
Impact of Anticoagulants in Reducing Mortality and Disability in Cardioembolic Stroke Patients

 , and
, and
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Patient Characteristics
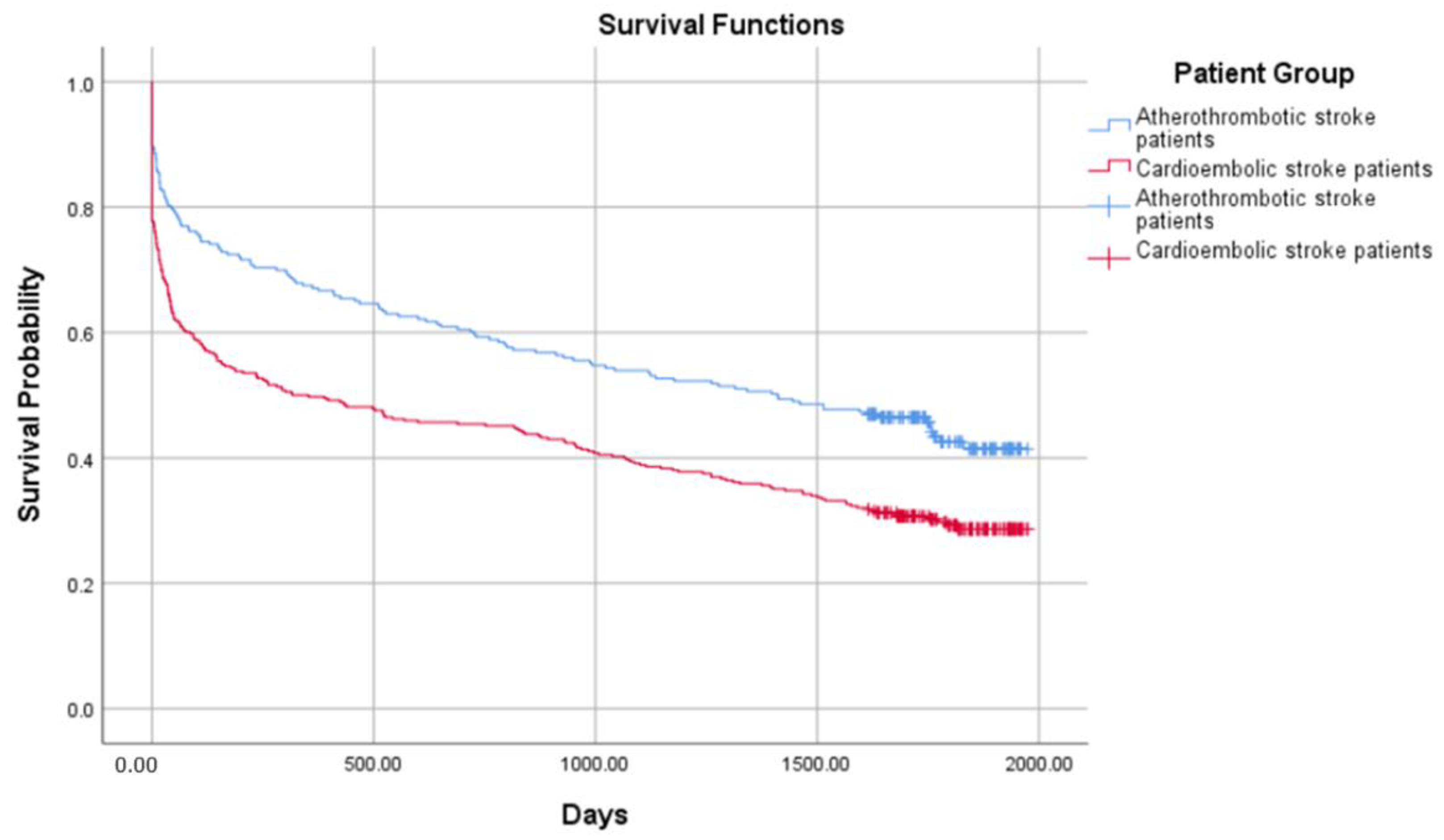
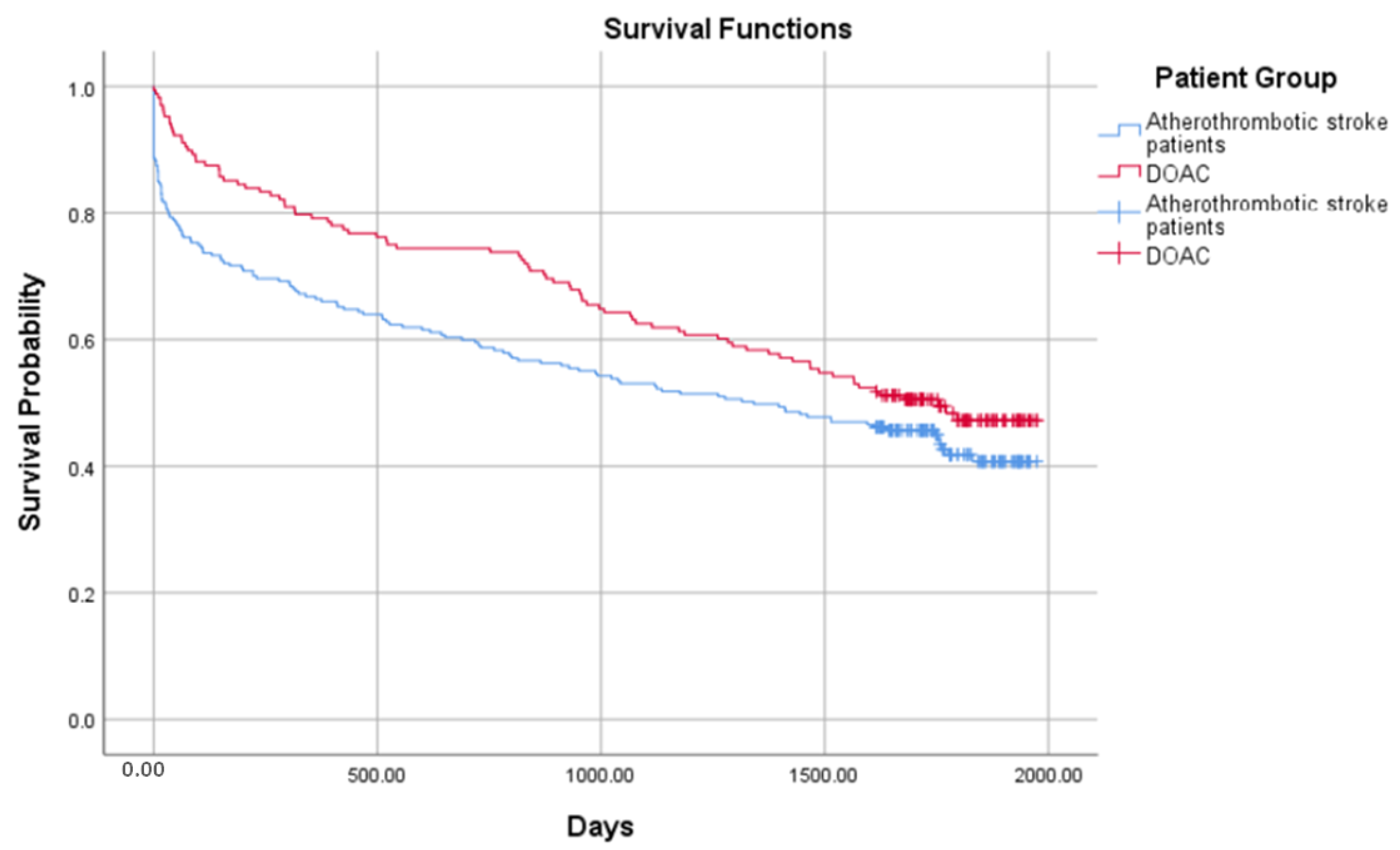
3.2. Survival Analysis
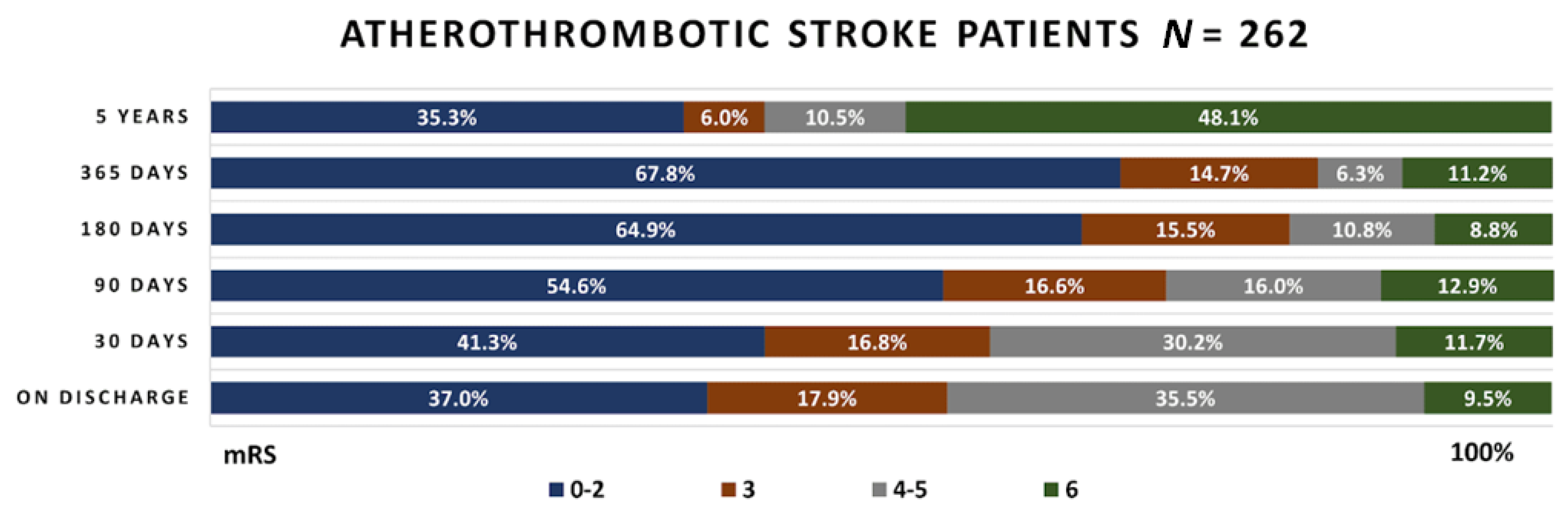
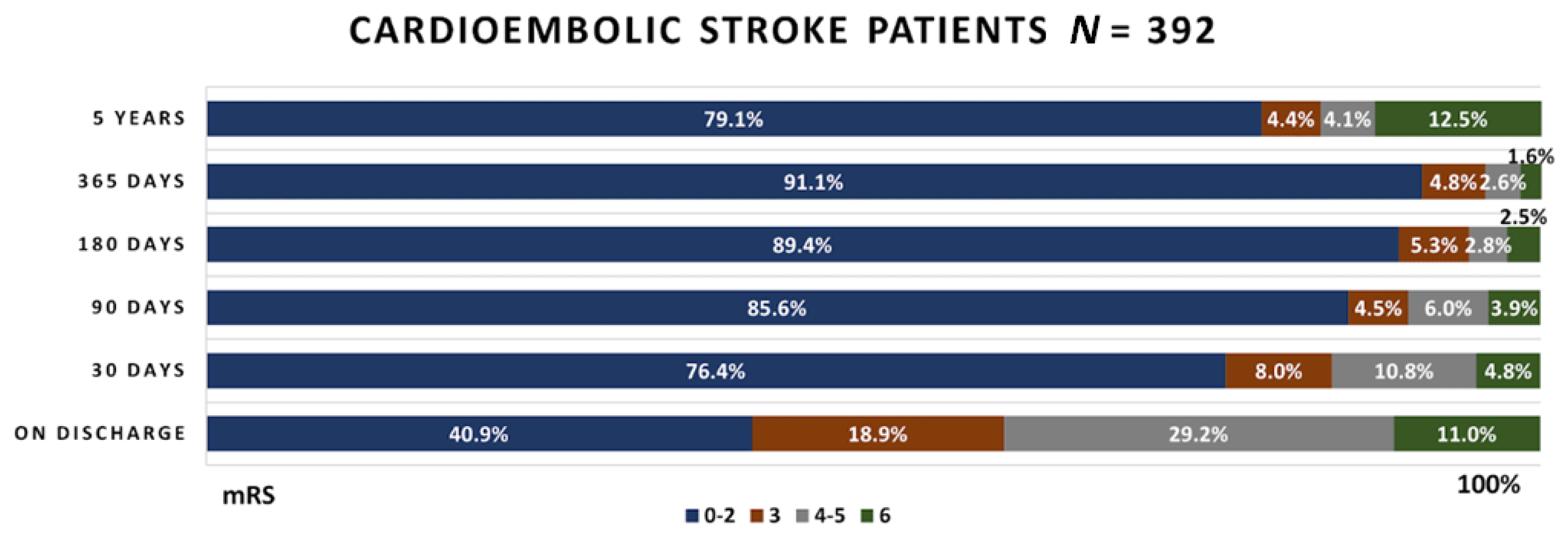
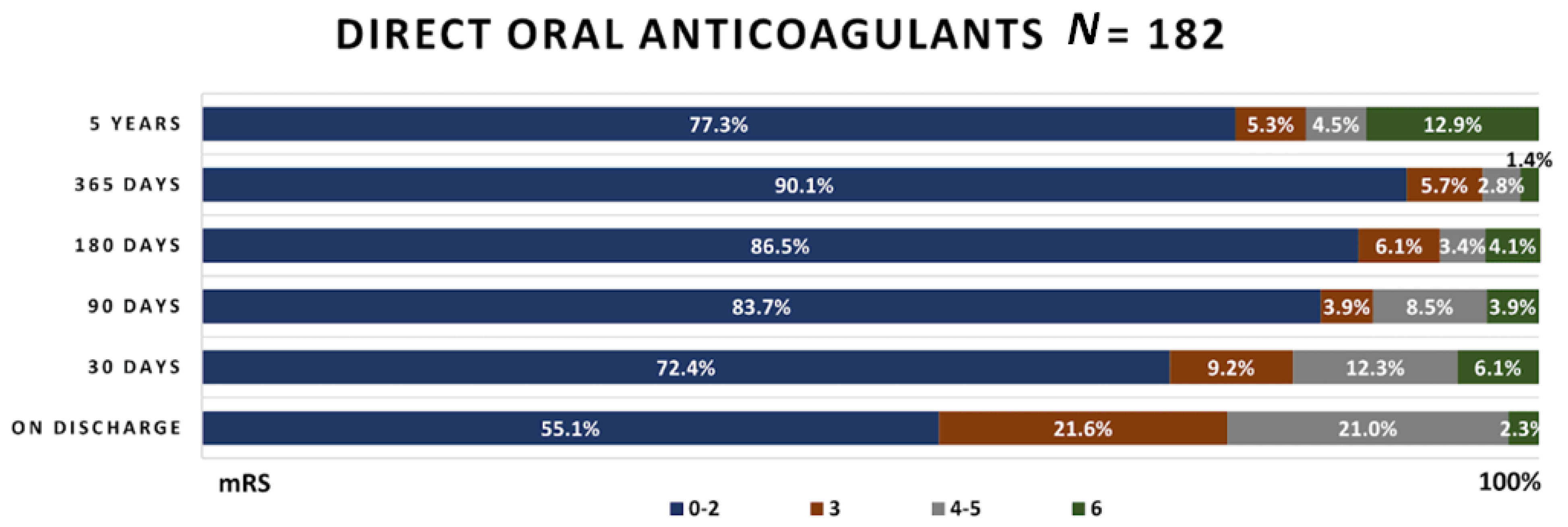
3.3. Functional Outcome Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- GBD 2015 Mortality and Causes of Death Collaborators. Global, regional, and national life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016, 388, 1459–1544, Erratum in Lancet 2017, 389, e1. [Google Scholar] [CrossRef]
- Arboix, A.; Alioc, J. Cardioembolic Stroke: Clinical Features, Specific Cardiac Disorders and Prognosis. Curr. Cardiol. Rev. 2010, 6, 150–161. [Google Scholar] [CrossRef]
- Ferro, J.M. Brain embolism—Answers to practical questions. J. Neurol. 2003, 250, 139–147. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.-H.; Park, K.-Y.; Shin, J.-H.; Cha, J.-K.; Kim, H.-Y.; Kwon, J.-H.; Oh, H.G.; Lee, K.B.; Kim, D.-E.; Ha, S.-W.; et al. Symptomatic Hemorrhagic Transformation and Its Predictors in Acute Ischemic Stroke with Atrial Fibrillation. Eur. Neurol. 2010, 64, 193–200. [Google Scholar] [CrossRef]
- Zhang, J.; Yang, Y.; Sun, H.; Xing, Y. Hemorrhagic transformation after cerebral infarction: Current concepts and challenges. Ann. Transl. Med. 2014, 2, 81. [Google Scholar] [CrossRef]
