.E.B., Berliner, L., Briere, J., Hendrix, C.T., Jenny, C., Reid, T.A., Eds.; Sage Publications Inc.: Thousand Oaks, CA, USA.
- National Child Protection Agency. Child Abuse & Neglect Korea 2016; National Child Protection Agency: Seoul, Korea, 2016.
- Fong, H.F.; Alegria, M.; Bair-Merritt, M.H.; Beardslee, W. Factors associated with mental health services referrals for children investigated by child welfare. Child Abus. Negl. 2018, 79, 401–412. [Google Scholar] [CrossRef]
- Kim, D. A study on the longitudinal trajectories of use time and the related factors for the children in community children centers. Korean J. Soc. Welf. Stud. 2018, 49, 159–180. [Google Scholar] [CrossRef]
- Shin, S.; Jang, J.; Kim, C. The oral health behaviors for children and teachers by teacher-supervised toothbrushing in community child center. J. Dent. Hyg. Sci. 2012, 12, 572–582. [Google Scholar]
- Moon, J.; Kang, M. The Prevalence and Predictors of Unmet Medical Needs among the Elderly Living Alone in Korea: An Application of the Behavioral Model for Vulnerable Populations. Health. Soc. Welf. Rev. 2016, 36, 480–510. [Google Scholar]
- Kim, D.E.; Ahn, S. Factors Influencing Unmet Healthcare Needs among the Elderly with Cognitive Impairment in Korea. J. Korean Acad. Nurs. Adm. 2020, 26, 100–109. [Google Scholar] [CrossRef]
- Chuang, E.; Wells, R.; Aarons, G.A. Identifying depression in a national sample of caregivers investigated in regard to their child’s welfare. Psychiatr. Serv. 2014, 65, 911–917. [Google Scholar] [CrossRef]
- King, C.; Khanijahani, A. Unmet health care needs among children of mothers exposed to violence. Child Abus. Negl. 2020, 101, 104363. [Google Scholar] [CrossRef]
- Thompson, R.; Lindsey, M.A.; English, D.J.; Hawley, K.M.; Lambert, S.; Browne, D.C. The influence of family environment on mental health need and service use among vulnerable children. Child. Welf. 2007, 86, 57–74. [Google Scholar]
- Cornelius, J.R.; Pringle, J.; Jernigan, J.; Kirisci, L.; Clark, D.B. Correlates of mental health service utilization and unmet need among a sample of male adolescents. Addict. Behav. 2001, 26, 11–19. [Google Scholar] [CrossRef]
- Bhandari, A.; Wagner, T. Self-reported utilization of health care services: Improving measurement and accuracy. Med. Care Res. Rev. 2006, 63, 217–235. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics | Category | n (%) | Total Score (M ± SD) | Item Score (M ± SD) | |
|---|---|---|---|---|---|
| Predisposing factors | Gender | Boys | 146 (42.9) | ||
| Girls | 194 (57.1) | ||||
| Area of residence | Metropolitan region | 128 (37.6) | |||
| Non-metropolitan region | 212 (62.4) | ||||
| Enabling factors | Type of health insurance | National Health Insurance | 149 (43.8) | ||
| Medical Aid | 191 (56.2) | ||||
| Living with parents | Both parents | 224 (65.9) | |||
| One parent/other | 116 (34.1) | ||||
| Caregiver after school | Present | 167 (49.1) | |||
| Absent (one day or more/week) | 173 (50.9) | ||||
| Degree of conversation with parents | 8.2 ± 3.5 | 2.1 ± 0.9 | |||
| Degree of activities with parents | 5.6 ± 2.3 | 2.8 ± 1.1 | |||
| Degree of indifference by parents | 6.3 ± 2.5 | 2.1 ± 0.8 | |||
| Degree of abuse by parents | 5.2 ± 2.0 | 2.6 ± 1.0 | |||
| Duration of daily stay at CCC (min) | 174.9 ± 75.1 | 174.9 ± 75.1 | |||
| Satisfaction with teachers at CCC | 18.5 ± 4.3 | 3.7 ± 0.9 | |||
| Need factors | Number of diseases | 1.6 ± 1.0 | 1.6 ± 1.0 | ||
| Perceived physical symptoms | 15.0 ± 4.8 | 1.9 ± 0.6 | |||
| Unmet healthcare needs | Yes | 96 (28.2) | |||
| No | 244 (71.8) | ||||
| Factor | Characteristics | Category | Unmet Healthcare Needs | χ2 or t | p | Φ (p)/ Cohen’s d | |
|---|---|---|---|---|---|---|---|
| Yes | No | ||||||
| Predisposing factors | Gender | Boys | 39 (26.7) | 107 (73.3) | 0.18 | 0.68 | 0.03 (0.59) |
| Girls | 57 (29.4) | 137 (70.6) | |||||
| Area of residence | Metropolitan region | 38 (29.7) | 90 (70.3) | 0.11 | 0.74 | −0.03 (0.64) | |
