
Efficacy and Effectiveness of Extracorporeal Shockwave Therapy in Patients with Myofascial Pain or Fibromyalgia: A Scoping Review

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
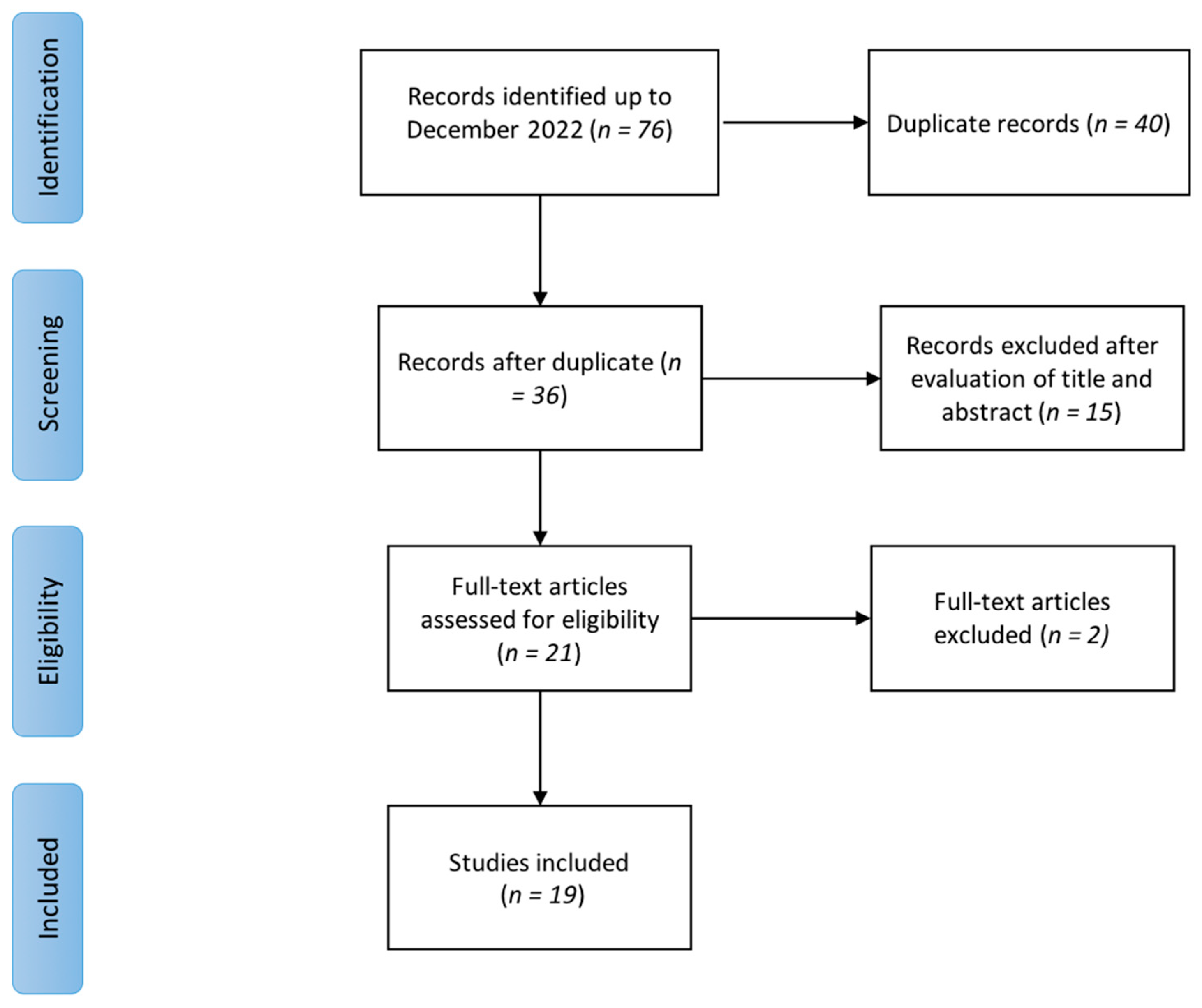
2.1. Search Strategy
2.2. Study Selection
2.3. Data Extraction and Quality Assessment
3. Results
3.1. Radial ESWT
3.2. Focused ESWT
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Poveda-Pagán, E.J.; Lozano-Quijada, C.; Segura-Heras, J.V.; Peral-Berna, M.; Lumbreras, B. Referred Pain Patterns of the Infraspinatus Muscle Elicited by Deep Dry Needling and Manual Palpation. J. Altern Complement. Med. 2017, 23, 890–896. [Google Scholar] [CrossRef] [PubMed]
- Cao, Q.W.; Peng, B.G.; Wang, L.; Huang, Y.Q.; Jia, D.L.; Jiang, H.; Lv, Y.; Liu, X.G.; Liu, R.G.; Li, Y.; et al. Expert consensus on the diagnosis and treatment of myofascial pain syndrome. World J. Clin. Cases 2021, 9, 2077–2089. [Google Scholar] [CrossRef] [PubMed]
- Jin, F.; Guo, Y.; Wang, Z.; Badughaish, A.; Pan, X.; Zhang, L.; Qi, F. The pathophysiological nature of sarcomeres in trigger points in patients with myofascial pain syndrome: A preliminary study. Eur. J. Pain. 2020, 24, 1968–1978. [Google Scholar] [CrossRef] [PubMed]
- Shah, J.P.; Danoff, J.V.; Desai, M.J.; Parikh, S.; Nakamura, L.Y.; Phillips, T.M.; Gerber, L.H. Biochemicals associated with pain and inflammation are elevated in sites near to and remote from active myofascial trigger points. Arch. Phys. Med. Rehabil. 2008, 89, 16–23. [Google Scholar] [CrossRef]
- Mazza, D.F.; Boutin, R.D.; Chaudhari, A.J. Assessmen.nt of Myofascial Trigger Points via Imaging: A Systematic Review. Am. J. Phys. Med. Rehabil. 2021, 100, 1003–1014. [Google Scholar] [CrossRef]
- Bair, M.J.; Krebs, E.E. Fibromyalgia. Ann. Intern. Med. 2020, 172, ITC33. [Google Scholar] [CrossRef]
- Koppenhaver, S.L.; Walker, M.J.; Rettig, C.; Davis, J.; Nelson, C.; Su, J.; Fernández-de-Las-Peñas, C.; Hebert, J.J. The association between dry needling-induced twitch response and change in pain and muscle function in patients with low back pain: A quasi-experimental study. Physiotherapy 2017, 103, 131–137. [Google Scholar] [CrossRef] [Green Version]
- Rha, D.W.; Shin, J.C.; Kim, Y.K.; Jung, J.H.; Kim, Y.U.; Lee, S.C. Detecting local twitch responses of myofascial trigger points in the lower-back muscles using ultrasonography. Arch. Phys. Med. Rehabil. 2011, 92, 1576–1580. [Google Scholar] [CrossRef]
- Ryskalin, L.; Morucci, G.; Natale, G.; Soldani, P.; Gesi, M. Molecular Mechanisms Underlying the Pain-Relieving Effects of Extracorporeal Shock Wave Therapy: A Focus on Fascia Nociceptors. Life 2022, 12, 743.e1. [Google Scholar] [CrossRef]
- Aschermann, I.; Noor, S.; Venturelli, S.; Sinnberg, T.; Mnich, C.D.; Busch, C. Extracorporal Shock Waves Activate Migration, Proliferation and Inflammatory Pathways in Fibroblasts and Keratinocytes, and Improve Wound Healing in an Open-Label, Single-Arm Study in Patients with Therapy-Refractory Chronic Leg Ulcers. Cell Physiol Biochem. 2017, 41, 890–906. [Google Scholar] [CrossRef]
