
Comparison of Femoral Component Rotation between Robotic-Assisted vs. Soft-Tissue Tensor Total Knee Arthroplasty with Anatomic Implants

 , , , , , and
, , , , , and
Abstract
1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| OA | osteoarthritis |
| DMOADs | disease-modifying osteoarthritis drugs |
| SYSADOAs | symptomatic slow acting drugs for OA |
| TKA | total knee arthroplasty |
| RATKA | robotic-assisted total knee arthroplasty |
| THA | total hip arthroplasty |
| ROM | range of motion |
| CT | computed tomography |
| EKA—ESSKA | European Knee Associates—European Society of Sports Traumatology, Knee Surgery and Arthroscopy |
| MR | measured resection |
| TEA | transepicondylar axis |
| PCA | posterior condylar axis |
| APA | anterior–posterior axis |
| GB | gap balancing |
| STROBE | Strengthening the Reporting of Observational Studies in Epidemiology |
| PS | posterior stabilized |
| HTO | high tibial osteotomy |
| PCL | posterior cruciate ligament |
| BMI | body mass index |
| PJI | periprosthetic joint infection |
References
- Grässel, S.; Muschter, D. Recent advances in the treatment of osteoarthritis. F1000Research 2020, 9, 325. [Google Scholar] [CrossRef] [PubMed]
- Lützner, J.; Kasten, P.; Günther, K.-P.; Kirschner, S. Surgical options for patients with osteoarthritis of the knee. Nat. Rev. Rheumatol. 2009, 5, 309–316. [Google Scholar] [CrossRef]
- Rönn, K.; Reischl, N.; Gautier, E.; Jacobi, M. Current Surgical Treatment of Knee Osteoarthritis. Arthritis 2011, 2011, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Bourne, R.B.; McCalden, R.W.; MacDonald, S.J.; Mokete, L.; Guerin, J. Influence of Patient Factors on TKA Outcomes at 5 to 11 Years Followup. Clin. Orthop. Relat. Res. 2007, 464, 27–31. [Google Scholar] [CrossRef] [PubMed]
- Bourne, R.B.; Chesworth, B.M.; Davis, A.M.; Mahomed, N.N.; Charron, K.D.J. Patient Satisfaction after Total Knee Arthroplasty: Who is Satisfied and Who is Not? Clin. Orthop. Relat. Res. 2010, 468, 57–63. [Google Scholar] [CrossRef]
- Gunaratne, R.; Pratt, D.N.; Banda, J.; Fick, D.P.; Khan, R.J.; Robertson, B.W. Patient Dissatisfaction Following Total Knee Arthroplasty: A Systematic Review of the Literature. J. Arthroplast. 2017, 32, 3854–3860. [Google Scholar] [CrossRef]
- Schwartz, F.H.; Lange, J. Factors That Affect Outcome Following Total Joint Arthroplasty: A Review of the Recent Literature. Curr. Rev. Musculoskelet. Med. 2017, 10, 346–355. [Google Scholar] [CrossRef]
- Anakwe, R.E.; Jenkins, P.J.; Moran, M. Predicting Dissatisfaction After Total Hip Arthroplasty: A Study of 850 Patients. J. Arthroplast. 2011, 26, 209–213. [Google Scholar] [CrossRef]
