Lower Vitamin D During Acute Exacerbation Is Associated with Very Severe Chronic Obstructive Pulmonary Disease

 , , ,
, , ,  ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Patients and Measurements
2.3. Statistical Analysis
3. Results
3.1. Serum Parameters by COPD Severity
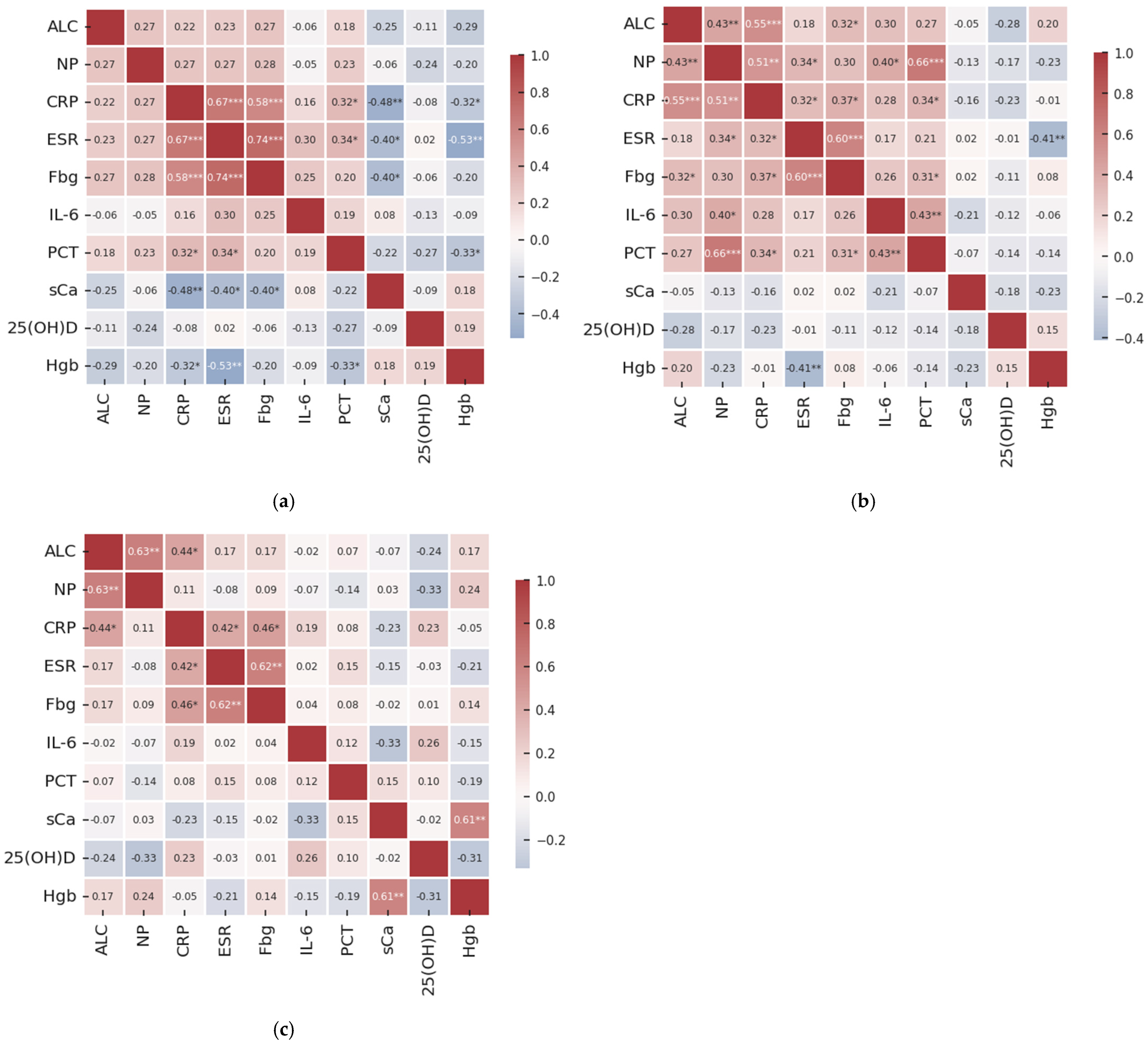
3.2. Correlational Patterns by COPD Severity
3.3. Discriminatory Ability of IL-6 and 25(OH)D Across COPD Severity Stages
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Popețiu, R.O.; Donath-Miklos, I.; Borta, S.M.; Rus, L.A.; Vîlcea, A.; Nica, D.V.; Pușchiță, M. Serum YKL-40 levels, leukocyte profiles, and acute exacerbations of advanced COPD. J. Clin. Med. 2023, 12, 6106. [Google Scholar] [CrossRef]
- Wheaton, A.G.; Liu, Y.; Croft, J.B.; VanFrank, B.; Croxton, T.L.; Punturieri, A.; Postow, L.; Greenlund, K.J. Chronic obstructive pulmonary disease and smoking status—United States, 2017. Morb. Mortal. Wkly. Rep. 2019, 68, 533–538. [Google Scholar] [CrossRef] [PubMed]
- Boers, E.; Barrett, M.; Su, J.G.; Benjafield, A.V.; Sinha, S.; Kaye, L.; Malhotra, A. Global burden of chronic obstructive pulmonary disease through 2050. JAMA Netw. Open 2023, 6, e2346598. [Google Scholar] [CrossRef] [PubMed]
- Zheng, X.-Y.; Zheng, Y.-J.; Liao, T.-T.; Xu, Y.-J.; Liu, L.; Wang, Y.; Xiao, N.; Li, C.; He, Z.-X.; Tan, X.-M.; et al. Effects of occupational exposure to dust, gas, vapor and fumes on chronic bronchitis and lung function. J. Thorac. Dis. 2024, 16, 356–367. [Google Scholar] [CrossRef]
- Mannino, D.M.; Roberts, M.H.; Mapel, D.W.; Zhang, Q.; Lunacsek, O.; Grabich, S.; Pollack, M.F. National and local direct medical cost burden of COPD in the United States. Chest 2024, 165, 1093–1106. [Google Scholar] [CrossRef]
- Chen, S.; Kuhn, M.; Prettner, K.; Yu, F.; Yang, T.; Bärnighausen, T.; Wang, C. The global economic burden of chronic obstructive pulmonary disease for 204 countries and territories in 2020–50: A health-augmented macroeconomic modelling study. Lancet Glob. Health 2023, 11, e1183–e1193. [Google Scholar] [CrossRef] [PubMed]
- Pratt, A.J.; Purssell, A.; Zhang, T.; Luks, V.P.; Bauza, X.; Mulpuru, S.; Cowan, J. Complexity in clinical diagnoses of acute exacerbation of chronic obstructive pulmonary disease. BMC Pulm. Med. 2023, 23, 298. [Google Scholar] [CrossRef]
- Ahmad, R.; Sarraj, B.; Razzaque, M.S. Vitamin D and mineral ion homeostasis: Endocrine dysregulation in chronic diseases. Front. Endocrinol. 2025, 16, 1493986. [Google Scholar] [CrossRef]
- Maes, K.; Gayan-Ramirez, G.; Janssens, W. Vitamin D and the Lung. In Feldman and Pike’s Vitamin D, 5th ed.; Feldman, D., Pike, J.W., Meyer, M., Eds.; Elsevier: Amsterdam, The Netherlands, 2024; Volume 1, pp. 997–1012. [Google Scholar] [CrossRef]