- Bogousslavsky, J.; Regli, F.; Uské, A.; Maeder, P. Early spontaneous hematoma in cerebral infarct: Is primary cerebral hemorrhage overdiagnosed? Neurology 1991, 41, 837. [Google Scholar] [CrossRef] [PubMed]
- Masiliūnas, R.; Dapkutė, A.; Grigaitė, J.; Lapė, J.; Valančius, D.; Bacevičius, J.; Katkus, R.; Vilionskis, A.; Klimašauskienė, A.; Ekkert, A.; et al. High Prevalence of Atrial Fibrillation in a Lithuanian Stroke Patient Cohort. Medicina 2022, 58, 800. [Google Scholar] [CrossRef] [PubMed]
- Jurjans, K.; Vikmane, B.; Vetra, J.; Miglane, E.; Kalejs, O.; Priede, Z.; Millers, A. Is Anticoagulation Necessary for Severely Disabled Cardioembolic Stroke Survivors? Medicina 2019, 55, 586. [Google Scholar] [CrossRef]
- Mihejeva, I.; Vetra, A.; Bērziņa, G. Factors associated with long-term mortality for stroke unit patients in Latvia. Brain Behav. 2018, 8, e01152. [Google Scholar] [CrossRef]
- Jurjāns, K.; Noviks, I.; Volčeka, D.; Zandersone, L.; Meilerte, K.; Miglāne, E.; Stepens, A.; Millers, A. The adaption and evaluation of a Latvian version of the National Institutes of Health Stroke Scale. J. Int. Med. Res. 2017, 45, 1861–1869. [Google Scholar] [CrossRef]
- Patel, R.D.; Starkman, S.; Hamilton, S.; Craig, S.; Grace, A.; Conwit, R.; Saver, J.L. The Rankin Focused Assessment-Ambulation: A Method to Score the Modified Rankin Scale with Emphasis on Walking Ability. J. Stroke Cereb. Dis. 2016, 25, 2172–2176. [Google Scholar] [CrossRef] [PubMed]
- Sulter, G.; Steen, C.; De Keyser, J. Use of the Barthel Index and Modified Rankin Scale in Acute Stroke Trials. Stroke 1999, 30, 1538–1541. [Google Scholar] [CrossRef] [PubMed]
