
Recommendations for Perioperative Care in Liver Resection: The EUPEMEN (EUropean PErioperative MEdical Networking) Protocol
 , , , , , , , , , , , , and
, , , , , , , , , , , , and
Abstract
1. Introduction
2. The EUPEMEN Initiative
3. The EUPEMEN Protocol in Liver Surgery
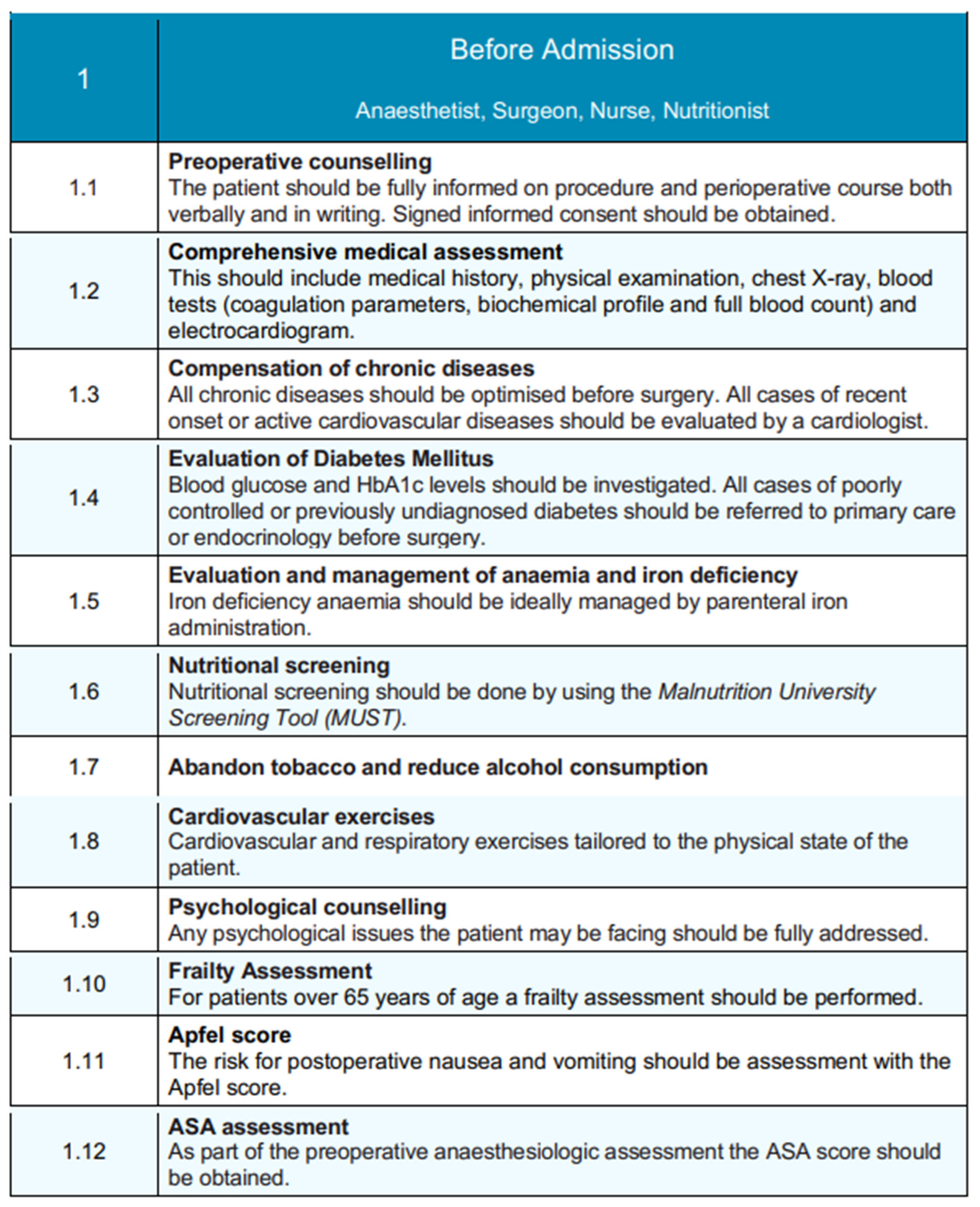
3.1. Before Admission
3.2. Perioperative Phase
3.2.1. Immediate Preoperative
3.2.2. Intraoperative Phase
3.2.3. Immediate Postoperative Phase
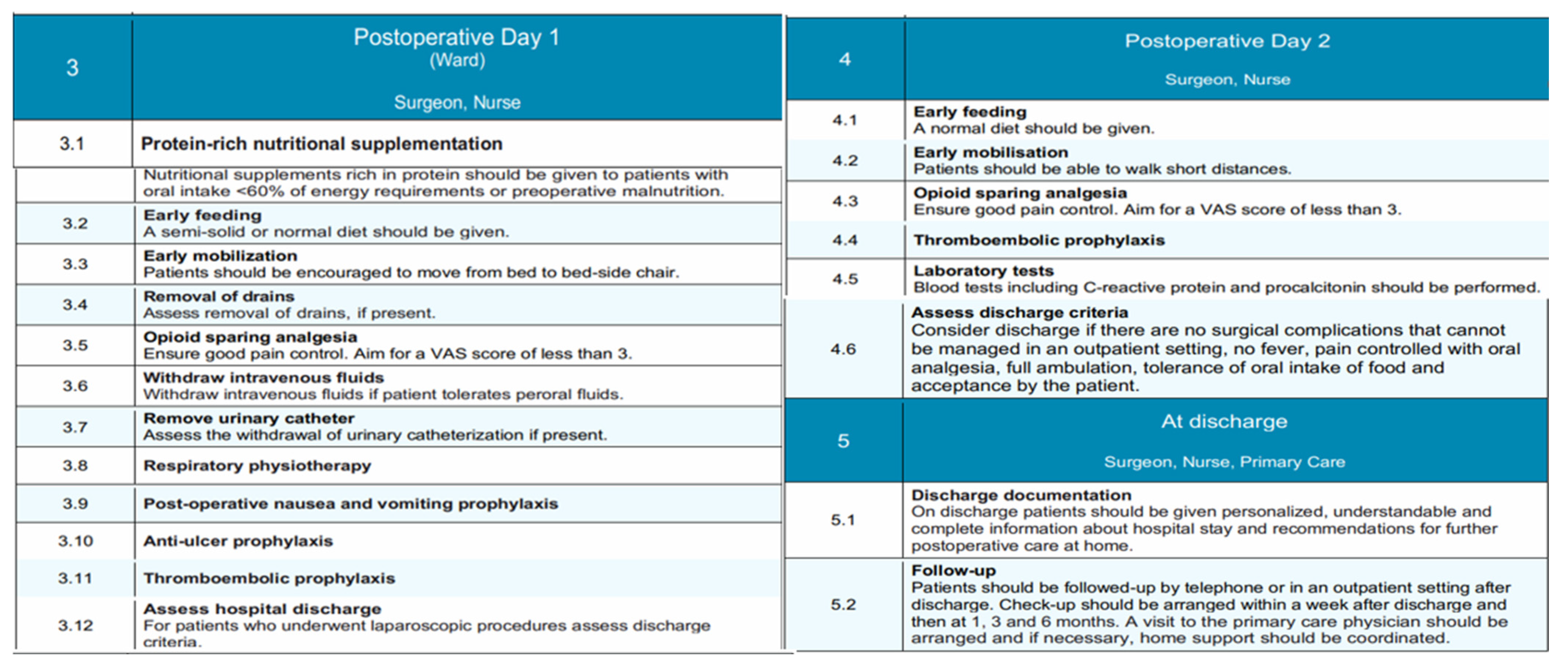
3.3. Postoperative Day 1 and 2 (Ward)
3.4. Discharge
4. Discussion
5. Enhanced Recovery After Surgery (ERAS) for Liver Resections
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| EUPEMEN | European Perioperative Medical Networking |
| ERAS | Enhanced Recovery After Surgery |
| Via RICA | Via Clinica de Recuperacion Intensificada en Cirugia Del Adulto |
| MUST | Malnutrition Universal Screening Tool |
| PONV | Postoperative Nausea and Vomiting |
| ASA | American Society of Anesthesiologists |
| LMWH | Low Molecular Weight Heparin |
| SSIs | Surgical Site Infections |
| WHO | World Health Organization |
| RSI | Rapid Sequence Induction |
| FiO2 | Fraction of Inspired Oxygen |
| EtCO2 | End-tidal carbon dioxide |
| GDT | Goal-directed fluid therapy |
| VAS | Visual Analogue Scale |
| LoS | Length of Stay |
References
