

Neural Basis of Etiopathogenesis and Treatment of Cervicogenic Orofacial Pain


Abstract
1. Introduction
2. Data Collection and Analysis
3. Epidemiology
4. Clinical Anatomy of Cervico-Cranial Junction
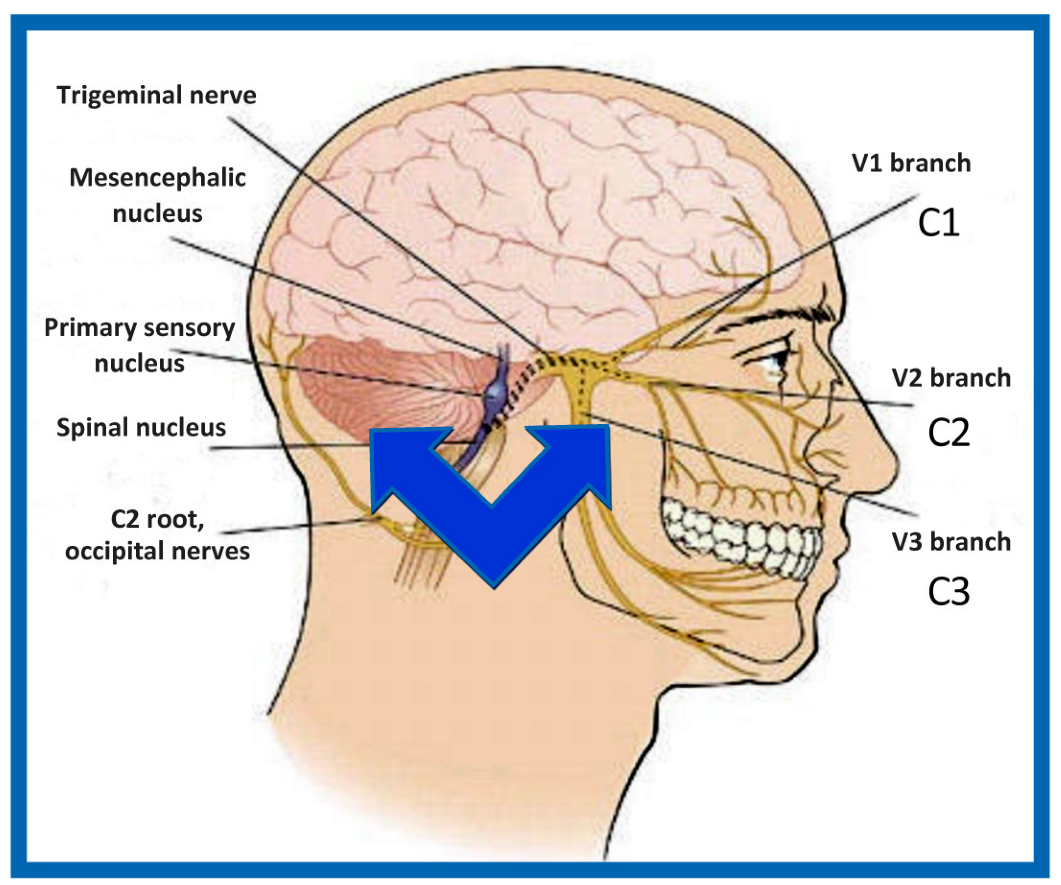
4.1. Spinal Nerves
4.2. Spinal System and Trigeminocervical Convergence
4.2.1. Trigeminocervical Nucleus
4.2.2. Pontine Trigeminal Nucleus
4.2.3. Mesencephalic Nucleus
4.2.4. Motor Trigeminal Nucleus
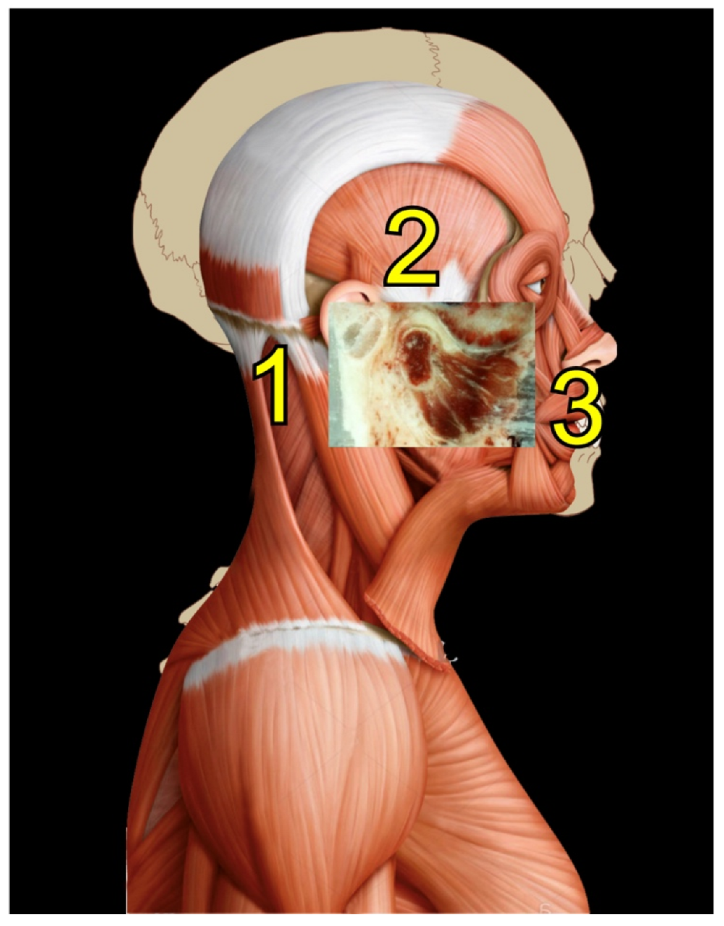
4.3. Temporomandibular Joint
Temporomandibular Function
5. Integrative Function of the Cervico-Cranial Complex
6. Novel Concepts of Functional Synthesis of Cervico-Cranial Interactions
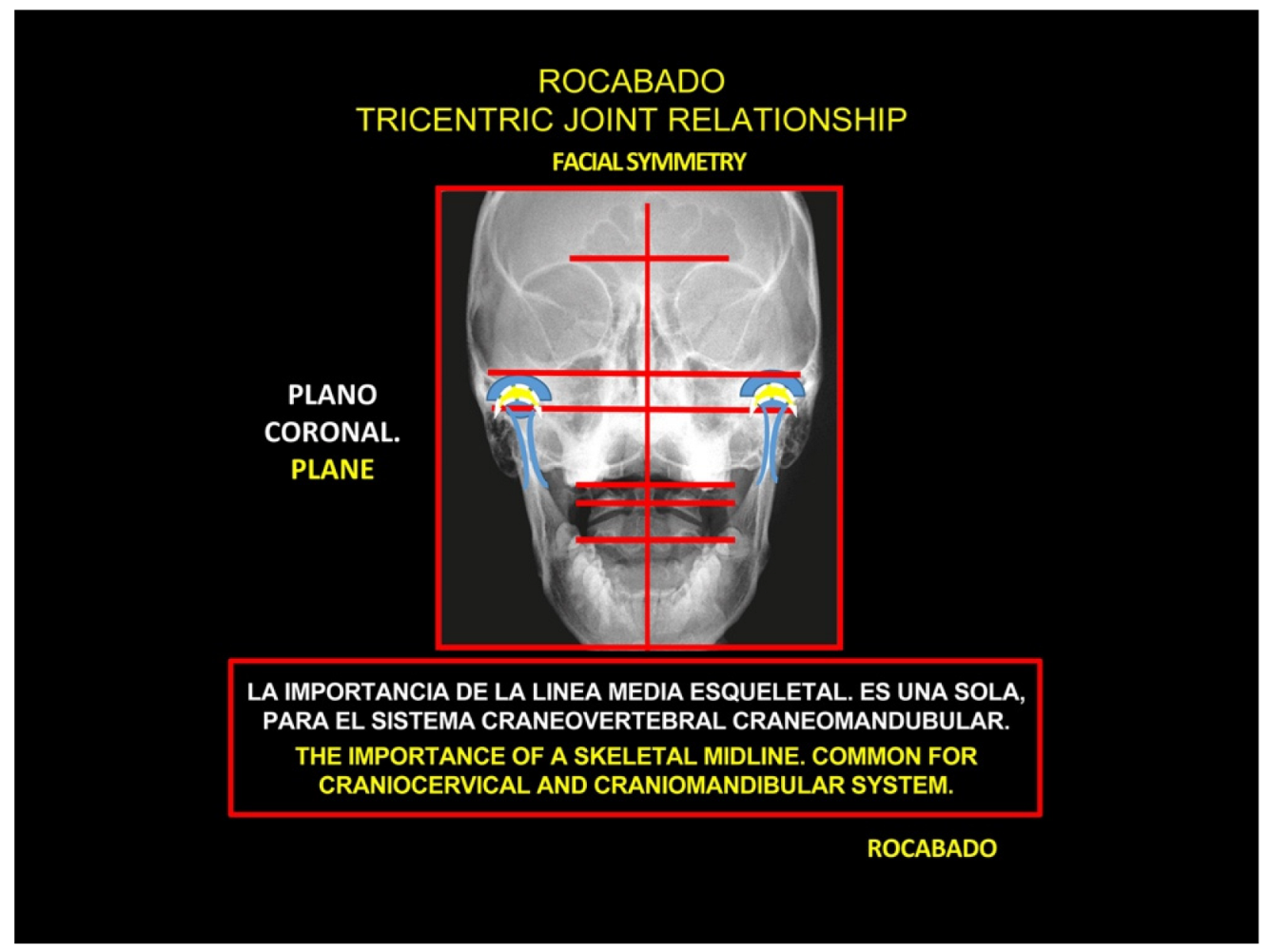
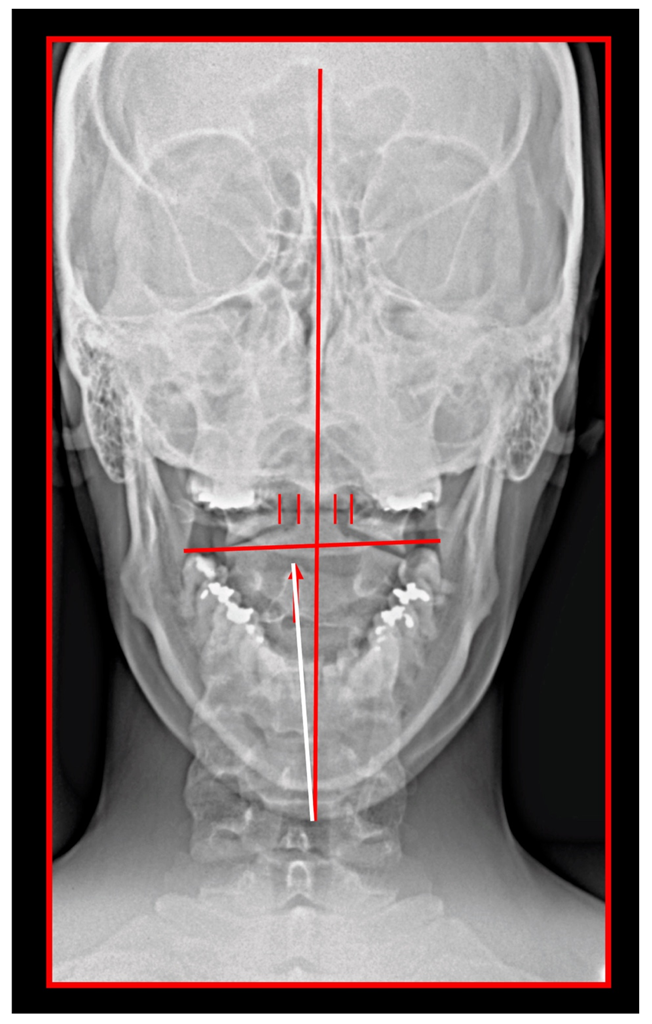
6.1. Rocabado Tricentric Concept of Mouth Sensorimotor Control
The Importance of the Skeletal Midline
6.2. Concept of Cervical Origin of Bruxism
7. Clinical Syndromes in Cervicogenic Orofacial Pain
7.1. Cervical Spondylosis
7.2. Occipital Neuralgia
7.3. Ponticulus Posticus Syndrome
7.4. Triggered Pain
7.5. Atypical Facial (Oro-Facial) Pain
7.6. Pain Due to Iatrogenic Causes
8. Diagnosis of Cervicogenic Orofacial Pain
8.1. Diagnostic Criteria
8.2. Importance of Prompt and Accurate Diagosis
8.3. Local Anesthetic Blockade as a Diagnostic Tool
9. Differential Diagnosis
9.1. Dissecting Aneurysms
9.2. Lesions of the Posterior Cranial Fossa
9.3. Migraine
9.4. Neck-Tongue Syndrome
9.5. Miscellaneous
10. Diagnostic Use of Imaging Techniques
10.1. Neck X-ray
10.2. Computed Tomography of Cervical Spine
10.3. Magnetic Resonance Imaging of Cervical Spine
10.4. Sonography of Cervical Area
11. Treatment
11.1. Conservative Treatment
11.2. Orthopedic Manual Therapy
11.3. Correction of Body Posture to Address TMJ Dysfunction
11.4. Treatments Based of Concepts of Trigeminal-Cervical Convergence
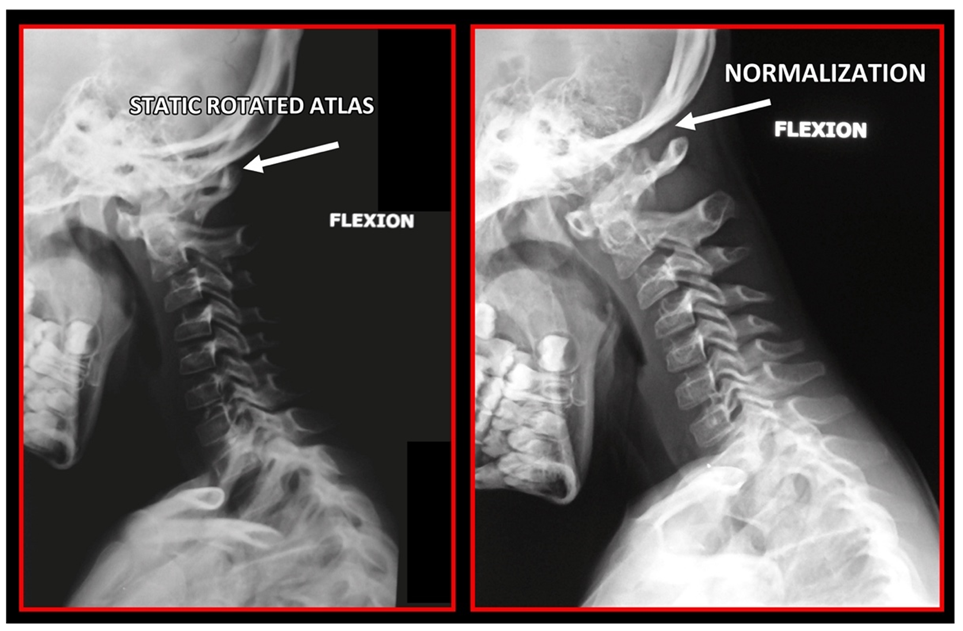
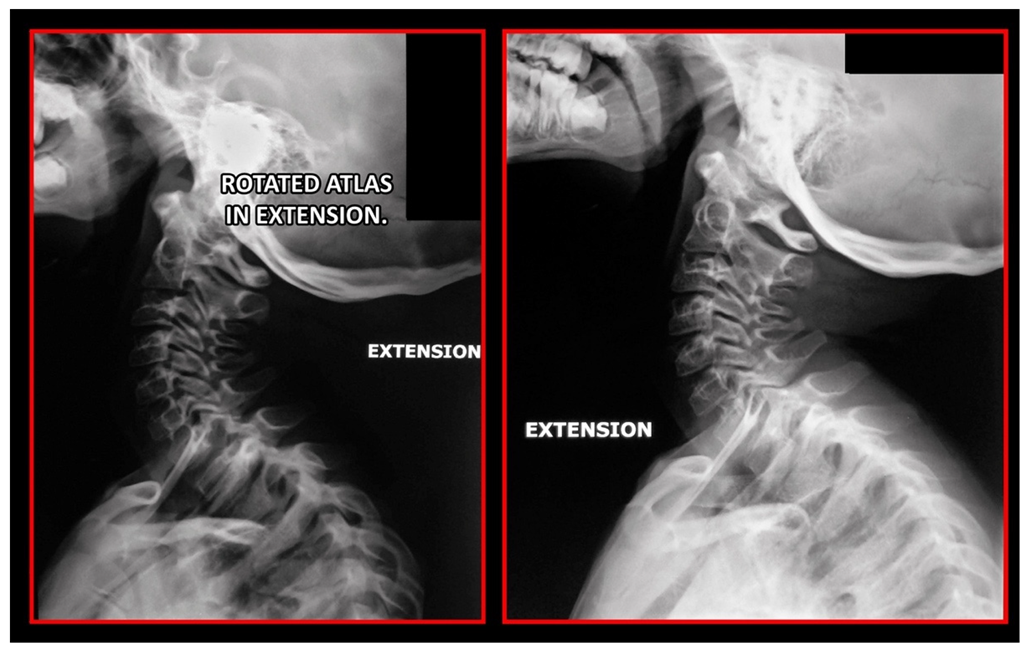
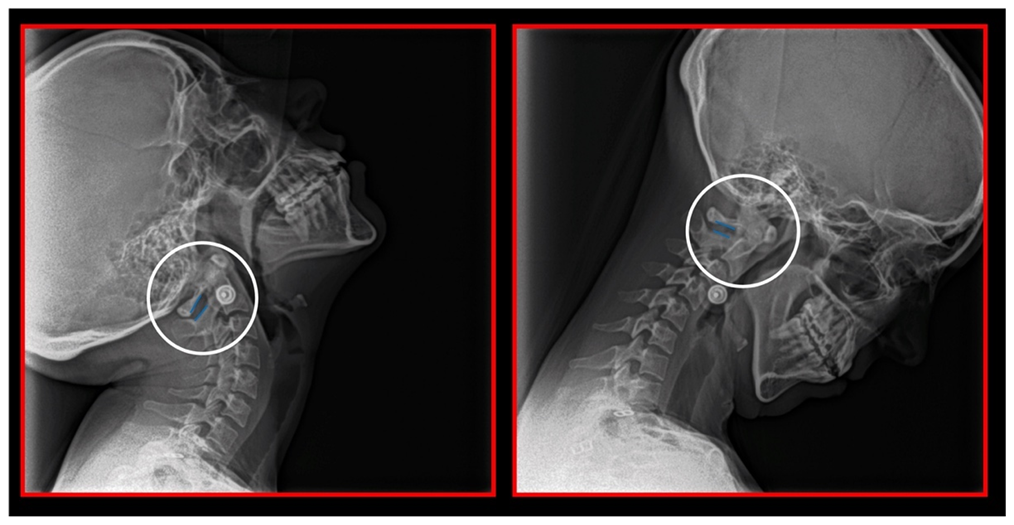
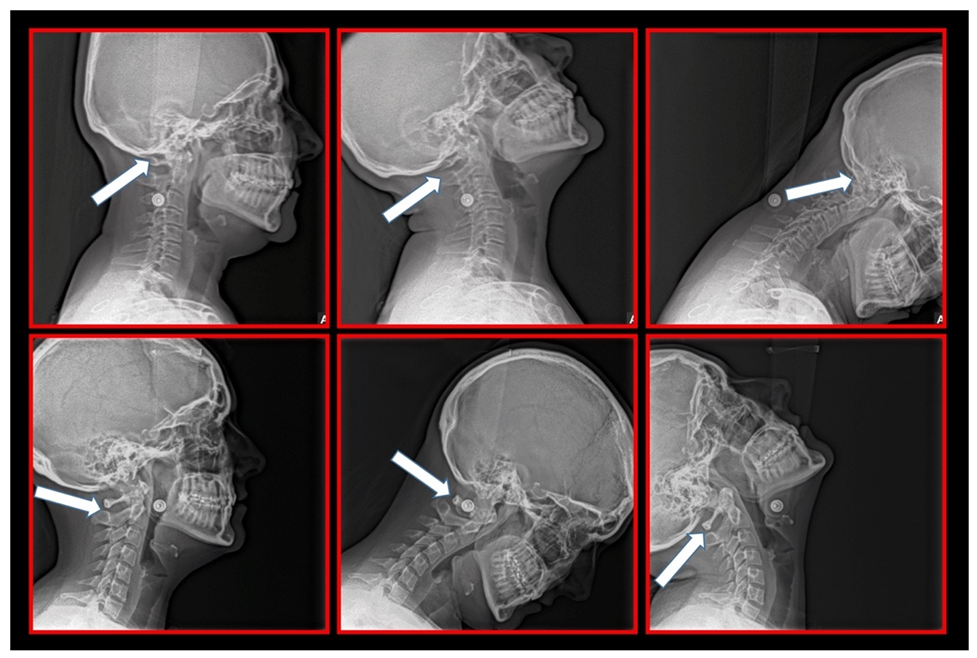
11.5. Axis and Atlas Derotation
11.6. Treatments Focused on Temporomandibular Joint
11.7. Treatment of Occlusion
11.8. Other Therapeutic Modalities
12. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Verma, S.; Tripathi, M.; Chandra, P.S. Cervicogenic Headache: Current Perspectives. Neurol. India. 2021, 69, 194–198. [Google Scholar]
- Van Suijlekom, H.A.; Lamé, I.; Stomp-van den Berg, S.G.; Kessels, A.G.; Weber, W.E. Quality of Life of Patients with Cervicogenic Headache: A Comparison with Control Subjects and Patients With Migraine or Tension-Type Headache. Headache 2003, 43, 1034–1041. [Google Scholar] [CrossRef] [PubMed]
- Fernandez, M.; Moore, C.; Tan, J.; Lian, D.; Nguyen, J.; Bacon, A.; Christie, B.; Shen, I.; Waldie, T.; Simonet, D.; et al. Spinal manipulation for the management of cervicogenic headache: A systematic review and meta-analysis. Eur. J. Pain. 2020, 24, 1687–1702. [Google Scholar] [CrossRef] [PubMed]
- Bogduk, N. The anatomical basis for cervicogenic headache. J. Manipulative Physiol. Ther. 1992, 15, 67–70. [Google Scholar] [PubMed]
- Bogduk, N.; Govind, J. Cervicogenic headache: An assessment of the evidence on clinical diagnosis, invasive tests, and treatment. Lancet Neurol. 2009, 8, 959–968. [Google Scholar] [CrossRef]
- Bogduk, N. The neck and headaches. Neurol. Clin. 2014, 32, 471–487. [Google Scholar] [CrossRef]
- Headache Classification Subcommittee of the International Headache Society. The International Classification of Headache Disorders: 2nd edition. Cepthalagia 2004, 24, 9–160. [Google Scholar]
- Headache Classification Subcommittee of the International Headache Society. The International Classification of Headache Disorders 3rd edition (beta version). Cephalgia 2013, 33, 629–808. [Google Scholar] [CrossRef]
- Sjaastad, O.; Fredriksen, T.A.; Pfaffenrath, V. Cervicogenic Headache: Diagnostic Criteria. Headache. J. Head Face Pain 1998, 38, 442–445. [Google Scholar] [CrossRef]
- Barmherzig, R.; Kingston, W. Occipital Neuralgia and Cervicogenic Headache: Diagnosis and Management. Curr. Neurol. Neurosci. Rep. 2019, 19, 20. [Google Scholar] [CrossRef]
- Fredriksen, T.A.; Antonaci, F.; Sjaastad, O. Cervicogenic headache: Too important to be left undiagnosed. J. Headache Pain 2015, 16, 6. [Google Scholar] [CrossRef] [PubMed]