- Lu, K.; Tan, J.S.; Li, T.Q.; Yuan, J.; Wang, H.; Wang, W. An inverse causal association between genetically predicted vitamin D and chronic obstructive pulmonary disease risk. Front. Nutr. 2023, 10, 1111950. [Google Scholar] [CrossRef]
- Mullin, M.L.; Milne, S. Vitamin D deficiency in chronic obstructive pulmonary disease. Curr. Opin. Pulm. Med. 2023, 29, 96–103. [Google Scholar] [CrossRef]
- Zhu, Z.; Wan, X.; Liu, J.; Zhang, D.; Luo, P.; Du, W.; Fan, X. Vitamin D status and chronic obstructive pulmonary disease risk: A prospective UK biobank study. BMJ Open Respir. Res. 2023, 13, e064136. [Google Scholar] [CrossRef] [PubMed]
- Lokesh, K.S.; Chaya, S.K.; Jayaraj, B.S.; Praveena, A.S.; Krishna, M.; Madhivanan, P.; Mahesh, P.A. Vitamin D deficiency is associated with chronic obstructive pulmonary disease and exacerbation of COPD. Clin. Respir. J. 2021, 15, 389–399. [Google Scholar] [CrossRef] [PubMed]
- Zhu, M.; Wang, T.; Wang, C.; Ji, Y. The association between vitamin D and COPD risk, severity, and exacerbation: An updated systematic review and meta-analysis. Int. J. Chronic Obstr. Pulm. Dis. 2016, 11, 2597–2607. [Google Scholar] [CrossRef]
- Hanson, C.; Rutten, E.P.A.; Wouters, E.F.M.; Rennard, S. Diet and vitamin D as risk factors for lung impairment and COPD. Transl. Res. 2013, 162, 219–236. [Google Scholar] [CrossRef]
- Zhou, L.; Han, C.; Zhou, Y. The role of severe vitamin D deficiency in predicting the risk of severe exacerbation in patients with chronic obstructive pulmonary disease. Int. J. Chronic Obstr. Pulm. Dis. 2025, 20, 171–179. [Google Scholar] [CrossRef]
- Morsi, M.Y.M.; Shalan, I.M.; Sayed, W.H. Study of the role of vitamin d deficiency in patients with acute exacerbation of chronic obstructive pulmonary disease. Al-Azhar Int. Med. J. 2023, 4, 2. [Google Scholar] [CrossRef]
- Bhat, M.; Dar, S.; Waseem, M.; Nadeem, M. Baseline vitamin d as a predictor of mortality among hospitalized patients with acute exacerbations of chronic obstructive pulmonary disease in an endemically vitamin D-deficient area in North India. Indian J. Respir. Care 2020, 9, 88. [Google Scholar] [CrossRef]
- Burkes, R.M.; Ceppe, A.S.; Doerschuk, C.M.; Couper, D.; Hoffman, E.A.; Comellas, A.P.; Viviano, L. Associations among 25-Hydroxyvitamin d levels, lung function, and exacerbation outcomes in COPD: An analysis of the SPIROMICS cohort. Chest 2020, 157, 856–865. [Google Scholar] [CrossRef] [PubMed]
- Bellocchia, M.; Boita, M.; Patrucco, F.; Ferrero, C.; Verri, G.; Libertucci, D.; Bucca, C. Vitamin D deficiency and COPD exacerbations: Effect of vitamin D supplementation. Eur. Respir. J. 2015, 46, 3961. [Google Scholar] [CrossRef]
- Malinovschi, A.; Masoero, M.; Bellocchia, M.; Ciuffreda, A.; Solidoro, P.; Mattei, A.; Bucca, C. Severe vitamin D Deficiency is associated with frequent exacerbations and hospitalization in COPD patients. Respir. Res. 2014, 15, 131. [Google Scholar] [CrossRef]