- Simplicio, C.L.; Purita, J.; Murrell, W.; Santos, G.S.; Dos Santos, R.G.; Lana, J.F.S.D. Extracorporeal shock wave therapy mechanisms in musculoskeletal regenerative medicine. J. Clin. Orthop Trauma. 2020, 11, S309–S318. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [Green Version]
- Taheri, P.; Vahdatpour, B.; Andalib, S. Comparative study of shock wave therapy and Laser therapy effect in elimination of symptoms among patients with myofascial pain syndrome in upper trapezius. Adv. Biomed. Res. 2016, 5, 138. [Google Scholar] [CrossRef]
- Király, M.; Bender, T.; Hodosi, K. Comparative study of shockwave therapy and low-level laser therapy effects in patients with myofascial pain syndrome of the trapezius. Rheumatol. Int. 2018, 38, 2045–2052. [Google Scholar] [CrossRef]
- Aktürk, S.; Kaya, A.; Çetintaş, D.; Akgöl, G.; Gülkesen, A.; Kal, G.A.; Güçer, T. Comparision of the effectiveness of ESWT and ultrasound treatments in myofascial pain syndrome: Randomized, sham-controlled study. J. Phys. Ther Sci. 2018, 30, 448–453. [Google Scholar] [CrossRef] [Green Version]
- Rahbar, M.; Samandarian, M.; Salekzamani, Y.; Khamnian, Z.; Dolatkhah, N. Effectiveness of extracorporeal shock wave therapy versus standard care in the treatment of neck and upper back myofascial pain: A single blinded randomised clinical trial. Clin. Rehabil. 2021, 35, 102–113. [Google Scholar] [CrossRef]
- Gezgİnaslan, Ö.; GÜmÜŞ Atalay, S. High-Energy Flux Density Extracorporeal Shock Wave Therapy Versus Traditional Physical Therapy Modalities in Myofascial Pain Syndrome: A Randomized-controlled, Single-Blind Trial. Arch. Rheumatol. 2019, 35, 78–89. [Google Scholar] [CrossRef]
- Taheri, P.; Naderi, M.; Khosravi, S. Extracorporeal Shock Wave Therapy Versus Phonophoresis Therapy for Neck Myofascial Pain Syndrome: A Randomized Clinical Trial. Anesth Pain Med. 2021, 11, e112592. [Google Scholar] [CrossRef]
- Walsh, R.; Kinsella, S.; McEvoy, J. The effects of dry needling and radial extracorporeal shockwave therapy on latent trigger point sensitivity in the quadriceps: A randomised control pilot study. J. Bodyw. Mov. Ther. 2019, 23, 82–88. [Google Scholar] [CrossRef] [Green Version]
- Luan, S.; Zhu, Z.M.; Ruan, J.L.; Lin, C.N.; Ke, S.J.; Xin, W.J.; Liu, C.C.; Wu, S.L.; Ma, C. Randomized Trial on Comparison of the Efficacy of Extracorporeal Shock Wave Therapy and Dry Needling in Myofascial Trigger Points. Am. J. Phys. Med. Rehabil. 2019, 98, 677–684. [Google Scholar] [CrossRef]
- Manafnezhad, J.; Salahzadeh, Z.; Salimi, M.; Ghaderi, F.; Ghojazadeh, M. The effects of shock wave and dry needling on active trigger points of upper trapezius muscle in patients with non-specific neck pain: A randomized clinical trial. J. Back Musculoskelet. Rehabil. 2019, 32, 811–818. [Google Scholar] [CrossRef] [PubMed]