- Agarwal, V.; Divatia, J.V. Enhanced recovery after surgery in liver resection: Current concepts and controversies. Korean J. Anesthesiol. 2019, 72, 119–129. [Google Scholar] [CrossRef] [PubMed]
- Kehlet, H.; Wilmore, D.W. Evidence-based surgical care and the evolution of fast-track surgery. Ann. Surg. 2008, 248, 189–198. [Google Scholar] [CrossRef]
- Bayramov, N.; Mammadova, S. A review of the current ERAS guidelines for liver resection, liver transplantation and pancreatoduodenectomy. Ann. Med. Surg. 2022, 82, 104596. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Damania, R.; Cocieru, A. Impact of enhanced recovery after surgery protocols on postoperative morbidity and mortality in patients undergoing routine hepatectomy: Review of the current evidence. Ann. Transl. Med. 2017, 5, 341. [Google Scholar] [CrossRef]
- van Dam, R.M.; Hendry, P.O.; Coolsen, M.M.E.; Bemelmans, M.H.A.; Lassen, K.; Revhaug, A.; Fearon, K.C.H.; Garden, O.J.; Dejong, C.H.C. Initial experience with a multimodal enhanced recovery programme in patients undergoing liver resection. Br. J. Surg. 2008, 95, 969–975. [Google Scholar] [CrossRef]
- Melloul, E.; Hübner, M.; Scott, M.; Snowden, C.; Prentis, J.; Dejong, C.H.C.; Garden, O.J.; Farges, O.; Kokudo, N.; Vauthey, J.; et al. Guidelines for Perioperative Care for Liver Surgery: Enhanced Recovery After Surgery (ERAS) Society Recommendations. World J. Surg. 2016, 40, 2425–2440. [Google Scholar] [CrossRef]