- Williamson, A.; Martineau, A.R.; Jolliffe, D.; Sheikh, A.; Janssens, W.; Sluyter, J.; Griffiths, C.J. Vitamin D for the management of chronic obstructive pulmonary disease. Cochrane Database Syst. Rev. 2024, 9, CD013744. [Google Scholar] [CrossRef]
- Martineau, A.R.; Jolliffe, D.A.; Hooper, R.L.; Greenberg, L.; Aloia, J.F.; Bergman, P.; Camargo, C.A. Vitamin D supplementation to prevent acute respiratory tract infections: Systematic review and meta-analysis of individual participant data. BMJ 2017, 356, i6583. [Google Scholar] [CrossRef] [PubMed]
- Kunisaki, K.M.; Niewoehner, D.E.; Connett, J.E. Vitamin D Levels and risk of acute exacerbations of chronic obstructive pulmonary disease: A prospective cohort study. Am. J. Respir. Crit. Care Med. 2012, 185, 286–290. [Google Scholar] [CrossRef]
- Rocha, L.; Figueiredo, B.; Martins, S.E. How important is Vitamin D supplementation in the prevention of exacerbations in patients with chronic obstructive pulmonary disease (COPD): An evidence-based review. Cureus 2025, 17, e43562. [Google Scholar] [CrossRef]
- Ko, F.W.; Chan, K.P.; Hui, D.S.; Goddard, J.R.; Shaw, J.G.; Reid, D.W.; Yang, I.A. Acute exacerbation of COPD. Respirology 2016, 21, 1152–1165. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.W.R.; Leung, J.M.; Sin, D.D. A systematic review of diagnostic biomarkers of COPD exacerbation. PLoS ONE 2016, 11, e0158843. [Google Scholar] [CrossRef]
- Mou, S.; Zhang, W.; Deng, Y.; Tang, Z.; Jiang, D. Comparison of CRP, procalcitonin, neutrophil counts, eosinophil counts, sTREM-1, and OPN between pneumonic and nonpneumonic exacerbations in COPD patients. Can. Respir. J. 2022, 2022, 7609083. [Google Scholar] [CrossRef]
- Ramya, P.A.; Mohapatra, M.M.; Saka, V.K.; Kar, R.; Chakkalakkoombil, S.V.; Vemuri, M.B. Haematological and inflammatory biomarkers among stable COPD and acute exacerbations of COPD patients. Sultan Qaboos Univ. Med. J. 2023, 23, 239–244. [Google Scholar] [CrossRef] [PubMed]
- Sun, W.; Cao, Z.; Ma, Y.; Wang, J.; Zhang, L.; Luo, Z. Fibrinogen, a promising marker to evaluate severity and prognosis of acute exacerbation of chronic obstructive pulmonary disease: A retrospective observational study. Int. J. Chronic Obstr. Pulm. Dis. 2022, 17, 1299–1310. [Google Scholar] [CrossRef]
- Gjerazi, J.; Tashi, E.; Tashi, I.; Bushati, J. Seric markers and cell profile in blood and sputum in chronic obstructive pulmonary disease exacerbations (AECOPD). Int. J. Respir. Pulm. Med. 2019, 6, 109. [Google Scholar] [CrossRef]
- Ilisie, M.; Davidescu, L.; Genda, A.; Ulmeanu, R. Fibrinogen and CRP biomarkers in patients with exacerbation of COPD group C and D. Eur. Respir. J. 2014, 44, 3996. [Google Scholar] [CrossRef]