- Sjaastad, O.; Bakkteig, L.S. Prevalence of cervicogenic headache: Vaga study of headach epidemiology. Acta Neurol. Scand. 2008, 38, 442–445. [Google Scholar] [CrossRef] [PubMed]
- Knackstedt, H.; Bansevicius, D.; Aaseth, K.; Grande, R.B.; Lundqvist, C.; Russel, M.B. Cervicogenic headache in the general population: The Akershus study of chronic headache. Cephalalgia 2010, 30, 1468–1476. [Google Scholar] [CrossRef] [PubMed]
- Evers, S. Comparison of cervicogenic headache with migraine. Cephalalgia 2008, 28, 16–17. [Google Scholar] [CrossRef] [PubMed]
- Lord, S.; Barnsley, L.; Wallis, B.; Bogduk, N. Third occipital headache: A prevalence study. J. Neurol. Neurosurg. Psychiatr. 1994, 57, 1187–1190. [Google Scholar] [CrossRef] [PubMed]
- Rocabado, M.; Iglarsh, Z.A. Musculoskeletal Approach to Maxillofacial Pain; J. B. Lippincott Comp.: Philadelphia, PA, USA, 1991. [Google Scholar]
- Dvorak, J.; Penning, L.; Hayek, J.; Panjabi, M.M.; Grob, D.; Zehnder, R. Functional diagnostics of the cervical spine using computer tomography. Neuroradiology 1988, 30, 132–137. [Google Scholar] [CrossRef]
- Williams, P.L.; Bannister, H. Gray’s Anatomy, 38th ed.; Churchill Livingstone: New York, NY, USA, 1995. [Google Scholar]
- Kikuta, S.; Jenkins, S.; Kusukawa, J.; Iwanaga, J.; Loukas, M.; Tubbs, R.S. Ansa cervicalis: A comprehensive review of its anatomy, variations, pathology, and surgical applications. Anat. Cell Biol. 2019, 52, 221–225. [Google Scholar] [CrossRef]
- Moore, K.L.; Dalley, A.F.; Agur, A.M.R. Moore Clinically Oriented Anatomy, 7th ed.; Lippincott Williams & Wilkins: Baltimore, MD, USA, 2014. [Google Scholar]
- Renton, T.; Egbuniwe, O. Pain. Part 2A: Trigeminal Anatomy Related to Pain. Dent. Update 2015, 42, 238–240. [Google Scholar] [CrossRef]
- Lazarov, N.E. Neurobiology of orofacial proprioception. Brain Res. Rev. 2007, 56, 362–383. [Google Scholar] [CrossRef]
- Bogduk, N. Cervicogenic headache: Anatomic basis and pathophysiologic mechanisms. Curr. Pain Head Rep. 2001, 5, 382–386. [Google Scholar] [CrossRef]
- Biondi, D.M. Cervicogenic headache: A review of diagnostic and treatment strategies. J. Am. Osteopath. Assoc. 2005, 105, 16–22. [Google Scholar]
- Biondi, D.M. Noninvasive treatments for headache. Expert. Rev. Neurother. 2005, 5, 355–362. [Google Scholar] [CrossRef] [PubMed]
- Okeson, J.P. Management of Temporomandibular Disorders and Occlusion, 8th ed.; Elsevier: New York, NY, USA, 2020. [Google Scholar]
- Kerr, F.W. Facial, vagal and glossopharyngeal nerves in the cat. Afferent connections. Arch. Neurol. 1962, 6, 264–281. [Google Scholar] [CrossRef] [PubMed]
- Kerr, F.W. The divisional organization of afferent fibres of the trigeminal nerve. Brain 1963, 86, 721–732. [Google Scholar] [CrossRef]
- Cetas, J.S.; Saedi, T.; Burchiel, K.J. Destructive procedures for the treatment of nonmalignant pain: A structured literature review. J. Neurosurg. 2008, 109, 389–404. [Google Scholar] [CrossRef]
- Giovanni, A.; Giorgia, A. The neurophysiological basis of bruxism. Heliyon 2021, 7, e07477. [Google Scholar] [CrossRef]
- Louvi, A.; Yoshida, M.; Grove, E.A. The derivatives of the Wnt3a lineage in the central nervous system. J. Comp. Neurol. 2007, 504, 550–569. [Google Scholar] [CrossRef] [PubMed]
- Lund, J.P. Mastication and its control by the brain stem. Crit. Rev. Oral Biol. Med. 1991, 2, 33–64. [Google Scholar] [CrossRef]
- Cody, F.W.; Lee, R.W.; Taylor, A. A functional analysis of the components of the mesencephalic nucleus of the fifth nerve in the cat. J. Physiol. 1972, 226, 249–261. [Google Scholar] [CrossRef]
- Daunicht, W.J.; Jaworski, E.; Eckmiller, R. Afferent innervation of extraocular muscles in the rat studied by retrograde and anterograde horseradish peroxidase transport. Neurosci. Lett. 1985, 56, 143–148. [Google Scholar] [CrossRef]
- Porter, J.D.; Spencer, R.F. Localization of morphology of cat extraocular muscle afferent neurons identified by retrograde transport of horseradish peroxidase. J. Comp. Neurol. 1982, 204, 56–64. [Google Scholar] [CrossRef] [PubMed]
- Dessem, D.; Luo, P. Jaw–muscle spindle afferent feedback to the cervical spinal cord in the rat. Exp. Brain Res. 1999, 128, 451–459. [Google Scholar] [CrossRef] [PubMed]
