
Cervico-Dorsal Intramedullary Spinal Cord Abscess with Aspergillus fumigates following Pulmonary Infection in an Immunocompetent Patient

 and
and
Abstract
1. Introduction
2. Detailed Case Description
- Gram-stained smears showed an intense inflammatory reaction with neutrophils;
- Ziehl-Neelsen-stained smear was negative for acid fast bacilli;
- Culture for Mycobacterium tuberculosis was negative;
- Twenty colonies of Aspergillus spp. were identified in fungal culture.
3. Discussion
- Three-month duration of pulmonary symptoms;
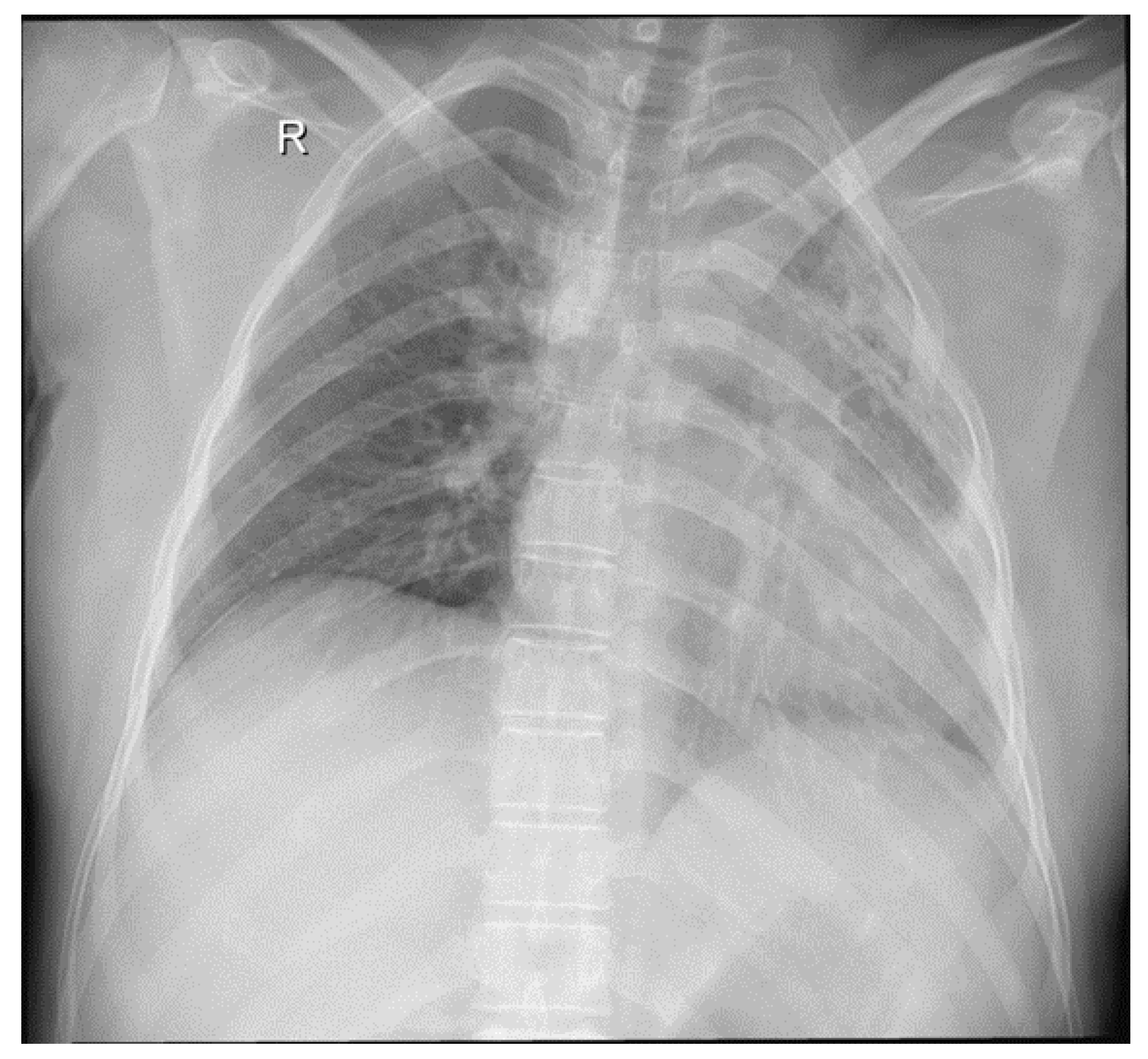
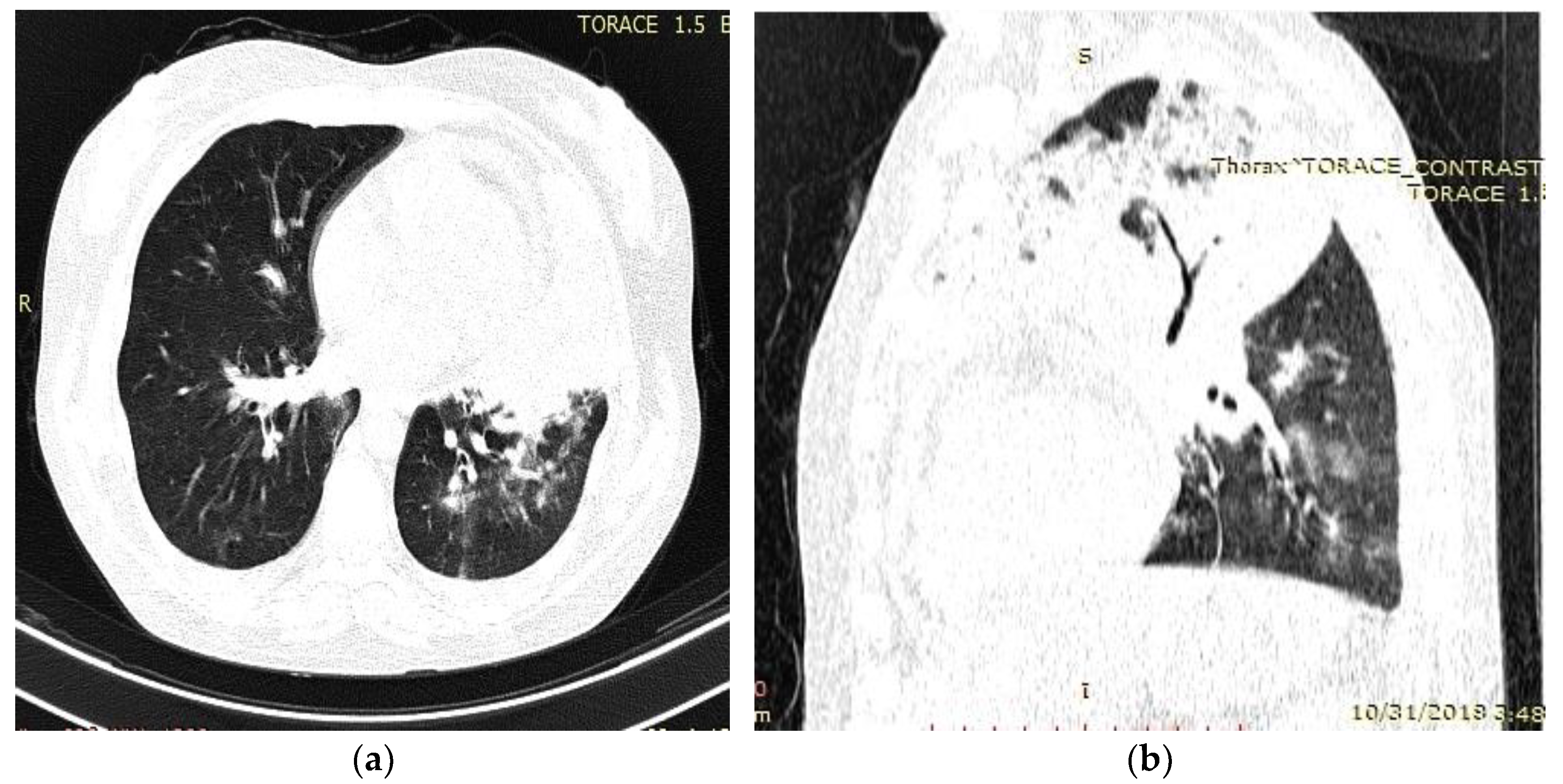
