

How I Follow Hodgkin Lymphoma in First Complete (Metabolic) Remission?


Abstract
1. Introduction
2. The Short Overview of Hodgkin Lymphoma Treatment
3. How to Detect the Relapse of Hodgkin Lymphoma
4. Survivorship among HL patients with First Complete Remission
5. Secondary Solid Tumors
5.1. Secondary Breast Cancer
5.2. Secondary Pulmonary Cancer
6. Secondary Hematological Malignancies
7. Cardiovascular Toxicity
8. Sexual Gonadal Toxicity
8.1. Male Survivors
8.2. Female Survivors
9. Brentuximab Vedotin-Induced Neuropathy
10. Fatigue and Quality of Life
11. Thyorid Dysfunction
12. Where Are We Now in 2023? Maximizing Cure Rate and Minimizing Toxicity
12.1. Advanced Disease
12.1.1. BrECADD
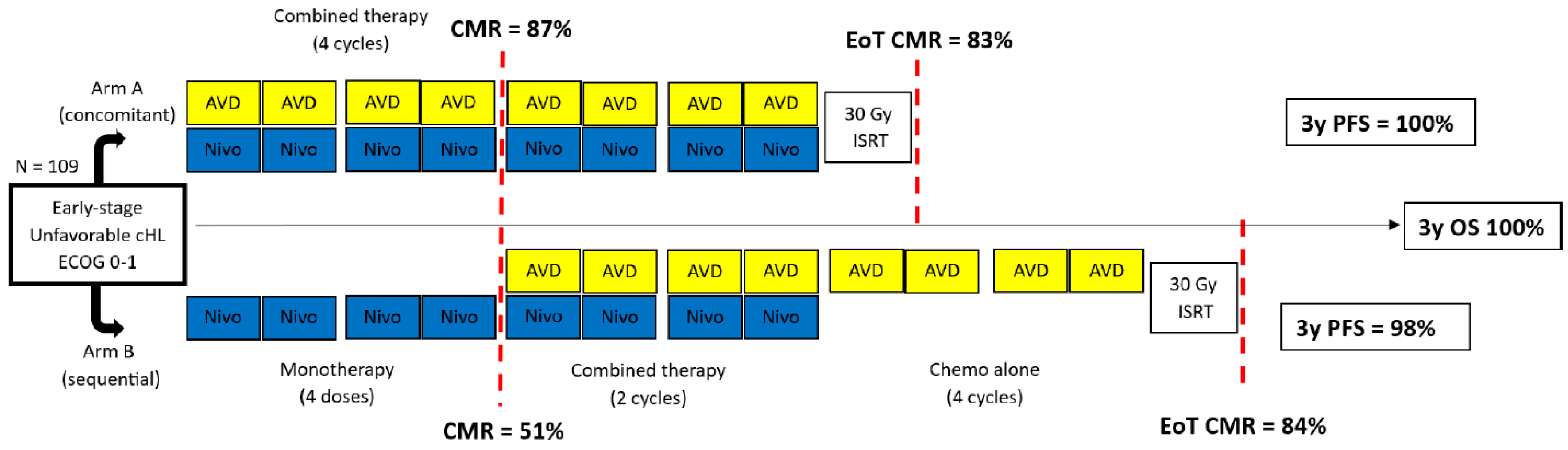
12.1.2. Nivolumab
12.1.3. The Role and Improvement of Radiotherapy in HL
13. Conclusions
Funding
Conflicts of Interest
Abbreviations
| HL | Hodgkin lymphoma |
| MOPP | mechlorethamine, vincristine, procarbazine, and prednisone |
| ASCO | American Society of Clinical Oncology |
| ABVD | doxorubicin, bleomycin, vinblastine, and dacarbazine |
| BEACOPPesc | bleomycin, etoposide, doxorubicin, cyclophosphamide, vincristine, procarbazine, and prednisone |
| INRT | involved-node radiotherapy |
| PET-CT | positron emission tomography–computed tomography |
| PFS | progression-free survival |
| OS | overall survival |
| HD | Hodgkin disease |
| EFS | event-free survival |
| GHSG | German Hodgkin Study Group |
| BV | brentuximab vedotin |
| AVD | doxorubicin, vinblastine, and dacarbazine |
| RCT | randomized clinical trial |
| PET | positron emission tomography |
| ESMO | European Society of Medical Oncology |
| US | United States |
| NCCN | National Comprehensive Cancer Care |
| CT | computed tomography |
| ACR | American College of Radiology |
| MSCT | multislice computed tomography |
| USD | Unites States dollar |
| PPV | positive predictive value |
| GELTAMO | group of lymphomas/autologous bone marrow transplantation |
| mSV | millisievert |
| NPV | negative predictive value |
| iPET | interim positron emission tomography |
| SMR | standard mortality ratio |
| CI | confidential interval |
| SBC | secondary breast cancer |
| RR | relative risk |
| Gy | gray |
| SEER | surveillance, epidemiology, and end results |
| NSLC | non-small cell lung cancer |
| SCLC | small cell lung cancer |
| tAML | therapy-related acute myeloid leukemia |
| tMDS | therapy-related myelodysplastic syndrome |
| CHD | chronic heart disease |
| VHD | valvular heart disease |
| HF | heart failure |
| CR | complete remission |
| EORTC | European Organisation for. Research and Treatment of Cancer |
| LYSA | The Lymphoma Study Association |
| LSQ | Life Situation Questionnaire |
| PBVD | lyposomal doxorubicin, bleomycin, vinblastine, and dacarbazine |
| MR | magnetic resonance |
| ART | artificial reproductive techniques |
| POF | premature ovarian failure |
| GNRH-a | gonadotropin-releasing hormone analogs |
| BVIN | brentuximab vedotin-induced neuropathy |
| CMR | complete metabolic remission |
| AE | adverse event |
| QoL | quality of life |
| SF36 | 36-Item Short Form Health |
| BrECAPP | brentuximab vedotin, etoposide, doxorubicin, procarbazine, and prednisone |
| BrECADD | brentuximab vedotin, etoposide, doxorubicin, cyclophosphamide, dacarbazine, and dexamethasone |
| TRMB | treatment-related morbidity |
| HR | hazard ratio |
| PD-1/PD-L1 | programmed death-1, programmed death-ligand 1 |
| ALT | alanine transaminase |
| AST | aspartate transferase |
| BV-APE-PC | brentuximab vedotin, doxorubicin, bleomycin, vincristine, etoposide, prednisone, and cyclophosphamide |
References
- SEER Cancer Stat Facts: Hodgkin Lymphoma. Available online: https://seer.cancer.gov/statfacts/html/hodg.html (accessed on 16 September 2023).
