A Review of Knowledge, Belief and Practice Regarding Osteoporosis among Adolescents and Young Adults



Abstract
1. Introduction
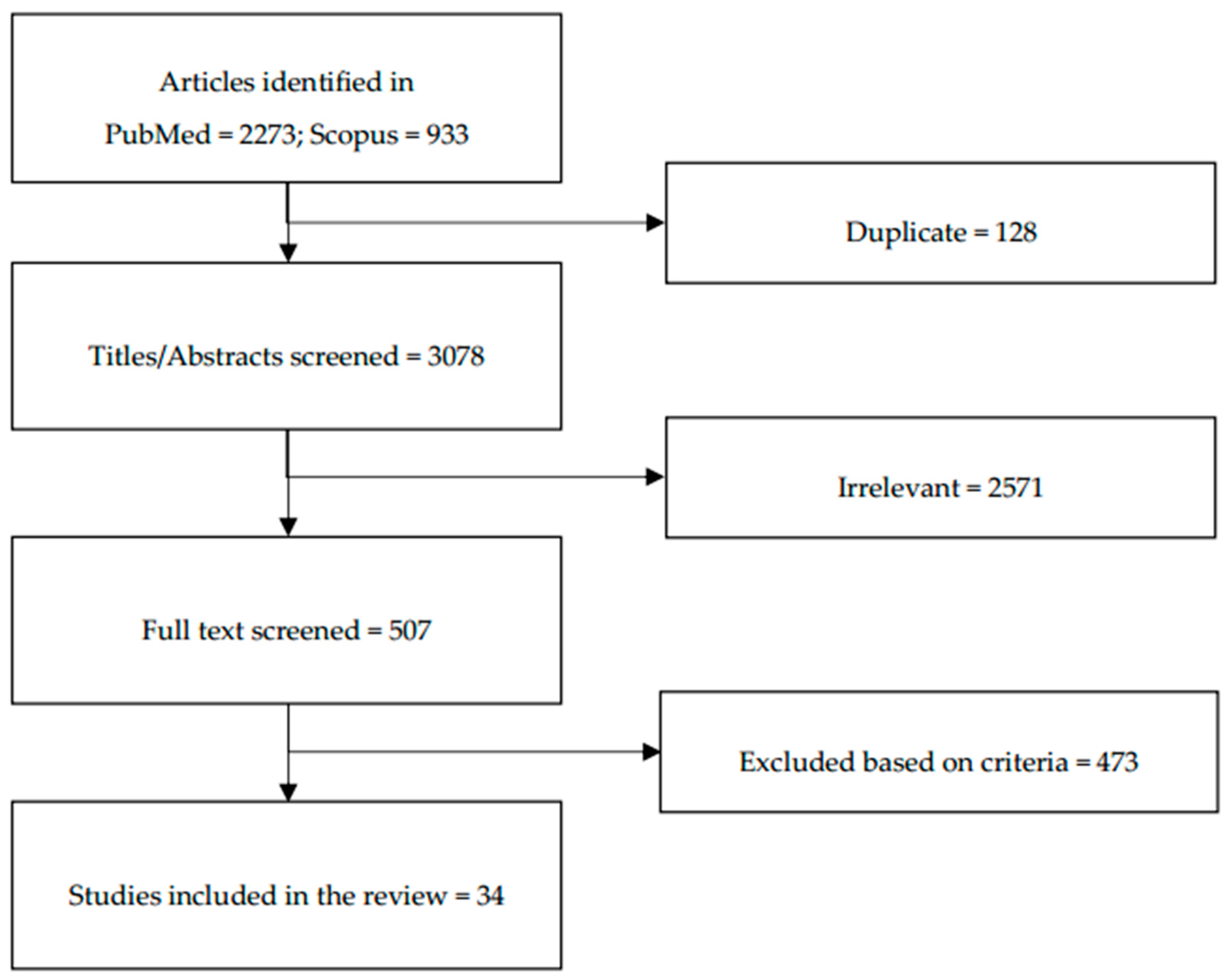
2. Materials and Methods
3. Results
3.1. Knowledge Regarding Osteoporosis Among Adolescents and Young Adults
3.2. Beliefs Regarding Osteoporosis among Adolescents and Young Adults
3.3. Practices Affecting Bone Health Among Adolescents and Young Adults
3.4. Relationship between Knowledge, Lifestyle and Dietary Habits with Bone Health among Adolescents and Young Adults
4. Perspectives
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Yamamoto, K. Definition and diagnostic criteria of osteoporosis in Japan. Clin. Calcium 2001, 11, 19–24. [Google Scholar] [PubMed]
- Svedbom, A.; Ivergård, M.; Hernlund, E.; Rizzoli, R.; Kanis, J.A. Epidemiology and economic burden of osteoporosis in Switzerland. Arch. Osteoporos. 2014, 9, 187. [Google Scholar] [CrossRef] [PubMed]
- Wade, S.W.; Strader, C.; Fitzpatrick, L.A.; Anthony, M.S.; O’Malley, C.D. Estimating prevalence of osteoporosis: Examples from industrialized countries. Arch. Osteoporos. 2014, 9, 182. [Google Scholar] [CrossRef] [PubMed]
- Njeze Ngozi, R.; Ikechukwu, O.; Miriam, A.; Olanike, A.-U.; Akpagbula Ulugo, D.; Njeze Nneze, C. Awareness of Osteoporosis in a Polytechnic in Enugu, South East Nigeria. Arch. Osteoporos. 2017, 12, 51. [Google Scholar] [CrossRef] [PubMed]
- NIH Consensus Development Panel. Osteoporosis Prevention, Diagnosis, and Therapy. JAMA 2001, 285, 785–795. [Google Scholar] [CrossRef]
- Stagi, S.; Cavalli, L.; Iurato, C.; Seminara, S.; Brandi, M.L.; de Martino, M. Bone metabolism in children and adolescents: Main characteristics of the determinants of peak bone mass. Clin. Cases Miner. Bone Metab. 2013, 10, 172–179. [Google Scholar] [PubMed]
- O’Brien, M. Exercise and osteoporosis. Irish J. Med. Sci. 2001, 170, 58–62. [Google Scholar] [CrossRef] [PubMed]
- McKay, H.A.; Bailey, D.A.; Mirwald, R.L.; Davison, K.S.; Faulkner, R.A. Peak bone mineral accrual and age at menarche in adolescent girls: A 6-year longitudinal study. J. Pediatr. 1998, 133, 682–687. [Google Scholar] [CrossRef]
- Wahba, S.A.; El-shaheed, A.A.; Tawheed, M.S.; Mekkawy, A.A. Osteoporosis knowledge, beliefs, and behaviours among Egyption female students. JASMR 2010, 5, 173–180. [Google Scholar]
- Bollenbacher, V.A. Effects of an Osteoporosis Educational Intervention: Knowledge and Self-Efficacy of Prevention in Young Adult Collegiate Females. Valpo Scholar. 2014. Available online: https://scholar.valpo.edu/cgi/viewcontent.cgi?article=1056&context=ebpr (accessed on 26 February 2018).