- Radiological evidence of chronic pulmonary lesion;
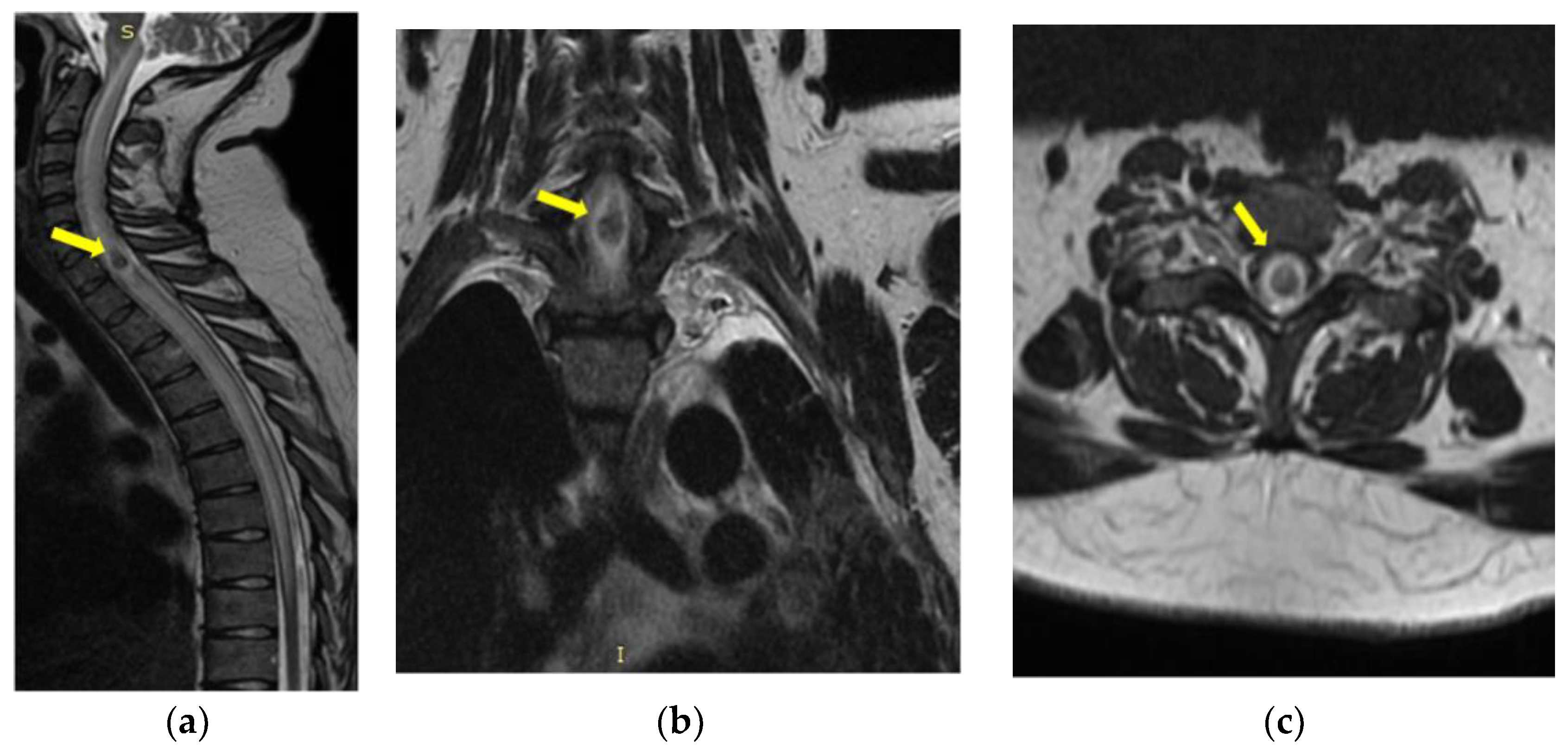
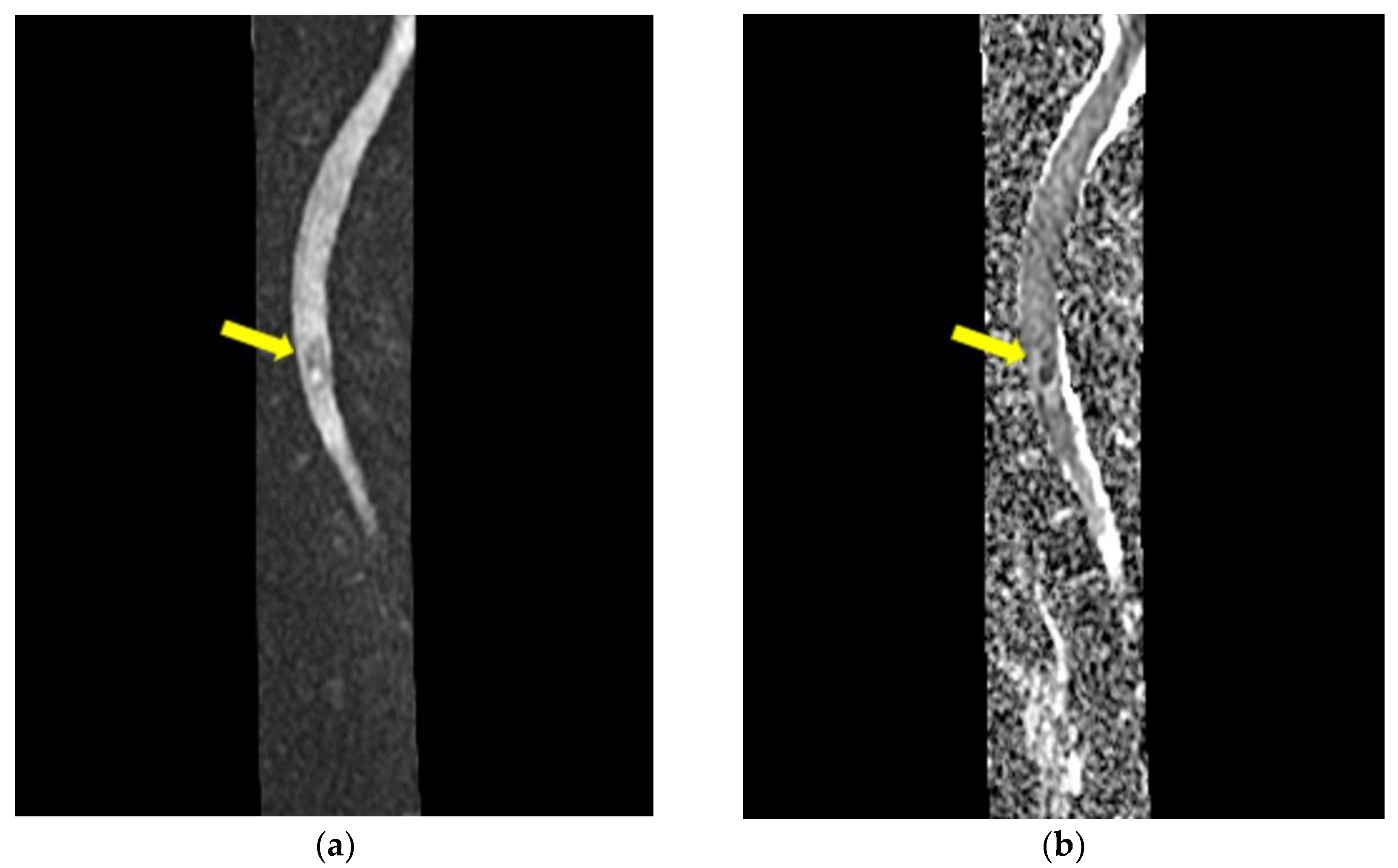
- Mycological demonstration of Aspergillus fumigates hyphae by microscopy from spu-tum, microscopy and culture from bronchial aspirate, and histopathological evi-dence of the presence of Aspergillus fumigates hyphae with dichotomous branching in the spinal cord biopsy;
- Exclusion of other pulmonary pathogens, such as tuberculosis mycobacteria;
- Lack of major discernible immunodeficiency, such as AIDS, leukemia, or organ trans-plant, but working in a humid space with molds on its walls.
