

Paradoxical Psoriasis Induced by Ustekinumab: A Comprehensive Review and Case Report


 ,
,  ,
,
Abstract
1. Introduction
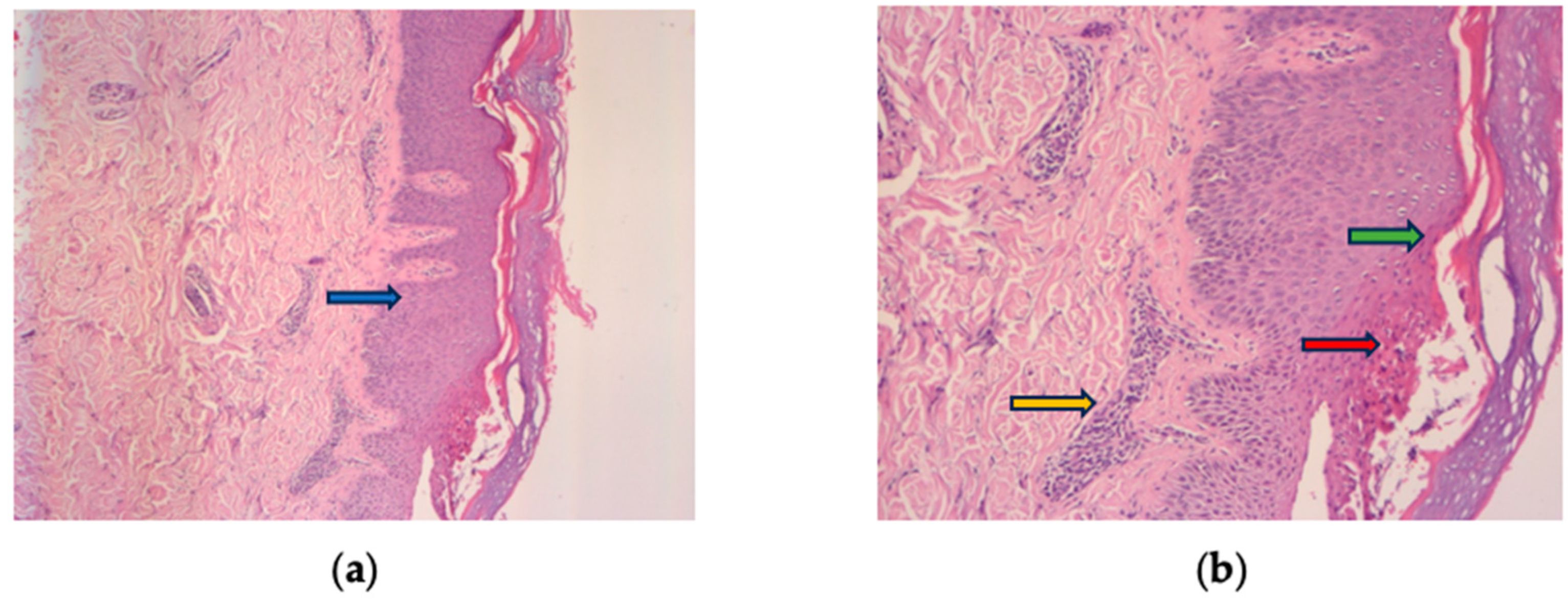
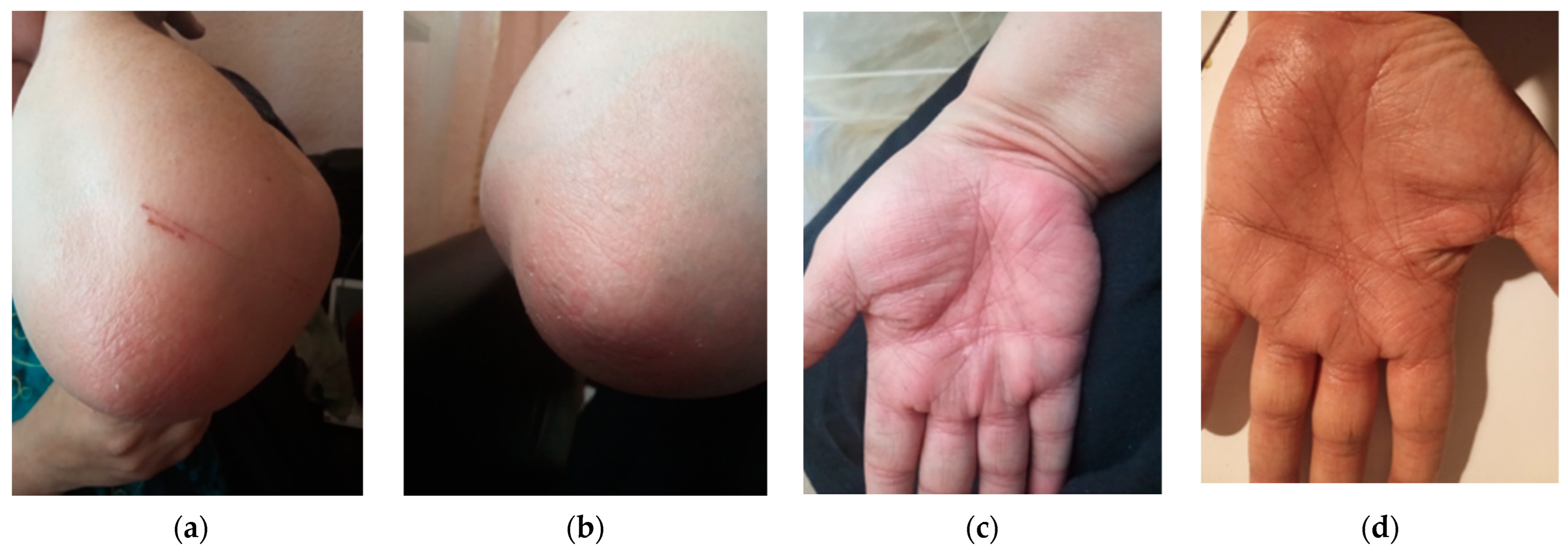
2. Case Report
3. Literature Review
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bettenworth, D. Assessment of stricturing Crohn’s disease: Current clinical practice and future avenues. World J. Gastroenterol. 2016, 22, 1008. [Google Scholar] [CrossRef] [PubMed]
- Reinisch, W.; Sandborn, W.J.; Rutgeerts, P.; Feagan, B.G.; Rachmilewitz, D.; Hanauer, S.B.; Lichtenstein, G.R.; De Villiers, W.J.S.; Blank, M.; Lang, Y.; et al. Long-term Infliximab Maintenance Therapy for Ulcerative Colitis: The ACT-1 and -2 Extension Studies. Inflamm. Bowel Dis. 2012, 18, 201–211. [Google Scholar] [CrossRef] [PubMed]
- Schnitzler, F.; Fidder, H.; Ferrante, M.; Noman, M.; Arijs, I.; Van Assche, G.; Hoffman, I.; Van Steen, K.; Vermeire, S.; Rutgeerts, P. Mucosal healing predicts long-term outcome of maintenance therapy with infliximab in Crohn’s disease. Inflamm. Bowel Dis. 2009, 15, 1295–1301. [Google Scholar] [CrossRef] [PubMed]
- European Medicines Agency. EMA Stelara. 2018. Available online: https://www.ema.europa.eu/en/medicines/human/EPAR/stelara (accessed on 14 October 2023).