- Ioannidis, O.; Anestiadou, E.; Ramirez, J.M.; Fabbri, N.; Ubieto, J.M.; Feo, C.V.; Pesce, A.; Rosetzka, K.; Arroyo, A.; Kocián, P.; et al. The EUPEMEN (EUropean PErioperative MEdical Networking) Protocol for Acute Appendicitis: Recommendations for Perioperative Care. J. Clin. Med. 2024, 13, 6943. [Google Scholar] [CrossRef] [PubMed]
- Pesce, A.M.P.F.; Ramírez, J.M.; Fabbri, N.; Ubieto, J.M.; Bellosta, A.P.; Arroyo, A.; Sánchez-Guillén, L.; Whitley, A.; Kocián, P.; Rosetzka, K.; et al. The EUropean PErioperative MEdical Networking (EUPEMEN) project and recommendations for perioperative care in colorectal surgery: A quality improvement study. Int. J. Surg. 2024, 110, 4796–4803. [Google Scholar] [CrossRef] [PubMed]
- Ioannidis, O.; Ramirez, J.M.; Ubieto, J.M.; Feo, C.V.; Arroyo, A.; Kocián, P.; Sánchez-Guillén, L.; Bellosta, A.P.; Whitley, A.; Enguita, A.B.; et al. The EUPEMEN (EUropean PErioperative MEdical Networking) Protocol for Bowel Obstruction: Recommendations for Perioperative Care. J. Clin. Med. 2023, 12, 4185. [Google Scholar] [CrossRef]
- Ramirez, J.M.; Ruiz-López, P.; Gurumeta, A.A. CLINICAL PATHWAY Recovery Intensification for Optimal Care in Adult’s Surgery. Available online: https://www.researchgate.net/publication/354723117 (accessed on 24 April 2023).