- Eftekharsadat, B.; Fasaie, N.; Golalizadeh, D.; Babaei-Ghazani, A.; Jahanjou, F.; Eslampoor, Y.; Dolatkhah, N. Comparison of efficacy of corticosteroid injection versus extracorporeal shock wave therapy on inferior trigger points in the quadratus lumborum muscle: A randomized clinical trial. BMC Musculoskelet. Disord. 2020, 21, 695. [Google Scholar] [CrossRef] [PubMed]
- Li, W.; Wu, J. Treatment of Temporomandibular Joint Disorders by Ultrashort Wave and Extracorporeal Shock Wave: A Comparative Study. Med. Sci Monit. 2020, 26, e923461. [Google Scholar] [CrossRef]
- Sugawara, A.T.; Lima, M.D.C.; Dias, C.B. Predictive factors of response in radial Extracorporeal Shock-waves Therapy for Myofascial and Articular Pain: A retrospective cohort study. J. Back Musculoskelet. Rehabil. 2021, 34, 485–490. [Google Scholar] [CrossRef] [PubMed]
- Jeon, J.H.; Jung, Y.J.; Lee, J.Y.; Choi, J.S.; Mun, J.H.; Park, W.Y.; Seo, C.H.; Jang, K.U. The effect of extracorporeal shock wave therapy on myofascial pain syndrome. Ann. Rehabil. Med. 2012, 36, 665–674. [Google Scholar] [CrossRef] [PubMed]
- Ji, H.M.; Kim, H.J.; Han, S.J. Extracorporeal shock wave therapy in myofascial pain syndrome of upper trapezius. Ann. Rehabil Med. 2012, 36, 675–680. [Google Scholar] [CrossRef] [Green Version]
- Park, K.D.; Lee, W.Y.; Park, M.H.; Ahn, J.K.; Park, Y. High- versus low-energy extracorporeal shock-wave therapy for myofascial pain syndrome of upper trapezius: A prospective randomized single blinded pilot study. Medicine 2018, 97, e11432. [Google Scholar] [CrossRef]
- Kamel, F.H.; Basha, M.; Alsharidah, A.; Hewidy, I.M.; Ezzat, M.; Aboelnour, N.H. Efficacy of Extracorporeal Shockwave Therapy on Cervical Myofascial Pain Following Neck Dissection Surgery: A Randomized Controlled Trial. Ann. Rehabil. Med. 2020, 44, 393–401. [Google Scholar] [CrossRef]
- Moghtaderi, A.; Khosrawi, S.; Dehghan, F. Extracorporeal shock wave therapy of gastroc-soleus trigger points in patients with plantar fasciitis: A randomized, placebo-controlled trial. Adv. Biomed. Res. 2014, 3, 99. [Google Scholar] [CrossRef]
- Hong, J.O.; Park, J.S.; Jeon, D.G.; Yoon, W.H.; Park, J.H. Extracorporeal Shock Wave Therapy Versus Trigger Point Injection in the Treatment of Myofascial Pain Syndrome in the Quadratus Lumborum. Ann. Rehabil. Med. 2017, 41, 582–588. [Google Scholar] [CrossRef] [Green Version]
- Yalçın, Ü. Comparison of the effects of extracorporeal shockwave treatment with kinesiological taping treatments added to exercise treatment in myofascial pain syndrome. J. Back Musculoskelet. Rehabil. 2021, 34, 623–630. [Google Scholar] [CrossRef]
- Gerwin, R. Botulinum toxin treatment of myofascial pain: A critical review of the literature. Curr. Pain. Headache Rep. 2012, 16, 413–422. [Google Scholar] [CrossRef]
- Ramon, S.; Gleitz, M.; Hernandez, L.; Romero, L.D. Update on the efficacy of extracorporeal shockwave treatment for myofascial pain syndrome and fibromyalgia. Int J. Surg. 2015, 24, 201–206. [Google Scholar] [CrossRef]