- Jacobs, C.A.; Christensen, C.P.; Karthikeyan, T. Patient and Intraoperative Factors Influencing Satisfaction Two to Five Years After Primary Total Knee Arthroplasty. J. Arthroplast. 2014, 29, 1576–1579. [Google Scholar] [CrossRef]
- Drexler, M.; Dwyer, T.; Chakravertty, R.; Farno, A.; Backstein, D. Assuring the happy total knee replacement patient. Bone Jt. J. 2013, 95-B, 120–123. [Google Scholar] [CrossRef]
- Newman, C.R.; Walter, W.L.; Talbot, S. Femoral rotational asymmetry is a common anatomical variant. Clin. Anat. 2018, 31, 551–559. [Google Scholar] [CrossRef] [PubMed]
- Slevin, O.; Schmid, F.A.; Schiapparelli, F.-F.; Rasch, H.; Amsler, F.; Hirschmann, M.T. Coronal femoral TKA position significantly influences in vivo patellar loading in unresurfaced patellae after primary total knee arthroplasty. Knee Surg. Sport. Traumatol. Arthrosc. 2017, 25, 3605–3610. [Google Scholar] [CrossRef]
- Valkering, K.P.; Breugem, S.J.; Bekerom, M.P.V.D.; Tuinebreijer, W.; van Geenen, R.C. Effect of rotational alignment on outcome of total knee arthroplasty. Acta Orthop. 2015, 86, 432–439. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.; Wang, L.; Liu, Y.; He, J.; Lian, Q.; Li, D.; Jin, Z. Effect of component mal-rotation on knee loading in total knee arthroplasty using multi-body dynamics modeling under a simulated walking gait. J. Orthop. Res. 2015, 33, 1287–1296. [Google Scholar] [CrossRef] [PubMed]
- Skowronek, P.; Arnold, M.; Starke, C.; Bartyzel, A.; Moser, L.B.; Hirschmann, M.T. Intra- and postoperative assessment of femoral component rotation in total knee arthroplasty: An EKA knee expert group clinical review. Knee Surg. Sports Traumatol. Arthrosc. 2020, 29, 772–782. [Google Scholar] [CrossRef]
- Kim, Y.-H.; Park, J.-W.; Kim, J.-S.; Park, S.-D. The relationship between the survival of total knee arthroplasty and postoperative coronal, sagittal and rotational alignment of knee prosthesis. Int. Orthop. 2013, 38, 379–385. [Google Scholar] [CrossRef]
- Franceschini, V.; Nodzo, S.R.; Della Valle, A.G. Femoral Component Rotation in Total Knee Arthroplasty: A Comparison Between Transepicondylar Axis and Posterior Condylar Line Referencing. J. Arthroplast. 2016, 31, 2917–2921. [Google Scholar] [CrossRef]
- Geiger, F.; Parsch, D. Intraoperative assessment of femoral component rotational alignment in total knee arthroplasty. Arch. Orthop. Trauma Surg. 2007, 128, 267–270. [Google Scholar] [CrossRef]
- Stoeckl, B.; Nogler, M.; Krismer, M.; Beimel, C.; de la Barrera, J.-L.M.; Kessler, O. Reliability of the Transepicondylar Axis as an Anatomical Landmark in Total Knee Arthroplasty. J. Arthroplast. 2006, 21, 878–882. [Google Scholar] [CrossRef]