- Cooper, I.A.; Rana, C.; Madigan, J.P.; Motteram, R.; Maritz, J.S.; Turner, C.N. Combination chemotherapy (MOPP) in the man-agement of advanced Hodgkin’s disease. A progress report on 55 patients. Med. J. Aust. 1972, 1, 41–49. [Google Scholar] [CrossRef]
- ASCO Connection. ASCO Announces “Top 5” Advances in Modern Oncology. Available online: https://connection.asco.org/magazine/features/asco-announces-%E2%80%9Ctop-5%E2%80%9D-advances-modern-oncology (accessed on 16 September 2023).
- Fuchs, M.; Goergen, H.; Kobe, C.; Kuhnert, G.; Lohri, A.; Greil, R.; Sasse, S.; Topp, M.S.; Schäfer, E.; Hertenstein, B.; et al. Positron Emission Tomography–Guided Treatment in Early-Stage Favorable Hodgkin Lymphoma: Final Results of the International, Randomized Phase III HD16 Trial by the German Hodgkin Study Group. J. Clin. Oncol. 2019, 37, 2835–2845. [Google Scholar] [CrossRef]
- Skoetz, N.; Will, A.; Monsef, I.; Brillant, C.; Engert, A.; Von Tresckow, B. Comparison of first-line chemotherapy including escalated BEACOPP versus chemotherapy including ABVD for people with early unfavourable or advanced stage Hodgkin lymphoma. Cochrane Database Syst. Rev. 2017, 5, CD007941. [Google Scholar] [CrossRef]
- Borchmann, P.; Goergen, H.; Kobe, C.; Lohri, A.; Greil, R.; Eichenauer, D.A.; Zijlstra, J.M.; Markova, J.; Meissner, J.; Feuring-Buske, M.; et al. PET-guided treatment in patients with advanced-stage Hodgkin’s lymphoma (HD18): Final results of an open-label, international, randomised phase 3 trial by the German Hodgkin Study Group. Lancet 2017, 390, 2790–2802. [Google Scholar] [CrossRef]
- Viviani, S.; Zinzani, P.L.; Rambaldi, A.; Brusamolino, E.; Levis, A.; Bonfante, V.; Vitolo, U.; Pulsoni, A.; Liberati, A.M.; Specchia, G.; et al. ABVD versus BEACOPP for Hodgkin’s Lymphoma When High-Dose Salvage Is Planned. N. Engl. J. Med. 2011, 365, 203–212. [Google Scholar] [CrossRef]
- Ansell, S.M.; Radford, J.; Connors, J.M.; Długosz-Danecka, M.; Kim, W.-S.; Gallamini, A.; Ramchandren, R.; Friedberg, J.W.; Advani, R.; Hutchings, M.; et al. Overall Survival with Brentuximab Vedotin in Stage III or IV Hodgkin’s Lymphoma. N. Engl. J. Med. 2022, 387, 310–320. [Google Scholar] [CrossRef] [PubMed]
- Johnson, P.; Federico, M.; Kirkwood, A.; Fosså, A.; Berkahn, L.; Carella, A.; D’amore, F.; Enblad, G.; Franceschetto, A.; Fulham, M.; et al. Adapted Treatment Guided by Interim PET-CT Scan in Advanced Hodgkin’s Lymphoma. New Engl. J. Med. 2016, 374, 2419–2429. [Google Scholar] [CrossRef] [PubMed]
- Vellemans, H.; André, M.P.E. Review of Treatment Options for the Management of Advanced Stage Hodgkin Lymphoma. Cancers 2021, 13, 3745. [Google Scholar] [CrossRef] [PubMed]
- Casasnovas, R.-O.; Bouabdallah, R.; Brice, P.; Lazarovici, J.; Ghesquieres, H.; Stamatoullas, A.; Dupuis, J.; Gac, A.-C.; Gastinne, T.; Joly, B.; et al. PET-adapted treatment for newly diagnosed advanced Hodgkin lymphoma (AHL2011): A randomised, multicentre, non-inferiority, phase 3 study. Lancet Oncol. 2019, 20, 202–215. [Google Scholar] [CrossRef] [PubMed]
- Zinzani, P.L.; Broccoli, A.; Gioia, D.M.; Castagnoli, A.; Ciccone, G.; Evangelista, A.; Santoro, A.; Ricardi, U.; Bonfichi, M.; Brusamolino, E.; et al. Interim Positron Emission Tomography Response–Adapted Therapy in Advanced-Stage Hodgkin Lymphoma: Final Results of the Phase II Part of the HD0801 Study. J. Clin. Oncol. 2016, 34, 1376–1385. [Google Scholar] [CrossRef]
- Gallamini, A.; Tarella, C.; Viviani, S.; Rossi, A.; Patti, C.; Mulé, A.; Picardi, M.; Romano, A.; Cantonetti, M.; La Nasa, G.; et al. Early Chemotherapy Intensification with Escalated BEACOPP in Patients with Advanced-Stage Hodgkin Lymphoma with a Positive Interim Positron Emission Tomography/Computed Tomography Scan After Two ABVD Cycles: Long-Term Results of the GITIL/FIL HD 0607 Trial. J. Clin. Oncol. 2018, 36, 454–462. [Google Scholar] [CrossRef]
- Press, O.W.; Li, H.; Schöder, H.; Straus, D.J.; Moskowitz, C.H.; LeBlanc, M.; Rimsza, L.M.; Bartlett, N.L.; Evens, A.M.; Mittra, E.S.; et al. US Intergroup Trial of Response-Adapted Therapy for Stage III to IV Hodgkin Lymphoma Using Early Interim Fluorodeoxyglucose–Positron Emission Tomography Imaging: Southwest Oncology Group S0816. J. Clin. Oncol. 2016, 34, 2020–2027. [Google Scholar] [CrossRef]