- Goodwin, G.M.; Luschei, E.S. Effects of destroying spindle afferents from jaw muscles on mastication in monkeys. J. Neurophysiol. 1974, 37, 967–981. [Google Scholar] [CrossRef] [PubMed]
- Ongerboer de Visser, B.W. Afferent limb of the human jaw reflex: Electrophysiologic and anatomic study. Neurology 1982, 32, 563–566. [Google Scholar] [CrossRef]
- Luschei, E.S. Central projections of the mesencephalic nucleus of the fifth nerve: An autoradiographic study. J. Comp. Neurol. 1987, 263, 137–145. [Google Scholar] [CrossRef]
- Daunton, N.G. Sensory components of bite–force response in the rat. J. Comp. Physiol. Psychol. 1977, 91, 203–220. [Google Scholar] [CrossRef]
- Eichner, K. Über eine Gruppeneinteilung der Lückengebisse für die Prothetik. Dtsch. Zahnärztl. Z. 1955, 10, 1831–1834. [Google Scholar]
- Malet, J. Implant Dentistry at Glance, 1st ed.; Wiley-Blackwell: London, UK, 2012. [Google Scholar]
- Cheynet, F.; Guyot, L.; Richard, O.; Layoun, W.; Gola, R. Discomallear and malleomandibular ligaments: Anatomical study and clinical applications. Surg. Radiol. Anat. 2003, 25, 152–157. [Google Scholar] [CrossRef]
- Connelly, S.T.; Tartaglia, G.M.; Silva, R.G. Contemporary Management of Temporomandibular Disorders. Fundamentals and Pathways to Diagnosis, 1st ed.; Springer: Zurich, Switzerland, 2019. [Google Scholar]
- Olmos, S.R.; Kritz–Silverstein, D.; Halligan, W.; Silverstein, S.T. The effect of condyle fossa relationships on head posture. J. Craniomand. Pract. 2005, 23, 48–52. [Google Scholar] [CrossRef]
- Von Piekartz, H.J.M.; Schouten, S.; Aufdemkampe, G. Neurodynamic responses in children with migraine or cervicogenic headache versus a control group. A comparative study. Man. Ther. 2007, 12, 153–160. [Google Scholar] [CrossRef]
- Wei, W. Neural Mechanisms of Motion Processing in the Mammalian Retina. Annu. Rev. Vis. Sci. 2018, 4, 165–192. [Google Scholar] [CrossRef] [PubMed]
- D’Attilio, M.; Filippi, M.R.; Femminella, B.; Festa, F.; Tecco, S. The influence of an experimentally–induced malocclusion on vertebral alignment in rats: A controlled pilot study. Cranio 2005, 23, 119–129. [Google Scholar] [CrossRef]
- D’Attilio, M.; Scarano, A.; Quaranta, A.; Festa, F.; Caputi, S.; Piattelli, A. Modification of condyle anatomy following a monolateral bite rise: A histological study in rat. Int. J. Immunopathol. Pharmacol. 2007, 20, 43–47. [Google Scholar] [CrossRef] [PubMed]
- Cardinal, L.; da Silva, T.R.; Andujar, A.L.F.; Gribel, B.F.; Dominguez, G.C.; Janakiraman, N. Evaluation of the three-dimensional (3D) position of cervical vertebrae in individuals with unilateral posterior crossbite. Clin. Oral Investig. 2022, 26, 463–469. [Google Scholar] [CrossRef] [PubMed]
- Šedý, J. Response to: Cardinal L, da Silva TR, Andujar ALF, Gribel BF, Dominguez GC, Janakiraman N. Evaluation of the three-dimensional (3D) position of cervical vertebrae in individuals with unilateral posterior crossbite. Clin. Oral Invest. 2021, 25, 6961. [Google Scholar] [CrossRef]
- Di Vece, L.; Faleri, G.; Picciotti, M.; Guido, L.; Giorgetti, R. Does a transverse maxillary deficit affect the cervical vertebrae? A pilot study. Am. J. Orthod. Dentofacial. Orthop. 2010, 137, 515–519. [Google Scholar] [CrossRef]
- McGuinness, N.J.; McDonald, J.P. Changes in natural head position observed immediately and one year after rapid maxillary expansion. Eur. J. Orthod. 2006, 28, 126–134. [Google Scholar] [CrossRef]
- Greenbaum, T.; Dvir, Z.; Reiter, S.; Winocur, E. Cervical flexion-rotation test and physiological range of motion—A comparative study of patients with myogenic temporomandibular disorder versus healthy subjects. Musculoskelet. Sci. Pract. 2017, 27, 7–13. [Google Scholar] [CrossRef]
- Korbmacher, H.; Koch, L.; Eggers-Stroeder, G.; Kahl-Nieke, B. Associations between orthopaedic disturbances and unilateral crossbite in children with asymmetry of the upper cervical spine. Eur. J. Orthod. 2007, 29, 100–104. [Google Scholar] [CrossRef]
- Milidonis, M.K.; Kraus, S.L.; Segal, R.L.; Widmer, C.G. Genioglossi muscle activity in response to changes in anterior/neutral head posture. Am. J. Orthod. Dentofacial. Orthop. 1993, 103, 39–44. [Google Scholar] [CrossRef]