- Broadbent, E.; Kahokehr, A.; Booth, R.J.; Thomas, J.; Windsor, J.A.; Buchanan, C.M.; Wheeler, B.R.; Sammour, T.; Hill, A.G. A brief relaxation intervention reduces stress and improves surgical wound healing response: A randomised trial. Brain Behav. Immun. 2012, 26, 212–217. [Google Scholar] [CrossRef]
- Kruzik, N. Benefits of Preoperative Education for Adult Elective Surgery Patients. AORN J. 2009, 90, 381–387. [Google Scholar] [CrossRef] [PubMed]
- Ronco, M.; Iona, L.; Fabbro, C.; Bulfone, G.; Palese, A. Patient education outcomes in surgery: A systematic review from 2004 to 2010. Int. J. Evid.-Based Healthc. 2012, 10, 309–323. [Google Scholar] [CrossRef]
- Kristensen, S.D.; Knuuti, J.; Saraste, A.; Anker, S.D.; Bøtker, H.E.; De Hert, S.; Ford, I.; Gonzalez-Juanatey, J.R.; Gorenek, B.; Heyndrickx, G.R.; et al. 2014 ESC/ESA Guidelines on non-cardiac surgery: Cardiovascular assessment and management: The Joint Task Force on non-cardiac surgery: Cardiovascular assessment and management of the European Society of Cardiology (ESC) and the European Society of Anaesthesiology (ESA). Eur. Heart J. 2014, 35, 2383–2431. [Google Scholar] [CrossRef]
- Deftereos, I.; Djordjevic, A.; Carter, V.M.; McNamara, J.; Yeung, J.M.; Kiss, N. Malnutrition screening tools in gastrointestinal cancer: A systematic review of concurrent validity. Surg. Oncol. 2021, 38, 101627. [Google Scholar] [CrossRef] [PubMed]
- Gaskill, C.E.; Kling, C.E.; Varghese, T.K.; Veenstra, D.L.; Thirlby, R.C.; Flum, D.R.; Alfonso-Cristancho, R. Financial benefit of a smoking cessation program prior to elective colorectal surgery. J. Surg. Res. 2017, 215, 183–189. [Google Scholar] [CrossRef] [PubMed]
- Shabanzadeh, D.M.; Sørensen, L.T. Alcohol consumption increases post-operative infection but not mortality: A systematic review and meta-analysis. Surg. Infect. 2015, 16, 657–668. [Google Scholar] [CrossRef] [PubMed]
- Dalton, A.; Zafirova, Z. Preoperative Management of the Geriatric Patient: Frailty and Cognitive Impairment Assessment. Anesthesiol. Clin. 2018, 36, 599–614. [Google Scholar] [CrossRef]
- Apfel, C.C.; Greim, C.A.; Haubitz, I.; Grundt, D.; Goepfert, C.; Sefrin, P.; Roewer, N. The discriminating power of a risk score for postoperative vomiting in adults undergoing various types of surgery. Acta Anaesthesiol. Scand. 1998, 42, 502–509. [Google Scholar] [CrossRef]
- Afshari, A.; Fenger-Eriksen, C.; Monreal, M.; Verhamme, P. European guidelines on perioperative venous thromboembolism prophylaxis. Eur. J. Anaesthesiol. 2018, 35, 112–115. [Google Scholar] [CrossRef]
- Vivas, D.; Roldán, I.; Ferrandis, R.; Marin, F.; Roldan, V.; Tello-Montoliu, A.; Ruiz-Nodar, J.M.; Gómez-Doblas, J.J.; Martín, A.; Llau, J.V.; et al. Perioperative and Periprocedural Management of Antithrombotic Therapy: Consensus Document of SEC, SEDAR, SEACV, SECTCV, AEC, SECPRE, SEPD, SEGO, SEHH, SETH, SEMERGEN, SEMFYC, SEMG, SEMICYUC, SEMI, SEMES, SEPAR, SENEC, SEO, SEPA, SERVEI, SECOT and AEU. Rev. Española De Cardiol. (Engl. Ed.) 2018, 71, 553–564. [Google Scholar] [CrossRef]
- Bilku, D.K.; Dennison, A.R.; Hall, T.C.; Metcalfe, M.S.; Garcea, G. Role of preoperative carbohydrate loading: A systematic review. Ann. R. Coll. Surg. Engl. 2014, 96, 15–22. [Google Scholar] [CrossRef] [PubMed]
- Md, S.; Mccall, J.; Gp, H.; Soop, M.; Nygren, J. Preoperative Carbohydrate Treatment for Enhancing Recovery after Elective Surgery (Review). 2014. Available online: http://www.thecochranelibrary.com (accessed on 24 April 2023).