- Vitkina, T.I.; Sidletskaya, K.A. The role of interleukin-6 signaling in development of systemic inflammation in chronic obstructive pulmonary disease. Bull. Physiol. Pathol. Respir. 2018, 69, 97–106. [Google Scholar] [CrossRef]
- Zhang, J.; Bai, C. The significance of serum interleukin-8 in acute exacerbations of chronic obstructive pulmonary disease. Tanaffos 2018, 17, 13–21. [Google Scholar]
- Huang, A.X.; Lu, L.W.; Liu, W.J.; Huang, M. Plasma inflammatory cytokine IL-4, IL-8, IL-10, and TNF-α levels correlate with pulmonary function in patients with asthma-chronic obstructive pulmonary disease overlap syndrome. Med. Sci. Monit. 2016, 22, 2800–2808. [Google Scholar] [CrossRef]
- Balasubramanian, A.; Henderson, R.J.; Putcha, N.; Fawzy, A.; Raju, S.; Hansel, N.N.; MacIntyre, N.R.; Jensen, R.L.; Kinney, G.L.; Stringer, W.W.; et al. Haemoglobin as a biomarker for clinical outcomes in chronic obstructive pulmonary disease. ERJ Open Res. 2021, 7, 00318–02021. [Google Scholar] [CrossRef]
- Luo, Z.; Zhang, W.; Chen, L.; Xu, N. Prognostic value of neutrophil: Lymphocyte and platelet: Lymphocyte ratios for 28-day mortality of patients with AECOPD. Int. J. Gen. Med. 2021, 14, 2839–2848. [Google Scholar] [CrossRef] [PubMed]
- Yoon, E.C.; Koo, S.-M.; Park, H.Y.; Kim, H.C.; Kim, W.J.; Kim, K.U.; Jung, K.-S.; Yoo, K.H.; Yoon, H.K.; Yoon, H.-Y. Predictive role of white blood cell differential count for the development of acute exacerbation in Korean chronic obstructive pulmonary disease. Int. J. Chronic Obstr. Pulm. Dis. 2024, 19, 17–31. [Google Scholar] [CrossRef]
- Deep, A.; Behera, P.R.; Subhankar, S.; Rajendran, A.; Rao, C.M. Serum electrolytes in patients presenting with acute exacerbation of chronic obstructive pulmonary disease (COPD) and their comparison with stable COPD Patients. Cureus 2023, 15, e37482. [Google Scholar] [CrossRef]
- Qin, J.; Deng, X.; Wei, A.; Qin, Y.; Wu, Y.; Liao, L.; Lin, F. Correlation between hypocalcemia and acute exacerbation of chronic obstructive pulmonary disease in the elderly. Postgrad. Med. 2019, 131, 319–323. [Google Scholar] [CrossRef]
- Pantzaris, N.D.; Spilioti, D.X.; Psaromyalou, A.; Koniari, I.; Velissaris, D. The use of serum procalcitonin as a diagnostic and prognostic biomarker in chronic obstructive pulmonary disease exacerbations: A literature review update. J. Clin. Med. Res. 2018, 10, 545–551. [Google Scholar] [CrossRef]
- Qiyuan, P.; Changyang, L.; Gaigai, L.; Ju, Q.; Xun, Z. Prognostic value of procalcitonin in acute exacerbation of chronic obstructive pulmonary disease: A systematic review and meta-analysis. PLoS ONE 2024, 19, e0312099. [Google Scholar] [CrossRef] [PubMed]
- Jafari Nejad, S.H.; Behzadi, A.; Shafiepour, M.; Dalfardi, B.; Langari, A.A.; Ahmadipour, H.; Fekri, M.S. Comparison of serum procalcitonin levels between patients with acute exacerbation of chronic obstructive pulmonary disease (AECOPD) and patients with chronic obstructive pulmonary disease. Curr. Respir. Med. Rev. 2023, 19, 146–153. [Google Scholar] [CrossRef]