- Hsieh, C.H.; Wang, C.Y.; McCubbin, M.; Zhang, S.; Inouye, J. Factors influencing osteoporosis preventive behaviours: Testing a path model. J. Adv. Nurs. 2008, 62, 336–345. [Google Scholar] [CrossRef] [PubMed]
- Sharma, S.V.; Hoelscher, D.M.; Kelder, S.H.; Diamond, P.; Day, R.S. Hergenroeder, a psychosocial factors influencing calcium intake and bone quality in middle school girls. J. Am. Diet. Assoc. 2010, 110, 932–936. [Google Scholar] [CrossRef] [PubMed]
- Piaseu, N.; Schepp, K.; Belza, B. Causal analysis of exercise and calcium intake behaviours for osteoporosis prevention among young women in Thailand. Health Care Women Int. 2002, 23, 364–376. [Google Scholar] [CrossRef] [PubMed]
- Tyler, C.V.; Werner, J.J.; Panaite, V.; Snyder, S.M.; Ford, D.B.; Conway, J.L.; Young, C.W.; Powell, B.L.; Smolak, M.J.; Zyzanski, S.J. Barriers to supplemental calcium use among women in suburban family practice: A report from the cleveland clinic ambulatory research network (CleAR-eN). JABFM 2008, 21, 293–299. [Google Scholar] [CrossRef] [PubMed]
- Barzanji, A.T.; Alamri, F.A.; Mohamed, A.G. Osteoporosis: A study of knowledge, attitude and practice among adults in Riyadh, Saudi Arabia. J. Community Health 2013, 38, 1098–1105. [Google Scholar] [CrossRef] [PubMed]
- WHO. Health Topics: Adolescent Health. Available online: http://www.who.int/topics/adolescent_health/en/ (accessed on 1 May 2018).
- Alamri, F.A.; Saeedi, M.Y.; Mohamed, A.; Barzanii, A.; Aldayel, M.; Ibrahim, A.K. Knowledge, attitude, and practice of osteoporosis among Saudis. J. Egypt. Publ. Health Assoc. 2015, 90, 171–177. [Google Scholar] [CrossRef] [PubMed]
- Al-Raddadi, R.; Bahijri, S.; Borai, A.; AlRaddadi, Z. Prevalence of lifestyle practices that might affect bone health in relation to vitamin D status among female Saudi adolescents. Nutrition 2018, 45, 108–113. [Google Scholar] [CrossRef] [PubMed]
- Al-daghri, N.M.; Aljohani, N.; Al-attas, O.S.; Krishnaswamy, S.; Alfawaz, H. Dairy products consumption and serum 25-hydroxyvitamin D level in Saudi children and adults. Int. J. Clin. Exp. Pathol. 2015, 8, 8480–8486. [Google Scholar] [PubMed]
- Ediriweera de Silva, R.E.; Haniffa, M.R.; Gunathillaka, K.D.K.; Atukorala, I.; Fernando, E.D.; Perera, W.L. A descriptive study of knowledge, beliefs and practices regarding osteoporosis among female medical school entrants in Sri Lanka. Asia Pac. Fam. Med. 2014, 13, 15. [Google Scholar] [CrossRef] [PubMed]
- Gammage, K.L.; Gasparotto, J.; Mack, D.E.; Klentrou, P. Gender differences in osteoporosis health beliefs and knowledge and their relation to vigorous physical activity in university students. J. Am. Coll. Health 2011, 60, 58–64. [Google Scholar] [CrossRef] [PubMed]
- Shanthi Johnson, C.; McLeod, W.; Kennedy, L.; McLeod, K. Osteoporosis health beliefs among younger and older men and women. Health Educ. Behav. 2008, 35, 721–733. [Google Scholar] [CrossRef] [PubMed]
- Marcinow, M.L.; Randall Simpson, J.A.; Whiting, S.J.; Jung, M.E.; Buchholz, A.C. Young adults’ perceptions of calcium intake and health: A qualitative study. Health Educ. Behav. 2017, 44, 898–906. [Google Scholar] [CrossRef] [PubMed]
- Chouinard, L.E.; Simpson, J.R.; Buchholz, A.C. Predictors of bone mineral density in a convenience sample of young Caucasian adults living in Southern Ontario. Appl. Physiol. Nutr. Metab. 2012, 714, 706–714. [Google Scholar] [CrossRef] [PubMed]
- Puttapitakpong, P.; Chaikittisilpa, S.; Panyakhamlerd, K.; Nimnuan, C.; Jaisamrarn, U.; Taechakraichana, N. Inter-correlation of knowledge, attitude, and osteoporosis preventive behaviours in women around the age of peak bone mass. BMC Women Health 2014, 14, 35. [Google Scholar] [CrossRef] [PubMed]
- Iwasaki, E.; Morakote, N.; Chaovistsaree, S.; Matsuo, H. Bone mineral density and bone turnover among young women in Chiang Mai, Thailand. Kobe J. Med. Sci. 2014, 59, E149–E156. [Google Scholar] [PubMed]
- Seo, S.; Chun, S.; Newell, M.A.; Yun, M. Association between alcohol consumption and Korean young women’s bone health: A cross sectional study from the 2008 to 2011 Korea national health and nutrition examination survey. BMJ Open 2015, 5. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.; So, W.; Kim, J.; Sung, D.J. Relationship between bone-specific physical activity scores and measures for body composition and bone mineral density in healthy young college women. PLoS ONE 2016, 11, e0162127. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Jung, M.; Hong, Y.; Park, J.; Choi, B. Physical activity in adolescence has a positive effect on bone mineral density in young men. J. Prev. Med. Publ. Health 2013, 46, 89–95. [Google Scholar] [CrossRef] [PubMed]
- Park, D.-I.; Choi-Kwon, S.; Han, K. Health behaviours of Korean female nursing students in relation to obesity and osteoporosis. Nurs. Outlook 2015, 63, 504–511. [Google Scholar] [CrossRef] [PubMed]
- Amre, H.; Safadi, R.; Jarrah, S.; Al-Amer, R.; Froelicher, E. Jordanian nursing students’ knowledge of osteoporosis. Int. J. Nurs. Pract. 2008, 14, 228–236. [Google Scholar] [CrossRef] [PubMed]
- Al-Zu’bi, A.; Almuhtaseb, N.; Amayreh, I. Osteoporosis awareness in a sample of teenage girls in Jordan. Jordan Med. J. 2010, 44, 420–426. [Google Scholar]
- Khan, Y.H.; Sarriff, A.; Khan, A.H.; Mallhi, T.H. Knowledge, attitude and practice (KAP) survey of osteoporosis among students of a tertiary institution in Malaysia. J. Pharm. Res. 2014, 13, 155–162. [Google Scholar] [CrossRef]