- Mohl, N. Head posture and its role in occlusion. Int. J. Orthod. 1977, 15, 6–14. [Google Scholar] [PubMed]
- Ohmure, H.; Miyawaki, S.; Nagata, J.; Ikeda, K.; Yamasaki, K.; Al–Kalaly, A. Influence of forward head posture on condylar position. J. Oral Rehabil. 2008, 35, 795–800. [Google Scholar] [CrossRef] [PubMed]
- Paco, M.; Duarte, J.A.; Pinho, T. Orthodontic Treatment and Craniocervical Posture in Patients with Temporomandibular Disorders: An Observational Study. Int. J. Environ. Res. Public Health 2021, 18, 3295. [Google Scholar] [CrossRef] [PubMed]
- Sandoval, C.; Díaz, A.; Manríquez, G. Relationship between craniocervical posture and skeletal class: A statistical multivariate approach for studying Class II and Class III malocclusions. Cranio 2019, 29, 1–8. [Google Scholar] [CrossRef]
- Proffit, W.R. Contemporary Orthodontics, 6th ed.; Elsevier: New York, NY, USA, 2019. [Google Scholar]
- McNamara, J.A., Jr. Early intervention in the transverse dimension: Is it worth the effort? Am. J. Orthod. Dentofacial. Orthop. 2002, 121, 572–574. [Google Scholar] [CrossRef]
- Michelotti, A.; Iodice, G.; Piergentili, M.; Farella, M.; Martina, R. Incidence of temporomandibular joint clicking in adolescents with and without unilateral posterior cross-bite: A 10-year follow-up study. J. Oral Rehabil. 2016, 43, 16–22. [Google Scholar] [CrossRef]
- Fiorrilo, L. Spine and TMJ: A Pathophysiology report. J. Funct. Morphol. Kinesiol. 2020, 5, 24. [Google Scholar] [CrossRef]
- Cruccu, G.; Ongerboer de Visser, B.W. The jaw reflexes. The International Federation of Clinical Neurophysiology. Electroencephalogr. Clin. Neurophysiol. 1999, 52, 243–247. [Google Scholar]
- Morquette, P.; Lavoie, R.; Fhima, M.D.; Lamoureux, X.; Verdier, D.; Kolta, A. Generation of the masticatory central pattern and its modulation by sensory feedback. Prog. Neurobiol. 2012, 96, 340–355. [Google Scholar] [CrossRef]
- Dellow, P.G.; Lund, J.P. Evidence for central timing of rhythmical mastication. J. Physiol. 1971, 215, 1–13. [Google Scholar] [CrossRef]
- Sessle, B.J.; Yao, D.; Nishiura, H.; Yoshino, K.; Lee, J.C.; Martin, R.E.; Murray, G.M. Properties and plasticity of the primate somatosensory and motor cortex related to orofacial sensorimotor function. Clin. Exp. Pharmacol. Physiol. 2005, 32, 109–114. [Google Scholar] [CrossRef] [PubMed]
- Hamm, T.M.; Trank, T.V.; Turkin, V.V. Correlations between neurograms and locomotor drive potentials in motoneurons during fictive locomotion: Implications for the organization of locomotor commands. Prog. Brain Res. 1999, 123, 331–339. [Google Scholar] [PubMed]
- Rocabado, M. Theoretical and Hans–on Master Class: Cervical and Craniomandibular Dysfunctions, 1st ed.; SynergyOAcademy: Cluj-Napoca, Romania, 2018. [Google Scholar]
- Rocabado, M. Theoretical and Hans–on Master Class II: Cervical and Craniomandibular Dysfunctions, 1st ed.; SynergyOAcademy: Cluj-Napoca, Romania, 2018. [Google Scholar]
- Goadsby, P.J.; Ratsch, T. On the functional neuroanatomy of neck pain. Cephalalgia 2008, 28, 1–7. [Google Scholar] [CrossRef]
- Campbell, D.G.; Parsons, C.M. Referred head pain and its concomitants. J. Nerv. Ment. Dis. 1944, 99, 544–551. [Google Scholar] [CrossRef]
- Feinstein, B.; Langton, J.B.K.; Jameson, R.M.; Schiller, F. Experiments on referred pain from deep somatic tissues. J. Bone Joint Surg. 1954, 36, 981–997. [Google Scholar] [CrossRef]
- Dreyfuss, P.; Michaelsen, M.; Fletcher, D. Atlanto-occipital and lateral atlanto-axial joint pain patterns. Spine 1994, 19, 1125–1131. [Google Scholar] [CrossRef]
- Dwyer, A.; Aprill, C.; Bogduk, N. Cervical zygapophysial joint pain patterns I: A study in normal volunteers. Spine 1990, 15, 453–457. [Google Scholar]
- Schellhas, K.P.; Smith, M.D.; Gundry, C.R.; Pollei, S.R. Cervical discogenic pain: Prospective correlation of magnetic resonance imaging and discography in asymptomatic subjects and pain suff erers. Spine 1996, 21, 300–312. [Google Scholar] [CrossRef]
- Grubb, S.A.; Kelly, C.K. Cervical discography: Clinical implications from 12 years of experience. Spine 2000, 25, 1382–1389. [Google Scholar] [CrossRef]
- Ashina, S.; Bendtsen, L.; Lyngberg, A.C.; Lipton, R.B.; Hajiyeva, N.; Jensen, R. Prevalence of neck pain in migraine and tension-type headache: A population study. Cephalalgia 2015, 35, 211–219. [Google Scholar] [CrossRef]
