Needs and Barriers of Teen Mothers in Rural Eastern Uganda: Stakeholders’ Perceptions Regarding Maternal/Child Nutrition and Health


Abstract
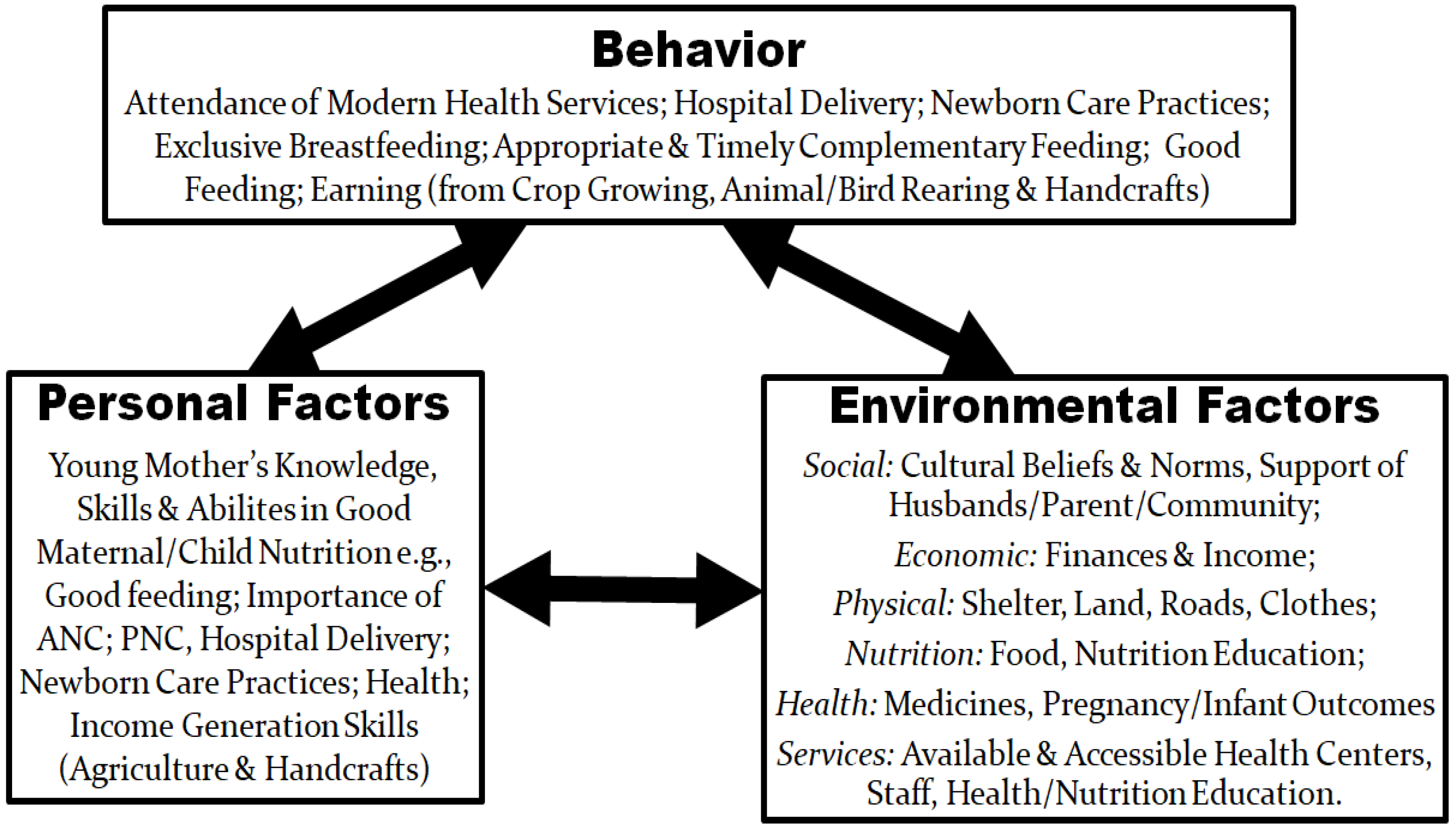
1. Introduction
2. Materials and Methods
2.1. Study Site
2.2. Inclusion Criteria
2.3. Study Sample and Recruitment
2.4. Data Collection
2.5. Data Analysis
3. Results
3.1. Demographic Characteristics of the Respondents
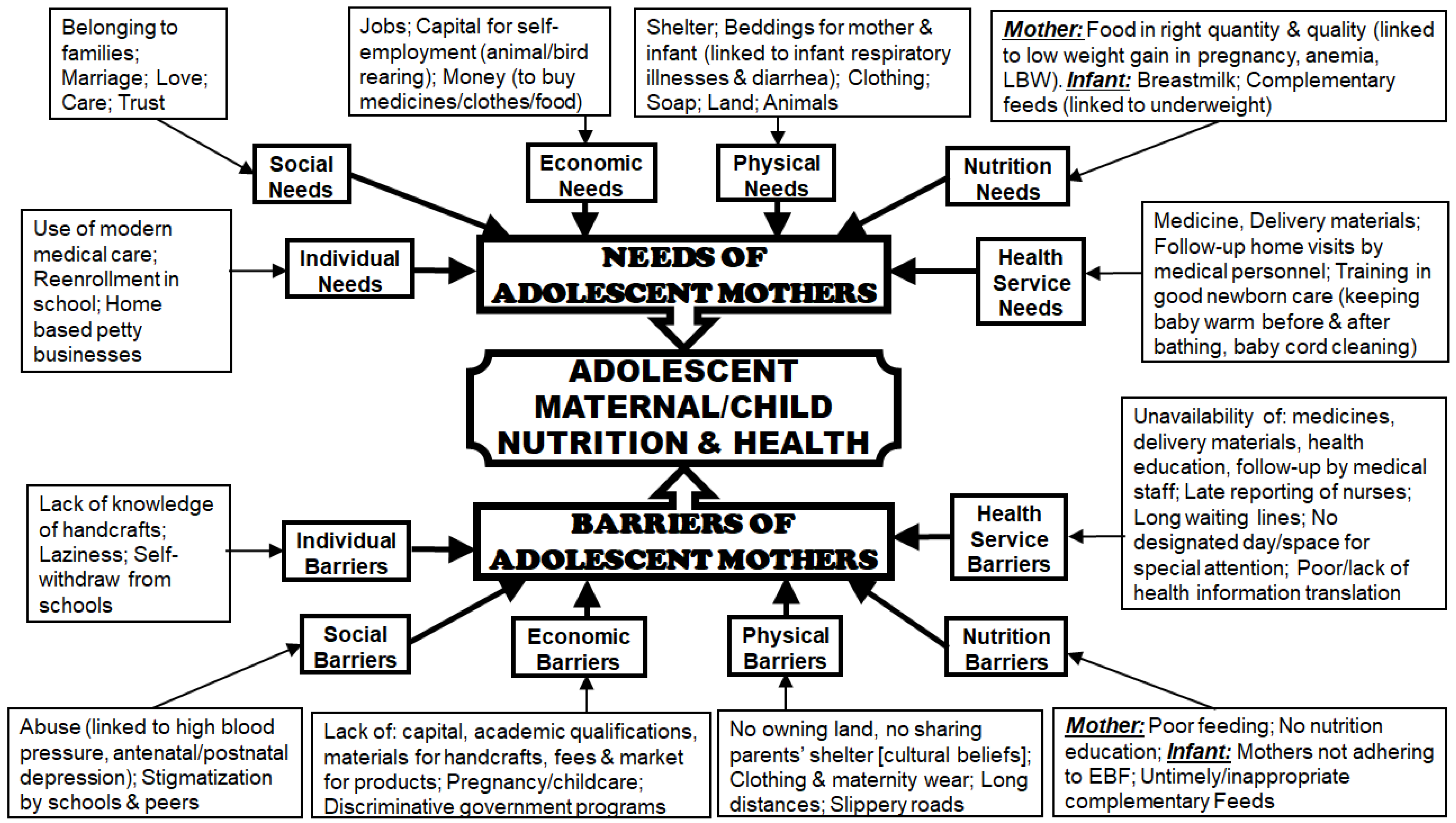
3.2. Perceived Needs and Barriers of Young Mothers
3.3. Individual Level
3.3.1. Needs at Individual Level
3.3.2. Barriers at Individual Level
3.4. Social Environment Level
3.4.1. Needs at Social Environment Level
3.4.2. Barriers at Social Environment Level
3.5. Economic Environment Level
3.5.1. Needs at Economic Environment Level
3.5.2. Barriers at Economic Environment Level
3.6. Physical Environment Level
3.6.1. Needs at the Physical Environment Level
3.6.2. Barriers at the Physical Environment Level
3.7. Nutrition Environment Level
3.7.1. Needs at Nutrition Environment Level
3.7.2. Barriers at Nutrition Environment Level
3.8. Health Service Environment Level
3.8.1. Needs at Health Service Environment Level
3.8.2. Barriers at Health Service Environment Level
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgements
Conflicts of Interest
Ethics Standards Disclosure
References
- UBOS (Uganda Bureau of Statistics) and ICF International Inc. Uganda Demographic and Health Survey. Available online: https://dhsprogram.com/pubs/pdf/FR333/FR333.pdf (accessed on 10 September 2018).