- Travell, J.G.; Simons, D.G. Myofascial Pain Dysfunction the Trigger Point Manual, 2nd ed.; Williams & Wilkins: Baltimore, MD, USA, 1999. [Google Scholar]
- Sarzi-Puttini, P.; Giorgi, V.; Marotto, D.; Atzeni, F. Fibromyalgia: An update on clinical characteristics, aetiopathogenesis and treatment. Nat. Rev. Rheumatol. 2020, 16, 645–660. [Google Scholar] [CrossRef]
- Grayston, R.; Czanner, G.; Elhadd, K.; Goebel, A.; Frank, B.; Üçeyler, N.; Malik, R.A.; Alam, U. A systematic review and meta-analysis of the prevalence of small fiber pathology in fibromyalgia: Implications for a new paradigm in fibromyalgia etiopathogenesis. Semin. Arthritis Rheum. 2019, 48, 933–940. [Google Scholar] [CrossRef]
- Sorg, H.; Zwetzich, I.; Tilkorn, D.J.; Kolbenschlag, J.; Hauser, J.; Goertz, O.; Spindler, N.; Langer, S.; Ring, A. Effects of Extracorporeal Shock Waves on Microcirculation and Angiogenesis in the in vivo Wound Model of the Diver Box. Eur. Surg. Res. 2021, 62, 134–143. [Google Scholar] [CrossRef]
- Hausdorf, J.; Lemmens, M.A.; Heck, K.D.; Grolms, N.; Korr, H.; Kertschanska, S.; Steinbusch, H.W.; Schmitz, C.; Maier, M. Selective loss of unmyelinated nerve fibers after extracorporeal shockwave application to the musculoskeletal system. Neuroscience 2008, 155, 138–144. [Google Scholar] [CrossRef]
- Wolfe, F.; Clauw, D.J.; Fitzcharles, M.A.; Goldenberg, D.L.; Häuser, W.; Katz, R.L.; Mease, P.J.; Russell, A.S.; Russell, I.J.; Walitt, B. 2016 Revisions to the 2010/2011 fibromyalgia diagnostic criteria. Semin. Arthritis Rheum. 2016, 46, 319–329. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| (“Extracorporeal Shockwave Therapy”[Mesh] or “High-Energy Shock Waves”[Mesh]) and (“Fibromyalgia”[Mesh] or “Myofascial Pain Syndromes”[Mesh]) |
|---|
| “shockwave” and “myofascial” |
| “shock wave” and “myofascial” |
| “shockwave” and “myofascial pain” |
| “shock wave” and “myofascial pain” |
| “shock wave” and “fibromyalgia” |
| “shockwave” and “fibromyalgia” |
| Inclusion criteria Clinical studies (interventional and observational) about the efficacy and effectiveness of radial or focused ESWT on:
|
Exclusion criteria
|
| Author, Year | Study Design | Site of Application | Sample Size: Total (Group) | Intervention (ESWT Protocol) | Control | Outcomes | Timing | Main Findings |
|---|---|---|---|---|---|---|---|---|
| Taheri et al. 2016 [13] | RCT | Neck, shoulder (upper trapezius) | 46 (26 intervention group, 20 control group) | SW: 1000 pulses EFD: 3 J/m2 and 10 Hz + stretching + not-specified drugs T: once a week for 3 weeks | Laser therapy (Indolaser device, type Ga-AL-As with 6 J/cm2, average power 100 mW, for total of 3 min on each spot for 10 sessions) + stretching + not-specified drugs | pain (VAS 1–10); disability (NDI; SPADI) | T0: baseline T1: at 5 weeks T2: at 7 weeks | Both rESWT and laser therapy proved to be effective in reducing pain and improving disability. Laser therapy showed statistically significant higher benefits at VAS and NDI compared to rESWT only at 5 weeks follow-up. |