- Adams, H.P., Jr.; Bendixen, B.H.; Kappelle, L.J.; Biller, J.; Love, B.B.; Gordon, D.L.; Marsh, E.E., 3rd. Classification of subtype of acute ischemic stroke. Definitions for use in a multicenter clinical trial. TOAST. Trial of Org 10172 in Acute Stroke Treatment. Stroke 1993, 24, 35–41. [Google Scholar] [CrossRef] [PubMed]
- Malek, E.G.; Elbejjani, M.; Abbas, R.; Al Ahad, M.A.; Isma’Eel, H.; Makki, A. TOAST classification and risk factors of ischemic stroke in Lebanon. Acta Neurol. Scand. 2020, 141, 294–300. [Google Scholar] [CrossRef]
- Spence, J.D. Cardioembolic stroke: Everything has changed. Stroke Vasc. Neurol. 2018, 3, 76–83. [Google Scholar] [CrossRef]
- Karelis, G.; Micule, M.; Klavina, E.; Haritoncenko, I.; Kikule, I.; Tilgale, B.; Polaka, I. The Riga East University Hospital Stroke Registry—An Analysis of 4915 Consecutive Patients with Acute Stroke. Medicina 2021, 57, 632. [Google Scholar] [CrossRef]
- Guglielmi, V.; LeCouffe, N.E.; Zinkstok, S.M.; Compagne, K.C.; Eker, R.; Treurniet, K.M.; Tolhuisen, M.L.; van der Worp, H.B.; Jansen, I.G.; van Oostenbrugge, R.J.; et al. Collateral Circulation and Outcome in Atherosclerotic Versus Cardioembolic Cerebral Large Vessel Occlusion. Stroke 2019, 50, 3360–3368. [Google Scholar] [CrossRef]
- Griñán, K.; Arboix, A.; Massons, J.; Díez, L.; Vergés, E.; Gil, F.; Arboix-Alió, J.; Sánchez-López, M.J.; García-Eroles, L. Cardioembolic Stroke: Risk Factors, Clinical Features, and Early Outcome in 956 Consecutive Patients. Rev. Investg. Clin. 2020, 73, 023–030. [Google Scholar] [CrossRef]