- Suriawati, A.A.; Majid, H.A.; Al-Sadat, N.; Mohamed, M.N.A.; Jalaludin, M.Y. Vitamin D and calcium intakes, physical activity, and calcaneus bmc among school-going 13-year old Malaysian adolescents. Nutrients 2016, 8, 666. [Google Scholar] [CrossRef] [PubMed]
- Ford, M.A.; Bass, M.; Zhao, Y.; Bai, J.-B.; Zhao, Y. Osteoporosis knowledge, self-efficacy, and beliefs among college students in the USA and China. J. Osteoporos. 2011, 2011, 729219. [Google Scholar] [CrossRef] [PubMed]
- Mu, M.; Wang, S.; Sheng, J.; Zhao, Y.; Wang, G.; Liu, K.Y.; Hu, C.L.; Tao, F.B.; Wang, H.L. Dietary patterns are associated with body mass index and bone mineral density in Chinese freshmen. J. Am. Coll. Nutr. 2014, 33, 120–128. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.-W.; Yang, S.-C.; Wang, R.-H.; Lin, M.L. Osteoporosis prevention behaviours practiced among youth in Taichung City, Taiwan. Am. J. Health Behav. 2012, 36, 736–745. [Google Scholar] [CrossRef] [PubMed]
- Sayed-Hassan, R.; Bashour, H.; Koudsi, A. Osteoporosis knowledge and attitudes: A cross-sectional study among female nursing school students in Damascus. Arch. Osteoporos. 2013, 8, 149. [Google Scholar] [CrossRef] [PubMed]
- Uddin, R.; Huda, N.H.; Jhanker, Y.M.; Jesmeen, T.; Imam, M.Z.; Akter, S. Awareness regarding the Importance of Calcium and vitamin D among the undergraduate pharmacy students in Bangladesh. BMC Res. Notes 2013, 6, 134. [Google Scholar] [CrossRef] [PubMed]
- Sidor, P.; Głąbska, D.; Włodarek, D. Analysis of the dietary factors contributing to the future osteoporosis risk in young Polish women. Natl. Inst. Publ. Health 2016, 67, 279–285. [Google Scholar]
- Tonnesen, R.; Hovind, P.H.; Jensen, L.T.; Schwarz, P. Determinants of vitamin D status in young adults: Influence of lifestyle, sociodemographic and anthropometric factors. BMC Public Health 2016, 16, 385. [Google Scholar] [CrossRef] [PubMed]
- Eleftheriou, K.I.; Rawal, J.S.; James, L.E.; Payne, J.R.; Loosemore, M.; Pennell, D.J.; Drenos, F.; Haddad, F.S.; Humphries, S.E.; Sanders, J.; et al. Bone structure and geometry in young men: The influence of smoking, alcohol intake and physical activity. Bone 2013, 52, 17–26. [Google Scholar] [CrossRef] [PubMed]
- Ghaffari, M.; Nasirzadeh, M.; Rakhshanderou, S.M.H.B.; Harooni, J. Osteoporosis-related knowledge among students of a medical sciences university in Iran: Calcium intake and physical activity. J. Med. Life 2015, 8, 203–208. [Google Scholar] [PubMed]
- Bilal, M.; Haseeb, A.; Merchant, A.Z.; Rehman, A.; Arshad, M.H.; Malik, M.; Rehman, A.H.U.; Rani, P.; Farhan, E.; Rehman, T.S.; et al. Knowledge, beliefs and practices regarding osteoporosis among female medical school entrants in Pakistan. Asia Pac. Fam. Med. 2017, 16, 6. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, V.H.; Wang, Z. Osteoporosis knowledge of students in relevant healthcare academic programs. J. Osteoporos. 2012, 2–5. [Google Scholar] [CrossRef] [PubMed]
- Hervás, G.; Ruiz-Litago, F.; Irazusta, J.; Fernández-Atutxa, A.; Fraile-Bermúdez, A.B.; Zarrazquin, I. Physical activity, physical fitness, body composition, and nutrition are associated with bone status in university students. Nutrients 2018, 10, 61. [Google Scholar] [CrossRef] [PubMed]
- Ito, S.; Ishida, H.; Uenishi, K.; Murakami, K.; Sasaki, S. The relationship between habitual dietary phosphorus and calcium intake, and bone mineral density in young Japanese women: A cross-sectional study. Asia Pac. J. Clin. Nutr. 2011, 20, 411–417. [Google Scholar] [PubMed]
- Liberato, S.C.; Bressan, J.; Hills, A.P. The role of physical activity and diet on bone mineral indices in young men: A cross-sectional study. J. Int. Soc. Sports Nutr. 2013, 10, 1. [Google Scholar] [CrossRef] [PubMed]
- Chan, M.F.; Kwong, W.S.; Zang, Y.L.; Wan, P.Y. Evaluation of an osteoporosis prevention education programme for young adults. J. Adv. Nurs. 2007, 57, 270–285. [Google Scholar] [CrossRef] [PubMed]
- Du, S.; Mroz, T.A.; Zhai, F.; Popkin, B.M. Rapid income growth adversely affects diet quality in China—Particularly for the poor! Soc. Sci. Med. 2004, 59, 1505–1515. [Google Scholar] [CrossRef] [PubMed]
- Heaney, R.P.; Abrams, S.; Dawson-Hughes, B.; Looker, A.; Marcus, R.; Matkovic, V.; Weaver, C. Peak bone mass. Osteoporos. Int. 2000, 11, 985–986. [Google Scholar] [CrossRef] [PubMed]
- Hammad, L.F.; Benajiba, N. Lifestyle factors influencing bone health in young adult women in Saudi Arabia. Afr. Health Sci. 2017, 17, 524–531. [Google Scholar] [CrossRef] [PubMed]
- Fehily, A.M.; Coles, R.J.; Evans, W.D.; Elwood, P.C. Factors affecting bone density in young adults. Am. J. Clin. Nutr. 1992, 56, 579–586. [Google Scholar] [CrossRef] [PubMed]
- Laitinen, K.; Valimaki, M. Alcohol and bone. Calcif. Tissue Int. 1991, 49, S70–S73. [Google Scholar] [CrossRef] [PubMed]
- Maurel, D.B.; Boisseau, N.; Benhamou, C.L.; Jaffre, C. Alcohol and bone: Review of does effects and mechanisms. Osteoporos. Int. 2012, 23, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Stránský, M.; Ryšavá, L. Nutrition as prevention and treatment of osteoporosis. Physiol. Res. 2009, 58, 7–11. [Google Scholar]
- Holland, A. Osteoporosis knowledge translation for young adults: New directions for prevention programs. Health Promot. Chronic Dis. Prev. Can. 2017, 37, 229–237. [Google Scholar] [CrossRef] [PubMed]