- Viviani, S.; Vanazzi, A.; Frassoni, S.; Rusconi, C.; Rossi, A.; Romano, A.; Patti, C.; Schiavotto, C.; Sorasio, R.; Marasco, V.; et al. High-dose chemotherapy and autologous stem cell transplant as first salvage treatment for relapsed or refractory Hodgkin Lymphoma in the era of PET-adapted strategies. Leuk. Lymphoma, 2024; online ahead of print. [Google Scholar] [CrossRef]
- Brice, P. Managing relapsed and refractory Hodgkin lymphoma. Br. J. Haematol. 2008, 141, 3–13. [Google Scholar] [CrossRef]
- Dalal, M.; Gupta, J.; Price, K.; Zomas, A.; Miao, H.; Ashaye, A. Efficacy and safety of front-line treatments for advanced Hodgkin lymphoma: A systematic literature review. Expert Rev. Hematol. 2020, 13, 907–922. [Google Scholar] [CrossRef]
- Eichenauer, D.A.; Aleman, B.M.P.; André, M.; Federico, M.; Hutchings, M.; Illidge, T.; Engert, A.; Ladetto, M.; ESMO Guidelines Committee. Hodgkin lymphoma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2018, 29, iv19–iv29. [Google Scholar] [CrossRef] [PubMed]
- Follows, G.A.; Barrington, S.F.; Bhuller, K.S.; Culligan, D.J.; Cutter, D.J.; Gallop-Evans, E.; Kassam, S.; Osborne, W.; Sadullah, S.; Townsend, W.; et al. Guideline for the first-line management of Classical Hodgkin Lymphoma—A British Society for Haematology guideline. Br. J. Haematol. 2022, 197, 558–572. [Google Scholar] [CrossRef] [PubMed]
- Hoppe, R.T.; Advani, R.H.; Ai, W.Z.; Ambinder, R.F.; Armand, P.; Bello, C.M.; Benitez, C.M.; Chen, W.; Dabaja, B.; Daly, M.E.; et al. NCCN Guidelines® Insights: Hodgkin Lymphoma, Version 2.2022. J. Natl. Compr. Cancer Netw. 2022, 20, 322–334. [Google Scholar] [CrossRef] [PubMed]
- Ng, A.; Constine, L.S.; Advani, R.; Das, P.; Flowers, C.; Friedberg, J.; Hodgson, D.C.; Schwartz, C.L.; Wilder, R.B.; Wilson, L.D.; et al. ACR Appropriateness Criteria: Follow-Up of Hodgkin’s Lymphoma. Curr. Probl. Cancer 2010, 34, 211–227. [Google Scholar] [CrossRef] [PubMed]
- Zinzani, P.L.; Stefoni, V.; Tani, M.; Fanti, S.; Musuraca, G.; Castellucci, P.; Marchi, E.; Fina, M.; Ambrosini, V.; Pellegrini, C.; et al. Role of [18F]Fluorodeoxyglucose Positron Emission Tomography Scan in the Follow-Up of Lymphoma. J. Clin. Oncol. 2009, 27, 1781–1787. [Google Scholar] [CrossRef] [PubMed]
- Gandikota, N.; Hartridge-Lambert, S.; Migliacci, J.C.; Yahalom, J.; Portlock, C.S.; Schöder, H. Very low utility of surveillance imaging in early-stage classic Hodgkin lymphoma treated with a combination of doxorubicin, bleomycin, vinblastine, and dacarbazine and radiation therapy. Cancer 2015, 121, 1985–1992. [Google Scholar] [CrossRef]
- Glober, G.; Gunther, J.; Fang, P.; Milgrom, S.; Korivi, B.R.; Jensen, C.T.; Wagner-Bartak, N.A.; Ahmed, S.; Lee, H.J.; Nair, R.; et al. Imaging Surveillance of Limited-stage Classic Hodgkin Lymphoma Patients After PET–CT-documented First Remission. Clin. Lymphoma Myeloma Leuk. 2020, 20, 533–541. [Google Scholar] [CrossRef] [PubMed]
- Lee, A.I.; Zuckerman, D.S.; Abbeele, A.D.V.D.; Aquino, S.L.; Crowley, D.; Toomey, C.; Lacasce, A.S.; Feng, Y.; Neuberg, D.S.; Hochberg, E.P. Surveillance imaging of Hodgkin lymphoma patients in first remission: A clinical and economic analysis. Cancer 2010, 116, 3835–3842. [Google Scholar] [CrossRef] [PubMed]
- Cheson, B.D.; Fisher, R.I.; Barrington, S.F.; Cavalli, F.; Schwartz, L.H.; Zucca, E.; Lister, T.A. Recommendations for initial evaluation, stag-ing, and response assessment of Hodgkin and non-Hodgkin lymphoma: The Lugano classification. J. Clin. Oncol. 2014, 32, 3059–3068. [Google Scholar] [CrossRef] [PubMed]
- Mocikova, H.; Obrtlikova, P.; Vackova, B.; Trneny, M. Positron emission tomography at the end of first-line therapy and during follow-up in patients with Hodgkin lymphoma: A retrospective study. Ann. Oncol. 2010, 21, 1222–1227. [Google Scholar] [CrossRef] [PubMed]
- El-Galaly, T.C.; Mylam, K.J.; Brown, P.; Specht, L.; Christiansen, I.; Munksgaard, L.; Johnsen, H.E.; Loft, A.; Bukh, A.; Iyer, V.; et al. Positron emission tomography/computed tomography surveillance in patients with Hodgkin lymphoma in first remission has a low positive predictive value and high costs. Haematologica 2012, 97, 931–936. [Google Scholar] [CrossRef] [PubMed]