- Johnston, M.M.; Jordan, S.E.; Charles, A.C. Pain referral patterns of the C1 to C3 nerves: Implications for headache disorders. Ann. Neurol. 2013, 74, 145–148. [Google Scholar] [CrossRef] [PubMed]
- Shimohata, K.; Hasegawa, K.; Onodera, O.; Nishizawa, M.; Shimohata, T. The clinical features, risk factors, and surgical treatment of cervicogenic headache in patients with cervical spine disorders. Headache 2017, 57, 1109–1117. [Google Scholar] [CrossRef] [PubMed]
- Amevo, B.; Aprill, C.; Bogduk, N. Abnormal instantaneous axes of rotation in patients with neck pain. Spine 1992, 17, 748–756. [Google Scholar] [CrossRef] [PubMed]
- Watson, D.H.; Trott, P.H. Cervical headache: An investigation of natural head posture and upper cervical flexor muscle performance. Cephalalgia 1993, 13, 272–284. [Google Scholar] [CrossRef]
- Okeson, J.P. Orofacial Pain: Guidelines for Assessment, Diagnosis and Management, 1st ed.; Quintessence: Chicago, IL, USA, 1996. [Google Scholar]
- Paesani, D.A. Bruxism: Theory and Practice, 1st ed.; Quintessence Publishing: Berlin, Germany, 2010. [Google Scholar]
- Harness, D.M.; Peltier, B. Comparison of MMPI scores with self-report of sleep disturbance and bruxism in the facial pain population. Cranio 1992, 10, 70–74. [Google Scholar] [CrossRef]
- Pierce, C.J.; Chrisman, K.; Bennett, M.E.; Close, J.M. Stress, anticipatory stress, and psychologic measures related to sleep bruxism. J. Orofac. Pain 1995, 9, 51–56. [Google Scholar]
- Rugh, J.D.; Harlan, J. Nocturnal bruxism and temporomandibular disorders. Adv. Neurol. 1988, 49, 329–341. [Google Scholar]
- Bandodkar, S.; Tripathi, S.; Chand, P.; Singh, S.V.; Arya, D.; Kumar, L.; Singh, M.; Singhal, R.; Tripathi, A. A study to evaluate psychological and occlusal parameters in bruxism. J. Oral Biol. Craniofac. Res. 2022, 12, 38–41. [Google Scholar] [CrossRef]
- Franks, A.S. Cervical spondylosis presenting as the facial pain of temporomandibular joint disorder. Ann. Phys. Med. 1968, 9, 193–196. [Google Scholar] [CrossRef]
- Koopman, J.S.; Dieleman, J.P.; Huygen, F.J.; de Mos, M.; Martin, C.G.; Sturkenboom, M.C. Incidence of facial pain in the general population. Pain 2009, 147, 122–127. [Google Scholar] [CrossRef]
- Choi, I.I.; Jeon, S.R. Neuralgias of the head: Occipital neuralgia. J. Korean Med. Sci. 2016, 31, 479–488. [Google Scholar] [CrossRef] [PubMed]
- Khanfour, A.A.; El Sekily, N.M. Relation of the vertebral artery segment from C1 to C2 vertebrae: An anatomical study. Alexandria J. Med. 2015, 51, 143–151. [Google Scholar] [CrossRef]
- Allen, W. The varieties of the atlas in the human subject, and the homologies of its transverse processes. J. Anat. Physiol. 1879, 14, 18–27. [Google Scholar] [PubMed]
- Pekala, P.A.; Henry, B.M.; Pekala, J.R.; Hsieh, W.C.; Vikse, J.; Sanna, B.; Walocha, J.A.; Tubbs, R.S.; Tomaszewski, K.A. Prevalence of foramen arcuale and its clinical significance: A meta-analysis of 55,985 subjects. J. Neurosurg. Spine 2017, 27, 276–290. [Google Scholar] [CrossRef] [PubMed]
- Friedrich, R.E. Ponticulus posticus is a frequent radiographic finding on lateral cephalograms in nevoid basal cell carcinoma syndrome (Gorlin-Goltz syndrome). Anticancer Res. 2014, 34, 7395–7399. [Google Scholar]
- Limousin, C.A. Foramen arcuale and syndrome of Barre-Lieou. Its surgical treatment. Int. Orthop. 1980, 4, 19–23. [Google Scholar] [CrossRef]
- Li, Y.; Peng, B. Pathogenesis, Diagnosis, and Treatment of Cervical Vertigo. Pain Physician 2015, 18, E583–E595. [Google Scholar]
- Travell, J.G.; Simons, D. Myofascial Pain and Dysfunction, 1st ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2013. [Google Scholar]
- Zhuang, X.; Tan, S.; Huang, Q. Understanding of myofascial trigger points. Chin. Med. J. 2014, 127, 4271–4277. [Google Scholar]
- Gerwin, R.D.; Dommerholt, J.; Shah, J.P. An expansion of Simons integrated hypothesis of trigger point formation. Curr. Pain Headache Rep. 2004, 8, 468–475. [Google Scholar] [CrossRef]
- Sharav, Y.; Singer, E.; Schmidt, E.; Dionne, R.A.; Dubner, R. The analgesic effect of amitriptyline on chronic facial pain. Pain 1987, 31, 199–209. [Google Scholar] [CrossRef]
- Clarkson, E.; Jung, E. Atypical Facial Pain. Dent. Clin. North Am. 2020, 64, 249–253. [Google Scholar] [CrossRef] [PubMed]