- Schoenfeld, R.E.; Ng, P.; Henderson, K.; Wu, S.-Y. Using the internet to educate adolescents about osteoporosis: Application of a tailored web-education system. Health Promot. Pract. 2010, 11, 104–111. [Google Scholar] [CrossRef] [PubMed]
- Takahata, Y. Usefulness of circuit training at home for improving bone mass and muscle mass while losing fat mass in undergraduate female students. Lipids Health Dis. 2018, 17, 104. [Google Scholar] [CrossRef] [PubMed]
- Sanaeinasab, H.; Tavakoli, R.; Karimizarchi, A.; Amini, Z.H.; Farokhian, A.; Najarkolaei, F.R. The effectiveness of education using the health belief model in preventing osteoporosis among female students. East. Mediterr. Health J. 2013, 19 (Suppl. 3), 38–44. [Google Scholar] [CrossRef]
- Zhang, Y.-P.; Li, X.-M.; Wang, D.-L.; Guo, X.-Y.; Guo, X. Evaluation of educational program on osteoporosis awareness and prevention among nurse students in China. Nurs. Health Sci. 2012, 14, 74–80. [Google Scholar] [CrossRef] [PubMed]
- Bohaty, K.; Rocole, H.; Wehling, K.; Waltman, N. Testing the effectiveness of an educational intervention to increase dietary intake of calcium and vitamin D in young adult women. J. Am. Acad. Nurse Pract. 2008, 20, 93–99. [Google Scholar] [CrossRef] [PubMed]
- Goodman, S.; Morrongiello, B.; Meckling, K. A randomized, controlled trial evaluating the efficacy of an online intervention targeting vitamin D intake, knowledge and status among young adults. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 116. [Google Scholar] [CrossRef] [PubMed]
- Ha, E.; Caine-bish, N.; Holloman, C.; Lowry-gordon, K. Evaluation of effectiveness of class-based nutrition intervention on changes in soft drink and milk consumption among young adults. Nutr. J. 2009, 6, 4–9. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Studies | Primary Objective | Populations | Locations | Age | Study Design | Findings |
|---|---|---|---|---|---|---|
| Good knowledge regarding osteoporosis | ||||||
| Amre et al. (2008) [31] | To explore baccalaureate nursing students’ knowledge of osteoporosis for beginning practice in the community | 85 senior baccalaureate nursing students (58 male & 27 female) in the final 4 years of university | Jordan | 19–32 years (mean age 21.74 ± 1.86) | Cross-sectional study using Osteoporosis Knowledge Questionnaire (OKQ) and Osteoporosis Knowledge Test (OKT) |
|
| Chen et al. (2012) [37] | To examine demographic characteristics, knowledge, and attitudes of adolescents on osteoprotective practices in Taichung City, Taiwan | 329 (120 male and 209 female) randomly selected high schools and colleges students | Taichung City, Taiwan | Adolescents (senior high school students) and young adults (undergraduates) | Cross-sectional study using Osteoporosis Knowledge Scale (OKS) |
|
| Khan et al. (2014) [33] | To evaluate knowledge and perceptions of osteoporosis among university students in Malaysia | 461 students (214 male and 247 female): 165 Malay, 147 Chinese, 125 Indian, 24 Others | Universiti Sains Malaysia (USM) Penang, Malaysia | Mean age 24.61 ± 5.51 years | Cross-sectional study using a pre-validated self-design questionnaire was used to assess the knowledge regarding osteoporosis |
|
| Uddin et al. (2013) [39] | To understand the level of gap of knowledge and awareness regarding the essentiality of calcium and vitamin D among pharmacy students at undergraduate level in Bangladesh | 713 (350 male and 363 female) undergraduate pharmacy students from different public and private universities | Dhaka and Chittagong cities of Bangladesh, India | Age 18 to 20 years | A questionnaire was devised to get a gross idea about the preliminary and basic knowledge on calcium and vitamin D |
|
| Poor knowledge regarding osteoporosis | ||||||
| Bilal et al. (2017) [44] | To assess knowledge, attitudes and practices about osteoporosis among female medical school entrants in Karachi | 400 female medical school entrants of DOW University of Health Sciences (DUHS) and Jinnah Sindh Medical University (JSMU) | Karachi, Pakistan | Mean age 19.4 ± 1.2 years | Cross-sectional study using a pre-validated Osteoporosis Knowledge Assessment Tool (OKAT) |
|
| Ediriweera de Silva et al. (2014) [20] | To determine the knowledge, beliefs and practices regarding osteoporosis among young females entering medical schools in Sri Lanka | 186 female medical school entrants | Faculties of Medicine, Universities of Colombo and Kelaniya, Sri Lanka | Mean age 20.7 ± 2.1 years | Cross-sectional study using a validated Osteoporosis Knowledge Assessment Tool (OKAT) |
|
| Gammage et al. (2011) [21] | To examine gender differences in osteoporosis-related knowledge in university students | 527 participants (351 women & 176 men) from first-year university courses in a kinesiology department | Brock University, St. Catharines, Ontorio, Canada | College-aged | Cross-sectional study using Osteoporosis Knowledge Tool (OKT) |
|
| Ghaffari et al. (2015) [43] | To investigate the health faculty students’ awareness of osteoporosis (calcium intake and physical activity). | 228 female undergraduate students in the health faculty, Shahid Beheshti University of Medical Sciences | Iran | 18–24 years old (mean age 22.17 ± 2.66 years) | A validated questionnaire to assess knowledge regarding osteoporosis was used |
|