- Oreiro, M.B.; Martín, R.; Gomez, P.; Muñoz, N.L.; Rodriguez, A.; Liébana, M.; Navarro, B.; Sánchez-González, B.; Marí, P.; de Oteiza, J.P.; et al. SEGHI Study: Defining the Best Surveillance Strategy in Hodgkin Lymphoma after First-Line Treatment. Cancers 2021, 13, 2412. [Google Scholar] [CrossRef] [PubMed]
- Smith-Bindman, R.; Lipson, J.; Marcus, R.; Kim, K.P.; Mahesh, M.; Gould, R.; de González, A.B.; Miglioretti, D.L. Radiation Dose Associated with Common Computed Tomography Examinations and the Associated Lifetime Attributable Risk of Cancer. Arch. Intern. Med. 2009, 169, 2078–2086. [Google Scholar] [CrossRef]
- Picardi, M.; Pugliese, N.; Cirillo, M.; Zeppa, P.; Cozzolino, I.; Ciancia, G.; Pettinato, G.; Salvatore, C.; Quintarelli, C.; Pane, F. Advanced-stage Hodgkin Lymphoma: US/Chest Radiography for Detection of Relapse in Patients in First Complete Remission—A Randomized Trial of Routine Surveillance Imaging Procedures. Radiology 2014, 272, 262–274. [Google Scholar] [CrossRef]
- Andersen, M.D.; Hamilton-Dutoit, S.; Modvig, L.; Vase, M.; Christiansen, I.; Christensen, J.H.; Dahl-Sørensen, R.B.; Stoltenberg, D.; Kamper, P.; D’Amore, F. Late recurrence of lymphoid malignancies after initial treatment for Hodgkin lymphoma—A study from the Danish Lymphoma Registry. Br. J. Haematol. 2022, 198, 50–61. [Google Scholar] [CrossRef]
- Bröckelmann, P.J.; Goergen, H.; Kohnhorst, C.; von Tresckow, B.; Moccia, A.; Markova, J.; Meissner, J.; Kerkhoff, A.; Ludwig, W.-D.; Fuchs, M.; et al. Late Relapse of Classical Hodgkin Lymphoma: An Analysis of the German Hodgkin Study Group HD7 to HD12 Trials. J. Clin. Oncol. 2017, 35, 1444–1450. [Google Scholar] [CrossRef]
- Núñez-García, B.; Clemente, M.B.; Sánchez, J.C.; Royuela, A.; de Ibargüen, B.C.S.; Méndez, M.; López-Ibor, J.V.; Martínez, M.; Traseira, C.; Garitaonaindia, Y.; et al. Long-term outcomes in Hodgkin lymphoma survivors. Temporary trends and comparison with general population. Hematol. Oncol. 2023, 41, 407–414. [Google Scholar] [CrossRef]
- Ibrahim, E.M.; Abouelkhair, K.M.; Kazkaz, G.A.; Elmasri, O.A.; Al-Foheidi, M. Risk of second breast cancer in female Hodgkin’s lymphoma survivors: A meta-analysis. BMC Cancer 2012, 12, 197. [Google Scholar] [CrossRef] [PubMed]
- Conway, J.L.; Connors, J.M.; Tyldesley, S.; Savage, K.J.; Campbell, B.A.; Zheng, Y.Y.; Hamm, J.; Pickles, T. Secondary Breast Cancer Risk by Radiation Volume in Women with Hodgkin Lymphoma. Int. J. Radiat. Oncol. Biol. Phys. 2017, 97, 35–41. [Google Scholar] [CrossRef]
- Milano, M.T.; Li, H.; Gail, M.H.; Constine, L.S.; Travis, L.B. Long-Term Survival Among Patients with Hodgkin’s Lymphoma Who Developed Breast Cancer: A Population-Based Study. J. Clin. Oncol. 2010, 28, 5088–5096. [Google Scholar] [CrossRef]
- Bakkach, J.; Pellegrino, B.; Elghazawy, H.; Novosad, O.; Agrawal, S.; Mechita, M.B. Current overview and special considerations for second breast cancer in Hodgkin lymphoma survivors. Crit. Rev. Oncol. Hematol. 2021, 157, 103175. [Google Scholar] [CrossRef] [PubMed]
- Diller, L.; Nancarrow, C.M.; Shaffer, K.; Matulonis, U.; Mauch, P.; Neuberg, D.; Tarbell, N.J.; Litman, H.; Garber, J. Breast Cancer Screening in Women Previously Treated for Hodgkin’s Disease: A Prospective Cohort Study. J. Clin. Oncol. 2002, 20, 2085–2091. [Google Scholar] [CrossRef]
- Lorigan, P.; Radford, J.; Howell, A.; Thatcher, N. Lung cancer after treatment for Hodgkin’s lymphoma: A systematic review. Lancet Oncol. 2005, 6, 773–779. [Google Scholar] [CrossRef]
- Lin, L.; Wang, D.; Chen, H. The characteristics and survival of second primary lung cancer after Hodgkin’s lymphoma: A comparison with first primary lung cancer using the SEER database. PLoS ONE 2023, 18, e0285766. [Google Scholar] [CrossRef]
- Hoffman, R.M.; Atallah, R.P.; Struble, R.D.; Badgett, R.G. Lung Cancer Screening with Low-Dose CT: A Meta-Analysis. J. Gen. Intern. Med. 2020, 35, 3015–3025. [Google Scholar] [CrossRef] [PubMed]