| Kiraly et al. 2018 [14] | RCT | Neck, shoulder (upper trapezius) | 61 (30 intervention group vs. 31 control group) | SW: 1000 + 1000 EFD: 1.5 bar and 10 Hz, 0.25 mJ/mm2 aroune the TP, subsequently 2 bar 10 Hz 0.25 mJ/mm2 on TP T: once a week for 3 weeks | Laser therapy (soft laser treatment daily for 15 days with 2000 Hz, 800 mW, 3 J/cm2 for 2 min on palpable trigger points and with 5000 Hz, 2000 mW, 9 J/cm2, for 2 min on trapezius muscles and trigger points | pain (VAS 0–100); disability (NDI); QoL (SF-36) | T0: baseline T1: at 3 weeks T2: at 15 weeks | Both rESWT and laser have proven to effectively improve pain tolerance, neck functionality, and quality of life, but the clinical effectiveness of rESWT was found to be higher. |
| Akturk et al. 2018 [15] | RCT | Neck | 60 (20 rESWT, 20 US, and 20 sham rESWT) | SW: 2000–3000 shock/session, 200–400 shocks/trigger point EFD: 1.6−3.0 bar, 200–400 shocks/trigger point T: maximum 3 min/session, with at most 3-day intervals between sessions for a total of 4 sessions | US treatment for 2 weeks for 5 days a week (10 sessions), each session lasting for 5 min at a dose of 1.5 w/cm2 Sham ESWT same timing as for rESWT group | Pain (pressure pain threshold PPT, pain score, VAS) QoL (SF-36) Hospital anxiety and depression scale (HADS) | T0: Before treatment T1: 2 weeks later the end of treatment T2: 4 weeks after the end of treatment | rESWT is as effective as US. rESWT and US are significantly more effective than sham rESWT in reducing pain and improving QoL but make no difference in HADS. |
| Rahbar et al. 2021 [16] | RCT | Neck, Upper back | 72 (24 rESWT + exercise, 24 US + hot pack + self-stretch-exercises, 24 self-stretch-exercises) | SW: 2000 pulses EFD: 60 mJ/m2 5 Hz T: once a week for 4 weeks | Group 2 US + hot pack + self-stretch-exercises Group 3 self-stretch-exercises | Pain (PPT, VAS) Disability (NDI) | T0: before treatment T1: first week of treatment T2: fourth week of treatment | rESWT and US were equally effective in improving pain and reducing disability and were significantly more effective than control. |
| Gezginaslan et al. 2020 [17] | RCT | Neck and shoulder | 94 (49 rESWT, 45 superficial hot pack + TENS + US) | SW: 1500 to 4500 pulses EFD: 0.26 mJ/mm2. T: Seven sessions with three days interval | Superficial hot pack, TENS, and US were administered five times a week for two weeks. Continuous US at 1 Mhz was applied at a dose of 1.5 watt/cm2 for six minutes daily. TENS was applied for 30 min, and HP was applied 20 min daily. | Pain (VAS) Sleep (Pittsburgh Sleep Quality Index—PSQI) Fatigue (Fatigue Scale) Disability (Functional Assessment of Chronic Illness Therapy—FACIT, NDI) Depression (Beck Depression Inventory—BDI) QoL (SF-36) | T0: before interventions T1: after one month of interventions | rESWT was more effective than a combination of hot packs, TENS, and US in reducing pain and improving sleep quality, disability, depression, and QoL. |