- Brady, M.C.; Kinn, S.; Stuart, P.; Ness, V. Preoperative fasting for adults to prevent perioperative complications. Cochrane Database Syst. Rev. 2003, 2010, CD004423. [Google Scholar] [CrossRef]
- Allegranzi, B.; Zayed, B.; Bischoff, P.; Kubilay, N.Z.; de Jonge, S.; de Vries, F.; Gomes, S.M.; Gans, S.; Wallert, E.D.; Wu, X.; et al. New WHO recommendations on intraoperative and postoperative measures for surgical site infection prevention: An evidence-based global perspective. Lancet Infect. Dis. 2016, 16, e288–e303. [Google Scholar] [CrossRef]
- Badia, J.M.; Casey, A.L.; Petrosillo, N.; Hudson, P.M.; Mitchell, S.A.; Crosby, C. Impact of surgical site infection on healthcare costs and patient outcomes: A systematic review in six European countries. J. Hosp. Infect. 2017, 96, 1–15. [Google Scholar] [CrossRef]
- De Jager, E.; McKenna, C.; Bartlett, L.; Gunnarsson, R.; Ho, Y.H. Postoperative Adverse Events Inconsistently Improved by the World Health Organization Surgical Safety Checklist: A Systematic Literature Review of 25 Studies. World J. Surg. 2016, 40, 1842–1858. [Google Scholar] [CrossRef]
- Haynes, A.B.; Weiser, T.G.; Berry, W.R.; Lipsitz, S.R.; Breizat, A.-H.S.; Dellinger, E.P.; Herbosa, T.; Joseph, S.; Kibatala, P.L.; Lapitan, M.C.M.; et al. A Surgical Safety Checklist to Reduce Morbidity and Mortality in a Global Population. N. Engl. J. Med. 2009, 360, 491–499. [Google Scholar] [CrossRef]
- Wallace, C.; McGuire, B. Rapid sequence induction: Its place in modern anaesthesia. Contin. Educ. Anaesth. Crit. Care Pain 2014, 14, 130–135. [Google Scholar] [CrossRef]
- Pahade, A.; Mowar, A.; Singh, V.; Kharayat, U. Intraoperative Electrocardiogram Monitoring Induced Bispectral Index Interference—A Misleading Heart–Mind Connection. J. Indian Coll. Anaesthesiol. 2022, 1, 77–79. [Google Scholar] [CrossRef]
- Becker, D.E.; Casabianca, A.B. Respiratory Monitoring: Physiological and Technical Considerations. Anesth. Prog. 2009, 56, 14–20. [Google Scholar] [CrossRef]
- Tarello, D.; Giogà, F.; Lauterio, A.; Becchetti, C.; Perricone, G.; Santi, G.; Ragazzi, M.; Monti, G.; Lazzeri, M. Respiratory and physical therapy in the intensive care unit after liver transplantation for acute-on-chronic liver failure: A case report. Monaldi Arch. Chest Dis. 2024. [Google Scholar] [CrossRef]
- Koenen, M.; Passey, M.; Rolfe, M. “Keeping Them Warm”—A Randomized Controlled Trial of Two Passive Perioperative Warming Methods. J. Perianesthesia Nurs. 2017, 32, 188–198. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Kendrick, J.; Kaye, A.; Tong, Y.; Belani, K.; Urman, R.; Hoffman, C. Goal-directed fluid therapy in the perioperative setting. J. Anaesthesiol. Clin. Pharmacol. 2019, 35, 29–34. [Google Scholar] [CrossRef]
- Makaryus, R.; Miller, T.E.; Gan, T.J. Current concepts of fluid management in enhanced recovery pathways. Br. J. Anaesth. 2018, 120, 376–383. [Google Scholar] [CrossRef]
- Bacchin, M.R.; Ceria, C.M.; Giannone, S.; Ghisi, D.; Stagni, G.; Greggi, T.; Bonarelli, S. Goal-directed fluid therapy based on stroke volume variation in patients undergoing major spine surgery in the prone position. Spine 2016, 41, E1131–E1137. [Google Scholar] [CrossRef] [PubMed]
- Anyaehie, K.B.; Duryea, E.; Wang, J.; Echebelem, C.; Macias, D.; Sunna, M.; Ogunkua, O.; Joshi, G.P.; Gasanova, I. Multimodal opioid-sparing pain management for emergent cesarean delivery under general anesthesia: A quality improvement project. BMC Anesthesiol. 2022, 22, 239. [Google Scholar] [CrossRef] [PubMed]