- Chua, C.C.; Fleming, S.; Wei, A.H. Clinicopathological aspects of therapy-related acute myeloid leukemia and myelodysplastic syndrome. Best Pract. Res. Clin. Haematol. 2019, 32, 3–12. [Google Scholar] [CrossRef]
- Delwail, V.; Jais, J.; Colonna, P.; Andrieu, J. Fifteen-year secondary leukaemia risk observed in 761 patients with Hodgkin’s disease prospectively treated by MOPP or ABVD chemotherapy plus high-dose irradiation. Br. J. Haematol. 2002, 118, 189–194. [Google Scholar] [CrossRef]
- Koontz, M.Z.; Horning, S.J.; Balise, R.; Greenberg, P.L.; Rosenberg, S.A.; Hoppe, R.T.; Advani, R.H. Risk of Therapy-Related Secondary Leukemia in Hodgkin Lymphoma: The Stanford University Experience Over Three Generations of Clinical Trials. J. Clin. Oncol. 2013, 31, 592–598. [Google Scholar] [CrossRef]
- Eichenauer, D.A.; Thielen, I.; Haverkamp, H.; Franklin, J.; Behringer, K.; Halbsguth, T.; Klimm, B.; Diehl, V.; Sasse, S.; Rothe, A.; et al. Therapy-related acute myeloid leukemia and myelodysplastic syndromes in patients with Hodgkin lymphoma: A report from the German Hodgkin Study Group. Blood 2014, 123, 1658–1664. [Google Scholar] [CrossRef]
- Franklin, J.; Eichenauer, D.A.; Becker, I.; Monsef, I.; Engert, A. Optimisation of chemotherapy and radiotherapy for untreated Hodgkin lymphoma patients with respect to second malignant neoplasms, overall and progression-free survival: Individual participant data analysis. Cochrane Database Syst. Rev. 2017, 2017, CD008814. [Google Scholar] [CrossRef]
- Van Nimwegen, F.A.; Schaapveld, M.; Janus, C.P.M.; Krol, A.D.G.; Petersen, E.J.; Raemaekers, J.M.M.; Kok, W.E.M.; Aleman, B.M.P.; Van Leeuwen, F.E. Cardiovascular Disease After Hodgkin Lymphoma Treatment: 40-year disease risk. JAMA Intern. Med. 2015, 175, 1007–1017. [Google Scholar] [CrossRef] [PubMed]
- Maraldo, M.V.; Giusti, F.; Vogelius, I.R.; Lundemann, M.; van der Kaaij, M.; Ramadan, S.; Meulemans, B.; Henry-Amar, M.; Aleman, B.M.P.; Raemaekers, J.; et al. Cardiovascular disease after treatment for Hodgkin’s lymphoma: An analysis of nine collaborative EORTC-LYSA trials. Lancet Haematol. 2015, 2, e492–e502. [Google Scholar] [CrossRef] [PubMed]
- Hodgson, D.C.; Pintilie, M.; Yun, L.; Tsang, R.; Yu, E.; Sussman, J.; Meyer, R.M. Clinically significant delayed cardiac morbidity following ABVD chemotherapy for Hodgkin lymphoma: A population-based study. J. Clin. Oncol. 2010, 28, 8059. [Google Scholar] [CrossRef]
- Elbl, L.; Vasova, I.; Kral, Z.; Tomaskova, I.; Smardova, L.; Wagnerova, B.; Jedlicka, F.; Vorlicek, J. Evaluation of Acute and Early Cardiotoxicity in Survivors of Hodgkin’s Disease Treated with ABVD or BEACOPP Regimens. J. Chemother. 2006, 18, 199–208. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.; Yang, M.; Ping, L.; Xie, Y.; Wang, X.; Zhu, J.; Song, Y. Chemotherapy with a Pegylated Liposomal Doxorubicin-Containing Regimen in Newly Diagnosed Hodgkin Lymphoma Patients. Cardiovasc. Toxicol. 2021, 21, 12–16. [Google Scholar] [CrossRef]
- van Leeuwen-Segarceanu, E.M.; Bos, W.-J.W.; Dorresteijn, L.D.; Rensing, B.J.; van der Heyden, J.A.; Vogels, O.J.; Biesma, D.H. Screening Hodgkin lymphoma survivors for radiotherapy induced cardiovascular disease. Cancer Treat. Rev. 2011, 37, 391–403. [Google Scholar] [CrossRef]
- Harel, S.; Ferme, C.; Poirot, C. Management of fertility in patients treated for Hodgkin’s lymphoma. Haematologica 2011, 96, 1692–1699. [Google Scholar] [CrossRef]
- Rueffer, U.; Breuer, K.; Josting, A.; Lathan, B.; Sieber, M.; Manzke, O.; Grotenhermen, F.-J.; Tesch, H.; Bredenfeld, H.; Koch, P.; et al. Male gonadal dysfunction in patients with Hodgkin’s disease prior to treatment. Ann. Oncol. 2001, 12, 1307–1311. [Google Scholar] [CrossRef] [PubMed]
- van der Kaaij, M.A.; Heutte, N.; van Echten-Arends, J.; Raemaekers, J.M.; Carde, P.; Noordijk, E.M.; Ferme, C.; Thomas, J.; Eghbali, H.; Brice, P.; et al. Sperm quality before treatment in patients with early stage Hodgkin’s lymphoma enrolled in EORTC-GELA Lymphoma Group trials. Haematologica 2009, 94, 1691–1697. [Google Scholar] [CrossRef]
- Amin, M.S.A.; Brunckhorst, O.; Scott, C.; Wrench, D.; Gleeson, M.; Kazmi, M.; Ahmed, K. ABVD and BEACOPP regimens’ effects on fertility in young males with Hodgkin lymphoma. Clin. Transl. Oncol. 2021, 23, 1067–1077. [Google Scholar] [CrossRef] [PubMed]