- Sandborn, W.J.; Feagan, B.G.; Danese, S.; O’Brien, C.D.; Ott, E.; Marano, C.; Baker, T.; Zhou, Y.; Volger, S.; Tikhonov, I.; et al. Safety of Ustekinumab in Inflammatory Bowel Disease: Pooled Safety Analysis of Results from Phase 2/3 Studies. Inflamm. Bowel Dis. 2021, 27, 994–1007. [Google Scholar] [CrossRef] [PubMed]
- Papp, K.; Gottlieb, A.B.; Naldi, L.; Pariser, D.; Ho, V.; Goyal, K.; Fakharzadeh, S.; Chevrier, M.; Calabro, S.; Langholff, W.; et al. Safety Surveillance for Ustekinumab and Other Psoriasis Treatments From the Psoriasis Longitudinal Assessment and Registry (PSOLAR). J. Drugs Dermatol. JDD 2015, 14, 706–714. [Google Scholar] [PubMed]
- Schön, M.P.; Boehncke, W.-H. Psoriasis. N. Engl. J. Med. 2005, 352, 1899–1912. [Google Scholar] [CrossRef]
- Nestle, F.O.; Kaplan, D.H.; Barker, J. Psoriasis. N. Engl. J. Med. 2009, 361, 496–509. [Google Scholar] [CrossRef]
- Leonardi, C.L.; Kimball, A.B.; Papp, K.A.; Yeilding, N.; Guzzo, C.; Wang, Y.; Li, S.; Dooley, L.T.; Gordon, K.B. Efficacy and safety of ustekinumab, a human interleukin-12/23 monoclonal antibody, in patients with psoriasis: 76-week results from a randomised, double-blind, placebo-controlled trial (PHOENIX 1). Lancet 2008, 371, 1665–1674. [Google Scholar] [CrossRef]
- Lu, J.; Lu, Y. Paradoxical psoriasis: The flip side of idiopathic psoriasis or an autocephalous reversible drug reaction? J. Transl. Autoimmun. 2023, 7, 100211. [Google Scholar] [CrossRef]
- Conrad, C.; Di Domizio, J.; Mylonas, A.; Belkhodja, C.; Demaria, O.; Navarini, A.A.; Lapointe, A.-K.; French, L.E.; Vernez, M.; Gilliet, M. TNF blockade induces a dysregulated type I interferon response without autoimmunity in paradoxical psoriasis. Nat. Commun. 2018, 9, 25. [Google Scholar] [CrossRef]
- Fania, L.; Morelli, M.; Scarponi, C.; Mercurio, L.; Scopelliti, F.; Cattani, C.; Scaglione, G.L.; Tonanzi, T.; Pilla, M.A.; Pagnanelli, G.; et al. Paradoxical psoriasis induced by TNF-α blockade shows immunological features typical of the early phase of psoriasis development. J. Pathol. Clin. Res. 2020, 6, 55–68. [Google Scholar] [CrossRef] [PubMed]
- Seneschal, J.; Milpied, B.; Vergier, B.; Lepreux, S.; Schaeverbeke, T.; Taïeb, A. Cytokine imbalance with increased production of interferon-α in psoriasiform eruptions associated with antitumour necrosis factor-α treatments. Br. J. Dermatol. 2009, 161, 1081–1088. [Google Scholar] [CrossRef] [PubMed]
- Ya, J.; Hu, J.Z.; Nowacki, A.S.; Khanna, U.; Mazloom, S.; Kabbur, G.; Husni, M.E.; Fernandez, A.P. Family history of psoriasis, psychological stressors, and tobacco use are associated with the development of tumor necrosis factor-α inhibitor-induced psoriasis: A case-control study. J. Am. Acad. Dermatol. 2020, 83, 1599–1605. [Google Scholar] [CrossRef] [PubMed]
- Zheng, J.; Gao, Y.; Ding, Y. Successful management of infliximab-induced generalized pustular psoriasis without therapy discontinuation in a patient with psoriatic arthritis. Dermatol. Ther. 2019, 32, e13132. [Google Scholar] [CrossRef] [PubMed]
- Murphy, M.J.; Cohen, J.M.; Vesely, M.D.; Damsky, W. Paradoxical eruptions to targeted therapies in dermatology: A systematic review and analysis. J. Am. Acad. Dermatol. 2022, 86, 1080–1091. [Google Scholar] [CrossRef] [PubMed]
- Lupu, A.; Tieranu, C. TNFα inhibitor induced lupus-like syndrome (TAILS) in a patient with IBD. Curr. Health Sci. J. 2014, 40, 285–288. [Google Scholar] [PubMed]
- Barahimi, M.; Lee, S.; Clark-Snustad, K. Pustular Rash in Crohn’s Patient on Ustekinumab Raises Concern for Drug-Induced Paradoxical Psoriasis. Case Rep. Gastroenterol. 2021, 15, 662–666. [Google Scholar] [CrossRef]