- Dean, H.F.; King, E.; Gane, D.; Hocking, D.; Rogers, J.; Pullyblank, A. Introduction of a care bundle effectively and sustainably reduces patient-reported surgical site infection in patients undergoing colorectal surgery. J. Hosp. Infect. 2020, 105, 156–161. [Google Scholar] [CrossRef]
- Joshi, G.P.; Chung, F.; Vann, M.A.; Ahmad, S.; Gan, T.J.; Goulson, D.T.; Merrill, D.G.; Twersky, R. Society for ambulatory anesthesia consensus statement on perioperative blood glucose management in diabetic patients undergoing ambulatory surgery. Anesth. Analg. 2010, 111, 1378–1387. [Google Scholar] [CrossRef]
- Xu, R.; Hu, X.; Sun, Z.; Zhu, X.; Tang, Y. Incidence of postoperative hypothermia and shivering and risk factors in patients undergoing malignant tumor surgery: A retrospective study. BMC Anesthesiol. 2023, 23, 31. [Google Scholar] [CrossRef]
- Ghai, B.; Jafra, A.; Bhatia, N.; Chanana, N.; Bansal, D.; Mehta, V. Opioid sparing strategies for perioperative pain management other than regional anaesthesia: A narrative review. J. Anaesthesiol. Clin. Pharmacol. 2022, 38, 3–10. [Google Scholar] [CrossRef]
- Castelino, T.; Fiore, J.F.; Niculiseanu, P.; Landry, T.; Augustin, B.; Feldman, L.S. The effect of early mobilization protocols on postoperative outcomes following abdominal and thoracic surgery: A systematic review. Surgery 2016, 159, 991–1003. [Google Scholar] [CrossRef]
- de Almeida, E.; de Almeida, J.; Landoni, G.; Galas, F.R.B.G.; Fukushima, J.; Fominskiy, E.; de Brito, C.; Cavichio, L.; de Almeida, L.; Ribeiro-Jr, U.; et al. Early mobilization programme improves functional capacity after major abdominal cancer surgery: A randomized controlled trial. Br. J. Anaesth. 2017, 119, 900–907. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.; Yang, Z.; Tan, H. Perioperative nutritional support and fluid therapy in patients with liver diseases. Hepatobiliary Surg. Nutr. 2014, 3, 140–148. [Google Scholar] [CrossRef] [PubMed]
- Wolk, S.; Linke, S.; Bogner, A.; Sturm, D.; Meißner, T.; Müssle, B.; Rahbari, N.N.; Distler, M.; Weitz, J.; Welsch, T. Use of Activity Tracking in Major Visceral Surgery—The Enhanced Perioperative Mobilization Trial: A Randomized Controlled Trial. J. Gastrointest. Surg. 2019, 23, 1218–1226. [Google Scholar] [CrossRef]
- Kendall, F.; Oliveira, J.; Peleteiro, B.; Pinho, P.; Bastos, P.T. Inspiratory muscle training is effective to reduce postoperative pulmonary complications and length of hospital stay: A systematic review and meta-analysis. Disabil. Rehabil. 2018, 40, 864–882. [Google Scholar] [CrossRef] [PubMed]
- Alaparthi, G.K.; Augustine, A.J.; Anand, R.; Mahale, A. Comparison of Diaphragmatic Breathing Exercise, Volume and Flow Incentive Spirometry, on Diaphragm Excursion and Pulmonary Function in Patients Undergoing Laparoscopic Surgery: A Randomized Controlled Trial. Minim. Invasive Surg. 2016, 2016, 1967532. [Google Scholar] [CrossRef]
- Shepperd, S.; Lannin, N.A.; Clemson, L.M.; Mccluskey, A.; Cameron, I.D.; Barras, S.L. Discharge planning from hospital to home. Cochrane Database Syst. Rev. 2013, 2013, CD000313. [Google Scholar] [CrossRef]
- Golemi, I.; Salazar Adum, J.P.; Tafur, A.; Caprini, J. Venous thromboembolism prophylaxis using the Caprini score. Dis.-A-Mon. 2019, 65, 249–298. [Google Scholar] [CrossRef]