- Lambertini, M.; Del Mastro, L.; Pescio, M.C.; Andersen, C.Y.; Azim, H.A.; Peccatori, F.A.; Costa, M.; Revelli, A.; Salvagno, F.; Gennari, A.; et al. Cancer and fertility preservation: International recommendations from an expert meeting. BMC Med. 2016, 14, 1. [Google Scholar] [CrossRef]
- van der Kaaij, M.; van Echten-Arends, J.; Heutte, N.; Meijnders, P.; Abeilard-Lemoisson, E.; Spina, M.; Moser, E.; Allgeier, A.; Meulemans, B.; Lugtenburg, P.; et al. Cryopreservation, semen use and the likelihood of fatherhood in male Hodgkin lymphoma survivors: An EORTC-GELA Lymphoma Group cohort study. Hum. Reprod. 2014, 29, 525–533. [Google Scholar] [CrossRef]
- Machet, A.; Poudou, C.; Tomowiak, C.; Gastinne, T.; Gardembas, M.M.; Systchenko, T.; Moya, N.; Debiais, C.; Levy, A.; Gruchet, C.; et al. Hodgkin lymphoma and female fertility: A multicenter study in women treated with doxorubicin, bleomycin, vinblastine, and dacarbazine. Blood Adv. 2023, 7, 3978–3983. [Google Scholar] [CrossRef]
- Behringer, K.; Mueller, H.; Goergen, H.; Thielen, I.; Eibl, A.D.; Stumpf, V.; Wessels, C.; Wiehlpütz, M.; Rosenbrock, J.; Halbsguth, T.; et al. Gonadal Function and Fertility in Survivors After Hodgkin Lymphoma Treatment Within the German Hodgkin Study Group HD13 to HD15 Trials. J. Clin. Oncol. 2013, 31, 231–239. [Google Scholar] [CrossRef] [PubMed]
- Demeestere, I.; Racape, J.; Dechene, J.; Dupuis, J.; Morschhauser, F.; De Wilde, V.; Lazarovici, J.; Ghesquieres, H.; Touati, M.; Sibon, D.; et al. Gonadal Function Recovery in Patients with Advanced Hodgkin Lymphoma Treated With a PET-Adapted Regimen: Prospective Analysis of a Randomized Phase III Trial (AHL2011). J. Clin. Oncol. 2021, 39, 3251–3260. [Google Scholar] [CrossRef]
- Viviani, S.; Dellino, M.; Ramadan, S.; Peracchio, C.; Marcheselli, L.; Minoia, C.; Guarini, A. Fertility preservation strategies for patients with lymphoma: A real-world practice survey among Fondazione Italiana Linfomi centers. Tumori J. 2022, 108, 572–577. [Google Scholar] [CrossRef]
- Behringer, K.; Wildt, L.; Mueller, H.; Mattle, V.; Ganitis, P.; van den Hoonaard, B.; Ott, H.W.; Hofer, S.; Pluetschow, A.; Diehl, V.; et al. No protection of the ovarian follicle pool with the use of GnRH-analogues or oral contraceptives in young women treated with escalated BEACOPP for advanced-stage Hodgkin lymphoma. Final results of a phase II trial from the German Hodgkin Study Group. Ann. Oncol. 2010, 21, 2052–2060. [Google Scholar] [CrossRef]
- Velasco, R.; Domingo-Domenech, E.; Sureda, A. Brentuximab-Induced Peripheral Neurotoxicity: A Multidisciplinary Approach to Manage an Emerging Challenge in Hodgkin Lymphoma Therapy. Cancers 2021, 13, 6125. [Google Scholar] [CrossRef] [PubMed]
- Steiner, R.E.; Hwang, S.R.; Khurana, A.; Habermann, T.M.; Epperla, N.; Annunzio, K.; Allen, P.B.; Baird, K.; Paulino, D.; Alderuccio, J.P.; et al. Impact of cumulative dose of brentuximab vedotin on outcomes of frontline therapy for advanced-stage Hodgkin lymphoma. Blood Adv. 2023, 7, 7485–7493. [Google Scholar] [CrossRef]
- Bröckelmann, P.J.; McMullen, S.; Ben Wilson, J.; Mueller, K.; Goring, S.; Stamatoullas, A.; Zagadailov, E.; Gautam, A.; Huebner, D.; Dalal, M.; et al. Patient and physician preferences for first-line treatment of classical Hodgkin lymphoma in Germany, France and the United Kingdom. Br. J. Haematol. 2019, 184, 202–214. [Google Scholar] [CrossRef] [PubMed]
- Rüffer, J.; Flechtner, H.; Tralls, P.; Josting, A.; Sieber, M.; Lathan, B.; Diehl, V. Fatigue in long-term survivors of Hodgkin’s lymphoma; a report from the German Hodgkin Lymphoma Study Group (GHSG). Eur. J. Cancer 2003, 39, 2179–2186. [Google Scholar] [CrossRef]
- Trachtenberg, E.; Gurion, R.; Mashiach, T.; Tadmor, T.; Kedmi, M.; Dann, E.J. Recognizing severe fatigue and decline in quality of life in Hodgkin lymphoma survivors. Leuk. Lymphoma 2019, 60, 3449–3454. [Google Scholar] [CrossRef] [PubMed]
- Eikeland, S.A.; Smeland, K.B.; Simensen, V.C.; Fagerli, U.-M.; Bersvendsen, H.S.; Kiserud, C.E.; Fosså, A. Chronic fatigue in long-term survivors of Hodgkin’s lymphoma after contemporary risk-adapted treatment. Acta Oncol. 2023, 62, 80–88. [Google Scholar] [CrossRef]