| Taheri et al. 2021 [18] | RCT | Upper trapezius | 37 (18 rESWT, 19 Phonophoresis) | SW: 2000 pulses EFD: 0.2 mj/mm2 with 10 Hz frequency T: three sessions once a week for three weeks | Phonophoresis with hydrocortisone gel 1%, 1 MHz frequency, and 1.2 Wt/cm2 power over the trigger points on the trapezius muscle for 10 min. Three times a week for three weeks | Pain (VAS) Disability (NDI) | T0: before the first Session T1: and one week after the second session | Both phonophoresis and rESWT effectively decreased pain and neck disability with the superiority of rESWT. |
| Walsh et al. 2019 [19] | pilot RCT | Thigh (quadriceps) | 21 (7 rESWT; 7 DN; 7 control group) | SW: 1000 pulses at 20 Hz EFD: up to 5 bars T: 3 sessions per week Surrounding tissue was treated with 2000 pulses at 20 Hz up to 3 bars | DN: acupuncture needle in the most painful TrPs in Vastus Lateralis and Vastus Medialis or control from 30 s to 2 min Control: rest for 7 min in each of the four positions used to measure PPT. | pain (PPT measured with algometer) | T0: baseline T1: at 23–25 days T2: 28 days | rESWT and DN were both effective in reducing pain, but DN can be associated with post-treatment soreness. |
| Luan et al. 2019 [20] | RCT | Neck (upper trapezius) | 65 (32 rESWT; 33 DN) | SW: 2000 pulses EFD: 0.10 mJ/mm2 T: once a week for 3 weeks | DN into MTrPs for 10 s once a week for three weeks | Pain (VAS, PPT) Disability (NDI), and shear wave ultrasound elastography of the upper trapezius MTrPs | T0: baseline T1: 15–30 min after the first treatment T2: 1 month after treatment T3: at 3 months after treatment | rESWT and DN were both effective in reducing pain and disability and in reducing the shear modulus of myofascial trigger points. |
| Manafnezhad et al. 2019 [21] | RCT | Neck (upper trapezius) | 70 (35 rESWT; 35 DN) | SW: 1000 pulses EFD: 60 mj, 16 Hz T: once a week for 3 weeks | DN with fast-in and fast-out needling technique (1–2 min) | Pain (PPT, NPRS) Disability (NDI) | PPT and NPRS (0–10) were assessed before each treatment session and one week after last session; NDI before first treatment and one week after last session | rESWT and DN were equally effective in reducing pain and disability. |
| Eftekharsadat et al. 2020 [22] | RCT | Low Back (quadratus lumborum) | 54 (27 rESWT; 27 corticosteroid trigger point injection—TPI) | SW: 1500 pulses/session EFD: 0.1 mJ/mm2 /min, frequency of 10–16 Hz, and pulse rate of 160/min in total | TPI of 40 mg triamcinolone + 2 mL of lidocaine 2% | Pain (VAS, PPT) Disability (ODI) QoL (SF36) | T0: before interventions T1: after two weeks from treatment T2: after four weeks of treatment | Corticosteroid TPI was more effective than rESWT in reducing pain and disability in the short term. However, rESWT was more effective in reducing pain and disability and improving QoL at 1 month. |