- Spitalului Clinic Județean de Urgență Arad. Available online: https://www.scjarad.ro/pneumologie-i/ (accessed on 26 April 2025).
- Grelus, A.; Nica, D.V.; Miklos, I.; Belengeanu, V.; Ioiart, I.; Popescu, C. Clinical significance of measuring global hydroxymethylation of white blood cell DNA in prostate cancer: Comparison to psa in a pilot exploratory study. Int. J. Mol. Sci. 2017, 18, 2465. [Google Scholar] [CrossRef]
- Global Initiative for Chronic Obstructive Lung Disease. Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease. 2023. Available online: https://goldcopd.org/wp-content/uploads/2023/03/GOLD-2023-ver-1.3-17Feb2023_WMV.pdf (accessed on 4 April 2025).
- Cooper, B.G.; Stocks, J.; Hall, G.L.; Culver, B.; Steenbruggen, I.; Carter, K.W.; Thompson, B.R.; Graham, B.L.; Miller, M.R.; Ruppel, G.; et al. The Global Lung Function Initiative (GLI) network: Bringing the world’s respiratory reference values together. Breathe 2017, 13, e56–e64. [Google Scholar] [CrossRef]
- Song, F.; Bachmann, M.O. Cumulative subgroup analysis to reduce waste in clinical research for individualised medicine. BMC Med. 2016, 14, 197. [Google Scholar] [CrossRef] [PubMed]
- Georgescu, M.; Drăghici, G.A.; Oancea, E.F.; Dehelean, C.A.; Şoica, C.; Vlăduţ, N.V.; Nica, D.V. Effects of cadmium sulfate on the brown garden snail Cornu aspersum: Implications for DNA Methylation. Toxics 2021, 9, 306. [Google Scholar] [CrossRef]
- Drăghici, G.A.; Dehelean, C.; Pinzaru, I.; Bordean, D.M.; Borozan, A.; Tsatsakis, A.M.; Nica, D. Soil copper uptake by land snails: A semi-field experiment with juvenile Cantareus aspersus snails. Environ. Toxicol. Pharmacol. 2019, 72, 103243. [Google Scholar] [CrossRef]
- Yuan, L.; Ni, J. The association between tobacco smoke exposure and vitamin D levels among US general population, 2001–2014: Temporal variation and inequalities in population susceptibility. Environ. Sci. Pollut. Res. 2022, 29, 32773–32787. [Google Scholar] [CrossRef]
- Sicard, P.; Agathokleous, E.; Anenberg, S.C.; De Marco, A.; Paoletti, E.; Calatayud, V. Trends in urban air pollution over the last two decades: A global perspective. Sci. Total Environ. 2023, 858, 160064. [Google Scholar] [CrossRef]
- Nieri, D.; Daniele, M.; Lombardi, S.; Bazzan, E.; Santerini, S.; De Cusatis, G.; Neri, T. Circulating extracellular vesicles are associated with disease severity and interleukin-6 levels in COPD: A pilot study. J. Clin. Med. 2021, 10, 5014. [Google Scholar] [CrossRef]
- Yadav, R.S.; Kant, S.; Tripathi, P.M.; Pathak, A.K.; Mahdi, A.A. Transcript levels of COX-2, TNF-α, IL-6 and IL-10 in chronic obstructive pulmonary disease: An association with smoking and severity. Res. J. Biotechnol. 2022, 17, 90. [Google Scholar] [CrossRef]