- WHO/UNFPA. Adolescent Pregnancy: A Review of the Evidence. Available online: http://www.unfpa.org/publications/adolescent-pregnancy (accessed on 10 September 2018).
- Glanz, K.; Rimer, B.K.; Viswanath, K. (Eds.) Health Behavior and Health Education: Theory, Research, and Practice, 4th ed.; Jossey-Bass: San Francisco, CA, USA, 2008; ISBN 978-0-7879-9614-7. [Google Scholar]
- McKenzie, J.F.; Smeltezer, J.L. Planning, Implementing, and Evaluating Health Promotion Programs, 2nd ed.; Allyn and Bacon: Boston, MA, USA, 1997; pp. 96–114. [Google Scholar]
- Bandura, A. Health promotion by social cognitive means. Health Educ. Behav. 2004, 31, 143–164. [Google Scholar] [CrossRef] [PubMed]
- Glanz, K. Behavioural and Social Sciences Research: Social and Behavioral Theories 2017. Available online: http://www.esourceresearch.org/Portals/0/Uploads/Documents/Public/Glanz_FullChapter.pdf (accessed on 10 September 2018).
- Creswell, J.W. Research Design: Qualitative, Quantitative, and Mixed Approaches, 4th ed.; SAGE Publications, Inc.: Thousand Oaks, CA, USA, 2014; ISBN 9781452226101. [Google Scholar]
- Ritchie, L.; Lewis, L. Qualitative Research Practice: A Guide for Social Science Students and Researchers, 1st ed.; SAGE Publications: Washington, DC, USA, 2003. [Google Scholar]
- Bisman, J. Postpositivism and accounting research. A (personal) primer on critical realism. AAFBJ 2010, 4, 1–25. [Google Scholar]
- Hutton, E. An Examination of Postpositivism and Postmodernism. Available online: http://ericahutton.blogspot.ca/2009/03/examination-of-postpositivism.html (accessed on 11 September 2018).
- Crossan, F. Research philosophy: Towards an understanding. Nurse Res. 2003, 11, 46–55. [Google Scholar] [CrossRef] [PubMed]
- Racher, F.E; Robin, S. Are phenomenology and postpositivism strange bedfellows? West J. Nurs. Res. 2003, 25, 464–481. [Google Scholar] [CrossRef] [PubMed]
- Clark, A.M. The qualitative-quantitative debate: Moving from positivism and confrontation to post-positivism and reconciliation. J. Adv. Nurs. 1998, 27, 1242–1249. [Google Scholar] [CrossRef] [PubMed]
- Swift, J.A; Tischler, V. Qualitative research in nutrition and dietetics: Getting started. J. Hum. Nutr. Diet 2010, 23, 559–566. [Google Scholar] [CrossRef] [PubMed]
- UBOS (Uganda Bureau of Statistics). Republic of Uganda: National Population and Housing Census 2014. Available online: http://www.ubos.org/onlinefiles/uploads/ubos/NPHC/2014%20National%20Census%20Main%20Report.pdf (accessed on 11 September 2018).