- Daniëls, L.A.; Oerlemans, S.; Krol, A.D.G.; van de Poll-Franse, L.V.; Creutzberg, C.L. Persisting fatigue in Hodgkin lymphoma survivors: A systematic review. Ann. Hematol. 2013, 92, 1023–1032. [Google Scholar] [CrossRef]
- Loge, J.H.; Abrahamsen, A.F.; Ekeberg, O.; Kaasa, S. Fatigue and Psychiatric Morbidity Among Hodgkin’s Disease Survivors. J. Pain Symptom Manag. 2000, 19, 91–99. [Google Scholar] [CrossRef]
- Agostinelli, G.; Muzzatti, B.; Serpentini, S.; Spina, M.; Annunziata, M.A. Cancer-Related Psychological Distress in Lymphoma Survivor: An Italian Cross-Sectional Study. Front. Psychol. 2022, 13, 872329. [Google Scholar] [CrossRef]
- Carroll, B.T.; Kathol, R.G.; Noyes, R., Jr.; Wald, T.G.; Clamon, G.H. Screening for depression and anxiety in cancer patients using the Hospital Anxiety and Depression Scale. Gen. Hosp. Psychiatry 1993, 15, 69–74. [Google Scholar] [CrossRef]
- Macklin-Doherty, A.; Jones, M.; Coulson, P.; Bruce, C.; Chau, I.; Alexander, E.; Iyengar, S.; Taj, M.; Cunningham, D.; Swerdlow, A. Risk of thyroid disorders in adult and childhood Hodgkin lymphoma survivors 40 years after treatment. Leuk. Lymphoma 2022, 63, 562–572. [Google Scholar] [CrossRef]
- Eichenauer, D.A.; Plütschow, A.; Kreissl, S.; Sökler, M.; Hellmuth, J.C.; Meissner, J.; Mathas, S.; Topp, M.S.; Behringer, K.; Klapper, W.; et al. Incorporation of brentuximab vedotin into first-line treatment of advanced classical Hodgkin’s lymphoma: Final analysis of a phase 2 randomised trial by the German Hodgkin Study Group. Lancet Oncol. 2017, 18, 1680–1687. [Google Scholar] [CrossRef]
- Borchmann, P.; Moccia, A.A.; Greil, R.; Schneider, G.; Hertzberg, M.; Schaub, V.; Hüttmann, A.; Keil, F.; Dierlamm, J.; Hänel, M.; et al. Brecadd is non-inferior to Ebeacopp in patients with advanced stage classical Hodgkin lymphoma: Efficacy results of the GHSG phase III HD21 Trial. Hematol. Oncol. 2023, 41, 881–882. [Google Scholar] [CrossRef]
- Borchmann, P.; Moccia, A.; Greil, R.; Schneider, G.; Hertzberg, M.S.; Schaub, V.; Huettmann, A.; Keil, F.; Hänel, M.; Novak, U.; et al. Comprehensive Analysis of Treatment Related Morbidity and Progression—Free Survival in the GHSG Phase III HD21 Trial. Blood 2023, 142, 3057. [Google Scholar] [CrossRef]
- Ferdinandus, J.; Schneider, G.; Fosså, A.; Moccia, A.; Greil, R.; Hertzberg, M.S.; Zijlstra, J.M.; Kamper, P.; Molin, D.L.; Kerkhoff, A.; et al. Pregnancies and Childbirth Following Advanced-Stage Hodgkin Lym-phoma Treatment with Brecadd or Beacopp in the Randomized Phase III GHSG HD21 Trial. Blood 2023, 142, 4437. [Google Scholar] [CrossRef]
- De Goycoechea, D.; Stalder, G.; Martins, F.; Duchosal, M.A. Immune Checkpoint Inhibition in Classical Hodgkin Lymphoma: From Early Achievements towards New Perspectives. J. Oncol. 2019, 2019, 9513701. [Google Scholar] [CrossRef] [PubMed]
- Ramchandren, R.; Domingo-Domènech, E.; Rueda, A.; Trněný, M.; Feldman, T.A.; Lee, H.J.; Provencio, M.; Sillaber, C.; Cohen, J.B.; Savage, K.J.; et al. Nivolumab for Newly Diagnosed Advanced-Stage Classic Hodgkin Lymphoma: Safety and Efficacy in the Phase II CheckMate 205 Study. J. Clin. Oncol. 2019, 37, 1997–2007. [Google Scholar] [CrossRef]
- Herrera, A.F.; LeBlanc, M.; Castellino, S.M.; Li, H.; Rutherford, S.C.; Evens, A.M.; Davison, K.; Punnett, A.; Hodgson, D.; Parsons, S.K.; et al. Nivolumab(N)-AVD improves progression-free survival compared to Brentuximab vedotin(BV)-avd in advanced stage (AS) classic Hodgkin Lymphoma (HL): Results of Swog S1826. Hematol. Oncol. 2023, 41, 33–35. [Google Scholar] [CrossRef]
- Castellino, S.M.; Pei, Q.; Parsons, S.K.; Hodgson, D.; McCarten, K.; Horton, T.; Cho, S.; Wu, Y.; Punnett, A.; Dave, H.; et al. Brentuximab Vedotin with Chemotherapy in Pediatric High-Risk Hodgkin’s Lymphoma. N. Engl. J. Med. 2022, 387, 1649–1660. [Google Scholar] [CrossRef] [PubMed]
- Witkowska, M.; Majchrzak, A.; Smolewski, P. The Role of Radiotherapy in Hodgkin’s Lymphoma: What Has Been Achieved during the Last 50 Years? BioMed. Res. Int. 2015, 2015, 485071. [Google Scholar] [CrossRef] [PubMed]