- Pieper, B.; Sieggreen, M.; Freeland, B.; Kulwicki, P.; Frattaroli, M.; Sidor, D.; Stasik, S.; Salerno, C.; Weissfeld, L.; Bindas, E.; et al. Wound Care: Discharge Information Needs of Patients After Surgery. J. Wound Ostomy Cont. Nurs. 2006, 33, 281–289. [Google Scholar] [CrossRef]
- Kehlet, H. Multimodal approach to control postoperative pathophysiology and rehabilitation. Br. J. Anaesth. 1997, 78, 606–617. [Google Scholar] [CrossRef]
- Taurchini, M.; Del Naja, C.; Tancredi, A. Enhanced Recovery After Surgery: A patient centered process. J. Vis. Surg. 2018, 4, 40. [Google Scholar] [CrossRef]
- Senturk, J.C.; Kristo, G.; Gold, J.; Bleday, R.; Whang, E. The Development of Enhanced Recovery after Surgery Across Surgical Specialties. J. Laparoendosc. Adv. Surg. Tech. 2017, 27, 863–870. [Google Scholar] [CrossRef] [PubMed]
- Coolsen, M.M.E.; Van Dam, R.M.; Van Der Wilt, A.A.; Slim, K.; Lassen, K.; Dejong, C.H.C. Systematic review and meta-analysis of enhanced recovery after pancreatic surgery with particular emphasis on pancreaticoduodenectomies. World J. Surg. 2013, 37, 1909–1918. [Google Scholar] [CrossRef]
- Greco, M.; Capretti, G.; Beretta, L.; Gemma, M.; Pecorelli, N.; Braga, M. Enhanced recovery program in colorectal surgery: A meta-analysis of randomized controlled trials. World J. Surg. 2014, 38, 1531–1541. [Google Scholar] [CrossRef]
- Ljungqvist, O.; Young-Fadok, T.; Demartines, N. The History of Enhanced Recovery after Surgery and the ERAS Society. J. Laparoendosc. Adv. Surg. Tech. 2017, 27, 860–862. [Google Scholar] [CrossRef]
- Li, L.; Chen, J.; Liu, Z.; Li, Q.; Shi, Y. Enhanced recovery program versus traditional care after hepatectomy: A meta-analysis. Medicine 2017, 96, e8052. [Google Scholar] [CrossRef]
- Zhao, Y.; Qin, H.; Wu, Y.; Xiang, B. Enhanced recovery after surgery program reduces length of hospital stay and complications in liver resection. Medicine 2017, 96, e7628. [Google Scholar] [CrossRef] [PubMed]
- Noba, L.; Rodgers, S.; Chandler, C.; Balfour, A.; Hariharan, D.; Yip, V.S. Enhanced Recovery After Surgery (ERAS) Reduces Hospital Costs and Improve Clinical Outcomes in Liver Surgery: A Systematic Review and Meta-Analysis. J. Gastrointest. Surg. 2020, 24, 918–932. [Google Scholar] [CrossRef]
- Martin, D.; Roulin, D.; Grass, F.; Addor, V.; Ljungqvist, O.; Demartines, N.; Hübner, M. A multicentre qualitative study assessing implementation of an Enhanced Recovery After Surgery program. Clin. Nutr. 2018, 37, 2172–2177. [Google Scholar] [CrossRef] [PubMed]
- Mithany, R.H.; Daniel, N.; Shahid, M.H.; Aslam, S.; Abdelmaseeh, M.; Gerges, F.; Gill, M.U.; Abdallah, S.B.; Hannan, A.; Saeed, M.T.; et al. Revolutionizing Surgical Care: The Power of Enhanced Recovery After Surgery (ERAS). Cureus 2023, 15, e48795. [Google Scholar] [CrossRef]
- Joliat, G.; Kobayashi, K.; Hasegawa, K.; Thomson, J.; Padbury, R.; Scott, M.; Brustia, R.; Scatton, O.; Cao, H.S.T.; Vauthey, J.; et al. Guidelines for Perioperative Care for Liver Surgery: Enhanced Recovery After Surgery (ERAS) Society Recommendations 2022. World J. Surg. 2023, 47, 11–34. [Google Scholar] [CrossRef]
- Ioannidis, O.; Anestiadou, E.; Ramirez, J.M.; Fabbri, N.; Ubieto, J.M.; Feo, C.V.; Pesce, A.; Rosetzka, K.; Arroyo, A.; Kocián, P.; et al. Improving Perioperative Care in Gastric Surgery: Insights from the EUropean PErioperative MEdical Networking (EUPEMEN) Project. J. Clin. Med. 2025, 14, 2108. [Google Scholar] [CrossRef] [PubMed]