| Li and Wu 2020 [23] | Case-control study | TMJ | 80 (40 rESWT; 40 ultrashort wave—UW) | SW: 1000–1500 pulses EFD: 8 Hz frequency T: once a week for four weeks | UW was applied by placing the electrodes 2 to 3 cm to the mandibular joint, and each treatment lasted 15 min once a day for 5 a week for 4 weeks. | Pain (VAS); Pain-free maximum mouth opening (MMO); Friction index: mandibular movement (MM), joint noise (JN), joint press (JP), and disability index (DI).) | T0: before the treatment T1: four weeks after therapy | rESWT was more effective than UW in reducing pain and improving functional indexes of temporomandibular joint and mouth. |
| Sugawara et al. 2021 [24] | Retrospective study | MPS or AP | 1580 | According to clinician experience (1983 ± 406.5 pulses/session, 14.00 ± 2.05 Hz and 2.5 ± 0.5 bar) for two sessions | None | Pain (VAS) | T0: before the first Session T1: and one week after the second session | rESWT decreased pain above all in patients with intense myofascial pain (VAS > 70 mm). |
| Author, Year | Study Design | Site of Application | Sample Size: Total (Group) | Intervention (ESWT Protocol) | Control | Outcomes | Timing | Main Findings |
|---|---|---|---|---|---|---|---|---|
| Jeon et al. 2012 [25] | RCT | Neck (trapezius) | 30 (15 × 2 groups) | SW: 1500 pulses EFD: 0.10 mJ/mm2 T: once a week for 3 weeks | TPI treatments and 5 TENS treatments were given 5 times a week with a duration of 20 min a day. | Pain (VAS, PRS, MPQ) Neck ROM | T0: before first therapy T1: after first therapy T2: after third therapy | No significant between-group differences were found for pain (VAS, MPQ, and PRS) and ROM at 1 week after the first and third treatment. |
| Ji et al. 2012 [26] | RCT | Neck (upper trapezius) | 20 (9 fESWT groups vs. 11 in the control group) | SW: 1000 pulses EFD: 0.056 mJ/mm2 T: twice a week for 4 sessions | Ineffective ESWT (0.001 mJ/mm2). | pain (VAS, PPT); | T0: baseline T1: right after fourth treatment | Intervention significantly reduced pain (VAS) and increased PPT compared to control group. |
| Park et al. 2018 [27] | RCT | Neck (upper trapezius) | 30 (15 × 2 groups) | SW: 1500 pulses EFD: 0.210 mJ/mm2 T: once a week for 2 weeks | SW: 1500 pulses EFD: 0.068 mJ/mm2 T: once a week for 2 weeks | Pain (VNS, pain threshold) Disability (NDI) Neck ROM | T0: before treatment T1: after treatment | High-energy ESWT was more effective than low-energy ESWT in improving NDI score and neck flexion ROM at 2-week follow-up |
| Kamel et al. 2020 [28] | RCT | Neck (upper trapezius) | 46 (23 × 2 groups) | SW: 1000 pulses EFD: 0.25 mL/mm2 T: once a week for 4 weeks + Topical 1% diclofenac gel (3 times/day for 4 weeks) | Only topical 1% diclofenac gel (3 times/day for 4 weeks) | Pain (VAS, PPT) Neck ROM | T0: baseline T1: after 2 weeks from treatment T2: after 4 weeks from treatment | Intervention showed a significant improvement in pain (VAS and PPT) and ROM (lateral bending and rotation bilaterally) compared to control group in patients with MPS after neck dissection surgery at 4 weeks. |