- Singh, S.; Verma, S.K.; Kumar, S.; Ahmad, M.K.; Nischal, A.; Singh, S.K.; Dixit, R.K. Correlation of severity of chronic obstructive pulmonary disease with potential biomarkers. Immunol. Lett. 2018, 196, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Abd Elnaby, E.A.; Abd Elnaiem, S.S.; Mostafa, A.I.; Sabry, D.; Alnaggar, A.R.I.; Haswa, M.K. Assessment of serum interleukin 6 level in patients with chronic obstructive pulmonary disease: Is it related to disease severity? Egypt. J. Bronchol. 2019, 13, 575–579. [Google Scholar] [CrossRef]
- Wei, J.; Xiong, X.F.; Lin, Y.H.; Zheng, B.X.; Cheng, D.Y. Association between serum interleukin-6 concentrations and chronic obstructive pulmonary disease: A systematic review and meta-analysis. PeerJ 2015, 3, e1199. [Google Scholar] [CrossRef]
- de Moraes, M.R.; da Costa, A.C.; Corrêa, K.D.S.; Junqueira-Kipnis, A.P.; Rabahi, M.F. Interleukin-6 and interleukin-8 blood levels’ poor association with the severity and clinical profile of ex-smokers with COPD. Int. J. Chronic Obstr. Pulm. Dis. 2014, 9, 735–743. [Google Scholar] [CrossRef]
- Harvanová, G.; Duranková, S. Inflammatory process: Factors inducing inflammation, forms and manifestations of inflammation, immunological significance of the inflammatory reaction. Alergol. Pol.-Pol. J. Allergol. 2025, 12, 54–61. [Google Scholar] [CrossRef]
- Mulvanny, A.; Pattwell, C.; Beech, A.; Southworth, T.; Singh, D. Validation of sputum biomarker immunoassays and cytokine expression profiles in COPD. Biomedicines 2022, 10, 1949. [Google Scholar] [CrossRef] [PubMed]
- Gamble, E.; Qiu, Y.; Wang, D.; Zhu, J.; Vignola, A.M.; Kroegel, C.; Jeffery, P.K. Variability of bronchial inflammation in chronic obstructive pulmonary disease: Implications for study design. Eur. Respir. J. 2006, 27, 293–299. [Google Scholar] [CrossRef]
- Xiong, X.F.; Zhu, M.; Wu, H.X.; Wu, Z.H.; Fan, L.L.; Cheng, D.Y. T-cell immune status in patients with acute exacerbation of chronic obstructive pulmonary disease: A case-control study. Front. Med. 2025, 12, 1433844. [Google Scholar] [CrossRef]
- Wilkinson, T.M. Immune Checkpoints in Chronic Obstructive Pulmonary Disease. Eur. Respir. Rev. 2017, 26, 170045. [Google Scholar] [CrossRef]
- Zheng, Z.; Zhu, B.; Zhu, B.; Xiao, C. Vitamin D deficiency is associated with the severity of COPD: A systematic review and meta-analysis. Int. J. Chronic Obstr. Pulm. Dis. 2015, 10, 1907–1916. [Google Scholar] [CrossRef] [PubMed]
- Blondeel, A.; Hermans, F.; Breuls, S.; Wuyts, M.; De Maeyer, N.; Verniest, T.; Demeyer, H. The Association of weather conditions with day-to-day variability in physical activity in patients with COPD. ERJ Open Res. 2023, 9, 00640-02023. [Google Scholar] [CrossRef] [PubMed]