- Benzaquen, M.; Flachaire, B.; Rouby, F.; Berbis, P.; Guis, S. Paradoxical pustular psoriasis induced by ustekinumab in a patient with Crohn’s disease-associated spondyloarthropathy. Rheumatol. Int. 2018, 38, 1297–1299. [Google Scholar] [CrossRef]
- Suh, H.Y.; Ahn, J.Y.; Park, M.Y.; Youn, J.I. Exacerbation of infliximab-induced paradoxical psoriasis after ustekinumab therapy. J. Dermatol. 2018, 45, 332–333. [Google Scholar] [CrossRef]
- Darwin, E.; Deshpande, A.; Lev-Tov, H. Development of Drug-Induced Inverse Psoriasis in a Patient with Crohn’s Disease. ACG Case Rep. J. 2018, 5, e47. [Google Scholar] [CrossRef]
- Lee, H.Y.; Woo, C.H.; Haw, S. Paradoxical Flare of Psoriasis after Ustekinumab Therapy. Ann. Dermatol. 2017, 29, 794. [Google Scholar] [CrossRef] [PubMed]
- Hay, R.A.S.; Pan, J.Y. Paradoxical flare of pustular psoriasis triggered by ustekinumab, which responded to adalimumab therapy. Clin. Exp. Dermatol. 2014, 39, 751–752. [Google Scholar] [CrossRef] [PubMed]
- Caca-Biljanovska, N.; V’lckova-Laskoska, M.; Laskoski, D. Successful management of ustekinumab-induced pustular psoriasis without therapy discontinuation. Acta Dermatovenerol. Croat. ADC 2013, 21, 202–204. [Google Scholar] [PubMed]
- Wenk, K.S.; Claros, J.M.; Ehrlich, A. Flare of pustular psoriasis after initiating ustekinumab therapy. J. Dermatol. Treat. 2012, 23, 212–214. [Google Scholar] [CrossRef] [PubMed]
- Gregoriou, S.; Kazakos, C.; Christofidou, E.; Kontochristopoulos, G.; Vakis, G.; Rigopoulos, D. Pustular psoriasis development after initial ustekinumab administration in chronic plaque psoriasis. Eur. J. Dermatol. 2011, 21, 104–105. [Google Scholar] [CrossRef] [PubMed]
- Safa, G.; Martin, A.; Darrieux, L. Exacerbation of Infliximab-Induced Palmoplantar Psoriasis Under Ustekinumab Therapy in a Patient With Ankylosing Spondylitis. JCR J. Clin. Rheumatol. 2011, 17, 385–386. [Google Scholar] [CrossRef] [PubMed]
- Papp, K.A.; Langley, R.G.; Lebwohl, M.; Krueger, G.G.; Szapary, P.; Yeilding, N.; Guzzo, C.; Hsu, M.-C.; Wang, Y.; Li, S.; et al. Efficacy and safety of ustekinumab, a human interleukin-12/23 monoclonal antibody, in patients with psoriasis: 52-week results from a randomised, double-blind, placebo-controlled trial (PHOENIX 2). Lancet 2008, 371, 1675–1684. [Google Scholar] [CrossRef]
- Nast, A.; Jacobs, A.; Rosumeck, S.; Werner, R.N. Efficacy and Safety of Systemic Long-Term Treatments for Moderate-to-Severe Psoriasis: A Systematic Review and Meta-Analysis. J. Investig. Dermatol. 2015, 135, 2641–2648. [Google Scholar] [CrossRef]
- Galluzzo, M.; Boca, A.N.; Botti, E.; Potenza, C.; Malara, G.; Malagoli, P.; Vesa, S.; Chimenti, S.; Buzoianu, A.D.; Talamonti, M.; et al. IL12B (p40) Gene Polymorphisms Contribute to Ustekinumab Response Prediction in Psoriasis. Dermatology 2016, 232, 230–236. [Google Scholar] [CrossRef]
- Cabaleiro, T.; Prieto-Pérez, R.; Navarro, R.; Solano, G.; Román, M.; Ochoa, D.; Abad-Santos, F.; Daudén, E. Paradoxical psoriasiform reactions to anti-TNFα drugs are associated with genetic polymorphisms in patients with psoriasis. Pharmacogenom. J. 2016, 16, 336–340. [Google Scholar] [CrossRef]
- Loft, N.D.; Skov, L.; Iversen, L.; Gniadecki, R.; Dam, T.N.; Brandslund, I.; Hoffmann, H.J.; Andersen, M.R.; Dessau, R.B.; Bergmann, A.C.; et al. Associations between functional polymorphisms and response to biological treatment in Danish patients with psoriasis. Pharmacogenom. J. 2018, 18, 494–500. [Google Scholar] [CrossRef] [PubMed]
- Hetherington, S.; McGuirk, S.; Powell, G.; Cutrell, A.; Naderer, O.; Spreen, B.; Lafon, S.; Pearce, G.; Steel, H. Hypersensitivity reactions during therapy with the nucleoside reverse transcriptase inhibitor abacavir. Clin. Ther. 2001, 23, 1603–1614. [Google Scholar] [CrossRef] [PubMed]