- Lawrence, M.; Pringle, J.; Kerr, S.; Booth, J.; Govan, L.; Roberts, N.J. Multimodal Secondary Prevention Behavioral Interventions for TIA and Stroke: A Systematic Review and Meta-Analysis. PLoS ONE 2015, 10, e0120902. [Google Scholar] [CrossRef]
- Kim, J.-T.; Park, M.-S.; Choi, K.-H.; Cho, K.-H.; Kim, B.J.; Han, M.-K.; Park, T.H.; Park, S.-S.; Lee, K.B.; Lee, B.-C.; et al. Different Antiplatelet Strategies in Patients With New Ischemic Stroke While Taking Aspirin. Stroke 2016, 47, 128–134. [Google Scholar] [CrossRef]
- Halkes, P.H.; Van Gijn, J.; Kappelle, L.J.; Koudstaal, P.J.; Algra, A. Classification of Cause of Death After Stroke in Clinical Research. Stroke 2006, 37, 1521–1524. [Google Scholar] [CrossRef] [PubMed]
- Beume, L.-A.; Hieber, M.; Kaller, C.P.; Nitschke, K.; Bardutzky, J.; Urbach, H.; Weiller, C.; Rijntjes, M. Large Vessel Occlusion in Acute Stroke. Stroke 2018, 49, 2323–2329. [Google Scholar] [CrossRef] [PubMed]
- Stueckelschweiger, L.; Tiedt, S.; Puhr-Westerheide, D.; Fabritius, M.P.; Mueller, F.; Kellert, L.; Maurus, S.; Grosu, S.; Rueckel, J.; Herzberg, M.; et al. Decomposing Acute Symptom Severity in Large Vessel Occlusion Stroke: Association With Multiparametric CT Imaging and Clinical Parameters. Front. Neurol. 2021, 12, 651387. [Google Scholar] [CrossRef] [PubMed]
- Zigure, I.; Tomilova, A.; Kikule, I.; Karelis, G. Oral anticoagulant use among patients hospitalized with stroke in riga east clinical university hospital. Neurol. Semin. 2018, 22, 280–281. [Google Scholar]