- UNDP. Republic of Uganda Poverty Status Report 2014: Structural Change and Poverty Reduction in Uganda 2014. Available online: http://planipolis.iiep.unesco.org/sites/planipolis/files/ressources/uganda_poverty_status_report_2014.pdf (accessed on 10 October 2018).
- World Bank Group. The Uganda Poverty Assessment Report 2016. Farms Cities and Good Fortune: Assessing Poverty Reduction in Uganda from 2006 to 2013. Available online: http://pubdocs.worldbank.org/en/381951474255092375/pdf/Uganda-Poverty-Assessment-Report-2016.pdf (accessed on 10 October 2018).
- UBOS (Uganda Bureau of Statistics)-Jinja District. Higher Local Government Statistical Abstract 2009. Available online: http://www.ubos.org/onlinefiles/uploads/ubos/2009_HLG_%20Abstract_printed/jinja%20district%202009%20statistical%20abstract%20FINAL1.pdf (accessed on 11 September 2018).
- Tongco, M.D.C. Purposive sampling as a tool for informant selection. Ethnobot. Res. Appl. 2007, 5, 147–158. [Google Scholar] [CrossRef]
- Draper, A.; Swift, J.A. Qualitative research in nutrition and dietetics: Data collection issues. J. Hum. Nutr. Diet 2011, 24, 3–12. [Google Scholar] [CrossRef]
- Attride-Stirling, J. Thematic networks: An analytic tool for qualitative research. Commission for health improvement, England. In Qualitative Research; SAGE Publications: Washington, DC, USA, 2001. [Google Scholar]
- Smith, J.; Firth, J. Qualitative data analysis: Application of the framework approach. Nurse Res. 2011, 18, 52–62. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Using Thematic Analysis in Psychology. Available online: http://eprints.uwe.ac.uk/11735/2/thematic_analysis_revised (accessed on 10 September 2018).
- Leerlooijer, J.N.; Kok, G.; Weyusya, J.; Bos, A.E.; Ruiter, R.A.; Rijsdijk, L.E.; Nshakira, N.; Bartholomew, L.K. Applying Intervention Mapping to develop a community-based intervention aimed at improved psychological and social well-being of unmarried teenage mothers in Uganda. Health Educ. Res. 2014, 29, 598–610. [Google Scholar] [CrossRef]
- Kaye, D.K. Negotiating the transition from adolescence to motherhood: Coping with prenatal and parenting stress in teenage mothers in Mulago hospital, Uganda. BMC Public Health 2008, 8, 83. [Google Scholar] [CrossRef] [PubMed]
- Atuyambe, L.; Mirembe, F.; Annika, J.; Kirumira, E.K.; Faxelid, E. Seeking safety and empathy: Adolescent health seeking behavior during pregnancy and early motherhood in central Uganda. J. Adolesc. 2009, 32, 781–796. [Google Scholar] [CrossRef] [PubMed]
- Atuyambe, L.; Mirembe, F.; Johansson, A.; Kirumira, E.K.; Faxelid, E. Experiences of pregnant adolescents—Voices from Wakiso district, Uganda. African Health Sci. 2005, 5, 304–309. [Google Scholar]
- Atuyambe, L.; Mirembe, F.; Tumwesigye, N.M.; Annika, J.; Kirumira, E.K.; Faxelid, E. Adolescent and adult first time mothers’ health seeking practices during pregnancy and early motherhood in Wakiso district, central Uganda. Reprod Health 2008, 5, 13. [Google Scholar] [CrossRef] [PubMed]
- Kyomuhendo, G.B. Low use of rural maternity services in Uganda: Impact of women’s status, traditional beliefs and limited resources. Reprod Health Matters 2003, 11, 16–26. [Google Scholar] [CrossRef]
- WHO. Monitoring the Building Blocks of Health Systems. A Handbook of Indicators and Their Measurement Strategies 2010. Available online: http://www.who.int/healthinfo/systems/WHO_MBHSS_2010_full_web.pdf (accessed on 10 October 2018).