- Yiu, Z.Z.N.; Becher, G.; Kirby, B.; Laws, P.; Reynolds, N.J.; Smith, C.H.; Warren, R.B.; Griffiths, C.E.M.; BADBIR Study Group; Browne, F.; et al. Drug Survival Associated With Effectiveness and Safety of Treatment With Guselkumab, Ixekizumab, Secukinumab, Ustekinumab, and Adalimumab in Patients With Psoriasis. JAMA Dermatol. 2022, 158, 1131. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Author and Year [Reference] | Patient ID | Age | Sex | Previous Psoriasis History | Ustekinumab Treatment Duration | Dose of UST | How Long after UST Did Lesions Appear | Type of Paradoxical Psoriasis | Location of Paradoxical Psoriasis | Severity (PASI Score) | How Was Paradoxical Psoriasis Flare Controlled | Comorbidities | Therapy Prior to UST | Time to Resolution | Management Strategy (Discontinuation, Switching to Other Agent, Etc.) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Our case | 1 | 39 | Female | Three years (from 2020 to 2023) | Three years | Psoriasiform (biopsy-proven) | Hands, elbows, and scalp | Topical steroids | Crohn’s Disease (CD) | Infliximab, adalimumab | Continued UST with topical treatment | ||||
| Barahimi et al., 2021 [18] | 2 | 51 | Male | No history of psoriasis | Three years | 90 mg | Three flares separated lasting several weeks; one flare per year | Subcorneal pustular dermatosis | Hands, body, face, extremities, and scalp | 10–15 (moderate) | Topical corticosteroids; second flare managed with discontinuation | Crohn’s disease and enteropathic arthritis | Adalimumab, infliximab, and methotrexate | Three weeks | Discontinuation of UST during flares and restarting therapy once flares resolved |
| Benzaquen et al., 2018 [19] | 3 | 58 | Female | No history of psoriasis | Three weeks | 390 mg | Three weeks | Paradoxical Palmoplantar Pustular Psoriasis | Right hand palm | 0–5 (mild) | Discontinuation, golimumab | Asthma, corticosteroid-induced osteoporosis, arthritis, Crohn’s disease, spondyloarthropathy | Systemic corticosteroids, mesalazine, azathioprine, adalimumab, and infliximab | 15 days | Discontinuation of UST, switched to golimumab |
| Suh et al., 2018 [20] | 4 | 30 | Male | 6-year history of psoriasis | Two weeks | 45 mg | One week after the first injection | Possibly pustular psoriasis, but not definitively diagnosed | Trunk, lower extremities, scalp, palms, and soles | Not available | Discontinuation, oral cyclosporin and a topical agent | Not available | Previously treated with infliximab phototherapy, acitretin, and cyclosporine. | One week | Discontinuation of UST and initiation of treatment with oral cyclosporin and a topical agent |
| Darwin et al., 2018 [21] | 5 | 56 | Female | Palmoplantar psoriasis | 15 months | 90 mg monthly | 15 months | Inverse psoriasis | Inter-gluteal cleft and genital area | 0–5 (mild) | Tacrolimus cream daily and pulsed clobetasol cream as necessary on weekends | Crohn’s disease, rheumatoid arthritis | Infliximab, adalimumab, thalidomide, and hydroxychloroquine | Not provided | Medications were not halted as her Crohn’s disease was well controlled under the current medication regimen |
| Lee et al., 2017 [22] | 6 | 24 | Male | 7-year history of psoriasis vulgaris | 12 weeks | 45 mg | After the third injection | Plaque psoriasis | Face, trunk, and extremities | 10–15 (moderate) | Systemic steroid and NBUVB phototherapy | None | NBUVB phototherapy, acitretin, methotrexate, and cyclosporine | Two weeks | Addition of systemic steroid and NBUVB phototherapy, but patient discontinued treatments after 2 weeks and was lost to follow-up |