- May, A.; Hoffmann, J. Facial pain beyond trigeminal neuralgia. Curr. Opin. Neurol. 2021, 34, 373–377. [Google Scholar] [CrossRef] [PubMed]
- Marklund, M.; Braem, M.J.A.; Verbraecken, J. Update on oral appliance therapy. Eur. Respir. Rev. 2019, 28, 190083. [Google Scholar] [CrossRef] [PubMed]
- Antonaci, F.; Ghirmai, S.; Bono, S.; Sandrini, G.; Nappi, G. Cervicogenic headache: Evaluation of the original diagnostic criteria. Cephalalgia 2001, 21, 573–583. [Google Scholar] [CrossRef] [PubMed]
- Van Suijlekom, J.A.; de Vet, H.C.W.; van den Berg, S.G.M.; Weber, W.E.J. Interobserver reliability of diagnostic criteria for cervicogenic headache. Cephalalgia 1999, 19, 817–823. [Google Scholar] [CrossRef] [PubMed]
- van Suijlekom, H.A.; de Vet, H.C.W.; van den Berg, S.G.M.; Weber, W.E.J. Interobserver reliability in physical examination of the cervical spine in patients with headache. Headache 2000, 40, 581–586. [Google Scholar] [CrossRef]
- Grzesiak, R.C. Psychologic considerations in temporomandibular dysfunction. A biopsychosocial view of symptom formation. Dent. Clin. North Am. 1991, 35, 209–226. [Google Scholar] [CrossRef]
- Fillingim, R.B.; Ohrbach, R.; Greenspan, J.D.; Sanders, A.E.; Rathnayaka, N.; Maixner, W.; Slade, G.D. Associations of Psychologic Factors with Multiple Chronic Overlapping Pain Conditions. J. Oral Facial Pain Headache 2020, 34, 85–100. [Google Scholar] [CrossRef]
- Van Suijlekom, H.; Van Zundert, J.; Narouze, S.; Van Kleef, M.; Mekhail, N. Cervicogenic headache. Pain Pract. 2010, 10, 124–130. [Google Scholar] [CrossRef]
- Lampl, C.; Rudolph, M.; Deligianni, C.I.; Mitsikostas, D.D. Neck pain in episodic migraine: Premonitory symptom or part of the attack? J. Headache Pain 2015, 16, 566. [Google Scholar] [CrossRef]
- Kuhn, W.F.; Kuhn, S.C.; Gilberstadt, H. Occipital neuralgias: Clinical recognition of a complicated headache. A case series and literature review. J. Orofac. Pain 1997, 11, 158–165. [Google Scholar]
- de Sousa, J.E.; Halfon, M.J.; Bonardo, P.; Reisin, R.C.; Fernández Pardal, M.M. Different pain patterns in patients with vertebral artery dissections. Neurology 2005, 64, 925–926. [Google Scholar] [CrossRef] [PubMed]
- Saeed, A.B.; Shuaib, A.; Al Sulaiti, G.; Emery, D. Vertebral artery dissection: Warning symptoms, clinical features and prognosis in 26 patients. Can. J. Neurol. Sci. 2000, 27, 292–296. [Google Scholar] [CrossRef] [PubMed]
- Campos, C.R.; Calderaro, M.; Scaff, M.; Conforto, A.B. Primary headaches and painful spontaneous cervical artery dissection. J. Headache Pain 2007, 8, 180–184. [Google Scholar] [CrossRef] [PubMed]
- Hack, G.D.; Koritzer, R.T.; Robinson, W.L.; Hallgren, R.C.; Greenman, P.E. Anatomic relation between the rectus capitis posterior minor muscle and the dura mater. Spine 1995, 20, 2484–2486. [Google Scholar] [CrossRef]
- Hallgren, R.C.; Pierce, S.J.; Prokop, L.L.; Rowan, J.J.; Angela, L.S. Electromyographic activity of rectus capitis posterior minor muscles associated with voluntary retraction of the head. Spine J. 2014, 14, 104–112. [Google Scholar] [CrossRef]
- Hallgren, R.C.; Pierce, S.J.; Sharma, D.B.; Rowan, J.J. Forward Head Posture and Activation of Rectus Capitis Posterior Muscles. J. Am. Osteopath. Assoc. 2017, 117, 24–31. [Google Scholar] [CrossRef]
- Blumenfeld, A.; Siavoshi, S. The challenges of cervicogenic headache. Curr. Pain Headache Rep. 2008, 22, 47. [Google Scholar] [CrossRef]
- Lance, J.W.; Anthony, M. Neck tongue syndrome on sudden turning of the head. J. Neurol. Neurosurg. Psychiatr. 1980, 43, 97–101. [Google Scholar] [CrossRef]
- Bogduk, N. An anatomical basis for neck tongue syndrome. J. Neurol. Neurosurg. Psychiatr. 1981, 44, 202–208. [Google Scholar] [CrossRef]
- Jansen, J.; Markakis, E.; Rama, B.; Hildebrandt, J. Hemicranial attacks or permanent hemicrania—A sequel of upper cervical root compression. Cephalalgia 1989, 9, 123–130. [Google Scholar] [PubMed]
- Poletti, C.E.; Sweet, W.H. Entrapment of the C2 root and ganglion by the atlanto-epistrophic ligament: Clinical syndrome and surgical anatomy. Neurosurgery 1990, 27, 288–291. [Google Scholar] [CrossRef] [PubMed]