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Elad, D.; Segal, E. Diagnostic Aspects of Veterinary and Human Aspergillosis. Front. Microbiol. 2018, 9, 1303. [Google Scholar] [CrossRef] [PubMed]
- Findlay, G.H.; Roux, H.F.; Simson, I.W. Skin manifestations of disseminated aspergillosis. Br. J. Dermatol. 1971, 85, 94–97. [Google Scholar] [CrossRef]
- Nannini, E.C.; Paphitou, N.I.; Ostrosky-Zeichner, L. Peritonitis due to Aspergillus and zygomycetes in patients undergoing peritoneal dialysis: Report of 2 cases and review of the literature. Diagn. Microbiol. Infect. Dis. 2003, 46, 49–54. [Google Scholar] [CrossRef] [PubMed]
- Latgé, J.P. Aspergillus fumigatus and Aspergillosis. Clin. Microbiol. Rev. 1999, 12, 310–350. [Google Scholar] [CrossRef]
- Hori, A.; Kami, M.; Kishi, Y.; Machida, U.; Matsumura, T.; Kashima, T. Clinical significance of extra-pulmonary involvement of invasive aspergillosis: A retrospective autopsy-based study of 107 patients. J. Hosp. Infect. 2002, 50, 175–182. [Google Scholar] [CrossRef]
- Fortún, J.; Meije, Y.; Fresco, G.; Moreno, S. Aspergillosis. Clinical forms and treatment. Enferm. Infecc. Microbiol. Clin. 2012, 30, 201–208. [Google Scholar] [CrossRef]
- Dogra, V.; Sinha, A.K.; Saxena, R.; Talwar, D. Aspergillus march: From ABPA to aspergilloma to subacute invasive aspergillosis. Allergy Asthma Clin. Immunol. 2016, 12, 64. [Google Scholar] [CrossRef]
- López-Cortés, L.E.; Garcia-Vidal, C.; Ayats, J.; Gudiol, C.; Bodro, M.; Sánchez-Ortega, I.; Peña, C.; Carratalá, J. Invasive aspergillosis with extrapulmonary involvement: Pathogenesis, clinical characteristics and prognosis. Rev. Iberoam. Micol. 2012, 29, 139–143. [Google Scholar] [CrossRef]
- Cicek, N.; Yildiz, N.; Kadayif, E.K.; Gokce, I.; Alpay, H. Invasive aspergillosis in a patient with end stage renal disease. Med. Mycol. Case Rep. 2017, 18, 12–14. [Google Scholar] [CrossRef]
- Sethi, S.; Siraj, F.; Kalra, K.L.; Chopra, P. Aspergillus vertebral osteomyelitis in immunocompetent patients. Indian J. Orthop. 2012, 46, 246–250. [Google Scholar] [CrossRef]
- Tendolkar, U.; Sharma, A.; Mathur, M.; Ranadive, N.; Sachdev, M. Epidural mass due to Aspergillus flavus causing spinal cord compression—A case report and brief update. Indian J. Med. Microbiol. 2005, 23, 200–203. [Google Scholar] [CrossRef]
- Heinemann, S.; Symoens, F.; Gordts, B.; Jannes, H.; Nolard, N. Environmental investigations and molecular typing of Aspergillus flavus during an outbreak of postoperative infections. J. Hosp. Infect. 2004, 57, 149–155. [Google Scholar] [CrossRef]
- Gunaratne, P.S.; Wijeyaratne, C.N.; Chandrasiri, P.; Sivakumaran, S.; Sellahewa, K.; Perera, P.; Fernando, R.; Wanigasinghe, J.; Jayasinghe, S.; Ranawala, R.; et al. An outbreak of Aspergillus meningitis following spinal anaesthesia for caesarean section in Sri Lanka: A post-tsunami effect? Ceylon Med. J. 2006, 51, 137–142. [Google Scholar] [CrossRef]
- Solomon, G.M.; Hjelmroos-Koski, M.; Rotkin-Ellman, M.; Hammond, S.K. Airborne Mold and Endotoxin Concentrations in New Orleans, Louisiana, after Flooding, October through November 2005. Environ Health Perspect. 2006, 114, 1381–1386. [Google Scholar] [CrossRef]
- Chakrabarti, A.; Chatterjee, S.S.; Das, A.; Shivaprakash, M.R. Invasive aspergillosis in developing countries. Med. Mycol. 2011, 49 (Suppl. S1), S35–S47. [Google Scholar] [CrossRef]