| Njeze et al. (2017) [4] | To determine the awareness of osteoporosis and factors that determine awareness of osteoporosis | 500 respondents from a polytechnic | Enugu, South East Nigeria | Less than 20 to 51 years old and above (mean age 26.5 ± 7.4 years) | Cross-sectional study using a self-design questionnaire |
|
| Sayed-Hasaan, Bashour and Koudsi (2013) [38] | To determine the level of osteoporosis knowledge and beliefs among nursing college students in Damascus | 353 female students in nursing college | Damascus, Syria | Mean age 19.9 years | Cross-sectional study using osteoporosis-related tools (Arabic version), namely the Osteoporosis Knowledge Assessment Tool (OKAT) |
|
| Difference in osteoporosis knowledge based on sex, study program and country | ||||||
| Alamri et al. (2015) [17] | To assess knowledge, attitude, and practices for osteoporosis among Saudi general population and to identify its determining factors | 1830 respondents (1062 male and 728 female) | Every region in the Kingdom of Saudi Arabia | Age 18 years or older (Mean age 37.1 ± 14.3 years in male & 36.3 ± 13.6 years in female) | Cross-sectional study using a pre-validated self-design questionnaire was used to assess the knowledge regarding osteoporosis |
|
| Ford et al. (2011) [35] | To differences in osteoporosis knowledge, self-efficacy, and health beliefs among China and American college students | 408 US and 409 Chinese undergraduate students (342 male, 468 female) from University of Mississippi Withheld During Review, United States and Tianjin Medical University Withheld During Review, Peoples Republic of China respectively | United States and China | Mean age 19.38 ± 1.25 years | Validated Osteoporosis Knowledge Test (OKT) was used |
|
| Nguyen and Wang (2012) [45] | To investigate osteoporosis knowledge in students who were soon to be nurses, pharmacists, physical therapists, and dietitians | 206 female students of University of Missouri | Columbia | 21 to 27 years | Revised version of Osteoporosis Knowledge Test (OKT) was used |
|
| Sources of osteoporosis knowledge | ||||||
| Al-Zu’bi, Almuhtaseb and Amayreyh (2010) [32] | To assess the knowledge in a group of teenage girls about risk factors and lifestyle affecting osteoporosis | 320 girls attending the 8–10th grade | Schools from east and west of Amman, the capital city in Jordan | 13–17 years (mean age 14.4 ± 0.9 years) | Self-design questionnaire to assess knowledge of risk factors regarding osteoporosis was used |
|
| Barzanji, Alamri and Mohamed (2013) [15] | To assess the awareness of adults in Riyadh about osteoporosis and its associated factors as well as compare knowledge, attitude and practice levels of men and women | 505 participants from eight malls | Riyadh city, Saudi Arabia | Mean age 33.78 ± 10.46 years | Cross-sectional study using pre-coded Arabic questionnaire |
|
| Puttapitakpong et al. (2014) [25] | To assess the inter-correlation of knowledge, attitude and osteoporosis preventive behaviours in women around the age of peak bone mass. | 430 women attending the Gynecology Clinic | King Chulalongkorn Memorial Hospital, Bangkok, Thailand | 20–35 years’ old | Cross-sectional study using a pre-validated self-design questionnaire |
|
| Studies | Primary Objective | Populations | Location | Age | Study Design | Findings |
|---|---|---|---|---|---|---|
| Perceived high susceptibility regarding osteoporosis (men > women) | ||||||
| Alamri et al. (2015) [17] | To assess knowledge, attitude, and practices for osteoporosis among Saudi general population and to identify its determining factors | 1830 respondents (1062 male and 728 female) | Every region in the Kingdom of Saudi Arabia | Age 18 years or older (Mean age 37.1 ± 14.3 years in male & 36.3 ± 13.6 years in female) | Cross-sectional study using a pre-validated self-design questionnaire was used to assess the health belief regarding osteoporosis |
|
| Perceived high susceptibility regarding osteoporosis (women > men) | ||||||
| Ford et al. (2011) [35] | To differences in osteoporosis knowledge, self-efficacy, and health beliefs among China and American college students | 408 US and 409 Chinese undergraduate students (342 male, 468 female) from University of Mississippi Withheld During Review, United States and Tianjin Medical University Withheld During Review, Peoples Republic of China respectively | United States and China | Mean age 19.38 ± 1.25 years | Validated Osteoporosis Health Belief Scale (OHBS) was used |
|
| Gammage et al. (2011) [21] | To examine gender differences in osteoporosis-related knowledge in university students | 527 participants (351 women & 176 men) from first-year university courses in a kinesiology department | Brock University, St. Catharines, Ontorio, Canada | College-aged | Cross-sectional study using Osteoporosis Health Belief Scale (OHBS) |
|
| Shanthi et al. (2008) [22] | To compare osteoporosis health beliefs among different age and gender groups | 300 participants (45 male and 97 female: 18–25 years old) | University town in Canada | Three age groups (18 to 25, 30 to 50, and 50-plus) | Cross-sectional study using Osteoporosis Health Belief Scale (OHBS) questionnaire |
|
| Perceived low susceptibility regarding osteoporosis | ||||||