- Jerosch, J.; Peuker, E.; Philipps, B.; Filler, T.J. Interindividual reproducibility in perioperative rotational alignment of femoral components in knee prosthetic surgery using the transepicondylar axis. Knee Surgery. Sports Traumatol. Arthrosc. 2002, 10, 194–197. [Google Scholar] [CrossRef]
- Dennis, D.A.; Komistek, R.D.; Kim, R.H.; Sharma, A. Gap Balancing versus Measured Resection Technique for Total Knee Arthroplasty. Clin. Orthop. Relat. Res. 2010, 468, 102–107. [Google Scholar] [CrossRef] [PubMed]
- Daines, B.K.; Dennis, D.A. Gap Balancing vs. Measured Resection Technique in Total Knee Arthroplasty. Clin. Orthop. Surg. 2014, 6, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Siddiqi, A.; Mont, M.A.; Krebs, V.E.; Piuzzi, N.S. Not All Robotic-assisted Total Knee Arthroplasty Are the Same. J. Am. Acad. Orthop. Surg. 2020, 29, 45–59. [Google Scholar] [CrossRef] [PubMed]
- Onggo, J.R.; Onggo, J.D.; De Steiger, R.; Hau, R. Robotic-assisted total knee arthroplasty is comparable to conventional total knee arthroplasty: A meta-analysis and systematic review. Arch. Orthop. Trauma Surg. 2020, 140, 1533–1549. [Google Scholar] [CrossRef]
- Babazadeh, S. The relevance of ligament balancing in total knee arthroplasty: How important is it? A systematic review of the literature. Orthop. Rev. 2009, 1, e26. [Google Scholar] [CrossRef]
- Song, S.J.; Park, C.H.; Bae, D.K. What to Know for Selecting Cruciate-Retaining or Posterior-Stabilized Total Knee Arthroplasty. Clin. Orthop. Surg. 2019, 11, 142–150. [Google Scholar] [CrossRef]
- Benazzo, F.; Rossi, S.M.P.; Danesino, G.; Klersy, C.; Perelli, S.; Ghiara, M. Computed tomography evaluation of total knee arthroplasty implants position after two different surgical methods of implantation. Int. Orthop. 2018, 43, 139–149. [Google Scholar] [CrossRef]
- Battenberg, A.K.; Netravali, N.A.; Lonner, J.H. A novel handheld robotic-assisted system for unicompartmental knee arthroplasty: Surgical technique and early survivorship. J. Robot. Surg. 2019, 14, 55–60. [Google Scholar] [CrossRef]
- Berger, R.; Rubash, H.; Seel, M.J.; Thompson, W.H.; Crossett, L.S. Determining the rotational alignment of the femoral component in total knee arthroplasty using the epicondylar axis. Clin. Orthop. Relat. Res. 1993, 286, 40–47. [Google Scholar] [CrossRef]
- Galea, V.P.; Botros, M.A.; Madanat, R.; Nielsen, C.S.; Bragdon, C. Promising early outcomes of a novel anatomic knee system. Knee Surgery. Sports Traumatol. Arthrosc. 2018, 27, 1067–1074. [Google Scholar] [CrossRef]
- Scigliano, N.M.; Carender, C.N.; Glass, N.A.; Deberg, J.; Bedard, N.A. Operative Time and Risk of Surgical Site Infection and Periprosthetic Joint Infection: A Systematic Review and Meta-Analysis. Iowa Orthop. J. 2022, 42, 155–161. [Google Scholar]