- Hollis, J.L.; Seward, K.; Kocanda, L.; Collins, C.E.; Tully, B.; Brett, K.; Hunter, M.; Foureur, M.; Schumacher, T.; Lawrence, W.; et al. Evaluating a train-the-trainer model for scaling-up Healthy Conversation Skills training: A pre-post survey using the Theoretical Domains Framework. Patient Educ. Couns. 2022, 105, 3078–3085. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Aspect | Standard ERAS Protocol | EUPEMEN Protocol |
|---|---|---|
| Scope of Application | Global recommendations, generalized pathways | European-focused, procedure-specific adaptation |
| Development Process | Expert consensus by international societies | Multidisciplinary European network, consensus + clinical input |
| Procedure Specificity | General principles, adaptable | Highly detailed, procedure-specific protocols (e.g., liver, gastric, appendicitis) |
| Implementation Tools | Guidelines and clinical pathways | Online platform, multilingual manuals, train-the-trainer, audits |
| Target Audience | Surgeons, anesthetists, perioperative teams | Full multidisciplinary teams, incl. dietitians, nurses, primary care |
| Barriers Addressed | Limited guidance on barriers | Cultural, organizational, and resource barriers actively addressed |
| Monitoring and Sustainability | Variable adherence, limited audits | Embedded auditing and continuous improvement processes |
| Patient Engagement | Emphasized but center-dependent | Standardized counseling, shared decision-making, informed consent |
| Aim | Enhance recovery and reduce hospital stay | Harmonize European care, improve outcomes, reduce costs |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Published by MDPI on behalf of the Lithuanian University of Health Sciences. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ioannidis, O.; Koltsida, A.; Anestiadou, E.; Ramirez, J.M.; Fabbri, N.; Ubieto, J.M.; Feo, C.V.; Pesce, A.; Rosetzka, K.; Arroyo, A.; et al. Recommendations for Perioperative Care in Liver Resection: The EUPEMEN (EUropean PErioperative MEdical Networking) Protocol. Medicina 2025, 61, 978. https://doi.org/10.3390/medicina61060978
Ioannidis O, Koltsida A, Anestiadou E, Ramirez JM, Fabbri N, Ubieto JM, Feo CV, Pesce A, Rosetzka K, Arroyo A, et al. Recommendations for Perioperative Care in Liver Resection: The EUPEMEN (EUropean PErioperative MEdical Networking) Protocol. Medicina. 2025; 61(6):978. https://doi.org/10.3390/medicina61060978
Chicago/Turabian StyleIoannidis, Orestis, Aggeliki Koltsida, Elissavet Anestiadou, Jose M. Ramirez, Nicolò Fabbri, Javier Martínez Ubieto, Carlo Vittorio Feo, Antonio Pesce, Kristyna Rosetzka, Antonio Arroyo, and et al. 2025. "Recommendations for Perioperative Care in Liver Resection: The EUPEMEN (EUropean PErioperative MEdical Networking) Protocol" Medicina 61, no. 6: 978. https://doi.org/10.3390/medicina61060978
APA StyleIoannidis, O., Koltsida, A., Anestiadou, E., Ramirez, J. M., Fabbri, N., Ubieto, J. M., Feo, C. V., Pesce, A., Rosetzka, K., Arroyo, A., Kocián, P., Sánchez-Guillén, L., Bellosta, A. P., Whitley, A., Enguita, A. B., Teresa-Fernandéz, M., Bitsianis, S., & Symeonidis, S. (2025). Recommendations for Perioperative Care in Liver Resection: The EUPEMEN (EUropean PErioperative MEdical Networking) Protocol. Medicina, 61(6), 978. https://doi.org/10.3390/medicina61060978