| Hay et al., 2014 [23] | 7 | 47 | Male | 15-year history of plaque psoriasis | One month | 45 mg | Before the second dose, one month later | Pustular psoriasis | 60% of body surface area | >15 (severe) | Discontinuation and adalimumab | Psoriatic arthropathy | Methoxetrate, acitretin, ciclosporin, and narrowband ultraviolet B phototherapy | Two weeks | Discontinuation of UST, switching to adalimumab |
| Caca-Biljanovska et al., 2013 [24] | 8 | 34 | Female | Severe plaque psoriasis since the age of 10 | >18 months | 45 mg | Week 10, after two injections | Pustular psoriasis | Trunk and limbs | >15 (severe) | Topical corticosteroids and intensification of UST | NA | Topical corticosteroids, psoralen plus ultraviolet A irradiation (PUVA), and acitretin | Four weeks | Continued UST therapy |
| Wenk et al., 2012 [25] | 9 | 37 | Female | 10-year history of plaque psoriasis | 12 weeks, injection at day 0, week 4, and week 12 | 45-mg | Four days after first injection and subsequently after second and third injection | Pustular psoriasis | Trunk and limbs | >15 (severe) | Discontinuation and systemic and topical steroids | Psoriatic arthritis | Infliximab, adalimumab, cyclosporine, acitretin, narrow band ultraviolet B irradiation, etanercept, methotrexate, systemic steroid treatment, topical steroids, and acitretin | Not specified | Discontinuation of UST and switch to acitretin |
| Gregoriou et al., 2011 [26] | 10 | 54 | Female | 5-year history of plaque psoriasis | NA | 45 mg | Two days after first injection | Pustular psoriasis | Trunk and both upper and lower extremities | >15 (severe) | Discontinuation of UST and replacement with methotrexate 25 mg per week with folic acid supplementation | Diabetes type II, hypertension, and hypercholesterolemia | Metformin 500 mg BID for diabetes type II, ramipril 2.5 mg QD for hypertension, and simvastatin 20 mg QD for hypercholesterolemia, topical corticosteroids, calcipotriol, and a calcipotriol-betamethasone dipropionate two compound formulation for 3 years | Two months | Discontinuation of UST and replacement with methotrexate 25 mg per week with folic acid supplementation |
| Safa et al., 2011 [27] | 11 | 35 | Female | No personal history but had a family history | Started at weeks 0 and 4 | 45 mg | After six weeks and two injections | Exacerbation of Infliximab-induced palmoplantar psoriasis | Palms and soles | Not specified | Improved with oral methotrexate after discontinuation of ustekinumab | Ankylosing spondylitis | Nonsteroidal anti-inflammatory drugs, adalimumab, etanercept, and infliximab | Two months | Discontinuation of ustekinumab |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Olteanu, A.O.; Klimko, A.; Tieranu, I.; Orzan, O.A.; Toma, C.V.; Ionescu, E.M.; Preda, C.M.; Tieranu, C.G. Paradoxical Psoriasis Induced by Ustekinumab: A Comprehensive Review and Case Report. Medicina 2024, 60, 106. https://doi.org/10.3390/medicina60010106
Olteanu AO, Klimko A, Tieranu I, Orzan OA, Toma CV, Ionescu EM, Preda CM, Tieranu CG. Paradoxical Psoriasis Induced by Ustekinumab: A Comprehensive Review and Case Report. Medicina. 2024; 60(1):106. https://doi.org/10.3390/medicina60010106
Chicago/Turabian StyleOlteanu, Andrei Ovidiu, Artsiom Klimko, Ioana Tieranu, Olguta Anca Orzan, Cristian Valentin Toma, Elena Mirela Ionescu, Carmen Monica Preda, and Cristian George Tieranu. 2024. "Paradoxical Psoriasis Induced by Ustekinumab: A Comprehensive Review and Case Report" Medicina 60, no. 1: 106. https://doi.org/10.3390/medicina60010106
APA StyleOlteanu, A. O., Klimko, A., Tieranu, I., Orzan, O. A., Toma, C. V., Ionescu, E. M., Preda, C. M., & Tieranu, C. G. (2024). Paradoxical Psoriasis Induced by Ustekinumab: A Comprehensive Review and Case Report. Medicina, 60(1), 106. https://doi.org/10.3390/medicina60010106