| Bilal et al. (2017) [44] | To assess knowledge, attitudes and practices about osteoporosis among female medical school entrants in Karachi | 400 female medical school entrants of DOW University of Health Sciences (DUHS) and Jinnah Sindh Medical University (JSMU) | Karachi, Pakistan | Mean age 19.4 ± 1.2 years | Cross-sectional study using a pre-validated Osteoporosis Health Belief Scale (OHBS) |
|
| Chen et al. (2012) [37] | To examine demographic characteristics, knowledge, and attitudes of adolescents on osteoprotective practices in Taichung City, Taiwan | 329 (120 male and 209 female) randomly selected high schools and colleges students | Taichung City, Taiwan | Adolescents (senior high school students) and young adults (undergraduates) | Cross-sectional study using Osteoporosis Attitude Scale (OAS) questionnaire |
|
| Ediriweera de Silva et al. (2014) [20] | To determine the knowledge, beliefs and practices regarding osteoporosis among young females entering medical schools in Sri Lanka | 186 female medical school entrants | Faculties of Medicine, Universities of Colombo and Kelaniya, Sri Lanka | Mean age 20.7 ± 2.1 years | Cross-sectional study using Osteoporosis Health Belief Scale (OHBS) questionnaire |
|
| Khan et al. (2014) [33] | To evaluate knowledge and perceptions of osteoporosis among university students in Malaysia | 461 students (214 male and 247 female): 165 Malay, 147 Chinese, 125 Indian, 24 Others | University Sains Malaysia (USM) Penang, Malaysia | Mean age 24.61 ± 5.51 years | Cross-sectional study using a pre-validated self-design questionnaire was used to assess the perceptions regarding osteoporosis |
|
| Sayed-Hasaan, Bashour and Koudsi (2013) [38] | To determine the level of osteoporosis knowledge and beliefs among nursing college students in Damascus | 353 female students in nursing college | Damascus, Syria | Mean age 19.9 years | Cross-sectional study using Osteoporosis Health Belief Scale (OHBS) questionnaire |
|
| Barrier to osteoprotective behaviours | ||||||
| Marcinow et al. (2017) [23] | To determine young adults’ knowledge of calcium in relation to health, facilitators and barriers to adequate calcium intake | 53 participants (18 male and 35 female) | Communities in Guelph and surrounding areas, Ontorio, Canada | 18–34 years’ old | Attitudes and Beliefs Focus Group Study, by using a semi-structured interview guide, guided by social cognitive theory |
|
| Studies | Primary Objective | Populations | Location | Age | Study Design | Findings |
|---|---|---|---|---|---|---|
| Actively engaged in osteoprotective behaviours | ||||||
| Chen et al. (2012) [37] | To examine demographic characteristics, knowledge, and attitudes of adolescents on osteoprotective practices in Taichung City, Taiwan | 329 (120 male and 209 female) randomly selected high schools and colleges students | Taichung City, Taiwan | Adolescents (senior high school students) and young adults (undergraduates) | Cross-sectional study using Osteoporosis Lifestyle Scale (OLS) questionnaires |
|
| Not actively engaged in osteoprotective behaviours | ||||||
| Al-Raddadi et al. (2018) [18] | To estimate the prevalence of behaviours affecting bone health and vitamin D status and to identify factors associated with vitamin D deficiency among Saudi adolescent females | 421 female adolescents | Secondary schools in Jeddah City, Saudi Arabia | Mean age 17.2 ± 1.2 years | Cross-sectional study using self-design questionnaire |
|
| Al-Zu’bi, Almuhtaseb & Amayreyh (2010) [32] | To assess the knowledge in a group of teenage girls about risk factors and lifestyle affecting osteoporosis | 320 girls attending the 8–10th grade | School from east and west of Amman, the capital city in Jordan, Arab | 13–17 years (mean age 14.4 ± 0.9 years) | Self-design questionnaire to assess lifestyle of students |
|
| Barzanji, Alamri and Mohamed (2013) [15] | To assess the awareness of adults in Riyadh about osteoporosis and its associated factors as well as compare knowledge, attitude and practice levels of men and women | 505 participants from eight malls | Riyadh city, Saudi Arabia | Mean age 33.78 ± 10.46 years | Cross-sectional study using pre-coded Arabic questionnaire |
|
| Bilal et al. (2017) [44] | To assess knowledge, attitudes and practices about osteoporosis among female medical school entrants in Karachi | 400 female medical school entrants of DOW University of Health Sciences (DUHS) and Jinnah Sindh Medical University (JSMU) | Karachi, Pakistan | Mean age 19.4 ± 1.2 years | Cross-sectional study using self-design questionnaire |
|
| Ediriweera de Silva et al. (2014) [20] | To determine the knowledge, beliefs and practices regarding osteoporosis among young females entering medical schools in Sri Lanka | 186 female medical school entrants | Faculties of Medicine, Universities of Colombo and Kelaniya, Sri Lanka | Mean age 20.7 ± 2.1 years | Cross-sectional study using modified validated food frequency questionnaire and questions regarding positive and negative behaviours towards osteoporosis |
|
| Park et al. (2015) [30] | To examine dietary intakes and patterns, health behaviours in relation to obesity and bone mineral density (BMD) | 160 females nursing students | College in Seoul, Republic of Korea | Mean age 20.6 ± 1.48 | Cross-sectional study examines dietary habits (3- day food dairy collection) and health behaviours |
|