- Atiku, J. Fertility reduction programmes should accompany land reforms. Afr. Women Health 1994, 2, 16–20. [Google Scholar] [PubMed]
- Ahikire, J.; Madanda, A. A Survey on Re-Entry of Pregnant Girls in Primary and Secondary Schools in Uganda. Available online: http://www.education.go.ug/files/downloads/gender_Report%20on%20Girls%20Re-ntry%20in%20school.pdf (accessed on 27 August 2018).
- Farmer, P. An anthropology of structural violence. Curr. Anthropol. 2004, 45, 305–325. [Google Scholar] [CrossRef]
- Page-Reeves, J.; Niforatos, J.; Mishra, S.; Regino, L.; Gingrich, A.; Bulten, R. Health disparity and structural violence: How fear undermines health among immigrants at risk for diabetes. J. Health Dispar. Res. Pract. 2013, 6, 30–47. [Google Scholar]
- Roberts, J.H. Structural violence and emotional health: A message from Easington, a former mining community in northern England. Anthropol. Med. 2009, 16, 37–48. [Google Scholar] [CrossRef]
- Montesanti, S.R.; Thurston, W.E. Mapping the role of structural and interpersonal violence in the lives of women: Implications for public health interventions and policy. BMC Womens Health 2015, 15, 100. [Google Scholar] [CrossRef]
- Montesanti, S.R. The role of structural and interpersonal violence in the lives of women: A conceptual shift in prevention of gender-based violence. BMC Womens Health 2015, 15, 93. [Google Scholar] [CrossRef] [PubMed]
- Lewis, S.; Russell, A. Young smokers’ narratives: Public health, disadvantage and structural violence. Soc. Health Illn. 2013, 35, 746–760. [Google Scholar] [CrossRef] [PubMed]
- Farmer, P. On suffering and structural violence: A view from below. Race Ethn. 2009, 3, 11–28. [Google Scholar]
- Kirstenstoebenau. Getting Girls back to School in Post-Conflict Uganda 2015. Available online: http://www.educationinnovations.org/blog/getting-girls-back-school-post-conflict-uganda (accessed on 11 October 2018).
- Palacios-Lopez, A.; Christiaensen, L.; Kilic, T. How much of the labor in African agriculture is provided by women? Food Policy 2017, 67, 52–63. [Google Scholar] [CrossRef] [PubMed]
- World Bank. Gender and Economic Growth in Uganda. Unleashing the Power of Women. Available online: http://siteresources.worldbank.org/INTAFRREGTOPGENDER/Resources/gender_econ_growth_ug.pdf (accessed on 11 October 2018).
- Muchomba, F.M. Women’s land tenure security and household human capital: Evidence from Ethiopia’s land certification. World Dev. 2017, 98, 310–324. [Google Scholar] [CrossRef] [PubMed]
- World Bank. Uganda National Education Profile 2014 Update 2014. Available online: https://www.epdc.org/sites/default/files/documents/EPDC%20NEP_Uganda.pdf (accessed on 10 September 2018).
- Negash, C.; Whiting, S.J.; Henry, C.J.; Belachew, T.; Hailemariam, T.G. Association between maternal and child nutritional status in Hula, rural Southern Ethiopia: A cross sectional study. PLoS ONE 2015, 10, e0142301. [Google Scholar] [CrossRef] [PubMed]
- Wakisa Ministries. Helping Teenage Mothers Return to School 2017. Available online: http://www.wakisaministries.com/updates/helping-teenage-mothers-return-school (accessed on 11 October 2018).