- De Brandt, J.; Beijers, R.J.; Chiles, J.; Maddocks, M.; McDonald, M.L.N.; Schols, A.M.; Nyberg, A. Update on the etiology, assessment, and management of COPD cachexia: Considerations for the clinician. Int. J. Chronic Obstr. Pulm. Dis. 2022, 17, 2957–2976. [Google Scholar] [CrossRef]
- Mjid, M.; Zargouni, A.; Hedhli, A.; Euchi, K.; Ouahchi, Y.; Cheikhrouhou, S.; Dhahri, B. Does corticosteroid intake increase the risk of vitamin D deficiency in Tunisia’s COPD patients? Afr. Health Sci. 2023, 62, 1315. [Google Scholar]
- Fu, L.; Fei, J.; Tan, Z.X.; Chen, Y.H.; Hu, B.; Xiang, H.X.; Xu, D.X. Low vitamin D status is associated with inflammation in patients with chronic obstructive pulmonary disease. J. Immunol. 2021, 206, 515–523. [Google Scholar] [CrossRef]
- Fang, L.; Liu, K.; Liu, C.; Wang, X.; Ma, W.; Xu, W.; Sun, C. Tumor Accomplice: T cell exhaustion induced by chronic inflammation. Front. Immunol. 2022, 13, 979116. [Google Scholar] [CrossRef]
- Nikkholgh, A.; Tavakoli, F.; Alborzi, N.; Araste, F. Vitamin D attenuates cardiac hypertrophy in rats through mRNA Regulation of interleukin-6 and its receptor. Res. Cardiovasc. Med. 2023, 12, 123–128. [Google Scholar] [CrossRef]
- Xu, L.; Lee, M.; Jeyabalan, A.; Roberts, J.M. The Relationship of hypovitaminosis D and IL-6 in preeclampsia. Am. J. Obstet. Gynecol. 2013, 210, 149.e1–149.e7. [Google Scholar] [CrossRef]
- Lanser, L.; Fuchs, D.; Kurz, K.; Weiss, G. Physiology and inflammation driven pathophysiology of iron homeostasis—Mechanistic insights into anemia of inflammation and its treatment. Nutrients 2021, 13, 3732. [Google Scholar] [CrossRef]
- Iamartino, L.; Brandi, M.L. The calcium-sensing receptor in inflammation: Recent updates. Front. Physiol. 2022, 13, 1059369. [Google Scholar] [CrossRef]
- Qi, Y.; Yan, Y.; Tang, D.; Han, J.; Zhu, X.; Cui, M.; Fan, F. Inflammatory and immune mechanisms in COPD: Current status and therapeutic prospects. J. Inflamm. Res. 2024, 17, 6603–6618. [Google Scholar] [CrossRef] [PubMed]
- Overhage, J.M.; Overhage, L.M. Sensible Use of Observational Clinical Data. Stat. Methods Med. Res. 2013, 22, 7–13. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| n | Age | Origin Area | Sex | Smoking Status | ||||
|---|---|---|---|---|---|---|---|---|
| Urban | Rural | Female | Male | Non-Smoker | Smoker | |||
| Mild-to-moderate COPD | 40 | 67 (57–75) | 19 (47.5%) | 21 (52.5%) | 18 (45.0%) | 22 (55.0%) | 26 (65.0%) | 14 (35.0%) |
| Severe COPD | 41 | 62 (54–73) | 27 (65.85%) | 14 (34.15%) | 17 (41.46%) | 24 (58.54%) | 24 (58.54%) | 17 (41.46%) |
| Very severe COPD | 24 | 67 (58–72) | 19 (79.17%) | 5 (20.83%) | 10 (41.66%) | 14 (58.34%) | 13 (54.17%) | 11 (45.83%) |
| Sensitivity Analysis | |||||
|---|---|---|---|---|---|
| Variable | AUC | Optimal Threshold | Sensitivity | Specificity | p-Value |