- Xu, T.; Zhang, J.T.; Yang, M.; Zhang, H.; Liu, W.Q.; Kong, Y.; Xu, T.; Zhang, Y.H. Dyslipidemia and outcome in patients with acute ischemic stroke. Biomed. Environ. Sci. 2014, 27, 106–110. [Google Scholar] [CrossRef]
- Khan, R.S.U.; Nawaz, M.; Khan, S.; Raza, H.A.; Nazir, T.; Anwar, M.S.; Nadeem, H.M.F.; Rehman, Z.U.; Akram, A. Prevalence of Dyslipidemia in Ischemic Stroke Patients: A Single-Center Prospective Study From Pakistan. Cureus 2022, 14, e25880. [Google Scholar] [CrossRef]
- Sohail, A.; Khatri, I.A.; Mehboob, N. Effect of dyslipidemia on severity and outcome of stroke using mRS scores in Northern Pakistani population. Rawal Med. J. 2013, 38, 345–350. [Google Scholar]
- Bowman, T.S.; Sesso, H.D.; Ma, J.; Kurth, T.; Kase, C.S.; Stampfer, M.J.; Gaziano, J.M. Cholesterol and the Risk of Ischemic Stroke. Stroke 2003, 34, 2930–2934. [Google Scholar] [CrossRef]
- Chavda, V.; Chaurasia, B.; Fiorindi, A.; Umana, G.E.; Lu, B.; Montemurro, N. Ischemic Stroke and SARS-CoV-2 Infection: The Bidirectional Pathology and Risk Morbidities. Neurol. Int. 2022, 14, 391–405. [Google Scholar] [CrossRef]
- Martí, M.G.; Boschín, V.; Puchades, F.; Cerdán, A.; Cunquero, A.; Sanz, F.; Tamarit, J.J. Ictus isquémico por oclusión de la arteria basilar en una paciente puérpera con infección por SARS-CoV-2 [Ischaemic stroke due to basilar artery occlusion in a puerperal patient with SARS-CoV-2 infection]. Rev Neurol. 