- Leerlooijer, J.N.; Bos, A.E.; Ruiter, R.A.; van Reeuwijk, M.A.; Rijsdijk, L.E.; Nshakira, N.; Kok, G. Qualitative evaluation of the teenage mothers project in Uganda: A community-based empowerment intervention for unmarried teenage mothers. BMC Public Health 2013, 13, 816. [Google Scholar] [CrossRef]
- Nabugoomu, J.; Namutebi, A.; Kaaya, A.N.; Nasinyama, G. Nutrition education influences vitamin A-related knowledge, attitudes and practices of child caregivers towards the production of orange-fleshed sweet potato in Uganda. J. Food Nutri. Sci. 2015, 3, 38–46. [Google Scholar] [CrossRef]
- Nabugoomu, J.; Namutebi, A.; Kaaya, A.N.; Nasinyama, G. Nutrition education influences child feeding knowledge attitudes and practices of child caregivers in Uganda. Am. J. Health Res. 2015, 3, 82–90. [Google Scholar] [CrossRef]
- Nabugoomu, J.; Hanning, R.M. Nutrition of adolescent mothers in the majority world: Challenges and strategies. In Women’s Health in the Majority World; Elit, L., Chamberlain, J., Eds.; Nova Sciences Publishers: Hauppauge, NY, USA, 2015. [Google Scholar]
- Henry, C.J.; Whiting, S.J.; Regassa, N. Complementary feeding practices among infant and young children in southern Ethiopia: Review of the findings from a Canada-Ethiopia project. J. Agric. Sci. 2015, 7, 29–30. [Google Scholar] [CrossRef]
- Shefner-Rogers, C. Moving Toward a Social Ecological Communication for Development Approach for Improving Children’s Health in Viet Nam. Available online: http://www.unicef.org/cbsc/files/VIETNAM_ChildHealth.pdf (accessed on 10 September 2018).
- Berti, P.R; Mildon, A.; Siekmans, K.; Main, B.; Macdonald, C. An adequacy evaluation of a 10-year, four-country nutrition and health programme. Int. J. Epidemiol. 2010, 39, 613–629. [Google Scholar] [CrossRef] [PubMed]
- National Institutes of Health. National Action Plan to Improve Health Literacy. Available online: https://cdn1.sph.harvard.edu/wp-content/uploads/sites/135/2012/09/national_action_plan_to_improve_health_literacy.pdf (accessed on 22 November 2018).



{kind=link}
{kind=link}
| Respondent Category | Gender | Number | |
|---|---|---|---|
| Male | Female | ||
| Pregnant Adolescents | 0 | 11 | 11 |
| Lactating Adolescents | 0 | 14 | 14 |
| Mothers of Adolescent Mothers | 0 | 5 | 5 |
| Grandmothers of Adolescent Mothers | 0 | 6 | 6 |
| Educators | 9 | 7 | 16 |
| Health-related Personnel | 4 | 15 | 19 |
| Agricultural Officers | 3 | 0 | 3 |
| Religious Leaders | 3 | 0 | 3 |
| Parish/Sub-county/District Administrators | 13 | 6 | 19 |
| NGO Staff | 3 | 2 | 5 |
| Total | 35 | 66 | 101 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nabugoomu, J.; Seruwagi, G.K.; Corbett, K.; Kanyesigye, E.; Horton, S.; Hanning, R. Needs and Barriers of Teen Mothers in Rural Eastern Uganda: Stakeholders’ Perceptions Regarding Maternal/Child Nutrition and Health. Int. J. Environ. Res. Public Health 2018, 15, 2776. https://doi.org/10.3390/ijerph15122776
Nabugoomu J, Seruwagi GK, Corbett K, Kanyesigye E, Horton S, Hanning R. Needs and Barriers of Teen Mothers in Rural Eastern Uganda: Stakeholders’ Perceptions Regarding Maternal/Child Nutrition and Health. International Journal of Environmental Research and Public Health. 2018; 15(12):2776. https://doi.org/10.3390/ijerph15122776
Chicago/Turabian StyleNabugoomu, Josephine, Gloria K Seruwagi, Kitty Corbett, Edward Kanyesigye, Susan Horton, and Rhona Hanning. 2018. "Needs and Barriers of Teen Mothers in Rural Eastern Uganda: Stakeholders’ Perceptions Regarding Maternal/Child Nutrition and Health" International Journal of Environmental Research and Public Health 15, no. 12: 2776. https://doi.org/10.3390/ijerph15122776
APA StyleNabugoomu, J., Seruwagi, G. K., Corbett, K., Kanyesigye, E., Horton, S., & Hanning, R. (2018). Needs and Barriers of Teen Mothers in Rural Eastern Uganda: Stakeholders’ Perceptions Regarding Maternal/Child Nutrition and Health. International Journal of Environmental Research and Public Health, 15(12), 2776. https://doi.org/10.3390/ijerph15122776