| Moghtaderi et al. 2014 [29] | RCT | Gastrocnemius–soleus; heel region | 40 (20 × 2 groups) | SW: 3000 + 400 each trigger point EFD: 0.2 mJ/mm2 T: three sessions every week | SW: 3000 pulses EFD: 0.2 mJ/mm2 on heel region T: three sessions every week | Pain (VAS) Disability (Roles and Maudsley score, RM) | T0: baseline T1: eight weeks after treatment | Intervention was more effective than control for improvement of pain and activity (VAS and modified RM score) at 8 weeks follow-up |
| Hong et al. 2017 [30] | Retrospective study | Quadratus lumborum | 30 (15 × 2 groups) | SW: 2000 pulses EFD: 0.085–0.148 mJ/mm2 T: three times at 3-day interval | TPI three times at the tender point at 3-day intervals | Pain (VAS, PPT) Disability (ODI, Roles and Maudsley RM, Quebec Back Pain Disability Scale QBS) | T0: before the initial treatment T1:immediately after the third treatment T2: 1 month after treatment | Intervention was more effective than control for pain reduction (VAS and PPT) immediately after treatment and at 1-month follow-up; no statistically significant between-group differences were found for disability indexes (ODI, RM score, QBS). |
| Ümit Yalçın 2021 [31] | Retrospective study | Neck (upper trapezius) | 262 (75 ESWT exercise group, 82 KT + exercise group, 105 exercise group) | SW:1500 pulses EFD: 0.056 mJ/mm2 T: three sessions every week | X-shaped KT (2 bands of 7.5 cm long I tape glued one after the other, crossing each other) applied every four days for a total three times in twelve days by the same physician | Pain (PPT, VAS) Disability (NDI) Neck ROM | T0: baseline T1: after three months from treatment | Intervention was significantly more effective than KT and control in reducing pain and increasing PPT, NDI score and controlateral lateral flexion |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Paoletta, M.; Moretti, A.; Liguori, S.; Toro, G.; Gimigliano, F.; Iolascon, G. Efficacy and Effectiveness of Extracorporeal Shockwave Therapy in Patients with Myofascial Pain or Fibromyalgia: A Scoping Review. Medicina 2022, 58, 1014. https://doi.org/10.3390/medicina58081014
Paoletta M, Moretti A, Liguori S, Toro G, Gimigliano F, Iolascon G. Efficacy and Effectiveness of Extracorporeal Shockwave Therapy in Patients with Myofascial Pain or Fibromyalgia: A Scoping Review. Medicina. 2022; 58(8):1014. https://doi.org/10.3390/medicina58081014
Chicago/Turabian StylePaoletta, Marco, Antimo Moretti, Sara Liguori, Giuseppe Toro, Francesca Gimigliano, and Giovanni Iolascon. 2022. "Efficacy and Effectiveness of Extracorporeal Shockwave Therapy in Patients with Myofascial Pain or Fibromyalgia: A Scoping Review" Medicina 58, no. 8: 1014. https://doi.org/10.3390/medicina58081014
APA StylePaoletta, M., Moretti, A., Liguori, S., Toro, G., Gimigliano, F., & Iolascon, G. (2022). Efficacy and Effectiveness of Extracorporeal Shockwave Therapy in Patients with Myofascial Pain or Fibromyalgia: A Scoping Review. Medicina, 58(8), 1014. https://doi.org/10.3390/medicina58081014