| Non-metropolitan region | 58 (27.4) | 154 (72.6) | |||||
| Enabling factors | Type of health insurance | National Health Insurance | 47 (31.5) | 102 (68.5) | 1.16 | 0.28 | 0.07 (0.23) |
| Medical Aid | 49 (25.7) | 142 (74.3) | |||||
| Living with parents | Both parents | 65 (29.0) | 159 (71.0) | 0.1 | 0.75 | −0.02 (0.66) | |
| One parent/other | 31 (26.7) | 85 (73.3) | |||||
| Caregiver after school | Present | 37 (22.2) | 130 (77.8) | 5.41 | 0.02 | 0.13 (0.01) | |
| Absent (one day or more/week) | 59 (34.1) | 114 (65.9) | |||||
| Degree of conversation with parents | 2.1 ± 0.8 | 2.0 ± 0.1 | −0.28 | 0.78 | −0.03 | ||
| Degree of activities with parents | 2.8 ± 1.2 | 2.8 ± 1.1 | 0.97 | 0.84 | 0.02 | ||
| Degree of indifference by parents | 2.3 ± 0.8 | 2.0 ± 0.8 | −3.17 | 0.002 * | −0.38 | ||
| Degree of abuse by parents | 2.7 ± 1.0 | 2.6 ± 1.0 | −1.13 | 0.26 | −0.14 | ||
| Duration of daily stay at CCC (min) | 188.6 ± 86.1 | 169.6 ± 69.7 | −2.12 | 0.04 | −0.25 | ||
| Satisfaction with teachers at CCC | 3.4 ± 0.8 | 3.8 ± 0.8 | 4.05 | <0.001 * | 0.48 | ||
| Need factors | Number of diseases | 1.5 ± 0.9 | 1.6 ± 1.0 | 0.73 | 0.47 | 0.09 | |
| Perceived physical symptoms | 2.0 ± 0.6 | 1.8 ± 0.6 | −2.69 | 0.01 * | −0.32 | ||
| Factor | Characteristics | Category | Model 1 | Model 2 | Model 3 |
|---|---|---|---|---|---|
| OR (95% CI) | OR (95% CI) | OR (95% CI) | |||
| Predisposing factors | Gender | Boys (ref.) | 1 | 1 | 1 |
| Girls | 1.13 (0.70, 1.83) | 1.24 (0.73, 2.10) | 1.15 (0.67, 1.98) | ||
| Area of residence | Metropolitan region (ref.) | 1 | 1 | 1 | |
| Non-metropolitan region | 0.90 (0.55, 1.46) | 0.98 (0.57, 1.68) | 0.95 (0.55, 1.64) | ||
| Enabling factors | Type of health insurance | National Health Insurance (ref.) | 1 | 1 | |
| Medical Aid | 0.86 (0.51, 1.47) | 0.88 (0.51, 1.51) | |||
| Living with parents | Both parents (ref.) | 1 | 1 | ||
| One parent/other | 0.93 (0.53, 1.66) | 0.92 (0.52, 1.65) | |||
| Caregiver after school | Present (ref.) | 1 | 1 | ||
| Absent (one day or more/week) | 1.97 (1.17, 3.29) * | 1.95 (1.16, 3.27) * | |||
| Degree of conversation with parents | 1.15 (0.84, 1.56) | 1.12 (0.82, 1.54) | |||
| Degree of activities with parents | 1.00 (0.74, 1.34) | 1.02 (0.76, 1.38) | |||
| Degree of indifference by parents | 1.40 (1.06, 1.85) * | 1.33 (1.002, 1.77) * | |||
| Degree of abuse by parents | 1.17 (0.90, 1.52) | 1.13 (0.87, 1.47) | |||
| Duration of daily stay at CCC (min) | 1.28 (0.99, 1.65) | 1.32 (1.01, 1.71) * | |||
| Satisfaction with teachers at CCC | 0.66 (0.51, 0.87) * | 0.65 (0.49, 0.85) * | |||
| Need factors | Number of diseases | 0.83 (0.64, 1.08) | |||
| Perceived physical symptoms | 1.33 (1.02, 1.73) * | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baek, S.; Choi, E.-H.; Lee, J. Unmet Healthcare Needs of Children in Vulnerable Families in South Korea: Finding from the Community Child Center Child Panel Survey. Int. J. Environ. Res. Public Health 2020, 17, 8241. https://doi.org/10.3390/ijerph17218241
Baek S, Choi E-H, Lee J. Unmet Healthcare Needs of Children in Vulnerable Families in South Korea: Finding from the Community Child Center Child Panel Survey. International Journal of Environmental Research and Public Health. 2020; 17(21):8241. https://doi.org/10.3390/ijerph17218241
Chicago/Turabian StyleBaek, Suyon, Eun-Hi Choi, and Jungeun Lee. 2020. "Unmet Healthcare Needs of Children in Vulnerable Families in South Korea: Finding from the Community Child Center Child Panel Survey" International Journal of Environmental Research and Public Health 17, no. 21: 8241. https://doi.org/10.3390/ijerph17218241
APA StyleBaek, S., Choi, E.-H., & Lee, J. (2020). Unmet Healthcare Needs of Children in Vulnerable Families in South Korea: Finding from the Community Child Center Child Panel Survey. International Journal of Environmental Research and Public Health, 17(21), 8241. https://doi.org/10.3390/ijerph17218241