| IL-6 | 0.635 | 2.86 | 0.528 | 0.835 | 0.042 * |
| 25(OH)D | 0.631 | 10.3 | 0.515 | 0.725 | 0.048 * |
| IL-6 + 25(OH)D | 0.653 | 0.289 | 0.572 | 0.778 | |
| LOO Regression | |||||
| β | OR | 95% CI Lower | 95% CI Upper | p-Value | |
| const | −0.178 | 0.83 | 0.31 | 2.25 | 0.724 |
| IL6 | −0.006 | 0.99 | 0.97 | 1.01 | 0.481 |
| 25(OH)D | −0.061 | 0.94 | 0.88 | 0.99 | 0.047 * |
| Variable | Reference Range | Mild-to-Moderate COPD | Severe COPD | Very Severe COPD | p-Value |
|---|---|---|---|---|---|
| ALC (×103/µL) | 4.00–10.00 | 9.70 (8.06–13.10) | 10.02 (8.09–11.55) | 10.60 (6.88–13.05) | 0.989 |
| NP (%) | 45–80 | 69.50 (61.30–81.75) | 74.80 (64.30–81.60) | 72.20 (66.70–77.40) | 0.638 |
| CRP (mg/L) | <5.00 | 10.15 (3.74–24.17) | 11.04 (6.01–29.16) | 16.54 (4.14–57.04) | 0.564 |
| ESR (mm/h) | 0–30 | 25 (10–30) | 20 (10–30) | 15 (5–35) | 0.543 |
| Fbg (mg/dL) | 200–400 | 441 (337–598) | 468 (382–538) | 441 (323–508) | 0.478 |
| IL-6 (pg/mL) | 0.00–7.00 | 6.83 (3.16–14.37) | 9.23 (4.18–13.69) | 3.37 (2.11–9.18) | 0.033 * |
| PCT (ng/dL) | 0.00–0.50 | 0.06 (0.04–0.12) | 0.06 (0.04–0.11) | 0.05 (0.03–0.12) | 0.819 |
| sCa (mg/dL) | 8.60–10.00 | 7.38 (7.37–7.41) | 7.39 (7.34–7.42) | 7.33 (7.21–7.41) | 0.297 |
| 25(OH)D (ng/mL) | 30–100 | 16.36 (9.89–25.69) | 16.43 (9.18–21.23) | 10.92 (7.52–19.66) | 0.047 * |
| Hgb (g/dL) | 11.70–17.30 | 13.70 (12.15–15.24) | 14.30 (12.90–15.70) | 13.75 (12.30–14.70) | 0.448 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Published by MDPI on behalf of the Lithuanian University of Health Sciences. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rus, L.A.; Popețiu, R.O.; Borta, S.M.; Vîlcea, A.; Nica, D.V.; Vintilă, T.; Măran, S.A.; Pușchiță, M. Lower Vitamin D During Acute Exacerbation Is Associated with Very Severe Chronic Obstructive Pulmonary Disease. Medicina 2025, 61, 979. https://doi.org/10.3390/medicina61060979
Rus LA, Popețiu RO, Borta SM, Vîlcea A, Nica DV, Vintilă T, Măran SA, Pușchiță M. Lower Vitamin D During Acute Exacerbation Is Associated with Very Severe Chronic Obstructive Pulmonary Disease. Medicina. 2025; 61(6):979. https://doi.org/10.3390/medicina61060979
Chicago/Turabian StyleRus, Larisa Alexandra, Romana Olivia Popețiu, Simona Maria Borta, Anamaria Vîlcea, Dragoș Vasile Nica, Teodor Vintilă, Stana Alina Măran, and Maria Pușchiță. 2025. "Lower Vitamin D During Acute Exacerbation Is Associated with Very Severe Chronic Obstructive Pulmonary Disease" Medicina 61, no. 6: 979. https://doi.org/10.3390/medicina61060979
APA StyleRus, L. A., Popețiu, R. O., Borta, S. M., Vîlcea, A., Nica, D. V., Vintilă, T., Măran, S. A., & Pușchiță, M. (2025). Lower Vitamin D During Acute Exacerbation Is Associated with Very Severe Chronic Obstructive Pulmonary Disease. Medicina, 61(6), 979. https://doi.org/10.3390/medicina61060979