- Sharma, D.; Shukla, A.; Kumar, K. Role of preoperative calculation of condylar twist angle (CTA) by CT scan in optimizing femoral component rotation during TKA. Musculoskelet. Surg. 2017, 101, 207–212. [Google Scholar] [CrossRef] [PubMed]
- Figueroa, J.; Guarachi, J.P.; Matas, J.; Arnander, M.; Orrego, M. Is computed tomography an accurate and reliable method for measuring total knee arthroplasty component rotation? Int. Orthop. 2015, 40, 709–714. [Google Scholar] [CrossRef] [PubMed]
- Heesterbeek, P.J.C.; Jacobs, W.C.H.; Wymenga, A.B. Effects of the Balanced Gap Technique on Femoral Component Rotation in TKA. Clin. Orthop. Relat. Res. 2008, 467, 1015–1022. [Google Scholar] [CrossRef] [PubMed]
- Tsukiyama, H.; Kuriyama, S.; Kobayashi, M.; Nakamura, S.; Furu, M.; Ito, H.; Matsuda, S. Medial rather than lateral knee instability correlates with inferior patient satisfaction and knee function after total knee arthroplasty. Knee 2017, 24, 1478–1484. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| Age > 50 | Prior HTO or another lower limb surgery before TKR |
| Confirmed osteoarthritis treated with standard doses of non-steroid anti-inflammatory drugs before surgery | Rheumatoid arthritis, positive rheumatoid factor in serum |
| Moderate-to-severe osteoarthritis lasting more than three years | Erythrocyte-sedimentation rate or C-reactive protein over the normal range |
| Primary TKA, PS implant, no patella resurfacing | Qualification for a CR implant |
| Flexion contracture of the knee >15° | |
| Post-TKA CT scan available for assessment |
| Baseline Group Characteristics | ||||
|---|---|---|---|---|
| Fuzion | Measured Resection Technique | Navio | p-Value | |
| BMI (body mass index—kg/m2) | 30.15 ± 4.01 | 30.28 ± 4.42 | 31.29 ± 4.93 | 0.46 |
| Age (years) | 68.81 ± 7.31 | 71.16 ± 7.13 | 67.25 ± 6.05 | <0.05 |
| Male: female (No. of subjects) | 12:19 | 18:21 | 15:46 | 0.0678 |
| Comparison between Groups (p-Value) | ||||
|---|---|---|---|---|
| Group | Mean Rotation (Degrees); Positive Value Indicates External Rotation | vs. Fuzion | vs. Measured Resection Technique | vs. Navio |
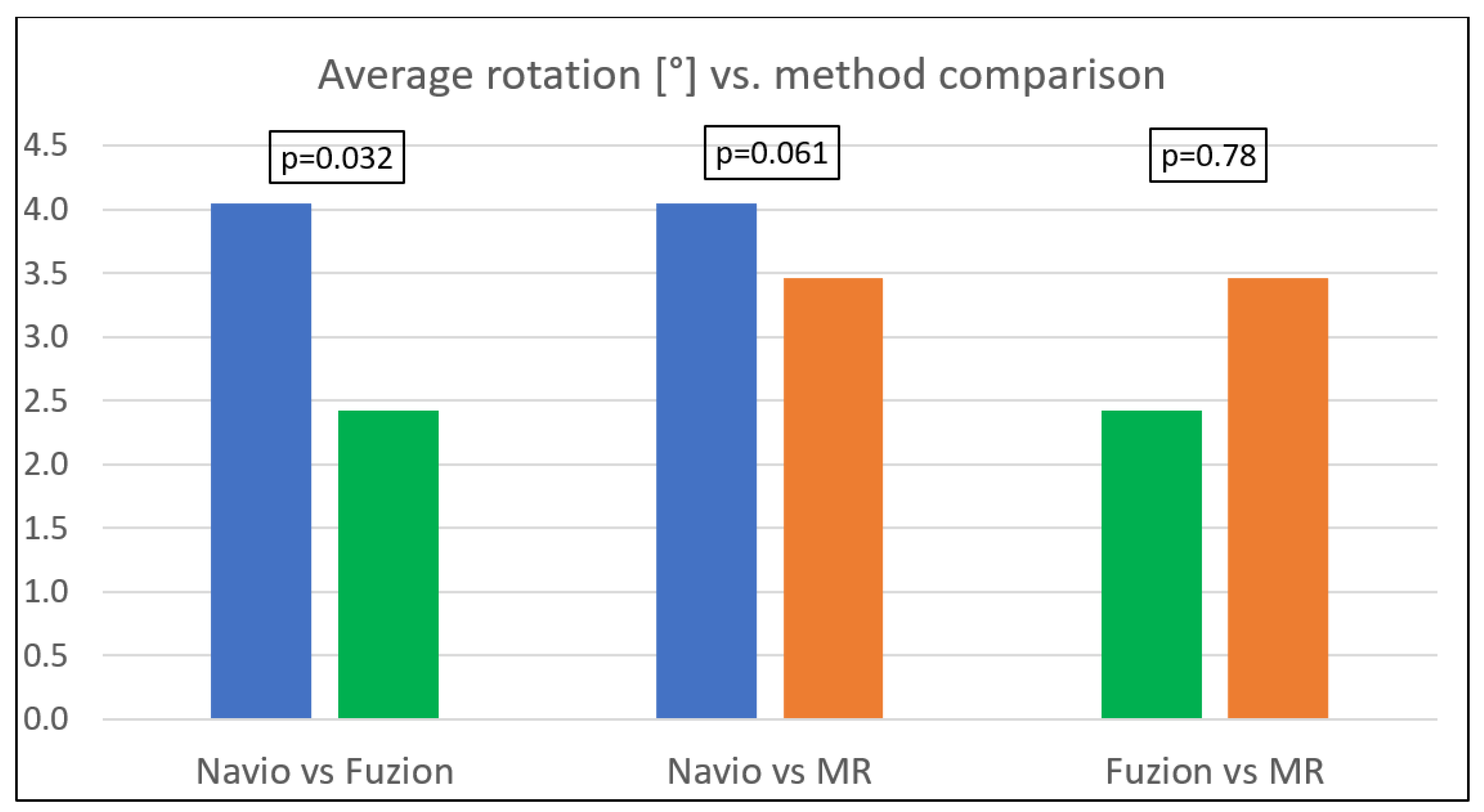
| Fuzion | 2.42 ± 2.87 | - | 0.78 | 0.0321 |
| Measured-resection technique | 3.46 ± 1.86 | 0.78 | - | 0.0613 |
| Navio | 4.05 ± 1.89 | 0.0321 | 0.0613 | - |
| Difference between the groups | 0.0137 | |||
| Comparison between Groups (p-Value) | |||||
|---|---|---|---|---|---|
| Group | Number of Subjects (Post-TKA Subjects with External Rotation of the Component/Total Number of Subjects in Group) | Percentage | vs. Fuzion | vs. Measured Resection Technique | vs. Navio |
| Fuzion | 26/31 | 83.87 | - | >0.05 | >0.05 |
| Measured-resection technique | 39/39 | 100.00 | >0.05 | - | >0.05 |