- Fuchs, M.; Jacob, A.S.; Kaul, H.; Kobe, C.; Kuhnert, G.; Pabst, T.; Greil, R.; Bröckelmann, P.J.; Topp, M.S.; Just, M.; et al. Follow-up of the GHSG HD16 trial of PET-guided treatment in early-stage favorable Hodgkin lymphoma. Leukemia 2023, 38, 160–167. [Google Scholar] [CrossRef] [PubMed]
- Koshy, M.; Rich, S.E.; Mahmood, U.; Kwok, Y. Declining Use of Radiotherapy in Stage I and II Hodgkin’s Disease and Its Effect on Survival and Secondary Malignancies. Int. J. Radiat. Oncol. Biol. Phys. 2012, 82, 619–625. [Google Scholar] [CrossRef] [PubMed]
- Borchmann, P.; Plütschow, A.; Kobe, C.; Greil, R.; Meissner, J.; Topp, M.S.; Ostermann, H.; Dierlamm, J.; Mohm, J.; Thiemer, J.; et al. PET-guided omission of radiotherapy in early-stage unfavourable Hodgkin lymphoma (GHSG HD17): A multicentre, open-label, randomised, phase 3 trial. Lancet Oncol. 2021, 22, 223–234. [Google Scholar] [CrossRef]
- Engert, A.; Haverkamp, H.; Kobe, C.; Markova, J.; Renner, C.; Ho, A.; Zijlstra, J.; Král, Z.; Fuchs, M.; Hallek, M.; et al. Reduced-intensity chemotherapy and PET-guided radiotherapy in patients with advanced stage Hodgkin’s lymphoma (HD15 trial): A randomised, open-label, phase 3 non-inferiority trial. Lancet 2012, 379, 1791–1799. [Google Scholar] [CrossRef]
- Gallamini, A.; Kurlapski, M.; Zaucha, J.M. FDG-PET/CT for the Management of Post-Chemotherapy Residual Mass in Hodgkin lymphoma. Cancers 2021, 13, 3952. [Google Scholar] [CrossRef]
- Vassilakopoulos, T.P.; Liaskas, A.; Pereyra, P.; Panayiotidis, P.; Angelopoulou, M.K.; Gallamini, A. Incorporating Monoclonal Antibodies into the First-Line Treatment of Classical Hodgkin Lymphoma. Int. J. Mol. Sci. 2023, 24, 13187. [Google Scholar] [CrossRef]
- Fornecker, L.-M.; Lazarovici, J.; Aurer, I.; Casasnovas, R.-O.; Gac, A.-C.; Bonnet, C.; Bouabdallah, K.; Feugier, P.; Specht, L.; Molina, L.; et al. Brentuximab Vedotin Plus AVD for First-Line Treatment of Early-Stage Unfavorable Hodgkin Lymphoma (BREACH): A Multicenter, Open-Label, Randomized, Phase II Trial. J. Clin. Oncol. 2023, 41, 327–335. [Google Scholar] [CrossRef]
- Bröckelmann, P.J.; Bühnen, I.; Meissner, J.; Trautmann-Grill, K.; Herhaus, P.; Halbsguth, T.V.; Schaub, V.; Kerkhoff, A.; Mathas, S.; Bormann, M.; et al. Nivolumab and Doxorubicin, Vinblastine, and Dacarbazine in Early-Stage Unfavorable Hodgkin Lymphoma: Final Analysis of the Randomized German Hodgkin Study Group Phase II NIVAHL Trial. J. Clin. Oncol. 2023, 41, 1193–1199. [Google Scholar] [CrossRef]

{kind=link}
| Trial | Regimen | n | PFS (%) | OS (%) |
|---|---|---|---|---|
| GHSG HD 18 trial [6] | BEACOPPescx2 if iPET+ randomization to BEACOPPesc x4–6 | 217 | 89.7%(5y) | 96.4% (5y) |
| BECOPPescx2 if PET positive BEACOPPesc+R4–6 | 217 | 88.1% (5y) | 93.9% (5y) | |
| BEACOPPescx2 if PET-BEACOPPesc2 | 501 | 92.2% (5y) | 97.7% (5y) | |
| BEACOPPescx2 if PET-BEACOPP escx4–6 | 504 | 90.8% (5y) | 95.4% (5y) | |
| LYSA AHL 2011 [11] | BEACOPPesc2 if iPET-ABVDx4 | 319 | 85.7% (5y) | 96.4% (5y) |
| BEACOPPesc2 if iPET-BEACOPPesc4 | 49 | NA | NA | |
| BEACOPPesc6 regardless of iPET | 401 | 86.2% (5y) | 95.2% (5y) | |
| RATHL [9] | ABVDx2 if iPET-AVDx4 | 470 | 84.4 (3y) | 97.2% (3y) |
| ABVD if -PET-ABVDx4 | 465 | 85.7 (3y) | 97.6% (3y) | |
| ABVDx2 if iPET+ BEACOPPesc21/14 (number of cycles varied) | 172 | 67.6%(3y) | 87.8%(3y) | |
| Southwest Oncology Group S0816 [14] | ABVDx2 if iPET negative ABVDx4 | 271 | 82% (2y) | NA |
| ABVDx2 if iPET+ BEACOPPescx6 | 60 | 64% (2y) | NA |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Milunović, V. How I Follow Hodgkin Lymphoma in First Complete (Metabolic) Remission? Medicina 2024, 60, 344. https://doi.org/10.3390/medicina60020344
Milunović V. How I Follow Hodgkin Lymphoma in First Complete (Metabolic) Remission? Medicina. 2024; 60(2):344. https://doi.org/10.3390/medicina60020344
Chicago/Turabian StyleMilunović, Vibor. 2024. "How I Follow Hodgkin Lymphoma in First Complete (Metabolic) Remission?" Medicina 60, no. 2: 344. https://doi.org/10.3390/medicina60020344
APA StyleMilunović, V. (2024). How I Follow Hodgkin Lymphoma in First Complete (Metabolic) Remission? Medicina, 60(2), 344. https://doi.org/10.3390/medicina60020344