- Jansen, J.; Bardosi, A.; Hildebrandt, J.; Lucke, A. Cervicogenic, hemicranial attacks associated with vascular irritation or compression of the cervical nerve root C2. Clinical manifestations and morphological findings. Pain 1989, 39, 203–212. [Google Scholar] [CrossRef]
- Kuritzky, A. Cluster headache-like pain caused by an upper cervical meningioma. Cephalalgia 1984, 4, 185–186. [Google Scholar] [CrossRef] [PubMed]
- Sharma, R.R.; Parekh, H.C.; Prabhu, S.; Gurusinghe, N.T.; Bertolis, G. Compression of the C-2 root by a rare anomalous ectatic vertebral artery. J.Neurosurg. 1993, 78, 669–672. [Google Scholar] [CrossRef] [PubMed]
- Hildebrandt, J.; Jansen, J. Vascular compression of the C2 and C3 roots—Yet another cause of chronic intermittent hemicrania? Cephalalgia 1984, 4, 167–170. [Google Scholar] [CrossRef]
- Hanzelka, T.; Dušek, J.; Ocásek, F.; Kučera, J.; Šedý, J.; Beneš, J.; Pavlíková, G.; Foltán, R. Movement of the patient and the cone beam computed tomography scanner: Objectives and possible solutions. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2013, 116, 769–773. [Google Scholar] [CrossRef][Green Version]
- Minervini, G. Teledentistry in the management of patients with dental and temporomandibular disorders. Biomed Res. Int. 2022, 2022, 7091153. [Google Scholar] [CrossRef]
- Haas, M.; Bronfort, G.; Evans, R.; Schulz, C.; Vavrek, D.; Takaki, L.; Hanson, L.; Leininger, B.; Neradilek, M.B. Dose-response and efficacy of spinal manipulation for care of cervicogenic headache: A dual-center randomized controlled trial. Spine J. 2018, 18, 1741–1754. [Google Scholar] [CrossRef]
- Jull, G.; Trott, P.; Potter, H.; Zito, G.; Niere, K.; Shirley, D.; Emberson, J.; Marschner, I.; Richardson, C. A randomized controlled trial of exercise and manipulative therapy for cervicogenic headache. Spine 2002, 27, 1835–1843. [Google Scholar] [CrossRef]
- Thompson, J.R.; Brody, A.G. Factors in the position of the mandible. J. Am. Dent. Assoc. 1942, 29, 925–941. [Google Scholar] [CrossRef]
- Hansson, T.; Henée, W.; Hesse, J. Funktionsstörungen im Kausystem, 1st ed.; Hüthig Buch-Verlag: Heidelberg, Germany, 1990. [Google Scholar]
- Hansson, T.L.; Christensen Minor, C.A.; Wagnon Taylor, D.L. Physical Therapy in Craniomandibular Disorders, 1st ed.; Quintessenz-Verlag: Berlin, Germany, 1992. [Google Scholar]
- Freesmeyer, W.B. Zahnärztliche Funktionstherapie, 1st ed.; Hanser-Verlag: München, Germany, 1993. [Google Scholar]
- Gelb, H. New Concepts in Craniomandibular and Chronic Pain Management, 1st ed.; Mosby-Wolfe: London, UK, 1994. [Google Scholar]
- Bergbreiter, C. Untersuchung über die Zusammenhänge Zwischen der Fehlstatik und den Funktionellen Befunden des Craniomandibulären Systems; Inaug. Diss., Med. Fak.: Tübingen, Germany, 1993. [Google Scholar]
- Stute, W. Sakrokraniomandibuläre Integrationsstörungen. In Ganzheitliche Zahnheilkunde in der Praxis; Becker, W., Ed.; Spitta-Verlag: Balingen, Germany, 1996. [Google Scholar]
- Wallace, C.; Klineberg, I. Management of Craniomandibular Disorders. Part II: Assessment of Patients with Craniocervical Dysfunction. J. Orofacial Pain 1994, 8, 42–54. [Google Scholar] [PubMed]
- Coy, R.E.; Flocken, J.E.; Adib, F. Musculoskeletal etiology and therapy of craniomandibular pain and dysfunction. Cranio Clin. Int. 1991, 1, 163–173. [Google Scholar] [PubMed]
- Shup, W.; Zernial, P. Zahnärztliche und kieferorthopädische Behandlungsmöglichkeiten bei Craniomandibulärer Dysfunktion. Fachvereinigung deutscher Kieferorthopäden. (KFO-1G); W. Scupp: Köln, Germany, 1996. [Google Scholar]
- Rocabado, M. Atlas Clínico II, Congruencia Cráneo-cérvico-mandibular, Aplicación Clínica, 1st ed.; Instituto Rocabado: Santiago de Chile, Chile, 2021. [Google Scholar]
- Aniri, M.; Jull, G.; Bullock-Saxton, J.; Darnell, R.; Lander, C. Cervical musculoskeletal impairment in frequent intermittent headache. Part 2: Subjects with concurrent headache types. Cephalgia 2007, 27, 891–898. [Google Scholar] [CrossRef]
- Dreyfuss, P.; Dreser, S.J.; Cole, A.; Mayo, K. Sacroiliac joint pain. J. Am. Acad. Orthop. Surg. 2004, 12, 255–265. [Google Scholar] [CrossRef]
- Hilton, J. On Rest and Pain: A Course of Lectures on the Influence of Mechanical and Physiological Rest in the Treatment of Accidents and Surgical Diseases, and the Diagnostic Value of Pain, delivered at the Royal College of Surgeons of England in the years 1860, 1861, and 1862; William Wood & Company: West Chester, PA, USA, 1863. [Google Scholar]