| Navio | 59/61 | 96.72 | >0.05 | >0.05 | - |
| Difference between the groups | 0.0124 | ||||
| Comparison between Groups (p-Value): | |||||
|---|---|---|---|---|---|
| Group | Number of Subjects (Post-TKA Subjects with 0° and Internal Rotation of the Component/Total Number of Subjects in Group) | Percentage | vs. Fuzion | vs. Measured Resection Technique | vs. Navio |
| Fuzion | 5/31 | 16.13 | - | >0.05 | >0.05 |
| Measured-resection technique | 0/39 | 0.00 | >0.05 | - | >0.05 |
| Navio | 2/61 | 3.28 | >0.05 | >0.05 | - |
| Difference between the groups | 0.0124 | ||||
| Comparison between Groups (p-Value): | |||||
|---|---|---|---|---|---|
| Group | Number of Subjects | Percentage | vs. Fuzion | vs. Measured Resection Technique | vs. Navio |
| Fuzion | 8/31 | 25.81 | - | >0.05 | >0.05 |
| Measured-resection technique | 16/39 | 41.03 | >0.05 | - | >0.05 |
| Navio | 14/61 | 22.95 | >0.05 | >0.05 | - |
| Difference between the groups | 0.14 | ||||
| Group | Number of Subjects | Minimum (Degrees) | Maximum (Degrees) |
|---|---|---|---|
| Fuzion | 31 | −3.00 | 7.00 |
| Measured-resection technique | 39 | 0 | 8.00 |
| Navio | 61 | −2.00 | 9.00 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maciąg, B.M.; Kordyaczny, T.; Maciąg, G.J.; Łapiński, M.; Jegierski, D.; Świderek, J.; Tsitko, H.; Dorocińska, M.; Żarnovsky, K.; Świercz, M.; et al. Comparison of Femoral Component Rotation between Robotic-Assisted vs. Soft-Tissue Tensor Total Knee Arthroplasty with Anatomic Implants. Medicina 2023, 59, 880. https://doi.org/10.3390/medicina59050880
Maciąg BM, Kordyaczny T, Maciąg GJ, Łapiński M, Jegierski D, Świderek J, Tsitko H, Dorocińska M, Żarnovsky K, Świercz M, et al. Comparison of Femoral Component Rotation between Robotic-Assisted vs. Soft-Tissue Tensor Total Knee Arthroplasty with Anatomic Implants. Medicina. 2023; 59(5):880. https://doi.org/10.3390/medicina59050880
Chicago/Turabian StyleMaciąg, Bartosz M., Tomasz Kordyaczny, Grzegorz J. Maciąg, Marcin Łapiński, Dawid Jegierski, Jakub Świderek, Hanna Tsitko, Monika Dorocińska, Krystian Żarnovsky, Maciej Świercz, and et al. 2023. "Comparison of Femoral Component Rotation between Robotic-Assisted vs. Soft-Tissue Tensor Total Knee Arthroplasty with Anatomic Implants" Medicina 59, no. 5: 880. https://doi.org/10.3390/medicina59050880
APA StyleMaciąg, B. M., Kordyaczny, T., Maciąg, G. J., Łapiński, M., Jegierski, D., Świderek, J., Tsitko, H., Dorocińska, M., Żarnovsky, K., Świercz, M., Stępiński, P., Adamska, O., & Stolarczyk, A. (2023). Comparison of Femoral Component Rotation between Robotic-Assisted vs. Soft-Tissue Tensor Total Knee Arthroplasty with Anatomic Implants. Medicina, 59(5), 880. https://doi.org/10.3390/medicina59050880