| Sidor, Glabska & Wlodarek (2016) [40] | To analyze the osteoporosis risk, based on diet assessment in young Polish women | 75 young Polish women | Warsaw, Poland | 20–30 years (mean age 24.1 ± 3.4) | Three-day dietary record was used |
|
| Effect of lifestyle on vitamin D status | ||||||
| Al-daghri et al. (2015) [19] | To investigate vitamin D status and its association with consumption frequencies of various dairy products in Saudi population | 820 adolescents and 565 young adults | Different primary health care centers within Riyadh, Saudi Arabia | Adolescents: 327 boys (mean age 14.9 ±1.6 years) and 493 girls (mean age 14.8 ± 1.6) Young Adults: 249 men (mean age 27.9 ± 0.8) and 316 women (32.2 ± 0.6) | A qualitative food frequency questionnaire was used |
|
| Tonneson et al. (2016) [41] | To investigate the association between lifestyle and vitamin D status in a sample of untreated young adults | 738 young adults (361 male and 339 female) | Educational institutions in the Copenhagen area, Denmark | Women: mean age 22 ± 2.2 years Men: mean age 21.6 ± 2.3 years | Cross-sectional study assessing exercise and smoking habits, alcohol intake and dietary habits |
|
| Studies | Primary Objective | Populations | Location | Age | Study Design | Findings |
|---|---|---|---|---|---|---|
| Effect of knowledge regarding osteoporosis on bone health | ||||||
| Iwasaki et al. (2013) [26] | To investigate the influence of lifestyle on bone mineral density (BMD) and bone turnover among young women in Chiang Mai, Thailand | 177 healthy women | Chiang Mai University hospital, Chiang Mai, Thailand | 20–30 years (mean age 23.4 ± 2.5) | Modified version of the Osteoporosis Knowledge Test (OKT) was used |
|
| Effect of lifestyle habits (physical activity, smoking, alcohol drinking) on bone health | ||||||
| Eleftheriou et al. (2013) [42] | The association of smoking, alcohol consumption and prior exercise with lower limb bone volume, composition and structure in a large cohort of healthy Caucasian males | 723 healthy male military recruits on entry to Army training | United Kingdom | 16–18 years (mean age 19.92 ± 0.09 years) | Self-design questionnaire used to assess lifestyle factors |
|
| Seo et al. (2015) [27] | To assess the association between alcohol consumption and healthy Korean young women bone | 1176 healthy women | Sahmyook University, Seoul, South Korea | 19–30 years (mean age 24.68 ± 0.12 years) | Cross-sectional study by Alcohol Use Disorders Identification Test (AUDIT) scores and drinking consumption; frequency and amount |
|
| Effect of past physical activity on bone health | ||||||
| Kim et al. (2016) [28] | To investigate the relationship between bone-specific physical activity (BPAQ) scores, body composition, and bone mineral density (BMD) in healthy young college women | 73 college women | Universities in Seoul and Gyeonggi province, South Korea | 19–26 years (mean age 21.7 ± 1.8 years) | Cross-sectional study using food intake questionnaire and bone-specific physical activity questionnaire |
|
| Kim et al. (2013) [29] | To determine factors associated with the bone mineral density (BMD) of university students | 111 male students from School of Medicine | Chung-Ang University, College, Seoul, South Korea | 19–34 years (Mean age 23.2 years | Global Physical Activity Questionnaire and food frequency questionnaire (FFQ) were used |
|
| Effect of dietary habit (calcium intake) on bone health | ||||||
| Chouinard, Simpson and Buchholz (2012) [24] | To identify predictors of bone mineral density (BMD) in young, healthy adults | 261 (77 male and 184 female) subjects | University of Guelph in southwestern Ontario, Canada | 18–33 years (mean age 21.4 ± 2.1 years) | Cross-sectional study using physical activity questionnaire for adults (PAQ-AD) and self-administered food frequency questionnaire (FFQ) |
|
| Hervas et al. (2018) [46] | To analyze the relationship of physical activity (PA), physical fitness, body composition, and dietary intake with bone stiffness index (SI) in young university students | 156 (61 male, 95 female) young adults from different university degree programs | University of the Basque Country | 18–21 years old (mean age 18.74 ± 0.77 years) | Five days’ dietary record was used |
|
| Ito et al. (2011) [47] | To examine habitual phosphorus and calcium intake and the calcium/phosphorus intake ratio on the bone mineral density (BMD) in young Japanese women | 441 first-year female students of Kagawa Nutrition University | Japan | 18–22 years | Dietary habits during the preceding month were assessed using diet history questionnaire (DHQ) |
|
| Iwasaki et al. (2013) [26] | To investigate the influence of lifestyle on bone mineral density (BMD) and bone turnover among young women in Chiang Mai, Thailand | 177 healthy women | Chiang Mai University hospital, Chiang Mai, Thailand | 20–30 years (mean age 23.4 ± 2.5) | Self-design questionnaire consists of lifestyle-relating factors: eating habits, diet history and exercise experience |
|
| Liberato, Bressan and Hills (2013) [48] | To examine the relationship between dietary factors and physical activity on bone mineralization in young men. | 35 men from the local community | City of Brisbane, Australia | 18–25 years | Cross-sectional study where food intake was assessed using household estimates in a food record |
|