- Rocabado, M.; Gutierrez, R.; Gutierrez, M.F.; Gutierrez, M.J. Case report: Anterior open bite correction treatment by dental treatment and physical therapy through craniocervical mandibular and occlusal stabilization. Cranio 2021, 10, 1–6. [Google Scholar] [CrossRef]
- Kang, J.H. Neck associated factors related to migraine in adolescents with painful temporomandibular disorders. Acta Odontol Scand. 2021, 79, 43–51. [Google Scholar] [CrossRef]
- von Piekartz, H.; Lüdtke, K. Effect of treatment of temporomandibular disorders (TMD) in patients with cervicogenic headache: A single-blind, randomized controlled study. Cranio 2011, 29, 43–56. [Google Scholar] [CrossRef]
- Williamson, E.H. Eugene, H. Williamson on occlusion and TMJ dysfunction. Interview by S. Brandt. J. Clin. Orthod 1981, 15, 333–350. [Google Scholar]
- Williamson, E.H. Eugene, H. Williamson on occlusion and TMJ dysfunction (Part 2). J. Clin. Orthod. 1981, 15, 393–404+409–410. [Google Scholar]
- Dawson, P.E. Functional Occlusion: From TMJ to Smile Design, 1st ed.; Elsevier: St. Louis, MO, USA, 2007. [Google Scholar]
- Greven, G.; Piehslinger, E.; Haberl, T.; Betzl, C. Correlation between Internal Derangement of the Temporo-Mandibular Joint and Ipsi-Lateral Mediotrusive Molar Interferences-A Condylographic Study Using Virtual Articulation. Int. J. Dent. Oral Health 2020, 6, 1–6. [Google Scholar]
- Gross, A.; Langevin, P.; Burnie, S.J.; Bédard-Brochu, M.S.; Empey, B.; Dugas, E.; Faber-Dobrescu, M.; Andres, C.; Graham, N.; Goldsmith, C.H.; et al. Manipulation and mobilisation for neck pain contrasted against an inactive control or another active treatment. Cochrane Database Syst. Rev. 2015, 23, 4249. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Zhang, X.L.; Ding, H.; Tao, Y.Q.; Zhan, H.S. Comparative study on effects of manipulation treatment and transcutaneous electrical nerve stimulation on patients with cervicogenic headache. J. Chin. Integr. Med./Zhong. Xi. Yi. 2007, 5, 403–406. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Deyo, R.A.; Walsh, N.E.; Schoenfeld, L.S.; Ramamurthy, S. Can trials of physical treatments be blinded? The example of transcutaneous electrical nerve stimulation for chronic pain. Am. J. Phys. Med. Rehabil. 1990, 69, 6–10. [Google Scholar] [CrossRef]































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| A. Any headache fulfilling criterion C. |
| B. Clinical and/or imaging evidence of a disorder or lesion within the cervical spine or soft tissues of the neck, known to be able to cause headache. |
| C. Evidence of causation demonstrated by at least two of the following: 1. headache has developed in temporal relation to the onset of the cervical disorder or appearance of the lesion; 2. headache has significantly improved or resolved in parallel with improvement in or resolution of the cervical disorder or lesion; 3. cervical range of motion is reduced and headache is made significantly worse by provocative maneuvers; 4. headache is abolished following diagnostic blockade of a cervical structure or its nerve supply. |
| D. Not better accounted for by another ICHD-3 diagnosis. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Šedý, J.; Rocabado, M.; Olate, L.E.; Vlna, M.; Žižka, R. Neural Basis of Etiopathogenesis and Treatment of Cervicogenic Orofacial Pain. Medicina 2022, 58, 1324. https://doi.org/10.3390/medicina58101324
Šedý J, Rocabado M, Olate LE, Vlna M, Žižka R. Neural Basis of Etiopathogenesis and Treatment of Cervicogenic Orofacial Pain. Medicina. 2022; 58(10):1324. https://doi.org/10.3390/medicina58101324
Chicago/Turabian StyleŠedý, Jiří, Mariano Rocabado, Leonardo Enrique Olate, Marek Vlna, and Radovan Žižka. 2022. "Neural Basis of Etiopathogenesis and Treatment of Cervicogenic Orofacial Pain" Medicina 58, no. 10: 1324. https://doi.org/10.3390/medicina58101324
APA StyleŠedý, J., Rocabado, M., Olate, L. E., Vlna, M., & Žižka, R. (2022). Neural Basis of Etiopathogenesis and Treatment of Cervicogenic Orofacial Pain. Medicina, 58(10), 1324. https://doi.org/10.3390/medicina58101324