- Jiang, Z.; Wang, Y.; Jiang, Y.; Xu, Y.; Meng, B. Vertebral osteomyelitis and epidural abscess due to Aspergillus nidulans resulting in spinal cord compression: Case report and literature review. J. Int. Med. Res. 2013, 41, 502–510. [Google Scholar] [CrossRef]
- Studemeister, A.; Stevens, D.A. Aspergillus vertebral osteomyelitis in immunocompetent hosts: Role of triazole antifungal therapy. Clin. Infect. Dis. 2011, 52, e1–e6. [Google Scholar] [CrossRef]
- Nakazato, I.; Kamada, Y.; Taira, T.; Iwamasa, T. Massive spinal cord necrosis associated with adult T-cell leukemia caused by aspergillus. Virchows Arch. Pathol. Anat. Histopathol. 1993, 243, 397–400. [Google Scholar] [CrossRef]
- Fernandez de Orueta, L.; Andrés, R.; Elías, T.; Pintado, V. Vertebral aspergillosis in a cirrhotic patient: An uncommon cause of spondylitis. Enferm. Infecc. Microbiol. Clin. 2012, 30, 219–220. [Google Scholar] [CrossRef]
- Sherif, R.; Segal, B.H. Pulmonary Aspergillosis: Clinical presentation, diagnostic tests, management and complications. Curr. Opin. Pulm. Med. 2010, 16, 242–250. [Google Scholar] [CrossRef]
- Nicolle, A.; de la Blanchardière, A.; Bonhomme, J.; Hamon, M.; Leclercq, R.; Hitier, M. Aspergillus vertebral osteomyelitis in immunocompetent subjects: Case report and review of the literature. Infection 2013, 41, 833–840. [Google Scholar] [CrossRef] [PubMed]
- McCaslin, A.F.; Lall, R.R.; Wong, A.P.; Lall, R.R.; Sugrue, P.A.; Koski, T.R. Thoracic spinal cord intramedullary aspergillus invasion and abscess. J. Clin. Neurosci. 2015, 22, 404–406. [Google Scholar] [CrossRef] [PubMed]
- Binder, R.E.; Faling, L.J.; Pugatch, R.D.; Mahasaen, C.; Snider, G.L. Chronic necrotizing pulmonary aspergillosis: A discrete clinical entity. Medicine 1982, 61, 109–124. [Google Scholar] [CrossRef] [PubMed]
- Kontoyiannis, D.P.; Bodey, G.P. Invasive aspergillosis in 2002: An update. Eur. J. Clin. Microbiol. Infect. Dis. 2002, 21, 161–172. [Google Scholar] [CrossRef] [PubMed]
- Libshitz, H.I.; Pagani, J.J. Aspergillosis and mucormycosis: Two types of opportunistic fungal pneumonia. Radiology 1981, 140, 301–306. [Google Scholar] [CrossRef]
- Abers, M.S.; Ghebremichael, M.S.; Timmons, A.K.; Warren, H.S.; Poznansky, M.C.; Vyas, J.M. A Critical Reappraisal of Prolonged Neutropenia as a Risk Factor for Invasive Pulmonary Aspergillosis. Open Forum Infect. Dis. 2016, 3, ofw036. [Google Scholar] [CrossRef]
- Richardson, W.; Ortiz, D.M.; Cantu, M.A.; Villalobos, F.; Newton, O.A. Fatal Cutaneous and Disseminated Nosocomial Aspergillosis. A Case Report. Pediatr. Res. 1999, 45, 172. [Google Scholar] [CrossRef]
- Hou, X.; Zhang, H.; Kou, L.; Lu, W.; Lu, J.; Li, J. Clinical features and diagnosis of chronic pulmonary aspergillosis in Chinese patients. Medicine 2017, 96, e8315. [Google Scholar] [CrossRef]
- Rossouw, I.; Goedhals, D.; van der Merwe, J.; Stallenberg, V.; Govender, N. A rare, fatal case of invasive spinal aspergillosis in an antiretroviral-naive, HIV-infected man with pre-existing lung colonization. J. Med. Microbiol. 2011, 60 Pt 10, 1534–1538. [Google Scholar] [CrossRef]
- Karakousis, P.C.; Magill, S.S.; Gupta, A. Paraplegia caused by invasive spinal aspergillosis. Neurology 2007, 69, 222–223. [Google Scholar] [CrossRef]
- Sheth, N.K.; Varkey, B.; Wagner, D.K. Spinal cord aspergillus invasion--complication of an aspergilloma. Am. J. Clin. Pathol. 1985, 84, 763–769. [Google Scholar] [CrossRef]