| Mu et al. (2014) [36] | To examine associations between dietary patterns and body mass index (BMI) and bone mineral density (BMD) in Chinese freshmen. | 1319 college freshmen | 4 universities in Hefei, China | 16–20 years (mean age 18.1 ± 1.2 years) | Cross-sectional study using modified food-frequency questionnaire |
|
| Suriawati et al. (2016) [34] | To investigate the relationship between the dietary intake of calcium and vitamin D, physical activity, and bone mineral content (BMC) in 13-year-old Malaysian adolescents | 289 adolescents (99 male, 190 female) school children from selected public secondary schools from the central and northern regions of Peninsular Malaysia) | Malaysia | 13-year-old | Cross-sectional study using seven-day diet histories questionnaire |
|
| Studies | Design | Location | Setting | Population | Intervention Descriptions | Outcomes |
|---|---|---|---|---|---|---|
| Educational intervention to modify knowledge, attitude and practices towards osteoporosis | ||||||
| Schoenfeld et al. (2010) [58] | Tailored Web-Education System (TWEEDS) Tool and Web Site Development | New York | School | n = 89, age 13 to 17 years, mean age 15.7 years | Online pre- and postintervention surveys (45 min) evaluated participants’ pre- and postintervention osteoporosis knowledge, attitudes, preventive practices, and postintervention intent to change healthy bone practices. Participants completed the Web-based program that provided detailed information about osteoporosis, and healthy bone practices, immediately after completing the pre-test and just prior to completing the post-test |
|
| Sanaeinasab et al. (2013) [59] | Quasi-experimental study | Female students resided in a town near Tehran | School | n = 45, 15 to 16 years’ old | Three group sessions of 60 min per week educational programme based on the Health Belief Model. Lecture, question and answer, brain-storming, group discussion with pamphlets about the role of nutrition and physical activity in disease prevention and a booklet on osteoporosis. |
|
| Takahata (2018) [60] | Circuit exercise training | Baika Women’s University, Osaka, Japan | School | n = 41, mean age 18.5 ± 0.6 years | Circuit training which involves performing both anaerobic and aerobic exercise continuously for 3 months (5 mins × 3 sets =15 mins, do the exercise at least 3 days in a week) |
|
| Zhang et al. (2012) [61] | One group quasi-experimental study | Shaanxi, Northwest China | Nursing school | n = 256, mean age 18.80 ± 1.55 years | 2.5-h lecture followed by 30 min open discussion, and 20 min for questions and answers. The lecturer summarized the content matter delivered during the program following the question-and-answer period to reinforce teaching and learning objectives. The educational program addressed the definition, prevalence, and etiology of osteoporosis; risk factor identification; physical signs of the disease; preventive and diagnostic measures; and treatment |
|
| Educational intervention to improve Calcium and/or Vitamin D intake | ||||||
| Bohaty et al. (2008) [62] | Convenience sampling method | Lincoln, Nebraska, and Ankeny, Iowa. | Day-care center | n = 80, 19 to 29 years, mean age 22.3 ± 3.1 years | 8 weeks, ten 45-min slide show presentations on the importance of dietary intake of calcium and vitamin D in preventing osteoporosis. The slide show was followed by an interactive group discussion regarding problems with increasing dietary intake of calcium and vitamin D. After the intervention, subjects received a packet to take home that included an educational handout from the NOF (n.d.) and an outline of the slide show presentation. |
|
| Goodman, Morrongiello & Meckling (2016) [63] | Randomized controlled trial | Guelph and throughout Ontario. | Community | n = 90, 18 to 25 years | The intervention group watched a video, received online information and tracked intake of vitamin D using a mobile application for 12 weeks. |
|
| Ha et al. (2009) [64] | Class based nutrition intervention | Midwest university | School | n = 80, 18 to 24 years | 15 weeks’ class lectures (3 times per weeks for 50 min) focused on healthful dietary choices related to prevention of chronic diseases and were combined with interactive hands on activities and dietary feedback |
|
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chan, C.Y.; Mohamed, N.; Ima-Nirwana, S.; Chin, K.-Y. A Review of Knowledge, Belief and Practice Regarding Osteoporosis among Adolescents and Young Adults. Int. J. Environ. Res. Public Health 2018, 15, 1727. https://doi.org/10.3390/ijerph15081727
Chan CY, Mohamed N, Ima-Nirwana S, Chin K-Y. A Review of Knowledge, Belief and Practice Regarding Osteoporosis among Adolescents and Young Adults. International Journal of Environmental Research and Public Health. 2018; 15(8):1727. https://doi.org/10.3390/ijerph15081727
Chicago/Turabian StyleChan, Chin Yi, Norazlina Mohamed, Soelaiman Ima-Nirwana, and Kok-Yong Chin. 2018. "A Review of Knowledge, Belief and Practice Regarding Osteoporosis among Adolescents and Young Adults" International Journal of Environmental Research and Public Health 15, no. 8: 1727. https://doi.org/10.3390/ijerph15081727
APA StyleChan, C. Y., Mohamed, N., Ima-Nirwana, S., & Chin, K.-Y. (2018). A Review of Knowledge, Belief and Practice Regarding Osteoporosis among Adolescents and Young Adults. International Journal of Environmental Research and Public Health, 15(8), 1727. https://doi.org/10.3390/ijerph15081727