2022, 75, 97–100. (In Spanish) [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Antithrombotic Therapy | Atherothrombotic Stroke Group 40.1% (N = 262) | Cardioembolic Stroke Group 59.9% (N = 392) | DOAC Group 27.8% (N = 182) | p (between Atherothrombotic and Cardioembolic Stroke Groups) | p (between Atherothrombotic Stroke Group and DOAC Group) |
|---|---|---|---|---|---|
| IVT | 16.8% (n = 44) | 17.6% (n = 69) | 25.3% (n = 46) | 0.103 | 0.001 |
| EVT | 1.1% (n = 3) | 3.3% (n = 13) | 4.4% (n = 8) | ||
| IVT + EVT | 4.6% (n = 12) | 7.7% (n = 30) | 9.3% (n = 17) |
| Atherothrombotic Stroke Group 40.1% (N = 262) | Cardioembolic Stroke Group 59.9% (N = 392) | DOAC Group 27.8% (N = 182) | p (between Atherothrombotic and Cardioembolic Stroke Groups) | p (between Atherothrombotic Stroke Group and DOAC Group) | |
|---|---|---|---|---|---|
| Average age (IQR) | 71 (64–79) | 79 (72–84) | 75 (69–82) | <0.01 | <0.001 |
| Coronary heart disease | 14.8% (n = 35) | 16.9% (n = 36) | 17.0% (n = 31) | 0.809 | 0.497 |
| Congestive heart failure | 24.8% (n = 59) | 41.8% (n = 89) | 42.3% (n = 77) | 0.001 | <0.001 |
| Prior myocardial infarction | 8% (n = 20) | 12% (n = 45) | 13% (n = 13%) | 0.107 | 0.05 |
| Arterial hypertension | 84.9% (n = 202) | 83.1% (n = 177) | 82.4% (n = 150) | 0.706 | 0.616 |
| Dyslipidemia | 54.6% (n = 143) | 26.5% (n = 104) | 47.8% (n = 87) | 0.407 | 0.031 |
| Recurrent stroke or TIA | 28.2% (n = 67) | 25.4% (n = 54) | 25.3% (n = 46) | <0.001 | <0.001 |
| Diabetes mellitus | 23.1% (n = 55) | 14.1% (n = 30) | 15.4% (n = 28) | 0.084 | 0.114 |
| Chronic kidney disease | 3% (n = 7) | 6% (n = 22) | 4% (n = 8) | 0.73 | 0.308 |