- Guermazi, A.; Gluckman, E.; Tabti, B.; Miaux, Y. Invasive central nervous system aspergillosis in bone marrow transplantation recipients: An overview. Eur. Radiol. 2003, 13, 377–388. [Google Scholar] [CrossRef]
- Horn, D.; Sae-Tia, S.; Neofytos, D. Aspergillus osteomyelitis: Review of 12 cases identified by the Prospective Antifungal Therapy Alliance registry. Diagn Microbiol. Infect Dis. 2009, 63, 384–387. [Google Scholar] [CrossRef]
- Al-Maskari, N.; Hussain, I.; Jumaa, S.; Al-Shail, E.A. Aspergillus flavus-Induced Brain Abscess in an Immunocompetent Child. Sultan Qaboos Univ. Med. J. 2016, 16, e246–e249. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Laboratory Analysis | 1st Admission (County Hospital, Focsani) | 2nd Admission (Thoracic Surgery Unit, Iasi) | 3rd Admission (Institute of Pneumology, Bucharest) | 4th Admission (Neurosurgery, Iasi) |
|---|---|---|---|---|
| Erythrocytes | 2.7 × 106/mm3 | 2.6 × 106/mm3 | 1.86 × 106/mm3 | 3.89 × 106/mm3 |
| Hemoglobin | 8.1 g/dL | 6.5 g/dL | 5.3 g/dL | 12 g/dL |
| Hematocrit | 28.9% | 24% | 17.5% | 35.6% |
| Leucocytes | 30.5 × 103/mm3 | 35.67 × 103/mm3 | 29 × 103/mm3 | 11.23 × 103/mm3 |
| Neutrophils | 86.4% (20.35 × 103/μL) | 85.5% (30.49 × 103/μL) | 95.7% (28.27 × 103/μL) | 62.9% (7.06 × 103/μL) |
| Basophiles | 2.3% | 0% | 0.1% | 0.6% |
| Eosinophils | 0.5% | 0.1% | 0.1% | 1.8% |
| Monocytes | 4% | 4.1% | 1.8% | 4.3% |
| Lymphocytes | 5.7% | 10.3% | 2.3% | 26.4% |
| Thrombocytes | 788 × 103/μL | 1130 × 103/μL | 817 × 103/μL | 388 × 103/μL |
| Fibrinogen | 791 mg/mL | not available | not available | 399 mg/dL |
| ESR | 115 mm/h | 140 mm/h | 160 mm/h | 68 mm/h |
| Antibodies to HIV-1 and HIV-2 | negative | not available | negative | negative |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mereuta, V.D.; Sava, A.; Stan, C.I.; Eva, L.; Dumitrescu, G.F.; Dobrin, N.; Tudorache, C.; Chiriac, A.; Strambu, I.R.; Chiran, D.A.; et al. Cervico-Dorsal Intramedullary Spinal Cord Abscess with Aspergillus fumigates following Pulmonary Infection in an Immunocompetent Patient. Medicina 2023, 59, 806. https://doi.org/10.3390/medicina59040806
Mereuta VD, Sava A, Stan CI, Eva L, Dumitrescu GF, Dobrin N, Tudorache C, Chiriac A, Strambu IR, Chiran DA, et al. Cervico-Dorsal Intramedullary Spinal Cord Abscess with Aspergillus fumigates following Pulmonary Infection in an Immunocompetent Patient. Medicina. 2023; 59(4):806. https://doi.org/10.3390/medicina59040806
Chicago/Turabian StyleMereuta, Vasile Deniss, Anca Sava, Cristinel Ionel Stan, Lucian Eva, Gabriela Florenta Dumitrescu, Nicolaie Dobrin, Cornelia Tudorache, Alexandru Chiriac, Irina Ruxandra Strambu, Dragos Andrei Chiran, and et al. 2023. "Cervico-Dorsal Intramedullary Spinal Cord Abscess with Aspergillus fumigates following Pulmonary Infection in an Immunocompetent Patient" Medicina 59, no. 4: 806. https://doi.org/10.3390/medicina59040806
APA StyleMereuta, V. D., Sava, A., Stan, C. I., Eva, L., Dumitrescu, G. F., Dobrin, N., Tudorache, C., Chiriac, A., Strambu, I. R., Chiran, D. A., & Dumitrescu, A. M. (2023). Cervico-Dorsal Intramedullary Spinal Cord Abscess with Aspergillus fumigates following Pulmonary Infection in an Immunocompetent Patient. Medicina, 59(4), 806. https://doi.org/10.3390/medicina59040806