| Smoking | 8% (n = 20) | 1% (n = 4) | 1% (n = 2) | <0.001 | 0.002 |
| NIHSS-LV on admission (IQR) | 6 (4–10) | 8 (4–15) | 7 (3–13) | 0.379 | 0.698 |
| NIHSS-LV at discharge (IQR) | 3 (2–6) | 3 (2–9) | 3 (1–5) | 0.004 | 0.009 |
| Atherothrombotic Stroke vs. Cardioembolic Stroke | Atherothrombotic Stroke vs. Patients Taking DOAC | |||
|---|---|---|---|---|
| Cofactor | Hazard Ratio | p Value | Hazard Ratio | p Value |
| Age | 1.059 | <0.001 | 1.045 | <0.001 |
| Reperfusion therapy | 0.844 | 0.1 | 0.540 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jurjāns, K.; Cērpa, M.; Baborikina, A.; Kalējs, O.; Miglāne, E. Impact of Anticoagulants in Reducing Mortality and Disability in Cardioembolic Stroke Patients. Medicina 2022, 58, 1323. https://doi.org/10.3390/medicina58101323
Jurjāns K, Cērpa M, Baborikina A, Kalējs O, Miglāne E. Impact of Anticoagulants in Reducing Mortality and Disability in Cardioembolic Stroke Patients. Medicina. 2022; 58(10):1323. https://doi.org/10.3390/medicina58101323
Chicago/Turabian StyleJurjāns, Kristaps, Marija Cērpa, Alise Baborikina, Oskars Kalējs, and Evija Miglāne. 2022. "Impact of Anticoagulants in Reducing Mortality and Disability in Cardioembolic Stroke Patients" Medicina 58, no. 10: 1323. https://doi.org/10.3390/medicina58101323
APA StyleJurjāns, K., Cērpa, M., Baborikina, A., Kalējs, O., & Miglāne, E. (2022). Impact of Anticoagulants in Reducing Mortality and Disability in Cardioembolic Stroke Patients. Medicina, 58(10), 1323. https://doi.org/10.3390/medicina58101323